
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 20 December 2021
Sec. Child and Adolescent Psychiatry
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.778291
This article is part of the Research Topic Insights in Child and Adolescent Psychiatry: 2021 View all 10 articles
 Xiuxiu Ding1†Jun Wang1,2†Ning Li1Wanying Su1Hao Wang1Qiuxia Song1Xianwei Guo1Mingming Liang1Qirong Qin3Liang Sun4Mingchun Chen5
Xiuxiu Ding1†Jun Wang1,2†Ning Li1Wanying Su1Hao Wang1Qiuxia Song1Xianwei Guo1Mingming Liang1Qirong Qin3Liang Sun4Mingchun Chen5 Yehuan Sun1*
Yehuan Sun1*Anxiety is one of the most common psychological disorders among children. Few studies have investigated the prevalence and comprehensive factors for anxiety among preschool children in China. This study aimed to assess the prevalence of anxiety and explore influential factors at multiple levels including individual, prenatal and perinatal, and family factors, associated with anxiety symptoms among preschool children. The multisite cross-sectional study was conducted in Anhui Province and included 3,636 preschool children aged 3–6 years. Anxiety symptoms of children were assessed using the Chinese version of the Spence Preschool Anxiety Scale. Logistic regression analyses were performed to explore associations between factors at multiple levels and significant anxiety symptoms, and the model was validated internally using 10-fold cross-validation. Among the participants, 9.1% of children had significant anxiety symptoms. Girls reported more significant anxiety symptoms. Children's poor dietary habits, sleep disturbances, autistic tendencies, and left-behind experience; maternal poor prenatal emotional symptoms; and more caregivers' anxiety symptoms were significantly associated with anxiety symptoms among children. The result of 10-fold cross-validation indicated that the mean area under the curve, sensitivity, specificity, and accuracy were 0.78, 70.45%, 78.18%, and 71.15%, respectively. These factors were slightly different among different subtypes of anxiety symptoms. The results of this study suggested that anxiety symptoms in preschool children were prevalent, particularly in girls. Understanding early-life risk factors for anxiety is crucial, and efficient prevention and intervention strategies should be implemented in early childhood even pregnancy.
Anxiety is one of the most common psychological disorders among children and is associated with serious academic and social impairments and even adulthood psychological problems (1–4). Studies have demonstrated that the anxiety age of onset is approximately 6 years old (4–6). Preschool children's anxiety is generally moderately stable and tends to persist into childhood and adolescence (7, 8). A longitudinal study from Canada has indicated that 14.7% of preschool children maintain constantly elevated anxiety symptoms from 1.5 to 5.0 years of age (9). One recent study exploring the trajectories of anxiety symptoms from preschool to school age has suggested that high stable anxiety beginning at preschool age is associated with lower school engagement, poorer peer relations, and greater functional impairment during the later school age (10). Researchers have proposed that preschool age may be an optimal developmental window for anxiety prevention or early intervention (11).
Currently, considerable research efforts have been made to improve knowledge surrounding the aetiology of anxiety, which is believed to be affected by genetic vulnerability and environmental factors (10, 12–18). Previous classical twin studies point genetic background as the predominant factor for the emergence of anxiety-related behaviours (19), while a 30–40% heritability is reported (20). Individual internal characteristics such as age, gender, and children's emotional and behavioural characteristics are involved in susceptibility to anxiety. Some studies have shown that younger children report higher anxiety symptoms than older children (21, 22). Regarding gender differences, the results show a relatively incongruent picture in previous research (2, 22–24). Children's behavioural problems such as sleep disturbances, depression, high behavioural inhibition, attention-deficit hyperactivity disorder symptoms, and peer victimisation seem to predict follow-up anxiety (3, 10, 25). The influence of external environmental factors throughout foetal and early childhood involving prenatal, perinatal, and parental and family factors cannot be underestimated (12, 26, 27). With the development of the developmental origins of adult disease (DOHaD) theory (28), researchers traced these factors back to the pregnancy period according to the foetal programming mechanisms (29, 30). Evidence from cohort studies has indicated that preterm birth, caesarean section, hypertensive disorders of pregnancy, prenatal and postnatal anxiety, depression, and distress increase the risk of offspring anxiety (14, 27, 31–33). Given that the family exerts important influence on a child's development, researchers have noted the role of family factors in child anxiety. Some adverse family factors such as parental corporal punishment and abuse are positively associated with childhood anxiety (16, 34). Additionally, children who were separated from parents too early have more anxiety symptoms (17). In addition, one study has proposed a novel evidence for environmental transmission, and the anxiety of parents and children may influence each other in different ways (12). Severe early adversities may trigger chronic and neurobiologically distinct internalising symptoms starting from the preschool period (15). Therefore, it is of great importance to understand the impacts of early-life risk factors on children's anxiety. Thus far, numerous studies surrounding these issues are predominantly focused on school-aged children and from Western countries. However, only a few studies with small sample sizes and exploring only limited factors have been conducted among preschool children in China (35–37).
Taken together, the findings from previous research show that it is critical to better understand anxiety symptoms during the preschool period and its potential risk factors to minimise the negative effects on these children. In the current study, we hypothesised that exposure to prenatal and perinatal adversities, individual problematic behaviours, and adverse family environmental factors from pregnancy to early childhood might increase the risks of preschool children's anxiety. This study aims to ascertain whether comprehensive factors including individual, prenatal, perinatal, and family factors are associated with anxiety among preschool children and provide scientific evidence supporting the use of early-life interventions based on multisite cross-sectional survey.
This multisite cross-sectional study was conducted in 26 kindergartens of four counties including Funan county in Fuyang City, Changfeng county and Fexi county in Hefei City, and Bowang district (same as county administrative level) in Ma'anshan City, located in the north, middle, and south of Anhui Province from September 2019 to January 2020. A total of 3,802 questionnaires were distributed in the initial investigation. Finally, 3,636 effective questionnaires were collected with a total response rate of 95.6%, after checking for completeness and logic. Participants, including 3,636 preschool children aged 3–6 years and their primary caregivers, voluntarily participated in the investigation. Children and their caregivers with cognitive impairment, deafness, or language communication barriers and children with severe mental or physical illnesses were excluded. Prior to data collection, caregivers' consent was obtained. Then, caregivers were invited to complete a structured questionnaire through a face-to-face interview. The study was approved by the Ethics Committee of Anhui Medical University (20180402), and confidentiality was assured.
