 Nicole Racine
Nicole Racine Jenney Zhu1,2
Jenney Zhu1,2 Sheri Madigan
Sheri Madigan- 1Department of Psychology, University of Calgary, Calgary, AB, Canada
- 2Alberta Children's Hospital Research Institute, Calgary, AB, Canada
- 3Child Abuse Service, Alberta Children's Hospital, Alberta Health Services, Calgary, AB, Canada
Children exposed to child sexual abuse (CSA) vary considerably with regards to their presenting concerns and treatment needs. One factor creating heterogeneity amongst children experiencing CSA is their history of experiencing other victimizations (i.e., poly-victimized or not). However, little is known about risk factors for poly-victimization as well as differences in protective factors among these two groups. Additionally, there is currently limited understanding of whether poly-victimization is associated with greater trauma symptoms in children exposed to CSA and being seen for trauma treatment. Using a clinical sample of 117 children who were sexually abused (64 CSA only and 53 poly-victimized) ranging from age 3–18 years, the current study examined demographic characteristics, abuse characteristics, trauma symptoms, and protective factors using casefile review methodology. After accounting for other risk factors, parental abuse history and protective factors were significantly associated with child poly-victimization status. Children exposed to poly-victimization were more likely to have financial concerns = 4.16, p = 0.04, parents with abuse histories = 8.93, p = 0.003, and parents with histories of mental health or substance use difficulties = 4.02, p = 0.045. Although cumulative trauma symptoms scores were higher for children who were poly-victimized compared to CSA only, t(115) = −2.24, p = 0.03, multiple regression analyses showed that poly-victimization status was not significantly associated with child trauma symptoms after accounting for other demographic and abuse characteristics. Assessing and understanding the extent to which children exposed to CSA have experienced other forms of maltreatment is critical for identifying children who may be most at risk of poor outcomes.
Introduction
Child sexual abuse (CSA) is one of the most pernicious forms of childhood adversity. With 13% of children worldwide experiencing sexual abuse (1), the cumulative mental health and physical health consequences associated with CSA are substantial (2–5). Upwards of 50% of children develop trauma symptoms following exposure to CSA and require psychological treatment or intervention (6). Yet, the experience and subsequent treatment needs of children who have been sexually abused are varied. Several variables contribute to the presenting symptoms and treatment needs of children who have been sexually abused, including abuse severity (7), abuse frequency (8), and perpetrator characteristics (9, 10). An additional factor that may differentiate children with a history of CSA is whether or not they have also been exposed to other forms of abuse in addition to CSA, a term known as poly-victimization (11). Previous research has shown that children who have been poly-victimized are more likely to have emotional difficulties in adulthood than those exposed to CSA only and unexposed children (12). However, there is limited understanding of what risk factors may contribute to poly-victimization as well as how children exposed to poly-victimization may differ from children exposed to CSA only. Understanding factors that contribute to the differential profiles of CSA and their related experiences could inform treatment planning and decision making for children exposed to single vs. multiple forms of maltreatment.
Exposure to childhood sexual abuse is a complex and multi-faceted experience. The experience of one child who has been sexually abused can differ widely from the experience of another. Indeed, the term CSA is used to describe a wide range of experiences that vary in characteristics, such as the severity and chronicity of the abuse, relationship to the perpetrator, and age at which it occurred (13). These characteristics have been shown to be inter-related (13), with younger age of abuse onset and being abused by a family member being closely linked. These variables are also important determinants of the outcomes for children who have been sexually abused, including greater development of trauma symptoms and mental health difficulties amongst those with more severe and chronic sexual abuse, and those whose sexual abuse perpetrator was intrafamilial (8). Outcomes for children who have experienced CSA may also vary based on whether the child has been exposed to other forms of abuse. Finkelhor et al. coined the term poly-victimization, which refers to the exposure of multiple forms of victimization, including child abuse (14). Children who experience one form of abuse or maltreatment are highly likely to experience other forms of victimization (8, 15, 16) indicating that experiences of abuse co-occur and can be cumulative. This may in part be attributable to the pathways that lead to exposure to abuse and poly-victimization, such as living in a violent or chaotic family and/or neighborhood (17). In line with developmental theory on cumulative risk (18, 19), the accumulation of abuse experiences is an important consideration with regards to children's clinical presentations and may be an important determinant of children's outcomes in trauma treatment (20).
While poly-victimization has been a burgeoning area of research, limited research has examined differences in demographics, abuse characteristics, and trauma symptoms among children exposed to CSA only as compared to children exposed to CSA in addition to other forms of maltreatment. Additionally, there is also a limited understanding of the risk factors for poly-victimization in clinical samples. One study showed that children exposed to both sexual and physical abuse have more psychiatric diagnoses and mental health difficulties than children exposed to CSA only and physical abuse only (21). Another study conducted in Korea examined differences in abuse characteristics and mental health symptoms among children exposed to CSA only vs. children exposed to CSA plus other interpersonal traumas (e.g., witnessing violent crime, witnessing domestic violence) (22). They found that poly-victimized children were more likely to be older, be in single-parent families, have longer durations of CSA, and have perpetrators within the family compared to children exposed to CSA only (22). The rate of psychiatric diagnoses and severe behavior problems were also higher among children who were exposed to CSA in addition to other forms of interpersonal trauma (22). The current study builds on previous research and provides a novel contribution in three main ways: (1) we identify risk factors for poly-victimization in a community-based setting, (2) we examine whether protective factors differ among children who are poly-victimized vs. children exposed to CSA only, and (3) we examine whether poly-victimization is significantly associated with child trauma symptoms above and beyond other demographic and abuse characteristics. Our use of a community-based clinical sample makes the findings from the current study highly clinically relevant to service providers working with children exposed to CSA.
In addition to understanding differences in abuse characteristics and mental health symptoms for children exposed to CSA only vs. children who are poly-victimized, it is also important to consider differences in parental characteristics and protective factors at the outset of treatment. Parent mental health and well-being have been identified as important determinants of children's adaptation following exposure to CSA (23). That is, children who have a parent or caregiver who is emotionally supportive and available are more likely to disclose CSA (24), and also more likely to have successful treatment outcomes (25). A parent's own mental health or substance use difficulties as well as previous exposure to trauma may act as barriers in being able to provide this support. Identifying differences in protective factors is also an important consideration. For example, protective factors, including individual skills and use of social supports, have been shown to moderate the association between poly-victimization and the onset of psychological problems (26). Additionally, previous research has shown that children who have fewer protective factors are at increased risk for dropping out of trauma treatment (20). Thus, understanding whether there are differences in protective factors for children who have been poly-victimized is critical for informing treatment goals and targets.
