
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 09 February 2022
Sec. Child and Adolescent Psychiatry
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.768206
This article is part of the Research Topic Rising Stars in Child and Adolescent Psychiatry View all 5 articles
 Frederick Russet1*†
Frederick Russet1*† Veronique Humbertclaude1†Nikolina Davidovic Vrljicak2
Veronique Humbertclaude1†Nikolina Davidovic Vrljicak2 Gwen C. Dieleman3Katarina Dodig-Ćurković4
Gwen C. Dieleman3Katarina Dodig-Ćurković4 Tomislav Franic2Suzanne E. Gerritsen3
Tomislav Franic2Suzanne E. Gerritsen3 Giovanni de Girolamo5Gaelle Hendrickx6Hala Kerbage1,7Fiona McNicholas8Athanasios Maras9,10
Giovanni de Girolamo5Gaelle Hendrickx6Hala Kerbage1,7Fiona McNicholas8Athanasios Maras9,10 Santosh Paramala11,12,13Moli Paul14,15
Santosh Paramala11,12,13Moli Paul14,15 Aurélie Schandrin16Ulrike M. E. Schulze17Cathy Street14Helena Tuomainen14
Aurélie Schandrin16Ulrike M. E. Schulze17Cathy Street14Helena Tuomainen14 Dieter Wolke14
Dieter Wolke14 Swaran P. Singh14Sabine Tremmery6,18‡
Swaran P. Singh14Sabine Tremmery6,18‡ Diane Purper-Ouakil1,7‡ for the Milestone Consortium
Diane Purper-Ouakil1,7‡ for the Milestone ConsortiumBackground: In mental health, transition refers to the pathway of young people from child and adolescent to adult services. Training of mental health psychiatrists on transition-related topics offers the opportunity to improve clinical practice and experiences of young people reaching the upper age limit of child and adolescent care.
Methods: National psychiatrist's organizations or experts from 21 European countries were surveyed 1/ to describe the status of transition in adult psychiatry (AP) and child and adolescent psychiatry (CAP) postgraduate training in Europe; 2/ to explore the amount of cross-training between both specialties. This survey was a part of the MILESTONE project aiming to study and improve the transition process of young people at the service boundary.
Results: Transition was a mandatory topic in the AP curriculum of 1/19 countries (5%) and in the CAP curriculum of 4/17 countries (24%). Most topics relevant for transition planning were addressed during AP training in 7/17 countries (41%) to 10/17 countries (59%), and during CAP training in 9/11 countries (82%) to 13/13 countries (100%). Depending on the training models, theoretical education in CAP was mandatory during AP training in 94% (15/16) to 100% of the countries (3/3); and in AP during CAP training in 81% (13/16) to 100% of the countries (3/3). Placements were mandatory in CAP during AP training in 67% (2/3) to 71% of the countries (12/17); and in AP during CAP training in 87% (13/15) to 100% of the countries (3/3).
Discussion and Conclusion: Specific training about transition is limited during CAP and AP postgraduate training in Europe. Cross-training between both specialties offers a basis for improved communication between child and adult services but efforts should be sustained in practical training. Recommendations are provided to foster further development and meet the specific needs of young people transitioning to adult services.
In mental health care, transition refers to the pathway of a young person from a child and adolescent mental health service (CAMHS) to an adult mental health service (AMHS). This health services transition occurs at a particularly vulnerable developmental stage, when young people are also simultaneously going through social, family and academic life transitions (1, 2). Discontinuity of care may therefore have harmful consequences for those with ongoing mental health needs in various life domains (3). Unfortunately, only a minority experience good transitional care (4, 5), mostly because of a limited co-ordination between services and the lack of effective evidence-based interventions in transitional care (6, 7). Health services and policy makers from countries around the world are increasingly recognizing the importance of improving transitions from CAMHS to AMHS and developing effective interventions and models of care that are youth-informed and oriented (6, 8, 9). The European Union of Medical Specialists-Child and Adolescent Psychiatry (UEMS-CAP) is currently working on European guidelines for Transitional care (see www.uemscap.eu/working-group).
An optimal transition involves a coordinated, purposeful, planned and patient-centered process, ideally involving a period of parallel care/joint work between services, to ensure a smooth transition (5, 10, 11). Previous qualitative research showed that young people transitioning between services perceive the consistency of clinicians and periods of parallel care as being among key factors enabling effective CAMHS to AMHS transition (12, 13). This highlights the importance of having clinicians in both services trained in navigating the various aspects of transitional care.
Training of mental health professionals on transition-related topics could therefore facilitate the process at the clinical level and improve clinical practice. Among existing studies on psychiatry training across Europe (14–22), only one focused on transitional care and revealed that, according to trainees, practical and theoretical training on this topic occurred, respectively, in only 27.8 and 16.7% of European countries (21). A systematic review of psychiatrist's training in Europe highlighted that a training specifically dedicated to transition was included only in the United Kingdom (UK) and in Ireland (23). The existing literature points toward gaps in teaching about the process and planning of transition, calling for proper training in “transition psychiatry” in the postgraduate curriculum (24).
Improving knowledge about clinical presentations of mental disorders in adolescence and specific communication skills are other possible areas of training. Some mental health professionals may not feel comfortable or lack the expertise and interviewing techniques needed to work with young people and their families (25–28). Only 17% of Adult Psychiatry (AP) trainees and 35% of General Psychiatry trainees have lectures on adolescent psychopathology, vs. 61% of Child and Adolescent Psychiatry (CAP) trainees (21).
Furthermore, the transition literature shows clinical and conceptual differences between child and adult mental health service models that may lead to mutual misperceptions (4, 29) and may impede the coordination and collaborative working between services that is needed. Training content and training models may account for the cultural divide existing between CAMHS and AMHS, characterized by different beliefs and attitudes, a lack of understanding of different service structures and different working practices related to communication and information transfer (27). In Europe, trainees in AP and CAP follow a separate specialized training from the start of postgraduate studies in 55% countries (21), but there are no studies on the impact of training models on transitional care.
One of the aims of the “MILESTONE project,” a EU-funded research programme exploring the transition of young people from CAMHS to AMHS in eight countries (www.milestone-transitionstudy.eu/) (30), is to study the training of professionals in transitional care. This survey has been designed in the context of the MILESTONE project to describe the current status of transition and related issues in AP and CAP postgraduate training in Europe. It also examines the respective content of AP and CAP postgraduate training, with a particular focus on the amount of theoretical and practical cross training between both specialties (e.g., training in CAP in the AP or General Psychiatry curriculum, and vice-versa).
Data collection was carried out between 2015 and 2018. This research did not require ethical approval as no personal data were collected.
