
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 28 July 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.701810
 Izza Mounir1*†
Izza Mounir1*† Loick Menvielle2
Loick Menvielle2 Samir Perlaza3†
Samir Perlaza3† Denis Chênevert4Jo-Hanna Planchard5
Denis Chênevert4Jo-Hanna Planchard5 Roxane Fabre6
Roxane Fabre6 Michel Benoit7
Michel Benoit7 Amine Benyamina8Benjamin Rolland9Faredj Cherikh1†
Amine Benyamina8Benjamin Rolland9Faredj Cherikh1† Renaud David10†
Renaud David10†Background and Aims: This work aims to assess the impact of the COVID-19 pandemic on hospital workers' psychological parameters and attitudes toward substance use, before and during the French COVID-19 lockdown.
Methods: An online survey was proposed to the staff of the University Hospital of Nice and Sainte-Marie psychiatric hospital in France from May 18 to June 6, 2020 assessing changes in daily habits, psychological distress and changes in substance use, including smoking.
Results: A total of 702 respondents (80.3% female) filled out the survey. Overall, most of the workers reported increased stress, irritability, sadness, decreased motivation, and a worse quality of sleep after the beginning of the COVID-19 lockdown. Additionally, hospital workers who were more likely to use tobacco during the COVID-19 lockdown reported increased sadness (OR = 1.23, p < 0.001), loss of motivation (OR = 0.86, p < 0.05), alcohol consumption (OR = 3.12, p < 0.001), lower incomes (OR = 1.69, p < 0.05), living alone (OR = 1.77, p < 0.001) and doing less physical activity (OR = 0.36, p < 0.001).
Conclusion: During the first lockdown, significant psychological changes (sadness, distress, irritability) associated with changes in tobacco use and physical activity were reported. Such results should encourage hospital leaders to implement dedicated policies to better accompany hospital workers' psychological distress.
In March 2020, the World Health Organisation declared the coronavirus disease 2019 (COVID-19) to be a pandemic, one of the most dramatic global tragedies in the twenty-first century. Since then, hospital workers have been overwhelmed, which threatens their physical health (1). In general, public health emergencies affect individuals and communities through different perspectives. Individuals are often subject to anxiety, stress, depression, loneliness, insecurity, confusion, and stigma. Communities are affected by economic losses, social distancing, mobility restrictions, lockdowns, closing businesses and schools, and insufficient resources for appropriate medical service. All these elements together lead to a sequence of emotional reactions and unhealthy behaviors such as distress, psychiatric conditions and excessive substance use (2). These was evidenced during the SARS outbreak in 2003, whose repercussions pursue even years after the epidemic (3, 4). The psychological impact of lockdown during this SARS pandemic induced higher levels of depression (5), irritability and anxiety (6). In the particular case of health care providers, alcohol abuse and dependence symptoms were reported even up to 3 years later. This population self-declared alcohol abuse as a coping strategy and was found significantly related with hyperarousal (7).
These findings ripple through populations affected by the COVID-19 pandemic and pave the way for substance abuse. In China, the psychological impact of COVID-19 is translated into severe anxiety responses present in one third of the general population (8, 9). Other studies in Spain (10), France (11) and Australia (12) reported an increment of symptoms of anxiety, depression, or irritability, which comes often together with significant augmentation of consumption of both alcohol and tobacco; the willingness to practice physical activity; and the quality of sleep.
The first national lockdown in France started on March 17 and ended on May 11, 2020. Unfortunately, the impact of these preventive measures on hospital workers is difficult to assess due to the lack of data. Nonetheless, insufficient supply of tests, limited treatment options, inadequate personal protective equipment and other medical equipment, as well as, prolonged workloads have been observed in most health centers. This may require professional mental health intervention to smooth down long term consequence on hospital workers (2). These psychological distress effects tent to aggravate when lockdowns and other social distancing measures are announced by goverments, c.f., lockdown extensions in Spain (10). In France, the COVID-19 prevention study (13) and the coronavirus and confinement longitudinal survey study (14) highlight the negative impact of the lockdown on the general population in terms of depression and other behaviors such as tobacco use, sleep disorder and weight gain. This reinforces the thesis that worsening the mental health plays a central role in the appearance of harmful lifestyle habits, such as alcohol, tobacco, sleep disorders, low quality diet and deficient physical activity (15, 16).
