
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 06 January 2022
Sec. Psychological Therapy and Psychosomatics
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.724034
This article is part of the Research Topic Recent Advances in Diagnosis and Treatment of Comorbid Conditions in Eating Disorders View all 8 articles
 Daniel J. Devoe1*
Daniel J. Devoe1* Alida Anderson1
Alida Anderson1 Anees Bahji1Manya Singh1
Anees Bahji1Manya Singh1 Scott B. Patten1Andrea Soumbasis1
Scott B. Patten1Andrea Soumbasis1 Ana Ramirez Pineda1
Ana Ramirez Pineda1 Jordyn Flanagan1Candice Richardson2Tom Lange1
Jordyn Flanagan1Candice Richardson2Tom Lange1 Gina Dimitropoulos1,2†
Gina Dimitropoulos1,2† Georgios Paslakis3†
Georgios Paslakis3†Aim: Individuals with eating disorders (EDs) may present with impulse control disorders (ICDs) and behavioral addictions (BAs), which may result in additional suffering and treatment resistance. However, the prevalence of ICDs and BAs in EDs has not been systematically examined. Therefore, this systematic review and meta-analysis aimed to assess the prevalence of ICDs and BAs in ED samples.
Methods: A comprehensive electronic database search of the peer-reviewed literature was conducted in the following online databases: MEDLINE, PsycINFO, Embase, and CINAHL from their inception to May 2021. We restricted review eligibility to research studies reporting prevalence for ICDs or BAs in individuals with diagnosed EDs. The outcome for this review was the prevalence of ICDs or BAs in individuals with EDs. A series of random-effects meta-analyses were performed on eligible studies to estimate the pooled proportions and 95% confidence intervals (CIs).
Results: Thirty-five studies met the inclusion criteria, including a total of 9,646 individuals identified as having an ED, 18 of these studies specifically examined ICDs/BAs in AN, BN, and BED. Random-effects pooled estimates demonstrated that the comorbid prevalence of any ICD was 22%. The prevalence of comorbid pathological/compulsive buying was highest (19%), followed by kleptomania (18%), pathological internet use (12%), intermittent explosive disorder (4%), trichotillomania (3%), and gambling disorder (2%). In addition, the prevalence of stealing/shoplifting behaviors was 30% in those with EDs.
Conclusion: This is the first meta-analysis on the comorbid prevalence of EDs and ICDs/BAs. We found a moderate prevalence for these comorbid conditions, with approximately one out of five individuals with an ED also displaying a comorbid ICD/BA. Although causal inferences cannot be drawn, the numbers strongly suggest that clinical screening/monitoring of ICDs/BAs should be part of the clinical routine in cohorts with EDs. ED settings need either the capacity to manage these disorders or adequate access to relevant services. Further investigations are needed to reveal common underlying pathomechanisms.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42020202044.
Eating disorders (EDs) are severe and life-threatening psychiatric conditions with significant medical (e.g., cardiovascular, renal, and gastrointestinal) and psychological consequences that include an increased risk of suicide (1–4). EDs involve using restrictive or purging behaviors to regulate one's eating or to control weight and to manage negative attitudes and body image distortions (5). The most common EDs are anorexia nervosa (AN), bulimia nervosa (BN), and binge eating disorder (BED) (6). Still, they can also encompass other specified feeding and eating disorders, such as avoidant restrictive food intake disorder, pica, and rumination disorder. The lifetime prevalence of EDs in the general population has been reported to be as high as 5% (7–9), with a lower lifetime prevalence reported for AN (0.6%), 1.0% for BN, and a higher lifetime prevalence of 2.8% for BED (10). Furthermore, EDs incur high healthcare costs (2) and are associated with greater healthcare utilization, high rates of hospitalization, and increased emergency department visits (11).
Impulse control disorders (ICDs), characterized by repetitive or compulsive behaviors with negative consequences, stem from the inability to resist impulses or urges before engaging in the behavior or deriving a sense of gratification from engaging in the behavior (12). ICD subtypes are numerous and include gambling disorder, kleptomania, pyromania, compulsive sexual disorder, and intermittent explosive disorder (13). Closely related to ICDs are a subset of conditions known as Behavioral Addictions (BAs), described as sharing features with ICDs and substance use disorders (14). BAs refer to an addiction of a behavioral component rather than the ingestion of a substance with psychoactive properties (15) and currently include Gambling Disorder and Internet Gaming Disorder in the DSM-5. However, other known presentations of BAs are not represented in the DSM-5 yet are extensively explored in the literature, including technological addiction, sex addiction, compulsive buying, and work addiction (16). Similar to EDs, prevalence estimates of ICDs and BAs across the lifespan are high, ranging from 0.6 to 11.1% (17) and 1.2 to 8% (18, 19) across diagnostic categories for ICDs and BAs, respectively.
Research has focused on EDs and comorbid conditions in the past two decades to examine how concomitant disorders have influenced the illness course and pathways to and participation in treatment. Current estimates suggest that up to 70% of individuals with EDs have psychiatric comorbidities (20), including mood and anxiety disorders, personality disorders, and substance use disorders (5, 21). The presence of psychiatric comorbidities in EDs are costly, which may be associated with longer lengths of stay in treatment programs, higher dropout rates from programs, and poorer treatment outcomes, and tend to be mostly higher in individuals with severe and enduring EDs (20, 22). Hence, also the comorbidity between EDs and ICDs has been examined.
EDs are postulated to share similar personality profiles and neurobiological mechanisms contributing to the etiology and psychopathology of these disorders, such as emotional dysregulation, personality traits like high levels of novelty seeking and high levels of sensitivity to punishment and reward, and compulsivity. Research demonstrates that individuals with EDs present with higher rates of impulsivity and impulsive behaviors, including self-injury, substance use, stealing, and unsafe sexual practices (3, 12, 23–30). Similarly, EDs (particularly those with Bulimia Nervosa) and other BAs such as compulsive buying and gambling disorder share a propensity for impulsivity; for example, adults with compulsive buying have been shown to exhibit higher symptomatology of BN and BED compared to healthy controls (31), sharing low levels of inhibitory and activation control (32). Furthermore, individuals who present with comorbidities of EDs and BAs show a higher burden of general psychopathology and higher novelty-seeking (33). Other studies demonstrate changes in reward centers of the brain, e.g., in ventral striatal activity (34), which are crucial elements to the neurobiological profiles of EDs, ICDs, and BAs (35). There is also substantial empirical evidence supporting frameworks for a dimensional categorization of both behavioral addictions as well as eating disorders on the impulsive-compulsive spectrum (36). Finally, examining the comorbidity of eating disorders and behavioral addictions is important to design and implement novel therapeutic strategies in addition to established treatments (e.g., CBT). Novel strategies may address the above mentioned common underlying vulnerabilities (e.g., impulsivity or emotional dysregulation).
Despite a growing body of literature that demonstrates similarities in the underlying mechanisms and etiology of these disorders, no systematic review or meta-analysis has examined the prevalence, associations, and quality of the literature of studies conducted on ICDs or BAs in those with EDs. Systematic reviews and meta-analyses can explore heterogeneity and pool estimates when differences are due to sampling variability. Therefore, this systematic review and meta-analysis aimed to (1) assess the prevalence of ICDs or BAs in those diagnosed with EDs; (2) assess the prevalence of ICDs or BAs by ED subtype (e.g., AN, BN, and BED), and (3) assess the quality of peer-reviewed literature to date.
This systematic review and meta-analysis was registered with the PROSPERO database of systematic reviews (CRD42020202044). This review followed both the meta-analysis of observational studies in epidemiology (MOOSE) recommendations (37) and the preferred reporting for systematic reviews and meta-analyses (PRISMA) guidelines (38, 39).
