 Darron T. Smith
Darron T. Smith Sonya C. Faber
Sonya C. Faber NiCole T. Buchanan
NiCole T. Buchanan Dale Foster
Dale Foster Lilith Green
Lilith Green
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Psychiatry , 20 January 2022
Sec. Psychopathology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.774736
This article is part of the Research Topic Can Psychedelic Therapies open a New Frontier in Mental Healthcare (Or Will the Bubble Burst?) View all 22 articles
Psychedelic medicine is an emerging field that examines entheogens, psychoactive substances that produce non-ordinary states of consciousness (NOSC). 3,4-methylenedioxymethamphetamine (MDMA) is currently in phase-3 FDA clinical trials in the United States (US) and Canada to treat the symptoms of posttraumatic stress disorder (PTSD). MDMA is used in conjunction with manualized therapy, because of its effectiveness in reducing fear-driven stimuli that contribute to trauma and anxiety symptoms. In 2017, the FDA designated MDMA as a “breakthrough therapy,” signaling that it has advantages in safety, efficacy, and compliance over available medication for the treatment of trauma-, stress-, and anxiety-related disorders such as PTSD. In the US and Canada, historical and contemporary racial mistreatment is frequently experienced by Black people via a variety of macro and micro insults. Such experiences trigger physiological responses of anxiety and fear, which are associated with chronically elevated stress hormone levels (e.g., cortisol and epinephrine), similar to levels documented among those diagnosed with an anxiety disorder. This paper will explore the benefits of entheogens within psychedelic assisted-therapy and their potential benefits in addressing the sequelae of pervasive and frequent negative race-based experiences and promoting healing and thriving among Black, Indigenous and other People of Color (BIPOC). The author(s) discuss the ethical responsibility for providing psychedelic-assisted therapy within a culturally competent provider framework and the importance of psychedelic researchers to recruit and retain BIPOC populations in research and clinical training.
Post-traumatic stress disorder (PTSD) can be debilitating for many people, as triggers (thoughts, visuals, sounds, smells) reproduce the same physiological effect within the body as if the individual is experiencing the actual trauma again at that moment (1). The current, most successful methods of treating trauma or disorders caused by trauma can be incredibly harrowing for the patients involved, as they often require that patients retell and, thereby relive, their traumatic experiences (1). Though exposure-based therapies are the most effective for PTSD, individuals are asked to revisit traumatic events dozens of times until they become fully desensitized. These treatments often trigger extreme emotional reactions and can reactivate traumatic memories, which, in turn, may lead to a reluctance to seek professional mental health care (2). There is, however, a therapy through which patients have been able to experience past traumatic events while attenuating the anxious activation often associated with discussion of past traumas (3). The patient/client can examine their trauma and their past, explore it from different vantage points, discuss it without becoming retraumatized, process it in new ways, and eventually sever the associated misplaced feelings of guilt or shame. This is the promise of psychedelic medicine, which multiple studies have show can accelerate the healing process (4, 5).
These substances, long known in antiquity to provide therapeutic benefits, have only recently been rehabilitated and put to test in clinical studies to provide evidence for psychological distress. Psychedelic medicine is an emerging field of research, clinical and spiritual practice that examines substances classified as hallucinogens in the human mind, body, and spirit (6). Psychedelics, also referred to as entheogens, have been used for thousands of years worldwide in religious ceremonies, rituals, and healing (7). The discovery of the psychoactive properties of substances such as LSD has led to research into other classical psychedelics including mescaline and psilocybin, which are now offering a novel avenue for the treatment of patients with an array of psychiatric disorders that current medications cannot entirely help (8). However, this space has been largely limited to White people in the past 150 years for a multitude of reasons from lack of access to concerns of legality, particularly with the over-representation of black and brown inmates from drug-related offenses to the limitation in the racial makeup of research subjects and scholars (9, 10).
Throughout this paper, we will use PTSD as a model indication because there is a greater body of literature and more empirical studies addressing this indication. For people of color, however, the emotional injury of racial trauma is the overwhelming psychological harm for which improved tools are needed. Racial trauma, sometimes resulting in PTSD, has been neglected as a serious research subject, lacks established diagnostic criteria, and most alarmingly, suffers from a lack of clear treatment recommendations (11). Psychedelics are under observation as a useful tool for the treatment of racial trauma among a range of psychological disorders. In this paper, the authors will foreground the racial trauma specifically experienced by Black1 Americans, but we recognize more broadly the experiences of Black, Indigenous and people of color (BIPOC), who all share specific histories with racial oppression.
This paper will first provide a brief history of and examine the current status of psychedelic-assisted therapy as it pertains to BIPOC and the reason why these substances can be so helpful in treating race-based trauma. This paper also seeks to illuminate the multi-layered gap between the approval of these new substances and their use in BIPOC communities. Finally, the authors will discuss how this gap is being bridged and offer suggestions in improving greater access with regards to researchers and participants of color.
It is important to note that psychedelic substances are not designed to be a panacea of racial healing or trauma healing. Without a trained specialist in the treatment of trauma, and specifically race-based trauma, these experiences can leave the patient vulnerable to their emotions and further add to their trauma (e.g., (14)). In fact, true healing relies on societal change within multiple institutions and community support along with corrective interpersonal experiences of safety. When used appropriately in conjunction with integrative therapy and self-reflection processes, psychedelics can act as a powerful adjunct to psychological healing.
The authors of this manuscript are Black and White2 researchers in mental health and biotechnology, with direct experience treating patients with psychedelics or research interests in psychedelics. The authors have experienced or witnessed racism that has resulted in increased stress, depression, anger, shock, and trauma. It is the position of this paper that BIPOC individuals should be able to access approved psychedelic-assisted therapy treatments (with an experienced therapist/facilitator) for emotional healing after exposure to psychological trauma and the psychobiological consequences that can follow.
The authors have interviewed numerous Black people who have suffered from racial trauma as a result of large and small wounds from a lifetime of discrimination. These individuals are in immediate need of mental health services, yet express a fear of psychedelic medicine, in particular, the vulnerability that an altered consciousness brings with it. These concerns are not unfounded. Psychedelic-assisted therapy can be unsafe when it is led by an inexperienced provider or a therapist who does not understand the nuances of racism (14). This paper aims to shine a light on the situation of those in the BIPOC community who could benefit from psychedelic treatments and provide a road map for greater access to psychedelic-assisted treatment.
The first wave of the modern psychedelic movement in the US came in the 1950's and 1960's, at a time when young people were more openly experimenting with cannabis, heroin, and magic mushrooms (psilocybin). At the same time, scientists were studying these compounds, and clinical researchers were finding positive medicinal effects of psychedelics in the treatment of psychiatric disorders. These investigations yielded valuable information, though often from unwitting participants of color through government-funded research (15). The CIA actively studied the effects of lysergic acid diethylamide (LSD) and other mind-altering drugs to assess their use as agents of mind-control and psychological torture in over a hundred experiments under a project labeled MK Ultra (15). Often in the setting of prisons and hospitals, the limits of these substances were explored in test subjects who were not provided the courtesy of informed consent nor had the power to decline. Strauss and colleagues (15) in a recent review have documented the unjust and inhumane utilization of primarily Black racialized, incarcerated men and others institutionalized as psychiatric patients in numerous questionable experiments with shoddy and unethical methods.
Scientific research into psychedelics in the US ground to a halt in the 1970's. With ongoing political unrest over Civil Rights and the Vietnam war, the Nixon administration stoked fears of lawlessness in efforts to justify punitive action taken on this growing use into mind altering compounds. Nixon's “War on Drugs” campaign commenced in 1971 and would equate anti-Vietnam war protests along with Blacks and Latinos with newly designated illegal drugs (16). John Ehrlichman, former White House counsel and Chief Domestic Advisor under Nixon, ultimately admitted to Harper Magazine in 2016, “We knew we couldn't make it illegal to be either against the war or Black, but by getting the public to associate the hippies with marijuana and Blacks with heroin, and then criminalizing both heavily, we could disrupt those communities… Did we know we were lying about the drugs? Of course, we did” (17). Nixon set in motion decades of federal policies through the disproportionate arrests and incarceration of Black and Latino men for the transgression of experimenting with psychedelics and other healing substances.
The repercussions of the Nixon administration's heavy-handed federal drug policy took on a life of its own as each presidential administration has since continued policies aimed at the persecution and criminalization of racialized minorities for the use of these substances (e.g., Nancy Reagan's “Just Say No” campaign and Bill Clinton's 1994 crime bill were part of the effort to revisit and expand the War on Drugs; (16)). These unjust policies were carried forward, as it came to light later that the CIA was involved in the disbursement of drugs such as crack cocaine in the 1980's to Black neighborhoods and even profiting off the sales (18). This was all occurring despite the equivalent rate of sale and consumption in White communities (19, 20). For example, part of the Reagan-era Anti-Drug Abuse Act included a penalty known as the “100-to-1 sentencing ratio.” for the same amount of crack cocaine (typically used by Blacks) as powdered cocaine (typically used by Whites). A minimum penalty of 5 years was given for 5 grams of crack cocaine but for 500 grams of powdered cocaine, in a deliberate attempt to keep White Americans out of the dragnet (e.g., 21, 22). With the stroke of a presidential pen, Black men would find themselves in shambles, hampered with a trail of life-long negative consequences associated with having greater contact with biased law enforcement and the potential of lethal force (23).
The negative repercussions of this era remain an issue and have left stigmas in both the affected communities and the research into substances classified as illicit in the 1970's and 1980's. Psychedelic research later regained some traction in the 1990's, and its increase up to the current era has been slow. America is attempting to come full circle. The country is gradually reckoning with the racial trauma BIPOC have experienced historically at the hands of a racially biased society and its institutions (24). These traumas, occurring at the micro and macro level of society, include police violence and the explosion of the prison industrial complex sanctioned through the “War on Drugs.” Meanwhile, society is gradually recognizing that some of the very drugs at the root of the pathologic expansion of the modern prison industrial complex, which were originally intended to facilitate disproportionate incarceration of Black and Brown Americans to increase racial divisions, can instead allow for the healing of these traumas.
