 Bjørn Ingulfsvann Hagen
Bjørn Ingulfsvann Hagen Jan Stubberud
Jan Stubberud- 1Department of Research, Lovisenberg Diaconal Hospital, Oslo, Norway
- 2Department of Psychology, University of Oslo, Oslo, Norway
Objective: Information on the long-term effects of cognitive remediation (CR) in major depressive disorder (MDD) is lacking. The present study reports 2-year follow-up data from a previously published randomized controlled trial (RCT) from our research group, comparing Goal Management Training (GMT), a strategy-based CR intervention, to drill-and-practice computerized cognitive training (CCT). In previous work, we found comparable improvements in executive function (EF), in addition to reductions in depressive symptoms, following both GMT and CCT at 6-month follow-up.
Methods: Forty-two participants of the RCT, all diagnosed with MDD, were invited to complete rating-scales pertaining daily-life EF, rumination, and depressive symptoms. Explorative analyses compared the 2-year follow-up with previously published baseline and 6-month follow-up data, using non-parametric statistics. Similarly, GMT and CCT were compared at the 2-year follow-up, and completers were compared with non-completers.
Results: Twenty participants completed the study. Overall, completers (n = 20) and non-completers (n = 22) were similar. There were no significant differences between GMT (n = 11) and CCT (n = 9) for any outcome 2 years post-treatment. Reduction compared to baseline in depressive symptoms and rumination, but not in daily-life EFs, emerged for GMT only.
Conclusions: Findings suggest long-term improvements in mental health following GMT, while improvements in everyday EFs might require additional treatment or maintenance to sustain. Caution is warranted in the interpretation due to the small sample size and high attrition rates.
Introduction
Major depressive disorder (MDD) is a prevalent and debilitating condition that often includes a cyclic course of remission and relapse (1). Deficits in cognitive functions, including executive functions (EFs), are common in MDD, and frequently remain following the alleviation of affective symptoms (2, 3). These deficits, particularly executive dysfunction, negatively impact daily-life functioning and are associated with impaired emotion regulation capacities and increased levels of rumination (4, 5). Accordingly, impairments in EFs represent a risk factor for subsequent relapse and are central to long-term outcomes in MDD (6).
Cognitive remediation (CR) refer to a set of interventions aiming to produce durable and generalizable improvements in cognition, and in broad terms comprise two approaches, that are often combined. In short, drill-and-practice approaches involve exercises to improve cognitive functions, while strategy-based CR aim to promote the application of compensatory strategies in daily life (7). Overall, CR have yielded promising short-term results in MDD (8, 9). A recent meta-analysis including both drill-and-practice- and strategy-based approaches found a moderate effect of CR on cognitive functioning, including EFs, and small effects on depressive symptoms and daily functioning, when compared to non-CR control conditions (7). However, the improvements did not remain at follow-up, even if reassessments have typically been conducted 1–3 months post-treatment. The lack of durable treatment effects could partly be due to the limited number of studies with additional follow-up assessments (7). Furthermore, comparisons of long-term outcomes following drill-and-practice- and strategy-based approaches are lacking.
To our knowledge, only a couple of studies have evaluated the effectiveness of CR beyond 3 months. In a 1-year follow-up of a randomized controlled trial (RCT), Hoorelbeke et al. (10) identified reductions in depressive symptoms and rumination, and improved perceived daily-life EF, in a remitted depressed sample following drill-and-practice CR targeting executive processes. Still, no differences between the groups, a high cognitive load intervention group vs. a low cognitive load control group, emerged. Similarly, in a mixed sample of 153 participants (schizophrenia/schizoaffective disorder, bipolar disorder, depression), including MDD (n = 58), Twamley et al. (11) found improvements in cognitive functioning, depressive symptoms, and multiple measures of daily functioning, 2 years following CR. Interestingly, results were similar for strategy-based CR combined with supported employment and an enhanced supported employment control group (11).
