
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 09 December 2021
Sec. Addictive Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.751550
 Maximilian Meyer1*
Maximilian Meyer1* Isabel Sattler2Hanna Schilling2
Isabel Sattler2Hanna Schilling2 Undine E. Lang1
Undine E. Lang1 André Schmidt1
André Schmidt1 Flora Colledge2†
Flora Colledge2† Marc Walter1†
Marc Walter1†Background and Aims: Exercise addiction has not yet been designated as an addictive disorder in the DSM-5 due to a lack of detailed research. In particular, associations with other psychiatric diagnoses have received little attention. In this study, individuals with a possible exercise addiction are clinically assessed, in order to establish a profile of co-occurring psychiatric disorders in individuals with exercise addiction.
Methods: One hundred and fifty-six individuals who reported exercising more than 10 h a week, and continued to do so despite illness or injury, were recruited for the study. Those who met the cut-off of the Exercise Dependence Scale (n = 32) were invited to participate in a screening with the Structured Clinical Interview for DSM-5 (SCID-5-CV) and personality disorders (SCID-5-PD). Additionally, an interview based on the DSM-5 criteria of non-substance-related addictive disorders was conducted to explore the severity of exercise addiction symptoms.
Results: 75% of participants fulfilled the criteria for at least one psychiatric disorder. Depressive disorders (56.3%), personality disorders (46.9%) and obsessive-compulsive disorders (31.3%) were the most common disorders. Moreover, there was a significant positive correlation between the number of psychiatric disorders and the severity of exercise addiction (r = 0.549, p = 0.002).
Discussion: The results showed a variety of mental disorders in individuals with exercise addiction and a correlation between the co-occurrence of mental disorders and the severity of exercise addiction. Exercise addiction differs from other addictive und substance use disorders, as obsessive-compulsive (Cluster C), rather than impulsive (Cluster B) personality traits were most commonly identified.
Conclusions: Our results underscore the importance of clinical diagnostics, and indicate that treatment options for individuals with exercise addiction are required. However, the natural history and specific challenges of exercise addiction must be studied in more detail.
The term exercise addiction can be found in scientific literature dating back to the late 1970s (1). It is used to refer to individuals who lose control over their exercising habits and continue their regimen despite negative physical, psychological, and social consequences (2). Other terms like obligatory exercise, exercise dependence and compulsive exercise have emerged since (3, 4). Although the symptoms of exercise addiction have been described in the literature for over five decades, robust evidence for the classification as a behavioural disorder is still lacking (5, 6). The literature consists mostly of qualitative data and case reports listing self-reported symptoms of the phenomenon (7–9) while consistent and methodologically solid studies are scarce (2, 10). To assess unhealthy exercising behaviour, scholars have developed questionnaires based on the self-reported symptoms of their study subjects (11). Those questionnaires also highlight that a uniform understanding of the phenomenon is lacking: the Exercise Dependence Scale (EDS) (12) identifies individuals at risk of exercise dependence and the Obligatory Exercise Questionnaire (OEQ) (13) rates whether problems with obligatory exercise can be observed. Colledge et al. (14) have pointed out that in a review of 79 questionnaire-based studies addressing exercise addiction, five different questionnaires are employed, each of which is based on a distinct conceptual framework.
With the introduction of pathological gambling in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, “gambling disorder” is still the sole addictive disorder that is found in the category of “non-substance-related disorders.” Other behaviours with possible pathological characteristics have been discussed but not been added due to insufficient peer-reviewed evidence (10). Behaviours that show addictive or pathological traits and are therefore being investigated are internet-related behaviours like gaming (15), as well as sex, shopping, and exercise (5). Notably, there is an ongoing general discussion about the extent to which excessive behaviours can be compared to substance-related addictive disorders (16, 17). A main point of criticism is that criteria for substance-related addictions are often adapted and used for identifying behavioural addictions without it being clear whether those criteria are suitable for pathological behaviours (18). It also bears noting that the guidelines which might constitute a mental disorder are subject of debate (19). The DSM-5 characterises mental disorders as syndromes affecting the individual's cognition, emotion regulation, or behaviour. It further states that significant distress is usually associated with the underlying condition (20). Therefore, the demonstration of psychological distress caused by excessive behaviours is necessary to strengthen the argument for the addition of further non-substance-related disorders. Nonetheless, excessive behaviours show apparent similarities to substance-related addictions: dual-diagnoses are commonly made in individuals suffering from gambling disorder, particularly impulse-control disorders, mood disorders, anxiety disorders and other addictive (substance related) disorders (21). Petry et al. (22) reported that individuals with gambling addiction from a large national sample of the United States also suffered from alcohol use disorder (73.2%), personality disorders (60.8%), affective disorders (49.6%), anxiety disorders (41.3%), and 38.1% had a substance use disorder (excluding alcohol). This is in line with the findings of Kessler et al. (23), who reported that 96.3% of those with gambling disorder also meet the criteria for another mental disorder in their lifetime.
