
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 22 July 2021
Sec. Psychopathology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.701140
 Jessica Fernández-Sevillano1,2,3Susana Alberich2,3Iñaki Zorrilla1,2,3Itxaso González-Ortega2,3María Purificación López1,2,3Víctor Pérez3,4Eduard Vieta3,5
Jessica Fernández-Sevillano1,2,3Susana Alberich2,3Iñaki Zorrilla1,2,3Itxaso González-Ortega2,3María Purificación López1,2,3Víctor Pérez3,4Eduard Vieta3,5 Ana González-Pinto1,2,3*†
Ana González-Pinto1,2,3*† Pilar Saíz3,6†
Pilar Saíz3,6†Background: Neuropsychological alterations can lead to inaccurate perception, interpretation, and response to environmental information, which could be a risk factor for suicide.
Methods: Ninety-six subjects were recruited from the Psychiatry Department of the Araba University Hospital—Santiago, including 20 patients with a recent attempt and diagnosis of major depressive disorder (MDD) according to DSM-V, 33 MDD patients with history of attempted suicide, 23 non-attempter MDD patients, and 20 healthy controls. All participants underwent a clinical interview and neuropsychological assessment on the following cognitive domains: working memory, processing speed, decision-making, executive function, and attention. Backward multiple regressions were performed adjusting for significant confounding variables. For group comparisons, ANOVA and Bonferroni post-hoc tests were performed with a p < 0.05 significance level.
Results: The patient groups did not differ regarding severity of depression and stressful events in the last 6 months. In comparison to healthy controls, depressed patients with lifetime suicide attempts had more general trauma (p = 0.003), emotional abuse (p = 0.003), emotional negligence (p = 0.006), and physical negligence (p = 0.009), and depressed patients with recent suicide attempts had experienced more child sexual abuse (p = 0.038). Regarding neuropsychological assessment, all patient groups performed significantly worse than did healthy controls in processing speed, decision-making, and attention. Comparisons between patient groups indicated that recent suicide attempters had poorer performance on executive function in comparison to both depressed lifetime attempters and depressed non-attempters (B = 0.296, p = 0.019, and B = 0.301, p = 0.028, respectively). Besides, women with recent attempts had slightly better scores on executive function than males. Regarding the rest of the cognitive domains, there were no significant differences between groups.
Conclusion: Executive function performance is altered in recent suicide attempts. As impaired executive function can be risk factor for suicide, preventive interventions on suicide should focus on its assessment and rehabilitation.
Suicide is a major health issue worldwide involving nearly 800,000 deaths per year (1). Identifying risk factors can lead to a better understanding and prevention of this behavior (2). Age, sex, history of previous attempts, genetic predisposition, drug consumption, and early adversity, among others, have been extensively reported as relevant features that can predict a suicide attempt (3–6).
Additionally, neuropsychological performance has been linked to suicide in several studies across all the life span. Impaired complex cognition, social cognition, and episodic memory (7, 8) were reported in adolescents at risk of suicide. In children with a family history of suicide attempts, cognitive, attention, and language reasoning have been described, increasing their risk of reproducing a suicide attempt themselves (9). In contrast, McHugh et al. (10) found better cognitive functioning on processing speed, verbal learning, working memory, delayed memory, and verbal fluency in suicidal youngsters and young adults.
In adult and elderly populations, many studies have provided evidence of alterations in executive function (11–13), attention (14), memory (15), and decision-making (13, 16, 17) in suicide attempters. Deficits in these cognitive domains, especially executive function that organizes and directs behavior, can lead to an inaccurate perception, interpretation, retrieval, and response to environmental information, which may result in an inflexible, pessimistic way of thinking about their future and themselves (18). Thus, these cognitive deficits may imply a higher risk of suicide as a response to adverse life events. In summary, existing evidence supports a connection between cognition and suicide. However, these studies do not determine the specific cognitive alterations involved in a recent suicide attempt, that is, the current altered processes that surround and may contribute to suicidal behavior. Besides, these cognitive alterations are not unique to suicide and have also been described in depressive patients (19–24); therefore, it remains unclear which specific cognitive domains are altered in recent suicidal behavior. Considering data scarcity, the aim of this study was to explore cognitive alterations in recent suicide attempts. For this purpose, we compared the neuropsychological performance of depressed patients with a recent attempt, depressed patients with a history of suicide, depressed non-attempters, and healthy controls on the following cognitive domains: working memory, processing speed, decision-making, executive function, and attention.
