
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 07 January 2022
Sec. Schizophrenia
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.825681
This article is part of the Research Topic Negative Symptoms and Cognitive Impairment in Schizophrenia-Spectrum Disorders View all 15 articles
 Lynn Mørch-Johnsen1,2*
Lynn Mørch-Johnsen1,2* Runar Elle Smelror1,3
Runar Elle Smelror1,3 Dimitrios Andreou1,3,4
Dimitrios Andreou1,3,4 Claudia Barth1,3Cecilie Johannessen5
Claudia Barth1,3Cecilie Johannessen5 Kirsten Wedervang-Resell1
Kirsten Wedervang-Resell1 Laura A. Wortinger1,3Ricardo Díaz6Gamaliel Victoria7
Laura A. Wortinger1,3Ricardo Díaz6Gamaliel Victoria7 Torill Ueland8,9
Torill Ueland8,9 Ole A. Andreassen1,8Anne M. Myhre8,10
Ole A. Andreassen1,8Anne M. Myhre8,10 Bjørn Rishovd Rund9,11Rosa Elena Ulloa12
Bjørn Rishovd Rund9,11Rosa Elena Ulloa12 Ingrid Agartz1,3,4,13
Ingrid Agartz1,3,4,13Background: Early-onset psychosis (EOP) is among the leading causes of disease burden in adolescents. Negative symptoms and cognitive deficits predicts poorer functional outcome. A better understanding of the association between negative symptoms and cognitive impairment may inform theories on underlying mechanisms and elucidate targets for development of new treatments. Two domains of negative symptoms have been described in adult patients with schizophrenia: apathy and diminished expression, however, the factorial structure of negative symptoms has not been investigated in EOP. We aimed to explore the factorial structure of negative symptoms and investigate associations between cognitive performance and negative symptom domains in adolescents with EOP. We hypothesized that (1) two negative symptom factors would be identifiable, and that (2) diminished expression would be more strongly associated with cognitive performance, similar to adult psychosis patients.
Methods: Adolescent patients with non-affective EOP (n = 169) were included from three cohorts: Youth-TOP, Norway (n = 45), Early-Onset Study, Norway (n = 27) and Adolescent Schizophrenia Study, Mexico (n = 97). An exploratory factor analysis was performed to investigate the underlying structure of negative symptoms (measured with the Positive and Negative Syndrome Scale (PANSS)). Factor-models were further assessed using confirmatory factor analyses. Associations between negative symptom domains and six cognitive domains were assessed using multiple linear regression models controlling for age, sex and cohort. The neurocognitive domains from the MATRICS Consensus Cognitive Battery included: speed of processing, attention, working memory, verbal learning, visual learning, and reasoning and problem solving.
Results: The exploratory factor analysis of PANSS negative symptoms suggested retaining only a single factor, but a forced two factor solution corroborated previously described factors of apathy and diminished expression in adult-onset schizophrenia. Results from confirmatory factor analysis indicated a better fit for the two-factor model than for the one-factor model. For both negative symptom domains, negative symptom scores were inversely associated with verbal learning scores.
Conclusion: The results support the presence of two domains of negative symptoms in EOP; apathy and diminished expression. Future studies on negative symptoms in EOP should examine putative differential effects of these symptom domains. For both domains, negative symptom scores were significantly inversely associated with verbal learning.
Early-onset psychosis (EOP) is defined as the onset of a psychotic disorder before 18 years of age (1). Although EOP is rare [affecting about 0.05–0.5% of the general population (2–4)], it is among the leading causes of disease burden in adolescents (5). Negative symptoms are present in 37–50% of EOP at illness onset (6, 7), and offer a particular challenge concerning outcome and quality of life as they are associated with poor functional outcome (8), cognitive impairments (9), and multiple treatment failures (6).
Negative symptoms commonly refer to symptoms reflecting diminished normal functions and behaviors, including alogia, blunted affect, anhedonia, asociality, and avolition (10). Studies investigating the factorial structure of different negative symptom rating scales in adult-onset schizophrenia, suggest that negative symptoms consist of two or more factors (11, 12). Most consistently reported and investigated are the two domains: apathy, including avolition, asociality and anhedonia, and diminished expression, including blunted affect and alogia (11, 13–16). Previous studies examining the factorial structure of negative symptoms in the widely used Positive and Negative Syndrome Scale [PANSS; (17)] have confirmed the two domains, and the models have been largely convergent (13, 14, 18). The reported two-factor structure comprise of: (1) an apathy domain, including emotional withdrawal, passive social withdrawal, and active social avoidance and (2) a diminished expression domain, including blunted affect, poor rapport, lack of spontaneity, and motor retardation (13, 14). This structure has been supported by a confirmatory factor analysis in an adult schizophrenia sample (19), and validated against corresponding subdomains of the Brief Negative Symptom Assessment Scale (20). Investigations of the two negative symptom domains, separately, have reported differential associations with other clinical aspects of psychotic disorders and neurobiology, including functional outcome (21), cognitive impairments (22, 23), neuronal task activation (24), and white matter connectivity (25). Although the exact mechanisms still need to be elucidated, these results may indicate different underlying pathophysiology (26), which may require different treatment approaches. Current conceptualizations of negative symptoms advocate the importance of deconstructing this symptom construct into separate symptoms and dimensions to achieve a better understanding of the phenomenology, and the functional and biological correlates (15, 27).
In adult-onset schizophrenia, associations with cognitive deficits have been shown for both apathy and diminished expression when the domains have been investigated separately (26). Specific problems with executive functioning and working memory may be associated with motivational deficits and reduced goal directed behavior in the apathy domain (26). More general cognitive impairments, according to the “cognitive resource limitation model”, have been proposed to contribute to diminished expression symptoms (26, 28, 29). Some studies exploring the putative associations between cognition and the two negative symptom domains, have suggested a stronger association to cognitive impairments for diminished expression, than for apathy (22, 23, 30).
Adolescence is a sensitive developmental period associated with rapid neuro-maturational changes (31). Negative symptoms and cognitive difficulties are particularly challenging as currently available treatment is not adequately effective (32, 33). Studies of children and adolescents with EOP have demonstrated higher genetic heritability, poorer premorbid adjustment, longer duration of untreated psychosis (DUP), more severe illness course and outcome, and higher suicide rate, relative to patients with adult-onset psychosis (7, 34–36). These findings illustrate a crucial need for increased knowledge of pathological mechanisms associated with EOP. In a previous study from our group including an overlapping EOP sample with the present study, negative and disorganized symptoms were found to mediate the relationship between verbal learning and global functioning (37). However, to the best of our knowledge, the factorial structure of negative symptoms and how specific subdomains of negative symptoms relate with cognition, have not yet been investigated in adolescent patients with EOP. A better understanding of the phenomenology of negative symptoms, and how these symptoms relate to cognitive domains may improve early detection and inform theories on underlying mechanisms.