Individual characteristics included children's age, gender, body mass index (BMI), dietary habits, sleep disturbances, and autistic tendencies. Children's age and gender were collected by using a questionnaire based on primary caregivers' self-reports. Children's BMI was calculated by dividing the weight (kg) by height (m) squared (weight and height measured by investigators), and the World Health Organization Child Growth Standards for age- and sex-specific cutoffs were employed (38). Dietary habits of preschool children were assessed by caregivers' reports using the adapted Identification and Management of Feeding Difficulties scale (IMFeD) (39), which consists of 17 items, and higher total scores indicate better dietary habits. Cronbach's alpha coefficient of IMFeD was 0.887 in this study. Children's sleep disturbances were measured with the Children's Sleep Habits Questionnaire (CSHQ) (40), which contains 33 items and scores of every item based on caregivers' recollection of children's sleep behaviours occurring over a recent week. Higher total scores indicate greater sleep disturbances, and Cronbach's alpha value was 0.668 in this study. Autistic tendencies of preschool children were assessed using the Chinese version of the Clancy Autism Behaviour Scale (CABS) (41). The CABS contains 14 items, and higher total scores indicate greater autistic tendencies. Cronbach's alpha coefficient of the CABS was 0.809 in this study.
Data on prenatal and perinatal factors were obtained from the questionnaire including gestational age (weeks), birth weight (g), delivery mode, pregnancy complications (hypertension, diabetes, and anaemia), maternal prenatal and postnatal emotional symptoms, and exclusive breastfeeding. Preterm birth was defined as a gestational age < 37 weeks. Low birth weight was defined as infants with a birth weight below 2,500 g.
Information on region of kindergartens, parental education, parental marital status, parenting attitude, children's sibling, left-behind experience, and monthly household income (RMB) was collected from the questionnaire by the caregivers' response on the questionnaire. Left-behind experience was defined as the experience that children who had been left behind by one or both parent(s) who migrated to other cities for employment for more than 6 consecutive months. Contact physical abuse (hit or slapped the child on the bottom; hit or slapped the child on the hand, arm, or leg; pushed or shook the child, pulled the child's ears or other parts of the body; kicked the child very hard with the foot; hit or slapped the child on the face or head; hit or slapped the child on the bottom with an object; and hit the child very hard with fist) was assessed through the caregivers reporting the experience in the previous year. If one form of physical abuse was mentioned, the contact physical abuse variable was defined as “yes.” Caregiver's anxiety symptoms were evaluated using the Self-Rating Anxiety Scale (SAS) (42). The SAS contains 20 items in total, and the sum score of all items is the raw score. In the present study, the standard score which was calculated by multiplying 1.25 by the raw score was used. Higher standard scores of anxiety show a higher level of anxiety symptoms. Cronbach's alpha coefficient of the SAS was 0.82 (42).
Anxiety symptoms of preschool children were assessed using the Chinese version of the Spence Preschool Anxiety Scale (SPAS) (22). This scale has displayed good reliability and validity in a sample of Chinese preschool children (22, 36). The scale is a 28-item anxiety symptoms measure for preschool children. The SPAS includes 5 subscales: separation anxiety disorder, physical injury fears, social phobia, obsessive-compulsive disorder, and generalised anxiety disorder. Each subscale item was scored on a 5-point scale ranging from 0 (not at all true) to 4 (very often true). The scores of the total scale and each subscale could be obtained by calculating the sum of all relevant items. The total scale score was ≥48 having significant anxiety symptoms (43). Children with scores falling in the upper quartile of the distribution were deemed as having significant subtypes of anxiety symptoms, and the cutoff value was separation anxiety disorder ≥6, physical injury fears ≥12, social phobia ≥7, obsessive-compulsive disorder ≥6, and generalised anxiety disorder ≥5, respectively. In our study, Cronbach's alpha value for the subscales ranged from 0.613 to 0.728 and that for the total scale was 0.903.
Continuous variables are described as the mean ± standard deviation (SD), and differences between groups were tested by Student's t tests or analysis of variance. Categorical variables were expressed as frequencies and percentages, and the chi-squared (χ2) test was utilised for comparisons. Logistic regression analyses were conducted to explore the associations of children's total anxiety symptoms and anxiety symptoms in five subtypes with individual, prenatal and perinatal, and family factors; and odds ratio (OR) and its 95% confidence interval (CI) were reported. To select the optimal regression equation, variables with p < 0.05 were entered into multivariate logistic regression models and those with p < 0.10 were retained in the final model using the forward stepwise manner. The 10-fold cross-validation method was used to assess the performance (area under the curve (AUC), sensitivity, specificity, and accuracy) of the multivariate regression model to avoid overfitting. The entire dataset was divided into 10 non-overlapping equivalent subsets; nine subsets were used to produce a prediction model, and the model was validated with the last subset. The procedure was repeated 10 times to ensure that each subset was applied once for model verification. Cross-validation was performed using the “caret” and “pROC” package in R software (Version 4.1.0, R Foundation for Statistical Computing, Vienna, Austria). Other analyses were conducted using SPSS software version 23.0 (SPSS Inc., USA). All p-values < 0.05 (two-tailed test) were considered to be statistically significant.
A total of 3,802 questionnaires were issued; after checking for completeness and logic, 3,636 effective questionnaires were finally collected. Comparisons of some variables based on preschool children's anxiety symptoms are shown in Table 1. Of the 3,636 preschool children, the mean age was 4.5 ± 0.9 years; 45.8% were girls. The prevalence of anxiety symptoms was higher in girls than in boys. Significant differences between subjects displaying significant anxiety and those not displaying significant anxiety were detected in child dietary habits, sleep disturbances, and autistic tendencies; prenatal and postnatal emotional symptoms, pregnancy complications; and region of kindergartens, parental education, parenting attitude, children's sibling, left-behind experience, contact physical abuse, and caregivers' anxiety symptoms.