Ninety-six participants were recruited from the Psychiatry Department of the Araba University Hospital—Santiago. All patients were diagnosed of major depressive disorder (MDD) according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria and were receiving psychopharmacological treatment for their condition. The sample was categorized into the following groups: 20 depressed patients who were hospitalized after a recent suicide attempt (≤ 30 days), 33 patients with a past suicide attempt during their lifetime and hospitalized for MDD episodes, 23 without history of suicidal attempts and hospitalized for MDD episodes, and 20 healthy controls with no personal or family history of mental illness matched by age and sex with a reference group, that is, a recent suicide attempt group. Suicide attempt was defined as a “self-initiated sequence of behaviors by an individual who, at the time of the initiation, expected that the set of actions would lead to his or her own death” (DSM-5). The exclusion criteria for the three groups including patients were: presence of psychotic symptoms and other comorbid psychiatric disorders with the exception of tobacco use disorder, acute infections, neurological illness, intellectual disability, dementia, organic diseases that compromise cognitive functioning, and cognitive syndromes. In addition to this, the exclusion criteria for healthy controls included either personal or a family history of major psychiatric disorders. All participants were between 18 and 65 years old and had signed an informed consent. This study was approved by the ethical board of the Araba University Hospital and was conducted according to the Declaration of Helsinki (25).
After recruitment and signature of the informed consent, each participant had an interview with a psychologist for sociodemographic data collection and clinical assessment of depressive symptoms, stressful events, and childhood trauma. Depressive symptom severity was assessed using the 17-item Spanish version of the Hamilton Depression Rating Scale (HDRS) (26, 27), a structured instrument widely used in the psychiatric field (28–30) that offers a quantitative measure of the severity of depressive symptoms in a clinical population according to the criteria of the evaluator who conducts the clinical interview. Each item has between three and five possible responses with 0–2 or 0–4 scores, respectively, and the total score ranges from 0 to 52. The 17-item Spanish version has good reliability, with a Cronbach's α of 0.72, and validity with a correlation with other scales for depressive symptoms (Montgomery–Asberg and Beck's Depression Inventory) ranging from 0.8 to 0.9. Recent (6 months) stressful events were measured using the Spanish version of the List of Threatening Experiences (LTE) (31, 32), a 12-item brief questionnaire with yes/no responses regarding personal, relational, financial, and health problems. This questionnaire has a high test–retest reliability (κ = 0.61–0.87) and is a valid and reliable measure of stressful events in mental health, specifically in depression (OR = 1.64–2.57) (32), which has been previously used in studies with psychiatric populations (33–36). Childhood abuse and neglect were assessed with the Spanish version of the Childhood Trauma Questionnaire—Short Form (CTQ-SF) (37), a self-administered 28-item questionnaire with five Likert responses (never, rarely, sometimes, often, and always) that has been extensively used (38–43) to evaluate the maltreatment dimensions that were detected in the original factorial analysis for construct validity (44): emotional (Cronbach's α = 0.87), physical (Cronbach's α = 0.89) and sexual abuse (Cronbach's α = 0.94) and physical (Cronbach's α = 0.66) and emotional (Cronbach's α = 0.83) neglect (37).
Besides, the participants underwent a neuropsychological assessment using a standardized test on the following cognitive domains: working memory, processing speed, decision-making, executive function, and attention. The test and measures used in each domain (Table 1) were adapted from previous existing literature on cognitive assessment in mental disorders (50, 51).
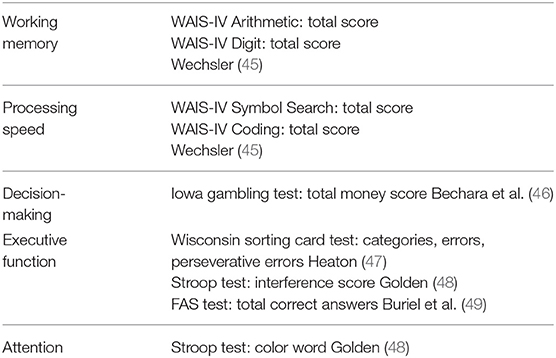
Table 1. Cognitive domains.
Statistical analysis was performed by an expert biomedical statistician. Data were checked for Gaussian distribution. Comparisons between groups regarding the sociodemographic and clinical variables were performed with ANOVA followed by Bonferroni post-hoc testing for continuous variables and chi-square for categorical variables. For the analyses of cognitive performance, measures selected from each test (Table 1) were gathered into the corresponding cognitive domain that is evaluated and the obtained scores were transformed to average z-scores. Backward multiple regressions were performed adjusting for the following confounding variables: age, sex, economic status, education, marital status, drug consumption (tobacco, cannabis, and alcohol), and severity of depressive symptoms according to the HDRS. In each model, only significant confounders were taken into account.