To build on previous research, the current study sought to explore differences in demographic factors, abuse characteristics, trauma symptoms, and protective factors between children referred for trauma treatment who were exposed to CSA only vs. those who have been poly-victimized. Previous work has focused on differences in abuse characteristics as well as psychiatric diagnoses and behavior problems among these two groups (22). The current study adds to this growing knowledge base by examining differences in trauma symptoms as well as protective factors. Children included in the current study are part of a community sample of children exposed to sexual abuse and thus findings are highly clinically relevant to community practice settings treating children who have been sexually abused and their families. Understanding differences in presenting trauma symptoms and protective factors can help disentangle the unique contribution of sexual abuse vs. other experiences of maltreatment and can provide valuable clinical information in terms of which children and families may require additional supports and resources to recover from their trauma.
Materials and Methods
Study Design
Data for the current study were extracted from the clinical files of children referred to a child abuse treatment service in Western Canada. Files reviewed were open between the dates of January 2016 and June 2017 and the case file review occurred between March 2017 and October 2018. Using guidelines for retrospective chart review (27), demographic characteristics (i.e., child age, sex, financial concerns, parent history of abuse, and parent mental health history), abuse characteristics (i.e., perpetrator, severity, and frequency), presenting trauma symptoms, and protective factors (e.g., support from caregivers, peers, and school) were extracted from clinical files by two trained coders using a standardized data extraction protocol. All information was based on information provided in a standard intake record form, clinician reports, case notes, questionnaires completed by children and families, and any medical documents included in the case files.
Participants
The current study was part of a larger retrospective case file review examining characteristics and treatment needs of children exposed to adversity more broadly and referred for psychosocial services at the Child Abuse Service (CAS) (28, 29). The CAS is a multi-disciplinary, psychosocial treatment team that assesses the impact of sexual abuse, as well as severe and complex physical abuse and neglect, and provides therapeutic intervention to address psychological and relational sequelae of abuse. Children are referred to the CAS from the hospital, medical clinics, community physicians, child welfare, parents/guardians, or via self-referral. Referral criteria for the CAS include: (1) exposure to sexual abuse and/or severe and complex physical abuse and/or neglect, and (2) the child is experiencing emotional, behavioral, or relational distress related to their abuse exposure, and (3) the child is under the age of 18 years at the time of referral. Children referred to and treated at the CAS are among the most severe and complex child abuse cases within the region. As described in previous research (28), more than 60% of cases are referred for a primary presenting concern of sexual abuse. As such, the sample of sexually abused children is largely representative of the population who is referred to the CAS. For 82.1% of children, the primary caregiver was the child's biological parent. In 76.1% of cases, the primary caregiver was the child's mother. It is common practice at the CAS to conduct assessments and treatments with non-offending caregivers, particularly in instances of sexual abuse. Thus, the sexual abuse perpetrator was not the primary caregiver involved with the child's treatment.
To be included in the current file review, children had to be assessed and/or treated at the CAS from January 2016 to March 2017 and were no longer receiving service (i.e., their file was closed). A total of 176 files were extracted, of which 117 had experienced sexual abuse. Sixty-four children were exposed only to sexual abuse while 53 children were exposed to sexual abuse in addition to at least one other form of maltreatment, including physical abuse, emotional abuse, physical neglect, and emotional neglect, and were thus considered to be in the poly-victimized group.
Measures
Demographic Information
Demographic information was gathered from an intake form completed by an intake worker at the time of referral. The intake form was completed with the referral source who was either the biological parent (72.1%), child welfare worker (10.8%), foster parent (4.5%), or another source such as a therapist, police officer, or extended family member (12.5%). Demographic information included in the current study were the child's age, sex (male or female), and financial difficulties (i.e., considered to have financial difficulties or not). Information about whether or not one of the child's parents had a history of child abuse (yes/no) as well as a history of mental health or substance use difficulties (yes/no) was also obtained from the referral source.
Abuse Types and Characteristics
At the time of referral, the types of abuse the child had experienced were collected. However, if the child reported additional abuse types upon meeting the therapist, these were also captured in the file review methodology. Potential abuse types included sexual abuse, physical abuse, emotional abuse, physical neglect, and emotional neglect. Based on definitions provided in previous research (30), sexual abuse was operationalized as any of the following being committed by an adult or individual at least 5 years older than the child: touched, fondled, oral sex, anal sex, or vaginal sex. Physical abuse was operationalized as being pushed, grabbed, slapped, object thrown at the child, or hit. Emotional abuse was defined as being sworn at, insulted, put down, humiliated, or threatened. Physical neglect was defined as failure to meet a child's basic physical needs such as provision of food, clean clothes, and protection from safety. Emotional neglect was operationalized as a child often or very often not feeling loved, a sense of belonging, or support from their caregivers. All abuse types were rated as being present (1) or absent (0) for each child. A total score across abuse types was calculated and participants were categorized as either having experienced child sexual abuse only (CSA only) or as having experienced poly-victimization.
Abuse characteristics were gathered as part of the intake interview (28). The child's relationship to the perpetrator was coded as either a non-family member (0) or as a family member (1). All biological parents, non-biological parents, siblings, and extended relatives were coded as being family members. Strangers and acquaintances were coded as non-family members. Abuse invasiveness was coded using a 4-point scale. A score of 1 referred to no physical contact such as indecent exposure or exposure to pornography, a code of 2 was assigned for fondling or touching, a code of 3 was assigned for oral sex, and a code of 4 was assigned for genital or anal penetration.