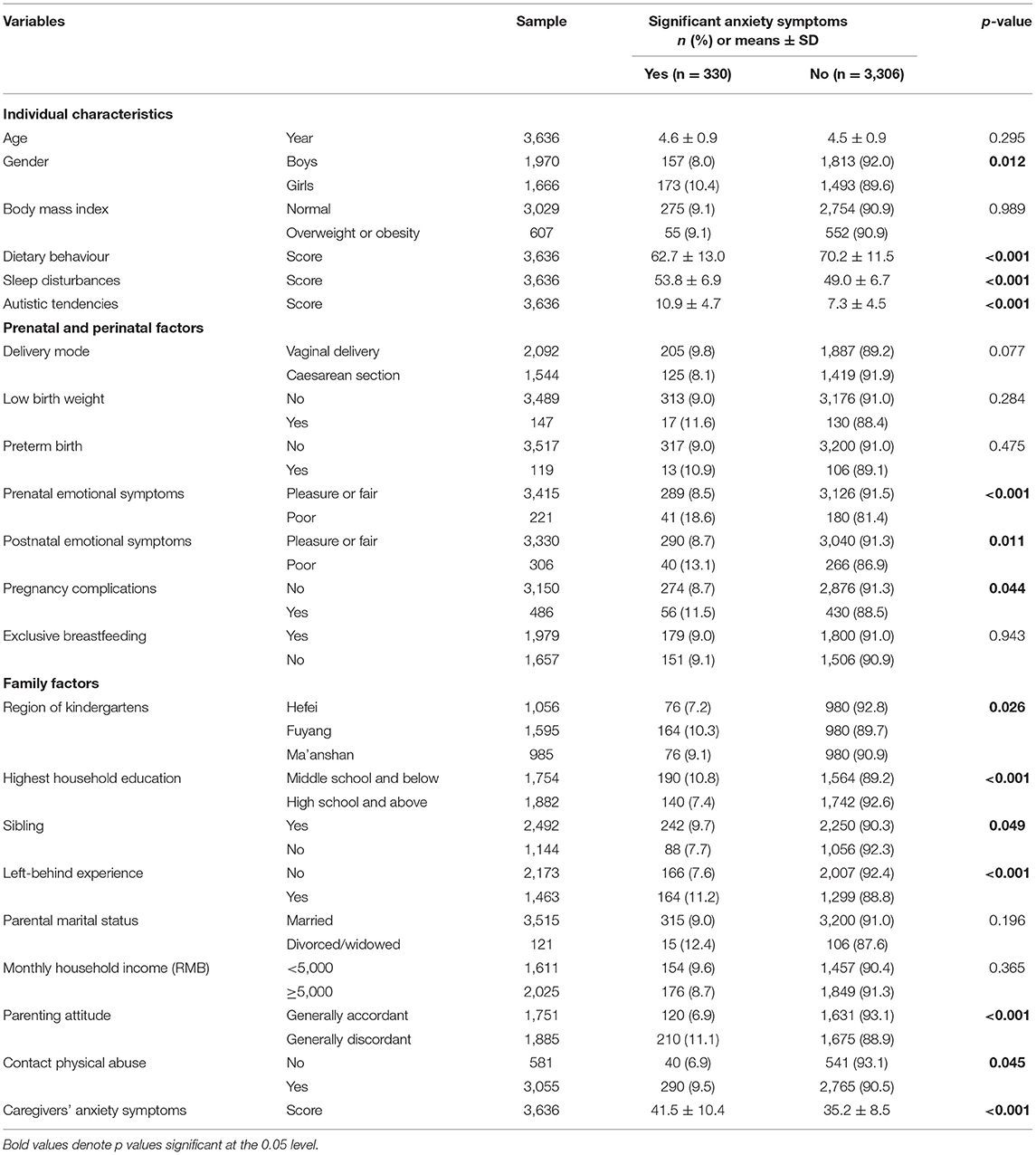
Table 1. Individual, prenatal and perinatal, and family factors by preschool children's anxiety symptoms.
As presented in Table 2, the mean total score of anxiety symptoms was 25.3 (SD = 15.5). A total of 330 (9.1%) children met the criteria for significant anxiety symptoms. When stratified by age, the results indicated that preschool children aged 3 years were found to score significantly higher on the separation anxiety disorder subscale (p = 0.017), with no significant difference in different age groups on scores of the total scale and other subscales. Significant gender differences were detected in the total anxiety scale and all subscales (p < 0.05).
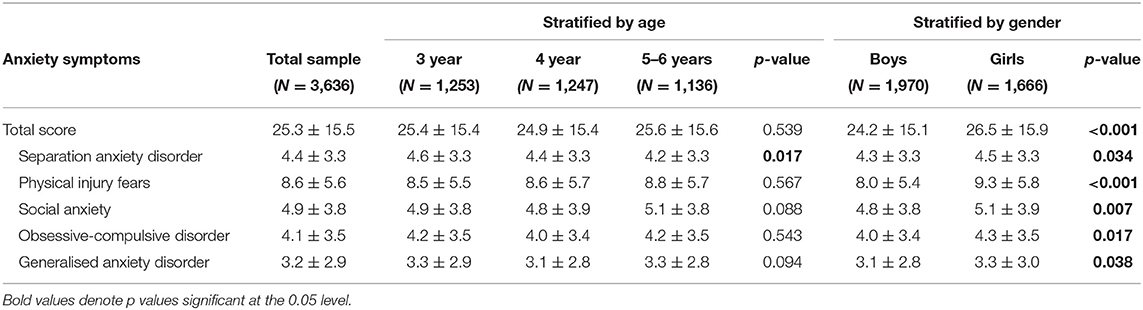
Table 2. Anxiety symptoms scores (mean ± SD) for overall sample and subgroups of preschool children.
Compared with their peers, children with significant anxiety symptoms were more likely to be girls and to have siblings; left-behind experience; poor dietary habits; more sleep disturbances; more autistic tendencies; mothers who had poor prenatal and postnatal emotional symptoms; mothers who had pregnancy complications; region of kindergartens in Fuyang; parents with middle school or less education or discordant parenting attitudes; experienced contact physical abuse; and caregivers with more anxiety symptoms (p < 0.05; Table 1).
The result of bivariate correlations indicated that children's gender, dietary habits, sleep disturbances, and autistic tendencies; prenatal and postnatal emotional symptoms and pregnancy complications; and parental education, monthly household income, parenting attitude, contact physical abuse, and caregivers' anxiety symptoms were associated with children's anxiety symptoms (Supplementary Table 1).
As shown in Table 3, the results of multivariate logistic regression analysis indicated that girls (OR = 1.50; p = 0.001), left-behind experience (OR = 1.29; p = 0.043), more sleep disturbances (OR = 1.05; p < 0.001), more autistic tendencies (OR = 1.12; p < 0.001), poor prenatal emotional symptoms (OR = 1.54; p = 0.027), and caregivers with more anxiety symptoms (OR = 1.03; p < 0.001) were associated with increased risks of significant anxiety symptoms. In contrast, better dietary habits (OR = 0.98; p < 0.001) were associated with a decreased risk of significant anxiety symptoms.