There were no significant differences between groups regarding sociodemographic variables (Table 2). In the recent attempt group, 35% of patients were recruited after an index attempt, 40% of patients reattempted for the second time, and 60% of patients had more than two reattempts. In the lifetime attempt group, 6.3% of patients had attempted suicide once, 34.4% twice, and 59.3% more than twice. Regarding psychiatric medication, the majority had similar treatments as 94% were under polytherapy consisting of antidepressants and benzodiazepines, whereas 6% of patients were under monotherapy of either of those treatments.
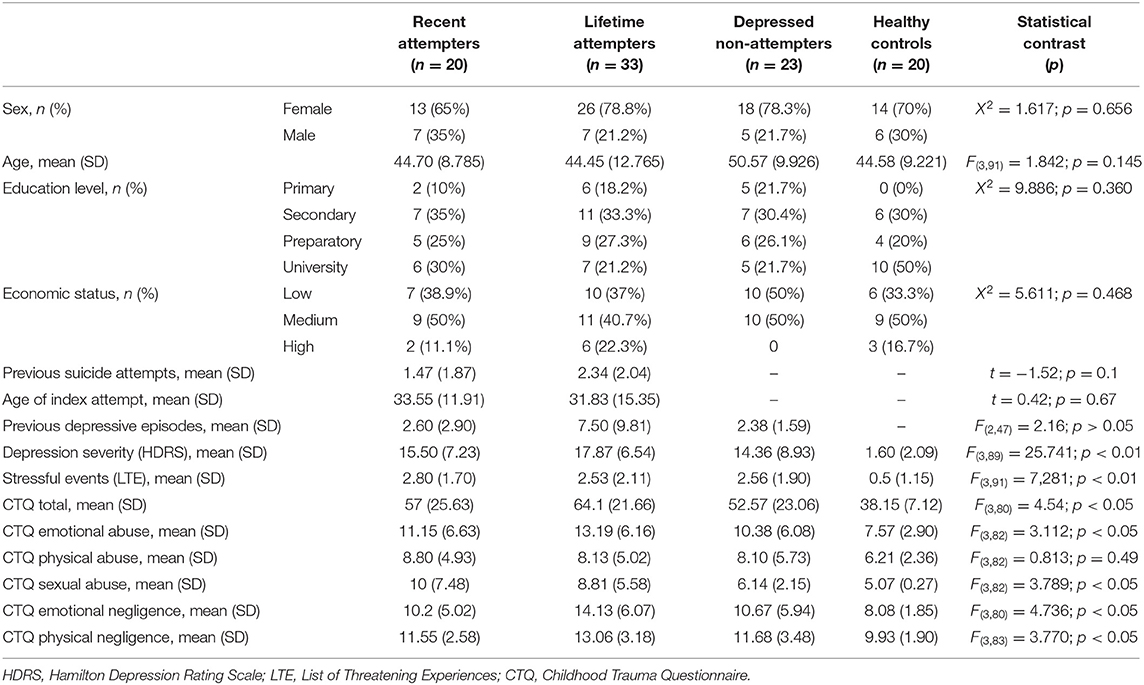
Table 2. Demographic and clinical variables.
In addition to having similar medication profiles, the severity of depressive symptoms was equally distributed across groups. Bonferroni post-hoc analyses revealed that all groups had significantly higher scores for depressive symptoms measured by the HDRS than did the healthy controls (p < 0.01 in each comparison), but the severity of depression was similar across patient groups. Besides, healthy controls had fewer stressful events in the last 6 months than each of the patient groups (p < 0.05 in each comparison).
Also, post-hoc analyses of the CTQ-SF scores indicate greater general trauma (p = 0.003), emotional abuse (p = 0.003), emotional negligence (p = 0.006), and physical negligence (p = 0.009) in patients with a history of suicide attempts in comparison to healthy controls. Besides, patients with recent suicide attempts reported higher scores of child sexual abuse (p = 0.038) than did healthy controls.
The scores on the five domains included in this study are presented in Table 3.
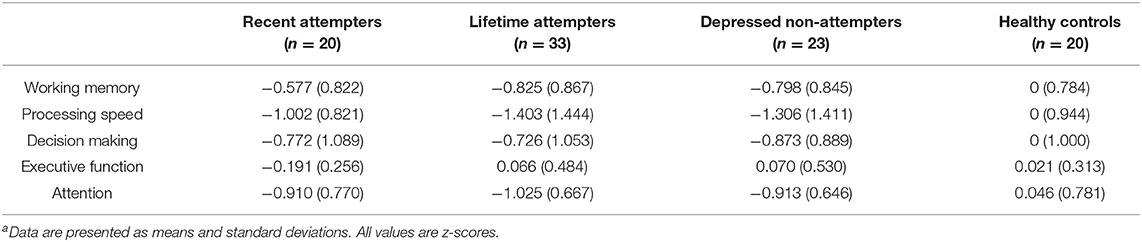
Table 3. Cognitive domains by groupa.