A comprehensive electronic database search of the peer-reviewed literature was conducted in the following online databases: MEDLINE, PsycINFO, Embase, and CINAHL from their inception to May 2021. The key words included two concepts: (1) various EDs [i.e., anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), or eating disorders not otherwise specified (EDNOS)] and (2) ICDs/BA (i.e., impulse control disorder total, pathological/compulsive buying, kleptomania, trichotillomania, intermittent explosive disorder, pyromania, pathological/compulsive gambling, technology addictions, and stealing/shoplifting). The electronic database searches and exhaustive list of keywords are provided in the Supplementary Material. Two blinded reviewers (A.A. and A.P.) independently performed title, abstract and full-text article screening using the online Covidence systematic review software (40). The reference lists of included articles were hand-searched for other relevant studies that might meet the inclusion criteria and were not found through online database searching.
Peer-reviewed studies were selected by two reviewers (A.A. and A.P.) for inclusion in this review if they met the following criteria: (1) research including participants with any EDs, anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), or eating disorders not otherwise specified (EDNOS) or reported total EDs, based on any DSM/ICD criteria; (2) reported on ICDs or BAs either clinician reported or self-reported (i.e., impulse control disorder total, pathological/compulsive buying, kleptomania, trichotillomania, intermittent explosive disorder, pyromania, pathological/compulsive gambling, technology addictions, and stealing/shoplifting); (3) reported the prevalence of ICDs or BAs in EDs, (4) contained cross-sectional data for the meta-analysis. In addition, this review excluded studies that: (1) looked at the relationship between EDs and substance abuse disorders; (2) had ineligible study designs such as case reports, review articles, opinion pieces, and editorials; and (3) had insufficient data for the meta-analysis. Disagreements were first discussed in a consensus meeting, and DD made the final decision for inclusion or exclusion.
Data abstraction was completed in duplicate (AA and AS), including the following study characteristics: author, year of publication, country, the control group, total sample size, types of ICDs or BAs, types of EDs, total ED sample size, age (mean ± SD), number of females/percent female, cohort or comparison group description, and outcomes reported. For the meta-analysis, the following data were extracted: (1) author, (2) year of publication, (3) ICDs or BAs type, (4) ED type, (5) numerator representing ICDs or BAs, and (6) the denominator representing EDs or ED subtype.
Studies included in this systematic review and meta-analysis were evaluated for quality using a modified Downs and Black instrument (41) by one author (TL). The modified Downs and Black checklist for cross-sectional studies utilizes 14-items to evaluate the risk of bias and provides a total score out of 15 points for each study. Thus, higher scores indicate greater quality. In addition, this quality assessment checklist contains yes/no questions, which are applied to a series of questions regarding the quality of each study.
Due to the expected heterogeneity between studies, the estimates were initially stratified by ED subgroup, and a series of DerSimonian and Laird (42) random-effects meta-analyses were performed on eligible studies to estimate pooled proportions and 95% CIs for ICDs and BAs for all EDs within those strata. All meta-analyses in this review utilized the Freeman-Tukey double arcsine transformation, which computes the weighted pooled estimate using a variance-stabilizing transformation and then performs a back-transformation on the pooled estimate. This approach is favorable in situations where there is zero count data, as it prevents zero count studies from being dropped from the analyses creating a bias in prevalence estimates. The exact confidence interval method was used as this is considered more conservative. Statistical heterogeneity was calculated utilizing the I2 statistic for subgroup meta-analysis that included four or more studies. All analyses were performed in STATA v.17 (43). To avoid double-counting in the meta-analysis, the data from the largest sample (i.e., denominator) was utilized in the case of two or more studies reporting in the same sample. Forest plots were created showing the proportion of those with either ICDs or BAs in individuals with EDs. Subgroup meta-analyses were used to distinguish the prevalence of ICDs or BAs in EDs types.
Electronic database searches identified 3,310 records; after duplicate references were removed, a total of 2,308 abstracts and titles were screened. The level of agreement between the two reviewers for screening titles and abstracts was moderate (κ = 0.60). After resolution of inconsistencies, a total of 60 studies were retrieved and reviewed in full text. Overall, 35 studies met the inclusion criteria and were included in the meta-analysis, see Figure 1.
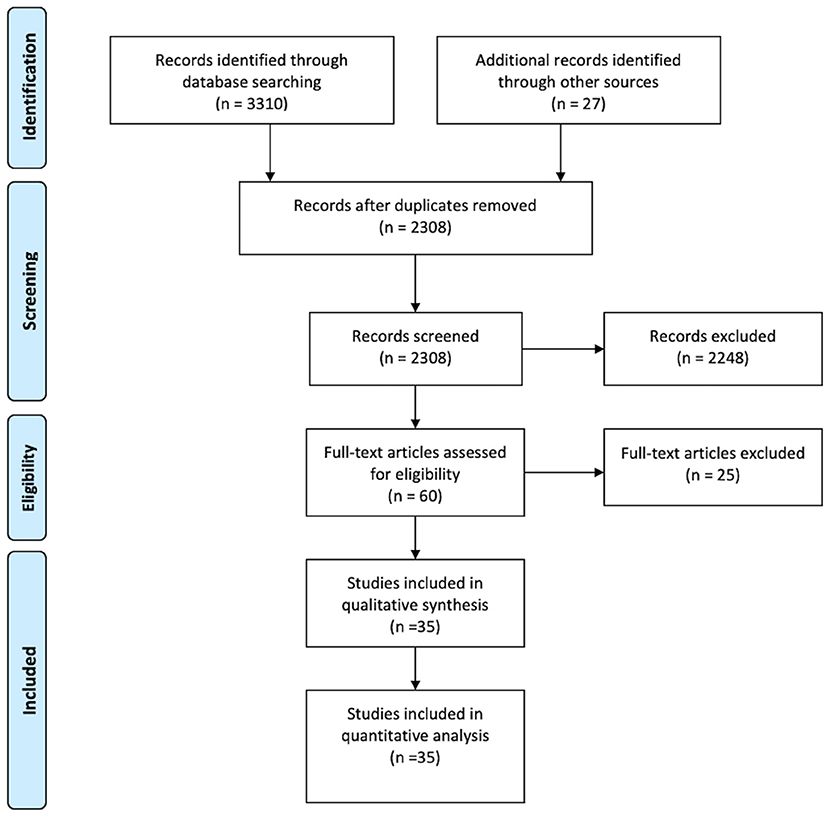
Figure 1. Screening flow diagram.
All studies included in this review are described in detail in Tables 1, 2. Studies were published between 1980 and 2019. Most studies were conducted in North America (n = 14), followed by Europe (n = 13) and Asia (n = 8). Twenty-two studies recruited ED individuals from a hospital setting or a specific eating disorder program, nine were recruited from outpatient clinics, and four were recruited from research study cohorts.