Within the context of COVID-19 lockdowns, groups with vulnerabilities to psychological distress effects are well identified: healthcare providers (17); people with past somatic diseases or current mental disorders, such as depression, anxiety or bipolar disorder (10); and people with substance use disorders. With the adoption of mobility restrictions and social distancing, usual places promoting physical activity and open-air activities were no longer accessible, which becomes an additional constraint to reduce psychological distress (12, 18).
Since 2014 in France, tobacco control policies have been implemented nationwide. In 2019, 30.4% of French people aged between 18 and 75 declared smoking, from which 24% with daily consumption (19). In the context of the first COVID-19 lockdown in France, our hypothesis is that hospital workers have changed their work habits; tobacco and alcohol use; and have experienced psychological distress, in terms of quality of sleep, motivation, stress, irritability and sadness.
A cross-sectional survey was sent by email to the staff of the University Hospital of Nice and the Sainte-Marie psychiatric hospital, between May and June 2020. The survey was anonymous and compliant with the French general data protection regulation and local laws (20). The population's characteristics are described in Table 1.

Table 1. Participants' characteristics and medical history.
The data was collected via a survey that was divided into three parts. The first part aims to collect information gender, age, current living situation and medical history concerning indicators of increased risk of severe COVID-19 illness [(21); See Table 1]. The second part gathers information about substance use and physical activity. This part also collects self-evaluation data on psychological distress values (sleep, sadness, irritability, motivation, stress) before and after the lockdown in a scale from zero to five. Zero and Five represent, respectively, the lowest and highest scores in sadness, irritability, stress, and motivation. Concerning the quality of sleep, zero and five represent the worse and the best sleep quality, respectively. The third part focuses on tobacco use with a Fagerström Test for Nicotine Dependence (FTND) and the french version of the tobacco craving questionnaire (FTCQ-12) which are valid and reliable self-report instruments (22). The Fagerström test is a six-item scale standard instrument for assessing the intensity of a physical addiction to nicotine with a total score varying from 0 to 10 (23). On the other hand, the FTCQ is a twelve-item scale test designed to assess tobacco craving in four factors: emotional, expectancy, compulsion, and purposefulness (24).
All the respondents (n = 702) were used in this survey, except for the Fagerström Test that concerned only tobacco users (n = 145). Percentages and frequencies, were used for categorical variables. Alternatively, the mean and the SD were used for quantitative variables. In order to test the evolution of the different scores between the period “before lockdown” and the period “after the lockdown,” paired Student's tests were used. The scores follow a Gaussian distribution, the Shapiro statistical test was used for validating this assumption. Tobacco use have been investigated as follows. A Student's t-test was used for the quantitative variables; and a Chi-square test was used for the qualitative variables. A multivariable logistic regression was constructed using the variables with a p-value smaller than 0.150 in univariate. Only variables with a p-value smaller than 0.05 were kept in the final model. Ninety-five percent confidence intervals have been shown. In the multivariable model, adjustment in p-value for multiple comparisons using Holm method was made with the p-adjust function. The analyzes were carried out using software R 3-5-1.
Participants characteristics are described in the Table 1. The population in this research is representative of the one in the University Hospital of Nice given that 74.11% female workers were registered in 2019. From the whole population, 20.7% use tobacco and 16.1% use alcohol. The rate of tobacco use is lower than that observed in the French population (30.4%) aged 18–75 in 2019 but closer to daily tobacco use in France (24%) (19). In our survey, the ratio of alcohol use is also lower than the ratio of French adults in 2018, which is 87% consumption at least once per year and 49% once a week (25). Otherwise, only a few participants had to change their dwelling (4.4%) or went through a decreased income (18.4%) during the first lockdown in France.
