 Shurong Hu1
Shurong Hu1 Caihua Wang
Caihua Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 08 October 2021
Sec. Psychological Therapy and Psychosomatics
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.714057
Mental health is a significant yet overlooked aspect of inflammatory bowel disease (IBD) patient care, with challenges in determining optimal treatments and psychological health resources. The most common psychological conditions in patients with IBD are anxiety and depression. The increased prevalence of these mental disorders appeals to mental screening of each person diagnosed with IBD at initial consultation. There are simple and clinically viable methods available to screen for mental problems. Psychological methods may be as or even more significant as a therapeutic modality. Herein we discuss the three major areas of psychological co-morbidity in IBD: (1) the prevalence and risk factors associated with anxiety and depression disorders for patients with IBD; (2) diagnosis of psychological disorders for patients with IBD; (3) treatment with patients with IBD and mental disorders. The gastroenterologists are encouraged to screen and treat these patients with IBD and mental disorders, which may improve outcomes.
Inflammatory Bowel Diseases (IBD), including Crohn's disease (CD) and ulcerative colitis (UC), are characterized as chronic and relapsing inflammatory disorders with the peak incidence around 20 years of age (1). The incidence and prevalence of IBD are increasing worldwide. In China, the incidence rate of IBD was 1.74 per 100,000 person-years (UC: 1.18 per 100,000; CD: 0.4 per 100,000) (1). The patients with IBD had significant physical, psychosocial, and economic burden related to high risk of adverse health outcomes, including morbidity, hospitalization, surgery, work disability and even mortality (2). Health-related quality of life (HRQoL) is a concept that includes domains related to physical factors (such as natural history of disease and medications), mental factors (such as anxiety and depression), and social factors (such as job status and occupations) (3). Anxiety and depression are the most common psychological disorders for patients with IBD. One recent study showed that patients with IBD and mental health disease generated significantly higher costs compared with patients without mental disorders (4). Psychological disorders in patients with IBD may lead to high risk of relapse and poor treatment compliance. Moreover, systematic literature review suggested that psychiatric treatment may be effective in reducing anxiety and depression disorders, gastrointestinal symptoms and disease activity (5).
It has long been believed that patients with IBD might have psychological illness, including symptoms of common mental disorders and somatization, which may be related to the complex bidirectional interaction via the gut-brain axis (6). In a study of 405 patients with IBD following for 2 years, the authors observed that patients with normal anxiety scores but who were active at baseline had a nearly 6-fold increase in the risk of anxiety symptoms (7). Therefore, the occurrence of anxiety and depression may be related to the manifestations of active intestinal inflammation related to brain-gut axis imbalance (6, 7).
The identified articles for this review used three different electronic databases: MEDLINE, PsychINFO, and EMBASE. The search terms were used: “inflammatory bowel diseases”, “ulcerative colitis”, “Crohn's disease”. The set operator AND was used to combine these terms with the following terms: “anxiety”, “depression”, and “mood disorder” or “mental disorder”. Herein we discuss the three major areas of psychological co-morbidity in IBD: (1) the prevalence and risk factors associated with anxiety and depression disorders for patients with IBD; (2) diagnosis of psychological disorders for patients with IBD; (3) treatment with patients with IBD and mental disorders. The clinicians are encouraged to detect and treat these patients with IBD and mental disorders, which may improve outcomes.
Compared with the general population, patients with IBD had a higher lifetime rate of psychiatric disorders such as anxiety and depression, which were known to have negative impact on the quality of their lives and the severity of disease (8, 9). Recently, in a systemic review and meta-analysis, the authors performed subgroup analyses by gender, disease location and disease activity, country and method used to define anxiety and depression (10). The meta-analysis showed that patients with IBD were exposed to high prevalence of symptoms of anxiety and depression, with approximately one in three patients affected by anxiety symptoms and one in four patients affected by depression symptoms (10). Furthermore, the prevalence of symptoms of anxiety or depression were higher inpatients with active IBD than in patients with inactive disease (10). Another study reported that patients with IBD had 3–5 times more likely to develop anxiety disorders and 2–4 times to develop depression disorders in the lifetime compared with general population (11).There was a Korea nationwide study with 46,707 non-IBD as control and 15,569 patients with IBD who were followed for 6 years, patients with IBD experienced significantly more anxiety (12.2 vs. 8.7%) and depression (8.0 vs. 4.7%) (12). One systematic review showed that patients with IBD had ~15 and 20%prevalence rate of depression and anxiety respectively (13). It was worth mentioning that one population-based study demonstrated that depression and anxiety disorders might precede IBD diagnosis by at least 5 years (14). In another population-based cohort study in Canada, nearly 80% of patients with IBD and anxiety were diagnosed with anxiety more than 2 years before the diagnosis of IBD (11).