Thus, we aimed to (1) explore the factorial structure of the negative symptom construct and (2) investigate associations between cognitive impairments and negative symptom domains in EOP. We hypothesized that two factors of negative symptoms will be identifiable; an apathy factor and a diminished expression factor, and that diminished expression is more strongly associated with cognitive impairments, in accordance with studies of adult patients [e.g., (22, 23)].
The subject sample included 169 adolescents with non-affective EOP with the following diagnoses: schizophrenia (n = 101), schizophreniform disorder (n = 33), schizoaffective disorder (n = 4), brief psychotic disorder (n = 2) and psychosis not otherwise specified (n = 29). Participants were recruited from three different cohorts: (1) the Thematically Organized Psychosis Study for Youth (Youth-TOP), Norway (n = 45, recruited from 2013 to 2019), (2) the Early-Onset Study, Norway (n = 27, recruited from 2005 to 2007) and (3) the Adolescent Schizophrenia Study, Mexico (n = 97, recruited from 2011 to 2020). The Norwegian cohorts were recruited from adolescent inpatient units and outpatient clinics in the south-east area of Norway (mainly the Oslo area). The Mexican cohort was recruited from an inpatient unit at the Child and Adolescent Psychiatric Hospital in Mexico City.
Inclusion criteria for the current study were: (1) A non-affective psychotic disorder, verified according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) (38), (2) age 12–18 years, and (3) adequate language abilities to complete the interviews and self-rating questionnaires. Patients were excluded if they had a substance-induced psychotic disorder, organic brain disease, previous moderate/severe head injury, or IQ outside of the normal range. IQ was formally tested in the participants from the Youth-TOP and Early-Onset Study using the Wechsler Abbreviated Scale of Intelligence (39), and participants with IQ below 70 were excluded. In the Adolescent Schizophrenia Study, IQ was considered within the normal range if the patient did not have significant developmental delays and was attending regular school without any formal educational support.
All participants (and/or legal guardians if age <16 years) were thoroughly informed about the study and signed a written consent form. The Youth-TOP and Early-Onset Study were approved by the Norwegian South-East Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate. The Adolescent Schizophrenia Study was approved by the Child Psychiatric Hospital Ethics Committee. All studies were conducted in accordance with the Helsinki declaration.
Diagnoses were established according to the DSM-IV, using the following structured interviews: (1) Youth-TOP study: the Schedule for Affective Disorders and Schizophrenia for School Aged Children – Present and Lifetime Version (K-SADS-PL) (40), (2) Early-Onset Study: the Structural Clinical Instrument of Diagnosis for DSM-IV Axis I disorders (SCID-I), module A-D (41), and (3) Adolescent Schizophrenia Study: the Mini International Neuropsychiatric Interview (MINI-KID) (42).
Global functioning was assessed using three different scales: the Youth-TOP study: the Children's Global Assessment Scale (CGAS) (43), (2) Early-Onset Study: the Global Assessment of Functioning Scale, split version (GAF-F) (44), (3) Adolescent Schizophrenia Study: the Personal and Social Performance Scale (PSP) (45).
Characteristic symptoms of psychosis, including negative symptoms were assessed using the PANSS (17). Although the PANSS was originally developed for adults, it has been used in several studies in adolescent patients (46, 47). In line with previous work in adult patients with schizophrenia (13, 14), negative symptom items from the negative symptom factor scores published by Marder and colleagues (48) were included for the exploratory factor analysis. The PANSS items included: n1 (blunted affect), n2 (emotional withdrawal), n3 (poor rapport), n4 (passive/apathetic social withdrawal), n6 (reduced spontaneity and flow of conversation), g7 (motor retardation), g16 (active social avoidance).
Six cognitive domains were investigated based on nine tests from the MATRICS Consensus Cognitive Battery (MCCB) (49): (1) Speed of processing [combining BACS Symbol coding (50), Trail making test, part A (51), and Category fluency (52)], (2) Attention/vigilance (Continuous performance test, identical pairs) (53), (3) Working memory [combining WMS-III Spatial span (54) and Letter-number span (55)], (4) Verbal learning (Hopkins verbal learning test, revised) (56), (5) Visual learning (Brief visuospatial memory test, revised) (57), and (6) Reasoning and problem solving (NAB Mazes) (58). Although the MCCB was developed for adult patients with schizophrenia, the cognitive tests have been successfully used in adolescent EOP patients (59–62) and healthy adolescents (63, 64). The social cognition test (MSCEIT: Managing emotions) (65) included in the MCCB has been shown to be less suitable for adolescents (61) and was therefore excluded from the analyses in the current study. A global composite cognition score was calculated based on the nine included tests.
Information on current use of psychotropic medication was assessed, and chlorpromazine (CPZ) equivalents (66) were calculated for antipsychotic medication.
Statistical analyses were performed with SPSS (version 27), except for the confirmatory factor analysis which was performed using R (version 4.0.5).
Demographic and clinical data were compared between cohorts using analysis of variance (ANOVA) and chi-square statistics. All tests were two-tailed.
The exploratory factor analysis (EFA, Principal Axis Factoring, SPSS) was performed to investigate the underlying structure of negative symptoms. The Kaiser-Meyer-Oklin (KMO) and Bartlett's test of sphericity were calculated to assess sampling adequacy. Number of factors to retain was determined based on Kaiser's criterion of an eigenvalue >1, and visual inspection of the scree plot. As two factors have been demonstrated in adult schizophrenia populations (13, 14, 18) we also explored setting the number of factors to be retained to two. The Promax oblique rotation was applied as we expected factors to be correlated, and items with loadings >0.3 were used for factor interpretation.