In a recent meta-review Colledge et al. (24) studied the range of symptoms reported in the literature, and proposed criteria for exercise addiction based on the DSM-5 criteria for gambling disorder (Table 1). These criteria are designed to serve as the basis for a clinical screening of symptoms which may indicate exercise addiction. Since these criteria were used in this study to rate the severity of the observed symptoms, the term exercise addiction is used concordantly.
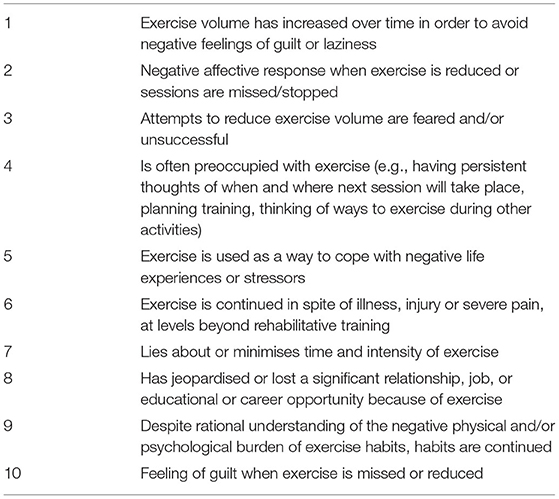
Table 1. Criteria developed for rating the severity of exercise addiction based on symptoms that have been reported to occur in individuals who exercise excessively (24).
In case of exercise addiction, the prevalence and range of co-occurring mental disorders has not yet been clinically examined. Eating disorders are frequently discussed within the context of excessive exercising habits (25) and indeed it seems intuitive that exercise might be practised simply for the purpose of weight control. Furthermore, some of the highest prevalence rates of exercise addiction (between 38 and 45%) are reported in individuals with diagnosed eating disorders (26). Exercising behaviour would therefore have to be considered a symptom of the underlying disorder rather than its own entity. In respect to this, the differentiation between primary and secondary exercise dependence has been proposed, with primary meaning that exercising habits are not a secondary feature of anorexia nervosa or bulimia nervosa (27). This distinction has been broadly adopted by scholars and the implication has been made that exercise dependence without co-occurring eating disorders is a rare phenomenon (28–30). However, Grandi et al. (31) have explicitly excluded those with eating disorders in their studies, and still found symptoms of exercise addiction, providing evidence that the phenomenon exists apart from eating disorders.
The theory that exercise addiction might be a maladaptive coping-strategy to escape from psychological hardship has also been discussed (4, 32). This is supported by robust evidence that exists for positive effects of physical exercise in individuals with major depression (33, 34). Indeed, it seems plausible that exercise might resemble a self-medicating coping pattern and is being used for affect-regulation and stress relief. It is also possible that exercise addiction might be related to emotional dysregulation (35) and higher levels of alexithymia (36) which are also commonly found in substance use disorders. However, to date, no studies with a longitudinal design examine the chronological relationship between exercise addiction and co-occurring mental disorders to test this theory.
In summary, doubts about the existence of primary exercise addiction and whether it should be regarded as a behavioural addiction are warranted. Although symptoms of exercise addiction are consistently reported in the literature, no clinical studies that examine the prevalence of a variety of mental disorders in individuals with exercise addiction are available. It is therefore unclear whether those with exercise addiction suffer from mental disorders more commonly than the general population, and whether they show the same pattern of co-occurring disorders that has been observed in other behavioural disorders like gambling disorder. It is also unclear whether the severity of exercise addiction symptoms affect and influence co-occurring disorders, and whether those disorders originate from the excessive exercising habits or vice versa.
Thorough clinical diagnostic screening is needed in individuals with exercise addiction to gather data on the prevalence of co-occurring disorders. This would make it possible to investigate whether co-occurring disorders are in fact limited to eating disorders or whether their range matches that of substance use disorders and pathological gambling. If exercise addiction occurs with a varying range of other diagnoses, this could be further evidence that it is a distinct mental disorder. We are the first group worldwide to systematically identify a population of individuals with exercise addiction and conduct gold-standard clinical diagnostic interviews; this study paves the way for a detailed, clinical description of the to-date insufficiently defined phenomenon of exercise addiction.
The present study investigates the co-occurrence of mental disorders in individuals with exercise addiction. We hypothesise that the range of co-occurring disorders matches those of other substance-related disorders, such as depressive disorders, personality disorders, and anxiety disorders, and is therefore not limited to eating disorders.
Individuals were recruited by advertisements in fitness studios, a local newspaper and via Unimarkt Basel, an online market platform run by the University of Basel. Recruitment took place between 2019 and 2021. The advertisements invited applicants between 18 and 70 years of age, exercising more than 10 h a week, and continuing their exercise despite illness or injuries to participate. These criteria were selected as they were judged to be indicative of a possible addictive disorder in line with DSM-5 criteria, yet also simple and clear enough to be communicated clearly on an advertising flyer or poster. CHF 40 were given for participation in the first examination and an additional 150 CHF were given for further participation in the study.