For this study, we used a 114-item questionnaire covering topics identified through a systematic review of the literature (23) and through the recommendations of the European Union of Medical Specialists (UEMS) and UEMS-CAP (31–35) (see Supplementary Material 1 for a synthesis). We verified the relevance and clarity of questions by sharing the questionnaire with members of the MILESTONE consortium. In the final version of the questionnaire (Supplementary Material 2), section 1 covered general aspects of psychiatry postgraduate training; section 2 focused on training in AP and section 3 focused on training in CAP. Specific questions addressed transition and related issues such as the developmental course of childhood disorders, adolescence-onset disorders and therapeutic issues (36).
All respondents to the survey were asked if arrangements in their country were likely to change soon. Those indicating this might be the case were recontacted at the end of the data collection period to check on any recent developments. In case of discrepancies between former and new information provided by the respondent, only the more recent one was included in the analysis.
Participant recruitment was based on purposeful sampling constructed to specifically target key informants. The relevant lead of each national psychiatrist's association from 39 European countries were contacted by the research team: Albania, Austria, Belgium, Bosnia, Bulgaria, Czech Republic, Cyprus, Croatia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Iceland, Italy, Latvia, Lithuania, Luxembourg, Malta, Moldavia, Montenegro, Netherlands, Norway, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, Turkey, Ukraine, and the United Kingdom (UK).
When official representatives were not available or declined participation, snowball sampling was used to contact university professors recommended by the national association or known to professionals involved in the MILESTONE Project.
Participants could answer using online or paper versions.
Data analysis is descriptive in nature, with missing data or inconsistent answers excluded by country for the corresponding questions.
We received completed questionnaires for 21/39 countries (54%) (Figure 1). Since the psychiatry postgraduate training in Luxembourg replicated the French model, it was excluded from the analysis. Among respondents, 50% were representatives of national psychiatry associations while 50% were from universities or research institutions engaged in training.

Figure 1. Mapping of the 3 training models.
Eight countries indicated plans to revise their training syllabus. By study completion, updated information was available from four of them, while the change was awaiting approval in one country and had not yet occurred in another one. The remaining two countries did not provide additional information.
Three models of training in CAP and AP training were identified. In the first model, trainees are provided with a general education in psychiatry including a training in both AP and CAP, with optional subspecialities (3/20 countries, 15%, hereafter referred to as generalist countries). In the second model, trainees follow a joint psychiatry core programme, followed by mandatory further specialization (7/20 countries, 35%). In the third model, CAP and AP are considered as independent specialities and trainees are provided with separate training from the start, with different programmes (10/20 countries, 50%). Countries with model 2 or 3 are referred to as countries with specialization route. Figure 1 depicts these three models.
Transition in itself is a mandatory topic in the AP curriculum only in Sweden (Table 1). However, it may be addressed through a related subject in 3/151. (20%) countries, during courses of CAP in the UK and Russia, or while addressing areas of clinical governance, team working, clinical management and care planning in Ireland.
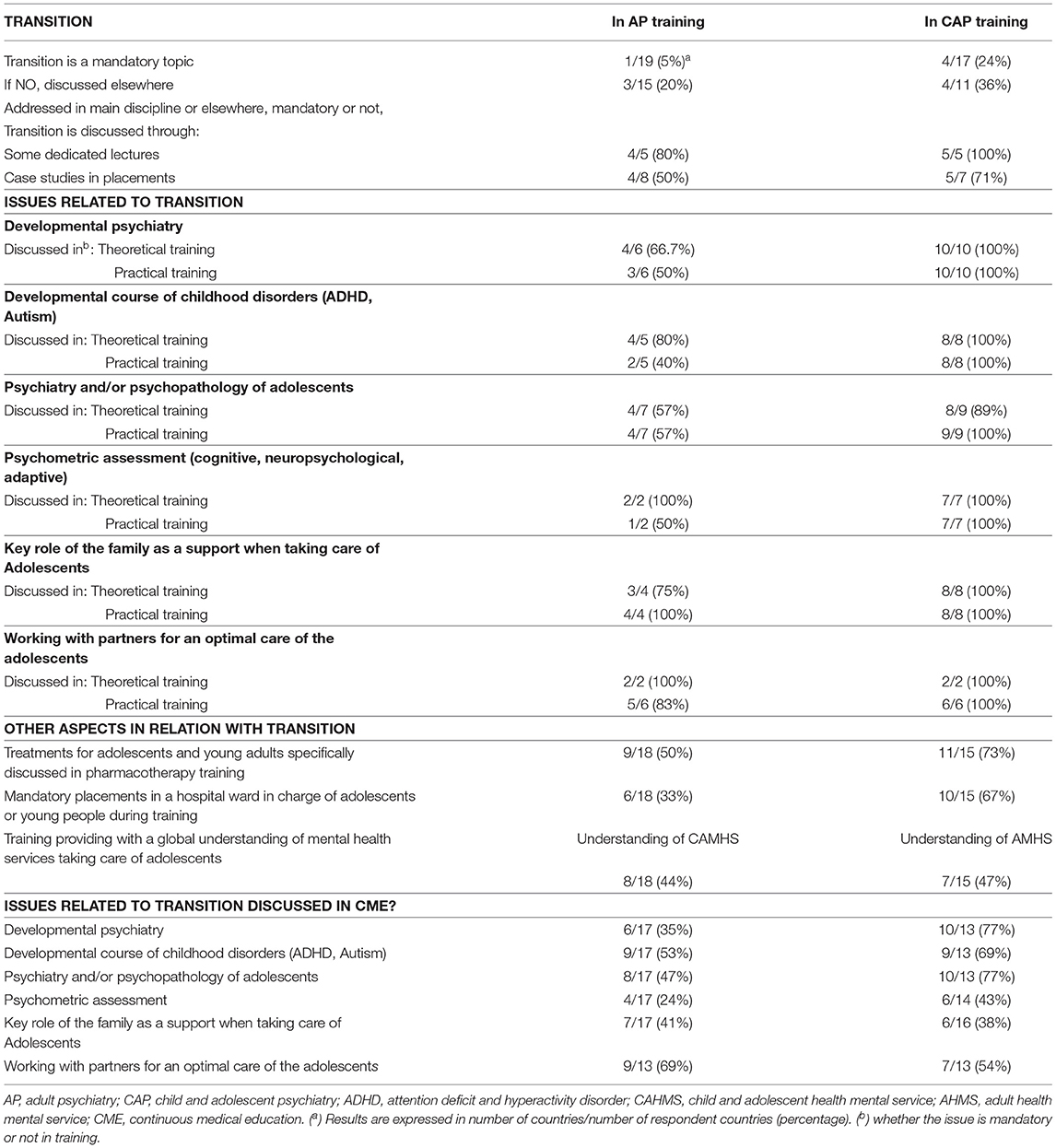
Table 1. Transition and related issues in AP and CAP training and in Continuing Medical Education.