To further assess the models derived from the exploratory factor analysis, confirmatory factor analysis was conducted using the Lavaan package in R (67). Because of non-normality of data, the maximum likelihood estimation with robust standard errors and Satorra-Bentler scaled test statistics was used (68). Two models were assessed: (1) a one-factor model (n1, n2, n3, n4, n6, g7 and g16), and (2) the two-factor model of diminished expression (n1, n3, n6 and g7) and apathy (n2, n4 and g16) (13, 14). Goodness-of-fit was evaluated using different indices: chi-square, comparative fit index (CFI >0.95), Tucker-Lewis index (TLI >0.95), root mean square error of approximation (RMSEA <0.06), and standardized root mean square residual (SRMR <0.08) (69). As chi-square may be affected by sample size, a normed chi-square was calculated by dividing the chi-square by degrees of freedom, and a value below 5.0 was considered acceptable (70).
Based on previously published negative symptom factor models in adult-onset schizophrenia using PANSS (13, 14), scores for avolition-apathy (n1 + n3 + n6 + g7) and diminished expression (n2 + n4 + n6) were calculated by summing the scores of items included in each factor. Putative associations between cognitive domains and negative symptom factors were investigated using separate multiple linear regression models, controlling for age, sex, and cohort. Sex-specific associations were assessed by exploring models including sex-by-negative domain interactions. The linear regression models were investigated for influential cases. Standardized residuals >3 were identified for the models in speed of processing (3 cases), working memory (1 case) and global cognition (2 cases). However, Cook's distances did not exceed a value of 1 and all cases were retained in the analyses. The cognitive raw tests scores from the MCCB were transformed to standard scores (Z scores) using the standardization function in SPSS. For composite scores such as speed of processing, working memory and global cognition, Z scores from the individual tests were summated and transformed into a composite Z score, in line with the recommended procedure from the MCCB standardization study (71). The TMT-A score included in the speed of processing domain was reversed as high scores on this test indicate lower performance.
As the cognitive domains are not independent, a modified Bonferroni correction that accounts for correlations between outcome variables was used (72). Applying this method resulted in a p-value threshold of p < 0.018 (accounting for 7 domains and an intra-class correlation coefficient of 0.714).
Significant associations between cognition and negative symptom domains were investigated for the influence of PANSS positive and depressive symptom factors (73) and antipsychotic medication (antipsychotic medication use, and among patient using antipsychotics; CPZ equivalents).
Demographic and clinical data for the patients are presented in Table 1, and comparisons on mean scores on cognitive domains in Table 2. The Adolescent Schizophrenia Study consisted of significantly more males, with greater symptom severity, and lower cognitive performance compared to the Youth-TOP and the Early-Onset study. Patients in the Youth-TOP study had more PANSS negative and disorganized symptoms compared to the Early-Onset study. Use of antipsychotic medication was more prevalent in the Adolescent Schizophrenia Study, but there were no significant differences in medication dose (CPZ-equivalents) between the cohorts.
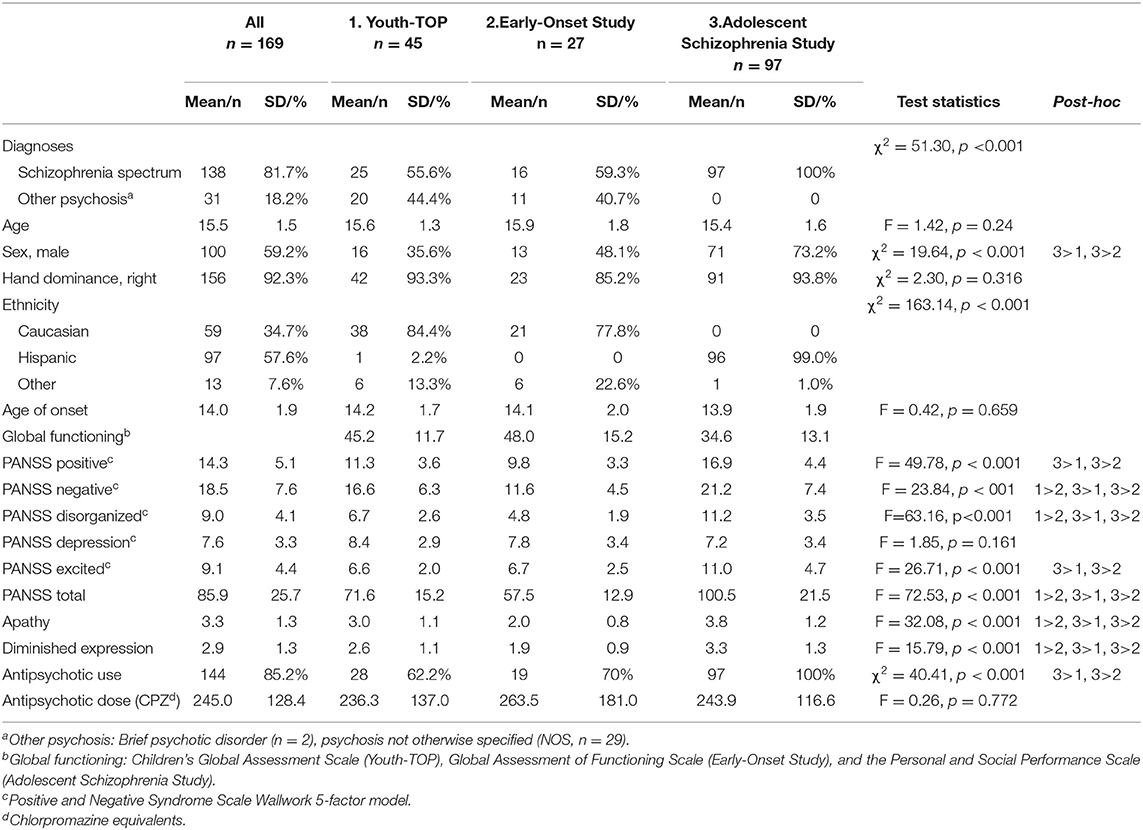
Table 1. Demographic and clinical data.
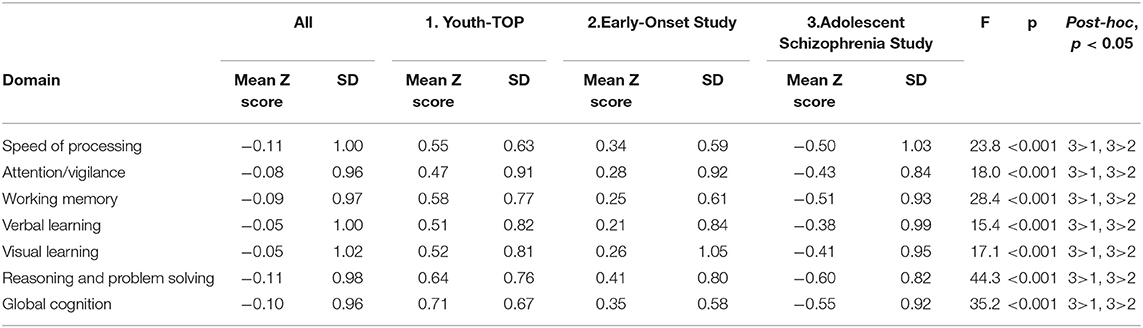
Table 2. Cognition across cohorts.