The present study report 2-year follow-up data from a RCT (n = 63) comparing a strategy-based CR intervention for improving EFs, Goal Management Training–GMT (12), with drill-and-practice computerized cognitive training (CCT), in a depression sample. In the RCT performed by our research group, improvements in performance-based measures of EFs and reductions in rumination were observed for both groups, with effects lasting at least 6 months post-treatment (13). At the same time, only participants in the GMT-group reported significant improvements in perceived daily-life EFs and reductions in depressive symptoms between baseline and the 6-month follow-up, even though between-group differences remained non-significant. Overall, these findings align with a recent meta-analysis including various neurocognitive disorders concluding that GMT is moderately effective in improving EFs and aspects of mental health (14). Nevertheless, only one study has reported follow-up analyses more than 2 years following GMT (15). Here, our research group found that improvements following GMT in EF and quality of life at 6-months follow-up, were no longer present at 5-years follow-up (15–17). In a similar vein, the lack of long-term follow-up studies is a limitation in the current literature on CR in MDD and likely represents an obstacle for clinical implementation (7, 9). Hence, the aim of the present study was to evaluate the long-term effects of CR, and concurrently compare a strategy-based approach to a drill-and-practice approach, in this context.
Materials and Methods
Procedures
Participants of the original RCT (clinical.trials.gov identifier NCT03338413) had all received a diagnosis of mild or moderate MDD according to ICD-10 criteria, either as primary- or secondary diagnosis, by a clinical psychologist during outpatient treatment that predated study participation by 0–24 months. No diagnostic reassessment was done prior to participation in either the original study, or at the 2-year follow-up. Additional inclusion criteria were self-reported EF difficulties on a customized telephone interview and being 18–60 years of age. Exclusion criteria included neurological conditions, drug use, lack of proficiency in Norwegian, or severe cognitive problems or mental disorders.
Those who completed the CR and the 6-month follow-up assessment of the original RCT (n = 42) were invited to participate in the present 2-year follow-up study through letters (two letters—an invitation, and a reminder 2 weeks later). Participation involved completing an online questionnaire comprising rating-scales addressing perceived daily-life EF, rumination, and depressive symptoms. The data were collected (November 2020–January 2021) and stored using the Service for Sensitive Data facilities, owned by the University of Oslo. All participants provided written informed consent, electronically signed, and collected using the same platform. A clinical psychologist was available for questions or concerns during participation. The project, including the 2-year follow-up, was approved by the Regional Committee for Medical and Health Research Ethics, South-Eastern Norway (identifier 2017/666).
Interventions
GMT is a manual-based metacognitive CR intervention aiming to improve EFs through teaching compensatory strategies, particularly directed at problem-solving and inhibition capacities (12). Mindfulness techniques for promoting sustained and focused attention are also included (14). In the present study, the training additionally comprised elements of cognitive restructuring of negative thoughts. The CCT consisted of seven exercises from the BrainHQ platform, addressing processing speed, social cognition, and EFs (attention and working memory). Both treatments entailed nine sessions, but the session frequency, treatment duration, group-sizes, and total hours of training differed (GMT = 2 h once a week for 9 weeks, 5–7 participants; CCT = 1 h twice a week for 4.5 weeks, 2–3 participants). See Hagen et al. (13) for a more detailed description of the study.
Measures
Perceived daily-life EF was measured using the 75-item Behavior Rating Inventory of Executive Function—Adult Version–BRIEF-A (18). The BRIEF-A consist of three index scores, the Behavioral Regulation Index (BRI; 30 items, total range = 30–90) and the Metacognition Index (MI; 40 items, total range = 40–120), which are combined to make the Global Executive Composite (GEC; total range = 70–210). The Beck Depression Inventory–BDI (19) was used to measure depressive symptom severity, with respondents indicating on a four-point scale (item range = 0–3; total range: 0–63) the extent to which they have experienced depressive symptoms during the previous week. The total score from the 22-item Ruminative Response Scale–RRS (20) was used to assess rumination (item range = 1–4). The Color-Word Interference Test—condition 4 from the Delis-Kaplan Executive Function System–D-KEFS (21), collected as part of the original RCT, was included as a performance-based measure of EF when comparing completers and non-completers.