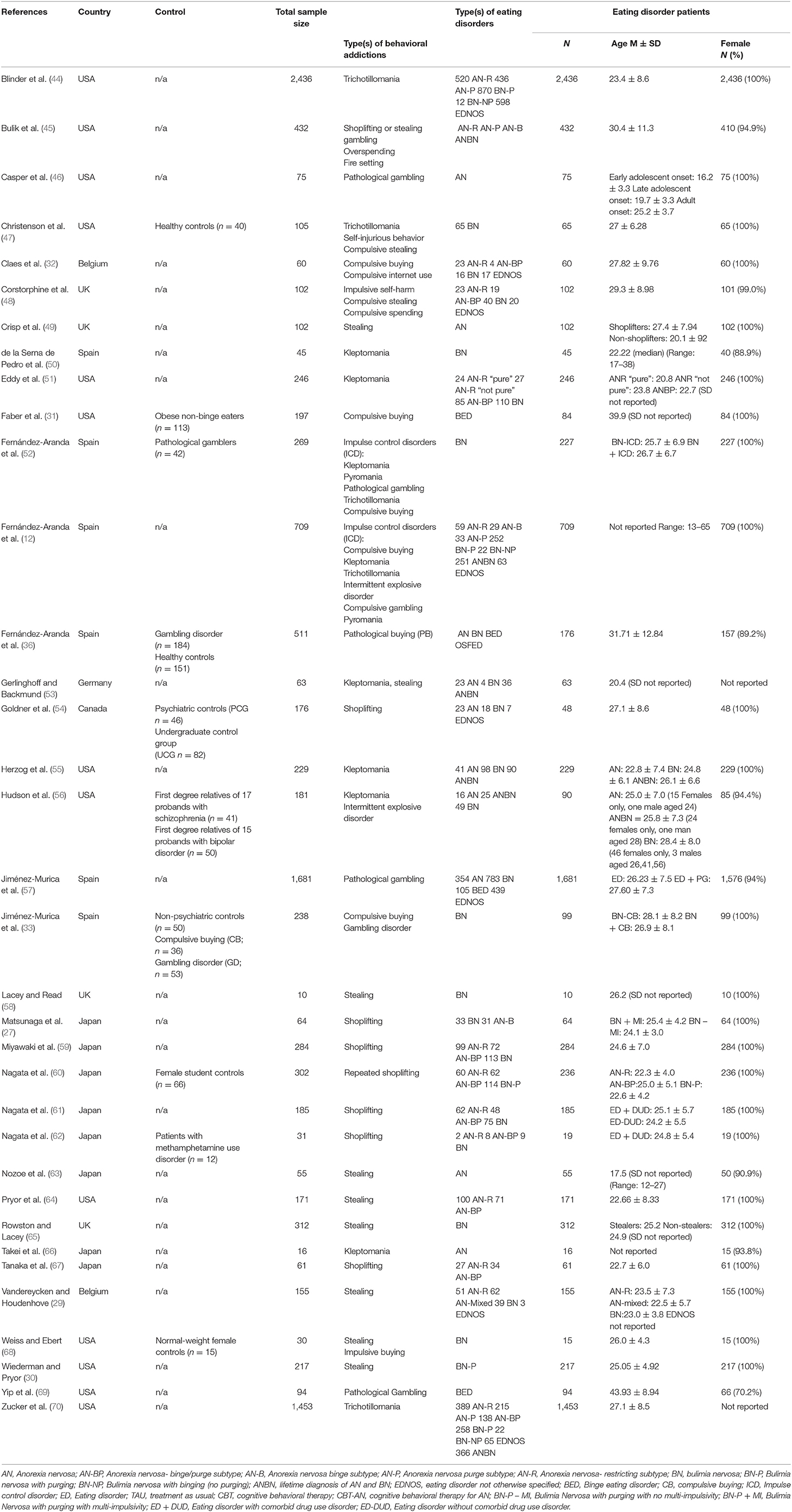
Table 1. Study and participant characteristics of included studies (N = 35).
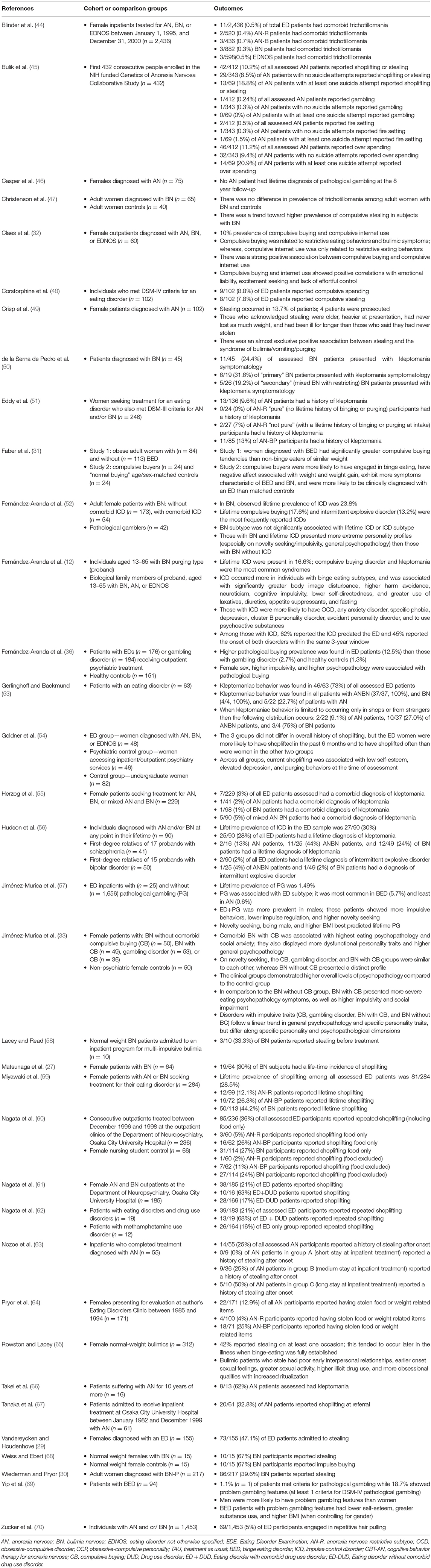
Table 2. Details of eating disorders and behavioral addictions results of included studies (N = 35).
A total of 9,646 individuals were identified as having an ED, ranging from sample sizes of 10 to 2,436 participants with EDs in individual studies. The mean age of individuals with EDs was 25.5 years (range 16.7–43.9), and the percentage of females was 97.7%.
All studies included in this systematic review were evaluated with the modified Downs and Black instrument (Supplementary Table 1). For cross-sectional studies, the average Downs and Black score was 10.4/15, indicating predominantly moderate-quality studies. Although most studies were of moderate quality, several failed to account for the effects of important covariates such as age and gender.
In studies that looked at total ICDs/BAs, random pooled estimates demonstrated a 22% comorbid prevalence in those with EDs (3 studies, N = 1,026), see Figure 2. When examining individual types, pathological/compulsive buying had the highest prevalence at 19% in those with EDs (9 studies, N = 3,338), followed by a 18% prevalence for kleptomania (9 studies, N = 2,997), 4% prevalence for intermittent explosive disorder (3 studies, N = 1,026), 3% prevalence for trichotillomania (5 studies, N = 4,890), and a 2% prevalence for pathological/compulsive gambling (5 studies, N = 2,618). Pyromania did not appear to be prevalent in those with EDs (3 studies, N = 704).
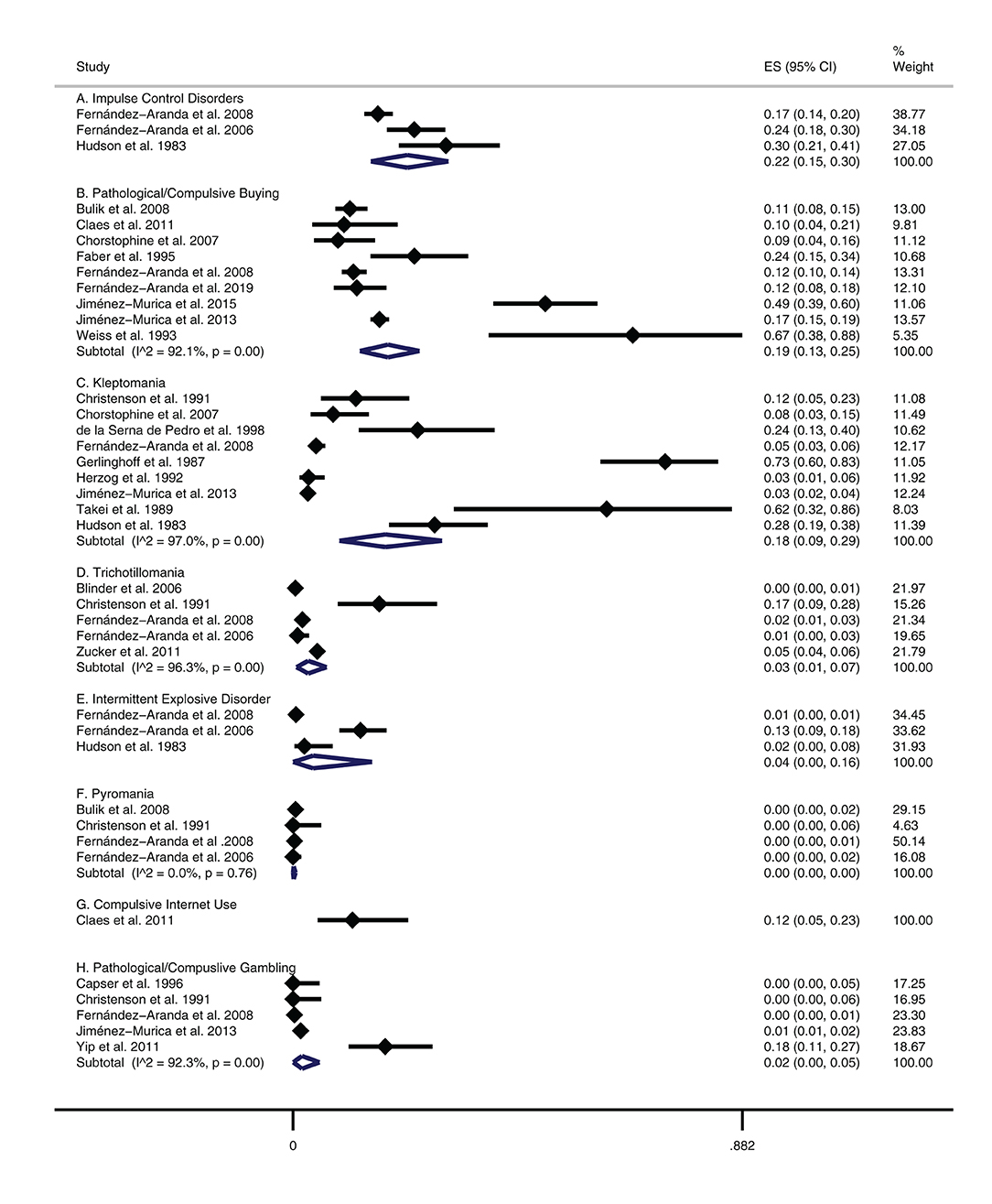
Figure 2. Prevalence of BAs/ICDs in patients with EDs.