The exploratory factor analysis showed excellent Kaiser-Meyer-Oklin value of 0.886, and a significant Bartlett's test (p < 0.001), indicating adequate sample size and correlation matrix for factor analysis. When considering both criteria of eigenvalue >1 and visual inspection of the scree plot, one factor was retained (eigenvalue of 4.758, explaining 68% of the variance). As shown in Table 3, when the model was forced to extract two factors, items n2, n4 and g16 loaded highly on factor 1 (corresponding to the avolition-apathy domain) and n1, n3, n6 and g7 loaded highly on factor 2 (corresponding to the diminished expression domain. Factors 1 and 2 were highly correlated 0.798. The two domains showed good internal consistency as demonstrated by a Cronbach's alpha of 0.852 for the apathy domain, and 0.890 for the diminished expression domain.
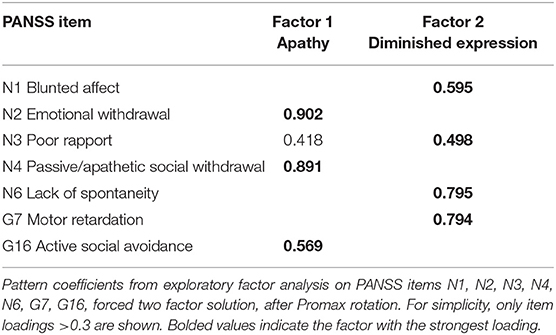
Table 3. Factor structure.
Results from the confirmatory factor analysis for the one- and two-factor models are presented in Table 4. Overall, goodness-of-fit statistics were better for a two-factor model than for a one-factor model, with a smaller chi-square as compared to the one-factor model, and values for normed chi-square (2.84), CFI (0.964), and SRMR (0.033) indicating a good fit.
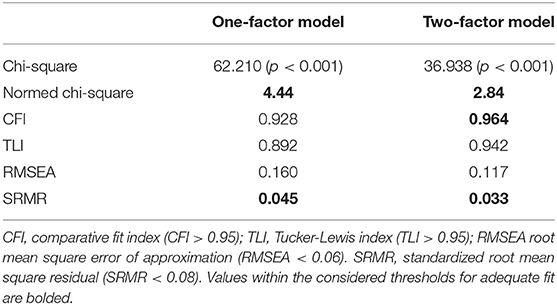
Table 4. Results from confirmatory factor analysis.
Negative symptom scores for both apathy (β = −0.257, p = 0.002) and diminished expression (β = −0.259, p = 0.001) were inversely associated with verbal learning scores. An association was also seen between diminished expression and speed of processing (β = −0.173, p = 0.024), but this result was not significant after correction for multiple comparisons. No other significant associations were observed between the negative symptom domains and cognitive performance (Table 5). There were no significant sex-by-negative domain interactions.
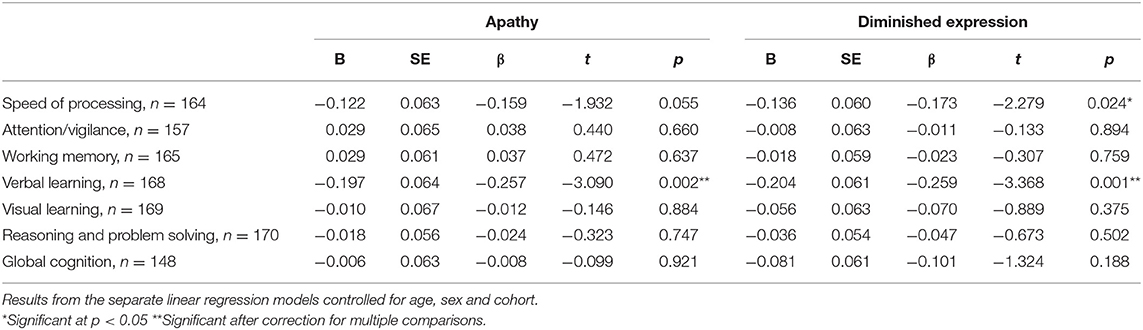
Table 5. Associations between negative symptom domains and cognition.
The association between verbal learning and the two negative symptom domains remained significant after controlling for positive psychotic symptoms, depressive symptoms and antipsychotic medication use and dose.
In the present study, we explored the factorial structure of negative symptoms in patients with EOP and investigated how domains of negative symptoms were related to cognition. Overall, our results indicated a factorial structure of two domains similar to what has been shown for PANSS negative symptoms in adults (13, 14). However, the two factors were highly correlated. Both negative symptom domains were significantly associated with verbal learning.
We performed an exploratory factor analysis to investigate the factorial structure of negative symptoms in EOP as to our knowledge, this has not been investigated in EOP before. When considering standard criteria for factor retention, such as retaining only factors with an eigenvalue above 1 or by investigating the scree plot, the results suggested that only one factor should be retained. However, because of the theoretically supported model of two factors from adult schizophrenia, we explored forcing the extraction of two factors. Interestingly, the pattern of item loadings that emerged were identical to the two-factor model described from factor analytic studies in adult patients with schizophrenia (13, 14). PANSS items addressing blunted affect, poor rapport, lack of spontaneity, and motor retardation loaded the highest on a factor corresponding to a diminished expression domain, and emotional withdrawal, passive social withdrawal, and active social avoidance loaded highest on a second factor corresponding to an apathy domain. We further assessed both a one-factor model and a two-factor model (13, 14) using confirmatory factor analysis. Goodness-of-fit indices were better for the two-factor model, supporting this latent structure of two domains of negative symptoms in EOP. Discrepancies in the results from the exploratory and confirmatory factor analyses may reflect the different methodology and rationale for the two methods. In the exploratory factor analysis, the number of factors are explored in a data-driven approach, while the confirmatory factor analysis tests a predefined factor-model. Our sample size, although large with respect to EOP studies, did not allow for splitting the sample to perform exploratory and confirmatory factor analyses in separate samples. As such, replications of the confirmatory factor analysis should be performed in independent samples for generalizability.