With regard to issues related to transition in the AP curriculum, the most frequently discussed were psychiatry and/or psychopathology of adolescents (10/17 countries, 59%), developmental course of childhood disorders (9/17, 53%), and developmental psychiatry (9/17, 47%), mandatorily discussed in respectively 6/15 responding countries (40%), 3/15 (20%) and 6/16 (38%) (Figure 2). Key role of the family (7/17, 41%), child psychometric assessments (3/17, 18%) or working with professional partners (5/17, 29%) were less often discussed, mandatorily discussed in respectively 2/15 responding countries (13%), 2/17 (12%) and 2/16 (13%). In terms of post-specialization training (Continuous Medical Education), a similar pattern was observed for issues related to transition (Table 1).
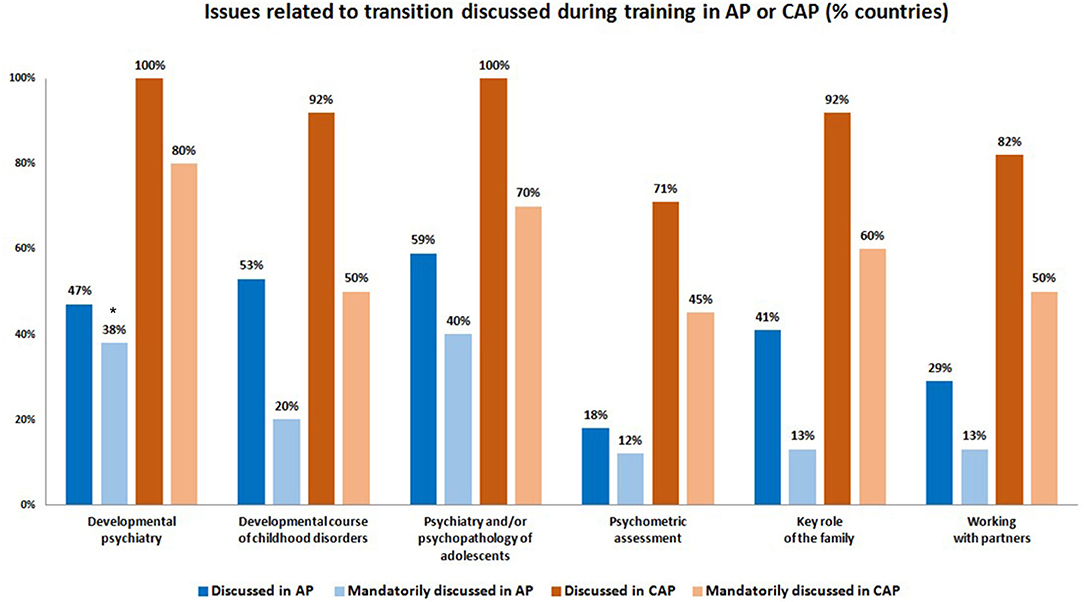
Figure 2. Issues related to transition discussed in AP and CAP training. (*) % mandatory = number of countries answering “yes” if an issue was mandatorily discussed / (number of countries responding to the question about the corresponding issue being discussed or not–number of non-responding countries to the question about the issue being mandatorily discussed or not).
Aspects related to youth and relevant to transitional care were reported to be addressed during AP training by 6/18 (33%) of respondents (e.g., mandatory placements in a hospital ward in charge of adolescents or young people) to 9/18 (50%) of respondents (e.g., treatments for adolescents and young adults specifically discussed in pharmacotherapy training) (Table 1).
Having some theoretical training in CAP along with AP theoretical education was considered mandatory in 18/19 countries (95%), more specifically in 15/16 countries with a specialization in AP (94%) and in 3/3 generalist countries (100%) (Table 2). In countries with a specialization route in AP, the content of CAP theoretical programme was different in AP education and in CAP education in 8/13 countries (62%).
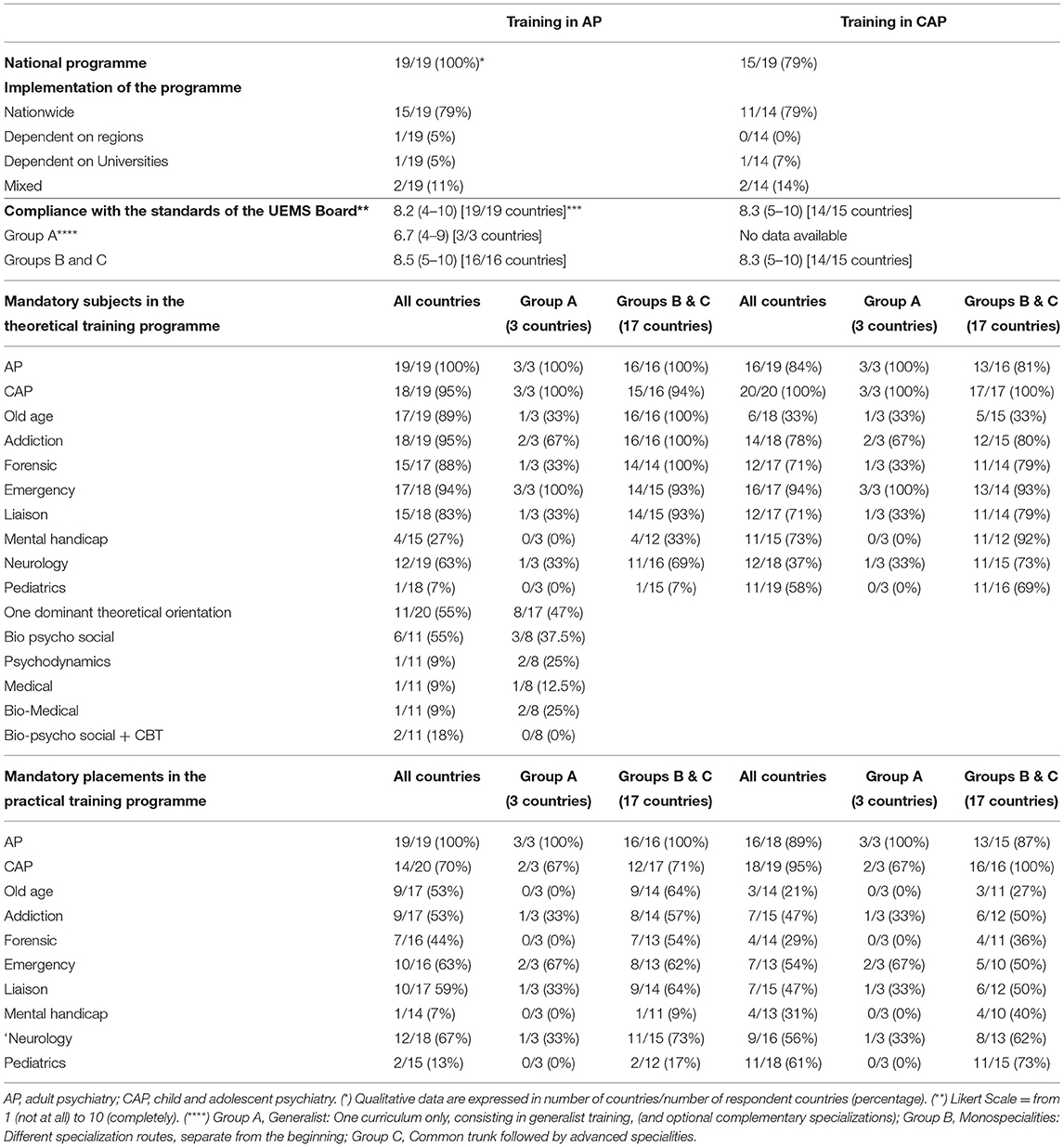
Table 2. Training and specialization in Adult Psychiatry and Child and Adolescent Psychiatry: theoretical and practical content.