Table 1 shows that hospital employees have a lower rate of depression (4.4%) and obesity (7.5%) than the general population in France. More specifically, according to the last survey conducted in 2017, 10% of the population has experienced a depressive episode (26) and 17% of the French population suffered obesity in 2019 (27).
Table 2 underlines the negative impact of the lockdown on tobacco consumption for hospital employees. According to the Fagerström test, it can be concluded that the nicotine dependence had increased up to 24% after the lockdown. Hospital workers who before the lockdown were not considered as dependent or weakly dependent to nicotine became moderately or strongly dependent. More specifically, the moderately dependent population increased from 18.6% to 24.8%, whereas, the strongly dependent population increased from 3.9% to 24.8%.
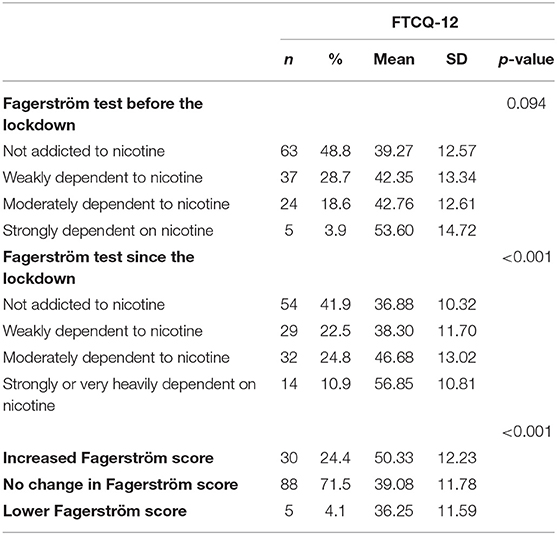
Table 2. Impact of Fagerstöm Test related to the lockdown and correlation to FTCQ-12.
Other studies made in France during the lockdown on the general population showed that tobacco use increased during this period. The results of this research are consistent with the french national public health agency's survey that found around a quarter of smokers (27%) had increased their tobacco consumption. Rossinot et al. (11) found that the proportion of participants who increased their consumption doubles the proportion of those who decreased it. Rolland et al. (28) reported more increases in addiction-related habits than decreases. More specifically, 35.6% of the population augmented tobacco use, from which 26.72% declared having moderately augmentation; and 8.92% declared an augmentation in a difficult-to-control manner.
To evaluate nicotine dependence with cravings, correlations between the Fagerström test and the French version of the Tobacco Craving Questionnaire (FTCQ-12) are presented in Table 2. There are no significant differences before the lockdown on nicotine dependence and tobacco craving (p = 0.094). After the lockdown, significantly (p < 0.001) higher tobacco craving scores (FTCQ-12) are observed for moderately nicotine-dependent individuals (mean = 46.68, SD = 13.02) compared to non-dependent individuals on nicotine (mean = 36.88, SD = 10.32). This implies a strong relation between a higher tobacco craving and increased scores on Fagerström test on hospital employees as a negative impact of the lockdown on tobacco use.
The results in Table 3 show significant negative effects for all the distress values on hospital workers after the lockdown (p < 0.001). The respondents reported having a lower quality of sleep, a higher stress, irritability, sadness and also a loss of motivation.
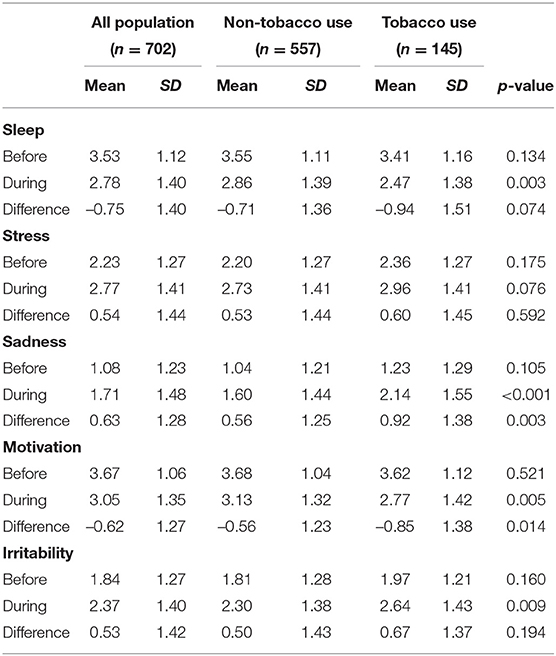
Table 3. Impact of the lockdown on psychological distress values.