Backward stepwise multiple regressions were performed and adjusted by significant confounders (age, sex, economic level, marital status, years of education, severity of depression, and substance consumption) with healthy controls as the reference group. Healthy controls performed significantly better in processing speed, decision-making, and attention than did all groups of depressed patients, with no differences between them (Table 4).
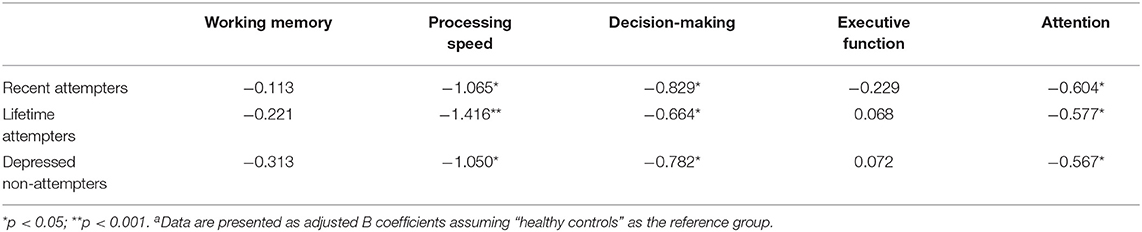
Table 4. Multiple regressiona.
As the main objective of this study was to determine the cognitive differences between recent suicide attempters and current non-suicidal depressed patients, the reference group for adjusted regressions was afterwards changed to recent attempters. The results yielded significant differences on the executive function domain. Both lifetime attempters and depressed non-attempters had significantly higher scores in this domain in comparison to recent attempters (B = 0.296, p = 0.019, and B = 0.301, p = 0.028, respectively); that is, recent suicide attempters had poorer performance on executive function. However, there were no significant differences between groups in the rest of the cognitive domains.
Further analyses showed that there was an interaction between group (depressed recent attempters, depressed lifetime attempters, and depressed non-attempters) and sex on executive performance (Table 5). According to these results, women with recent attempts had slightly better scores on executive function than did males. However, in the rest of the groups, men outperformed women, especially in depressed non-attempter patients, with a large effect size indicating a strong interaction between sex and group.
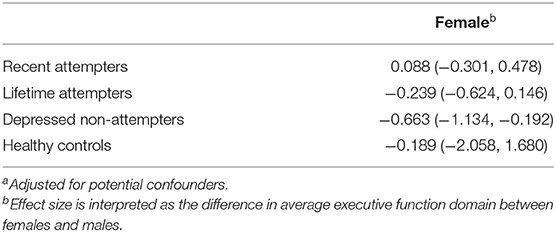
Table 5. Effect sizes of being female on executive functiona.
The main finding of this study is that MDD patients with suicide attempts in the last 30 days have significantly poorer performance on executive function compared to MDD patients with a previous history of suicide attempts and to MDD non-attempter patients. This finding indicates that suicide might be accompanied with an altered performance on executive function. Deficits in this cognitive domain have already been described in patients with a history of suicidality (12, 14, 52–56) and in depressed patients without suicidal behavior (23, 53), especially in those with poor treatment response (57), but to the best of our knowledge, this is the first study that compares MDD patients with recent attempts, MDD patients with lifetime attempts, MDD non-attempter patients, and healthy controls.
Executive function directs thought and behavior toward an objective in order to respond to current or future situational demands. According to the comprehensive model proposed by Miyake et al. (58), this implies the inhibition of responses, shifting between tasks and the constant update of the working memory. Other authors also include planning, decision-making, working memory, and error detection among its functions (59, 60). All in all, these processes allow the deliberate and intentional goal-directed response to environmental stimuli and are subject to the influence of individual factors, such as emotional regulation, personality traits, and even traumatic events (61–63). Deficits in these processes can lead to the dysregulation of emotion, thoughts, and actions (64), which might contribute to considering suicide as a solution under critical circumstances (15). In addition, these alterations may also increase interpersonal difficulties, increasing the risk of attempted suicide (17).
According to our results, sex has an influence on executive function. The slightly better performance of women in the recent attempt group may be possibly explained by the fact that higher impulsivity scores have been related to men (61), which implies a tendency to think and behave with less planning, error detection, cognitive flexibility, and inhibitory control (65), processes that are under control of the executive function. Therefore, men are more likely to make non-adaptive choices under demanding or stressing circumstances as risky behavior or suicide. However, depressed non-attempter men had significantly better executive function performance. This may be due to the fact that women have more severe cognitive symptoms of depression, such as rumination and hypochondria (66), and a greater impact on their functionality (67). Apart from psychological factors, there are also biological differences, such as sex hormones (68, 69), dysregulation of the hypothalamus–pituitary–adrenal (HPA) axis (70), and inflammatory parameters (71), that make depression more adverse for women.