An important implication of investigating subdomains of negative symptoms is that if such subdomains exist, they may have different biological and clinical correlates and may require different treatment strategies (15, 26). For instance, for the apathy domain, behavioral and neural dysfunctions related to motivation and goal-directed behavior have been shown, which have inspired the emerging research on targeted treatment options (26). Generally, models for underlying mechanisms of diminished expression are less clear (15, 26). One line of research points to cognitive deficits underlying symptoms of this domain (26, 28, 29). In support of this theory, a stronger association to cognitive deficits for diminished expression than apathy has been shown in some studies of adult patients with schizophrenia, although the overall differences are not large, and not consistent regarding the cognitive domains involved (22, 23, 30). In the present study of adolescents with EOP, apathy and diminished expression were similarly associated with lower verbal learning performance.
Overall, our results show that, although the factor analysis supports two domains of negative symptoms, these two domains could not be as clearly discriminated in our sample of patients with EOP as has been shown in previous studies of adult patients with schizophrenia (13, 14, 18). This may reflect differences between patients with adult- and early-onset schizophrenia. EOP has been associated with higher genetic heritability, poorer premorbid adjustment, longer duration of untreated psychosis (DUP), more severe illness course and outcome, and higher suicide rate, relative to patients with adult-onset psychosis (7, 34–36). Furthermore, the clinical presentation of underlying pathology may be different in adolescents who are in a period of life where the brain is rapidly changing, and cognitive abilities are developing.
Verbal learning deficits have been associated with earlier age of onset (74), and shown to be one of the earliest predictors of psychosis development in at-risk individuals (75, 76). Thus, verbal learning deficits and negative symptoms may be early markers for psychosis development and functional decline in youth. As cognitive assessment is better at predicting psychosis development in adolescents than in adults (77), our results indicate that clinicians working with young people need to be attentive to both verbal learning difficulties and negative symptoms. The patients presenting with these symptoms may represent a subgroup who may require closer follow-up and quick access to alternative treatment strategies in addition to antipsychotic medication, such as cognitive remediation. Furthermore, the results encourage future studies on how verbal learning and negative symptoms are associated and whether they relate to common underlying neurobiology.
Strengths of the study include a large and well-characterized sample of patients with early onset psychosis, which allowed for performing a factor analysis. Furthermore, a complete and standardized battery (MCCB) for cognitive testing was used. Nevertheless, some limitations should be mentioned. First, as a manifest diagnosis of a psychotic disorder is relatively rare in adolescents, combining samples from geographically different cohorts was necessary to obtain a sufficient sample size, however this may introduce unwanted variation related to cohort. There were significant cohort differences in sex, symptom severity and cognitive scores between cohorts. To address this concern all our multivariate analyses were controlled for cohort. Second, there are limitations to the PANSS as an assessment of negative symptoms (12). The ratings of negative symptoms in PANSS are based only on observation of behaviors, and not the subjective experience of the patients. For symptoms within the domain of apathy, this means that the patient's own experience of pleasure and motivation is not assessed. Newer scales for assessment of negative symptoms have been developed, so called “second-generation rating scales” (12), for instance the Brief Negative Symptom Scale (BNSS) (78) and the Clinical Assessment Interview for Negative Symptoms (CAINS) (79)) have been developed that include assessment of the subjective experience of symptoms within the apathy domain. However, these scales are currently not widely used in adolescents. Third, we included PANSS items for motor retardation (G7) and active social avoidance (G16) in the factor analysis, in line with previous factor analytic studies on negative symptoms in adult patients with schizophrenia. However, it should be noted, that recent guidelines from the European Psychiatric Association (12) on the assessment of negative symptoms advise against including these items as negative symptoms due to their inconsistent loading on the negative symptom factor. Fourth, high total PANSS scores indicate that some patients were in an acute or subacute phase of illness, which may have influenced their cognitive performance. Furthermore, positive symptoms, psychotropic medication, and depression may contribute to secondary negative symptoms. In our multivariate models on cognitive measures, we controlled for such possible secondary sources of negative symptoms (positive symptoms, depression and antipsychotic medication), but this did not change any results. Further, given the young age of the patients, we would expect them to be less influenced by chronicity and medication.
In conclusion, the results support the presence of two domains of negative symptoms in EOP, but the domains were highly correlated, and should be confirmed in independent samples. Contrary to our hypothesis of a stronger association between diminished expression and cognition, we found that for both domains, the negative symptom scores were similarly significantly associated with lower verbal learning scores. Based on the results, we recommend that future studies of negative symptoms in adolescents should examine differential effects of the two negative symptom domains. Furthermore, the association between negative symptoms and verbal learning warrants more studies on how these features are related and whether they for instance share common biological mechanisms that could be targeted for treatment.
The datasets presented in this article are not readily available because of legal and privacy restrictions. Requests to access the datasets should be directed to bHlubi5tb3JjaC1qb2huc2VuQG1lZGlzaW4udWlvLm5v
The studies involving human participants were reviewed and The Youth-TOP and Early-Onset Study were approved by the Norwegian South-East Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate. The Adolescent Schizophrenia Study was approved by the Child Psychiatric Hospital Ethics Committee, Mexico. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
LM-J, RS, and IA took part in designing the analyses for present study. LM-J carried out the statistical analysis. LM-J and RS managed the literature search and wrote the first draft of the manuscript. RS, CJ, KW-R, RD, GV, AM, BR, RU, and IA were involved in data collection. All authors, LM-J, RS, DA, CB, CJ, KW-R, RD, GV, LW, TU, OA, AM, BR, RU, and IA have contributed to and approved the manuscript.
This work was supported by the South-Eastern Norway Regional Health Authority (2019-108, 2019-099, 2004-259, 2006-186, 2020-020) and the Research Council of Norway (223273, 213700, 250358).
OA has received speaker's honorarium from Lundbeck and Sunovion and is a consultant for HealthLytix.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the study participants and the clinicians involved in recruitment and assessments in the studies. Furthermore, we would like to thank the University Center for Information Technology (USIT) at University of Oslo for statistical guidance.