In addition, there was a 12% prevalence for compulsive internet use, although this estimate was reported only on a single study and was imprecise (1 study, N = 60). Lastly, random pooled estimates demonstrated that stealing had a prevalence of 30% in those with EDs (13 studies, N = 3,749; see Supplementary Figure 1).
In studies that looked at total ICDs/BAs by ED subtype, there was a 24% prevalence in those with BN (1 study, N = 227), see Supplementary Figure 2. When examining individual ICDs/BAs by ED subtypes, compulsive buying had the highest prevalence at 42% in those with BN (3 studies, N = 341) followed by a 24% prevalence in those with BED (1 study, N = 84), an 11% prevalence in those with AN (1 study, N = 412). Kleptomania had the highest prevalence at 62% among those with AN (1 study, N = 13), followed by 11% among those with BN (3 studies, N = 337).
For individuals with BN, there was a 13% prevalence for intermittent explosive disorder (95% CI = 0.09–0.18; 1 study, N = 227), and a 3% prevalence for trichotillomania (2 studies, N = 292). For BED individuals, there was an 18% prevalence for pathological/compulsive gambling (1 study, N = 94). Neither pathological/compulsive gambling nor pyromania appeared to be prevalent in AN and BN studies.
The prevalence of stealing was 5% in AN-R (2 studies, N = 160), 19% for AN (4 studies, N = 630), 31% for AN-BP [anorexia nervosa binge eating/purging type (2 studies, N = 133), and 45% BN (4 studies, N = 658)], see Supplementary Figure 3.
This systematic review and meta-analysis have contributed to the knowledge base by being the first review to examine the pooled prevalence of comorbid ICDs or BAs in individuals with EDs. Overall, it was estimated that nearly one-quarter (22%) of all people with EDs would experience an ICD at some point during their lives. Most ICDs were more prevalent among individuals with the binge/purge subtype of EDs, such as BN and AN-BP, relative to restrictive EDs, such as AN-R. In addition, roughly one-third (30%) of individuals with ED experienced stealing/shoplifting behaviors. The quality of the literature was rated as being moderate-quality across studies; however, several failed to report and adjust for potential confounders. Overall, we conclude that ICDs are common co-occurring conditions among individuals with EDs, and clinicians should be aware of the frequency of ICDs when providing care for people with EDs.
The prevalence of comorbid ICDs/BAs, 22%, identified in this study closely resembles the prevalence of comorbid substance use disorders (SUDs) identified by a previous meta-analysis. The pooled prevalence was 22% (71). Clinicians must be aware of ICDs since they are associated with worse ED outcomes, particularly if they are undertreated (12, 52). In a similar vein, some personality traits (e.g., perfectionism, impulsivity, cognitive rigidity, and harm avoidance), psychiatric comorbidity, age of onset (e.g., early age of onset may contribute to poor prognosis), concurrent substance use disorders have been proposed as other risk factors that may play a role in deteriorating ED prognoses (72). Most notably, our meta-analysis identified an association between ICD and BN and AN-BP subtype compared to other ED diagnoses and ED behaviors. This supports previous literature indicating that individuals with binge-purge EDs (i.e., BN and AN-B) are more likely to struggle with ICDs, linked to more significant emotion regulation and impulse control difficulties (48, 73, 74).
Although our study did not identify and examine the differences in the comorbid ICDs/BAs ascertainment method, this may have contributed to statistical heterogeneity demonstrated between studies included in this review. For example, the DSM-III, DSM-IV, DSM-5, and the ICD have different specific criteria for other ICDs/Bas (6, 75–78). Furthermore, there are several self-report ED diagnostic instruments, such as the Eating Disorder Inventory (EDI) (79), and semi-structured interviews, such as the Eating Disorder Examination (EDE) (80). However, the reliability of these tools for detecting comorbid ICD/BA comorbidity may differ between studies using self-reported checklists (e.g., Eating Disorder Examination). In addition, individuals with ED often underestimate their impairments compared to informant reports (e.g., the information supplied by persons who are familiar with the patient, such as a supervisor, friend, partner, or family member), resulting in biased ICD/BA prevalence estimates (81, 82). Therefore, the diagnostic reliability could be improved further by incorporating collateral from multiple informants, especially when working with adolescents and young adults (83, 84). However, screening instruments will have a much better positive predictive value when the base rate, or prevalence of the condition, is higher in the population being screened. To that end, as this review provides an estimate of the prevalence of comorbid ICD/BAs, it can inform the best available base rate data for these disorders to date, which can support future epidemiological investigations.
Several studies have attempted to determine psychometrically robust tools for diagnosing comorbid ICDs, but there has generally been a poor correlation between rating scales (85–87). In addition, individuals may conceal the existence of ICDs/BAs due to shame and stigma, adding a layer of complexity to the screening process (88). For example, research has shown that individuals with gambling disorders experience stigma and are often stereotyped as selfish, greedy, or irresponsible, which may cause these individuals to delay help-seeking due to shame (89). Similarly, stigma research in individuals with AN has indicated that they believe the public trivializes their experiences by viewing their behaviors as within their control and by accrediting eating disorder behaviors solely to socio-cultural factors, which delays disclosing their illness (90). It may also be necessary to screen for ICDs and BAs in all EDs rather than EDs with bulimic-type psychopathology alone, as they appear to be comorbid with restrictive AN as well (e.g., pathological buying and kleptomania). As stratification by ED subtypes did not reconcile the heterogeneity in prevalence estimates, this suggests that the different instruments used to measure BAs/ICDs may differ (91–93).
One prospect for implementing and identifying treatment for individuals with these comorbid conditions is understanding the underlying pathophysiology of ICDs/BAs and the co-occurrence of SUDs. For example, both ICDs and BAs are postulated to share similar personality and neurobiological mechanisms (94). For instance, ICDs/BAs may share higher personality traits of impulsivity and sensation-seeking, with lower measures of harm avoidance (15). Furthermore, among women with co-occurring bulimia nervosa and ICDs, lower self-directedness, higher harm avoidance, and cooperativeness appear to be shared across disorders (12). In addition, research suggests that those with EDs and ICDs/BAs share a similar propensity for impulsivity (33, 95) and may have similar deficits in brain reward circuitry (34). Adding to this, it is worth noting that SUDs frequently co-occur with ICDs/BAS with the percentage of comorbid SUDs varying between 15 and 76% depending on the type of ICD/BA (96), and all conditions share similar characteristics of impulsivity. Thus, a transdiagnostic treatment approach targeting impulsivity in these comorbid conditions may help alleviate the burden that these individuals encounter, as there is mounting evidence supporting both pharmacological and behavioral treatments for impulsivity in SUDs (97), which has the potential to translate to efficacious therapies for individuals with EDs and comorbid ICDs/BAs. Finally, another potential option for treating ICDs/BAs in those with EDs is to take a personalized and flexible approach when treating those with EDs who have high levels of impulsivity (98).