Statistical Analyses
Completers and non-completers in the 2-year follow-up were compared, using the non-parametric Mann-Whitney U test, on previously collected data from baseline and the 6-month follow-up using demographic variables, a performance-based measure of EF, and the included outcome variables, in addition to change scores between baseline and the 6-month follow-up. Similarly, GMT and CCT were compared at the 2-year follow-up. For the whole sample, GMT, and CCT, 2-year follow-up data was compared with data from baseline and the 6-month post-treatment using the Wilcoxon signed-rank test.
An additional sensitivity analysis to ascertain the robustness of the conclusion, including all invited participants, was conducted for the BRIEF-A GEC, BDI, and RRS, using a linear mixed model for repeated measures. The model had an unstructured covariance matrix to estimate both within- and between effects. Group, Time, and Group-Time interactions were included as fixed group differences, and the restricted maximum likelihood method was used for estimation. The significance-level was p < 0.05 for all tests.
Results
Twenty participants (GMT, n = 11; CCT, n = 9) completed the 2-year follow-up, totalling 47.6% of the invited participants. Completers did not differ significantly from non-completers for most outcomes, neither at baseline, nor for change scores between baseline and the 6-month follow-up. One exception was that non-completers reported significantly higher levels of rumination at baseline (Table 1).
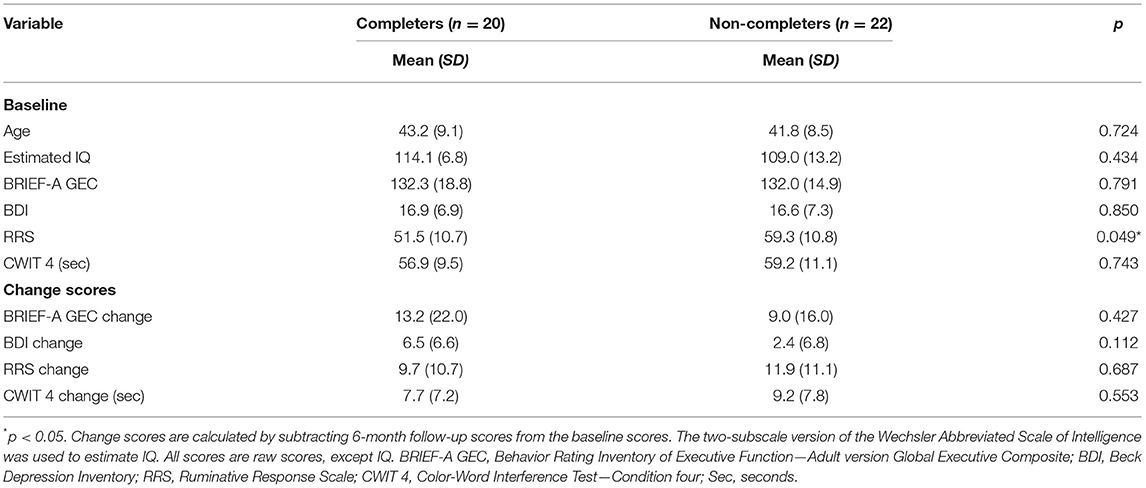
Table 1. Characteristics of completers and non-completers of the 2-year follow-up.
Compared to baseline, whole sample analysis (n = 20) revealed significant improvements in depressive symptoms and rumination, but not in perceived daily-life EF at the 2-year follow-up (Table 2). Similar results emerged for GMT, while no statistically significant changes emerged following CCT. No significant changes emerged for any group between the 6-month follow-up and the 2-year follow-up. Lastly, no significant between-group differences (GMT/CCT) emerged for any outcome at the 2-year follow-up (Table 2), and the sensitivity analysis produced similar results (Table 3). The data from baseline and the 6-month follow-up reported in Tables 1, 3 include subsets of data previously published in Hagen et al. (13).