During the initial screening, the Exercise Dependence Scale-21 (EDS-21) was used to identify individuals with possible exercise addiction. The EDS-21 is a validated 21-item questionnaire whose development was based on the DSM-IV criteria for substance use disorders (12). Each criterion (tolerance, withdrawal, intention effect, lack of control, time, reduction in other activities and continuance) is represented by a subscale, consisting of 3 items. Items are rated on a 6-point Likert-scale. Participants who score in the dependent range (i.e., 4 or 5 on the Likert-scale) on at least three criteria are rated “symptomatic, at-risk for exercise dependence” (12). Individuals who met this cut-off were invited to a second examination.
In the second examination, the Structured Assessment of Personality Abbreviated Scale (SAPAS) was conducted. The SAPAS is a brief screening tool for personality disorders that consists of 8 items and showed good sensitivity (0.94) and acceptable specificity (0.85), with the cut-off being set at 3 fulfilled items or more (37). Next, the Structured Clinical Interview for DSM-5 (SCID-5) was conducted to screen for mental disorders. The SCID-5-CV was used in every participant to screen for lifetime prevalence of depressive disorders and currently prevalent Axis I disorders. In addition, the SCID-5-PD was conducted on participants that met the cut-off of the SAPAS score. Third, participants were interviewed about their exercising habits and the extent of their exercise addiction.
Severity of exercise addiction symptomatology was assessed using the 10 item symptom checklist suggested by Colledge et al. (24) and shown in Table 1. These criteria were derived from available literature on the phenomenon of exercise addiction and used to further describe and assess the severity of symptoms. The degree of severity was rated severe if 9 or 10 criteria were fulfilled, moderate for 7 or 8, mild for 5 or 6 or subclinical if the participant fulfilled 4 criteria or less.
The EDS-21 was provided in paper-pencil form. Interviews were held face-to-face. Following the outbreak of COVID-19, the EDS-21 was provided online and interviews were held via the conferencing platform Zoom.
Data analysis was conducted using SPSS version 27. A one-way ANOVA was conducted to find out whether there was a difference between exercise addiction severity groups (subclinical, mild, moderate, and severe) and mean number of mental disorders in each group. A post-hoc Tukey test was used to identify which groups differ from each other. Level of significance was set at p < 0.05.
Pearson's r correlation coefficient was calculated to find out whether the number of fulfilled exercise addiction criteria correlated with total number of mental disorders. Two-sided level of significance was set at p < 0.05.
An independent t-test was conducted to find out whether the number of fulfilled exercise addiction criteria differed in individuals who participated in athletic competitions. Two-sided level of significance was set at p < 0.05.
Outliers exceeding two standard deviations in number of disorders were excluded for the calculation of Pearson's r and one-way ANOVA (n = 2).
One hundred and fifty-six individuals were recruited for screening, of which 32 met the cut-off of the EDS-21 and were invited to the second examination. Mean age of our sample was 27.9 years (SD = 12.5), comprising 16 men and 16 women. Exercise hours per week ranged from 5 to 55 (M = 17.2, SD = 10.3). Although a minimum of 10 h exercise per week was an explicit inclusion criterion, it emerged that one participant reduced their exercise activity between recruitment and completion of the interview, accounting for this discrepancy. 46.9% (n = 15) reported participation in competitions. The level of competition ranged from local leagues to national and world championship participation. None of our participants was a full-time professional athlete. Most participants reported doing multiple different sports. Fitness (strength training) was most common (n = 23), followed by running (n = 14) and cycling (n = 12). Other disciplines varied greatly and included handball, CrossFit, tennis, hiking, martial arts, yoga, basketball, hammer throw, swimming and climbing, among others.
Exercise addiction severity ranged from subclinical (0–4 criteria) to severe (9–10 criteria). A total of 8 (25%) participants fulfilled 4 criteria or fewer. Mild exercise addiction (5–6 criteria) was found in 25% (n = 8), moderate exercise addiction (7–8 criteria) was found in 37.5% (n = 12) and severe exercise addiction (9–10 criteria) was found in 12.5% (n = 4).
Participants were diagnosed with 32 different mental disorders as defined by the DSM-5, with a total of 100 diagnoses. Major depressive disorder was the most common and was found in 46.9% (n = 15), followed by obsessive-compulsive personality disorder (n = 8, 25%) and insomnia (n = 8, 25%). The complete range of disorders is listed in Table 2. No mental disorder was found in 25% (n = 8). One participant with moderate exercise addiction was found to have no mental disorders. All participants with more than seven fulfilled exercise addiction criteria also met the diagnostic criteria for at least one mental disorder.