By identifying factors related to the development of mental disorders in patients with IBD, it is possible to reverse anxiety and depressive disorders, not only to improve the quality of life, but also to improve the course of the disease. Based on data from the ISSEO cohort studies, factors associated with anxiety and depression disorders were severe disease, disease flares and socioeconomic deprivation (15). The Korea national study demonstrated a higher risk of new onset anxiety among individuals with CD (hazard ratio, 1.63) or UC (hazard ratio, 1.60) compared with matched controls. The risk ratios of depression after diagnosis of CD and UC are 2.09 and 2.00, respectively (12). This phenomenon was also observed in a case-control study in southern England, indicating that the risk of anxiety and depression is highest within 1 year after IBD diagnosis (16). Another prospective longitudinal follow-up conducted in Ontario, Canada showed that patients with abnormal anxiety HADS (Hospital Anxiety and Depression Scale, HADS) scores had higher IBD-related outcomes compared with patients whose anxiety scores did not increase (odds ratio, 3.36) (17). However, no difference was observed in those with abnormal depression HADS scores compared with those without elevated depression scores (odds ratio, 0.43) in IBD-related outcomes (17). Moreover, the results suggested that elevated anxiety HADS scores at baseline was an independent predictor of adverse IBD-related outcomes (17). A study of 204 patients with IBD (103 with UC and 101 with CD) showed that perceived stress was associated with mood disorders in IBD (18). However, in UC, other factors like a new diagnosis of IBD were related to anxiety and stress, while inpatient status and active diseases were related to depression. In CD, the factors such as abdominal pain, lower socioeconomic status were related to anxiety, while increasing age was related to depression (18).
Furthermore, large longitudinal studies had consistently shown more frequent IBD flares and worse disease activity in those with symptoms of anxiety and depression disorders (19). In a cohort of 2,007 patients followed over 9 years from the Swiss, the results showed an association between depressive symptoms and clinical recurrence of IBD (20). In a large longitudinal study of patients with IBD (1,516 with UC and 2,798 with CD) from USA with almost 2 years follow-up, Bharati Kochar et al. found that baseline depression patients with CD have an increased risk of recurrence (risk ratio, RR: 2.3), hospitalization (RR:1.3) or IBD-related surgery (RR:1.3). UC patients with baseline depression also have an increased risk of relapse (RR: 1.6), hospitalization (RR: 1.3), or surgery (RR: 1.8) at follow-up (21).
In conclusion, new onset of disease, disease activity, side effects of medications, stressful life events, inpatient status and lower socioeconomic status can easily affect the mood of one or two types of IBD (22). The increased prevalence of anxiety and depression disorders required a mental screening of each patient with IBD at initial consultation.
Identifying the psychological disorders of patients with IBD at the time of diagnosis or during the course of the disease is highly related to the patient's care, timely initiation of appropriate treatment, or improvement of the outcome of the disease (23, 24). Screening and monitoring the psychological disorders in patients with IBD play significant role in both primary care and specialist settings. Unfortunately, no IBD specific instruments to measure anxiety or depression disorders have been validated to date. Tools developed for common illnesses of depression and anxiety include self-reported or clinician-reported approaches, and structured clinician psychiatric interviews (25). One approach to determine anxiety and depression is to use existing screening measures that have established reliability and effectiveness, which are easy to score and can be coded into electronic medical records. No measure can replace the doctor's judgment, and all positive screenings should be linked to an action plan involving further patient evaluation and treatment (26). It was important that clinicians and researchers understood the strengths and weaknesses of the various screening tools, and were informed about the interpretation of the resultant scores. The questionnaire scales and cutoff used to define presence of patients with symptoms of anxiety or depression were different (10). The detailed characteristics of depression and anxiety symptom scales were described as follows (also listed in Table 1).
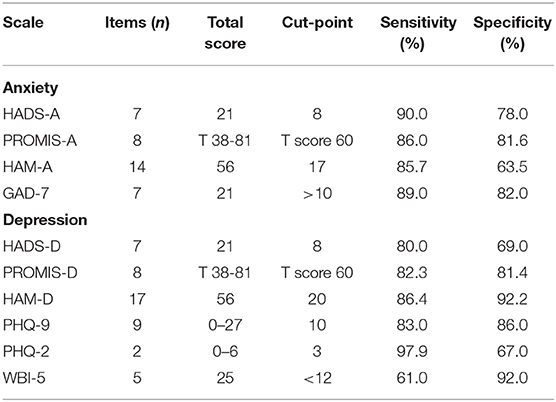
Table 1. A summary of the characteristics of the scales.
The SCID is a semi-structured clinical interview that uses DSM-IV (Diagnostic and Statistical Manual of Mental Disorders IV criteria) to identify mental illness. SCID-based diagnosis can be used as a reference standard for standard validity analysis (14). “SCID depression” refers to any current or lifetime SCID diagnosis of major depression or thymic disorder; “SCID anxiety disorder” refers to any current or lifetime SCID diagnosis of panic disorder (27).
The HADS is a 14-item self-report questionnaire used to assess anxiety (A) and depression (D) levels in the past week (28). Each question is assessed using a 4-point like rt scale and the total score is 42 (21 with depression and 21 with anxiety). And the higher scores, the larger degree of anxiety and depression. It has been extensively studied to describe the prevalence of anxiety and depression in IBD developed for outpatients. The items on the scale are less directly influenced by disease-related symptoms which are different from other scales (18, 29). The cut-point of 8 is used to identify possible anxiety or depression (18, 29). The detection sensitivity and specificity of HADS are 80 and 69% for depression, respectively, and 90 and 78% for anxiety (28). However, HADS-D and HADS-A are the lowest sensitivity relative to other measures.
The PROMIS, including Depression Short-Form 8a (PROMIS Depression) and Anxiety Short-Form 8a (PROMIS Anxiety), is an 8-item self-report questionnaire used to assess the level of anxiety and depression in the past week (30). The American Psychiatric Association has provided guidance on the use of a native scale for PROMIS Anxiety and Depression to identify the severity of psychological distress (31, 32). Among other outcome variables, the PROMIS instrument generates anxiety and depression scores (33). The raw scores for anxiety and depression are translated to standardized T-scores with a population mean of 50 ± 10 (30, 34). Unlike other measures, the PROMIS instruments are based on the item response theory framework to develop item banks, which allow delivery by computer-adaptive testing (33). PROMIS anxiety and depression can detect generalized anxiety screening positive (sensitivity 86.0%; specificity 81.6%) and possible major depression (sensitivity 82.3%; specificity 81.4%) (35). However, scoring PROMIS response patterns for research purposes can be very time-consuming.