Table 2. Two-year follow-up outcomes for GMT, CCT, and the whole sample.
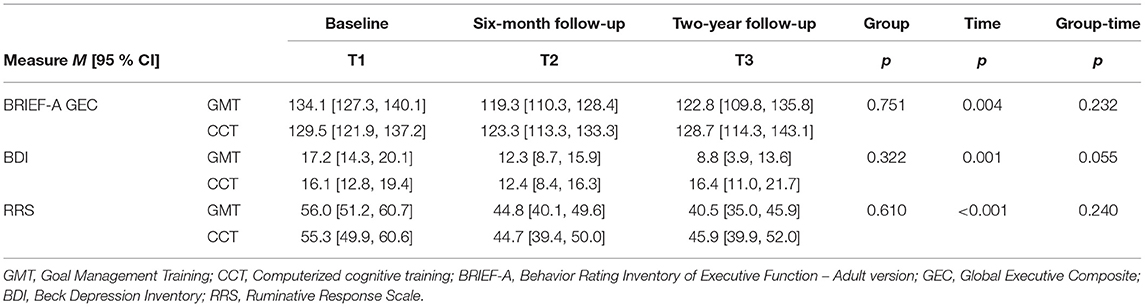
Table 3. Fixed effect estimates from the intention-to-treat linear mixed model sensitivity analysis.
Discussion
The aim of the present study was to evaluate the long-term effectiveness of CR in improving daily-life EF and reducing depressive symptoms and rumination, in MDD. Importantly, the number of non-completers exceeded the cut-offs for when attrition represents a threat to validity, increasing the risk of bias and challenging generalizability (22). Taken together with the small sample size, all statistical analyses should be considered exploratory, and findings are to be interpreted with caution due to the high attrition rates and low statistical power.
In contrast to the recent meta-analysis by Legemaat et al. (7), the present study identified long-term improvements in depressive symptoms, in addition to reduced rumination, following CR. Further, results suggest that these improvements are specific to GMT, and as such provide preliminary support of strategy-based CR being more effective in producing long-term improvements in mental health. Changes in perceived everyday EF did not sustain over the course of years in the present study, like previous evaluations of long-term effects following GMT (15). Concurrently, our findings align with previous research failing to find evidence of different long-term effectiveness between treatments (10, 11). On the other hand, the results are in contrast with Hoorelbeke et al. (10), where durable reductions in daily-life EF difficulties, depressive symptoms, and rumination following drill-and-practice CCT were reported.
The present study highlights the challenges associated with conducting longitudinal clinical studies. There is a need for high-quality reports on long-term effects beyond 6-months, as CR interventions in MDD is yet to provide convincing evidence of durable effects (7). A first step toward this goal is to plan and conduct large-scale studies with adequate statistical power (9, 22). Indeed, the sample sizes in previous research, particularly for interventions requiring considerable therapist involvement, have limited the prospects of conducting long-term follow-ups (7, 8). Steps for optimizing retention could additionally prove useful for attaining valid results over the course of years (23).
Findings from the present study does not indicate that patient characteristics reliably predict retention in CR. Previous research has identified disappointment with the perceived profits from treatment as one of the most common side-effects in CR (24), which may influence the commitment to complete follow-up assessments. Still, our exploratory analyses did not indicate that this was the case as neither self-reported nor performance-based improvement following treatment differed between completers and non-completers.
Limitations
In addition to the concerns related to the sample size, attrition rates, and lack of diagnostic reassessment, the following limitations should be noted. No performance-based measures were applied at the 2-year follow-up, and the study relied on self-report. Importantly, the outcome of the RCT was available to the participants, potentially introducing bias through revealing the active treatment. The GMT and CCT differed in treatment duration and frequency of sessions, challenging the comparison between the two, and the study lacked a no-intervention control group to isolate the effect of Time.