Table 3 compares tobacco consumers and non-consumers with the psychological distress values. Tobacco consumers face a worse quality of sleep (mean = 2.47, SD = 1.38, and p < 0.003), sadness (mean = 2.14, SD = 1.55, and p < 0.001), irritability (mean = 2.64, SD = 1.43, and p < 0.009) and went through a loss of motivation (mean = 2.77, SD = 1.42, and p < 0.005) compared to non-tobacco consumers.
In Table 4, the results showed a decrease in physical activity since the beginning of the lockdown. Those who were having less than 30 min of physical activity per day did not have a significant change after the lockdown. About a third of the population (33%) reported reduced exercise time since the COVID-19 lockdown. The population that did not practice any physical activity increased from 23.5% to 38% after the lockdown.
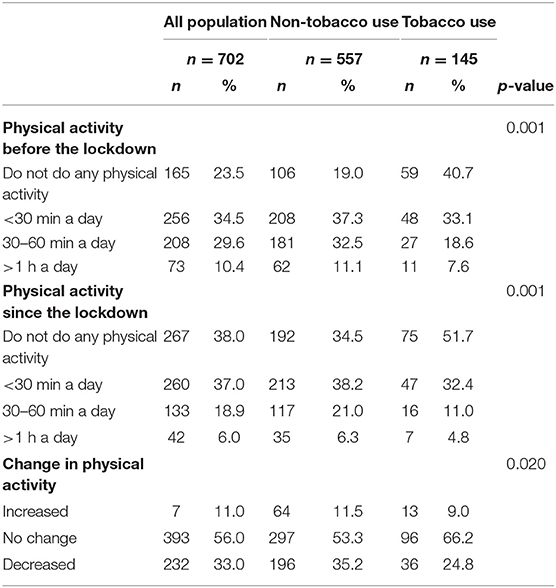
Table 4. Impact of the lockdown on physical activity.
In Table 5, correlations between physical activities and psychological distress values are presented. Since the lockdown, hospital workers reported poorer quality of sleep (mean = −1.00, SD = 1.45, and p < 0.001), more stress (mean = 0.67, SD =1.46, and p < 0.020), loss of motivation (mean = −0.84, SD = 1.37, and p < 0.001) and irritability (mean = 0.82, SD = 1.40, and p < 0.001). This implies a significant dependence between a reduced physical activity and worsening psychological values as previous studies showed (11, 29).

Table 5. Impact of the lockdown on psychological distress values correlating with physical activity.
Table 4 shows a significant negative association between tobacco consumers and physical activity. Tobacco users exercise less than non-users. For instance, before the lockdown, the population of smokers that do not practice any physical activity was 40.7%, whereas the nonsmoking counterpart was 19%. After the lockdown, these populations increased to 51% and 34.5%, respectively.
Given the psychological distress responses to COVID-19 lockdown shown before and the demonstrated benefits of physical activity over behavioral distress (30), further strategies to promote physical activity for hospital employees are required.
Table 6 shows the results of the adjusted OR of some independent variables with tobacco consumers. The profile that was identified to be the most at risk of increasing tobacco use corresponds to the population that satisfies the following criteria: (a) living alone [aOR 1.77, 95% CI (1.18–2.65) and p < 0.005]; (b) experiencing increased sadness [aOR 1.23, 95% CI (1.08–1.41), and p < 0.002]; (c) experiencing loss of motivation [aOR 0.86, 95% CI (0.74–1.00), and p < 0.043]; (d) receiving a lower income [aOR 1.69, 95% CI (1.04–2.70), and p < 0.031]; (e) consuming alcohol [aOR 3.12. 95% CI (1.92–5.05), and p < 0.001]; and (f) reducing physical activity [aOR 0.25, 95% CI (0.14–0.42), and p < 0.001].