As this paper will highlight, after decades of scientific research with organizations such as Multidisciplinary Association for Psychedelic Studies (MAPS), the use of psychedelics as an adjunct in the treatment of mental health disorders is on the verge of gaining legal ground within the medical community. Communities of color have notoriously been and are still left out of these spaces. The authors intend to illuminate this disparity and offer ideas to bridge the gap so that BIPOC can benefit from these resources and treatment opportunities as one way to help heal from the ills brought on by societal oppression.
Although many minoritized persons in North America experience discrimination based on their ethnicity, anti-Black sentiment remains one of the most pervasive types of negative stereotyping with significant and well-documented health impacts (25). Being Black in the US still means learning to live with the persistent threat of race-based stress in the form of slights, slurs, insults, violence and even death (25). A single negative racialized event can certainly trigger post-traumatic stress disorder, but the cumulative effects of racial trauma in the Black community are often the catalyst for a transformative traumatic event.
The DSM-5 defines PTSD as first having been exposed (directly or indirectly) to trauma, followed by symptoms from that exposure causing disruption in one's life in a multitude of ways. Criterion A specifically defines trauma as direct or indirect exposure to or threat of an experience that includes death, serious injury or sexual violence (26, p. 271). The indirect exposure includes witnessing an event, learning of a loved one's event or being exposed to “aversive details” of an event (26, p. 271). With these new guidelines, the DSM-5 provisions are more inclusive of the detrimental effects of modern forms of Black antipathy and bias than the previous fourth edition manual. This expanded definition of PTSD encompasses what clinicians already see—African Americans live with higher rates of PTSD, as reported in the scientific literature (27).
Racial events include a direct physical assault, a traumatic event (or trauma-inducing experiences) involving close family members as well as individuals frequently exposed to graphic details about trauma (28). Racially traumatizing events may comprise experiences such as relentless microaggressions, police profiling, and also systemic racism in law enforcement, healthcare and education. Black people throughout the US and Canada experience some form of racial microaggression as a near daily occurrence from the micro to the macro levels of society, including cultural and historical traumas (29). According to Sue and colleagues (30), “Almost all interracial encounters are prone to microaggressions.” Racial mistreatment or microaggressions are subtle acts of dehumanization that can range from poor service in restaurants and unsolicited hair touching to race-based doxxing or swatting, verbal insults and outright physical violence (25, 31, 32). These can be considered racially traumatizing experiences as research shows that the severity and prevalence of PTSD symptoms do not change as a function of if the experience meets Criterion A (33–35) as well as findings that demonstrate that such events are connected to PTSD symptoms above and beyond Criterion A (36).
Black communities are mentally and emotionally impacted by public displays of inhumanity (e.g., the epidemic of extrajudicial police killings; 37–39), as they routinely witness racialized tragedies committed against people who look similar to them and inhabit the same social circles. Part of the cycle of trauma for Black people is the discounting or outright denial of the injury's existence and one's racialized reality by other citizens who do not experience anti-black sentiment (40). With enough frequency and unpredictability, such racial stressors can lead to racial trauma, and the accumulation of these negative occurrences can have real long-lasting consequences for Black mental health ((41–43)).
In an extensive review of the causes of race-based trauma linked to PTSD in communities of color, Williams and colleagues (24) described racial trauma as a cumulative psychological injury caused by hate or fear of an individual due to their ethnicity or race that overwhelms the individual's ability to cope. Racial trauma is associated with severe physiological and psychological harm across BIPOC populations (44). The harm is especially pernicious because it is associated with an immutable characteristic or identity (e.g., one's race) which can cause the consequences to further worsen over time, resulting in symptoms of PTSD and a variety of other psychopathologies (24, 44). Notably, traumatic experiences and PTSD can initiate a cascade of consequent psychological, physiological and epigenetic effects on the body (45).
Ongoing racial dehumanization weathers the brain, mind, and body, leaving deep intergenerational scars at the molecular level (46). Those affected by racial trauma frequently report both psychological and physical symptoms that are associated with PTSD including trauma-related emotional arousal and reactivity (e.g., hypervigilance, irritability), labile mood, intrusive thoughts, exaggerated startle response, flashbacks, and sleep disturbances, such as insomnia and nightmares (47, 48). These symptoms are correlated with abnormal hormone and neurotransmitter levels (e.g., serotonin, GABA, dopamine, cortisol) as well as abnormal brain wave morphology (49). Such dysregulation of the brain and body leads to poor physical and psychological health outcomes (46, 50, 51).
Physiologically, the presence of ongoing arousal from daily systemic racism triggers a stress response within a feedback loop system known as the hypothalamic pituitary adrenal axis (HPA-axis), which is responsible for the proliferation of cortisol, epinephrine (i.e., adrenaline) and norepinephrine (52). This system regulates the body's fight, flight, or freeze response, which is often associated with increased heart rate, shallow breathing and fatigue. This process can be activated in as little as a moment of real or imagined threatening stress (53) and can leave the body susceptible to illness and disease, particularly when experienced frequently over time (54). Correspondingly, those subjected to racialized trauma have persistently elevated stress hormone (e.g., cortisol) levels, which is associated with gastrointestinal distress, hypertension, diabetes, heart disease, stroke, and an overall lowered immune response (38, 52).
Just as the body reacts poorly under chronic stress, the brain's stress response causes a disruption of neurotransmitters, neural networks and brain communication and signaling (55). Brain imaging of neurons has demonstrated how dendrites—tiny projections of branches at the terminal end of neurons— shrink in a stressful social environment (56). Studies utilizing quantitative electroencephalography (qEEG) also exhibited dysregulation of brainwave frequency homeostasis in similar circumstances (57–59). Brain frequencies function within a very narrow oscillatory window (60). If they oscillate in frequency or amplitude outside this normal range, it can signal pathology within the brain and mind (61). These frequencies can become dysregulated as a result of childhood trauma—neglect, emotional abuse, sexual abuse, food scarcity, lack of bond with primary care giver (i.e., birth mother), incarcerated family member—creating heightened vulnerability to later psychiatric illness (62). Trauma has numerous effects within the cortical framework, interfering with an individual's capacity to feel, think, and connect with others. Notably, many diagnosed with a trauma-related disorder describe a lack of pleasure and a disassociation from those around them including feelings of depression, difficulties with planning, thinking, and memory (63, 64).
Historically, psychiatry has underutilized the neuroscience of the brain and the medical community has been slow to utilize the newest brain science (65). Furthermore, as has been reported in other areas of medicine, there are disparities is the quality of care patients receive, with Black patients being less likely to receive psychiatric treatment referrals or to be diagnosed with PTSD by a licensed psychiatrist or psychologist, and PTSD secondary to racial trauma is under diagnosed and under treated (63, 66, 67). Raced-based PTSD results in profound physiological and psychological damage (63, 64, 68) that can cause permanent changes in the brain. Fortunately, the brain is plastic and amenable to change with effective treatment. Neurotransmitters, brainwaves and brain connectivity have been shown to normalize with utilization of neurotechnology devices and psychedelic medicines in conjunction with psychotherapy (61). With these treatments, patients have reported reduced symptomatology, limited side effects and an overall improvement in health (61). In concert, adaptive behavior, positive emotional states, and supportive relationships with others become more sustainable.
Despite the clear evidence of ongoing emotional harm to Black Americans caused by systemic racism, there has been relatively little research focused on interventions (11). Psychedelics are one avenue worth exploring for their potential to help alleviate racial trauma (69). MDMA-assisted psychotherapy has already been shown to be a highly effective approach for PTSD, with three administrations of MDMA substantially more effective than traditional pharmacologic treatment methods such as life-long prescription of SSRI medication (70, 71). As such, MDMA-assisted therapy was designated a “breakthrough therapy” by the FDA in 2017 and is now being made available through the Expanded Access (compassionate use) program.
Williams and colleagues (72) found significant reductions in depression, anxiety, and stress following naturalistic use of psychedelics for racial trauma. These results are consistent with the increasing evidence that psychedelic substances can catalyze healing for those suffering from various mental disorders (3). With the breakthrough designation of MDMA and psilocybin by the FDA for PTSD and depression (see Table 1) and the publication of at least 14 well-designed clinical studies on LSD, MDMA, psilocybin and ayahuasca for a range of mood disorders, the potential for hallucinogens as therapeutics is now being realized (73–75).
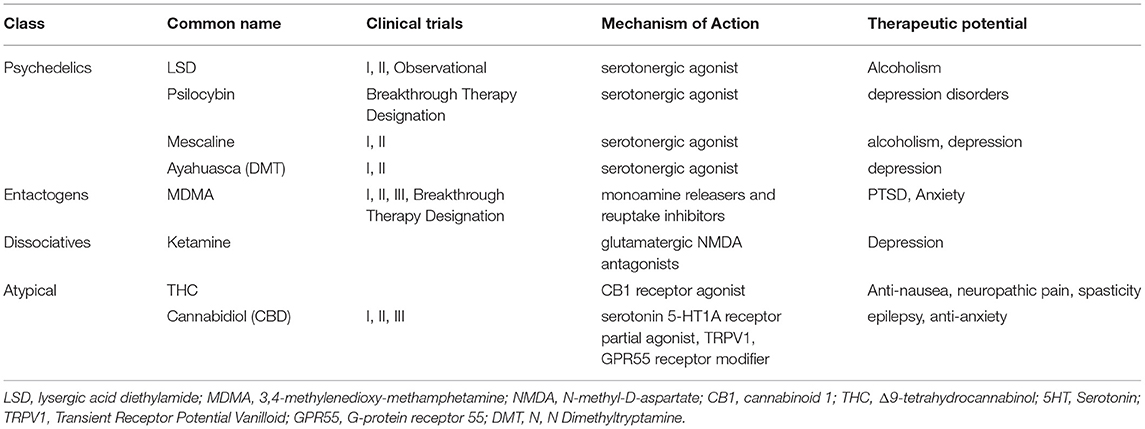
Table 1. Common psychedelic substances and research.