Trauma Symptoms
Trauma symptoms at the time of referral were coded as present (coded as 1) or absent (coded as 0) based on a list of 11 symptoms derived from the DSM-5 diagnostic criteria for Post-Traumatic Stress Disorder (31). These trauma symptoms were selected as they commonly present in children who have been exposed to child abuse (32). The 11 trauma symptoms systematically asked about in the intake process were: physical aggression, oppositional behavior, acting out in a sexual manner, symptoms of anxiety or fearfulness, presence of nightmares or sleep disturbance, changes in weight or appetite, preoccupation with or can't stop thinking about the abuse or adverse event, feelings of guilt or shame related to the abuse, persistently sad or withdrawn behavior, thoughts or attempts of self-harm or suicide, and substance use. The total sum of endorsed items was calculated. Examining the internal consistency of all the items, the Cronbach's alpha was 0.61, which is considered acceptable (33). The reliability for the summed trauma symptoms score was excellent (ICC = 0.90).
Protective Factors
Protective factors were coded using a cumulative score based on items from the Child and Youth Resilience Measure [CYRM-28; (34)]. The CYRM is typically administered as a self-report or caregiver report questionnaire (34), however, given the retrospective file review methods employed in the current study, we extracted information on the presence or absence of eight overall subscales pertaining to the individual child (i.e., personal skills, peer support, and social skills), caregiver (i.e., physical and psychological caregiving), and context (i.e., spiritual, educational, and cultural support) (35). Each subscale was scored as either present (1) or absent (0) based on information in the child's file. For the spiritual and cultural support variables, more than 80% of participants had no available data on these factors, therefore, responses on the spiritual and cultural variables were not included in the analyses. Internal consistency in the current study was acceptable with a Cronbach's alpha of 0.66. The intraclass correlation for the reliability score among coders for the total protective factors score was 0.69, which is considered adequate.
Data Analysis
All analyses were conducted in SPSS 25. Descriptive statistics, including means and percentages were estimated for child demographic factors. Differences in demographic, abuse, symptoms, and protective factors between children exposed to sexual abuse only vs. children who were poly-victimized were examined using chi-square tests for dichotomous variables and independent sample t-tests for continuous variables. Correlation and point-biserial correlations were calculated across all variables. Logistic regressions were calculated to examine what demographic characteristics and protective factors were associated with child poly-victimization status. Finally, a multiple regression analysis was conducted to examine whether poly-victimization status is significantly associated with child trauma symptoms above and beyond other demographic and abuse-related factors.
A power calculation was conducted using G*Power software (36) to determine the required sample size across CSA and poly-victimization groups. To detect a medium effect size (Cohen's d = 0.62), with a power of 0.95 and alpha of 0.05, an overall sample size of 116 participants (63 and 53 participants in each group) was needed. Thus, a sample size of 117 participants was adequate to detect a medium effect size in the current study.
Results
Descriptive Characteristics
All descriptive statistics are presented in Table 1. On average children were 10.59 years of age (Range: 3.92–17.67) and 77.8% (n = 91) were female. The majority of the sample did not report financial concerns (84.6%). More than half of parents in the sample had a history of child abuse themselves (54.7%) and the majority of parents (65.8%) had history of either mental illness or substance use difficulties. With regards to abuse characteristics, 55.6% of perpetrators were a family member. Frequencies of individual trauma symptoms and protective factors are presented in Table 1.
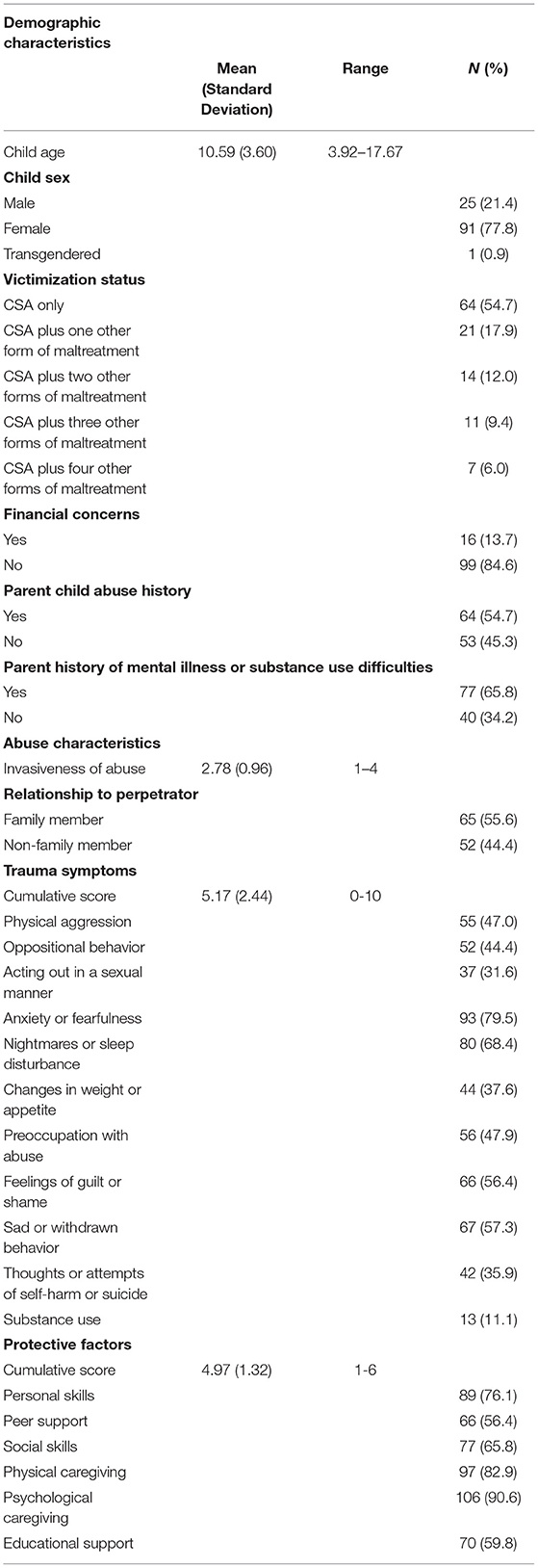
Table 1. Descriptive characteristics of the total sample (n = 117).
Pearson and Point-Biserial Correlations Among Study Variables
Correlations among study variables are presented in Table 2. Being poly-victimized was negatively associated with the protective factors score and positively associated with trauma symptoms and invasiveness of sexual abuse. Older children had higher cumulative trauma symptoms. Cumulative trauma symptoms and the protective factors score were negatively associated. Cumulative trauma symptoms were positively associated with a parental history of abuse and a parental history of mental health or addictions issues.