Conclusions
Findings suggest that improvements in mental health remain long-term following GMT, while enhanced daily-life EF might require additional treatment or maintenance (e.g., booster-sessions) to sustain. At the same time, results highlight a potential for increasing the durability of CR treatment effects. Future research should take measures to ensure high-quality results concerning long-term outcomes.
Data Availability Statement
The dataset for this article is not publicly available because of restrictions specified in the study consent-form, and conditions for approval from the local ethics committee, concerning patient confidentiality and participant privacy. Requests to access the data that support the findings of this study should be directed to author JS (ai5lLnN0dWJiZXJ1ZEBwc3lrb2xvZ2kudWlvLm5v).
Ethics Statement
The studies involving human participants were reviewed and approved by Regional Committee for Medical and Health Research Ethics, South-Eastern Norway (identifier 2017/666). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JS and BH contributed to the conceptualization of the study. JS contributed to the funding acquisition and acted as study PI. BH completed data collection, was responsible for data curation, and wrote the original article draft. Both authors contributed with revision of the original article draft and have approved the final manuscript.
Funding
This study was funded by The South-Eastern Norway Regional Health Authority (Grant No. 2019120) and the research fund at Lovisenberg Diaconal Hospital.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mueller TI, Leon AC, Keller MB, Solomon DA, Endicott J, Coryell W, et al. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry. (1999) 156:1000–6.
2. Hasselbalch BJ, Knorr U, Hasselbalch SG, Gade A, Kessing LV. Cognitive deficits in the remitted state of unipolar depressive disorder. Neuropsychology. (2012) 26:642–51. doi: 10.1037/a0029301
3. Semkovska M, Quinlivan L, O'Grady T, Johnson R, Collins A, O'Connor J, et al. Cognitive function following a major depressive episode: a systematic review and meta-analysis. Lancet Psychiatry. (2019) 6:851–61. doi: 10.1016/S2215-0366(19)30291-3
4. Knight MJ, Air T, Baune BT. The role of cognitive impairment in psychosocial functioning in remitted depression. J Affect Disord. (2018) 235:129–34. doi: 10.1016/j.jad.2018.04.051
5. Yang Y, Cao S, Shields GS, Teng Z, Liu Y. The relationships between rumination and core executive functions: A meta-analysis. Depression Anxiety. (2017) 34:37–50. doi: 10.1002/da.22539
6. Saragoussi D, Touya M, Haro JM, Jönsson B, Knapp M, Botrel B, et al. Factors associated with failure to achieve remission and with relapse after remission in patients with major depressive disorder in the PERFORM study. Neuropsychiatric Dis Treatment. (2017) 13:2151–65. doi: 10.2147/NDT.S136343
7. Legemaat AM, Semkovska M, Brouwer M, Geurtsen GJ, Burger H, Denys D, et al. Effectiveness of cognitive remediation in depression: a meta-analysis. Psychol Med. (2021) 14:1–16. doi: 10.1017/S0033291721001100
8. Therond A, Pezzoli P, Abbas M, Howard A, Bowie CR, Guimond S. The efficacy of cognitive remediation in depression: a systematic literature review and meta-analysis. J Affect Disord. (2021) 284:238–46. doi: 10.1016/j.jad.2021.02.009
9. Woolf C, Lampit A, Shahnawaz Z, Sabates J, Norrie LM, Burke D, et al. A systematic review and meta-analysis of cognitive training in adults with major depressive disorder. Neuropsychol Rev. (2021). doi: 10.1007/s11065-021-09487-3. [Epub ahead of print].