Other research in this area includes ketamine-assisted therapy. Halstead and colleagues (76) provided intensive outpatient treatment for a client with treatment-resistant PTSD due to racial trauma and childhood sexual abuse. During the 13-day therapeutic intervention, clinicians administered ketamine on four occasions, integrated with mindfulness-based cognitive therapy and functional analytic psychotherapy (FAP). The treatment providers were therapists of color, using a culturally informed approach and anti-oppression lens to conceptualize the client's trauma. This case study found significant reductions in symptoms post-treatment and sustained benefits 4 months after (76).
Under current development is an open-label proposal to MAPS for a comparative effectiveness study that explores the potential enhancement of neurofeedback therapy with MDMA treatment for African Americans in the deep South with race-based trauma. If funded, this study would be the first to examine the effectiveness of entheogens and neurofeedback therapy in concert as a treatment protocol. One of the authors on this paper, an interdisciplinary scholar, researcher and licensed physician associate in mental health, has proposed a prospective single-site, randomized, controlled two-arm, between-subject comparison open-label study assessing the safety and effectiveness of MDMA-assisted therapy in combination with neurofeedback therapy in participants diagnosed with PTSD whose index trauma is a racialized event.3
Once psychedelics become legal medicines, there are still grave concerns that they will remain out of reach to Black Americans. Black researchers have supported the use of entheogens such as MDMA for the healing of racial wounds with the critical caveat that providers must be well-equipped to work with clients of color or risk doing more harm than good (14). "As with much of medicine, many providers have not received in-depth and ongoing culturally sensitive training (79, 80). In fact, many providers harbor implicit biases themselves that have not been explored, to the detriment of their patients (e.g., (81–83)) and yet, they are also the gatekeepers to diagnosis and treatment. Numerous studies show that treatment and prescribing habits can differ based on patient race (84–88). Racial group affiliation is particularly influential when it comes to the diagnosis and management of mental health disorders. When presented with the same symptoms, physicians were more likely to diagnose Black patients with schizophrenia or bipolar disease while White patients were diagnosed with major depression (66, 89). The data is consistent with other studies and suggest that disparities in the diagnosis of schizophrenia result in part from clinicians misperceiving the relevance of mood symptoms among Blacks compared with other racial or ethnic groups. In addition, African American subjects have also been shown to be less likely to receive the most effective antipsychotic medications (89). Psychotropic prescription-writing habits of practitioners have been demonstrated to be significantly influenced by the provider's perception of the patient's emotional health only when it comes to their White patients and not in their Black patients. In all, these misperceptions lead to misdiagnosis, which in turn, impact treatment and prescribing patterns and lead to lower standards of care (90–93).
Specifically in the case of PTSD, publications show race disparities in the treatment and prescriptions of pharmacotherapy (94–96). For example, a racial hierarchy of treatment has been found in US veterans. Compared with White veterans, Latino veterans were less likely to receive a minimal trial of pharmacotherapy (96). Furthermore, African American veterans were the least likely to receive any treatment at all in the 6 months post diagnosis. This disparity in treatment of veterans with PTSD is a well-documented, significant, and ongoing issue that has been further demonstrated in a recent analysis of more than 1,500,000 veterans with PTSD (96). Despite being diagnosed with PTSD at similar rates across categories, females and Black veterans were less likely to receive PTSD disability awards, which hindered their ability to even begin treatment (97).4 It should be noted that the US Department of Veterans Affairs, who serve as the primary mental healthcare provider for many in the BIPOC community, are beholden to Federal restrictions on the use of psychedelics in treatment (98, 99).
The common and ongoing refrain in these studies is a lack of understanding of the emotional state of Black people, which results in habitual overdiagnosis with psychotic disorders, an underdiagnosis of mood and anxiety disorders, and simultaneous undertreatment in all areas of medicine (66, 88). Moreover, Black physicians represent only 2% of all US psychiatrists according to the American Psychiatric Association, revealing a dearth of representation (100). This further underscores the need for culturally informed clinicians training (101, pp. 37-42). What's more, there have been no manualized protocols or clinical trials for people of color with race-based trauma in psychedelic research. Given these existing disparities, concerns remain as to whether psychedelics will be appropriately provided to people of color.
In treating patients with alternative, plant-based medicines, it is also important to recognize receptiveness as a potential barrier to treatment within Black communities. Statistics show that Blacks in the US have the lowest use of any racial group for psychedelics. In addition, the starting age for psychedelics use is older than for all other racial groups (102). One explanation is simply that Blacks have been socialized to avoid psychedelics due to the disproportionate consequences of illicit use (9, 102). For instance, though arrests have dramatically dropped in states that have legalized cannabis, incarceration and life-consequences for use of mind-altering substances remain disproportionately high for communities of color in many states and counties in the US (103). In addition, Black individuals may, for good reasons, not perceive psychedelics as safe (9). The cultural stigma against psychedelic use makes it more difficult to convince Black individuals that psychedelic-assisted therapy could be a beneficial intervention. The destigmatization of psychedelics as a category remains an ongoing process, but the destigmatization of Blacks using psychotherapeutics remains further out of reach (74). Legitimizing psychedelics in the eyes of Black Americans will necessarily be a process in which those who have experienced successful therapy can convey the benefits to those suffering from treatable psychological trauma (104). A parallel societal change must also occur in which law enforcement, psychology and medicine becomes accepting and encouraging of seeing Black people as using these substances and experiencing healing from trauma. This may be a difficult road to walk, but for many seeking relief, it will be well worth the travel.
Clinical trials testing the safety and effectiveness of psychedelic-assisted psychotherapy use a protocol in which a psychedelic compound is combined with a defined sequence of therapy sessions with the goal of molding and supporting the patient's psychedelic experience. These protocols have developed into a standardized practice which, following FDA approval, will be legally required by governmental authorities every time psychedelic-assisted therapy is initiated. Use of psychedelics outside of this framework would, therefore, not be clinically or ethically acceptable. The types of sessions which are required to prepare patients, engender trust, and successfully establish a therapeutic relationship with the guiding facilitator include preparatory, medication, and integration sessions (105). The clinical facilitator's role is ultimately to assist in translating the experience into a therapeutic shift in cognition and behavior.
In order to best support patients in their future psychedelic-assisted therapy, MAPS was granted FDA approval to initiate a clinical study in 2010 where future potential providers enrolled in the volunteer trial for MDMA were permitted, according to the protocol, to receive a single dose of MDMA in conjunction with psychotherapy exactly as defined for patients in the pivotal phase III MDMA trial for patients. This step was an unprecedented but necessary step to give credibility to the clinicians and researchers who work in the psychedelic field, given the difficulty of legally organizing these types of experiences (106). The trial was designed to give providers this experience while collecting data on healthy volunteers.
Recent accounts of the experiences of BIPOC providers who have taken part in these early volunteer studies have now been published and highlight the potential as well as the challenges that other BIPOC participants may face in such trials ((14, 107)). In his psychedelic experience, a researcher who identifies as an Asian, queer male, described having vivid visions of hybrid animals and plants related to his cultural heritage, his sexual identity, and the intersectionality between the two (108). Insights gained from the integration of these experiences included proactive strategies to counter internalized racism, and the realization that he must radically accept the intersectionality of his sexual and cultural identity to overcome societal barriers of discrimination and internalized minority stress. It is important to note that the co-therapists in this study were a female of color and a White male. The author specifically highlighted the role of the therapist of color regarding his positive experience. He explained, “There was also an indescribable experience of being “seen” and “heard” as a queer person of color in a White heteronormative society simply by having an older female therapist of color siting patiently across the room, conveying acceptance, nurturance, and in a sense, non-judgmental “permission” to open up about my issues” ((108), p. 63; Buchanan, 2020).
In a differing account during the MAPS-sponsored MDMA trial, a Black female Marriage and Family Therapist describes her experience as a participant in an MDMA session. In this session, she reported initial feelings of freedom and ancestral connection, feeling the presence of her grandmother guiding her toward peace. These feelings transitioned to feelings of confusion, as racial wounds rose to the surface of her experience. When sharing her frustration with her sitting therapists, their lack of empathy led to a fundamental misinterpretation of her emotional state. Ultimately, she was received with a microaggression that deepened the disconnection between her mind and body and left her feeling grievously misunderstood. She stated that the MDMA would not allow her to isolate herself into her usual coping mechanisms and, instead, left her vulnerable to others. She suffered for many weeks from the trauma of the experience. Despite this, after much work to integrate her MDMA experience, two truths were made clear to her, “more Black folx deserve to feel human, free from the oppression and traumas we've endured, and that nothing can separate me from Divine Love” (14).
Buchanan (109) discusses these narratives and their connection to the larger Black community, and she is deeply critical of the preparation and training current psychedelic-assisted therapists and trainees are receiving to meet the needs of BIPOC populations. Facilitators first must unpack their own biases before they can then aid others in unpacking their traumas. Buchanan further notes that these therapy paradigms have not centered the needs of BIPOC people seeking healing and, hence, puts them at additional risk of harm. The participants are in a position of increased vulnerability given both the heart-opening effects of the entheogens, which strip people of their typical psychological protections used to navigate interracial interactions, and the fact that participants cannot exercise their right to leave because of the effects of the psychedelic substances. This should increase the requirements, Buchanan argues, for intersectional cultural humility (110, 111), deep and prolonged engagement in the providers' personal work on their social identities and connections to privilege and oppression (112), and understanding of identity-related factors, such as race, that influence set and setting (113).
Multiple studies have shown that people exhibit greater empathic resonance to individuals with a similar skin color (91, 114–116). The tendency to favor in-groups is so strong that the categorization of people into in-groups based on even temporary and arbitrary traits creates biases resulting in favoritism (117). In regard to White people's perception of Black people's pain, brain imaging reveals an anti-Black racial bias, (i.e. Black participant's pain was assessed less painful than White people's pain; (114, 118)). This kind of assessment of bias is compelling because it does not rely on the self-assessment of the participant, rather the mere viewing of an individual in pain causes a measurable sensorimotor resonance dependent on the perceived racial similarity between the victim and the observer (119). These studies provide a mechanism to help explain the reduction in empathy observed between Black patients and their White providers, and explain both the misinterpretations of mood symptoms in the diagnosis of schizophrenia and the disconnect in MDMA therapy, as described above (14, 66, 89).