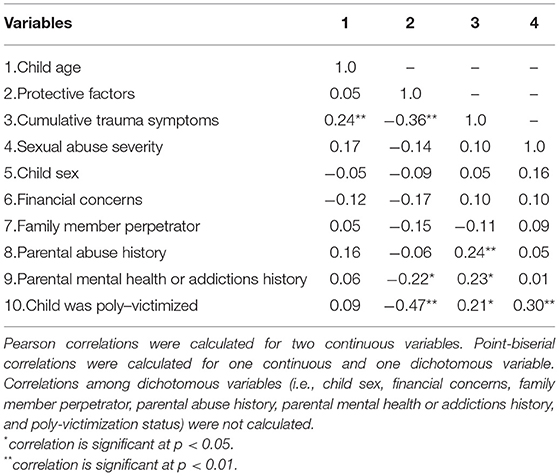
Table 2. Pearson and point-biserial correlations among study variables.
Examining Sociodemographic Risk Factors for Poly-Victimization
Using logistic regression, we examined whether child demographic factors and protective factors were associated with exposure to poly-victimization (See Table 3). In unadjusted analyses, having financial concerns, parental abuse history, and a parental history of mental health or addiction difficulties were associated with exposure to poly-victimization. A higher protective factors score was associated with decreased likelihood of being poly-victimized. When all significant variables were simultaneously entered into a logistic regression model, only the parental abuse history and cumulative protective factors score remained significantly associated with child poly-victimization status. A total of 41.6% of the variance in poly-victimization status was accounted for by the adjusted model.
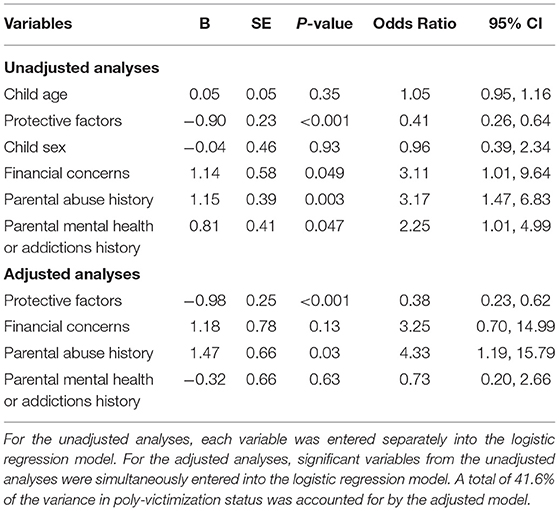
Table 3. Unadjusted and adjusted logistic regression analyses of risk factors for poly-victimization status.
Demographic and Abuse Characteristic Differences
Differences in demographic and abuse characteristics for children exposed to CSA only vs. children who were poly-victimized are presented in Table 4. Children exposed to CSA only vs. children who were poly-victimized did not differ in age or sex. Children who were poly-victimized were more likely to have financial concerns in their family, = 4.16, p = 0.04. Parents of children who were poly-victimized children were more likely to have a history of childhood abuse, = 8.93, p = 0.003, as well as a history of mental health or substance use difficulties, = 4.01, p = 0.045. Children who were poly-victimized were more likely to have been abused by a perpetrator who was a family member (69.8%) compared to CSA only children (43.8%) and had higher mean sexual abuse invasiveness scores, t(111) = −3.35, p = 0.001.
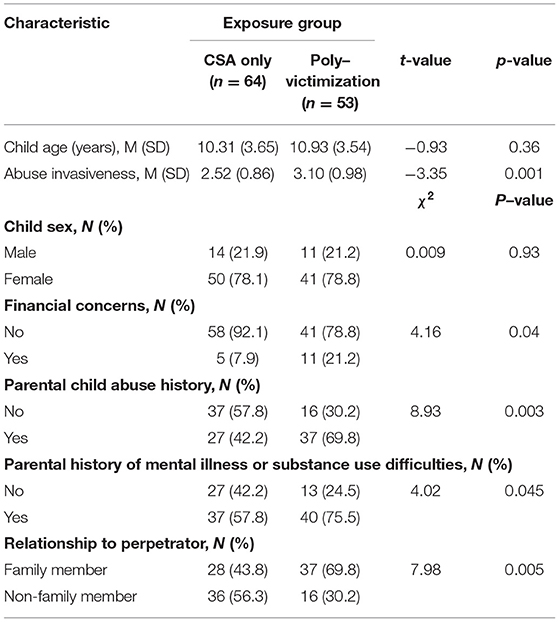
Table 4. Differences in demographic and abuse characteristics among children exposed to csa only vs. those who were poly-victimized.
Trauma Symptom Differences
Cumulative trauma symptoms scores were higher for children who were poly-victimized as compared to children exposed to CSA only, t(115) = −2.24, p = 0.03 (See Table 5). Examining specific trauma symptoms, physical aggression, sexual acting out, and substance use were more frequently endorsed for children who were poly-victimized as compared to children exposed to CSA only.
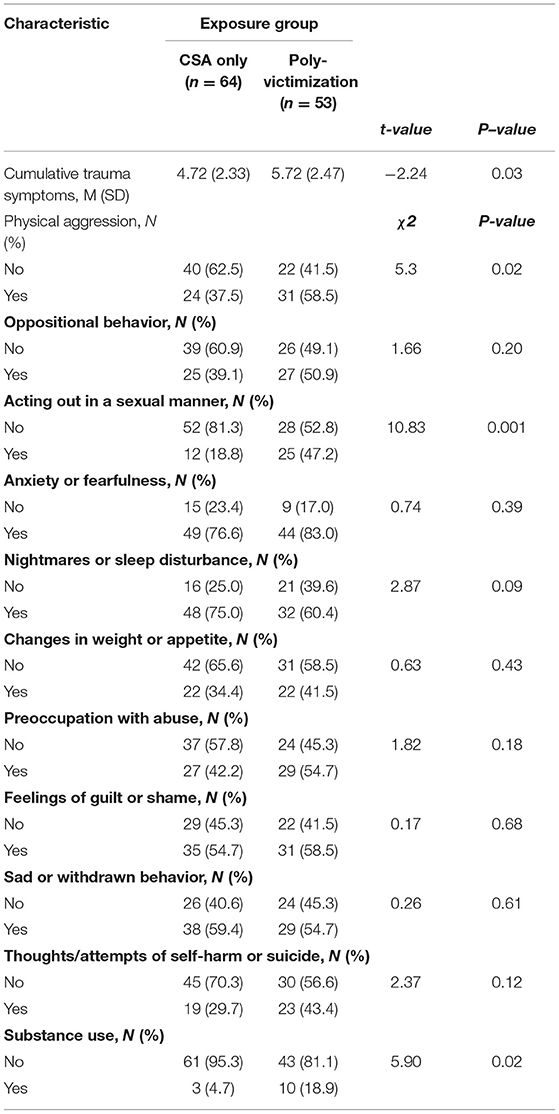
Table 5. Differences in trauma symptoms among children exposed to CSA only vs. those who were poly-victimized.