1. Werry JS, McClellan JM, Chard L. Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry. (1991) 30:457–65. doi: 10.1097/00004583-199105000-00017
2. Gillberg C, Wahlström J, Forsman A, Hellgren L, Gillberg IC. Teenage psychoses—epidemiology, classification and reduced optimality in the pre-, peri-and neonatal periods. J Child Psychol Psychiatry. (1986) 27:87–98. doi: 10.1111/j.1469-7610.1986.tb00624.x
3. Boeing L, Murray V, Pelosi A, McCabe R, Blackwood D, Wrate R. Adolescent-onset psychosis: prevalence, needs and service provision. Br J Psychiatry. (2007) 190:18–26. doi: 10.1192/bjp.190.1.18
4. Sikich L. Diagnosis and evaluation of hallucinations and other psychotic symptoms in children and adolescents. Child Adolesc Psychiatric Clin. (2013) 22:655–73. doi: 10.1016/j.chc.2013.06.005
5. Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10-24 years: a systematic analysis. Lancet. (2011) 377:2093–102. doi: 10.1016/S0140-6736(11)60512-6
6. Downs J, Dean H, Lechler S, Sears N, Patel R, Shetty H, et al. Negative symptoms in early-onset psychosis and their association with antipsychotic treatment failure. Schizophr Bull. (2018) 45:69–79. doi: 10.1093/schbul/sbx197
7. Stentebjerg-Olesen M, Pagsberg AK, Fink-Jensen A, Correll CU, Jeppesen P. Clinical characteristics and predictors of outcome of schizophrenia-spectrum psychosis in children and adolescents: a systematic review. J Child Adolesc Psychopharmacol. (2016) 26:410–27. doi: 10.1089/cap.2015.0097
8. Diaz-Caneja CM, Pina-Camacho L, Rodriguez-Quiroga A, Fraguas D, Parellada M, Arango C. Predictors of outcome in early-onset psychosis: a systematic review. NPJ Schizophr. (2015) 1:14005. doi: 10.1038/npjschz.2014.5
9. Nieto RG, Castellanos FX. A meta-analysis of neuropsychological functioning in patients with early onset schizophrenia and pediatric bipolar disorder. J Clin Child Adolesc Psychol. (2011) 40:266–80. doi: 10.1080/15374416.2011.546049
10. Kirkpatrick B, Fenton WS, Carpenter WT Jr, Marder SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull. (2006) 32:214–9. doi: 10.1093/schbul/sbj053
11. Blanchard JJ, Cohen AS. The structure of negative symptoms within schizophrenia: implications for assessment. Schizophr Bull. (2006) 32:238–45. doi: 10.1093/schbul/sbj013
12. Galderisi S, Mucci A, Dollfus S, Nordentoft M, Falkai P, Kaiser S, et al. EPA guidance on assessment of negative symptoms in schizophrenia. Eur Psychiatry. (2021) 64:e23. doi: 10.1192/j.eurpsy.2021.11
13. Fervaha G, Foussias G, Agid O, Remington G. Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr Scand. (2014) 130:290–9. doi: 10.1111/acps.12289
14. Khan A, Liharska L, Harvey PD, Atkins A, Ulshen D, Keefe RSE. Negative symptom dimensions of the positive and negative syndrome scale across geographical regions: implications for social, linguistic, and cultural consistency. Innov Clin Neurosci. (2017) 14:30–40. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5788249/
15. Galderisi S, Mucci A, Buchanan RW, Arango C. Negative symptoms of schizophrenia: new developments and unanswered research questions. Lancet Psychiatry. (2018) 5:664–77. doi: 10.1016/S2215-0366(18)30050-6
16. Foussias G, Remington G. Negative symptoms in schizophrenia: avolition and Occam's razor. Schizophr Bull. (2010) 36:359–69. doi: 10.1093/schbul/sbn094
17. Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
18. Liemburg E, Castelein S, Stewart R, van der Gaag M, Aleman A, Knegtering H, et al. Two subdomains of negative symptoms in psychotic disorders: established and confirmed in two large cohorts. J Psychiatr Res. (2013) 47:718–25. doi: 10.1016/j.jpsychires.2013.01.024
19. Jang SK, Choi HI, Park S, Jaekal E, Lee GY, Cho YI, et al. A two-factor model better explains heterogeneity in negative symptoms: evidence from the positive and negative syndrome scale. Front Psychol. (2016) 7:707. doi: 10.3389/fpsyg.2016.00707
20. Kaliuzhna M, Kirschner M, Carruzzo F, Hartmann-Riemer MN, Bischof M, Seifritz E, et al. Clinical, behavioural and neural validation of the PANSS amotivation factor. Schizophr Res. (2020) 220:38–45. doi: 10.1016/j.schres.2020.04.018
21. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry. (2014) 13:275–87. doi: 10.1002/wps.20167
22. Hartmann-Riemer MN, Hager OM, Kirschner M, Bischof M, Kluge A, Seifritz E, et al. The association of neurocognitive impairment with diminished expression and apathy in schizophrenia. Schizophr Res. (2015) 169:427–32. doi: 10.1016/j.schres.2015.10.032
23. Sevy S, Lindenmayer JP, Khan A, Ljuri I, Kulsa MKC, Jones O. Differential improvement of negative-symptom subfactors after cognitive remediation in low-functioning individuals with schizophrenia. Schizophr Res Cogn. (2020) 19:100145. doi: 10.1016/j.scog.2019.100145
24. Kirschner M, Hager OM, Bischof M, Hartmann MN, Kluge A, Seifritz E, et al. Ventral striatal hypoactivation is associated with apathy but not diminished expression in patients with schizophrenia. J Psychiatry Neurosci. (2016) 41:152–61. doi: 10.1503/jpn.140383
25. Amodio A, Quarantelli M, Mucci A, Prinster A, Soricelli A, Vignapiano A, et al. Avolition-apathy and white matter connectivity in schizophrenia: reduced fractional anisotropy between amygdala and insular cortex. Clin EEG Neurosci. (2018) 49:55–65. doi: 10.1177/1550059417745934
26. Begue I, Kaiser S, Kirschner M. Pathophysiology of negative symptom dimensions of schizophrenia - Current developments and implications for treatment. Neurosci Biobehav Rev. (2020) 116:74–88. doi: 10.1016/j.neubiorev.2020.06.004
27. Kaiser S, Lyne J, Agartz I, Clarke M, Morch-Johnsen L, Faerden A. Individual negative symptoms and domains - Relevance for assessment, pathomechanisms and treatment. Schizophr Res. (2017) 186:39–45. doi: 10.1016/j.schres.2016.07.013