Hamilton Anxiety Rating Scale (HAM-A) and Hamilton Depression Rating Scale (HAM-D) are the two oldest tools for assessing anxiety and depression (36, 37). These are scales assessed by clinicians and consist of 14 and 17 items respectively. They are used to assess the severity of patient anxiety and depression, which are the most used anxiety and depression scale assessed by clinicians in the world. Interestingly, the main value of HAM-A and HAM-D is to assess the patient's response to a course of treatment, not a diagnostic or screening tool (39). Through continuous use of the scale, doctors can evaluate the results of medication or psychotherapy (38). The detection sensitivity and specificity of HAM-A are 85.7 and 63.5% for anxiety, and 86.4 and 92.2% for depression, respectively.
The PHQ-9 is a self-administered scale developed by Spitzer et al. for screening depression which is freely available in more than 60 languages (39). The shorter versions without the suicidal item are PHQ-4 and PHQ-2. The total score is 27 and the cut off score for PHQ-9 is 10 (40). The management time of the questionnaire is <5 min. The PHQ scale is a multi-purpose instrument that can also be used to diagnose, monitor and measure the severity of depression (39). The sensitivity and specificity of this scale are 83 and 86%, respectively (41). While the detection sensitivity and specificity of PHQ-2 are 97 and 67% for depression, respectively (42).
The WBI-5 is a short questionnaire consisting of five simple non-invasive questions.
It has sufficient effectiveness in screening depression and measuring the results of clinical trials, and has been successfully applied in a wide range of research fields (43). Currently, WBI-5 has been translated into more than 30 languages and has been used in research projects around the world. The total score is 25, and score <12 is consistent with clinical depression (44). Moreover, the WBI-5 detects depression with 61% insensitivity and 92% in specificity (43).
SCL-A20 is a subscale of Symptom Checklist 90 Revised (SCL90-R) designed by Derogatis LR, which composed of 20 items and is used as a screening tool for anxiety (45). SCL90-R is composed of 90 items and assesses a wide range of mental symptoms, which have been widely used and proven to be reliable. Compared to SCL90-R, SCL-A20 takes a shorter time to administer. The cut off score of SCL-A20 for clinical anxiety is 30.
The GAD-7 is a 7-item self-report questionnaire assessing levels of anxiety over the last 2 weeks, which has demonstrated promise as a scale with good clinical applicability and powerful psychometric characteristics (46). It has demonstrated good reliability and structural validity (47, 48). The total score is 21, and score >10 is consistent with moderate anxiety. Furthermore, GAD-7 has a sensitivity of 89% for GAD and a specificity of 82%, which moderately good at screening panic disorder (sensitivity 74%, specificity 81%), social anxiety disorder (sensitivity 72%, specificity 80%) and post-traumatic stress disorder (sensitivity 66%, specificity 81%), etc., (47, 49). However, GAD-7 may not be able to capture the anxiety associated with anxiety disorders other than generalized anxiety disorder.
Moreover, a study systematically assessed the reliability and validity of multiple symptom rating scales for anxiety and depression in patients with IBD (14). The study showed that the symptom rating scales for anxiety and depression were similar in psychometric attributes. However, the anxiety scale was not as good as the depression scale (14). To be mentioned, most studies on self-reported symptom scales that assess anxiety and depression are conducted in primary care settings, but not in people with chronic diseases (such as IBD) who suffer from depression. The risk of illness and anxiety is particularly high, and the result may be higher (50). However, the accurate screening rate for mental disorders in primary care is estimated to be <50%, and the recognition rate for depression in primary care may be only 3.4% (51–53). Future research will need to determine to what extent the consistent use of the symptom scale in the IBD population will improve the detection of depression and anxiety. Clinicians evaluating patients with IBD should incorporate symptom scales into their practice, provided that when the score exceeds a certain cut-off point for the population, appropriate follow-up actions are available to clarify the background and manage symptoms. Unless we have more precise and standardized tools to quantify the psychological and inflammatory aspects of IBD, the dispute on the link between common mental disorders and IBD may continue. Therefore, clinicians may improve their detection of depression and anxiety through carrying out a symptom scale.
Supporting care that includes medical care and psychosocial, environmental, and behavioral interventions to improve health, which may achieve the highest health value (54). Both anxiety disorders and depression can be treated effectively by pharmacotherapy as well as psychotherapy (Table 2). Psychological therapies should be considered in patients with IBD and functional symptoms (55). Most cases of mental disorders can be successfully treated with behavioral interventions, such as cognitive behavioral therapy (CBT), hypnosis, and mindfulness techniques for patients with and without IBD (56–60). In CBT, CBT has not been studied to continuously change the outcome of the disease, but it can effectively improve medical compliance and underlying symptoms of anxiety or depression (61, 62). CBT is better than usual controls and treatments, but not better than other positive behavioral interventions. Mindfulness meditation programs can regulate pain, anxiety and depression of various physical health diseases (63). Hypnotherapy is a promising adjunctive treatment for IBD and has further proved beneficial for pain and anxiety in non-IBD populations (64, 65). One study demonstrated the effect of 12 hypnotherapy on patients with IBD taking steroids for 5 years, the result showed that 60% patients stopped using steroids after hypnotherapy (66). Although hypnosis is efficacious, there are few behavioral professionals trained in medical hypnosis.