There are several strengths of this study. First, to our knowledge, this is the largest systematic review of ICDs among people with EDs and the first meta-analysis. Second, the quality of the majority of studies evaluated was fair. Third, the study was methodologically rigorous, comprehensive, and adhered to the MOOSE guidelines.
However, some limitations should be considered in the appraisal of the evidence presented by this review. One of the most considerable limitations is the limited number of studies available. Consequently, some prevalence estimates only involved one or two studies. Another significant limitation is the high heterogeneity observed across studies for most estimates. There are many potential sources to this heterogeneity, including the wide range of tools used to define ICDs and EDs, the range in study years included in the review, and different classifications of ICDs/BAs. However, a meta-regression was not performed to examine these potential sources of heterogeneity due to the limited number of studies included in the subgroup meta-analyses. While our study identified comorbid ICD diagnoses rather than symptoms, these estimates represent the presence of a clinically significant psychiatric comorbidity, which may be of more relevance to most clinicians. However, ICD/BA symptoms in the absence of a clinical diagnosis can still cause significant functional impairment, primarily if the individual endorses one symptom less than is required for a diagnosis. Furthermore, there may be differential associations between specific ICD/BAs symptoms and ED diagnoses/subtypes undetected in individual studies yet may be detected in a combined sample. As is demonstrated in prior studies and replicated in the current study, the ED symptoms of binge eating and/purging are essential in this association—and perhaps a similar finding exists at the ICD symptom level (74).
While sex proportions were reported in overall samples, sex-specific prevalence estimates were only reported by a subset of studies, precluding extensive sex-based analyses. Due to a gross underrepresentation of males in existing ED literature (99), few identified studies exploring ICD/BA comorbidity in males with ED. Hence, our study may have been underpowered to find sex differences. One meta-analysis of community studies reported the 12-month and lifetime prevalence of EDs as 2.6- and 4.2-fold higher among women than men (100). Conversely, most ICD/BA diagnoses (i.e., pyromania, gambling disorder, intermittent explosive disorder, and oppositional defiant disorder) occur more frequently in men, except for kleptomania, which occurs three times more frequently among women (101, 102). Accordingly, while we found no relevant prevalence estimates of gambling disorder in BN, an ED predominantly diagnosed in women, studies reported an 18% prevalence in BED, an ED characterized by a more balanced woman-to-men ratio. Studies examining gender differences in compulsive buying have yielded mixed results. In a German community sample (103), compulsive buying occurred equally between men and women. However, women in a Spanish community sample showed a higher propensity for compulsive buying (104). Additionally, while upwards of 80% of compulsive buyers seeking treatment are women, this may reflect the notion that women are more likely to recognize and seek help for the problem rather than true differences in prevalence between genders (105). These findings might explain the differences in prevalence for the different types of ICDs/BAs in the current study samples of primarily women (97.8%) with EDs. Another aspect that may explain the differences in prevalence might be that the incidence of ICDs/BAs also tends to vary with age. For example, while oppositional defiant disorder and conduct disorder have the most significant incidence before adolescence (101), intermittent explosive disorder occurs at any point under age 40 (106).
To that end, as this is a study-level meta-analysis, a limitation of the methods is that individual-level characteristics were not explored. There was also a limited representation of studies from all geographic regions, which limited our ability to estimate the prevalence of comorbid ICD/BAs across all continents. There was little information about ICDs/BAs in specific EDs, such as night-eating syndrome, ARFID, or atypical anorexia. Consequently, the overall prevalence estimates presented in the current study are not representative of all individuals with ED, but rather AN, BN, and BED primarily. Finally, as with all meta-analyses, we were limited by the quality and quantity of existent studies, and our results reflect only what is available in terms of existing literature.
Future research is needed to understand better the prevalence of ICD/BAs in subgroups of ED individuals, especially males, children and adolescents, and older adults. Adolescents and young adults are especially important groups regarding ICD/BAs as this age group overlaps with a neurobiologically sensitive period for developing impulse control. This characteristic appears to influence the course of these disorders. Finally, given the bidirectional relationship between ICDs/BAs and EDs, and related conditions (55, 74, 107–110)—such as substance use disorders (SUDs) and personality disorders (PD), future research should examine the corresponding prevalence of these comorbidities in alternative primary populations (e.g., the prevalence of EDs in people with ICDs/BAs). In addition, future studies could examine the bidirectional causation by conducting longitudinal studies that examine EDs and ICDs/BAs. Future research directions might also involve additional studies exploring treatment options for individuals with co-occurring EDs and ICDs/BAs, particularly pharmacological interventions, rTMS, or combining the two with or without concomitant psychotherapies.
This is the first meta-analysis on the comorbid prevalence of EDs and ICDs/BAs. We found a moderate prevalence for these comorbid conditions, with approximately one out of five individuals with an ED also displaying a comorbid ICD/BA, with differences among subtypes. Although causal inferences cannot be drawn, the numbers strongly suggest that clinical screening/monitoring of ICDs/BAs should be part of the clinical routine in cohorts with EDs. ED settings need either the capacity to manage these disorders or adequate access to relevant services. Further investigations are needed to reveal common underlying pathomechanisms.
The raw data supporting the conclusions of this article will be made available by the lead author upon reasonable request.
DD, GD, SP, and GP contributed to conception and design of the study. DD organized the methods and conducted the meta-analysis and wrote the first draft of the manuscript. MS, AB, and GP wrote sections of the manuscript. AA, AS, AR, and JF screened titles, abstracts, and papers. AA, AS, AR, JF, and CR extracted data for tables, figures, and the meta-analysis. All authors contributed to manuscript revision, read, and approved the submitted version.
This work was supported by the O'Brien Institute for Public Health and Mathison Center for Mental Health Post-doctoral Scholarship, University of Calgary Cumming School of Medicine Post-doctoral Scholarship, and the Harley Hotchkiss - Samuel Weiss Postdoctoral Fellowship awarded to DD, the Cuthbertson and Fischer Chair in Pediatric Mental Health awarded to SP, and the Alberta Children's Hospital Foundation and the Alberta Children's Hospital Research Institute via GD.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.724034/full#supplementary-material
1. Crow SJ, Peterson CB, Swanson SA, Raymond NC, Specker S, Eckert ED, et al. Increased mortality in bulimia nervosa and other eating disorders. Am J Psychiatry. (2009) 166:1342–6. doi: 10.1176/appi.ajp.2009.09020247
2. de Oliveira C, Colton P, Cheng J, Olmsted M, Kurdyak P. The direct health care costs of eating disorders among hospitalized patients: a population-based study. Int J Eat Disord. (2017) 50:1385–93. doi: 10.1002/eat.22797
3. Mitchell JE, Crow S. Medical complications of anorexia nervosa and bulimia nervosa. Curr Opin Psychiatry. (2006) 19:438–43. doi: 10.1097/01.yco.0000228768.79097.3e
4. Robinson L, Aldridge V, Clark EM, Misra M, Micali N. A systematic review and meta-analysis of the association between eating disorders and bone density. Osteoporos Int. (2016) 27:1953–66. doi: 10.1007/s00198-015-3468-4
5. Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. (2020) 395:899–911. doi: 10.1016/S0140-6736(20)30059-3
6. American Psychiatric Association. DSM-V: Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: A. P. Association, Ed. (2013).