In practical training in AP, placements in CAP were mandatory in 14/20 countries (70%), more specifically in 12/17 countries with an AP specialization (71%) and in 2/3 generalist countries (67%) (Table 2). In countries with specialization route in AP, the mean number of mandatory placements in CAP was 1, 3 (10 respondents), for a mean total clinical experience of 5, 2 months (10 respondents). In generalist countries, the mean mandatory number and total duration of placements in CAP were respectively, 2 and 12 months (1 responding country).
The mean level of adherence with UEMS recommendations of the AP programmes was 8.2 (range 4–10), based on a Likert scale ranging from 0 (weak) to 10 (strong) (Table 2).
Table 2 illustrates the similarities and differences of content between AP and CAP theoretical training as regards important topics for transition. Results show considerable variation in terms of whether or not important topics for transition are covered. For example, intellectual disabilities and pediatrics were little addressed in the AP curriculum, respectively in 4/15 countries (27%) and in 1/18 countries (7%). In generalist countries, intellectual disabilities or pediatrics were not listed among the mandatory topics.
Table 3 shows the differences of content between AP and CAP in the theoretical content recommended by the UEMS. During AP training, 16/23 topics were addressed in more than two-third of countries. The least commonly addressed were diversity in psychiatry (in 9/18 countries, 50%), leadership, administration, management, economics (8/16 countries, 50%), psychological tests (10/19 countries, 53%), intellectual disabilities (10/17 countries, 59%).
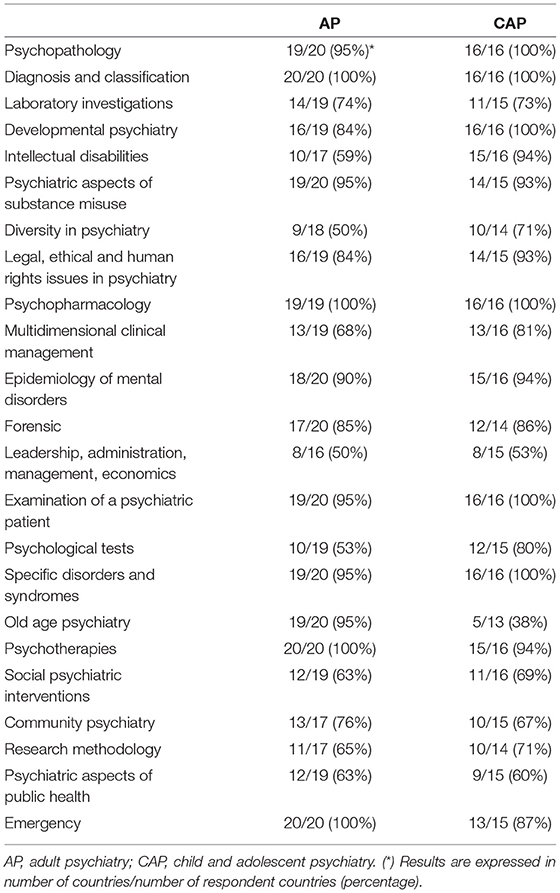
Table 3. Mandatory content of theoretical training in each speciality (according to UEMS recommendations).
As regards the practical training, and the mandatory placements in disciplines other than CAP during AP training (Table 2), five disciplines were mandatory in association with AP training in 9/17 countries (53%) to 14/20 countries (67%). The least frequent placements relevant for transition were forensic (in 7/16 responding countries, 44%), pediatrics (2/15 countries, 13%) and intellectual disabilities (1/14 countries, 7%). We observed the same pattern when countries with a specialization in AP were considered. In generalist countries, placements in emergency care were mandatory in 2/3 countries (67%), whereas placements in addiction services, neurology and liaison were requested in 1/3 countries (33%).
All countries had a national programme regarding AP training, implemented nationwide in 15/19 (79%) countries.
There was a dominant theoretical orientation in AP education in 11/20 countries (55%), mainly bio-psycho-social (55%, 6/11 responding countries) or a combination of bio-psycho-social and cognitive-behavioral (18%, 2/11).
Transition was reported to be a mandatory separate topic in the programme of CAP in 4/17 countries (24%) and was addressed through another subject within the curriculum in 4 of the other 11 responding countries (36%) (Table 1).
As regards the issues related to transition in the CAP curriculum, the most frequently discussed were developmental psychiatry and psychiatry and/or psychopathology of adolescents (both in 13/13 countries, 100%), developmental course of childhood disorders and key role of the family (both in 12/13 countries, 92%), mandatorily discussed in respectively, 8/10 responding countries (80%), 7/10 countries (70%), 5/10 countries (50%) and 6/10 countries (60%) (Figure 2). Psychometric assessment (10/14 countries, 71%) and working with partners (9/11 countries, 82%) were less often discussed and mandatorily discussed in respectively, 5/11 (45%) and 5/10 (50%) responding countries. In Continuous Medical Education, the same pattern was identified, except for developmental course of childhood disorders, who appeared among the most referenced issues.
Aspects related to youth and relevant to transitional care were reported to be addressed during CAP training in 7/15 (47%) of responding countries (e.g., training providing with a global understanding of mental health services taking care of adolescents) to 11/15 of responding countries (73%) (e.g., treatments for adolescents and young adults specifically discussed in pharmacotherapy training) (Table 1).
Having some theoretical training in AP along with CAP theoretical education was mandatory in 16/19 countries (84%), more specifically in 13/16 countries with specialization route in CAP (81%) and in 3/3 (100%) of generalist countries. In countries with a specialization route in CAP, the content of AP theoretical programme was different in AP education and in CAP education in 4/17 (24%) countries.