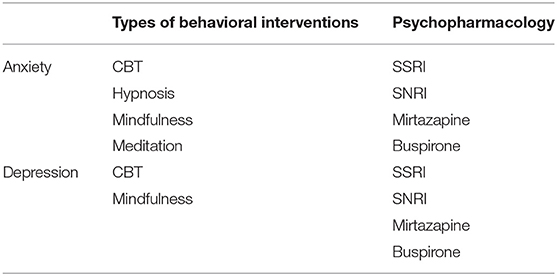
Table 2. The behavioral interventions and psychopharmacology treatment.
Along with psychotherapy, antidepressants have been recognized as treatments for gut–brain disorders that might benefit both psychological and gastrointestinal health (67). Antidepressants have been found to be effective for the treatment of depression, anxiety, and chronic pain syndromes, but the overall support for their efficacy is modest at best. Although there are no large randomized trials for patients with IBD, there is evidence that selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), and tricyclic antidepressants (TCAs) can reduce anxiety and depression psychotherapy when used in combination with the following drugs (68–70).
Several clinical trials have addressed the impact of SSRI treatment on gastrointestinal dysfunction (71). The impact of SSRI on IBD is controversial. Most studies have shown that SSRI treatment has some benefits for patients with IBD, while other studies have failed to prove superior to placebo, especially if patients with depression are excluded from the trial (72, 73). SSRI antidepressants can help relieve symptoms of depression, such as depression, irritability, feelings of worthlessness, irritability, anxiety, and trouble sleeping (74). SSRIs are generally well tolerated. However, like most antidepressants, SSRIs are associated with activation and increased suicidal ideation at higher doses.
SNRIs are a newer category that can block presynaptic serotonin and norepinephrine transporters, thereby increasing the post-synaptic stimulation of these receptors, which may be useful for refractory depression, anxiety, and chronic pain. The symptom is effective, and its side effects are similar to SSRIs and TCAs, with minor side effects (75).
Although TCA may have many serious side effects, TCA has shown some efficacy on functional gastrointestinal symptoms. In the Australian IBD treatment survey, approximately one-third of patients used antidepressants including TCA (69). The most common reason for this prescription is depression or anxiety, but TCA is rarely used for physical illness. A second retrospective study found that high-dose TCA prescribed for depression can reduce disease episodes, endoscopy and steroid use (76).
Mirtazapine is a noradrenergic and specific serotonergic antidepressant (NaSSA) with a variety of unique receptor activities, including blocking postsynaptic 5-HT2 and 5-HT3 receptors, Inhibition of presynaptic α2-adrenergic receptors, potent histamine H1 antagonism and moderate muscarinic receptor antagonism. The patients who did not tolerate SSRI therapy had efficacyfrom50 to 73% when treated with Mirtazapine (77). A study has shown that it is effective in the treatment of IBS, which is dominated by diarrhea and accompanied by depression and anxiety (78). If the side effects of sedation and weight gain can be tolerated, mirtazapine has a moderate effect on depression, and there is some support for the use of nausea and vomiting (68).
Compared with SSRIs, bupropion seems to be more effective in treating drowsiness and fatigue, but has less benefit in depression-related anxiety (73, 79). Bupropion targets the reuptake of dopamine and norepinephrine, has a moderate effect on depression, and has a certain supportive effect on fatigue and smoking cessation (68, 80). Buspirone has indications for generalized anxiety disorder, but studies have shown only small benefits. There is currently more and more evidence to treat functional dyspepsia (68). Unlike benzodiazepines, it has no side effects of physical dependence and cognitive impairment (81, 82).
Most of these drugs have physiological effects on the brain, immune system and gastroenterology (except bupropion), so their treatment and side effects are represented in these systems. In a national study in Denmark, it was found that the use of antidepressants is beneficial to the course of patients with UC and CD, especially those who did not use antidepressants before the onset of IBD (83). A systematic review showed that antidepressant treatment may have a beneficial effect on IBD activity, disease recurrence, IBD-related surgery, quality of life, and treatment compliance (5, 83–85). In the comparison of IBD depression patients who insisted and did not adhere to antidepressant treatment, the IBD activity, depression and anxiety of the patients who insisted on treatment decreased, and the quality of life improved (8). Some studies have shown that patients with IBD are more prone to depression, which can worsen the prognosis of IBD (86). Recently, an analysis of a large retrospective cohort study showed that patients with depression have a significantly higher risk of CD (adjusted HR: 2.11) and UC (adjusted HR: 2.23) (85). In addition, this study showed that SSRIs and TCAs have a protective effect on CD, while mirtazapine, SNRIs, SSRIs, serotonin modulators and TCAs have a protective effect on UC (85). The study showed that depression increases the risk of IBD, and the use of antidepressants during the treatment of depression may reduce this risk.
Psychological conditions like anxiety and depression are common and can affect the quality of life and the course of IBD. The increasing prevalence of these mental illnesses requires that every person diagnosed with IBD be mentally screened during the initial consultation. Therefore, it is necessary and feasible to call for patients with IBD to see a psychologist once a year. There are simple and clinically feasible tools that can be used to screen for psychological problems. Psychological factors are essential for proper IBD management, as there are complex interactions between the physical and emotional health of patients with IBD. Psychological methods may be as important as treatment methods, or even more important. Behavioral interventions can improve outcomes in part by changing relationships, compliance, and preventing recurrence. Antidepressants may have a beneficial effect on IBD activity, disease recurrence, IBD-related surgery, quality of life, and treatment compliance. The comprehensive management method of patients with IBD composed of gastroenterologists and psychiatrists should be included as the standard of care.