Protective Factor Differences
Differences in protective factors for children who were poly-victimized vs. CSA only are presented in Table 6. Children who were poly-victimized children had lower mean levels of protective factors than children exposed to CSA only, t(85) = 4.67, p < 0.001. Overall, children who were poly-victimized were less likely to have personal skills, peer-support, social skills, caregiver physical support, caregiver emotional support, and educational support, compared to children exposed to CSA only.
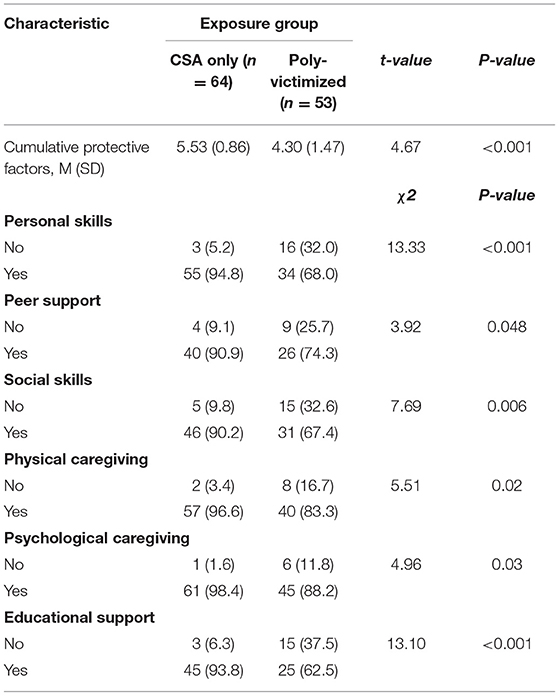
Table 6. Differences in protective factors among children exposed to CSA only vs. those who were poly-victimized.
Examining Factors Associated With Cumulative Trauma Symptoms
Using regression analyses, we examined whether demographic and abuse characteristics, including poly-victimization, were associated with cumulative child trauma symptoms (See Table 7). In unadjusted analyses, child age, parental abuse history, parental mental health or addictions history, and poly-victimization status were all positively associated with cumulative child trauma symptoms. Protective factors were negatively associated with child trauma symptoms. In adjusted analyses where all significant variables were entered simultaneously, only child age, and cumulative protective factors remained significant. After accounting for all other factors, poly-victimization status was not significantly associated with child trauma symptoms. A total of 18.8% of the variance in cumulative trauma symptoms was accounted for by the adjusted model.

Table 7. Unadjusted and adjusted regression analyses for cumulative trauma symptoms.
Discussion
Extant literature has documented the detrimental effects of sexual abuse on children's mental health and emotional well-being (2–4). However, there is significant variability in the individual characteristics and presenting concerns of children referred to mental health services following exposure to CSA and clinicians can benefit from indicators that can help identify which children are at increased risk for poor outcomes or require additional supports. Disentangling whether CSA in addition to other forms of maltreatment conveys additional risk on children's presenting trauma symptoms and protective factors at the outset of child trauma treatment could help inform treatment planning and resource allocation for families. Using a clinical sample of children exposed to CSA, the current study builds on prior research by examining risk factors for poly-victimization, differences in protective factors for poly-victimized children as compared to children exposed to CSA only, and exploring the relative contribution of poly-victimization to child trauma symptoms. We found that lower levels of protective factors and parental history of child abuse were associated with poly-victimization. When examining differences in demographic and abuse characteristics for children exposed to poly-victimization vs. CSA only, we found overall higher levels of family risk, including parental abuse history, parental substance use, and parental mental health difficulties. Children exposed to poly-victimization had a higher number of trauma symptoms and a lower number of protective factors. Although exposure to poly-victimization was associated with greater trauma symptoms, these findings were no longer significant after accounting for protective factors and child age. We discuss our findings and their clinical implications below.
We found that lower levels of protective factors and parental history of child abuse were associated with poly-victimization status. Generally, it may be that children who are exposed to poly-victimization experience more household family risk and fewer supports than children exposed to CSA only. According to the cycle of maltreatment hypothesis, parents who were exposed to child maltreatment themselves are more likely to have children who also experience maltreatment (37–39). Indeed, a previous meta-analysis demonstrated support for this hypothesis, including the specific transmission of neglect, physical, emotional, and sexual abuse across generations (37). Parents who have been abused themselves may have had sub-optimal models for parenting skills and strategies. In families with histories of maltreatment, there may also be increased likelihood of exposure to a family member who may perpetrate sexual abuse and a lack of adequate supervision on the part of the parent, who may have an altered sense of safety based on their own abuse experiences. Parent experiences of mental illness and substance use may also confer risk for child exposure to abuse through compromised parenting quality, reduced supervision, and exposure to environments where maltreatment is more likely to occur. For example, parent psychopathology, such as depression, may disrupt normative parenting practices, which in turn, can increase likelihood for child maltreatment (40). Of note, parents with their own abuse histories may be at increased risk for mental health difficulties, further perpetuating the cycle of maltreatment (41). Parental substance use may also compromise parenting quality, such that previous research has found an inverse relationship between parental drug use and parental involvement (42). Overall, this suggests that, through compromised parenting involvement and quality, parent experience of mental illness and substance use can increase the likelihood that the child is exposed to unsafe situations (43), which may increase risk for exposure to multiple forms of child maltreatment.