10. Hoorelbeke K, van den Bergh N, de Raedt R, Wichers M, Koster E. Preventing recurrence of depression: Long-term effects of a randomized controlled trial on cognitive control training for remitted depressed patients. Clin Psychol Sci. (2021) 9:615–33. doi: 10.1177/2167702620979775
11. Twamley EW, Thomas KR, Burton CZ, Vella L, Jeste Dv, Heaton RK, et al. Compensatory cognitive training for people with severe mental illnesses in supported employment: a randomized controlled trial. Schizophrenia Res. (2019) 203:41–8. doi: 10.1016/j.schres.2017.08.005
12. Levine B, Robertson IH, Clare L, Carter G, Hong J, Wilson BA, et al. Rehabilitation of executive functioning: an experimental–clinical validation of goal management training. J Int Neuropsychol Soc. (2000) 6:299–312.
13. Hagen BI, Lau B, Joormann J, Småstuen MC, Landrø NI, Stubberud J. Goal management training as a cognitive remediation intervention in depression: A randomized controlled trial. J Affect Disord. (2020) 275:268–77. doi: 10.1016/j.jad.2020.07.015
14. Stamenova V, Levine B. Effectiveness of goal management training® in improving executive functions: A meta-analysis. Neuropsychol Rehabil. (2019) 29:1569–99. doi: 10.1080/09602011.2018.1438294
15. Tornås S, Løvstad M, Solbakk A-K, Schanke A-K, Stubberud J. Use it or lose it? A 5-year follow-up study of goal management training in patients with acquired brain injury. J Int Neuropsychol Soc. (2019) 25:1082–87. doi: 10.1017/S1355617719000626
16. Tornås S, Løvstad M, Solbakk A-K, Schanke A-K, Stubberud J. Goal management training combined with external cuing as a means to improve emotional regulation, psychological functioning, and quality of life in patients with acquired brain injury: a randomized controlled trial. Arch Phys Med Rehabil. (2016) 97:1841–52. doi: 10.1016/j.apmr.2016.06.014
17. Tornås S, Løvstad M, Solbakk A-K, Evans J, Endestad T, Hol PK, et al. Rehabilitation of executive functions in patients with chronic acquired brain injury with goal management training, external cuing, and emotional regulation: a randomized controlled trial. J Int Neuropsychol Soc. (2016) 22:436–52. doi: 10.1017/S1355617715001344
18. Roth RM, Isquith PK, Gioia G. Behavioral Rating Inventory of Executive Function-Adult Version Professional manual, Psychological Assessment Resources, Lutz, FL. (2005).
19. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gener Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
20. Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: A psychometric analysis. Cognit Ther Res. (2003) 27:247–59. doi: 10.1023/A:1023910315561
21. Delis DC, Kaplan E, Kramer JH. Delis-Kaplan Executive Function System (D-KEFS) Examiner's Manual. San Antonio, TX: Psychological Corporation (2001).
22. Fewtrell MS, Kennedy K, Singhal A, Martin RM, Ness A, Hadders-Algra M, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dis Childhood. (2008) 93:458–61. doi: 10.1136/adc.2007.127316
23. Kaur M, Sprague S, Ignacy T, Thoma A, Bhandari M, Farrokhyar F. Practical tips for surgical research: how to optimize participant retention and complete follow-up in surgical research. Canad J Surg. (2014) 57:420–7. doi: 10.1503/cjs.006314
Keywords: cognitive remediation, depression, long-term, follow-up, executive function
Citation: Hagen BI and Stubberud J (2021) Goal Management Training and Computerized Cognitive Training in Depression—a 2-Year Follow-Up of a Randomized Controlled Trial. Front. Psychiatry 12:737518. doi: 10.3389/fpsyt.2021.737518
Received: 07 July 2021; Accepted: 31 August 2021;
Published: 24 September 2021.
Edited by:
Preethi Premkumar, London South Bank University, United KingdomReviewed by:
Manju Mehta, All India Institute of Medical Sciences, IndiaPadmavati Ramachandran, Schizophrenia Research Foundation, India
Copyright © 2021 Hagen and Stubberud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jan Stubberud, ai5lLnN0dWJiZXJ1ZEBwc3lrb2xvZ2kudWlvLm5v