Additionally, the neuropsychological assessment results revealed that all depressed patients with similar depression severity performed significantly worse than did healthy controls in processing speed, decision-making, and attention, but with no difference between groups. This suggests that depressed patients have alterations in these specific dimensions associated with their psychopathological process; that is, major depressive disorder is consistent with previous literature (21, 54, 72, 73). According to our findings, these alterations are different from those associated specifically with recent suicide attempts and, therefore, different cognitive processes are specifically more altered in each condition.
Apart from the neurocognitive deficits, traumatic life events are also associated with a higher risk of suicide. Patients with a history of childhood maltreatment (74–76) and sexual abuse (77) have an increased risk of suicidal behavior in their adult life. In our sample, patients with recent suicide attempts reported more child sexual abuse than the rest of the groups. Patients with a history of suicide reported more general trauma, emotional abuse, and negligence, and in general, patients had more recent stressful events than did the controls. Furthermore, the link between trauma, executive function alterations, and suicidal behavior has also been described by several authors. In a recent study by Zelazny et al. (76), higher scores on executive function were protective against suicide in individuals with childhood maltreatment. Carvalho et al. (78) found that maltreated children performed worse than did non-maltreated children in executive function tests, and according to the study by Dannehl et al. (79), these differences are also present in adults with a history of childhood adversity, especially in those with physical abuse and neglect.
In conclusion, recent suicidal behavior is specifically associated with deficits on executive function, which suggests a cognitive dysfunction on information processing and response, especially in critical events. As executive function can be trained and improved (80), cognitive screening and stimulation may be proposed as a strategy for suicide prevention in at-risk patients. Future studies are needed to identify possible differences between sex in each cognitive domain for a more personalized approach and for a better understanding of early detection vulnerability factors that may enable us to prevent suicide in at-risk patients.
This study has a number of limitations. Recent and past trauma events were assessed using self-administered and self-reported scales in MDD patients who can be biased when reporting this information. As more women have recently attempted suicide than men, the sex-related differences on executive function found in recent attempters must be interpreted with caution, and further confirmatory studies are advisable. Moreover, some factors that have been described in the literature as potentially influencing suicidal behavior in major depression, such as anxiety (81) or mixed symptoms (82), were not assessed.
The raw data supporting the conclusions of this article will be made available under request to the authors.
The studies involving human participants were reviewed and approved by CEIC EUSKADI. The patients/participants provided their written informed consent to participate in this study.
JF-S drafted and wrote the manuscript. SA performed statistical analyses and contributed to data interpretation. IZ, ML, VP, and EV revised the manuscript for important intellectual content and provided scientific advice. IG-O provided funding sources and scientific advice. PS and AG-P designed the study, corrected the manuscript, gave final approval of the version to be published, and ensured the scientific accuracy and integrity of the work. AG-P and PS should be considered joint senior authors. All authors contributed to the article and approved the submitted version.
This work was supported by Carlos III Health Research Institute [Grant Numbers PI15/00789, PI17/01433, PI18/01055, and PI19/00569 (co-financed by the European Regional Development Fund (ERDF)/European Social Fund Investing in your future, and the Government of the Principality of Asturias PCTI-2018-2022 IDI/2018/235). Foundation for Health Innovation and Research (BIOEF); Networking Center for Biomedical Research in Mental Health (CIBERSAM), the Basque Government (Grant No: 2017111104); and the University of the Basque Country (Grant No: 321218ELCY). The Psychiatric Research Department in Araba University Hospital is supported by the Stanley Research Foundation (Grant No: 03-RC-003). JF-S was a beneficiary of the Pre-PhD Training Programme of the Basque Government. No funding source in this study was involved in the study design, collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the paper for publication.