7. Smink FR, van Hoeken D, Hoek HW. Epidemiology, course, and outcome of eating disorders. Curr Opin Psychiatry. (2013) 26:543–8. doi: 10.1097/YCO.0b013e328365a24f
8. Stice E, Marti CN, Rohde P. Prevalence, incidence, impairment, and course of the proposed DSM-5 eating disorder diagnoses in an 8-year prospective community study of young women. J Abnorm Psychol. (2013) 122:445–57. doi: 10.1037/a0030679
9. Wade TD, Bergin JL, Tiggemann M, Bulik CM, Fairburn CG. Prevalence and long-term course of lifetime eating disorders in an adult Australian twin cohort. Aust N Z J Psychiatry. (2006) 40:121–8. doi: 10.1080/j.1440-1614.2006.01758.x
10. Hudson JI, Hiripi E, Pope HG Jr., Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. (2007) 61:348–58. doi: 10.1016/j.biopsych.2006.03.040
11. Ágh T, Kovács G, Supina D, Pawaskar M, Herman BK, Vokó Z, et al. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat Weight Disord. (2016) 21:353–64. doi: 10.1007/s40519-016-0264-x
12. Fernández-Aranda F, Pinheiro AP, Thornton LM, Berrettini WH, Crow S, Fichter MM, et al. Impulse control disorders in women with eating disorders. Psychiatry Res. (2008) 157:147–57. doi: 10.1016/j.psychres.2007.02.011
13. Grant JE, Chamberlain SR. Expanding the definition of addiction: DSM-5 vs. ICD-11. CNS Spectr. (2016) 21:300–3. doi: 10.1017/S1092852916000183
14. Starcevic V, Khazaal Y. Relationships between behavioural addictions and psychiatric disorders: what is known and what is yet to be learned? Front Psychiatry. (2017) 8:53. doi: 10.3389/fpsyt.2017.00053
15. Grant JE, Potenza MN, Weinstein A, Gorelick DA. Introduction to behavioral addictions. Am J Drug Alcohol Abuse. (2010) 36:233–41. doi: 10.3109/00952990.2010.491884
16. Zilberman N, Yadid G, Efrati Y, Neumark Y, Rassovsky Y. Personality profiles of substance and behavioral addictions. Addict Behav. (2018) 82:174–81. doi: 10.1016/j.addbeh.2018.03.007
17. Dell'Osso B, Altamura AC, Allen A, Marazziti D, Hollander E. Epidemiologic and clinical updates on impulse control disorders: a critical review. Eur Arch Psychiatry Clin Neurosci. (2006) 256:464–75. doi: 10.1007/s00406-006-0668-0
18. Koran LM, Faber RJ, Aboujaoude E, Large MD, Serpe RT. Estimated prevalence of compulsive buying behavior in the United States. Am J Psychiatry. (2006) 163:1806–12. doi: 10.1176/ajp.2006.163.10.1806
19. Villella C, Martinotti G, Di Nicola M, Cassano M, La Torre G, Gliubizzi MD, et al. Behavioural addictions in adolescents and young adults: results from a prevalence study. J Gambl Stud. (2011) 27:203–14. doi: 10.1007/s10899-010-9206-0
20. Keski-Rahkonen A, Mustelin L. Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr Opin Psychiatry. (2016) 29:340–5. doi: 10.1097/YCO.0000000000000278
21. Herpertz-Dahlmann B. Adolescent eating disorders: definitions, symptomatology, epidemiology and comorbidity. Child Adolesc Psychiatr Clin N Am. (2009) 18:31–47. doi: 10.1016/j.chc.2008.07.005
22. Touyz S, Le Grange D, Lacey H, Hay P, Smith R, Maguire S, et al. Treating severe and enduring anorexia nervosa: a randomized controlled trial. Psychol Med. (2013) 43:2501–11. doi: 10.1017/S0033291713000949
23. Solano R, Fernández-Aranda F, Aitken A, López C, Vallejo J. Self-injurious behaviour in people with eating disorders. Eur Eat Disord Rev. (2005) 13:3–10. doi: 10.1002/erv.618
24. Bulik CM, Klump KL, Thornton L, Kaplan AS, Devlin B, Fichter MM, et al. Alcohol use disorder comorbidity in eating disorders: a multicenter study. J Clin Psychiatry. (2004) 65:1000–6. doi: 10.4088/JCP.v65n0718
25. García-Vilches I, Badía-Casanovas A, Fernández-Aranda F, Jiménez-Murcia S, Turón-Gil V, Vallejo-Ruiloba J, et al. Characteristics of bulimic patients whose parents do or do not abuse alcohol. Eat Weight Disord. (2002) 7:232–8. doi: 10.1007/BF03327461
26. Grant JE, Kim SW. Clinical characteristics and associated psychopathology of 22 patients with kleptomania. Compr Psychiatry. (2002) 43:378–84. doi: 10.1053/comp.2002.34628
27. Matsunaga H, Kiriike N, Iwasaki Y, Miyata A, Matsui T, Nagata T, et al. Multi-impulsivity among bulimic patients in Japan. Int J Eat Disord. (2000) 27:348–52. doi: 10.1002/(SICI)1098-108X(200004)27:3<348::AID-EAT13>3.0.CO;2-F
28. Mitchell JE, Fletcher L, Gibeau L, Pyle RL, Eckert E. Shoplifting in bulimia nervosa. Compr Psychiatry. (1992) 33:342–5. doi: 10.1016/0010-440X(92)90042-O
29. Vandereycken W, van Houdenhove VD. Stealing behavior in eating disorders: characteristics and associated psychopathology. Compr Psychiatry. (1996) 37:316–21. doi: 10.1016/S0010-440X(96)90012-7
30. Wiederman MW, Pryor T. Multi-impulsivity among women with bulimia nervosa. Int J Eat Disord. (1996) 20:359–65. doi: 10.1002/(SICI)1098-108X(199612)20:4<359::AID-EAT3>3.0.CO;2-M
31. Faber RJ, Christenson GA, de Zwaan M, Mitchell J. Two forms of compulsive consumption: comorbidity of compulsive buying and binge eating. J Consum Res. (1995) 22:296–304. Available online at: http://www.jstor.org/stable/2489615
32. Claes L, Bijttebier P, Mitchell JE, de Zwaan M, Mueller A. The relationship between compulsive buying, eating disorder symptoms, and temperament in a sample of female students. Compr Psychiatry. (2011) 52:50–5. doi: 10.1016/j.comppsych.2010.05.003
33. Jiménez-Murcia S, Granero R, Moragas L, Steiger H, Israel M, Aymamí N, et al. Differences and similarities between bulimia nervosa, compulsive buying and gambling disorder. Eur Eat Disord Rev. (2015) 23:111–8. doi: 10.1002/erv.2340
34. Fineberg NA, Potenza MN, Chamberlain SR, Berlin HA, Menzies L, Bechara A, et al. Probing compulsive and impulsive behaviors, from animal models to endophenotypes: a narrative review. Neuropsychopharmacology. (2010) 35:591–604. doi: 10.1038/npp.2009.185
35. Balodis IM, Kober H, Worhunsky PD, Stevens MC, Pearlson GD, Potenza MN. Diminished frontostriatal activity during processing of monetary rewards and losses in pathological gambling. Biol Psychiatry. (2012) 71:749–57. doi: 10.1016/j.biopsych.2012.01.006
36. Fernández-Aranda F, Granero R, Mestre-Bach G, Steward T, Müller A, Brand M, et al. Spanish validation of the pathological buying screener in patients with eating disorder and gambling disorder. J Behav Addict. (2019) 8:123–34. doi: 10.1556/2006.8.2019.08
37. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
38. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) 339:b2700. doi: 10.1136/bmj.b2700
39. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement [journal article]. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
41. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Commun Health. (1998) 52:377–84. doi: 10.1136/jech.52.6.377
42. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
44. Blinder BJ, Cumella EJ, Sanathara VA. Psychiatric comorbidities of female inpatients with eating disorders. Psychosom Med. (2006) 68:454–62. doi: 10.1097/01.psy.0000221254.77675.f5
45. Bulik CM, Thornton L, Pinheiro AP, Plotnicov K, Klump KL, Brandt H, et al. Suicide attempts in anorexia nervosa. Psychosom Med. (2008) 70:378–83. doi: 10.1097/PSY.0b013e3181646765
46. Casper RC, Jabine LN. An eight-year follow-up: outcome from adolescent compared to adult onset anorexia nervosa. J Youth Adolesc. (1996) 25:499–517. doi: 10.1007/bf01537545
47. Christenson GA, Mitchell JE. Trichotillomania and repetitive behavior in bulimia nervosa. Int J Eat Disord. (1991) 10:593–98. doi: 10.1002/1098-108X(199109)10:5<593::AID-EAT2260100511>3.0.CO;2-8
48. Corstorphine E, Waller G, Lawson R, Ganis C. Trauma and multi-impulsivity in the eating disorders. Eat Behav. (2007) 8:23–30. doi: 10.1016/j.eatbeh.2004.08.009
49. Crisp AH, Hsu LK, Harding B. The starving hoarder and voracious spender: stealing in anorexia nervosa. J Psychosom Res. (1980) 24:225–31. doi: 10.1016/0022-3999(80)90012-4
51. Eddy KT, Keel PK, Dorer DJ, Delinsky SS, Franko DL, Herzog DB. Longitudinal comparison of anorexia nervosa subtypes. Int J Eat Disord. (2002) 31:191–201. doi: 10.1002/eat.10016
52. Fernández-Aranda F, Jiménez-Murcia S, Álvarez-Moya EM, Granero R, Vallejo J, Bulik CM. Impulse control disorders in eating disorders: clinical and therapeutic implications. Compr Psychiatry. (2006) 47:482–8. doi: 10.1016/j.comppsych.2006.03.002
53. Gerlinghoff M, Backmund H. Stehlen bei Anorexia nervosa und Bulimia nervosa [Stealing in anorexia nervosa and bulimia nervosa]. Fortschr Neurol Psychiatr. (1987) 55:343–46. doi: 10.1055/s-2007-1001837
54. Goldner EM, Geller J, Birmingham CL, Remick RA. Comparison of shoplifting behaviours in patients with eating disorders, psychiatric control subjects, and undergraduate control subjects. Can J Psychiatry. Revue canadienne de psychiatrie. (2000) 45:471–5. doi: 10.1177/070674370004500508
55. Herzog DB, Keller MB, Lavori PW, Kenny GM, Sacks NR. The prevalence of personality disorders in 210 women with eating disorders. J Clin Psychiatry. (1992) 53:147–52.