The lack of empathy toward Black (91) and other BIPOC individuals, based on out-group bias can be mirrored in the client-therapist relationship and cannot be expected to be bridged simply by psychedelics alone (also see Table 3 for further resources). Even in the absence of potent empathy-expanding compounds, clinicians of every background must hold up the mirror to consider if they have the cultural competence to offer therapy in a way that will not harm their client. This is not to imply that people only ever have empathy for their own in-group and that this is immutable. Research also suggests that racially-based sensitivity to others' pain can move from implicit to explicit if made salient (115). This underlines the importance of shining a light on these implicit racial disparities in the social and medical sciences. The current situation is that in the USA, most therapists are White, and most clients of color will be seeing a White therapist, this makes implicit bias an important topic. If therapists cannot not perceive the harm created by racial trauma, because they underestimate the effects of implicit bias or “colorblindness,” they will be unable to carry out this work, regardless of the manner in which it is carried out. We all see race (115, 119, 120) the question that remains is how we see it and what we do with this knowledge.
As underscored by the previously mentioned moving accounts of psychedelic-assisted therapy, culturally relevant therapy is necessary for success (121). Ethically, only culturally competent practitioners should administer psychedelic compounds, particularly to Black patients who have inevitably experienced some racial trauma by virtue of living in racialized societies. Otherwise, there is a significant risk of causing harm to the patient, and the field of study is left vulnerable to critique (14). In one initiative to address this problem, MAPS conducted a grant-funded conference and training to teach BIPOC how to carry out MDMA-assisted therapy for PTSD (122, 123). The idea being that BIPOC providers would have greater cultural competency through life experiences on how to treat those in their communities (124). Although the conference portion, which was organized by people of color, was well-received, the training portion of the meeting, as noted by MAPS themselves, was problematic (122). We think that it is important to touch specifically on some of the reasons for the difficulties of this training because elements of the issues that emerged in the meeting regularly plague initiatives that revolve around issues of race (e.g., 125), and if we do not ask and understand the reasons, there will be that much more difficulty in providing the future training required for psychedelic-assisted therapy.
A post-hoc analysis of the training provides an opportunity for improvement at multiple levels. Most prominently, in the execution of the training event, there was a lack of power sharing with knowledgeable people of color. The lead trainer, appointed by MAPS, was a White woman with no experience providing diversity education (122). In training such as these, strong emotions are expected because the trainers are breaking taboos around speaking about the intersection between race and identity and the role of the individual in an unjust society (125, 126). An issue which often emerges is the difference in empathy and perception of racial issues between the White participants and those of color (e.g., 113). Many White Americans are too often concerned with denials of BIPOC experiences and defensive strategies to avoid the hard truths of everyday racism (126). Others attempt to skip to uncritical, poorly thought-out solutions to address complex, systemic issues on the nation's racist past and contemporary realities. Due to this, White participants often require lengthy, fact-laden, sometimes trauma-inducing engagements regarding all the ways systemic racism impacts people of color (125, 127).
Racially conscious training requires intense and skillful conversations about race (128). Critical conversations about race, though necessary for the training, may trigger racial trauma in people of color, whose distress can then trigger interracial anxiety in many White people (e.g., 126, 129, 130). Unfortunately, this being the first event of its kind, MAPS staff were unprepared for the emergence of this trauma by the participants at the meeting. The Black psychologist who secured the grant was an experienced diversity trainer, but because the grant funds were awarded to MAPS, she had no decision-making power, control over the agenda, or ability to select senior members of the training team with experience buffering the type of trauma that can be triggered by the material. Instead, her students who were there to be trained were enlisted to help. In addition, the senior BIPOC participants who were present were not utilized to help other participants who were triggered by the material. The few BIPOC members of the MAPS-selected training team were not qualified to do this work and were themselves triggered and unable to support others. Further, as described in an account by MAPS themselves (122), proper care was not taken to protect the identity of former participants in the MAPS studies, one of whom attended the event as a participant but whose study video was shown to the group without consulting her beforehand. It was traumatic for the participant to see herself on screen, and this triggered fears in participants of color reminiscent of research abuses such as the Tuskegee Syphilis Study (15, 122). As a result, the landmark event was stymied, and some participants felt unsafe, with a few leaving before it was over. The training of the therapist cohort was never completed, as such MAPS did not keep its promise to the therapists of color and their funders.
Despite all these missteps, there is much to be learned from past events. In that respect, MAPS has an opportunity as an institution to improve on mistakes by creating a more positive and inclusive clinical pathway where BIPOC can thrive in their psychedelic training programs. Facilitators trained by MAPS, however, cannot be the sole solution to the dearth of Black clinicians. This burdens training and certification programs with a tremendous bottleneck, especially as Black clinicians are realistically more fearful of the legal and reputational impacts of trying illicit substances. The current US psychology workforce is only 4% Black (131). Of the approximately 6,000 doctoral graduates of clinical psychology programs in the USA each year, about half will become active in client care and approximately 10% (or about three hundred) of these providers are Black (26). But any licensed professional can be trained in the area of psychedelic-assisted therapy. This list includes licensed clinical social worker (LCSW), physician associate (PA), nurse practitioner (NP), medical doctor, licensed professional counselor (LPC), and more.
In attempts to find additional solutions to the lack of appropriately trained providers, the California Institute of Integral Studies (CIIS) operates one of the few academic programs dedicated to educating the next generation of psychedelic practitioners. The CIIS has developed a Certificate in Psychedelic-Assisted Therapies & Research (CPTR) program, which aims to educate and prepare a broad range of mental health professionals for work in the field. The CPTR program is a hybrid of online learning and in-person training retreats that has been occurring for the last 5 years. Scholarships and need-based aid have been established for individuals from underrepresented communities as an opportunity to promote equity within the CPTR program. Though there are efforts to create BIPOC and LGBTQIA+ diversity and representation among CPTR trainees, the majority of the staff and faculty remain White. This only further reinforces the field-wide standard of lacking BIPOC faculty and supervisors (e.g., 10).
It is increasingly evident that more creative suggestions should be undertaken to ensure a more rapid implementation timeline for psychedelics training. Pairing such training programs with psychology departments at Historically Black Colleges and Universities (HBCUs) could bode for one option. Trained culturally competent clinical psychologists are graduating from these institutions and could be recruited to help alleviate the current shortage. The authors strongly recommend academic centers at Predominately White Institutions (PWIs) with newly established psychedelic programs reach out to these HBCUs to initiate an overdue process of cooperation that would mutually benefit both programs. HBCUs, who typically train the majority of black psychologists, would gain access to and training in psychedelic knowledge. Meanwhile, the collaboration would expose typically white students from psychedelic research programs to more BIPOC in their field, and if done correctly, could potentially allow for cross-cultural, inclusive training. In all, the issue of culturally competent therapy is one which must be addressed, in part, by University training programs for psychedelic medicine (Table 2).

Table 2. Academic potential in psychedelics.
It is imperative to note that many practicing psychologists (both BIPOC and non-BIPOC) have not likely received adequate graduate level training in cultural competency (136, 137). Just as many medical schools have begun to include specific training in social medicine, it would behoove practitioners to introduce a more effective culturally sensitive, inclusion therapy in the training of new clinicians (138). This would go a long way in raising all aspects of mental health and therapeutic care above and beyond psychedelic-assisted therapy.
Although the path to greater empathy and cultural competency for therapists who want to undertake this kind of work may seem long, there are tools available for continuing education and self-assessment. Use of these tools are necessary to help prevent any harm to BIPOC in the therapeutic setting. We have provided a resource table (Table 3) for both therapists and clients to further educate themselves with opportunities for self-assessment.
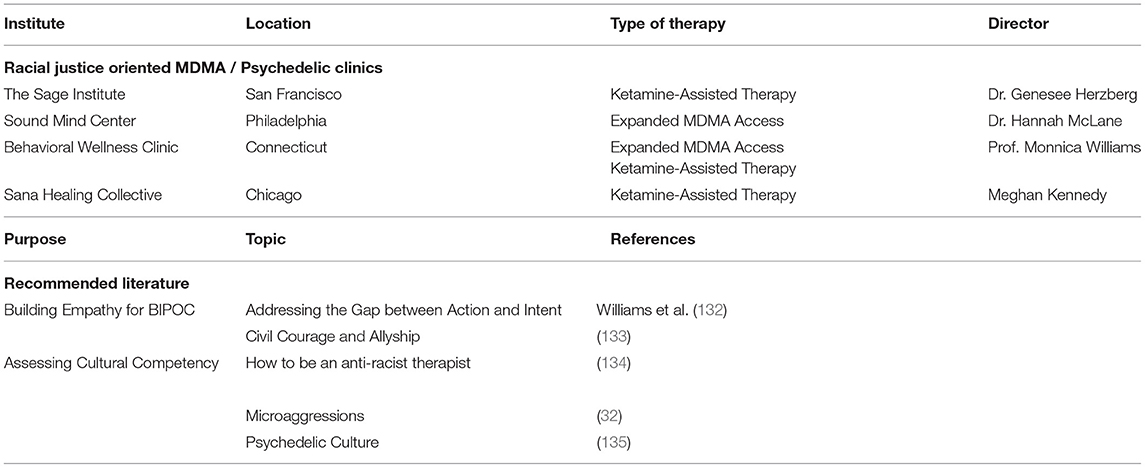
Table 3. Resource table.