Interestingly, child age, sex, and financial concerns were not significantly associated with poly-victimization after accounting for other variables. These findings differ from previous research that found that poly-victimized children in Korea were more likely to be older and be from families with lower household income than children exposed to CSA only (22). One reason for these findings may be that our measurement of financial concerns did not fully capture the financial needs and experiences of families. We may have found differences had we asked families to report on their household family income on a gradient. Given that financial resources have been shown to play a role in symptom reduction for individuals receiving psychological treatment following CSA (44), future research should include more fine-grained measures of family income.
In addition to differences in parental characteristics, we found that at treatment entry, cumulative trauma symptom scores were higher among poly-victimized children compared to children exposed to CSA alone. This finding is consistent with our hypotheses and is in line with the notion of cumulative risk, which suggests that exposure to a greater number of risk factors leads to greater negative outcomes (18). Whereas, previous research has found an association between the cumulative maltreatment and child trauma symptoms (29), the current study demonstrates this association in a clinical sample of youth directly receiving treatment for maltreatment experiences. Mechanistically, exposure to multiple forms of stress can lead to physiological dysregulation, or elevated allostatic load on the body, which in turn, can increase risk for mental health difficulties, such as trauma symptoms (45, 46). Exploring various trauma symptoms, the present research found that poly-victimized children exhibited greater externalizing difficulties, including physical aggression, sexual acting out, and substance use, but not internalizing symptoms (i.e., sadness, anxiety, shame/guilt) compared to children exposed to CSA only. Exposure to additional forms of abuse, such as physical abuse and domestic violence, may increase the propensity for externalizing difficulties. For example, previous research has demonstrated that children exposed to both domestic violence and physical abuse exhibited more externalizing symptoms compared to children exposed to either domestic violence or physical abuse alone (47). Additionally, these findings may support the notion that cumulative risk leads to cumulative outcomes (48). That is, increased exposure to maltreatment types may broaden the potential symptom outcomes that children experience, which has important implications for the delivery of trauma-based interventions.
An important and novel finding from the current study was that children exposed to poly-victimization were less likely to have any protective factors present across the social ecology at the outset of treatment. That is, children who were poly-victimized were less likely to have individual, familial, or school-level factors present. This is concerning as protective factors such as individual coping skills, peer relations, and support from a caregiver have been found to be associated with adaptive outcomes following exposure to maltreatment (49) and are associated with lower levels of trauma symptoms as well as a decreased likelihood of dropping out of treatment prematurely (20, 29). Indeed, we found that protective factors were associated with cumulative trauma symptoms at the outset of treatment in this sample, above and beyond poly-victimization status. Thus, identifying protective factors and supporting families to bolster or increase the protective factors that are present for the child are important treatment targets in trauma therapy, regardless of poly-victimization status.
Limitations
The current study should be considered in the context of some limitations. First, in order to provide clinically and ecologically valid findings, we employed retrospective file review methodology for the current study. However, this means that we were limited by the information that was present and recorded in the patient file. For example, there was limited information provided with regards to the child's cultural or religious supports. Future research that includes self-report questionnaires that specifically ask about diverse protective factors across the social ecology will be informative. Second, the presence of trauma symptoms was reported by the individual referring the child, meaning that this information was not provided via child or adolescent self-report. Previous research has demonstrated that a child's self-report of trauma symptoms may be more strongly associated with a diagnosis of post-traumatic stress disorder than a parent's report (50). Thus, a goal for future studies would be to obtain both parent and child reports of trauma symptoms. Third, child abuse exposure was also determined via self-report from referral sources and not explicitly obtained from child self-report or disclosures. Future research would benefit from detailed interviews to ascertain abuse exposures. Lastly, although we obtained information on parent exposure to childhood maltreatment, the type of maltreatment was not specified. Future research investigating the role of different forms of parent exposure to child maltreatment and risk for intergenerational transmission may be useful for prevention.
Conclusion and Clinical Implications
Children who are exposed to CSA are at considerable risk for experiencing disrupted physical and mental health trajectories (2, 6). Of these children, those who have experienced poly-victimization present with particularly challenging familial situations, increased symptom severity, and fewer protective factors. Taken together, our study suggests that both the individual and family-level risk for children who have been poly-victimized are elevated and warrant attention as part of trauma treatment. From a clinical perspective, acknowledging the potentially heightened level of individual and familial-level risk that may exist for children who have been poly-victimized is critical. For example, undertaking a thorough assessment that assesses a wide array of potential victimization experiences and their impact can be helpful (51). A novel contribution of the current study is that a lack of protective factors in the child's developmental ecology confers greater risk for poly-victimization and elevated child trauma symptoms. Thus, assessing and identifying protective factors that exist both inside and outside the home may provide critical information with regards to treatment planning. Questionnaires that specifically target protective factors across the child's social ecology, including at school and in the community (34), may help a clinician to identify where collaborative efforts across systems may be helpful. Additionally, in families where parents and caregivers have had their own previous trauma or are actively managing mental health or substance use issues, it is critical to ensure that these needs are met in order for the parent to be available and supportive to their child as part of trauma treatment (52). Future research that is longitudinal, multi-informant, and considers a broad array of protective factors and their potential mechanisms is needed.
Data Availability Statement
The datasets presented in this article are not readily available because of confidentiality of participant data. Requests to access the datasets should be directed to c2hlcmkubWFkaWdhbkB1Y2FsZ2FyeS5jYQ==.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Calgary Research Ethics Board. A waiver of consent was obtained due to the archival file review nature of the data in accordance with institutional requirements.
Author Contributions
NR and SM: conceptualization, methodology, formal analysis, and supervision. NR, SM, and CH: data curation, project administration, and funding acquisition. NR, SM, and JZ: writing—original draft preparation. NR, SM, JZ, and CH: writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
NR received post-doctoral funding from Alberta Innovates. SM receives support from the Canada Research Chairs program. JZ receives graduate student funding from the Social Sciences and Humanities Research Council. This project was supported by a Social Sciences and Humanities Research Council Partnership Engage Grant.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We acknowledge the contributions of members of the Determinants of Child Development Laboratory at the University of Calgary and the collaborative relationship with clinicians and staff at the Child Abuse Service.