56. Hudson JI, Pope HG Jr, Jonas JM, Yurgelun-Todd D. Phenomenologic relationship of eating disorders to major affective disorder. Psychiatry Res. (1983) 9:345–54. doi: 10.1016/0165-1781(83)90008-2
57. Jiménez-Murcia S, Steiger H, Isräel M, Granero R, Prat R, Santamaría JJ, et al. Pathological gambling in eating disorders: prevalence and clinical implications. Compr Psychiatry. (2013) 54:1053–60. doi: 10.1016/j.comppsych.2013.04.014
58. Lacey JH, Read TRC. Multi-impulsive bulimia: description of an inpatient eclectic treatment programme and a pilot follow-up study of its efficacy. Eur Eat Disord Rev. (1993) 1:22–ss31. doi: 10.1002/erv.2400010105
59. Miyawaki D, Goto A, Harada T, Yamauchi T, Iwakura Y, Terakawa H, et al. High prevalence of shoplifting in patients with eating disorders. Eat Weight Disord. (2018) 23:761–8. doi: 10.1007/s40519-018-0575-1
60. Nagata T, Kawarada Y, Kiriike N, Iketani T. Multi-impulsivity of Japanese patients with eating disorders: primary and secondary impulsivity. Psychiat Res. (2000) 94:239–50. doi: 10.1016/s0165-1781(00)00157-8
61. Nagata T, Kawarada Y, Ohshima J, Iketani T, Kiriike N. Drug use disorders in Japanese eating disorder patients. Psychiatry Res. (2002) 109:181–91. doi: 10.1016/s0165-1781(02)00007-0
62. Nagata T, Oshima J, Wada A, Yamada H, Kiriike N. Repetitive self-mutilation among Japanese eating disorder patients with drug use disorder: comparison with patients with methamphetamine use disorder. J Nerv Ment Dis. (2003) 191:319–23.
63. Nozoe S, Soejima Y, Yoshioka M, Naruo T, Masuda A, Nagai N, et al. Clinical features of patients with anorexia nervosa: assessment of factors influencing the duration of in-patient treatment. J Psychosom Res. (1995) 39:271–81. doi: 10.1016/0022-3999(94)00141-q
64. Pryor T, Wiederman MW, McGilley B. Clinical correlates of anorexia nervosa subtypes. Int J Eat Disord. (1996) 19:371–9.
65. Rowston WM, Lacey JH. Stealing in bulimia nervosa. Int J Soc Psychiatry. (1992) 38:309–13. doi: 10.1177/002076409203800410
66. Takei M, Nozoe S, Tanaka H, Soejima Y, Manabe Y, Takayama I, et al. Clinical features in anorexia nervosa lasting 10 years or more. Psychother Psychosom. (1989) 52:140–5. doi: 10.1159/000288315
67. Tanaka H, Kiriike N, Nagata T, Riku K. Outcome of severe anorexia nervosa patients receiving inpatient treatment in Japan: an 8-year follow-up study. Psychiatry Clin Neurosci. (2001) 55:389–96. doi: 10.1046/j.1440-1819.2001.00880.x
68. Weiss SR, Ebert MH. Psychological and behavioral characteristics of normal-weight bulimics and normal-weight controls. Psychosom Med. (1983) 45:293–303. doi: 10.1097/00006842-198308000-00004
69. Yip SW, White MA, Grilo CM, Potenza MN. An exploratory study of clinical measures associated with subsyndromal pathological gambling in patients with binge eating disorder. J Gambl Stud. (2011) 27:257–70. doi: 10.1007/s10899-010-9207-z
70. Zucker N, Von Holle A, Thornton LM, Strober M, Plotnicov K, Klump KL, et al. The significance of repetitive hair-pulling behaviors in eating disorders. J Clin Psychol. (2011) 67:391–403. doi: 10.1002/jclp.20770
71. Bahji A, Mazhar MN, Hudson CC, Nadkarni P, MacNeil BA, Hawken E. Prevalence of substance use disorder comorbidity among individuals with eating disorders: a systematic review and meta-analysis. Psychiatry Res. (2019) 273:58–66. doi: 10.1016/j.psychres.2019.01.007
72. Grilo CM, White MA, Masheb RM. DSM-IV psychiatric disorder comorbidity and its correlates in binge eating disorder. Int J Eat Disord. (2009) 42:228–34. doi: 10.1002/eat.20599
73. Bruce KR, Steiger H. Treatment implications of axis-II comorbidity in eating disorders. Eat Disord. (2004) 13:93–108. doi: 10.1080/10640260590893700
74. Dawe S, Loxton NJ. The role of impulsivity in the development of substance use and eating disorders. Neurosci Biobehav Rev. (2004) 28:343–51. doi: 10.1016/j.neubiorev.2004.03.007
75. American Psychiatric Association. DSM-III: Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: A. P. Association, Ed. (1980).
76. American Psychiatric Association. DSM-III-R: Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. A. P. Association, Ed. (1987).
77. American Psychiatric Association. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. 4th ed. A. P. Association, Ed. (1994).