There are organizations promoting Black people in psychedelics, including Chacruna's Racial Equity & Access Committee, The Ancestor Project, and People of Color Psychedelic Collective who are committed to bringing BIPOC agency and liberation to the forefront of the conversation. They seek to revolutionize psychedelic culture by making psychedelics more accessible to people of color while also combating the harms produced by the drug war and oppressive systems of injustice. To accomplish this, they are conducting community outreach to educate BIPOC about psychedelics' therapeutic and spiritual foundations, harm reduction, and general drug policy. By building inclusive spaces that allow BIPOC to safely explore psychedelics, they foster an environment that encourages vulnerability and collective healing. These organizations put BIPOC contributions to the field of psychedelics in the spotlight and hope to promote a narrative by and for communities of color. As the decriminalization and legalization of psychedelics becomes more commonplace, dedicated spaces that uplift and prioritize BIPOC voices and well-being are paramount to the evolution of the field of psychedelics.
The next phase of the psychedelic-assisted arm of this work is the Expanded Access Program, spearheaded by MAPS, which is now starting at multiple sites throughout the US. Expanded Access, also called Compassionate Use, allows patients to have use of an investigational medical product (one that has not yet been approved by the FDA) outside of a randomized clinical trial. The program's purpose is to grant access to potentially beneficial investigational treatments for people facing a serious or immediately life-threatening condition for which there is no satisfactory treatment currently available. This program will allow MDMA-assisted therapy to be available for people who have not responded to traditional therapies for PTSD, and it will also provide additional data on drug safety and how various subpopulations may respond to the treatment.
There are several sites in the US (Table 3) which are specifically focused on providing this expanded access care for people of color. These sites include Sage Institute, a center in California that has applied to be approved for expanded access and is specifically dedicated to providing high-quality, culturally responsive psychedelic therapy for underserved communities. The Sage Institute is active as both a therapeutic investigative site in San Francisco, and the colleagues at Sage have experience in ketamine-assisted therapy. SoundMind Center in Philadelphia, also on the list for expanded MDMA access, is a collective of psychiatrists, psychotherapists, and community organizers among others, dedicated to providing affordable, accessible, inclusive mental health care to Philadelphians, especially those who typically face marginalization within the healthcare system. The SoundMind collective currently has nine providers enrolled in FDA-approved training for MDMA assisted therapy and four others already certified in ketamine-assisted therapy. Behavioral Wellness Clinic in Connecticut, whose clinic personnel participated in the FDA-approved clinical trial of MDMA-assisted psychotherapy for PTSD, has a diverse FAP-trained and culturally-informed staff that includes seven members already trained on the FDA-approved MAPS protocol and are enrolled for final certification. The clinic also offers ketamine-assisted therapy for several indications, including racial trauma (76). These three sites will be the first specifically qualified to offer MDMA for patients suffering from racial trauma or PTSD caused by racial trauma.
Racially induced trauma and PTSD caused by racism are serious and widespread psychological issues that remain undertreated and under-researched (11). The body of literature, as reviewed in this paper, shows that people racialized as Black endure discrimination. And, in fact, Black individuals who suffer from racial trauma populate all areas of society regardless of socioeconomic status and educational attainment (77). These individuals are living with a heightened state of fear and trepidation, which has life-long repercussions (11). Such exposure to everyday racism takes its toll, leaving Black people vulnerable to a spectrum of diseases of the brain, mind, and body (139). In the wake of this daily systemic racism is a trail of inadequately treated patients with altered brain connectivity (140). The lack of treatment opportunities is a result of living in a racist society where BIPOC have been historically marginalized. This problem is multifaceted, multilayered and is emblematic of the general failings of American institutions—political, economic, education, healthcare, and justice—to make good on their promises of equality and inclusivity (e.g., higher education, 83, 103) (83). Despite these gross institutional injustices, there are solutions. Psychedelic-assisted treatment has great promise to provide relief for those suffering from PTSD and racial trauma (141). However, these new opportunities risk causing more harm to Black people than healing if personnel are not properly vetted and trained in both psychedelic therapy and race-based trauma. Although some universities are offering isolated courses, there is not a single university psychology or medical-based program offering a specialization in therapy for racial trauma (44). Thus, the current sites that are using culturally informed therapeutic practices need to be bolstered, and training programs with specific expertise in this area require accelerated funding.
Important measures have been assembled that allow for a more diverse recruitment of patients and culturally trained staff with the provision of functional ethical guidelines. However, there are still unmet needs in communities (military, BIPOC) suffering from PTSD and racial trauma (98). We, therefore, call for more explicit invitations for BIPOC medical professionals and psychology departments at HBCUs to become part of the conversation around the testing, prescription, therapeutic administration and commercialization of these medicines as they move into mainstream mental health care. Healing and well-being of the BIPOC community is dependent on such collaborations.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
DS worked on the initial draft, wrote a substantial portion of the sections, invited additional researchers, did the final edits for the paper, invited SF to help organize the sections, and invited LG to write about a section in the paper to include handling the conclusion and references. DF was invited to contribute regarding the brain and psychological impact of race-based trauma. NB wrote about race relations and its implications regarding racial trauma and psychedelic work. All authors contributed to the article and approved the submitted version.
SF was employed by the company Bioville GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to express their gratitude to Monnica Williams, Carsten Fisher, Tasha Sabino, Dana Strauss, Naomi Faber, and Manzar Zare for their assistance and input into this manuscript.
1. ^Black here refers to a “racial group” defined by the US government census. A racial group is often related to, but not equivalent to one's ethnic group identification and is not necessarily associated with genetic relatedness ((12)). For the purpose of this article, Black includes individuals racialized as Black (e.g., Black American, African American, or Black Canadian). These individuals may be native to or trace their origins to countries within the African Diaspora and where the native people typically share darker skin shades; however, settler-colonialism has resulted in Black people now having a full spectrum of skin shades. Importantly, Black is a social category, and as such, a person racialized as Black in the US or Canada may not be considered Black in other nations or societies (13).
2. ^It is important to understand “Whiteness” as a construct and not a skin color. Whiteness describes a privileged social and cultural group that acts as the accepted and elevated standard to which other racial groups are compared. It is a forced group membership that originated by oppressing people of color.
3. ^This same researcher is also developing a case study in which ketamine-assisted neurofeedback therapy is utilized in a transracial adoptee suffering race-based and abandonment trauma ((77, 78)).
4. ^More alarmingly, White veterans with misconduct separations were more likely to receive these disability awards than their Black counterparts who had no negative marks.
1. Brown LA, Williams M, Foa E. Psychotherapy for posttraumatic stress disorder. In: Simon N, Hollander E, Rothbaum B, Stein D, Editors. Textbook of Anxiety, Trauma, and OCD-Related Disorders, Third Edition. Washington, DC: American Psychiatric Publishing. ISBN: 978-1-61537-292-8 (2020). p. 543–56.
2. Imel Laska K, Jakupcak M, Simpson TL. Meta-analysis of dropout in treatments for posttraumatic stress disorder. J Consult Clin Psychol. (2013) 81:394–404. doi: 10.1037/a0031474
3. Read T. Psychedelic-assisted psychotherapy. In: Seminars in the Psychotherapies. Cambridge: Cambridge University Press (2021). p. 363.
4. Luoma JB, Chwyl C, Bathje GJ, Davis AK, Lancelotta R. A meta-analysis of placebo-controlled trials of psychedelic-assisted therapy. J Psychoactive Drugs. (2020) 52:289–99. doi: 10.1080/02791072.2020.1769878
5. Mitchell JM, Bogenschutz M, Lilienstein A, Harrison C, Kleiman S, Parker-Guilbert K, et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nat Med. (2021) 27:1025–33. doi: 10.1038/s41591-021-01336-3
6. Roberts TB. Psychoactive Sacramentals: Essays On Entheogens And Religion. San Francisco, CA: Council on Spiritual Practices (2001).
7. Labate BC, Cavnar C. Plant Medicines, Healing and Psychedelic Science: Cultural Perspectives. Santa Fe, NM: Springer (2018). doi: 10.1007/978-3-319-76720-8
8. Krediet E, Bostoen T, Breeksema J, van Schagen A, Passie T, Vermetten E. Reviewing the potential of psychedelics for the treatment of PTSD. Int J Neuropsychopharmacol. (2020) 23:385–400. doi: 10.1093/ijnp/pyaa018
9. George JR, Michaels TI, Sevelius J, Williams MT. The psychedelic renaissance and the limitations of a White-dominant medical framework: a call for indigenous and ethnic minority inclusion. J Psychedelic Stud. (2020) 4:4–15. doi: 10.1556/2054.2019.015
10. Michaels TI, Purdon J, Collins A, Williams MT. Inclusion of people of color in psychedelic-assisted psychotherapy: a review of the literature. BMC Psychiatry. (2018) 18:245. doi: 10.1186/s12888-018-1824-6
11. Williams MT, Haeny A, Holmes S. Posttraumatic Stress Disorder And Racial Trauma. PTSD Research Quarterly (2021) 32. p. 1–9.
12. Cerdeña JP, Plaisime MV, Tsai J. From race-based to race-conscious medicine: how anti-racist uprisings call us to act. Lancet. (2020) 396:1125–8. doi: 10.1016/S0140-6736(20)32076-6
13. Buchanan NT, Perez M, Prinstein MJ, Thurston IB. Upending racism in psychological science: Strategies to change how science is conducted, reported, reviewed, and disseminated. Am Psychol. [In Press]
14. Williams MT, Reed S, George J. Culture and psychedelic psychotherapy: ethnic and racial themes from three black women therapists. J Psychedelic Stud. (2020) 4:125–38. doi: 10.1556/2054.2020.00137
15. Strauss D, de la Salle S, Sloshower J, Williams MT. Research abuses against people of colour and other vulnerable groups in early psychedelic research. J Med Ethics. (2021). doi: 10.1136/medethics-2021-107262. [Epub ahead of print].