VP has been a consultant to or has received honoraria or grants from AB-Biotics, AstraZeneca, Bristol-Myers-Squibb, CIBERSAM, FIS- ISCiii, Janssen Cilag, Lundbeck, Otsuka, Servier, and Pfizer. EV has received grants and served as consultant, advisor, or CME speaker for the following entities: AB-Biotics, Abbott, Allergan, Angelini, AstraZeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, Farmindustria, Ferrer, Forest Research Institute, Galenica, Gedeon Richter, Glaxo-Smith-Kline, Janssen, Lundbeck, Otsuka, Pfizer, Roche, Sage, Sanofi-Aventis, Servier, Shire, Sunovion, Takeda, the Brain and Behaviour Foundation, the Generalitat de Catalunya (PERIS), the Spanish Ministry of Science, Innovation and Universities (CIBERSAM), EU Horizon 2020, and the Stanley Medical Research Institute. AG-P has received grants and served as consultant, advisor, or CME speaker for the following entities: Almirall, AstraZeneca, Bristol-Myers Squibb, Cephalon, Eli Lilly, Glaxo-Smith-Kline, Janssen-Cilag, Ferrer, Johnson & Johnson, Lundbeck, Merck, Otsuka, Pfizer, Sanofi-Aventis, Servier, Shering-Plough, Solvay, the Spanish Ministry of Science and Innovation (CIBERSAM), the Ministry of Science (Carlos III Institute), the Basque Government, the Stanley Medical Research Institute (03-RC-003), and Wyeth. PS has been a consultant to and/or has received honoraria or grants from Adamed, CIBERSAM, European Commission, GlaxoSmithKline, Government of the Principality of Asturias, Instituto de Salud Carlos III, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas, and Servier.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We want to acknowledge the Center for Biomedical Research in Mental Health (CIBERSAM), Carlos III Health Research Institute, the Basque Government, the University of the Basque Country (UPV/EHU), and Bioaraba Research Institute.
1. WHO. Suicide data. (2016) Available online at: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/
2. Pérez V, Elices M, Prat B, Vieta E, Blanch J, Alonso J, et al. The catalonia suicide risk code: a secondary prevention program for individuals at risk of suicide. J Affect Disord. (2020) 268:201–5. doi: 10.1016/j.jad.2020.03.009
3. Ayuso-Mateos JL, Baca-García E, Bobes J, Giner J, Giner L, Pérez V, et al. Recommendations for the prevention and management of suicidal behaviour. Rev Psiquiatr Salud Ment. (2012) 5:8–23. doi: 10.1016/j.rpsmen.2012.01.002
4. Dutta R, Ball HA, Siribaddana SH, Sumathipala A, Samaraweera S, McGuffin P, et al. Genetic and other risk factors for suicidal ideation and the relationship with depression. Psychol Med. (2017) 47:2438–49. doi: 10.1017/S0033291717000940
5. Gomez SH, Tse J, Wang Y, Turner B, Millner AJ, Nock MK, et al. Are there sensitive periods when child maltreatment substantially elevates suicide risk? results from a nationally representative sample of adolescents. Depress Anxiety. (2017) 34:734–41. doi: 10.1002/da.22650
6. Miret M, Caballero FF, Huerta-Ramírez R, Moneta MV, Olaya B, Chatterji S, et al. Factors associated with suicidal ideation and attempts in spain for different age groups. prevalence before and after the onset of the economic crisis. J Affect Disord. (2014) 163:1–9. doi: 10.1016/j.jad.2014.03.045
7. Ortuño-Sierra J, Aritio-Solana R, Casal ADG del, Fonseca-Pedrero E. Neurocognitive functioning in adolescents at risk for suicidal behaviors. Arch Suicide Res. (2020) 1–15. doi: 10.1080/13811118.2020.1746938. [Epub ahead of print].
8. Huber RS, Sheth C, Renshaw PF, Yurgelun-Todd DA, McGlade EC. Suicide ideation and neurocognition among 9- and 10-year old children in the adolescent brain cognitive development (ABCD) study. Arch Suicide Res. (2020) 1–15. doi: 10.1080/13811118.2020.1818657. [Epub ahead of print].