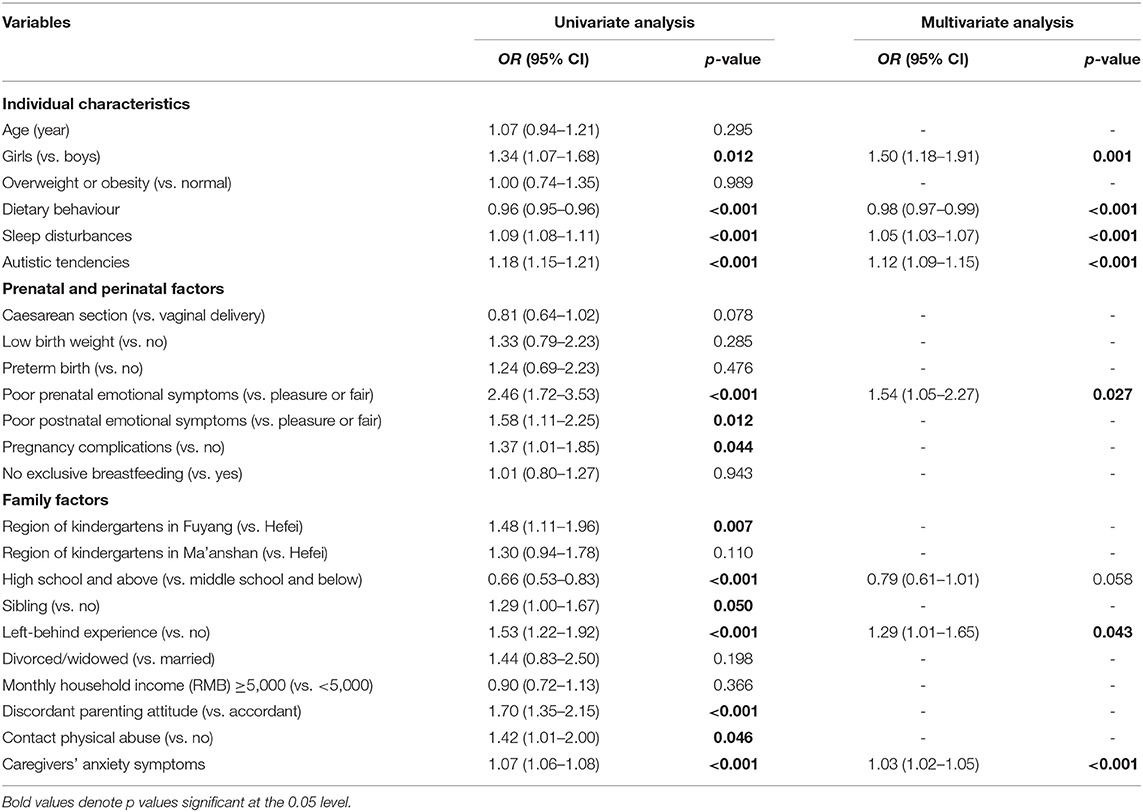
Table 3. Logistic regression models of significant anxiety symptoms and associated factors among preschool children.
To further investigate the relevant factors of five subtypes of anxiety symptoms among preschool children, the multivariate logistic regression analyses were separately performed (Table 4). The results of the analyses showed that girls, sleep disturbances, and more autistic tendencies were significantly associated with increased risks of all anxiety subtypes. Better dietary habits were associated with a decreased risk of all anxiety subtypes except for obsessive-compulsive disorder. Poor prenatal emotional symptoms increased the risks of generalised anxiety disorder, and poor postnatal emotional symptoms enhanced the odd of separation anxiety disorder. Pregnancy complications increased the risk of obsessive-compulsive disorder. The region of kindergartens in Ma'anshan was associated with increased risks of all anxiety subtypes except for separation anxiety disorder. Left-behind experience was at increased risk of physical injury fears. In addition, caregiver anxiety symptoms were significantly associated with increased odds of all anxiety subtypes.

Table 4. Multivariate logistic regression models anxiety symptoms in different subtypes and associated factors among preschool children.
The receiver operator characteristic (ROC) curve based on the highest accuracy of 10-fold cross-validation for the regression model of anxiety symptoms is presented in Figure 1. The result of 10-fold cross-validation indicated that the mean AUC, sensitivity, specificity, and accuracy were 0.78 (95% CI: 0.76–0.80), 70.45% (95% CI: 61.60–79.31%), 78.18% (95% CI: 71.50–84.87%), and 71.15% (95% CI: 63.67–78.64%), respectively. The multivariate regression models for most subtypes of anxiety symptoms demonstrated acceptable discriminative accuracy (Supplementary Table 2).
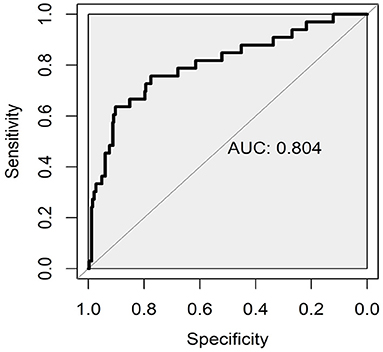
Figure 1. Receiver operating characteristic curves (ROC) for the predictive performance of regression model of anxiety symptoms.
Due to the scarcity of large sample data regarding preschool children's anxiety symptoms in China, we conducted this cross-sectional study, including 3,636 preschool children, to explore the prevalence of anxiety symptoms and comprehensive factors. The present study found that 9.1% of child participants had significant anxiety symptoms, which was within the reported prevalence range of 7.5–22.2% from European countries and America (2–4, 24, 44), and higher than the rate of 3.3% in one Chinese study (36), but lower than that of other two Chinese studies with rates of 14.1 and 15.2% (35, 43). The wide range of prevalence rates for anxiety may be due to the populations' inherent population differences among countries and various assessment scales being used in different studies. These prevalence rates indicate that the anxiety of preschool children cannot be ignored.