CW and YaC: conceptualization. SH: writing - original draft. YiC and CW: writing - review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Li X, Song P, Li J, Tao Y, Li G, Li X, et al. The disease burden and clinical characteristics of inflammatory bowel disease in the Chinese population: A systematic review and meta-analysis. Int J Environ Res Public Health. (2017) 14:238. doi: 10.3390/ijerph14030238
2. Burisch J, Jess T, Martinato M, Lakatos PL. The burden of inflammatory bowel disease in Europe. J Crohn's Colitis. (2013) 7:322–37. doi: 10.1016/j.crohns.2013.01.010
3. Ishak WW, Pan D, Steiner AJ, Feldman E, Mann A, Mirocha J, et al. Patient-reported outcomes of quality of life, functioning, and GI/psychiatric symptom severity in patients with inflammatory bowel disease (IBD). Inflamm Bowel Dis. (2017) 23:798–803. doi: 10.1097/MIB.0000000000001060
4. Szigethy E, Murphy SM, Ehrlich OG, Engel-Nitz NM, Heller CA, Henrichsen K, et al. Mental health costs of inflammatory bowel diseases. Inflamm Bowel Dis. (2021) 27:40–8. doi: 10.1093/ibd/izaa030
5. Tarricone I, Giulia M, Bonucci G, Rizzello F, Carini G, Muratori R, et al. Prevalence and effectiveness of psychiatric treatments for patients with IBD : A systematic literature review. J Psychosom Res. (2017) 101:68–95. doi: 10.1016/j.jpsychores.2017.07.001
6. Gracie DJ, Hamlin PJ, Ford AC. The influence of the brain-gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol Hepatol. (2019) 4:632–42. doi: 10.1016/S2468-1253(19)30089-5
7. Gracie DJ, Guthrie EA, Hamlin PJ, Ford AC. Bi-directionality of brain–gut interactions in patients with inflammatory bowel disease. Gastroenterology. (2018) 54:1635–46.e3. doi: 10.1053/j.gastro.2018.01.027
8. Yanartas O, Kani HT, Bicakci E, Kilic I, Banzragch M, Acikel C, et al. The effects of psychiatric treatment on depression, anxiety, quality of life, and sexual dysfunction in patients with inflammatory bowel disease. Neuropsychiatr Dis Treat. (2016) 12:673–83. doi: 10.2147/NDT.S106039
9. van den Brink G, Stapersma L, Marroun H El, Henrichs J, Szigethy EM, Utens EM, et al. Effectiveness of disease-specific cognitive-behavioural therapy on depression, anxiety, quality of life and the clinical course of disease in adolescents with inflammatory bowel disease: study protocol of a multicentre randomised controlled trial (HAPPY-IBD). BMJ Open Gastroenterol. (2016) 3: e000071. doi: 10.1136/bmjgast-2015-000071
10. Barberio B, Zamani M, Black CJ, Savarino E V, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. (2021) 6:359–70. doi: 10.1016/S2468-1253(21)00014-5
11. Walker JR, Ediger JP, Graff LA, Greenfeld JM, Clara I, Lix L, et al. The Manitoba IBD cohort study: A population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am J Gastroenterol. (2008) 103:1989–97. doi: 10.1111/j.1572-0241.2008.01980.x
12. Choi K, Chun J, Han K, Park S, Soh H, Kim J, et al. Risk of anxiety and depression in patients with inflammatory bowel disease : a nationwide, population-based study. J Clin Med. (2019) 8:654. doi: 10.3390/jcm8050654
13. Neuendorf R, Harding A, Stello N, Hanes D, Wahbeh H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J Psychosom Res. (2016) 87:70–80. doi: 10.1016/j.jpsychores.2016.06.001
14. Bernstein CN, Zhang L, Lix LM, Graff LA, Walker JR, Fisk JD, et al. The validity and reliability of screening measures for depression and anxiety disorders in inflammatory bowel disease. Inflamm Bowel Dis. (2018) 24:1867–75. doi: 10.1093/ibd/izy068
15. Nahon S, Lahmek P, Durance C, Olympie A, Lesgourgues B, Colombel JF, et al. Risk factors of anxiety and depression in inflammatory bowel disease. Inflamm Bowel Dis. (2012) 18:2086–91. doi: 10.1002/ibd.22888
16. Kurina LM, Goldacre MJ, Yeates D, Gill LE. Depression and anxiety in people with inflammatory bowel disease. J Epidemiol Community Health. (2001) 55:716–20. doi: 10.1136/jech.55.10.716
17. Narula N, Pinto-Sanchez MI, Calo NC, Ford AC, Bercik P, Reinisch W, et al. Anxiety but not depression predicts poor outcomes in inflammatory bowel disease. Inflamm Bowel Dis. (2019) 25:1255–61. doi: 10.1093/ibd/izy385
18. Goodhand JR, Wahed M, Mawdsley JE, Farmer AD, Aziz Q, Rampton DS. Mood disorders in inflammatory bowel disease: Relation to diagnosis, disease activity, perceived stress, and other factors. Inflamm Bowel Dis. (2012) 18:2301–9. doi: 10.1002/ibd.22916
19. Mikocka-Walus A, Andrews JM. It is high time to examine the psyche while treating IBD. Nat Rev Gastroenterol Hepatol. (2018) 15:329–30. doi: 10.1038/s41575-018-0004-y
20. Mikocka-Walus A, Pittet V, Rossel JB, von Känel R. Symptoms of Depression and Anxiety Are Independently Associated With Clinical Recurrence of Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. (2016) 14:829–35.e1. doi: 10.1016/j.cgh.2015.12.045