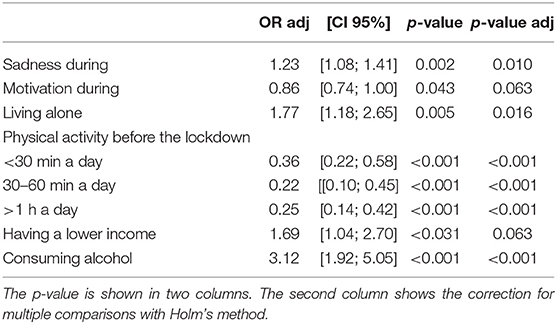
Table 6. Multivariable analysis on increasing the tobacco use related to the lockdown.
The present research examined the association between the first COVID-19 lockdown and the change in health behavior of hospital workers. The overarching conclusion is that the lockdown and the associated restrictive measures had a negative effect on this population. All aspects of psychological distress (sleep, sadness, motivation, irritability and stress) were significantly associated with changes in health behaviors (tobacco use and physical activity).
One of the main conclusions of this work is that living alone is a major risk factor for mental health issues and increased tobacco use. Similar results were found in other studies in the general french population. Rolland et al. (28) identified that being a female; not having a partner; being professionally active; and having a relatively low level of education are conditions associated with higher risk for increasing tobacco use. Rossinot et al. (11) described living alone as a strong risk factor for diet, sleep, physical activity, and tobacco consumption. In other countries, living alone has statistically strong significance with increased smoking during the lockdown. In Australia, Stanton et al. (12) showed that those who were not in a relationship had significantly higher depression, anxiety and stress scores compared to other categories of relationship status.
An interesting observation from the data obtained during this research is that participants that reported tobacco use, also reported lower scores in sleep quality and motivation; and higher scores in sadness and irritability. Similar observations have been reported in studies concerning the association between health-related behaviors and psychological distress factors. During the lockdown in France, Rossinot et al. (11) reported that deterioration on mental health (symptoms of anxiety, depression, or irritability) translates into worsening most behavioral indicators (tobacco and alcohol consumption, physical activity and sleep). These results are in concordance with the findings of the coronavirus and confinement longitudinal study (14) and the COVID-19 prevention studies in France (13). This observation has been made in the general population of other countries (12, 31–33).
It is important to highlight that the number of cigarettes smoked per day heavily increased withing the sampled population. This is justified by higher Fagerström scores in our survey. In the general population in Belgium (34), the odds of increasing tobacco use has doubled. In Poland, Sidor and Rzymski (35) conducted an online survey among 1097 adults during the lockdown showing that 45.2% of smokers had augmented their tobacco consumption. In China, Sun et al. (36) led an online survey among 6.416 adults and found that 20% of regular smokers had increased their tobacco use and 25.3% of ex-smokers had relapsed.
Another observation is that hospital staff decreased their physical activity during the lockdown. This decrease was more significant for tobacco users. One explanation is that during health crisis, hospital workers endure longer working schedules and increased tensions due to important responsibilities (9). This observation concurs with previous studies (12, 29) on general populations.
The above discussion highlights the behavioral response of hospital workers in times of stress and may, therefore, be valuable for providing the appropriate care and preventive actions in case of similar future events. This might include screenings for mental health problems, substance abuse, psychoeducation, and psychosocial support. Other alternatives include adaptation strategies and resilience capacities based on physical activities, sleep management, substance use control, increase motivation, integrate behavior change techniques, coaching, mindfullness groups, and counseling services on mental health.
This survey is based on participants' self-assessment on different parameters. The data analysis takes into account the subjectivity of these evaluations. More specifically, this survey aimed to capture participants' perceptions, feelings, and views on the impact of the COVID-19 pandemic and the associated lockdown. From this perspective, answers are assumed to be correct. Methods for analyzing data in which correctness is not the main assumption are presented in (37).