9. Jones JD, Boyd RC, Calkins ME, Moore TM, Ahmed A, Barzilay R, et al. Association between family history of suicide attempt and neurocognitive functioning in community youth. J Child Psychol Psychiatry. (2021) 62:58–65. doi: 10.1111/jcpp.13239
10. McHugh CM, Iorfino F, Crouse JJ, Tickell A, Nichles A, Zmicerevska N, et al. Neurocognitive functioning predicts suicidal behaviour in young people with affective disorders. J Affect Disord. (2021) 281:289–96. doi: 10.1016/j.jad.2020.11.077
11. Marzuk PM, Hartwell N, Leon AC, Portera L. Executive functioning in depressed patients with suicidal ideation. Acta Psychiatr Scand. (2005) 112:294–301. doi: 10.1111/j.1600-0447.2005.00585.x
12. McGirr A, Dombrovski AY, Butters MA, Clark L, Szanto K. Deterministic learning and attempted suicide among older depressed individuals: cognitive assessment using the wisconsin card sorting task. J Psychiatr Res. (2012) 46:226–32. doi: 10.1016/j.jpsychires.2011.10.001
13. Westheide J, Quednow BB, Kuhn K-U, Hoppe C, Cooper-Mahkorn D, Hawellek B, et al. Executive performance of depressed suicide attempters: the role of suicidal ideation. Eur Arch Psychiatry Clin Neurosci. (2008) 258:414–21. doi: 10.1007/s00406-008-0811-1
14. Keilp JG, Sackeim HA, Brodsky BS, Oquendo MA, Malone KM, Mann JJ. Neuropsychological dysfunction in depressed suicide attempters. Am J Psychiatry. (2001) 158:735–41. doi: 10.1176/appi.ajp.158.5.735
15. Richard-Devantoy S, Berlim MT, Jollant F. A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychol Med. (2014) 44:1663–73. doi: 10.1017/S0033291713002304
16. Jollant F, Bellivier F, Leboyer M, Astruc B, Torres S, Verdier R, et al. Impaired decision making in suicide attempters. Am J Psychiatry. (2005) 162:304–10. doi: 10.1176/appi.ajp.162.2.304
17. Jollant F, Guillaume S, Jaussent I, Castelnau D, Malafosse A, Courtet P. Impaired decision-making in suicide attempters may increase the risk of problems in affective relationships. J Affect Disord. (2007) 99:59–62. doi: 10.1016/j.jad.2006.07.022
18. Lara E, Olaya B, Garin N, Ayuso-Mateos JL, Miret M, Moneta V, et al. Is cognitive impairment associated with suicidality? A population-based study. Eur Neuropsychopharmacol J Eur Coll Neuropsychopharmacol. (2015) 25:203–13. doi: 10.1016/j.euroneuro.2014.08.010
19. Allott K, Fisher CA, Amminger GP, Goodall J, Hetrick S. Characterizing neurocognitive impairment in young people with major depression: state, trait, or scar? Brain Behav. (2016) 6:e00527. doi: 10.1002/brb3.527
20. Baune BT, Fuhr M, Air T, Hering C. Neuropsychological functioning in adolescents and young adults with major depressive disorder–a review. Psychiatry Res. (2014) 218:261–71. doi: 10.1016/j.psychres.2014.04.052
21. Chakrabarty T, Hadjipavlou G, Lam RW. Cognitive dysfunction in major depressive disorder: assessment, impact, and management. Focus J Life Long Learn Psychiatry. (2016) 14:194–206. doi: 10.1176/appi.focus.20150043
22. Grützner TM, Sharma A, Listunova L, Bartolovic M, Weisbrod M, Roesch-Ely D. Neurocognitive performance in patients with depression compared to healthy controls: association of clinical variables and remission state. Psychiatry Res. (2019) 271:343–50. doi: 10.1016/j.psychres.2018.11.047
23. Sommerfeldt SL, Cullen KR, Han G, Fryza BJ, Houri AK, Klimes-Dougan B. Executive attention impairment in adolescents with major depressive disorder. J Clin Child Adolesc Psychol Off J Soc Clin Child Adolesc Psychol Am Psychol Assoc Div 53. (2016) 45:69–83. doi: 10.1080/15374416.2015.1072823
24. Zhou F-C, Wang Y-Y, Zheng W, Zhang Q, Ungvari GS, Ng CH, et al. Prospective memory deficits in patients with depression: a meta-analysis. J Affect Disord. (2017) 220:79–85. doi: 10.1016/j.jad.2017.05.042
25. World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
26. Bobes J, Bulbena A, Luque A, Dal-Ré R, Ballesteros J, Ibarra N. Evaluación psicométrica comparativa de las versiones en español de 6, 17 y 21 ítems de la escala de valoración de hamilton para la evaluación de la depresión. Med Clínica. (2003) 120:693–700. doi: 10.1016/S0025-7753(03)73814-7
27. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. (1967) 6:278–96. doi: 10.1111/j.2044-8260.1967.tb00530.x
28. Failde I, Dueñas M, Agüera-Ortíz L, Cervilla JA, Gonzalez-Pinto A, Mico JA. Factors associated with chronic pain in patients with bipolar depression: a cross-sectional study. BMC Psychiatry. (2013) 13:112. doi: 10.1186/1471-244X-13-112
29. González-Ortega I, Alberich S, Echeburúa E, Aizpuru F, Millán E, Vieta E, et al. Subclinical depressive symptoms and continued cannabis use: predictors of negative outcomes in first episode psychosis. PloS ONE. (2015) 10:e0123707. doi: 10.1371/journal.pone.0123707
30. Healthy Quality Ontario. Psychotherapy for major depressive disorder and generalized anxiety disorder: a health technology assessment. Ont Health Technol Assess Ser. (2017) 17:1–167.