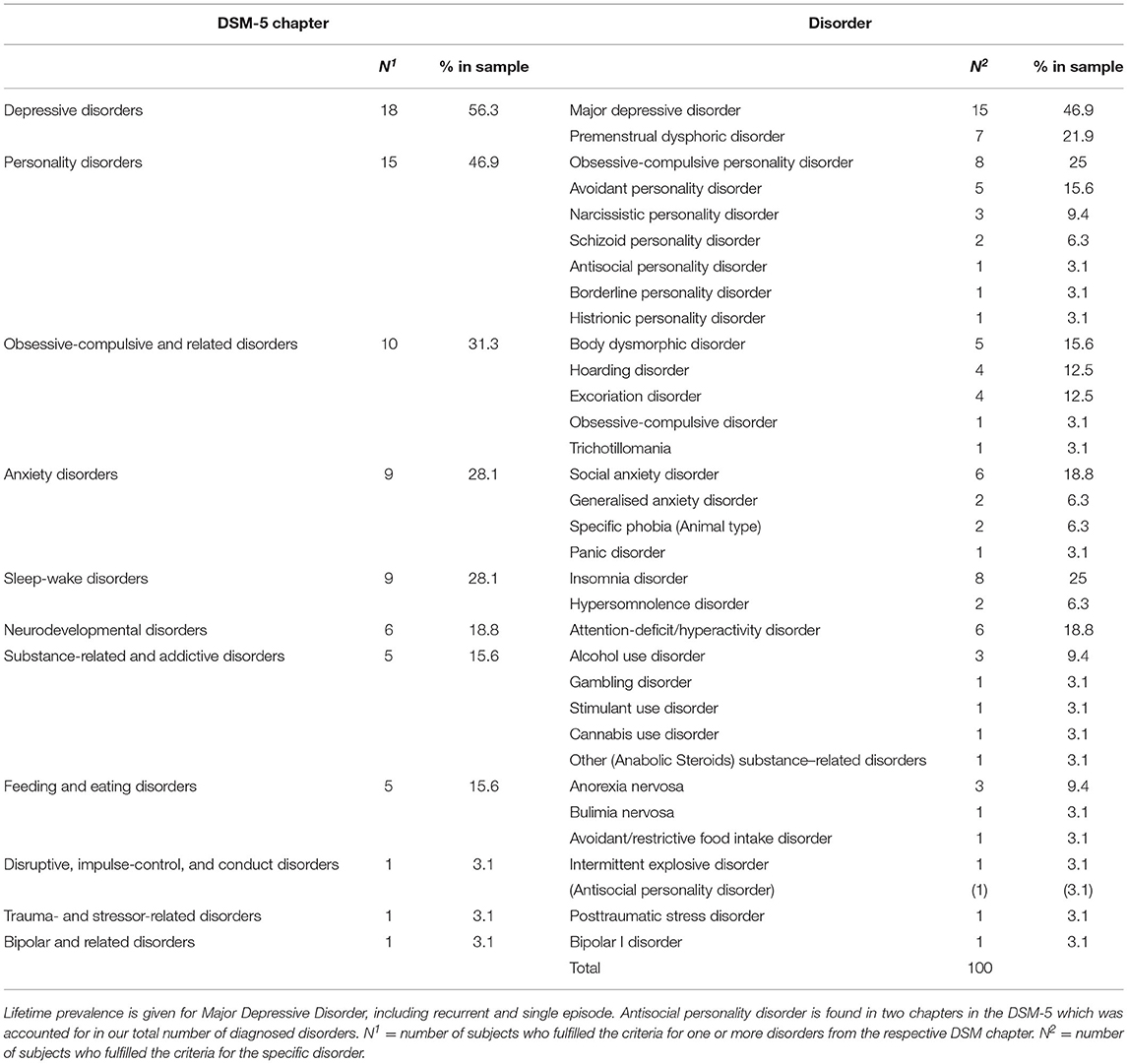
Table 2. DSM-5 chapters and their according disorders currently prevalent in our sample (n = 32).
There was a statistically significant difference between exercise addiction severity groups on total number of mental disorders as determined by one-way ANOVA [F(3, 26) = 3.54, p = 0.028]. The total number of disorders increased from subclinical exercise addiction (M = 0.17, SD = 0.41), to mild exercise addiction (M = 2.63, SD = 2.72), to moderate exercise addiction (M = 3.50, SD = 2.89), to severe exercise addiction (M = 3.50, SD = 2.40) (see Figure 1). A post-hoc Tukey test showed that only the subclinical group and the moderate group differed significantly at p < 0.05 (p = 0.021).
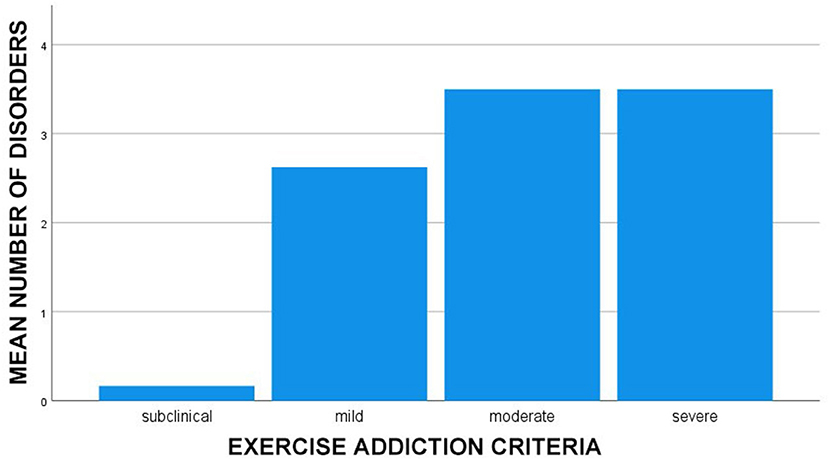
Figure 1. Mean number of mental disorders by severity of exercise addiction (n = 30). Outliers exceeding two standard variations in number of disorders (n = 2) were excluded.