21. Kochar B, Barnes EL, Long MD, Cushing KC, Galanko J, Martin CF, et al. Depression Is associated with more aggressive inflammatory bowel disease. Am J Gastroenterol. (2018) 113:80–5. doi: 10.1038/ajg.2017.423
22. Krishnan V, Nestler EJ. The molecular neurobiology of depression. Nature. (2008) 455:894–902. doi: 10.1038/nature07455
23. Weaver E, Szigethy E. Managing pain and psychosocial care in IBD: a primer for the practicing gastroenterologist. Curr Gastroenterol Rep. (2020) 22:20. doi: 10.1007/s11894-020-0757-7
24. Rozich JJ, Holmer A, Singh S. Effect of lifestyle factors on outcomes in patients with inflammatory bowel diseases. Am J Gastroenterol. (2020) 115:832–40. doi: 10.14309/ajg.0000000000000608
25. Ali GC, Ryan G, De Silva MJ. Validated screening tools for common mental disorders in low and middle income countries: a systematic review. PLoS ONE. (2016) 11:e0156939. doi: 10.1371/journal.pone.0156939
26. Regueiro M, Greer JB, Szigethy E. Etiology and treatment of pain and psychosocial issues. Gastroenterology. (2017) 152:430–9.e4. doi: 10.1053/j.gastro.2016.10.036
27. Lewis K, Marrie RA, Bernstein CN, Graff LA, Patten SB, Sareen J, et al. The prevalence and risk factors of undiagnosed depression and anxiety disorders among patients with inflammatory bowel disease. Inflamm Bowel Dis. (2019) 25:1674–80. doi: 10.1093/ibd/izz045
28. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale: an updated literature review. J Psychosom Res. (2002) 52:69–77. doi: 10.1016/S0022-3999(01)00296-3
29. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
30. Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, et al. The patient-reported outcomes measurement information system (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol. (2010) 63:1179–94. doi: 10.1016/j.jclinepi.2010.04.011
31. Tarescavage AM, Forner EH, Ben-Porath Y. Construct validity of DSM-5 level 2 assessments (PROMIS depression, anxiety, and anger): evidence from the MMPI-2-RF. Assessment. (2021) 28:788–95. doi: 10.1177/1073191120911092
32. McGuire FH, Carl A, Woodcock L, Frey L, Dake E, Matthews DD, et al. Differences in patient and parent informant reports of depression and anxiety symptoms in a clinical sample of transgender and gender diverse youth. LGBT Health. (2021) 8:404–11. doi: 10.1089/lgbt.2020.0478
33. Kroenke K, Yu Z, Wu J, Kean J, Monahan PO. Operating characteristics of PROMIS four-item depression and anxiety scales in primary care patients with chronic pain. Pain Med. (2014) 15:1892–901. doi: 10.1111/pme.12537
34. Pilkonis PA, Choi SW, Reise SP, Stover AM, Riley WT, Cella D, et al. Item banks for measuring emotional distress from the patient-reported outcomes measurement information system (PROMIS®): Depression, anxiety, and anger. Assessment. (2011) 18:263–83. doi: 10.1177/1073191111411667
35. Purvis TE, Neuman BJ, Riley LH, Skolasky RL. Comparison of PROMIS Anxiety and Depression, PHQ-8, and GAD-7 to screen for anxiety and depression among patients presenting for spine surgery. J Neurosurg Spine. (2019) 18:1–8. doi: 10.3171/2018.9.SPINE18521
36. Bech P. Measuring states of anxiety with clinician-rated and patient-rated scales. In: Selek S, editor. Different Views of Anxiety Disorders. IntechOpen (2011). p. 169–84.
37. Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K. Severity classification on the Hamilton depression rating scale. J Affect Disord. (2013) 150:384–8. doi: 10.1016/j.jad.2013.04.028
38. Kummer A, Cardoso F, Teixeira AL. Generalized anxiety disorder and the Hamilton Anxiety Rating Scale in Parkinson's disease. Arq Neuropsiquiatr. (2010) 68:495–501. doi: 10.1590/s0004-282x2010000400005
39. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
40. Manea L, Gilbody S, McMillan D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. CMAJ. (2012) 184:E191–6. doi: 10.1503/cmaj.110829
41. Marc LG, Henderson WR, Desrosiers A, Testa MA, Jean SE, Akom EE. Reliability and validity of the haitian creole PHQ-9. J Gen Intern Med. (2014) 29:1679–86. doi: 10.1007/s11606-014-2951-5
42. Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire-2: Validity of a two-item depression screener. Med Care. (2003) 41:1284–92. doi: 10.1097/01.MLR.0000093487.78664.3C
43. Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 well-being index: A systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
44. Blom EH, Bech P, Högberg G, Larsson JO, Serlachius E. Screening for depressed mood in an adolescent psychiatric context by brief self-assessment scales - testing psychometric validity of WHO-5 and BDI-6 indices by latent trait analyses. Health Qual Life Outcomes. (2012) 10:149. doi: 10.1186/1477-7525-10-149
45. Derogatis LR, Unger R. Symptom Checklist-90-Revised (2010). In: Weiner IB, Craighead WE. The Corsini Encyclopedia of Psychology. Available online at: https://doi.org/10.1002/9780470479216.corpsy0970
46. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
47. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
48. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
49. Swinson RP. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid Based Med. (2006) 11:184. doi: 10.1136/ebm.11.6.184
50. Mitchell AJ. Clinical utility of screening for clinical depression and bipolar disorder. Curr Opin Psychiatry. (2012) 25:24–31. doi: 10.1097/YCO.0b013e32834de45b
51. Sareen J, Stein MB, Campbell DW, Hassard T, Menec V. The relation between perceived need for mental health treatment, DSM diagnosis, and quality of life: A Canadian population-based survey. Can J Psychiatry. (2005) 50:87–94. doi: 10.1177/070674370505000203
52. Weiller E, Bisserbe JC, Maier W, Lecrubier Y. Prevalence and recognition of anxiety syndromes in five European primary care settings. A report from the WHO study on Psychological Problems in General Health Care. Br J Psychiatry. (1998) 34:18–23. doi: 10.1192/S0007125000293471
53. Wittchen HU, Mühlig S, Beesdo K. Mental disorders in primary care. Dialogues Clin Neurosci. (2003) 5:115–28. doi: 10.1159/000079760
54. Szigethy EM, Allen JI, Reiss M, Cohen W, Perera LP, Brillstein L, et al. White paper aga: the impact of mental and psychosocial factors on the care of patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. (2017) 15:986–97. doi: 10.1016/j.cgh.2017.02.037
55. Colombel JF, Shin A, Gibson PR, AGA. Clinical practice update on functional gastrointestinal symptoms in patients with inflammatory bowel disease: expert review. Clin Gastroenterol Hepatol. (2019) 17:380–90. doi: 10.1016/j.cgh.2018.08.001
56. McCombie AM, Mulder RT, Gearry RB. Psychotherapy for inflammatory bowel disease: A review and update. J Crohn's Colitis. (2013) 7:935–49. doi: 10.1016/j.crohns.2013.02.004
57. Szigethy E, Bujoreanu SI, Youk AO, Weisz J, Benhayon D, Fairclough D, et al. Randomized efficacy trial of two psychotherapies for depression in youth with inflammatory bowel disease. J Am Acad Child Adolesc Psychiatry. (2014) 53:726–35. doi: 10.1016/j.jaac.2014.04.014
58. Neilson K, Ftanou M, Monshat K, Salzberg M, Bell S, Kamm MA, et al. A Controlled study of a group mindfulness intervention for individuals living with inflammatory bowel disease. Inflamm Bowel Dis. (2016) 22:694–701. doi: 10.1097/MIB.0000000000000629
59. Gerbarg PL, Jacob VE, Stevens L, Bosworth BP, Chabouni F, Defilippis EM, et al. The effect of breathing, movement, and meditation on psychological and physical symptoms and inflammatory biomarkers in inflammatory bowel disease: a randomized controlled trial. Inflamm Bowel Dis. (2015) 21:2886–96. doi: 10.1097/MIB.0000000000000568
60. Shikatani B, Antony MM, Kuo JR, Cassin SE. The impact of cognitive restructuring and mindfulness strategies on postevent processing and affect in social anxiety disorder. J Anxiety Disord. (2014) 28:570–9. doi: 10.1016/j.janxdis.2014.05.012
61. Mikocka-Walus A, Bampton P, Hetzel D, Hughes P, Esterman A, Andrews JM. Cognitive-behavioural therapy for inflammatory bowel disease: 24-month data from a randomised controlled trial. Int J Behav Med. (2017) 24:127–35. doi: 10.1007/s12529-016-9580-9
62. Mikocka-Walus A, Bampton P, Hetzel D, Hughes P, Esterman A, Andrews JM. Cognitive-behavioural therapy has no effect on disease activity but improves quality of life in subgroups of patients with inflammatory bowel disease: A pilot randomised controlled trial. BMC Gastroenterol. (2015) 15:54. doi: 10.1186/s12876-015-0278-2
63. Goyal M, Singh S, Sibinga EMS, Gould NF, Rowland-Seymour A, Sharma R, et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern Med. (2014) 174:357–68. doi: 10.1001/jamainternmed.2013.13018
64. Keefer L, Keshavarzian A. Feasibility and acceptability of gut-directed hypnosis on inflammatory bowel disease: A brief communication. Int J Clin Exp Hypn. (2007) 55:457–66. doi: 10.1080/00207140701506565
65. Mawdsley JE, Jenkins DG, Macey MG, Langmead L, Rampton DS. The effect of hypnosis on systemic and rectal mucosal measures of inflammation in ulcerative colitis. Am J Gastroenterol. (2008) 103:1460–9. doi: 10.1111/j.1572-0241.2008.01845.x
66. Miller V, Whorwell PJ. Treatment of inflammatory bowel disease: A role for hypnotherapy? Int J Clin Exp Hypn. (2008) 56:306–17. doi: 10.1080/00207140802041884
67. Mikocka-Walus A, Ford AC, Drossman DA. Antidepressants in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. (2020) 17:184–92. doi: 10.1038/s41575-019-0259-y
68. Thorkelson G, Bielefeldt K, Szigethy E. Empirically supported use of psychiatric medications in adolescents and adults with IBD. Inflamm Bowel Dis. (2016) 22:1509–22. doi: 10.1097/MIB.0000000000000734
69. Goodhand JR, Greig FIS, Koodun Y, McDermott A, Wahed M, Langmead L, et al. Do antidepressants influence the disease course in inflammatory bowel disease? A retrospective case-matched observational study. Inflamm Bowel Dis. (2012) 18:1232–9. doi: 10.1002/ibd.21846