The population was composed by a majority of women. Nevertheless, this is in agreement with the women population working in the University Hospital of Nice (74% in 2019) and the fact that women respond more often than men to surveys is a well-known phenomenon. Therefore, this bias is not specific to this survey. The rate of tobacco smokers in our study (20.7%) was close to that observed in the general french population (24% in 2019) (19).
A limitation of this work is that the data encompasses only the first phase of the lockdown, and thus, long-term behaviors might not be accounted on this study.
Decision-making actions aiming to help hospital workers' health might benefit from tools capable of providing real-time monitoring. For instance, artificial intelligence can be used to gather data and guide adapted interventions aiming to anticipate negative effects. We believe that the results of our survey could help health systems and policymakers to better manage new waves of the pandemic, and the post-COVID-19 period.
In conclusion, our data suggests that negative changes in health behaviors are associated with increased psychological distress in hospital workers during the COVID-19 lockdown. Tobacco consumers are having increased psychological distress than their non-consuming counterparts. Health promotion strategies aimed at embracing or preserving positive health behaviors should go toward reducing critical and chronic increases in psychological distress during these unparalleled times. Ongoing assessment of the impact of lockdown and social distancing on health behaviors is needed to shape targeted health promotion strategies.
To our knowledge, no previous study has assessed the impact of a national COVID-19 containment measure on psychological distress values, physical activity and substance use on hospital workers. This work provides the first data analysis in this population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
IM, FC, RD, and SP participated in the design of the article, were involved in data synthesis, data interpretation, and drafted the manuscript. RF performed the statistical analysis. All authors read and approved the final manuscript.
The present study was supported by the University hospital of Nice, department of Gerontology Psychiatry and Department of Addiction, and the NICE BRAIN nonprofit association.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the contributions of the workers at the Sainte-Marie psychiatric hospital and the university hospital of Nice.
1. Ahn D.-G., Shin H.-J., Kim M.-H., Lee S., Kim H.-S., Myoung J., et al. (2020). Current status of epidemiology, diagnosis, therapeutics, and vaccines for novel coronavirus disease 2019 (COVID-19). J. Microbiol. Biotechnol. 30, 313–324. doi: 10.4014/jmb.2003.03011
2. Pfefferbaum B., North C. S. (2020). Mental health and the Covid-19 pandemic. New Engl. J. Med. 383, 510–512. doi: 10.1056/NEJMp2008017
3. Ko C. H., Yen C.-F., Yen J.-Y., Yang M.-J. (2006). Psychosocial impact among the public of the severe acute respiratory syndrome epidemic in Taiwan. Psychiatry Clin. Neurosci. 60, 397–403. doi: 10.1111/j.1440-1819.2006.01522.x
4. Lam M. H.-B., Wing Y.-K., Yu M. W.-M., Leung C.-M., Ma R. C., Kong A. P., et al. (2009). Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch. Intern. Med. 169, 2142–2147. doi: 10.1001/archinternmed.2009.384
5. Hawryluck L., Gold W. L., Robinson S., Pogorski S., Galea S., Styra R. (2004). Sars control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 10, 1206. doi: 10.3201/eid1007.030703
6. Lee S., Chan L. Y., Chau A. M., Kwok K. P., Kleinman A. (2005). The experience of sars-related stigma at amoy gardens. Soc. Sci. Med. 61, 2038–2046. doi: 10.1016/j.socscimed.2005.04.010
7. Wu P., Liu X., Fang Y., Fan B., Fuller C. J., Guan Z., et al. (2008). Alcohol abuse/dependence symptoms among hospital employees exposed to a sars outbreak. Alcohol Alcohol. 43, 706–712. doi: 10.1093/alcalc/agn073