Regarding individual characteristics, one interesting finding was that significant gender differences were detected for the scores of total and subtypes of anxiety symptoms. This finding was supported by one study, which has indicated that girls are affected significantly more often than boys by anxiety disorder, and gender differences might begin at preschool age (24). However, Franz found that girls reported significantly more separation anxiety disorder than boys did (2). On the contrary, no significant gender differences are detected for preschool children's anxiety in some other studies (22, 23). In contrast to gender differences, age differences only partially appeared. Although previous studies have indicated that younger children display higher scores of anxiety symptoms than older children (21, 22), the present study showed that 3-year-old children had higher scores of separation anxiety disorder, which may be attributed to their transition from the family to kindergarten. In China, most children, particularly the 3-year-old children, have just entered kindergarten. These children may experience a fear of separation as they attempt to adapt to the kindergarten life. The reasons for this separation anxiety are ambiguous, and more studies on the development and the mechanism of gender and age differences are needed for further investigation.
In addition, this study confirmed the associations between emotional and behavioural problems and anxiety among preschool children. The findings demonstrated that poor dietary habits, sleep disturbances, and autistic tendencies were associated with anxiety symptoms in preschool children. Indeed, the notion that problematic behaviours are often comorbid with mental disorders has been raised over the years (10, 45, 46). One study among 2- to 6-year-old children has indicated that anxiety symptoms are associated with a higher score of dietary behavioural problems (45). Sleep disturbances (such as late bedtime and short sleep duration) affect problematic behaviours including anxious behaviour in 5-year-old children (47). A longitudinal study has shown that infant sleep disturbances at 2 and 24 months predict anxiety symptoms at 3 years, and a bidirectional association with anxiety symptoms preceding later sleep problems seems to exist (25). Recent research has reported that anxiety symptoms are present in preschool children with autism spectrum disorder more than in typically developing children (45). In addition, a nationwide twin cohort study from Sweden discovers positive relationships between autistic-like traits and anxiety symptoms (48). This study provides more evidence on the effects of emotional and behavioural problems on preschool children's anxiety.
When referring to prenatal and perinatal factors, the results of univariate analysis revealed that poor prenatal and postnatal emotional symptoms and pregnancy complications were associated with significant anxiety symptoms in preschool children, and poor prenatal emotional symptoms were still statistically significant in multivariate analysis. Early exposure to adversities particularly during pregnancy may affect the development of the child's brain and mental health (30, 49). In line with this study, previous research has shown that children exposed to prenatal and postnatal adverse emotional symptoms are at higher risks of anxiety (27, 50). Evidence has indicated that prenatal stress has programming effects on the foetal hypothalamic–pituitary–adrenal (HPA) axis (51). Alterations in the foetal HPA axis can be long-term; therefore, the offspring may have an elevated risk of psychiatric disorders in childhood (52). Besides, associations between prenatal/perinatal risk factors and children's anxiety disorders could be mediated through parenting and family functioning or alterations in infant brain structure and function (53, 54). In addition, studies have indicated that prenatal and perinatal adversities have negative effects on mother–infant interactions, infant temperament, sleep, mental development, autism, and internalising behavior (55, 56). It should be noted that prenatal/perinatal factors and some individual factors reported above are prone to coexistence and accumulation, which can result in child anxiety.
Family played an important role in child development. A recent meta-analysis has shown that left-behind children (LBC) have an 85% higher risk of anxiety than non-LBC (57). Consistent with the literature, the results of this study revealed that LBC had a 29% increased risk of anxiety and a 46% increased risk of social anxiety. Parental labour migration and the resulting parent–child separation is common in China and leads to changes in the family environment (58). Although parental labour migration may bring economic benefits for families, it may generate hidden costs for the health of LBC (57, 59). Given that parental labour migration can sometimes not be avoided, multidimensional interventions including proactive policies and protective factors are warranted to prevent LBC from adverse health outcomes. Additionally, the results of this study suggested that caregivers' anxiety symptoms were positively associated with preschool children' anxiety symptoms. This finding is supported by theoretical models of the intergenerational transmission of anxiety, which indicates multiple pathways for the transmission of anxious cognition and behaviours (60, 61). Research has reported that caregivers or parents seem to create an anxiety-rearing environment by modelling anxious behaviours, exerting too much control over their children, and promoting anxious cognitions through the use of verbal threats, which fosters anxiety in the offspring (13, 60–63). Overall, more prospective studies are needed to clarify the association between caregivers' anxiety symptoms and preschool children's anxiety symptoms and relevant mechanistic research may benefit prevention and treatment intervention programs for anxiety.
While the underlying mechanisms of anxiety disorders are not fully understood, studies on animals and humans suggest that they are multifactorial disorders caused by the interaction between genetic and environmental factors. Researchers have proposed the genetic and epigenetic risks in the aetiology of anxiety disorders, especially in the case of familial aggregation (64, 65). Available data suggest that first-degree relatives of patients are more susceptible to developing an anxiety disorder compared with relatives of the healthy control group (20). Meanwhile, several risk genes contributing to the development of anxiety disorders have been identified (66). However, genetic factors do not act in isolation in anxiety disorders but rather interact with environmental factors. The interaction between genetic and environmental factors has been explained by epigenetic mechanisms in recent years (67, 68). The review by Babenko et al. (68, 69) concluded that prenatal stress can trigger epigenetic changes in the placenta and brain and then induce powerful influences on offspring mental health in human studies and animal models. Moreover, one study has demonstrated that effects of prenatal depressive symptoms and socioeconomic status on foetal brain development are partially modulated by genetic risk, which further confirmed gene–environment interdependence (70). Although this study included individual internal and external factors, genetic factors were limited. Future studies should pay more attention to the interaction between genetic and environmental factors.
One strength of this study is the larger sample size of preschool children and the age-appropriate validated measurement tools to assess children's anxiety symptoms. Another strength is that this study comprehensively explored factors at multiple levels of social ecology including individual, prenatal and perinatal, and family factors, which might provide a more holistic understanding of influencing factors for anxiety symptoms among preschool children. Despite these strengths, several limitations of this study should be noted. First, this study was based on the responses of a parental or other primary caregiver on a questionnaire, and prenatal and perinatal factors were retrospectively collected; hence, the possibility of reporting and recall bias cannot be eliminated. Second, preschool children were only selected from Anhui Province and a convenience sample. Thus, the external validity of the results and generalizability to the general population are partially limited. Third, this study employed a cross-sectional design, making it difficult to identify a causal relationship. Besides, in this study, these factors from pregnancy to early childhood occur sequentially or display coexistence and accumulation, and we cannot clarify their relationships. Although we applied relevant optimal models to control confounding factors, we still cannot clarify whether the interactions of the various factors amplify or attenuate the risk of child anxiety. Future longitudinal studies are required to examine causal pathways in these relationships and to determine the potential effects and interactions of prenatal, perinatal, and family factors on anxiety symptoms. Additionally, research on the underlying mechanism is important to implement prevention and intervention programs for anxiety.