16. Solomon R. Racism and its effect on cannabis research. Cannabis Cannabinoid Res. (2020) 5:2–5. doi: 10.1089/can.2019.0063
18. Agar M. The story of crack: towards a theory of illicit drug trends. Addict Res Theory. (2003) 11:3–29. doi: 10.1080/1606635021000059042
19. Hunt G, Kolind T, Antin T. Conceptualizing ethnicity in alcohol and drug research: Epidemiology meets social theory. J Ethn Subst Abuse. (2018) 17:187–98. doi: 10.1080/15332640.2017.1316223
20. McCabe SE, Morales M, Cranford JA, Delva J, McPherson MD, Boyd CJ. Race/ethnicity and gender differences in drug use and abuse among college students. J Ethn Subst Abuse. (2007) 6:75–95. doi: 10.1300/J233v06n02_06
21. Beckett K, Nyrop K, Pfingst L. Race, drugs, and policing: understanding disparities in drug delivery arrests. Criminology. (2006) 44:105–37. doi: 10.1111/j.1745-9125.2006.00044.x
22. Lassiter MD. Impossible criminals: the suburban imperatives of America's war on drugs. J Am History. (2015) 102:126–140. doi: 10.1093/jahist/jav243
23. DeSilver D, Lipka M, Fahmy D. 10 Things We Know About Race And Policing In The U.S. Pew Research. Available online at: https://www.pewresearch.org/fact-tank/2020/06/03/10-things-we-know-about-race-and-policing-in-the-u-s/ (accessed June 3, 2020).
24. Williams MT, Osman M, Gran-Ruaz S, Lopez J. Intersection of racism and PTSD: assessment and treatment of racism-related stress and trauma. Curr Treat Options Psychiatry. (2021) 8:1–19. doi: 10.1007/s40501-021-00250-2
25. Lavalley R, Johnson KR. Occupation, injustice, and anti-black racism in the United States of America. J Occu Sci. (2020) 1–13. doi: 10.1080/14427591.2020.1810111
26. American Psychological Association. How many psychology doctorates are awarded by U. S. Institutions? Monitor Psychol. (2014) 45:13. Available online at: http://www.apa.org/monitor/2014/07-08/datapoint
27. Himle JA, Baser RE, Taylor RJ, Campbell RD, Jackson JS. Anxiety disorders among African Americans, blacks of Caribbean descent, and non-Hispanic whites in the United States. J Anxiety Disord. (2009) 23:578–90. doi: 10.1016/j.janxdis.2009.01.002
28. Williams DR. Stress and the mental health of populations of color: advancing our understanding of race-related stressors. J Health Soc Behav. (2018) 59:466–85. doi: 10.1177/0022146518814251
29. Carter L, Davila C. Is it because I'm Black? Microaggressive experiences against Black professionals in sport and exercise psychology. Prof Psychol. (2017) 48:287. doi: 10.1037/pro0000145
30. Sue DW, Capodilupo CM, Torino GC, Bucceri JM, Holder AMB, Nadal KL, et al. Racial microaggressions in everyday life: implications for clinical practice. Am Psychol. (2007) 62:271–86. doi: 10.1037/0003-066X.62.4.271
31. DeAngelis T. Unmasking ‘Racial Microaggressions'. Monitor. American Psychological Association (2009). Available online at: https://www.apa.org/monitor/2009/02/microaggression
32. Williams MT. Managing Microaggressions: Addressing Everyday Racism in Therapeutic Spaces. New York, NY: Oxford University Press (2020). doi: 10.1093/med-psych/9780190875237.001.0001
33. Anders SL, Frazier PA, Frankfurt SB. Variations in criterion A and PTSD rates in a community sample of women. J Anxiety Disord. (2011) 25:176–84. doi: 10.1016/j.janxdis.2010.08.018
34. Lansing AE, Plante WY, Beck AN. Assessing stress-related treatment needs among girls at risk for poor functional outcomes: the impact of cumulative adversity, criterion traumas, and non-criterion events. J Anxiety Disord. (2017) 48:36–44. doi: 10.1016/j.janxdis.2016.09.007
35. Roberts AL, Dohrenwend BP, Aiello AE, Wright RJ, Maercker A, Galea S, et al. The stressor criterion for posttraumatic stress disorder: does it matter? J Clin Psychiatry. (2012) 73:e264–70. doi: 10.4088/JCP.11m07054
36. Loo CM, Fairbank JA, Scurfield RM, Ruch LO, King DW, Adams LJ, et al. Measuring exposure to racism: development and validation of a race-related stressor scale (RRSS) for Asian American Vietnam veterans. Psychol Assess. (2001) 13:503–20. doi: 10.1037/1040-3590.13.4.503
37. Bor J, Venkataramani AS, Williams DR, Tsai A. Police killings and their spillover effects on the mental health of black Americans: a population-based, quasi experimental study. Lancet. (2018) 392:302–10. doi: 10.1016/S0140-6736(18)31130-9
38. Sewell AA. Policing the block: pandemics, systemic racism, and the blood of America. City Community. (2020) 19:496–505. doi: 10.1111/cico.12517
39. Staggers-Hakim R. The nation's unprotected children and the ghost of mike brown, or the impact of national police killings on the health and social development of African American boys. J Hum Behav Soc Environ. (2016) 26:390–9. doi: 10.1080/10911359.2015.1132864
40. Camp NP, Voigt R, Jurafsky D, Eberhardt JL. The thin blue waveform: racial disparities in officer prosody undermine institutional trust in the police. J Pers Soc Psychol. (2021). doi: 10.1037/pspa0000270
41. Pierce C. Offensive mechanisms. In: Barbour F, Editors. The Black Seventies. Boston, MA: Porter Sargent (1970). p. 265–82.
42. Williams MT, Printz D, Ching T, Wetterneck CT. Assessing PTSD in ethnic and racial minorities: Trauma and racial trauma. Direct Psychi. (2018). 38:179–96.
43. Williams MT, Malcoun E, Sawyer BA, Davis DM, Nouri LB, Bruce SL. Cultural adaptations of prolonged exposure therapy for treatment and prevention of posttraumatic stress disorder in African Americans. Behav Sci. (2014) 4:102–24. doi: 10.3390/bs4020102
44. Comas-Díaz L, Hall GN, Neville HA. Racial trauma: theory, research, and healing: introduction to the special issue. Am Psychologist. (2019) 74:1. doi: 10.1037/amp0000442
45. Smith DT. The epigenetics of being black and feeling blue: understanding African American vulnerability to disease. In: Gause CP, Theodore Ranshaw RM, Editors. The Handbook of Research on Black Males: Quantitative, Qualitative and Multidisciplinary. Michigan State University Press (2019). p. 259–66. doi: 10.14321/j.ctv4g1qgh.25
46. Adam EK, Quinn ME, Tavernier R, McQuillan MT, Dahlke KA, Gilbert KE. Diurnal cortisol slopes and mental and physical health outcomes: a systematic review and meta-analysis. Psychoneuroendocrinology. (2017) 83:25–41. doi: 10.1016/j.psyneuen.2017.05.018
47. Vieweg WVR, Julius DA, Fernandez A, Beatty-Brooks M, Hettema JM, Pandurangi AK. Posttraumatic stress disorder: clinical features, pathophysiology, and treatment. Am J Med. (2006) 119:383–90. doi: 10.1016/j.amjmed.2005.09.027
48. Sijbrandij M, Engelhard IM, Lommen MJ, Leer A, Baas JM. Impaired fear inhibition learning predicts the persistence of symptoms of posttraumatic stress disorder (PTSD). J Psychiatr Res. (2013) 47:1991–7. doi: 10.1016/j.jpsychires.2013.09.008
49. Davis MT, Holmes SE, Pietrzak RH, Esterlis I. Neurobiology of chronic stress-related psychiatric disorders: evidence from molecular imaging studies. Chronic Stress. (2017) 1:2470547017710916. doi: 10.1177/2470547017710916
50. Rosso IM, Weiner MR, Crowley DJ, Silveri MM, Rauch SL, Jensen JE. Insula and anterior cingulate GABA levels in posttraumatic stress disorder: preliminary findings using magnetic resonance spectroscopy. Depress Anxiety. (2014) 31:115–23. doi: 10.1002/da.22155
51. Wolf EJ, Mitchell KS, Logue MW, Baldwin CT, Reardon AF, Aiello A, et al. The dopamine D3 receptor gene and posttraumatic stress disorder. J Trauma Stress. (2014) 27:379–87. doi: 10.1002/jts.21937
52. Adam EK, Heissel JA, Zeiders KH, Richeson JA, Ross EC, Ehrlich KB, et al. Developmental histories of perceived racial discrimination and diurnal cortisol profiles in adulthood: a 20-year prospective study. Psychoneuroendocrinology. (2015) 62:279–91. doi: 10.1016/j.psyneuen.2015.08.018
53. Campbell J, Ehlert U. Acute psychosocial stress: does the emotional stress response correspond with physiological responses?. Psychoneuroendocrinology. (2012) 37:1111–34. doi: 10.1016/j.psyneuen.2011.12.010
54. Gouin JP, Hantsoo L, Kiecolt-Glaser JK. Immune dysregulation and chronic stress among older adults: a review. Neuroimmunomodulation. (2008) 15:251–9. doi: 10.1159/000156468
55. Duman RS, Sanacora G, Krystal JH. Altered connectivity in depression: GABA and glutamate neurotransmitter deficits and reversal by novel treatments. Neuron. (2019) 102:75–90. doi: 10.1016/j.neuron.2019.03.013
56. Conrad CD, Ortiz JB, Judd JM. Chronic stress and hippocampal dendritic complexity: methodological and functional considerations. Physiol Behav. (2017) 178:66–81. doi: 10.1016/j.physbeh.2016.11.017
57. Hammond DC. What is neurofeedback: an update. J Neurother. (2011) 15:305–36. doi: 10.1080/10874208.2011.623090
58. Williams L. ‘Integrative neuroscience' and psychiatry: identifying cognitive, affective and brainwave markers of psychiatric disorder. Acta Neuropsychiatr. (2006) 18:338–338. doi: 10.1017/S0924270800032452
59. Bell AN, Moss D, Kallmeyer RJ. Healing the neurophysiological roots of trauma: a controlled study examining LORETA z-score neurofeedback and HRV biofeedback for chronic PTSD. NeuroRegulation. (2019) 6:54–54. doi: 10.15540/nr.6.2.54
60. Kahana MJ. The cognitive correlates of human brain oscillations. J Neurosci. (2006) 26:1669–72. doi: 10.1523/JNEUROSCI.3737-05c.2006
61. Ros T, Baars JB, Lanius RA, Vuilleumier P. Tuning pathological brain oscillations with neurofeedback: a systems neuroscience framework. Front Human Neurosci. (2014) 8:1008. doi: 10.3389/fnhum.2014.01008
62. Bluhm RL, Williamson PC, Osuch EA, Frewen PA, Stevens TK, Boksman K, et al. Alterations in default network connectivity in posttraumatic stress disorder related to early-life trauma. J Psychiatry Neurosci. (2009) 34:187–94.