The total number of disorders showed a strong positive correlation to the severity of exercise addiction (r = 0.506, p = 0.004) and is demonstrated in Figure 2.
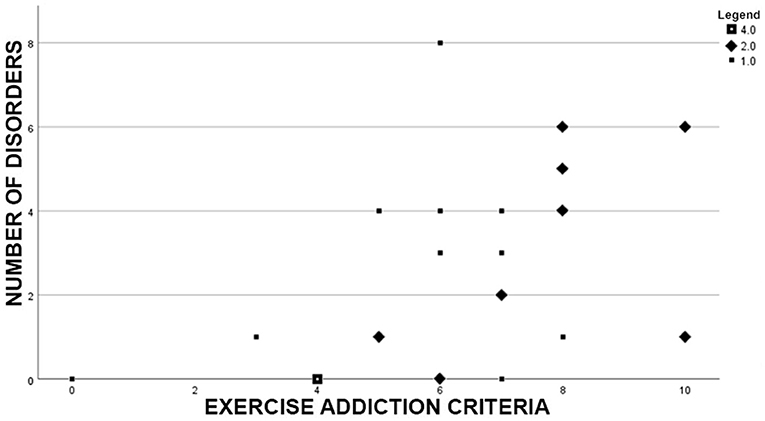
Figure 2. Scatterplot of our sample (n = 30) demonstrating the correlation between number of fulfilled exercise addiction criteria and number of disorders. Outliers exceeding two standard variations in number of disorders (n = 2) were excluded.
Table 3 compares found disorders according to their DSM-5 chapter in competing and non-competing participants. There was no statistically significant difference in the number of fulfilled exercise addiction criteria [t(30) = −0.20, p = 0.369] of participants who competed (M = 6.40, SD = 2.72), when compared to the rest of the sample (M = 6.24, SD = 2.05).
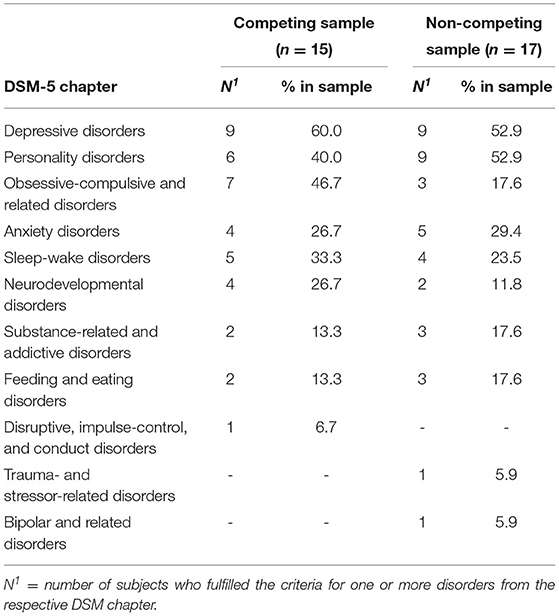
Table 3. Comparison of mental disorders by DSM-5 chapter between competing and non-competing participants.
This is the first study to systematically identify individuals with exercise addiction and conduct a gold-standard psychiatric diagnostic screening. Only individuals that met the cut-off of the EDS-21 (12) were invited for diagnostic screening. We found a high prevalence of mental disorders in individuals with exercise addiction, with 75% suffering from at least one disorder listed in the DSM-5. Additionally, the spectrum of disorders we found was broad: 32 different disorders were diagnosed in a sample of 32 participants (see Table 2).
The most common comorbidities in gambling disorder have been found to be alcohol use disorder, personality disorders, affective disorders, and anxiety disorders (22). Cluster B personality disorders are found the most in gambling addiction, followed by Cluster C and Cluster A disorders (38). In our sample, depressive disorders (56.3%), personality disorders (46.9%) and obsessive-compulsive disorders (31.3%) were the most common (Table 2). Cluster C personality disorders were particularly common with 40.6% of participants suffering from either obsessive-compulsive personality disorder (25%) or avoidant personality disorder (15.6%). This finding suggests that impulsive personality traits might be less prevalent in individuals with exercise addiction who rather seem to be located at the compulsive pole of the diagnostic spectrum. Notably, scholars have previously discussed two different dimensions of “unhealthy exercise”: a quantitative dimension (“excessive”) that takes duration, frequency and intensity of exercise into account and a qualitative dimension (“compulsive”), which is characterised by rigid exercise schedules, prioritisation of exercise over other activities and feeling of guilt and anxiety when exercise sessions are missed (39). As addiction is defined in the DSM-5 in terms of cognitive, physical, and behavioural characteristics, and not in quantitative terms, the “compulsive” dimension appears to be more relevant in the identification of exercise addiction.