In CAP practical training, placements in AP were mandatory in 17/19 countries (89%), more specifically in 13/15 (87%) countries with a CAP specialization and in 3/3 generalist countries (100%) (Table 2). In countries with specialization route in CAP, the mean number of mandatory placements in AP was 2,3 (12 respondents), for a mean total clinical experience of 14,6 months (12 respondents). In generalist countries, the mean mandatory number of placements in AP was 3 and mean total duration was 5 months.
The mean level of adherence with UEMS recommendations of the CAP programmes was 8.3 (range 5–10) (Table 2).
Regarding the theoretical content recommended by the UEMS (Table 3), 20/23 topics were addressed during CAP training in more than two-third of countries. Old age, psychiatric aspects of public health and leadership, administration, management, economics were the least addressed, respectively in 5/13 countries (38%), 9/15 countries (60%) and 8/15 countries (53%).
As regards the practical training, and the mandatory placements in disciplines other than AP during CAP training (Table 2), five disciplines were mandatory in association with CAP training in 47% (7/15) to 61% (11/18) of countries. The least frequent placements relevant for transition were intellectual disabilities (mandatory in 4/13 countries, 31%) and forensic (4/14, 29%). We observed the same pattern when countries with a specialization in CAP were considered.
CAP was considered an independent speciality in 15/20 countries (75%). Most countries (except Belgium, Cyprus and Spain) had a national programme, implemented nationwide in 11/14 responding countries (79%).
There was a dominant theoretical orientation in CAP education in 8/17 countries (47%): biopsychosocial in 3/8 (37.5%), psychodynamic in 2/8 (25%), medical in 1/8 (12.5%) and bio-medical in 2/8 (25%).
Training of psychiatrists is identified as a determining factor in improving transitional planning and care, both from the perspectives of trainees and youth experiencing transition between services (12, 13, 21, 23). A more informed training and education in transition in both AP and CAP curriculum is likely to facilitate transition and to have long term-effects in terms of mental health prevention. About half of all lifetime cases of mental illness start by the age of 14, rendering prevention and early treatment among adolescents all the more necessary, and emphasizing the importance for CAP specialists to be informed about general psychiatry (37). Around one-fourth of patients in AP aged 18–25 had previously received care at CAP (38), while around one-third of late teenagers/young adults at CAP need care from AP in adulthood (39). This stresses the importance of a smooth transition instead of rigid boundaries between disciplines, since mental disorders in adolescence predict mental health problems in adulthood (40). Parents of children treated in CAP are more likely to have mental health problems themselves, while children of patients treated in AP will be more prone to mental health difficulties. Providing a safe environment to children, for example in developing parental skills, plays a crucial role in preventing mental health conditions among youth and should be emphasized in all training routes. Early detection of emergent mental disorders is another topic that highlights the importance for specialists in both CAP and AP to develop knowledge in core competencies of each specialty.
This article provides the results of a survey describing the current status of training in transitional care in both AP and CAP postgraduate training across Europe. We also report data on the respective content of AP and CAP postgraduate training, with a particular focus on the amount of theoretical and practical cross-training between both specialties.
Previous findings showed that only 27% of trainees think that they have good knowledge in transitional care (21). Our results offer a potential explanation for this lack of knowledge of transition, as it is seldom a mandatory topic during AP training.
As regards issues related to transition, some progress is still required in the AP curriculum as they are addressed in only around half of the countries. For example, the AP-specific training programmes rarely address the issue of the key role of the family and related topics such as parent management techniques. Yet, the involvement of parents is essential in the early planning of transition (5) and at later stages in adult psychiatry, especially when patients are disabled and dependent on parental support.
Improved training in neurodevelopmental disorders, adolescent psychopathology and pharmacotherapy in the AP curriculum is also needed. Since intellectual disabilities do not disappear once a young person turns 18, the limited training on this issue in countries with AP specialization (theoretical training in 33% of countries [4/12] and placements in 9% [1/11]) is also an important gap. Training in this area for adult psychiatrists would allow a better consideration of this population and their specific needs in transition.
In the CAP curriculum, transition is addressed as a specific topic in 33% of countries (4/17) and most issues related to transition are addressed in more than 82% of the countries (9/11). However, these findings are not in line with the results from the above-mentioned study of Hendrickx et al. (21), in which CAP trainees from a larger sample, including 19 countries in common with ours, reported theoretical training in only 6 countries (16%). These differences between data from representatives of national associations and data from trainees suggest a possible gap between the national programmes and their implementation. In some countries, training in transition-relevant topics may also arrive at a late stage in the curriculum.
Transition is not a one-direction process sending young people from CAMHS to AMHS, but rather, is a continuous and closely connected care process based on shared decisions and planning between both services, involving young people and their caregivers as partners in decision-making early in the process. The development and implementation of guidelines (see www.uemscap.eu/working-group) to support transition of young people out of CAMHS would provide much needed guidance to clinicians about the transition process, options for transition pathways, and best practices in ensuring successful transitions (1, 36). These guidelines should be co-designed with youth, caregivers and clinicians, and be informed by the best available evidence. Such guidance would also be invaluable in helping those responsible for both AP and CAP curricula to ensure that all relevant topics are considered.
A recent scoping review identified 26 core components of successful CAMHS to AMHS transitions that could inform the basis for transitions pathways and guidelines (41). Among these components is the reciprocal core knowledge from both services that should be addressed through cross training as an essential component of optimal transitional care. The UEMS calls for a common trunk of core knowledge and skills in every national curriculum, including AP and developmental psychiatry, CAP, specific learning difficulties and intellectual disabilities. The high score of adherence of programmes to the UEMS recommendations (i.e., 8.2 in AP and 8.3/10 in CAP) is encouraging and the expected publication of specific UEMS recommendations for CAP is likely to improve responses to the specific needs of children, adolescents and young people during transition between services.
Collaborative working across services, involving joint meetings, communication, parallel working, as well as a shared cultural approach through education and training, are considered important for improving quality of transition and continuity of care (4, 27, 29). We tried to address these issues by exploring common topics and cross-training in the AP, CAP and generalist curricula.
Our data shows a joint theoretical base, but important variations in how this is actually addressed in training. Most topics recommended by the UEMS are mandatory in both AP and CAP training in the countries we studied. Some theoretical training in CAP is mandatorily associated with AP theoretical education in 18/19 countries (95%) and some theoretical training in AP is mandatorily associated with CAP theoretical education in 16/19 countries (84%). Among the other topics that we explored, emergency psychiatry, addiction, liaison and forensic are mandatory during AP training and CAP training in more than 63% of countries (12/19). However, this substantial joint theoretical base mostly concerns countries with a specialization route. In generalist countries, the common theoretical content is less comprehensive: AP, CAP and emergency psychiatry are the only three mandatory frequently addressed topics.