63. Carter RT. Racism and psychological and emotional injury: recognizing and assessing race-based traumatic stress. Couns Psychol. (2007) 35:13–105. doi: 10.1177/0011000006292033
64. Williams MT, Kanter JW, Ching TH. Anxiety, stress, and trauma symptoms in African Americans: Negative affectivity does not explain the relationship between microaggressions and psychopathology. J Racial Ethn Health Disparities. (2018) 5:919–27. doi: 10.1007/s40615-017-0440-3
65. Parnas J, Bovet P. Psychiatry made easy: operation (al) ism and some of its consequences. in Proceedings of Philosophical issues in psychiatry III: The nature and sources of historical change. (2015). p. 190–212. doi: 10.1093/med/9780198725978.003.0023
66. Gara MA, Minsky S, Silverstein SM, Miskimen T, Strakowski SM. A naturalistic study of racial disparities in diagnoses at an outpatient behavioral health clinic. Psychiatr serv. (2019) 70:130–4. doi: 10.1176/appi.ps.201800223
67. Neighbors HW, Trierweiler SJ, Ford BC, Muroff JR. Racial differences in DSM diagnosis using a semi-structured instrument: The importance of clinical judgment in the diagnosis of African Americans. J Health Soc Behav. (2003) 237–56. doi: 10.2307/1519777
68. Berger M, Sarnyai Z. More than skin deep: Stress neurobiology and mental health consequences of racial discrimination. Stress. (2015) 18:1–10. doi: 10.3109/10253890.2014.989204
69. Smith DT. Is Psychedelic Medicine the Antidote to Anti-black Racism in the US? Available online at: https://chacruna.net/psychedelic_medicine_treating_ptsd_racism/ (accessed January 18, 2021).
70. Mithoefer MC, Wagner MT, Mithoefer AT, Jerome L, Martin SF, Yazar-Klosinski B, et al. Durability of improvement in post-traumatic stress disorder symptoms and absence of harmful effects or drug dependency after 3, 4-methylenedioxymethamphetamine-assisted psychotherapy: a prospective long-term follow-up study. J Psychopharmacol. (2013) 27:28–39. doi: 10.1177/0269881112456611
71. Ot'alora M, Grigsby J, Poulter B, Van Derveer JW, Giron SG, Jerome L, et al. 3,4-Methylenedioxymethamphetamine-assisted psychotherapy for treatment of chronic posttraumatic stress disorder: a randomized phase 2 controlled trial. J Psychopharmacol. (2018) 32:1295–307. doi: 10.1177/0269881118806297
72. Williams MT, Davis AK, Xin Y, Sepeda ND, Grigas PC, Sinnott S, et al. People of color in North America report improvements in racial trauma and mental health symptoms following psychedelic experiences. Drugs: Educ Prevent Policy. (2021) 28:215–26. doi: 10.1080/09687637.2020.1854688
73. Feduccia AA, Jerome L, Klosinski B, Emerson A, Mithoefer MC, Doblin R. Breakthrough for trauma treatment: safety and efficacy of MDMA-assisted psychotherapy compared to paroxetine and sertraline. Front Psychiatry. (2019) 10:650. doi: 10.3389/fpsyt.2019.00650
74. Reiff CM, Richman EE, Nemeroff CB, Carpenter LL, Widge AS, Rodriguez CI, et al. Psychedelics and psychedelic-assisted psychotherapy. Am J psychiatry. (2020) 177:391–410. doi: 10.1176/appi.ajp.2019.19010035
75. Labate BC, Cavnar C. The Therapeutic Use Of Ayahuasca. Berlin, Heidelberg: Springer (2014). doi: 10.1007/978-3-642-40426-9
76. Halstead M, Reed S, Krause R, Williams MT. Ketamine-assisted psychotherapy for PTSD related to racial discrimination. Clin Case Stud. (2021) 20:310–30. doi: 10.1177/1534650121990894
77. Smith DT. White on black: can white parents teach black adoptive children how to understand and cope with racism? J Black Stud. (2011) 42:1195–230. doi: 10.1177/0021934711404237
78. Smith DT, Juarez BG. Race lessons in black and white: How do white adoptive parents socialize black adoptees in predominantly white communities. Adoption Quarterly. (2014) 18:108–37. doi: 10.1080/10926755.2014.895465
79. Benuto L, Singer J, Newlands RT, Casas JB. Training culturally competent psychologists: where are we and where do we need to go? Train Educ Prof Psychol. (2019) 13:56–63. doi: 10.1037/tep0000214
80. Fuertes JN, Stracuzzi TI, Bennett J, Scheinholtz J, Mislowack A, Hersh M, et al. Therapist multicultural competency: a study of therapy dyads. Psychotherapy. (2006) 43:480–90. doi: 10.1037/0033-3204.43.4.480
81. Cooper LA, Roter DL, Carson KA, Beach MC, Sabin JA, Greenwald AG, et al. The associations of clinicians' implicit attitudes about race with medical visit communication and patient ratings of interpersonal care. Am J Public Health. (2012) 102:979–87. doi: 10.2105/AJPH.2011.300558
82. Sabin JA, Greenwald AG. The influence of implicit bias on treatment recommendations for 4 common pediatric conditions: pain, urinary tract infection, attention deficit hyperactivity disorder, and asthma. Am J Public Health. (2012) 102:988–95. doi: 10.2105/AJPH.2011.300621
83. Williams MT. Adverse racial climates in academia: conceptualization, interventions, and call to action. New Ideas Psychol. (2019) 55:58–67. doi: 10.1016/j.newideapsych.2019.05.002
84. Daumit GL, Crum RM, Guallar E, Powe NR, Primm AB, Steinwachs DM, et al. Outpatient prescriptions for atypical antipsychotics for African Americans, Hispanics, and whites in the United States. Arch Gen Psychiatry. (2003) 60:121. doi: 10.1001/archpsyc.60.2.121
85. Diaz FJ, de Leon J. Excessive antipsychotic dosing in 2 US state hospitals. J Clin Psychiatry. (2002) 63:998–1003. doi: 10.4088/JCP.v63n1107
86. Han E, Liu GG. Racial disparities in prescription drug use for mental illness among population in US. J Ment Health Policy Econ. (2005) 8:131–43.
87. Szarek BL, Goethe JW. Racial differences in use of antipsychotics among patients with bipolar disorder. J Clin Psychiatry. (2003) 64:614–5. doi: 10.4088/JCP.v64n0518g
88. Londono Tobon A, Flores JM, Taylor JH, Johnson I, Landeros-Weisenberger A, Aboiralor O, et al. Racial implicit associations in psychiatric diagnosis, treatment, and compliance expectations. Acad psychiatry. (2021) 45:23–33. doi: 10.1007/s40596-020-01370-2
89. Kuno E, Rothbard AB. Racial disparities in antipsychotic prescription patterns for patients with schizophrenia. Am J Psychiatry. (2002) 159:567–72. doi: 10.1176/appi.ajp.159.4.567
90. Sleath B, Svarstad B, Roter D. Patient race and psychotropic prescribing during medical encounters. Patient Educ Couns. (1998) 34:227–38. doi: 10.1016/S0738-3991(98)00030-5
91. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci U S A. (2016) 113:4296–301. doi: 10.1073/pnas.1516047113
92. Morden NE, Chyn D, Wood A, Meara E. Racial inequality in prescription opioid receipt—role of individual health systems. N Eng J Med. (2021) 385:342–51. doi: 10.1056/NEJMsa2034159
93. Bareis N, Olfson M, Wall M, Stroup TS. Variation in psychotropic medication prescription for adults with schizophrenia in the United States. Psychiatr Serv. (2021) 1–19. doi: 10.1176/appi.ps.202000932. [Epub ahead of print].
94. Bernardy NC, Lund BC, Alexander B, Jenkyn AB, Schnurr PP, Friedman MJ. Gender differences in prescribing among veterans diagnosed with posttraumatic stress disorder. J Gen Intern Med. (2013) 28:S542–48.
95. Gross GM, Smith N, Holliday R, Rozek DC, Hoff R, Harpaz-Rotem I. Racial disparities in clinical outcomes of veterans affairs residential PTSD treatment between black and white veterans. Psychiatr Serv. (2021) 31:1–12. doi: 10.1176/appi.ps.202000783
96. Spoont MR, Nelson DB, Murdoch M, Sayer NA, Nugent S, Rector T, et al. Are there racial/ethnic disparities in VA PTSD treatment retention?. Depress Anxiety. (2015) 32:415–25. doi: 10.1002/da.22295
97. Redd AM, Gundlapalli AV, Suo Y, Pettey W, Brignone E, Chin DL, et al. Exploring disparities in awarding VA service-connected disability for post-traumatic stress disorder for active duty military service members from recent conflicts in Iraq and Afghanistan. Mil Med. (2020) 185:296–302. doi: 10.1093/milmed/usz208
98. Carlson MD, Endsley M, Motley D, Shawahin LN, Williams MT. Addressing the impact of racism on veterans of color: A race-based stress and trauma intervention. Psychol Violence. (2018) 8:748–62. doi: 10.1037/vio0000221
99. Belouin SJ, Henningfield JE. Psychedelics: where we are now, why we got here, what we must do. Neuropharmacology. (2018) 142:7–19. doi: 10.1016/j.neuropharm.2018.02.018
100. Milloy C. Black Psychiatrists are Few. They've Never Been More Needed. The Washington Post. Available online at: https://www.washingtonpost.com/local/black-psychiatrists-are-few-theyve-never-been-more-needed/2020/08/11/7df9eeea-dbeb-11ea-8051-d5f887d73381_story.html (accessed August 11, 2020).