8. Lima C. K. T., de Medeiros Carvalho P. M., Lima I. d. A. A. S., de Oliveira Nunes J. V. A., Saraiva J. S., et al. (2020). The emotional impact of coronavirus 2019-ncov (new coronavirus disease). Psychiatry Res. 287:112915. doi: 10.1016/j.psychres.2020.112915
9. Wang C., Pan R., Wan X., Tan Y., Xu L., Ho C. S., et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 17:1729. doi: 10.3390/ijerph17051729
10. García-Álvarez L., de la Fuente-Tomás L., García-Portilla M. P., Sáiz P. A., Lacasa C. M., Dal Santo F., et al. (2020). Early psychological impact of the 2019 coronavirus disease (COVID-19) pandemic and lockdown in a large spanish sample. J. Glob. Health 10:020505. doi: 10.7189/jogh.10.020505
11. Rossinot H., Fantin R., Venne J. (2020). Behavioral changes during Covid-19 confinement in France: a web-based study. Int. J. Environ. Res. Public Health 17:8444. doi: 10.3390/ijerph17228444
12. Stanton R., To Q. G., Khalesi S., Williams S. L., Alley S. J., Thwaite T. L., et al. (2020). Depression, anxiety and stress during Covid-19: associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 17:4065. doi: 10.3390/ijerph17114065
13. Chan-Chee C., Lon C., Lasbeur L., Lecrique J., Raude J., Arwidson P., et al. (2020). The mental health of the french facing the COVID-19 crisis: prevalence, evolution and determinants of anxiety disorders during the first two weeks of lockdown (coviprev study, march 23-25 and march 30-april 1st, 2020). Bull Epidmiol Hebd 2020, 2–9.
14. EHESP (2020). Etude Coconel: Impact Sur la Sant Mentale. Available online at: https://www.ehesp.fr/wp-content/uploads/2020/04/Etude-Coconel-Note-n2-impact-sante-mentale.pdf
15. Anton S. D., Miller P. M. (2005). Do negative emotions predict alcohol consumption, saturated fat intake, and physical activity in older adults? Behav. Modif. 29, 677–688. doi: 10.1177/0145445503261164
16. Clay J. M., Parker M. O. (2020). Alcohol use and misuse during the COVID-19 pandemic: a potential public health crisis? Lancet Public Health 5, e259. doi: 10.1016/S2468-2667(20)30088-8
17. Bai Y., Lin C.-C., Lin C.-Y., Chen J.-Y., Chue C.-M., Chou P. (2004). Survey of stress reactions among health care workers involved with the sars outbreak. Psychiatr. Serv. 55, 1055–1057. doi: 10.1176/appi.ps.55.9.1055
18. Ashdown-Franks G., Sabiston C. M., Stubbs B. (2019). The evidence for physical activity in the management of major mental illnesses: a concise overview to inform busy clinicians' practice and guide policy. Curr. Opin. Psychiatry 32, 375–380. doi: 10.1097/YCO.0000000000000526
19. Pasquereau A., Andler R., Arwidson P., Guignard R., NguyenThanh V. (2020). Consommation de tabac parmi les adultes: bilan de cinq années de programme national contre le tabagisme, 2014-2019. Bull. Epidmiol Hebd. 273–281.
20. Lemaire F. (2019). La loi Jardé: ce qui change. La Presse Med. 48, 238–242. doi: 10.1016/j.lpm.2019.01.006
21. CDC (2020). Evidence Used to Update the List of Underlying Medical Conditions That Increase a Person's Risk of Severe Illness From COVID-19. Atlanta, GA: CDC.
22. Underner M., Le Houezec J., Perriot J., Peiffer G. (2012). Les tests d'évaluation de la dépendance tabagique. Rev. Mal. Respir. 29, 462–474. doi: 10.1016/j.rmr.2011.09.051
23. Etter J.-F., Duc T. V., Perneger T. V. (1999). Validity of the Fagerström test for nicotine dependence and of the heaviness of smoking index among relatively light smokers. Addiction 94, 269–281. doi: 10.1046/j.1360-0443.1999.94226910.x
24. Berlin I., Singleton E. G., Heishman S. J. (2010). Validity of the 12-item french version of the tobacco craving questionnaire in treatment-seeking smokers. Nicotine Tob. Res. 12, 500–507. doi: 10.1093/ntr/ntq039
25. Richard J., Andler R., Cogordan C., Spilka S., Nguyen-Thanh V., le groupe Baromètre de Santé publique France 2017 (2019;(5-6):89–97.). La consommation d'alcool chez les adultes en France en 2017. Bull. Epidmiol. Hebd.