As opposed to theoretical training, practical cross-training in AP and CAP is not generalized: placements in AP are mandatorily associated with CAP training in 16/18 countries (89%) (in 13/15 countries with a specialization route in CAP, 87%); but placements in CAP are mandatorily associated with AP training in 14/20 countries (70%) (in 12/17 countries with a specialization route in AP, 71%). We found a higher proportion of mandatory placements in CAP within the AP-specialized curriculum than Oakley et al. (18) (i.e., 47%). Placements in AP within a CAP-specific route are similar to the 89% reported by Simmons et al. (20) and Barrett et al. (14), but this result is lower than the 100% reported by Oakley et al. (19). Therefore, it seems that placements in CAP have progressed in the AP curriculum, but placements in AP seem to have followed the opposite trend in the CAP curriculum. However, some caution is required in the comparison with the above-mentioned surveys: Oakley et al. (19) used a sample of trainees from 22 countries, with only 13 countries in common with ours; Simmons et al. (20) a sample of trainees from 28 countries, with only 17 countries in common; the survey of Barrett et al. (14) a sample of members of societies from 31 countries, with only 17 countries in common.
Furthermore, in contrast with our expectations, practical cross-training within both CAP as well as AP is not systematic within the generalist route, with CAP placements being mandatory in only 2/3 generalist countries (67%). Finally, our findings also suggest that mandatory placements in CAP during AP training are less numerous and represent a shorter practical experience in total than AP placements in CAP. However, these findings should be interpreted with caution due to the large proportion of missing information. The question of variable or limited exposure to CAP in AP training and, to a lesser degree, to AP in the CAP route was also raised elsewhere (14, 15, 19).
Concerns have been raised about the widespread specialization model across Europe which was described by Baessler et al. (22) and has been considered as a barrier to a common culture between CAP and AP (23). However, our findings about the adherence to UEMS standards highlight that separate specialities generally do provide a significant compulsory theoretical core cross-training, which is a facilitating factor for enhancing communication and information transfer. It is not clear if this theoretical cross-training is provided in joint sessions bringing together CAP and AP trainees, or in distinct groups. As regards the countries with a generalist curriculum, their adherence to UEMS standards is lower and offers no guarantee of practical cross-training.
Recommendations for improved training in transition care based on our findings are detailed in Table 4.
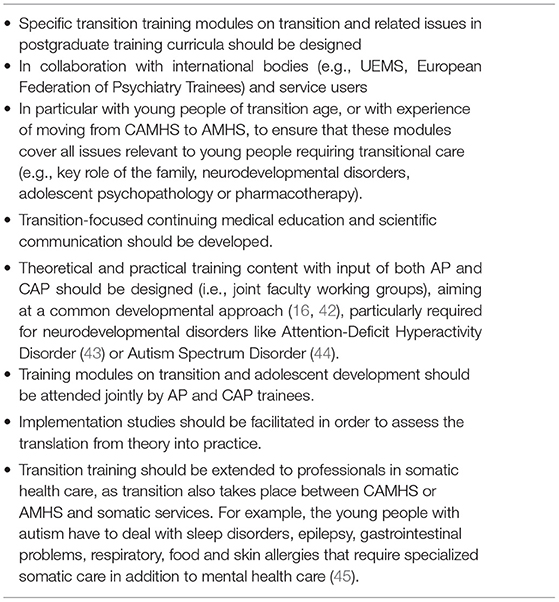
Table 4. Recommendations for improved training to transition care.
This survey is one of the first to specifically address the question of transition as a specific topic in postgraduate training programmes and to explore the question of cross-training between AP and CAP in relation to this topic. The responses by representatives of faculty and national associations complement existing data from reviews of literature, accessible curricula, trainees, as well as youths and their families (13, 21, 23).
However, a number of limitations need to be pointed out. Our conclusions should be considered as preliminary as they are based on small numbers and only 54% of the representatives of solicited European countries returned the survey. Nevertheless, the answers came from the most populated countries. Some of the items yielded missing or unclear data, but this was of limited influence as they mostly concerned secondary issues. Finally, among the countries with their syllabus due to be revised soon, only partial information was received.
It should also be emphasized that this study was limited to training in psychiatry, whereas transition planning also involves many other professionals, for example, psychologists, social workers, and mental health nurses. Training in transition and related topics is thus relevant in other curricula. Future enquiry also needs to address interdisciplinary treatment collaboration and information transfer.
Finally, we did not assess specific modalities in our analysis of theoretical cross-training. For example, it seems important to know whether training was provided in joint sessions bringing together CAP and AP trainees or in distinct groups of trainees.
This study suggests that specific training in transitional needs and management of patients in transitional care is still scarce across all training models. This may contribute to the well-recognized “transition gap” and should be addressed while designing best models of care and guidelines for transition. This situation calls for increased awareness of training gaps within psychiatry programmes and a need to enhance collaborative work and mutual understanding between CAP and AP services. A better postgraduate training on transition may thus proceed from programmes designed in joint faculty working groups and may take place through modules attended jointly by AP and CAP trainees. The role of those responsible for training programs at a local, national and international level to address the issue of transition and cross training between AP and CAP should also be considered. Finally, there is a need for further research on how best to develop specific training to transitional care that encompasses theoretical and practical knowledge which also includes strengthening collaborative teamwork, communication, information transfer and family involvement. Some further research should also be conducted on how this training would have an impact on the success of transitions experienced by young people. Apart from better clinicians, bridging the gap between services involves a change in research cooperation, transition planning, organization of care, mutual understanding about each other's workplaces, and bringing together different care cultures and different perspectives such as family-oriented care in CAP and individual-oriented care in AP.
The data that support the findings of this study are available on request to the authors at Zi1ydXNzZXRAY2h1LW1vbnRwZWxsaWVyLmZy.
The survey is part of the MILESTONE project, for which an ethics approval was granted by the Ethics Committee Comité de protection des personnes Sud Méditerranée I. No further ethical approval was required for this specific survey, as no personal data were collected.
Swaran Singh, Helena Tuomainen, Jason Madan, Jane Warwick, Cathy Street, Dieter Wolke, Moli Paul, Priya Tah, Rebecca Appleton, Alastair Canaway, James Griffin, Philip Wells, Rose-Marie Lomax (University of Warwick, UK), Giovanni de Girolamo, Giulia Signorini (Saint John of God Clinical Research Center, Italy), Paramala Santosh, Natalie Heaney, Mathilde Mastroianni, Laura Adams, Sagar-Ouriaghli I, Kate Lievesley, Jatinder Singh, Federico Fiori (Kings College London, UK), Diane Purper-Ouakil, Frédérick Russet, Virginie Maurice, Véronique Humbertclaude (Hôpital Saint Eloi, France), Athanasios Maras, Larissa van Bodegom, Mathilde Overbeek (Yulius Academie, the Netherlands), Ulrike Schulze, Melanie Saam, Ulrike Breuninger, Anne Sartor, Elena Tanase, Vehbi Sakar (University of Ulm, Germany), Sabine Tremmery, Gaëlle Hendrickx, Veronique De Roeck (KU Leuven, Belgium), Fiona McNicholas, Aleksandra Gronostaj, Ingrid Holme, Lesley O Hara (University College Dublin, Ireland), Tomislav Franić, Nikolina Davidović (University Hospital Split, Croatia), Frank Verhulst, Gwen Dieleman, Suzanne Gerritsen (Erasmus MC, The Netherlands), Kate Lievesley (HealthTracker, UK), Amanda Tuffrey, Anna Wilson, Charlotte Gatherer, Leanne Walker (Young project advisors, University of Warwick, UK), Andrea Wohner (concentris research management GmbH, Germany).