78. Grant JE, Atmaca M, Fineberg NA, Fontenelle LF, Matsunaga H, Janardhan Reddy YC, et al. Impulse control disorders and “behavioural addictions” in the ICD-11. World Psychiatry. (2014) 13:125–7. doi: 10.1002/wps.20115
79. Garner DM, Olmstead MP, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord. (1983) 2:15–34. doi: 10.1002/1098-108X(198321)2:2<15::AID-EAT2260020203>3.0.CO;2-6
80. Thomas JJ, Roberto CA, Berg KC. The Eating Disorder Examination: a semi-structured interview for the assessment of the specific psychopathology of eating disorders. Adv Eat Disord. (2014) 2:190–203. doi: 10.1080/21662630.2013.840119
81. Fairburn CG, Beglin SJ. Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord. (1994) 16:363–70.
82. Rosenman R, Tennekoon V, Hill LG. Measuring bias in self-reported data. Int J Behav Healthcare Res. (2011) 2:320–32. doi: 10.1504/IJBHR.2011.043414
83. Bryant-Waugh R, Micali N, Cooke L, Lawson EA, Eddy KT, Thomas JJ. Development of the Pica, ARFID, and rumination disorder interview, a multi-informant, semi-structured interview of feeding disorders across the lifespan: a pilot study for ages 10–22. Int J Eat Disord. (2019) 52:378–87. doi: 10.1002/eat.22958
84. Hughes EK, Allan E, Le Grange D, Sawyer S. “It depends who you ask”: perceptions of the family environment of adolescents presenting to a specialist eating disorders program. J Eat Disord. (2013) 1:O56. doi: 10.1186/2050-2974-1-S1-O56
85. Lombardo C, Cuzzolaro M, Vetrone G, Mallia L, Violani C. Concurrent validity of the Disordered Eating Questionnaire (DEQ) with the Eating Disorder Examination (EDE) clinical interview in clinical and non clinical samples. Eat Weight Disord. (2011) 16:e188–98. doi: 10.1007/BF03325131
86. Mond JM, Hay PJ, Rodgers B, Owen C, Beumont PJV. Validity of the eating disorder examination questionnaire (EDE-Q) in screening for eating disorders in community samples. Behav Res Ther. (2004) 42:551–67. doi: 10.1016/S0005-7967(03)00161-X
87. Rosen JC, Vara L, Wendt S, Leitenberg H. Validity studies of the eating disorder examination. Int J Eat Disord. (1990) 9:519–28. doi: 10.1002/1098-108X(199009)9:5andlt;519::AID-EAT2260090507andgt;3.0.CO;2-K
88. Sanchez H, Angus Clark D, Fields SA. The relationship between impulsivity and shame and guilt proneness on the prediction of internalizing and externalizing behaviors. Heliyon. (2019) 5:e02746. doi: 10.1016/j.heliyon.2019.e02746
89. Brown KL, Russell AMT. What can be done to reduce the public stigma of gambling disorder? Lessons from other stigmatised conditions. J Gambling Stud. (2020) 36:23–38. doi: 10.1007/s10899-019-09890-9
90. Dimitropoulos G, Freeman VE, Muskat S, Domingo A, McCallum L. “You don't have anorexia, you just want to look like a celebrity”: perceived stigma in individuals with anorexia nervosa. J Mental Health. (2016) 25:47–54. doi: 10.3109/09638237.2015.1101422
91. Chamberlain SR, Grant JE. Minnesota Impulse Disorders Interview (MIDI): validation of a structured diagnostic clinical interview for impulse control disorders in an enriched community sample. Psychiatry Res. (2018) 265:279–83. doi: 10.1016/j.psychres.2018.05.006
92. Grant JE, Levine L, Kim D, Potenza MN. Impulse control disorders in adult psychiatric inpatients. Am J Psychiatry. (2005) 162:2184–8. doi: 10.1176/appi.ajp.162.11.2184
93. Grant JE, Steinberg MA, Kim SW, Rounsaville BJ, Potenza MN. Preliminary validity and reliability testing of a structured clinical interview for pathological gambling. Psychiatry Res. (2004) 128:79–88. doi: 10.1016/j.psychres.2004.05.006
94. McElroy SL, Keck PE Jr., Pope HG Jr., Smith JM, Strakowski SM. Compulsive buying: a report of 20 cases. J Clin Psychiatry. (1994) 55:242–8.
95. Potenza MN. Non-substance addictive behaviors in the context of DSM-5. Addict Behav. (2014) 39:1–2. doi: 10.1016/j.addbeh.2013.09.004
96. Schreiber L, Odlaug BL, Grant JE. Impulse control disorders: updated review of clinical characteristics and pharmacological management. Front Psychiatry. (2011) 2:1. doi: 10.3389/fpsyt.2011.00001
97. Kozak K, Lucatch AM, Lowe DJE, Balodis IM, MacKillop J, George TP. The neurobiology of impulsivity and substance use disorders: implications for treatment. Ann N Y Acad Sci. (2019) 1451:71–91. doi: 10.1111/nyas.13977
98. Todisco P, Meneguzzo P, Garolla A, Antoniades A, Vogazianos P, Tozzi F. Impulsive behaviors and clinical outcomes following a flexible intensive inpatient treatment for eating disorders: findings from an observational study. Eat Weight Disord Stud Anorexia Bulimia Obes. (2021) 26:869–77. doi: 10.1007/s40519-020-00916-5
99. Limbers CA, Cohen LA, Gray BA. Eating disorders in adolescent and young adult males: prevalence, diagnosis, and treatment strategies. Adolesc Health Med Therap Volume. (2018) 9:111–6. doi: 10.2147/AHMT.S147480
100. Qian J, Hu Q, Wan Y, Li T, Wu M, Ren Z, et al. Prevalence of eating disorders in the general population: a systematic review. Shanghai Arch Psychiatry. (2013) 25:212–23. doi: 10.3969/j.issn.1002-0829.2013.04.003
101. Fariba K, Gokarakonda SB. Impulse Control Disorders. Treasure Island, FL: StatPearls. StatPearls Publishing Copyright 2021, StatPearls Publishing LLC (2021).
102. Hing N, Russell A, Tolchard B, Nower L. Risk factors for gambling problems: an analysis by gender. J Gambl Stud. (2016) 32:511–34. doi: 10.1007/s10899-015-9548-8
103. Mueller A, Mitchell JE, Crosby RD, Gefeller O, Faber RJ, Martin A, et al. Estimated prevalence of compulsive buying in Germany and its association with sociodemographic characteristics and depressive symptoms. Psychiatry Res. (2010) 180:137–42. doi: 10.1016/j.psychres.2009.12.001
104. Otero-López JM, Villardefrancos E. Prevalence, sociodemographic factors, psychological distress, and coping strategies related to compulsive buying: a cross sectional study in Galicia, Spain. BMC Psychiatry. (2014) 14:101. doi: 10.1186/1471-244X-14-101
105. Nicoli de Mattos C, Kim HS, Requião MG, Marasaldi RF, Filomensky TZ, Hodgins DC, et al. Gender differences in compulsive buying disorder: assessment of demographic and psychiatric co-morbidities. PLoS ONE. (2016) 11:e0167365. doi: 10.1371/journal.pone.0167365
106. Rynar L, Coccaro EF. Psychosocial impairment in DSM-5 intermittent explosive disorder. Psychiatry Res. (2018) 264:91–5. doi: 10.1016/j.psychres.2018.03.077
107. Cassin SE, von Ranson KM. Personality and eating disorders: a decade in review. Clin Psychol Rev. (2005) 25:895–916. doi: 10.1016/j.cpr.2005.04.012
108. Nøkleby H. Comorbid drug use disorders and eating disorders—a review of prevalence studies. Nordic Stud Alcoh Drugs. (2012) 29:303–14. doi: 10.2478/v10199-012-0024-9
109. Rosenvinge JH, Martinussen M, Ostensen E. The comorbidity of eating disorders and personality disorders: a meta-analytic review of studies published between 1983 and 1998. Eat Weight Disord EWD. (2000) 5:52–61. doi: 10.1007/BF03327480
Keywords: eating disorders, behavioral addictions, impulse control disorders (ICD), comorbidity, systematic review
Citation: Devoe DJ, Anderson A, Bahji A, Singh M, Patten SB, Soumbasis A, Ramirez Pineda A, Flanagan J, Richardson C, Lange T, Dimitropoulos G and Paslakis G (2022) The Prevalence of Impulse Control Disorders and Behavioral Addictions in Eating Disorders: A Systematic Review and Meta-Analysis. Front. Psychiatry 12:724034. doi: 10.3389/fpsyt.2021.724034
Received: 11 June 2021; Accepted: 23 November 2021;
Published: 06 January 2022.
Edited by:
Susanne Fischer, University of Zurich, SwitzerlandReviewed by:
Paolo Meneguzzo, University of Padua, ItalyCopyright © 2022 Devoe, Anderson, Bahji, Singh, Patten, Soumbasis, Ramirez Pineda, Flanagan, Richardson, Lange, Dimitropoulos and Paslakis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel J. Devoe, ZGphZGV2b2VAdWNhbGdhcnkuY2E=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.