28. Cohen AS, McGovern JE, Dinzeo TJ, Covington MA. Speech deficits in serious mental illness: a cognitive resource issue? Schizophr Res. (2014) 160:173–9. doi: 10.1016/j.schres.2014.10.032
29. Cohen AS, Morrison SC, Brown LA, Minor KS. Towards a cognitive resource limitations model of diminished expression in schizotypy. J Abnorm Psychol. (2012) 121:109–18. doi: 10.1037/a0023599
30. Garcia-Mieres H, Lundin NB, Minor KS, Dimaggio G, Popolo R, Cheli S, et al. A cognitive model of diminished expression in schizophrenia: the interface of metacognition, cognitive symptoms and language disturbances. J Psychiatr Res. (2020) 131:169–76. doi: 10.1016/j.jpsychires.2020.09.008
31. Dahl RE, Allen NB, Wilbrecht L, Suleiman AB. Importance of investing in adolescence from a developmental science perspective. Nature. (2018) 554:441–50. doi: 10.1038/nature25770
32. Fusar-Poli P, Papanastasiou E, Stahl D, Rocchetti M, Carpenter W, Shergill S, et al. Treatments of negative symptoms in schizophrenia: meta-analysis of 168 randomized placebo-controlled trials. Schizophr Bull. (2015) 41:892–9. doi: 10.1093/schbul/sbu170
33. Galderisi S, Kaiser S, Bitter I, Nordentoft M, Mucci A, Sabe M, et al. EPA guidance on treatment of negative symptoms in schizophrenia. Eur Psychiatry. (2021) 64:e21. doi: 10.1192/j.eurpsy.2021.13
34. Hoffmann A, Ziller M, Spengler D. Childhood-onset schizophrenia: insights from induced pluripotent stem cells. Int J Mol Sci. (2018) 19:3829. doi: 10.3390/ijms19123829
35. Ahn K, An S, Shugart YY, Rapoport J. Common polygenic variation and risk for childhood-onset schizophrenia. Mol Psychiatry. (2016) 21:94–6. doi: 10.1038/mp.2014.158
36. Remschmidt H, Martin M, Fleischhaker C, Theisen FM, Hennighausen K, Gutenbrunner C, et al. Forty-two-years later: the outcome of childhood-onset schizophrenia. J Neural Transm. (2007) 114:505–12. doi: 10.1007/s00702-006-0553-z
37. Smelror RE, Rund BR, Lonning V, Jorgensen KN, Wedervang-Resell K, Andreassen OA, et al. Negative and disorganized symptoms mediate the relationship between verbal learning and global functioning in adolescents with early-onset psychosis. Eur Child Adolesc Psychiatry. (2020) 29:1693–703. doi: 10.1007/s00787-020-01479-7
38. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed text rev. Washington, DC: American Psychiatric Association (2000).
39. Wechsler D. Wechsler Abbreviated Scale of Intelligence WASI: Manual. San Antonio, SA: Pearson/PsychCorp (1999).
40. Kaufman J, Birmaher B, Brent D, Rao UMA, Flynn C, Moreci P, et al. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. (1997) 36:980–8. doi: 10.1097/00004583-199707000-00021
41. First MB, Spitzer RL, Gibbon M, Williams JB. Structured clinical interview for DSM-IV-TR axis I disorders, research version. New York, NY: Biometrics Research, New York State Psychiatric Institute (2002).
42. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59 (Suppl 20):22−33;quiz 4–57. Available online at: https://www.psychiatrist.com/jcp/neurologic/neurology/mini-international-neuropsychiatric-interview-mini/
43. Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, et al. A children's global assessment scale (CGAS). Arch Gen Psychiatry. (1983) 40:1228–31. doi: 10.1001/archpsyc.1983.01790100074010
44. Pedersen G, Hagtvet KA, Karterud S. Generalizability studies of the global assessment of functioning–split version. Compr Psychiatry. (2007) 48:88–94. doi: 10.1016/j.comppsych.2006.03.008
45. Morosini PL, Magliano L, Brambilla La, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatrica Scandinavica. (2000) 101:323–9. doi: 10.1111/j.1600-0447.2000.tb10933.x
46. Ropcke B, Eggers C. Early-onset schizophrenia: a 15-year follow-up. Eur Child Adolesc Psychiatry. (2005) 14:341–50. doi: 10.1007/s00787-005-0483-6
47. Savitz AJ, Lane R, Nuamah I, Gopal S, Hough D. Efficacy and safety of paliperidone extended release in adolescents with schizophrenia: a randomized, double-blind study. J Am Acad Child Adolesc Psychiatry. (2015) 54:126–37.e1. doi: 10.1016/j.jaac.2014.11.009
48. Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry. (1997) 58:538–46. doi: 10.4088/JCP.v58n1205
49. Nuechterlein KH, Green MF, Kern RS, Baade LE, Barch DM, Cohen JD, et al. The MATRICS consensus cognitive battery, part 1: test selection, reliability, and validity. Am J Psychiatry. (2008) 165:203–13. doi: 10.1176/appi.ajp.2007.07010042
50. Keefe RSE, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The brief assessment of cognition in schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. (2004) 68:283–97. doi: 10.1016/j.schres.2003.09.011
51. Army Individual Test Battery. Manual of Directions and Scoring. Washington, DC: War Department (1944).
52. Spreen O, Strauss E. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary. 2nd edition. New York, NY: Oxford University Press (1998).
53. Cornblatt BA, Risch NJ, Faris G, Friedman D, Erlenmeyer-Kimling L. The continuous performance test, identical pairs version (CPT-IP): I. new findings about sustained attention in normal families. Psychiatry Res. (1988) 26:223–38. doi: 10.1016/0165-1781(88)90076-5
54. Wechsler D. WMS-III: Wechsler Memory Scale Administration and Scoring Manual. London, UK: The Psychological Corporation (1997).
55. Gold JM, Carpenter C, Randolph C, Goldberg TE, Weinberger DR. Auditory working memory and Wisconsin Card Sorting Test performance in schizophrenia. Arch Gen Psychiatry. (1997) 54:159–65. doi: 10.1001/archpsyc.1997.01830140071013
56. Brandt J, Benedict RHB. Hopkins Verbal Learning Test-Revised: Professional Manual. Lutz, FL: Psychological Assessment Resources (2001).