In conclusion, anxiety symptoms in preschool children were prevalent, particularly in girls. Many factors from pregnancy to preschool age involving children's poor dietary habits, sleep disturbances, autistic tendencies, left-behind experience, maternal poor pregnancy emotional symptoms, and more caregiver anxiety symptoms were associated with significant anxiety symptoms among preschool children. The findings highlighted the importance of understanding early-life risk factors for anxiety, and efficient prevention and intervention strategies should be implemented in early childhood even to the perinatal period.
All data generated or analyzed during this study are included in this article and Supplementary Material. Further inquires can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Anhui Medical University. Written informed consent to participate in this study was provided by the participant's legal guardian/next of kin.
XD designed this study and wrote the manuscript. NL, WS, HW, QS, XG, ML, QQ, LS, and MC recruited the participants, administered the assessment, and undertook the data collation and analysis. JW and YS guided and revised the writing. All authors listed have read the final manuscript and approved it for publication.
This work was supported by the National Natural Science Foundation of China (Grant Number: 81872704) and the Natural Science Foundation in Higher Education of Anhui (Grant Number: KJ2020A0208).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge the efforts of the research team, the local Centre for Disease Control and Prevention, and all kindergartens as well as all the children and families who participated in this research.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.778291/full#supplementary-material
1. Ezpeleta L, Keeler G, Erkanli A, Costello EJ, Angold A. Epidemiology of psychiatric disability in childhood and adolescence. J Child Psychol Psychiatry. (2001) 42:901–14. doi: 10.1111/1469-7610.00786
2. Franz LMBC, Angold AMRC, Copeland WPD, Costello EJPD, Towe-Goodman NPD, Egger HMD. Preschool anxiety disorders in pediatric primary care: prevalence and comorbidity. J Am Acad Child Psy. (2013) 52:1294–303. doi: 10.1016/j.jaac.2013.09.008
3. Wichstrøm L, Belsky J, Berg-Nielsen TS. Preschool predictors of childhood anxiety disorders: a prospective community study. J Child Psychol Psyc. (2013) 54:1327–36. doi: 10.1111/jcpp.12116
4. Petresco S, Anselmi L, Santos IS, Barros AJD, Fleitlich-Bilyk B, Barros FC, et al. Prevalence and comorbidity of psychiatric disorders among 6-year-old children: 2004 Pelotas birth cohort. Soc Psych Psych Epid. (2014) 49:975–83. doi: 10.1007/s00127-014-0826-z
5. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. (2005) 62:593. doi: 10.1001/archpsyc.62.6.593
6. Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L. et al. Lifetime prevalence of mental disorders in US adolescents: results from the national comorbidity survey replication-adolescent supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. (2010) 49:980–9. doi: 10.1016/j.jaac.2010.05.017
7. Bosquet M, Egeland B. The development and maintenance of anxiety symptoms from infancy through adolescence in a longitudinal sample. Dev Psychopathol. (2006) 18:517–50. doi: 10.1017/S0954579406060275
8. Bufferd SJ, Dougherty LR, Carlson GA, Rose S, Klein DN. Psychiatric disorders in preschoolers: continuity from ages 3 to 6. Am J Psychiatry. (2012) 169:1157–64. doi: 10.1176/appi.ajp.2012.12020268
9. Côté SM, Boivin M, Liu X, Nagin DS, Zoccolillo M, Tremblay RE. Depression and anxiety symptoms: onset, developmental course and risk factors during early childhood. J Child Psychol Psyc. (2009) 50:1201–8. doi: 10.1111/j.1469-7610.2009.02099.x
10. Kertz SJ, Sylvester C, Tillman R, Luby JL. Latent class profiles of anxiety symptom trajectories from preschool through school age. J Clin Child Adolesc. (2019) 48:316–31. doi: 10.1080/15374416.2017.1295380
11. Lau EX, Rapee RM. Prevention of anxiety disorders. Curr Psychiat Rep. (2011) 13:258–66. doi: 10.1007/s11920-011-0199-x
12. Ahmadzadeh YI, Eley TC, Leve LD, Shaw DS, Natsuaki MN, Reiss D, et al. Anxiety in the family: a genetically informed analysis of transactional associations between mother, father and child anxiety symptoms. J Child Psychol Psyc. (2019) 60:1269–77. doi: 10.1111/jcpp.13068
13. Field AP, Lester KJ, Cartwright-Hatton S, Harold GT, Shaw DS, Natsuaki MN, et al. Maternal and paternal influences on childhood anxiety symptoms: a genetically sensitive comparison. J Appl Dev Psychol. (2020) 68:101123. doi: 10.1016/j.appdev.2020.101123
14. Guhn M, Emerson SD, Mahdaviani D, Gadermann AM. Associations of birth factors and socio-economic status with indicators of early emotional development and mental health in childhood: a population-based linkage study. Child Psychiat Hum D. (2020) 51:80–93. doi: 10.1007/s10578-019-00912-6
15. Klein AM, Schlesier-Michel A, Otto Y, White LO, Andreas A, Sierau S, et al. Latent trajectories of internalizing symptoms from preschool to school age: a multi-informant study in a high-risk sample. Dev Psychopathol. (2019) 31:657–81. doi: 10.1017/S0954579418000214
16. Liu L, Wang M. Parental corporal punishment and child anxiety in China: the moderating role of HPA-axis activity. J Affect Disorders. (2020) 273:500–7. doi: 10.1016/j.jad.2020.04.055
17. Liu Z, Li X, Ge X. Left too early: the effects of age at separation from parents on Chinese rural children's symptoms of anxiety and depression. Am J Public Health. (2009) 99:2049–54. doi: 10.2105/AJPH.2008.150474