The total number of mental disorders in our sample increased with exercise addiction severity. Additionally, there was only one participant without a mental disorder who fulfilled seven or more exercise addiction criteria. While our statistical analysis does not account for the clinical severity of the respective conditions, this finding implies that with an increasing number of exercise addiction criteria the occurrence of a mental disorder is also more likely. This indicates that exercise addiction is found in individuals who are more likely to require psychiatric treatment.
Most interestingly, only five participants in our sample suffered from an eating disorder. This contradicts previous studies which reported a strong link between exercise addiction and eating disorders (28–30). The variety of sport disciplines practised in our sample supports the findings of Lichtenstein et al. (40), who found no difference in the prevalence of exercise addiction between team sports and endurance sports.
Besides eating disorders, exercise addiction might be secondary to other mental disorders such as obsessive-compulsive disorders. Scholars have previously reported on primary exercise addiction to show traditional addictive traits, whereas secondary exercise addiction was found to be more compulsive in nature (30). No strong link between exercise addiction and eating disorders was observed in our sample. However, this is not the case for obsessive-compulsive disorders and obsessive-compulsive personality disorders. Therefore, we are not able to rule out that exercise addiction symptoms might be secondary to this part of the diagnostic spectrum. Literature also indicates an association between body dysmorphic disorder and exercise addiction symptoms (41). However, our data suggests that these symptoms are not limited to body dysmorphic disorder or obsessive-compulsive disorder alone, as we found that only five and one participant(s) respectively met the diagnostic criteria for each specific disorder.
It might also be possible that our sample included multiple heterogenous groups of aspiring athletes, individuals suffering from eating disorders and individuals with body dysmorphic disorder, all of which would require a more careful interpretation of the respective role of exercise addiction symptoms. However, we do not think that this was the case regarding participation in athletic competitions. Even though we did not conduct statistical inference, the descriptive comparison of disorders by competing and non-competing participants (Table 3) did not differ noticeably. We also did not find a statistically significant difference between competing and non-competing participants in number of fulfilled exercise addiction criteria.
More than half of our sample suffered from a depressive disorder (56.3%) in their lifetime, with major depressive disorder being the most common (46.9%). Since exercise has been found to have positive effects on depression (33, 34), the theory that excessive exercise is used as self-medicating coping-pattern seems plausible. Further studies are needed to investigate the natural history of exercise addiction and its connexion to the emergence of depression longitudinally.
The importance of clinical distress caused by conditions that qualify as mental disorders is emphasised by the DSM-5 and in scientific literature (19). It bears noting, that we did not assess clinical distress or disability in detail or by the means of validated instruments specifically developed for this purpose. The 10 criteria for exercise addiction (Table 1) as well the fact that all participants scored above the threshold of the EDS-21 served as our measure for the presence of significant distress, as both instruments formulate items based on the experience of discomfort, distress, and impairment.
Finally, it is important to note that despite meeting and exceeding the EDS-21 cut-off for exercise dependence, we found that in 25% of our sample <5 exercise addiction criteria applied. This is a further indication that self-report questionnaires addressing exercise addiction may need to be redesigned, as numerous (2, 42, 43) studies now suggest that they are not adequate in differentiating between sportspeople and individuals with an addictive disorder.
Depression, Cluster-C personality disorders and other obsessive-compulsive disorders appear to be particularly common in subjects with exercise addiction. Our data therefore provides an indicator that the phenomenon of exercise addiction does co-occur with a variety of mental disorders. Our study shows that the phenomenon of exercise addiction occurs independently of eating disorders and body dysmorphic disorders. Since this is a cross-sectional study, it remains unclear whether symptoms of exercise addiction remain stable over time (and in relation to the respective mental disorders). It is also entirely possible that the observed exercising behaviour resembles a coping-strategy to deal with other psychological conditions or current life circumstances not detected in our interview. To deal with this limitation, exercise addiction symptoms need the be observed over longer periods of time to gather longitudinal data and to investigate the requirement of psychiatric and psychotherapeutic treatment.
Our study has several limitations. First, our sample size was small, which does not allow us to study the potential secondary nature of exercise addiction in different subgroups in more detail. Second, we used a cross-sectional design and are therefore not able to draw conclusions about the stability of symptoms over time. Third, we did not sample a matched control group (e.g., individuals who exercise more than 10 h a week but did not meet the EDS-21 cut-off) and are therefore not able to establish, whether the total number of mental disorders we found is in fact excessive among the population we studied. Finally, we used exercise addiction criteria as proposed in literature to assess exercise addiction severity. However, this scale is not a validated instrument, and its psychometric properties are unknown.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study procedures were carried out in accordance with the Declaration of Helsinki. The study was approved by the Ethikkommission Nordwest- und Zentralschweiz (EKNZ) on May 10th, 2019. All subjects were informed about the study and all provided informed consent.
MM wrote the first draft, conducted clinical interviews, performed statistical analysis, and takes responsibility for the integrity of the data and the accuracy of the data analysis. IS conducted clinical interviews. HS recruited participants and conducted initial screening. FC obtained funding. MW supervised the study. FC and MW designed the study and wrote the protocol. UL and AS revised the manuscript and provided substantial intellectual input. MM, IS, and FC had full access to all data in the study. All authors contributed to and have approved the final manuscript.