70. Cámara RJA, Ziegler R, Begré S, Schoepfer AM, Von Känel R. The role of psychological stress in inflammatory bowel disease: Quality assessment of methods of 18 prospective studies and suggestions for future research. Digestion. (2009) 80:129–39. doi: 10.1159/000226087
71. Ostovaneh MR, Saeidi B, Hajifathalian K, Farrokhi-Khajeh-Pasha Y, Fotouhi A, Mirbagheri SS, et al. Comparing omeprazole with fluoxetine for treatment of patients with heartburn and normal endoscopy who failed once daily proton pump inhibitors: Double-blind placebo-controlled trial. Neurogastroenterol Motil. (2014) 26:670–8. doi: 10.1111/nmo.12313
72. Tabas G, Beaves M, Wang J, Friday P, Mardini H, Arnold G. Paroxetine to treat irritable bowel syndrome not responding to high-fiber diet: A double-blind, placebo-controlled trial. Am J Gastroenterol. (2004) 99:914–20. doi: 10.1111/j.1572-0241.2004.04127.x
73. Papakostas GI, Stahl SM, Krishen A, Seifert CA, Tucker VL, Goodale EP, et al. Efficacy of bupropion and the selective serotonin reuptake inhibitors in the treatment of major depressive disorder with high levels of anxiety (anxious depression): A pooled analysis of 10 studies. J Clin Psychiatry. (2008) 69:1287–92. doi: 10.4088/JCP.v69n0812
74. Fujitsuka N, Asakawa A, Hayashi M, Sameshima M, Amitani H, Kojima S, et al. Selective serotonin reuptake inhibitors modify physiological gastrointestinal motor activities via 5-HT2c receptor and acyl ghrelin. Biol Psychiatry. (2009) 65:748–59. doi: 10.1016/j.biopsych.2008.10.031
75. Thase ME. Are SNRIs more effective than SSRIs? A review of the current state of the controversy. Psychopharmacol Bull. (2008) 41:58–85.
76. Iskandar HN, Cassell B, Kanuri N, Gyawali CP, Gutierrez A, Dassopoulos T, et al. Tricyclic antidepressants for management of residual symptoms in inflammatory bowel disease. J Clin Gastroenterol. (2014) 48:423–9. doi: 10.1097/MCG.0000000000000049
77. Croom KF, Perry CM, Plosker GL. Mirtazapine: A review of its use in major depression and other psychiatric disorders. CNS Drugs. (2009) 23:427–52. doi: 10.2165/00023210-200923050-00006
78. Akama F, Mikami K, Watanabe N, Kimoto K, Yamamoto K, Matsumoto H. Efficacy of mirtazapine on irritable bowel syndrome with anxiety and depression: A case study. J Nippon Med Sch. (2018) 85:330–3. doi: 10.1272/jnms.JNMS.2018_85-53
79. Papakostas GI, Nutt DJ, Hallett LA, Tucker VL, Krishen A, Fava M. Resolution of sleepiness and fatigue in major depressive disorder: a comparison of bupropion and the selective serotonin reuptake inhibitors. Biol Psychiatry. (2006) 60:1350–5. doi: 10.1016/j.biopsych.2006.06.015
80. Jefferson JW, Rush AJ, Nelson JC, VanMeter SA, Krishen A, Hampton KD, et al. Extended-release bupropion for patients with major depressive disorder presenting with symptoms of reduced energy, pleasure, and interest: Findings from a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. (2006) 67:865–73. doi: 10.4088/JCP.v67n0602
81. Lader M, Farr I, Morton S. A comparison of alpidem and placebo in relieving benzodiazepine withdrawal symptoms. Int Clin Psychopharmacol. (1993) 8:31–6. doi: 10.1097/00004850-199300810-00005
82. Lader M, Olajide D. A comparison of buspirone and placebo in relieving benzodiazepine withdrawal symptoms. J Clin Psychopharmacol. (1987) 7:11–5. doi: 10.1097/00004714-198702000-00003
83. Kristensen MS, Kjærulff TM, Ersbøll AK, Green A, Hallas J, Thygesen LC. The influence of antidepressants on the disease course among patients with Crohn's Disease and Ulcerative Colitis - A Danish Nationwide Register-Based Cohort Study. Inflamm Bowel Dis. (2019) 25:886–93. doi: 10.1093/ibd/izy367
84. Macer BJD, Prady SL, Mikocka-Walus A. Antidepressants in Inflammatory Bowel Disease: A Systematic Review. Inflamm Bowel Dis. (2017) 23:534–50. doi: 10.1097/MIB.0000000000001059
85. Frolkis AD, Vallerand IA, Shaheen AA, Lowerison MW, Swain MG, Barnabe C, et al. Depression increases the risk of inflammatory bowel disease, which may be mitigated by the use of antidepressants in the treatment of depression. Gut. (2019) 68:1606–12. doi: 10.1136/gutjnl-2018-317182
Keywords: depression disorders, anxiety disorders, inflammatory bowel disease, psychological treatment, diagnose of psychological disorders
Citation: Hu S, Chen Y, Chen Y and Wang C (2021) Depression and Anxiety Disorders in Patients With Inflammatory Bowel Disease. Front. Psychiatry 12:714057. doi: 10.3389/fpsyt.2021.714057
Received: 17 June 2021; Accepted: 30 August 2021;
Published: 08 October 2021.
Edited by:
Andreas Stengel, Charité – Universitätsmedizin Berlin, GermanyReviewed by:
Andrew S. Day, University of Otago, New ZealandCopyright © 2021 Hu, Chen, Chen and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caihua Wang, d2FuZ2NhaWh1YUB6anUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.