18. Silberg JL, Gillespie N, Moore AA, Eaves LJ, Bates J, Aggen S, et al. Shared genetic and environmental influences on early temperament and preschool psychiatric disorders in hispanic twins. Twin Res Hum Genet. (2015) 18:171–8. doi: 10.1017/thg.2014.88
19. Trzaskowski M, Zavos HM, Haworth CM, Plomin R, Eley TC. Stable genetic influence on anxiety-related behaviours across middle childhood. J Abnorm Child Psychol. (2012) 40:85–94. doi: 10.1007/s10802-011-9545-z
20. Hettema JM, Neale MC, Kendler KS. A review and meta-analysis of the genetic epidemiology of anxiety disorders. Am J Psychiatry. (2001) 158:1568–78. doi: 10.1176/appi.ajp.158.10.1568
21. Spence SH, Rapee R, McDonald C, Ingram M. The structure of anxiety symptoms among preschoolers. Behav Res Ther. (2001) 39:1293–316. doi: 10.1016/S0005-7967(00)00098-X
22. Wang M, Zhao J. Anxiety disorder symptoms in Chinese preschool children. Child Psychiat Hum D. (2015) 46:158–66. doi: 10.1007/s10578-014-0461-7
23. Lavigne JV, Lebailly SA, Hopkins J, Gouze KR, Binns HJ. The prevalence of ADHD, ODD, depression, and anxiety in a community sample of 4-year-olds. J Clin Child Adolesc Psychol. (2009) 38:315–28. doi: 10.1080/15374410902851382
24. Paulus FW, Backes A, Sander CS, Weber M, von Gontard A. Anxiety disorders and behavioral inhibition in preschool children: a population-based study. Child Psychiat Hum D. (2015) 46:150–7. doi: 10.1007/s10578-014-0460-8
25. Jansen PW, Saridjan NS, Hofman A, Jaddoe VW, Verhulst FC, Tiemeier H. Does disturbed sleeping precede symptoms of anxiety or depression in toddlers? the generation R study. Psychosom Med. (2011) 73:242–9. doi: 10.1097/PSY.0b013e31820a4abb
26. Towe-Goodman NRP, Franz LM, Copeland WP, Angold AM, Egger HM. Perceived family impact of preschool anxiety disorders. J Am Acad Child Psy. (2014) 53:437–46. doi: 10.1016/j.jaac.2013.12.017
27. Bendiksen B, Aase H, Diep LM, Svensson E, Friis S, Zeiner P. The Associations between pre- and postnatal maternal symptoms of distress and preschooler's symptoms of ADHD, oppositional defiant disorder, conduct disorder, and anxiety. J Atten Disord. (2020) 24:1057–69. doi: 10.1177/1087054715616185
28. Barker DJ. The origins of the developmental origins theory. J Intern Med. (2007) 261:412–7. doi: 10.1111/j.1365-2796.2007.01809.x
29. Lewis AJ, Austin E, Knapp R, Vaiano T, Galbally M. Perinatal maternal mental health, fetal programming and child development. Healthcare. (2015) 3:1212–27. doi: 10.3390/healthcare3041212
30. Lautarescu A, Craig MC, Glover V. Prenatal stress: effects on fetal and child brain development. Int Rev Neurobiol. (2020) 150:17–40. doi: 10.1016/bs.irn.2019.11.002
31. Dachew BA, Scott JG, Mamun A, Alati R. Hypertensive disorders of pregnancy and the risk of anxiety disorders in adolescence: findings from the Avon longitudinal study of parents and children. J Psychiatr Res. (2019) 110:159–65. doi: 10.1016/j.jpsychires.2019.01.001
32. Hentges RF, Graham SA, Fearon P, Tough S, Madigan S. The chronicity and timing of prenatal and antenatal maternal depression and anxiety on child outcomes at age 5. Depress Anxiety. (2020) 37:576–86. doi: 10.1002/da.23039
33. Ståhlberg T, Khanal P, Chudal R, Luntamo T, Kronström K, Sourander A. Prenatal and perinatal risk factors for anxiety disorders among children and adolescents: a systematic review. J Affect Disorders. (2020) 277:85–93. doi: 10.1016/j.jad.2020.08.004
34. Berber Çelik Ç, Odaci H. Does child abuse have an impact on self-esteem, depression, anxiety and stress conditions of individuals? Int J Soc Psychiatr. (2020) 66:171–8. doi: 10.1177/0020764019894618
35. Wu G, Bai L, Shi Q, Ren H, Wang H. Relationship between preschool children's anxiety and behavior problems. Chin J Woman Child Health Res. (2016) 27:1173–6. doi: 10.3969/j.issn.1673-5293.2016.10.003
36. Xu Y, Yan Q, Tong L. Study on the associations between parenting stress and anxiety symptoms among urban preschoolers. Chin J Child Health Care. (2020) 28:563–7. doi: 10.11852/zgetbjzz2019-1129
37. Zhou F, Zhu M, Jiang H, Feng X. The effect of early intervention in preschool children anxiety. China Mod Doctor. (2015) 53:59–61. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZDYS201511021&DbName=CJFQ2015
39. Deng C, Zhang W, Jin Y, Feng JH, Liu QJ, Liu YL, et al. Analysis of relationship between eating problems of 1-5 years old children and the feeding behavior. Chin J Child Health Care. (2012) 20:686–8. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ERTO201208009&DbName=CJFQ2012
40. Liu Z, Wang G, Tang H, Wen F, Li N. Reliability and validity of the children's sleep habits questionnaire in preschool-aged Chinese children. Sleep Biol Rhythms. (2014) 12:187–93. doi: 10.1111/sbr.12061
41. Sun X, Allison C, Auyeung B, Matthews FE, Zhang Z, Baron-Cohen S, et al. Comparison between a mandarin Chinese version of the childhood autism spectrum test and the Clancy autism behaviour scale in mainland China. Res Dev Disabil. (2014) 35:1599–608. doi: 10.1016/j.ridd.2014.02.005
42. Tanaka-Matsumi J, Kameoka VA. Reliabilities and concurrent validities of popular self-report measures of depression, anxiety, and social desirability. J Consult Clin Psychol. (1986) 54:328–33. doi: 10.1037//0022-006x.54.3.328
43. Fu Z, Hao J, Chen S, Qiao S, Guo L, Ding Y, et al. Investigation of the status of anxiety and related factors for the preschool children in Harbin. Chin J Child Health Care. (2013) 1:10–2. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ERTO201301003&DbName=CJFQ2013
44. Bufferd SJ, Dougherty LR, Carlson GA, Klein DN. Parent-reported mental health in preschoolers: findings using a diagnostic interview. Compr Psychiat. (2011) 52:359–69. doi: 10.1016/j.comppsych.2010.08.006