Funding for this study was provided by the Gertrud Thalmann Fonds of the University Psychiatric Clinics (UPK) Basel. The funding source was not involved in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Morgan WP. Negative addiction in runners. Phys Sportsmed. (1979) 7:55–77. doi: 10.1080/00913847.1979.11948436
2. Szabo A, Griffiths MD, de La Vega Marcos R, Mervó B, Demetrovics Z. Methodological and conceptual limitations in exercise addiction research. Yale J Biol Med. (2015) 88:303–8.
3. Macfarlane L, Owens G, Cruz BDP. Identifying the features of an exercise addiction: a Delphi study. J Behav Addict. (2016) 5:474–84. doi: 10.1556/2006.5.2016.060
4. Marques A, Peralta M, Sarmento H, Loureiro V, Gouveia É R, Gaspar de. Matos M. Prevalence of risk for exercise dependence: a systematic review. Sports Med. (2019) 49:319–30. doi: 10.1007/s40279-018-1011-4
5. Potenza MN. Non-substance addictive behaviors in the context of DSM-5. Addict Behav. (2014) 39:1–2. doi: 10.1016/j.addbeh.2013.09.004
6. Baekeland F. Exercise deprivation: sleep and psychological reactions. Arch Gen Psychiatry. (1970) 22:365–9. doi: 10.1001/archpsyc.1970.01740280077014
7. Bamber DJ, Cockerill IM, Rodgers S, Carroll D. “It's exercise or nothing”: a qualitative analysis of exercise dependence. Br J Sports Med. (2000) 34:423–30. doi: 10.1136/bjsm.34.6.423
9. Griffiths M. Exercise addiction: a case study. Addict Res. (1997) 5:161–8. doi: 10.3109/16066359709005257
10. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC (2013).
11. Freimuth M, Moniz S, Kim SR. Clarifying exercise addiction: differential diagnosis, co-occurring disorders, and phases of addiction. Int J Environ Res Public Health. (2011) 8:4069–81. doi: 10.3390/ijerph8104069
12. Hausenblas HA, Downs DS. How much is too much? the development and validation of the exercise dependence scale. Psychol Health. (2002) 17:387–404. doi: 10.1080/0887044022000004894
14. Colledge F, Buchner U, Schmidt A, Walter M. Does exercise addiction exist? a brief review on current measurement tools and future directions. Ment Health Addict Res. (2019) 4:1–4. doi: 10.15761/MHAR.1000181
15. Zajac K, Ginley MK, Chang R, Petry NM. Treatments for Internet gaming disorder and Internet addiction: a systematic review. Psychol Addict Behav. (2017) 31:979–94. doi: 10.1037/adb0000315
16. Billieux J, Schimmenti A, Khazaal Y, Maurage P, Heeren A. Are we overpathologizing everyday life? a tenable blueprint for behavioral addiction research. J Behav Addict JBA. (2015) 4:119. doi: 10.1556/2006.4.2015.009
17. Petry NM, Zajac K, Ginley MK. Behavioral addictions as mental disorders: to be or not to be? Annu Rev Clin Psychol. (2018) 14:399–423. doi: 10.1146/annurev-clinpsy-032816-045120
18. Kardefelt-Winther D, Heeren A, Schimmenti A, van Rooij A, Maurage P, Carras M, et al. How can we conceptualize behavioural addiction without pathologizing common behaviours? Addiction. (2017) 112:1709–15. doi: 10.1111/add.13763
19. Stein DJ, Phillips KA, Bolton D, Fulford KW, Sadler JZ, Kendler KS. What is a mental/psychiatric disorder? from DSM-IV to DSM-V. Psychol Med. (2010) 40:1759–65. doi: 10.1017/S0033291709992261
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC (2013).