FR and VH were in charge of the study design, conducted the data search and analysis, and wrote the first draft of the manuscript. DP-O and ST were in charge of Work Package lead, study design, and writing. ND, GD, KD-Ć, TF, SG, GG, GH, HK, FM, AM, SP, MP, AS, US, CS, HT, DW, and SS provided substantial contribution to the final manuscript. All authors read and approved the final manuscript.
The MILESTONE project received funding from the European Union's Seventh Framework Programme for research, technological development, and demonstration under Grant Agreement No. 602442. The European Commission (FP7 programme) had no involvement in the writing of the manuscript or in the decision to submit the manuscript for publication. SS was supported by the National Institute for Health Research (NIHR) Applied Research Centre (ARC) West Midlands.
The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. This Health Policy reflects only the author's views and the EU is not liable for any use that might be made of the information contained therein.
SP is employed by HealthTracker Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to express our great appreciation to all the representatives of national psychiatry associations and/or university professors who accepted to complete the Milestone questionnaire.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.768206/full#supplementary-material
1. ^Number of countries/number of respondent countries.
1. Singh SP, Paul M, Ford T, Kramer T, Weaver T, McLaren S, et al. Process, outcome and experience of transition from child to adult mental healthcare: Multiperspective study. Br J Psychiatry. (2010) 197:305–12. doi: 10.1192/bjp.bp.109.075135
2. Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. (2016) 387:2423–78. doi: 10.1016/S0140-6736(16)00579-1
3. Memarzia J, St Clair MC, Owens M, Goodyer IM, Dunn VJ. Adolescents leaving mental health or social care services: predictors of mental health and psychosocial outcomes one year later. BMC Health Serv Res. (2015) 15:185. doi: 10.1186/s12913-015-0853-9
4. Schandrin A, Capdevielle D, Boulenger J-P, Batlaj-Lovichi M, Russet F, Purper-Ouakil D. Transition from child to adult mental health services: A french retrospective survey. J Ment Health Train Educ Pract. (2016) 11: 286–93.
5. Singh S, Paul M, Islam Z, Weaver T, Kramer T, McLaren S, et al. Transition From CAMHS to Adult Mental Health Services (TRACK): A Study Of Service Organisation, Policies, Process and User And Carer Perspectives. Report for the Youth Mental Health Ontario, Toronto, ON, Canada. (2011).
6. Davidson S, Cappelli M. We've Got Growing up to do: Ontario Centre of Excellence for Children and Youth Mental Health Ontario, Ottawa, ON, Canada. (2011).
7. Hovish K, Weaver T, Islam Z, Paul M, Singh SP. Transition experiences of mental health service users, parents, and professionals in the United Kingdom: A qualitative study. Psychiatr Rehabil J. (2012) 35: 251–7. doi: 10.2975/35.3.2012.251.257
8. Carver J, Cappelli M, Davidson S. Taking the Next Step Forward: Building A Responsive Mental Health and Addictions System For Emerging Adults. Mental Health Commission of Canada Commission de la santé mentale du Canada (2015). Available online at: https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/Taking%252520the%252520Next%252520Step%252520Forward_0.pdf
9. Supporting Young People During Transition to Adult Mental Health Services. NSW Government (2018). Available online at: https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/GL2018_022.pdf
10. Singh SP, Tuomainen H. Transition from child to adult mental health services: needs, barriers, experiences and new models of care. World J. Psychiatry (2015) 14:358–61 doi: 10.1002/wps.20266
11. Signorini G, Singh SP, Marsanic VB, Dieleman G, Dodig-Curković K, Franic T, et al. The interface between child/adolescent and adult mental health services: results from a European 28-country survey. Eur Child Adolesc Psychiatry. (2018) 27:501–11.
12. Olibris B, Mulvale G, Carusone SC, Lin E, Domonchuk-Whalen M, Whittaker K. Spotlight on caroline families first wraparound program: lessons for advancing collaborative family-centred care for complex child and youth mental health. CJCMH. (2017) 36:191–204. doi: 10.7870/cjcmh-2017-012
13. Jivanjee P, Kruzich JM, Gordon LJ. The age of uncertainty: Parent perspectives on the transitions of young people with mental health difficulties to adulthood. J Child Fam Stud. (2009) 18:435–46. doi: 10.1007/s10826-008-9247-5
14. Barrett E, Jacobs B, Klasen H, Herguner S, Agnafors S, Banjac V, et al. The child and adolescent psychiatry: study of training in Europe (CAP-STATE). Eur Child Adolesc Psychiatry. (2020) 29:11–27.
15. Kumperscak HG, Clausen C, Anagnostopoulos D, Otasevic ZB, Marsanic VB, Burgic M, et al. Child and adolescent psychiatry training and mental health care in Southeast Europe. Eur Child Adolesc Psychiatry. (2020) 29:29–39.
16. Kuzman MR, Giacco D, Simmons M, Wuyts P, Bausch-Becker N, Favre G, et al. Psychiatry training in Europe: views from the trenches. Med Teach. (2012) 34:e708–e17.
17. Mayer S, Van der Gaag R, Dom G, Wassermann D, Gaebel W, Falkai P, et al. European Psychiatric Association (EPA) guidance on post-graduate psychiatric training in Europe. Eur Psychiatry. (2014) 29:101–06.
18. Lotz-Rambaldi W, Schäfer I, ten Doesschate R, Hohagen F. Specialist training in psychiatry in Europe–Results of the UEMS-survey. Eur Psychiatry. (2008) 23:157–68.
20. Simmons M, Barrett E, Wilkinson P, Pacherova L. Trainee experiences of child and adolescent psychiatry (cap) training in Europe: 2010–2011 survey of the European federation of psychiatric trainees (efpt) cap working group. Eur Child Adolesc Psychiatry. (2012) 21:433–42.
21. Hendrickx G, De Roeck V, Russet F, Dieleman G, Franic T, Maras A, et al. Transition as a topic in psychiatry training throughout Europe: trainees' perspectives. Eur Child Adolesc Psychiatry. (2020) 29:41–9.