45. Johnson CR, DeMand A, Shui A. Relationships between anxiety and sleep and feeding in young children with ASD. J Dev Phys Disabil. (2015) 27:359–73. doi: 10.1007/s10882-015-9419-3
46. Chase RM, Pincus DB. Sleep-related problems in children and adolescents with anxiety disorders. Behav Sleep Med. (2011) 9:224–36. doi: 10.1080/15402002.2011.606768
47. Suda M, Nagamitsu S, Obara H, Shimomura G, Ishii R, Yuge K, et al. Association between children's sleep patterns and problematic behaviors at age 5. Pediatr Int. (2020) 62:1189–96. doi: 10.1111/ped.14267
48. Lundström S, Chang Z, Kerekes N, Gumpert CH, Råstam M, Gillberg C, et al. Autistic-like traits and their association with mental health problems in two nationwide twin cohorts of children and adults. Psychol Med. (2011) 41:2423–33. doi: 10.1017/S0033291711000377
49. O'Donnell KJ, Glover V, Barker ED, O'Connor TG. The persisting effect of maternal mood in pregnancy on childhood psychopathology. Dev Psychopathol. (2014) 26:393–403. doi: 10.1017/S0954579414000029
50. Lawrence PJ, Creswell C, Cooper PJ, Murray L. The role of maternal anxiety disorder subtype, parenting and infant stable temperamental inhibition in child anxiety: a prospective longitudinal study. J Child Psychol Psyc. (2020) 61:779–88. doi: 10.1111/jcpp.13187
51. Weinstock M. Alterations induced by gestational stress in brain morphology and behaviour of the offspring. Prog Neurobiol. (2001) 65:427–51. doi: 10.1016/S0301-0082(01)00018-1
52. Moisiadis VG, Matthews SG. Glucocorticoids and fetal programming part 1: Outcomes. Nat Rev Endocrinol. (2014) 10:391–402. doi: 10.1038/nrendo.2014.73
53. Adamson B, Letourneau N, Lebel C. Prenatal maternal anxiety and children's brain structure and function: a systematic review of neuroimaging studies. J Affect Disorders. (2018) 241:117–26. doi: 10.1016/j.jad.2018.08.029
54. Matvienko-Sikar K, Murphy G, Murphy M. The role of prenatal, obstetric, and post-partum factors in the parenting stress of mothers and fathers of 9-month old infants. J Psychosom Obstet Gynaecol. (2018) 39:47–55. doi: 10.1080/0167482X.2017.1286641
55. Field T. Postnatal anxiety prevalence, predictors and effects on development: a narrative review. Infant Behav Dev. (2018) 51:24–32. doi: 10.1016/j.infbeh.2018.02.005
56. Wang C, Geng H, Liu W, Zhang G. Prenatal, perinatal, and postnatal factors associated with autism: a meta-analysis. Medicine. (2017) 96:e6696. doi: 10.1097/MD.0000000000006696
57. Fellmeth G, Rose-Clarke K, Zhao C, Busert LK, Zheng Y, Massazza A, et al. Health impacts of parental migration on left-behind children and adolescents: a systematic review and meta-analysis. Lancet. (2018) 392:2567–82. doi: 10.1016/S0140-6736(18)32558-3
58. Wen M, Lin D. Child development in rural China: children left behind by their migrant parents and children of nonmigrant families. Child Dev. (2012) 83:120–36. doi: 10.1111/j.1467-8624.2011.01698.x
59. Qin J, Albin B. The mental health of children left behind in rural China by migrating parents: a literature review. J Public Ment Health. (2010) 9:4–16. doi: 10.5042/jpmh.2010.0458
60. Fisak B, Grills-Taquechel AE. Parental modeling, reinforcement, and information transfer: risk factors in the development of child anxiety? Clin Child Fam Psych. (2007) 10:213–31. doi: 10.1007/s10567-007-0020-x
61. Murray L, Creswell C, Cooper PJ. The development of anxiety disorders in childhood: an integrative review. Psychol Med. (2009) 39:1413–23. doi: 10.1017/S0033291709005157
62. Aktar E, MajdandŽić M, de Vente W, Bögels SM. Parental social anxiety disorder prospectively predicts toddlers' fear/avoidance in a social referencing paradigm. J Child Psychol Psyc. (2014) 55:77–87. doi: 10.1111/jcpp.12121
63. McLeod BD, Wood JJ, Weisz JR. Examining the association between parenting and childhood anxiety: a meta-analysis. Clin Psychol Rev. (2007) 27:155–72. doi: 10.1016/j.cpr.2006.09.002
64. Meier SM, Deckert J. Genetics of anxiety disorders. Curr Psychiatry Rep. (2019) 21:16. doi: 10.1007/s11920-019-1002-7
65. Gottschalk MG, Domschke K. Novel developments in genetic and epigenetic mechanisms of anxiety. Curr Opin Psychiatry. (2016) 29:32–8. doi: 10.1097/YCO.0000000000000219
66. Schiele MA, Domschke K. Epigenetics at the crossroads between genes, environment and resilience in anxiety disorders. Genes, Brain and Behavior. (2018) 17:e12423. doi: 10.1111/gbb.12423
67. Bartlett AA, Singh R, Hunter RG. Anxiety and epigenetics. Adv Exp Med Biol. (2017) 978:145–66. doi: 10.1007/978-3-319-53889-1_8
68. Babenko O, Kovalchuk I, Metz GA. Stress-induced perinatal and transgenerational epigenetic programming of brain development and mental health. Neurosci Biobehav Rev. (2015) 48:70–91. doi: 10.1016/j.neubiorev.2014.11.013
69. Fatima M, Srivastav S, Mondal AC. Prenatal stress and depression associated neuronal development in neonates. Int J Dev Neurosci. (2017) 60:1–7. doi: 10.1016/j.ijdevneu.2017.04.001
Keywords: anxiety, preschool, child, left-behind, prenatal
Citation: Ding X, Wang J, Li N, Su W, Wang H, Song Q, Guo X, Liang M, Qin Q, Sun L, Chen M and Sun Y (2021) Individual, Prenatal, Perinatal, and Family Factors for Anxiety Symptoms Among Preschool Children. Front. Psychiatry 12:778291. doi: 10.3389/fpsyt.2021.778291
Received: 16 September 2021; Accepted: 19 November 2021;
Published: 20 December 2021.
Edited by:
David Cohen, Sorbonne Universités, FranceReviewed by:
Cedric Galera, Université de Bordeaux, FranceCopyright © 2021 Ding, Wang, Li, Su, Wang, Song, Guo, Liang, Qin, Sun, Chen and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yehuan Sun, eWhzdW5fYWhtdV9lZHVAeWVhaC5uZXQ=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.