101. American Psychological Association. Guidelines on Multicultural Education, Training, Research, Practice, Organizational Change for Psychologists. (2002). Available online at: https://www.apa.org/about/policy/multicultural-guidelines-archived.pdf
102. Jahn ZW, Lopez J, de la Salle S, Faber S, Williams MT. Racial/Ethnic differences in prevalence for hallucinogen use by age cohort: Findings from the 2018 National Survey on Drug Use and Health. J Psychedelic Stud. (2021) 5:69–82. doi: 10.1556/2054.2021.00166
103. Alexander M. The New Jim Crow: Mass Incarceration In The Age Of Colorblindness. The New Press (2010).
104. Williams MT. Why Black people should embrace psychedelic healing. In: Labate B, Cavnar C, Editors, Psychedelic Justice: Toward a Diverse and Equitable Psychedelic Culture Synergetic Press (2021). p. 3–7. Available online at: https://chacruna.net/why-black-people-should-embrace-psychedelic-healingreclaiming-our-cultural-birthright/
105. Bogenschutz MP, Forcehimes AA. Development of a psychotherapeutic model for psilocybin-assisted treatment of alcoholism. J Humanist Psychol. (2016) 57:389–414. doi: 10.1177/0022167816673493
106. Nielson EM, Guss J. The influence of therapists' first-hand experience with psychedelics on psychedelic-assisted psychotherapy research and therapist training. J Psychedelic Stud. (2018) 2:64–73. doi: 10.1556/2054.2018.009
107. Ching THW. Intersectional insights from an MDMA-assisted psychotherapy training trial: An open letter to racial/ethnic and sexual/gender minorities. J Psychedelic Stud. (2019) 4:61–8. doi: 10.1556/2054.2019.017
108. Ching TH. Intersectional insights from an MDMA-assisted psychotherapy training trial: an open letter to racial/ethnic and sexual/gender minorities. J Psychedelic Stud. (2020) 4:61–8.
109. Buchanan NT. Ensuring the psychedelic renaissance and radical healing reach the Black community: Commentary on Culture and Psychedelic Psychotherapy. J Psychedelic Stud. (2021) 4:142–5. doi: 10.1556/2054.2020.00145
110. Buchanan NT, Rios D, Case KA. Intersectional cultural humility: critical inquiry and praxis in psychology. Women Ther. (2020) 34:235–43. doi: 10.1080/02703149.2020.1729469
111. Buchanan NT, Wiklund LO. Intersectionality research in psychological science: resisting the tendency to disconnect, dilute, and depoliticize. Res Child Adolesc Psychopathol. (2021) 49:25–31. doi: 10.1007/s10802-020-00748-y
112. Buchanan NT, Wiklund LO. Why clinical science must change or die: Integrating intersectionality and social justice. Women Ther. (2020) 34:309–29. doi: 10.1080/02703149.2020.1729470
113. Neitzke-Spruill L. Race as a component of set and setting: How experiences of race can influence psychedelic experiences. J Psychedelic Stud. (2020) 4:51–60. doi: 10.1556/2054.2019.022
114. Harjunen VJ, Sjö P, Ahmed I, Saarinen A, Farmer H, Salminen M, et al. Increasing self-other similarity modulates ethnic bias in sensorimotor resonance to others' pain. Soc Cogn Affect Neurosci. (2021) nsab113:1–10. doi: 10.1093/scan/nsab113 [Epub ahead of print].
115. Mathur VA, Richeson JA, Paice JA, Muzyka M, Chiao JY. Racial bias in pain perception and response: experimental examination of automatic and deliberate processes. J Pain. (2014) 15:476–84. doi: 10.1016/j.jpain.2014.01.488
116. Azevedo RT, Macaluso E, Avenanti A, Santangelo V, Cazzato V, Aglioti SM. Their pain is not our pain: brain and autonomic correlates of empathic resonance with the pain of same and different race individuals. Hum Brain Mapp. (2013) 34:3168–81. doi: 10.1002/hbm.22133
117. Balliet D, Wu J, De Dreu CKW. Ingroup favoritism in cooperation: a meta-analysis. Psychol Bull. (2014) 140:1556–81. doi: 10.1037/a0037737
118. Berlingeri M, Gallucci M, Danelli L, Forgiarini M, Sberna M, Paulesu E. Guess who's coming to dinner: brain signatures of racially biased and politically correct behaviors. Neuroscience. (2016) 332:231–41. doi: 10.1016/j.neuroscience.2016.06.048
119. Zhou Y, Han S. Neural dynamics of pain expression processing: alpha-band synchronization to same-race pain but desynchronization to other-race pain. Neuroimage. (2021) 224:117400.
120. Malott KM, Schaefle S. Addressing clients' experiences of racism: a model for clinical practice. J Couns Dev. (2015) 93:361–9. doi: 10.1002/jcad.12034
121. Thrul J, Garcia-Romeu A. Whitewashing psychedelics: racial equity in the emerging field of psychedelic-assisted mental health research and treatment. Drugs Edu Prev Policy. (2021) 28:211–4. doi: 10.1080/09687637.2021.1897331
122. Carlin S. MDMA therapy training for communities of color. MAPS Bulletin. MAPS Bulletin Spring. (2020) 30. Available online at:https://maps.org/news/bulletin/articles/444-bulletinsummer-2020/8308-mdma-therapy-training-for-communities-of-color
123. Lekhtman A. The First-Ever MDMA Therapy Training For Communities Of Color Was Vital. (2019). Filter Magazine, Available online at: https://filtermagorg/mdma-therapy-peoplecolor/ (accessed August 22, 2019).
124. Williams MT, Labate B. Diversity, equity, and access in psychedelic medicine. J Psychedelic Stud. (2020) 4:1–3. doi: 10.1556/2054.2019.032
125. Sue DW, Torino GC, Capodilupo CM, Rivera DP, Lin AI. How white faculty perceive and react to difficult dialogues on race: implications for education and training. Couns Psychol. (2009) 37:1090–115. doi: 10.1177/0011000009340443
127. Gayles JG, Kelly BT, Grays S, Zhang JJ, Porter KP. Faculty teaching diversity through difficult dialogues: stories of challenges and success. J Stud Aff Res Pract. (2015) 52:300–12. doi: 10.1080/19496591.2015.1067223
128. Williams MT, Kanter JW, Peña A, Ching THW, Oshin L. Reducing microaggressions and promoting interracial connection: the racial harmony workshop. J Context Behav Sci. (2020) 16:153–61. doi: 10.1016/j.jcbs.2020.04.008
129. DiAngelo R. White fragility: Why It's So Hard For White People To Talk About Racism. Boston, MA: Beacon Press (2018).
130. Plant EA, Devine PG. The antecedents and implications of interracial anxiety. Pers Soc Psychol Bull. (2003) 29:790–801. doi: 10.1177/0146167203029006011
131. Lin L, Stamm K, Christidis P. Demographics of the U.S. psychology workforce: findings from the 2007-16 American Community Survey: (506742018-001) [Data set]. Am Psychol Assoc. (2018) 1–20. doi: 10.1037/e506742018-001
132. Williams MT. Unicorns, leprechauns, and White allies: Exploring the space between intent and action. The Behavior Therapist. (2021) 44:272–81.
133. Williams MT, Faber S, Nepton A, Ching TH. Racial justice allyship requires civil courage: a behavioral prescription for moral growth and change. Am Psychol. (2021).
134. Haeny AH, Holmes SC, Williams MT. Applying anti-racism to clinical care and research. JAMA Psychiatry. (2021) 78:1187–8. doi: 10.1001/jamapsychiatry.2021.2329
135. Labate BC, Cavnar C. Psychedelic Justice: Toward a Diverse and Equitable Psychedelic Culture. Santa Fe, NM: Synergetic Press (2021).
136. Larson KE, Bradshaw CP. Cultural competence and social desirability among practitioners: a systematic review of the literature. Child Youth Serv Rev. (2017) 76:100–11. doi: 10.1016/j.childyouth.2017.02.034
137. Stewart CE, Lee SY, Hogstrom A, Williams M. Diversify and conquer: a call to promote minority representation in clinical psychology. Behav Therapist. (2017) 40:74–9. doi: 10.1146/annurev.psych.60.110707.163651
138. Williams MT, La Torre J. Clinical supervision in delivery of CBT across race, ethnicity, and culture. In: Storch E, Abramowitz J, McKay D, Editors. Training and Supervision in Specialized Cognitive-Behavior Therapy: Methods, Settings, and Populations. American Psychological Association Press (2000).
139. Majors R. Black Mental Health and the New Millennium: Historical and Current Perspective on Cultural Trauma and ‘Everyday'Racism in White Mental Health Spaces—The Impact on the Psychological Well-being of Black Mental Health Professionals. In The International Handbook of Black Community Mental Health. Emerald Publishing Limited. (2020) 1–26. doi: 10.1108/978-1-83909-964-920201002
Keywords: African Americans, Black Americans, Black Canadian, racial trauma, race-based harassment and discrimination, psychedelic research, psychedelic-assisted therapy
Citation: Smith DT, Faber SC, Buchanan NT, Foster D and Green L (2022) The Need for Psychedelic-Assisted Therapy in the Black Community and the Burdens of Its Provision. Front. Psychiatry 12:774736. doi: 10.3389/fpsyt.2021.774736
Received: 12 September 2021; Accepted: 14 December 2021;
Published: 20 January 2022.
Edited by:
Antonio Metastasio, Camden and Islington NHS Foundation Trust, United KingdomReviewed by:
Gregory Fonzo, The University of Texas at Austin, United StatesCopyright © 2022 Smith, Faber, Buchanan, Foster and Green. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Darron T. Smith, ZHNtaXRoNDdAbWVtcGhpcy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.