22. Baessler F, Zafar A, Gargot T, da Costa MP, Biskup EM, De Picker L, et al. Psychiatry training in 42 European countries: A comparative analysis. Eur Neuropsychopharmacol. (2021) 46:68–82.
23. Russet F, Humbertclaude V, Dieleman G, Dodig-Curković K, Hendrickx G, Kovač V, et al. Training of adult psychiatrists and child and adolescent psychiatrists in europe: a systematic review of training characteristics and transition from child/adolescent to adult mental health services. BMC Med Educ. (2019) 19:204. doi: 10.1186/s12909-019-1576-0
24. Fegert, JM, Hauth, I, Banaschewski, T, Freyberger, HJ,. Transition From Adolescence to Adulthood: The Challenges to Establish “Transition Psychiatry.” Key Issues Paper by DGKJP and DGPPN. Available online at: https://www.escap.eu/events/past-escap-congresses/geneva/duplicate-of-madrid-keynote-and-symposiums/transitions-from-adolescence-to-adulthood-key-issue-paper
25. Davis M, Sondheimer DL. State child mental health efforts to support youth in transition to adulthood. J Behav Health Serv Res. (2005) 32:27–42.
26. Anderson Y. CAMHS to Adult Transition: HASCAS Tools for Transition: A Literature Review for Informed Practice. London, Health and social Care Advisory Service. (2006) Available online at: www. hascas.org.uk
27. McLaren S, Belling R, Paul M, Ford T, Kramer T, Weaver T, et al. ‘Talking a different language': An exploration of the influence of organizational cultures and working practices on transition from child to adult mental health services. BMC Health Serv Res. (2013) 13:254. doi: 10.1186/1472-6963-13-254
28. Paul M, Street C, Wheeler N, Singh SP. Transition to adult services for young people with mental health needs: a systematic review. J Child Psychol Psychiatry. (2015) 20:436–57.
29. Mulvale GM, Nguyen TD, Miatello AM, Embrett MG, Wakefield PA, Randall GE. Lost in transition or translation? Care philosophies and transitions between child and youth and adult mental health services: a systematic review. J Ment Health. (2016) 28:379–88.
30. Singh SP, Tuomainen H, De Girolamo G, Maras A, Santosh P, McNicholas F, et al. Protocol for a cohort study of adolescent mental health service users with a nested cluster randomised controlled trial to assess the clinical and cost-effectiveness of managed transition in improving transitions from child to adult mental health services (the MILESTONE study). BMJ Open (2017) 7:e016055.
31. Union Européenne des Médecins Spécialistes. Section for Psychiatry-European Board of Psychiatry. Charter on training of medical specialist in the EU-requirements for the speciality of psychiatry. Brussels: UEMS (2003).
32. Union Européenne des Médecins Spécialistes. Report of the UEMS Section for Psychiatry: The Profile of a Psychiatrist. Brussels: UEMS (2005).
33. Union Europeenne des Medecins Specialistes. European Framework for Competencies in Psychiatry. UEMS (2009). Available online at: http://uemspsychiatry.org/wp-content/uploads/2013/09/2009-Oct-EFCP.pdf
34. Union Europeenne des Medecins Specialistes. European Training Log-Book for Child and Adolescent Psychiatry. UEMS (2014). Available online at: http://www.uemscap.eu/training
35. Union Europeenne des Medecins Specialistes. Training Requirements for the Specialty of Child and Adolescent Psychiatry. European Standards of Postgraduate Medical Specialist Training. UEMS (2014). Available online at: http://www.uemscap.eu/training
36. National Institute for Health and Care Excellence. Transition From Children's to Adults' Services for Young People Using Health or Social Care Services. Clinical guideline NG43 (2016).
37. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of dsm-iv disorders in the national comorbidity survey replication. Arch Gen Psychiatry. (2005) 62:593–602.
38. Ramirez A, Ekselius L, Ramklint M. Mental disorders among young adults self-referred and referred by professionals to specialty mental health care. Psychiatr Serv. (2009) 60:1649–55.
39. Engqvist U, Rydelius P-A. Child and adolescent psychiatric patients and later criminality. BMC Public Health (2007) 7:1–14.
40. Patton GC, Coffey C, Romaniuk H, Mackinnon A, Carlin JB, Degenhardt L, et al. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet. (2014) 383: 1404–11.
41. Cleverley K, Rowland E, Bennett K, Jeffs L, Gore D. Identifying core components and indicators of successful transitions from child to adult mental health services: a scoping review. Eur Child Adolesc Psychiatry. (2020) 29:107–21. doi: 10.1007/s00787-018-1213-1
42. Lamb C, Hall D, Kelvin R, Van Beinum M. Working at the CAMHS/Adult Interface: Good Practice Guidance for the Provision of Psychiatric Services to Adolescents/Young Adults. London: Royal College of Psychiatrists (2008).
43. Hall CL, Newell K, Taylor J, Sayal K, Swift KD, Hollis C. ‘Mind the gap'-mapping services for young people with ADHD transitioning from child to adult mental health services. BMC psychiatry (2013) 13:186. doi: 10.1186/1471-244X-13-186
44. National Audit Office. Supporting People With Autism Through Adulthood: Report by the Controller and Auditor General (2009). Available online at: https://www.nao.org.uk/wp-content/uploads/2009/06/0809556es.pdf
Keywords: transition, transitional care, training, psychiatry, general adult psychiatry, adolescent psychiatry, child psychiatry, Europe
Citation: Russet F, Humbertclaude V, Davidovic Vrljicak N, Dieleman GC, Dodig-Ćurković K, Franic T, Gerritsen SE, de Girolamo G, Hendrickx G, Kerbage H, McNicholas F, Maras A, Paramala S, Paul M, Schandrin A, Schulze UME, Street C, Tuomainen H, Wolke D, Singh SP, Tremmery S and Purper-Ouakil D (2022) Are Psychiatrists Trained to Address the Mental Health Needs of Young People Transitioning From Child to Adult Services? Insights From a European Survey. Front. Psychiatry 12:768206. doi: 10.3389/fpsyt.2021.768206
Received: 31 August 2021; Accepted: 29 November 2021;
Published: 09 February 2022.
Edited by:
Benedetto Vitiello, University of Turin, ItalyReviewed by:
Paola Rocca, University of Turin, ItalyCopyright © 2022 Russet, Humbertclaude, Davidovic Vrljicak, Dieleman, Dodig-Ćurković, Franic, Gerritsen, de Girolamo, Hendrickx, Kerbage, McNicholas, Maras, Paramala, Paul, Schandrin, Schulze, Street, Tuomainen, Wolke, Singh, Tremmery and Purper-Ouakil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frederick Russet, Zi1ydXNzZXRAY2h1LW1vbnRwZWxsaWVyLmZy
†These authors share first authorship
‡Co-leaders for this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.