21. Potenza MN, Balodis IM, Derevensky J, Grant JE, Petry NM, Verdejo-Garcia A, et al. Gambling disorder. Nat Rev Dis Primers. (2019) 5:51. doi: 10.1038/s41572-019-0099-7
22. Petry NM, Stinson FS, Grant BF. Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. (2005) 66:564–74. doi: 10.4088/JCP.v66n0504
23. Kessler RC, Hwang I, LaBrie R, Petukhova M, Sampson NA, Winters KC, et al. DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychol Med. (2008) 38:1351–60. doi: 10.1017/S0033291708002900
24. Colledge F, Cody R, Buchner UG, Schmidt A, Pühse U, Gerber M, et al. Excessive exercise-a meta-review. Front Psychiatry. (2020) 11:521572. doi: 10.3389/fpsyt.2020.521572
25. Colledge F, Sattler I, Schilling H, Gerber M P, rbe U, Walter M. Mental disorders in individuals at risk for exercise addiction–a systematic review. Addict Behav Rep. (2020) 12:100314. doi: 10.1016/j.abrep.2020.100314
26. Cook B, Karr TM, Zunker C, Mitchell JE, Thompson R, Sherman R, et al. Primary and secondary exercise dependence in a community-based sample of road race runners. J Sport Exerc Psychol. (2013) 35:464–9. doi: 10.1123/jsep.35.5.464
27. de Coverley, Veale DM. Exercise dependence. Br J Addict. (1987) 82:735–40. doi: 10.1111/j.1360-0443.1987.tb01539.x
28. Bamber DJ, Cockerill IM, Rodgers S, Carroll D. Diagnostic criteria for exercise dependence in women. Br J Sports Med. (2003) 37:393–400. doi: 10.1136/bjsm.37.5.393
29. Harris N, Gee D. d'Acquisto D, Ogan D, Pritchett K. Eating disorder risk, exercise dependence, and body weight dissatisfaction among female nutrition and exercise science university majors. J Behav Addict. (2015) 4:206–9. doi: 10.1556/2006.4.2015.029
30. Cunningham HE, Pearman III S, Brewerton TD. Conceptualizing primary and secondary pathological exercise using available measures of excessive exercise. Int J Eat Disord. (2016) 49:778–92. doi: 10.1002/eat.22551
31. Grandi S, Clementi C, Guidi J, Benassi M, Tossani E. Personality characteristics and psychological distress associated with primary exercise dependence: an exploratory study. Psychiatry Res. (2011) 189:270–5. doi: 10.1016/j.psychres.2011.02.025
32. Blumenthal JA, Rose S, Chang JL. Anorexia nervosa and exercise. Implications from recent findings. Sports Med. (1985) 2:237–47. doi: 10.2165/00007256-198502040-00001
33. Wegner M, Helmich I, Machado S, Nardi AE, Arias-Carrion O, Budde H. Effects of exercise on anxiety and depression disorders: review of meta- analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets. (2014) 13:1002–14. doi: 10.2174/1871527313666140612102841
34. Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr Res. (2016) 77:42–51. doi: 10.1016/j.jpsychires.2016.02.023
35. De Berardis D, Fornaro M, Orsolini L, Ventriglio A, Vellante F, Di Giannantonio M. Emotional dysregulation in adolescents: implications for the development of severe psychiatric disorders, substance abuse, and suicidal ideation and behaviors. Brain Sci. (2020) 10:591. doi: 10.3390/brainsci10090591
36. De Berardis D, Fornaro M, Orsolini L. Editorial: “No Words for Feelings, Yet!” Exploring Alexithymia, Disorder of Affect Regulation, and the “Mind-Body” Connection. Front Psychiatry. (2020) 11:593462. doi: 10.3389/fpsyt.2020.593462
37. Moran P, Leese M, Lee T, Walters P, Thornicroft G, Mann A. Standardised Assessment of Personality–Abbreviated Scale (SAPAS): preliminary validation of a brief screen for personality disorder. Br J Psychiatry. (2003) 183:228–32. doi: 10.1192/bjp.183.3.228
38. Dowling NA, Cowlishaw S, Jackson AC, Merkouris SS, Francis KL, Christensen DR. The Prevalence of comorbid personality disorders in treatment-seeking problem gamblers: a systematic review and meta-analysis. J Pers Disord. (2015) 29:735–54. doi: 10.1521/pedi_2014_28_168
39. Adkins EC, Keel PK. Does “excessive” or “compulsive” best describe exercise as a symptom of bulimia nervosa? Int J Eat Disord. (2005) 38:24–9. doi: 10.1002/eat.20140
40. Lichtenstein MB, Larsen KS, Christiansen E, Støving RK, Bredahl TVG. Exercise addiction in team sport and individual sport: prevalences and validation of the exercise addiction inventory. Addict Res Theory. (2014) 22:431–7. doi: 10.3109/16066359.2013.875537
41. Corazza O, Simonato P, Demetrovics Z, Mooney R, van de Ven K, Roman-Urrestarazu A, et al. The emergence of Exercise Addiction, Body Dysmorphic Disorder, And Other Image-Related Psychopathological Correlates In Fitness Settings: A Cross Sectional study. PLoS ONE. (2019) 14:e0213060. doi: 10.1371/journal.pone.0213060
42. de la Vega R, Parastatidou IS, Ruíz-Barquín R, Szabo A. Exercise addiction in athletes and leisure exercisers: the moderating role of passion. J Behav Addict. (2016) 5:325–31. doi: 10.1556/2006.5.2016.043
Keywords: exercise addiction, SCID-5, exercise dependence, excessive exercising, behavioural addiction, diagnostic screening
Citation: Meyer M, Sattler I, Schilling H, Lang UE, Schmidt A, Colledge F and Walter M (2021) Mental Disorders in Individuals With Exercise Addiction—A Cross-Sectional Study. Front. Psychiatry 12:751550. doi: 10.3389/fpsyt.2021.751550
Received: 01 August 2021; Accepted: 12 November 2021;
Published: 09 December 2021.
Edited by:
Carlos Roncero, University of Salamanca, SpainReviewed by:
Mary Jo Larson, Brandeis University, United StatesCopyright © 2021 Meyer, Sattler, Schilling, Lang, Schmidt, Colledge and Walter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maximilian Meyer, bWF4aW1pbGlhbi5tZXllckB1cGsuY2g=
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.