References
1. Stoltenborgh M, van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. (2011) 16:79–101. doi: 10.1177/1077559511403920
2. Paolucci EO, Genuis ML, Violato C. A meta-analysis of the published research on the effects of child sexual abuse. J Psychol. (2001) 135:17–36. doi: 10.1080/00223980109603677
3. Hillberg T, Hamilton-Giachritsis C, Dixon L. Review of meta-analyses on the association between child sexual abuse and adult mental health difficulties: a systematic approach. Trauma Violence Abuse. (2011) 12:38–49. doi: 10.1177/1524838010386812
4. Paras ML, Murad MH, Chen LP, Goranson EN, Sattler AL, Colbenson KM, et al. Sexual abuse and lifetime diagnosis of somatic disorders: a systematic review and meta-analysis. JAMA. (2009) 302:550–61. doi: 10.1001/jama.2009.1091
5. Hailes HP, Yu R, Danese A, Fazel S. Long-term outcomes of childhood sexual abuse: an umbrella review. Lancet Psychiatry. (2019) 6:830–9. doi: 10.1016/S2215-0366(19)30286-X
6. Collin-Vezina D, Daigneault I, Hebert M. Lessons learned from child sexual abuse research: prevalence, outcomes, and preventive strategies. Child Adolesc Psychiatry Ment Health. (2013) 7:22. doi: 10.1186/1753-2000-7-22
7. Maikovich AK, Koenen KC, Jaffee SR. Posttraumatic stress symptoms and trajectories in child sexual abuse victims: an analysis of sex differences using the national survey of child and adolescent well-being. J Abnorm Child Psychol. (2009) 37:727–37. doi: 10.1007/s10802-009-9300-x
8. Perez-Fuentes G, Olfson M, Villegas L, Morcillo C, Wang S, Blanco C. Prevalence and correlates of child sexual abuse: a national study. Compr Psychiatry. (2013) 54:16–27. doi: 10.1016/j.comppsych.2012.05.010
9. Banyard VL, Williams LM. Characteristics of child sexual abuse as correlates of women's adjustment: a prospective study. J Marriage Family. (1996) 58:853–65. doi: 10.2307/353975
10. Ullman S. Relationship to perpetrator, disclosure, social reactions, and PTSD symptoms in child sexual abuse survivors. J Child Sexual Abuse. (2007) 16:19–36. doi: 10.1300/J070v16n01_02
11. Finkelhor D, Ormrod RK, Turner HA. Poly-victimization: a neglected component in child victimization. Child Abuse Negl. (2007) 31:7–26. doi: 10.1016/j.chiabu.2006.06.008
12. Rapsey CM, Scott KM, Patterson T. Childhood sexual abuse, poly-victimization and internalizing disorders across adulthood and older age: findings from a 25-year longitudinal study. J Affect Disord. (2019) 244:171–9. doi: 10.1016/j.jad.2018.10.095
13. Ventus D, Antfolk J, Salo B. The associations between abuse characteristics in child sexual abuse: a meta-analysis. J Sexual Aggress. (2017) 23:167–80. doi: 10.1080/13552600.2017.1318963
14. Finkelhor D, Ormrod RK, Turner HA. Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse Negl. (2007) 31:479–502. doi: 10.1016/j.chiabu.2006.03.012
15. Finkelhor D, Ormrod RK, Turner HA. Polyvictimization and trauma in a national longitudinal cohort. Dev Psychopathol. (2007) 19:149–66. doi: 10.1017/S0954579407070083
16. Kellogg ND, Menard SW. Violence among family members of children and adolescents evaluated for sexual abuse. Child Abuse Negl. (2003) 27:1367–76. doi: 10.1016/j.chiabu.2003.10.008
17. Finkelhor D, Ormrod R, Turner H, Holt M. Pathways to poly-victimization. Child Maltreat. (2009) 14:316–29. doi: 10.1177/1077559509347012
18. Evans GW, Li D, Whipple SS. Cumulative risk and child development. Psychol Bull. (2013) 139:1342–96. doi: 10.1037/a0031808
19. Rutter M. Statistical and personal interactions: facets and per-spectives. In: Allen DMV, editor. Human Development: Aninteractional Perspective. New York, NY: Academic Press (1983). p. 295–319.
20. Eirich R, Racine N, Garfinkel D, Dimitroopoulos G, Madigan S. Risk and protective factors for treatment dropout in a child maltreatment populatioon. Adv Resilience Sci. (2020) 1:165–77. doi: 10.1007/s42844-020-00011-9
21. Ackerman PT, Newton JE, McPherson WB, Jones JG, Dykman RA. Prevalence of post traumatic stress disorder and other psychiatric diagnoses in three groups of abused children (sexual, physical, and both). Child Abuse Negl. (1998) 22:759–74. doi: 10.1016/S0145-2134(98)00062-3
22. Choi J, Oh K. The effects of multiple interpersonal traumas on psychological maladjustment of sexually abused children in Korea. J Traum Stress. (2013) 26:149–57. doi: 10.1002/jts.21779
23. Yancey C, Hansen D. Relationship of personal, familial, and abuse-specific factors with outcome following childhood sexual abuse. Aggress Violent Behav. (2010) 15:410–21. doi: 10.1016/j.avb.2010.07.003
24. Azzopardi C, Madigan S, Kirkland-Burke M. Sexual abuse forensic evaluation with young children: program outcomes and predictors of disclosure. J Child Custody. (2014) 11:304–24. doi: 10.1080/15379418.2014.988901
25. Rosenthal S, Feiring C, Taska L. Emotional support and adjustment over a year's time following sexual abuse discovery. Child Abuse Negl. (2003) 27:641–61. doi: 10.1016/S0145-2134(03)00104-2
26. Huang L, Mossige S. Resilience and poly-victimization among two cohorts of norwegian youth. Int J Environ Res Public Health. (2018) 15:2852. doi: 10.3390/ijerph15122852
27. Gearing RE, Mian IA, Barber J, Ickowicz A. A methodology for conducting retrospective chart review research in child and adolescent psychiatry. J Can Acad Child Adolesc Psychiatry. (2006) 15:126–34.