26. Lon C., Chan Chee C., du Roscot E., le groupe Baromètre santé, 2017 (2018). La dépression en France chez les 18-75ans: résultats du baromètre santé 2017. Bull. Epidmiol. Hebd. 637–644.
27. Lauby-Secretan B., Dossus L., Marant-Micallef C., His M. (2019). Obésité et cancer. Bull. Cancer 106, 635–646. doi: 10.1016/j.bulcan.2019.04.008
28. Rolland B., Haesebaert F., Zante E., Benyamina A., Haesebaert J., Franck N. (2020). Global changes and factors of increase in caloric/salty food intake, screen use, and substance use during the early Covid-19 containment phase in the general population in France: survey study. JMIR Public Health Surveill. 6, e19630. doi: 10.2196/19630
29. Meyer J., McDowell C., Lansing J., Brower C., Smith L., Tully M., et al. (2020). Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. Int. J. Environ. Res. Public Health 17:6469. doi: 10.3390/ijerph17186469
30. Schuch F. B., Stubbs B., Meyer J., Heissel A., Zech P., Vancampfort D., et al. (2019). Physical activity protects from incident anxiety: a meta-analysis of prospective cohort studies. Depress. Anxiety 36, 846–858. doi: 10.1002/da.22915
31. Stubbs B., Vancampfort D., Firth J., Solmi M., Siddiqi N., Smith L., et al. (2018). Association between depression and smoking: a global perspective from 48 low-and middle-income countries. J. Psychiatr. Res. 103, 142–149. doi: 10.1016/j.jpsychires.2018.05.018
32. Hammami A., Harrabi B., Mohr M., Krustrup P. (2020). Physical activity and coronavirus disease 2019 (COVID-19): specific recommendations for home-based physical training. Manag. Sport Leisure 1–6. doi: 10.1080/23750472.2020.1757494
33. Kumar A., Nayar K. R. (2020). Covid 19 and its mental health consequences. J. Mental Health 180, 817–818. doi: 10.1001/jamainternmed.2020.1562
34. Vanderbruggen N., Matthys F., Van Laere S., Zeeuws D., Santermans L., Van den Ameele S., et al. (2020). Self-reported alcohol, tobacco, and cannabis use during Covid-19 lockdown measures: results from a web-based survey. Eur. Addict. Res. 26, 309–315. doi: 10.1159/000510822
35. Sidor A., Rzymski P. (2020). Dietary choices and habits during Covid-19 lockdown: experience from Poland. Nutrients 12, 1657. doi: 10.3390/nu12061657
36. Sun Y., Li Y., Bao Y., Meng S., Sun Y., Schumann G., et al. (2020). Brief report: increased addictive internet and substance use behavior during the Covid-19 pandemic in China. Am. J. Addict. 29, 268–270. doi: 10.1111/ajad.13066
Keywords: COVID-19, lockdown, tobacco, physical activity, psychological distress, health behaviors, hospital workers
Citation: Mounir I, Menvielle L, Perlaza S, Chênevert D, Planchard J-H, Fabre R, Benoit M, Benyamina A, Rolland B, Cherikh F and David R (2021) Psychological Distress and Tobacco Use Among Hospital Workers During COVID-19. Front. Psychiatry 12:701810. doi: 10.3389/fpsyt.2021.701810
Received: 28 April 2021; Accepted: 09 June 2021;
Published: 28 July 2021.
Edited by:
Ashwani Kumar Mishra, All India Institute of Medical Sciences, IndiaReviewed by:
Georgia Trakada, National and Kapodistrian University of Athens, GreeceCopyright © 2021 Mounir, Menvielle, Perlaza, Chênevert, Planchard, Fabre, Benoit, Benyamina, Rolland, Cherikh and David. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Izza Mounir, bW91bmlyLmlAY2h1LW5pY2UuZnI=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.