57. Benedict RHB. Brief Visuospatial Memory Test—Revised. Odessa, FL: Psychological Assessment Resources (1997).
58. Stern RA, White T. Neuropsychological Assessment Battery (NAB). Lutz, FL: Psychological Assessment Resources (2003).
59. Smelror RE, Johannessen C, Wedervang-Resell K, Jørgensen KN, Barth C, Andreou D, et al. Cognitive impairment profile in adolescent early-onset psychosis using the MATRICS Battery: age and sex effects. Neuropsychology. (2021) 35:300–9. doi: 10.1037/neu0000723
60. Victoria G, Apiquian R, Rosetti MF, Ulloa RE. Cognitive impairment and its improvement after six months in adolescents with schizophrenia. Schizophr Res Cogn. (2019) 17:100135. doi: 10.1016/j.scog.2019.100135
61. Holmen A, Juuhl-Langseth M, Thormodsen R, Melle I, Rund BR. Neuropsychological profile in early-onset schizophrenia-spectrum disorders: measured with the MATRICS battery. Schizophr Bull. (2010) 36:852–9. doi: 10.1093/schbul/sbn174
62. Nitzburg GC, Derosse P, Burdick KE, Peters BD, Gopin CB, Malhotra AK, et al. cognitive consensus battery (MCCB) performance in children, adolescents, and young adults. Schizophr Res. (2014) 152:223–8. doi: 10.1016/j.schres.2013.11.023
63. Smelror RE, Jørgensen KN, Lonning V, Kelleher I, Cannon M, DeRosse P, et al. Healthy adolescent performance with standardized scoring tables for the MATRICS consensus cognitive battery: a multisite study. Schizophr Bull. (2019) 45:773–83. doi: 10.1093/schbul/sby131
64. Stone WS, Mesholam-Gately RI, Giuliano AJ, Woodberry KA, Addington J, Bearden CE, et al. Healthy adolescent performance on the MATRICS Consensus Cognitive Battery (MCCB): Developmental data from two samples of volunteers. Schizophr Res. (2016) 172:106–13. doi: 10.1016/j.schres.2016.02.003
65. Mayer JD, Salovey P, Caruso D. Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT© V2.0). Toronto, ON: Multi-Health Systems (2002).
66. Andreasen NC, Pressler M, Nopoulos P, Miller D, Ho BC. Antipsychotic dose equivalents and dose-years: a standardized method for comparing exposure to different drugs. Biol Psychiatry. (2010) 67:255–62. doi: 10.1016/j.biopsych.2009.08.040
67. Rosseel Y. lavaan: an R Package for Structural Equation Modeling. J Stat Softw. (2012) 48:1–36. doi: 10.18637/jss.v048.i02
68. Satorra A, Bentler PM. Corrections to test statistics and standard errors in covariance structure analysis. In: von Eye A, Clogg CC, editor. Latent Variables Analysis: Applications for Developmental Research Thousand Oaks. CA: Sage Publications, Inc. p. 399–419.
69. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. (1999) 6:1–55. doi: 10.1080/10705519909540118
70. Wheaton B, Muthén B, Alwin DF, Summers GF. Assessing reliability and stability in panel models. Sociol Methodol. (1977) 8:84–136. doi: 10.2307/270754
71. Kern RS, Nuechterlein KH, Green MF, Baade LE, Fenton WS, Gold JM, et al. The MATRICS consensus cognitive battery, part 2: co-norming and standardization. Am J Psychiatry. (2008) 165:214–20. doi: 10.1176/appi.ajp.2007.07010043
72. Shi Q, Pavey ES, Carter RE. Bonferroni-based correction factor for multiple, correlated endpoints. Pharm Stat. (2012) 11:300–9. doi: 10.1002/pst.1514
73. Wallwork RS, Fortgang R, Hashimoto R, Weinberger DR, Dickinson D. Searching for a consensus five-factor model of the positive and negative syndrome scale for schizophrenia. Schizophr Res. (2012) 137:246–50. doi: 10.1016/j.schres.2012.01.031
74. Tuulio-Henriksson A, Partonen T, Suvisaari J, Haukka J, Lönnqvist J. Age at onset and cognitive functioning in schizophrenia. Br J Psychiatry. (2004) 185:215–9. doi: 10.1192/bjp.185.3.215
75. Carrión RE, Walder DJ, Auther AM, McLaughlin D, Zyla HO, Adelsheim S, et al. From the psychosis prodrome to the first-episode of psychosis: no evidence of a cognitive decline. J Psychiatr Res. (2018) 96:231–8. doi: 10.1016/j.jpsychires.2017.10.014
76. Seidman LJ, Shapiro DI, Stone WS, Woodberry KA, Ronzio A, Cornblatt BA, et al. Association of neurocognition with transition to psychosis: baseline functioning in the second phase of the North American prodrome longitudinal study. JAMA Psychiatry. (2016) 73:1239–48. doi: 10.1001/jamapsychiatry.2016.2479
77. Zhang T, Cui H, Wei Y, Tang X, Xu L, Hu Y, et al. Neurocognitive assessments are more important among adolescents than adults for predicting psychosis in clinical high risk. Biolo Psychiatry Cogn Neurosci Neuroimaging. (2021). S2451-9022(21)00195-6. doi: 10.1016/j.bpsc.2021.06.015. [Epub ahead of print].
78. Kirkpatrick B, Strauss GP, Nguyen L, Fischer BA, Daniel DG, Cienfuegos A, et al. The brief negative symptom scale: psychometric properties. Schizophr Bull. (2011) 37:300–5. doi: 10.1093/schbul/sbq059
Keywords: apathy, diminished expression, early-onset schizophrenia, MATRICS, MCCB, factor analysis
Citation: Mørch-Johnsen L, Smelror RE, Andreou D, Barth C, Johannessen C, Wedervang-Resell K, Wortinger LA, Díaz R, Victoria G, Ueland T, Andreassen OA, Myhre AM, Rund BR, Ulloa RE and Agartz I (2022) Negative Symptom Domains Are Associated With Verbal Learning in Adolescents With Early Onset Psychosis. Front. Psychiatry 12:825681. doi: 10.3389/fpsyt.2021.825681
Received: 30 November 2021; Accepted: 16 December 2021;
Published: 07 January 2022.
Edited by:
Armida Mucci, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Giulia Maria Giordano, University of Campania Luigi Vanvitelli, ItalyCopyright © 2022 Mørch-Johnsen, Smelror, Andreou, Barth, Johannessen, Wedervang-Resell, Wortinger, Díaz, Victoria, Ueland, Andreassen, Myhre, Rund, Ulloa and Agartz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lynn Mørch-Johnsen, bHlubi5tb3JjaC1qb2huc2VuQG1lZGlzaW4udWlvLm5v
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.