28. Racine N, Dimitropoulos G, Hartwick C, Eirich R, van Roessel L, Madigan S. Characteristics and service needs of maltreated children referred for mental health services at a child advocacy centre in Canada. J Can Acad Child Adolesc Psychiatry. (2021) 30:92–103.
29. Racine N, Eirich R, Dimitropoulos G, Hartwick C, Madigan S. Development of trauma symptoms following adversity in childhood: the moderating role of protective factors. Child Abuse Negl. (2020) 101:104375. doi: 10.1016/j.chiabu.2020.104375
30. Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/S0749-3797(98)00017-8
31. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC (2013).
32. Wherry J, Dunloop C. TSCC and TSCYC screening forms in a clinical sample: reliability, validity, and creating local clinical norms. Child Maltreatment. (2018) 23:74–84. doi: 10.1177/1077559517725207
33. Streiner D. Starting at the beginning: an introduction to coefficient alpha and internal consistency. J Personal Assess. (2003) 80:99–103. doi: 10.1207/S15327752JPA8001_18
34. Ungar M, Liebenberg L. Assessing resilience across cultures using mixed methods: construction of the child and youth resilience measure. J Mixed Methods Res. (2011) 5:126–49. doi: 10.1177/1558689811400607
35. Liebenberg L, Ungar M, Van de Vijver F. Validation of the Child and Youth Resilience Measure-28 (CYRM-28) among Canadian youth. Res Soc Work Pract. (2012) 22:219–26. doi: 10.1177/1049731511428619
36. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
37. H. vIM, Bakermans-Kranenburg MJ, Coughlan B, Reijman S. Annual research review: umbrella synthesis of meta-analyses on child maltreatment antecedents and interventions: differential susceptibility perspective on risk and resilience. J Child Psychol Psychiatry. (2020) 61:272–90. doi: 10.1111/jcpp.13147
38. Thornberry TP, Henry KL. Intergenerational continuity in maltreatment. J Abnorm Child Psychol. (2013) 41:555–69. doi: 10.1007/s10802-012-9697-5
39. Dubowitz H, Kim J, Black MM, Weisbart C, Semiatin J, Magder LS. Identifying children at high risk for a child maltreatment report. Child Abuse Negl. (2011) 35:96–104. doi: 10.1016/j.chiabu.2010.09.003
40. Dixon L, Browne K, Hamilton-Giachritsis C. Risk factors of parents abused as children: a mediational analysis of the intergenerational continuity of child maltreatment (Part I). J Child Psychol Psychiatry. (2005) 46:47–57. doi: 10.1111/j.1469-7610.2004.00339.x
41. Brook JS, Whiteman M, Balka EB, Cohen P. Parent drug use, parent personality, and parenting. J Genet Psychol. (1995) 156:137–51. doi: 10.1080/00221325.1995.9914812
42. Hindelang RL, Dwyer WO, Leeming FC. Adolescent risk-taking behavior: a review of the role of parental involvement. Curr Probl Pediatr. (2001) 31:63–83. doi: 10.1016/S1538-5442(01)70035-1
43. Cort NA, Gamble SA, Smith PN, Chaudron LH, Lu N, He H, et al. Predictors of treatment outcomes among depressed women with childhood sexual abuse histories. Depress Anxiety. (2012) 29:479–86. doi: 10.1002/da.21942
44. Madigan S, Cyr C, Eirich R, Fearon RMP, Ly A, Rash C, et al. Testing the cycle of maltreatment hypothesis: meta-analytic evidence of the intergenerational transmission of child maltreatment. Dev Psychopathol. (2019) 31:23–51. doi: 10.1017/S0954579418001700
45. McEwen B. Stress, adaptation, and disease. allostasis and allostatic load. Ann N Y Acad Sci. (1998) 840:33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
46. Rogosch FA, Dackis MN, Cicchetti D. Child maltreatment and allostatic load: consequences for physical and mental health in children from low-income families. Dev Psychopathol. (2011) 23:1107–24. doi: 10.1017/S0954579411000587
47. Moylan CA, Herrenkohl TI, Sousa C, Tajima EA, Herrenkohl RC, Russo MJ. The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. J Fam Violence. (2010) 25:53–63. doi: 10.1007/s10896-009-9269-9
48. Atkinson L, Beitchman J, Gonzalez A, Young A, Wilson B, Escobar M, et al. Cumulative risk, cumulative outcome: a 20-year longitudinal study. PLoS One. (2015) 10:e0127650. doi: 10.1371/journal.pone.0127650
49. Afifi TO, Macmillan HL. Resilience following child maltreatment: a review of protective factors. Can J Psychiatry. (2011) 56:266–72. doi: 10.1177/070674371105600505
50. Shemesh E, Newcorn JH, Rockmore L, Shneider BL, Emre S, Gelb BD, et al. Comparison of parent and child reports of emotional trauma symptoms in pediatric outpatient settings. Pediatrics. (2005) 115:e582–9. doi: 10.1542/peds.2004-2201
51. Finkelhor D, Hamby SL, Ormrod R, Turner H. The Juvenile Victimization Questionnaire: reliability, validity, and national norms. Child Abuse Negl. (2005) 29:383–412. doi: 10.1016/j.chiabu.2004.11.001
Keywords: sexual abuse, protective factor, risk factor, poly-victimization, child
Citation: Racine N, Zhu J, Hartwick C and Madigan S (2022) Differences in Demographic, Risk, and Protective Factors in a Clinical Sample of Children who Experienced Sexual Abuse Only vs. Poly-victimization. Front. Psychiatry 12:789329. doi: 10.3389/fpsyt.2021.789329
Received: 04 October 2021; Accepted: 03 December 2021;
Published: 12 January 2022.
Edited by:
Jordan Sibeoni, Université de Paris, FranceReviewed by:
Juan Carlos Sierra, University of Granada, SpainIlan Katz, University of New South Wales, Australia
Sheila Van Berkel, Leiden University, Netherlands
Copyright © 2022 Racine, Zhu, Hartwick and Madigan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheri Madigan, c2hlcmkubWFkaWdhbkB1Y2FsZ2FyeS5jYQ==