31. Brugha TS, Cragg D. The list of threatening experiences: the reliability and validity of a brief life events questionnaire. Acta Psychiatr Scand. (1990) 82:77–81. doi: 10.1111/j.1600-0447.1990.tb01360.x
32. Motrico E, Moreno-Küstner B, de Dios Luna J, Torres-González F, King M, Nazareth I, et al. Psychometric properties of the list of threatening experiences-LTE and its association with psychosocial factors and mental disorders according to different scoring methods. J Affect Disord. (2013) 150:931–40. doi: 10.1016/j.jad.2013.05.017
33. Casey PR, Dunn G, Kelly BD, Birkbeck G, Dalgard OS, Lehtinen V, et al. Factors associated with suicidal ideation in the general population: five-centre analysis from the ODIN study. Br J Psychiatry J Ment Sci. (2006) 189:410–5. doi: 10.1192/bjp.bp.105.017368
34. Cervilla JA, Molina E, Rivera M, Torres-González F, Bellón JA, Moreno B, et al. The risk for depression conferred by stressful life events is modified by variation at the serotonin transporter 5HTTLPR genotype: evidence from the Spanish PREDICT-gene cohort. Mol Psychiatry. (2007) 12:748–55. doi: 10.1038/sj.mp.4001981
35. Dalgard OS, Dowrick C, Lehtinen V, Vazquez-Barquero JL, Casey P, Wilkinson G, et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol. (2006) 41:444–51. doi: 10.1007/s00127-006-0051-5
36. Powers AD, Gleason MEJ, Oltmanns TF. Symptoms of borderline personality disorder predict interpersonal (but not independent) stressful life events in a community sample of older adults. J Abnorm Psychol. (2013) 122:469–74. doi: 10.1037/a0032363
37. Hernandez A, Gallardo-Pujol D, Pereda N, Arntz A, Bernstein DP, Gaviria AM, et al. Initial validation of the spanish childhood trauma questionnaire-short form: factor structure, reliability and association with parenting. J Interpers Violence. (2013) 28:1498–518. doi: 10.1177/0886260512468240
38. Gutiérrez B, Bellón JÁ, Rivera M, Molina E, King M, Marston L, et al. The risk for major depression conferred by childhood maltreatment is multiplied by BDNF and SERT genetic vulnerability: a replication study. J Psychiatry Neurosci JPN. (2015) 40:187–96. doi: 10.1503/jpn.140097
39. Brustenghi F, Mezzetti FAF, Di Sarno C, Giulietti C, Moretti P, Tortorella A. Eating disorders: the role of childhood trauma and the emotion dysregulation. Psychiatr Danub. (2019) 31:509–11.
40. Devi F, Shahwan S, Teh WL, Sambasivam R, Zhang YJ, Lau YW, et al. The prevalence of childhood trauma in psychiatric outpatients. Ann Gen Psychiatry. (2019) 18:15. doi: 10.1186/s12991-019-0239-1
41. Lee I, Strawn JR, Dwivedi AK, Walters M, Fleck A, Schwieterman D, et al. Childhood trauma in patients with self-reported stress-precipitated seizures. Epilepsy Behav EB. (2015) 51:210–4. doi: 10.1016/j.yebeh.2015.07.019
42. Xie W, Li H, Zou Y, Sun X, Shi C. A suicidal mind tends to maintain less negative information in visual working memory. Psychiatry Res. (2018) 262:549–57. doi: 10.1016/j.psychres.2017.09.043
43. Li X-B, Liu J-T, Zhu X-Z, Zhang L, Tang Y-L, Wang C-Y. Childhood trauma associates with clinical features of bipolar disorder in a sample of chinese patients. J Affect Disord. (2014) 168:58–63. doi: 10.1016/j.jad.2014.06.017
44. Bernstein DP, Fink L. Childhood Trauma Questionnaire A Retrospective Self-Report Manual San Antonio, TX The Psychological Corporation. (1998) Available online at: https://www.scirp.org/(S(351jmbntvnsjt1aadkposzje))/reference/ReferencesPapers.aspx?ReferenceID=593187 (accessed March 17, 2020).
45. Wechsler D. WAIS-IV. Escala de inteligencia de wechsler para adultos-IV. manual de aplicación y corrección. Madrid: NCS Pearson. (2012)
46. Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. (1994) 50:7–15. doi: 10.1016/0010-0277(94)90018-3
47. Heaton R. Wisconsin card sorting test manual. Psychological assessment resource. Incl Odess. (1981).
49. Buriel Y, Casanova JP, Rodés E, Fombuena NG, Böhm P. Fluencia verbal. Estudio normativo piloto en una muestra española de adultos jóvenes (20 a 49 años). Neurol Publ Soc Esp Neurol. (2004) 19:153–9.
50. Bernardo M, Bioque M, Parellada M, Ruiz JS, Cuesta MJ, Llerena A, et al. Assessing clinical and functional outcomes in a gene–environment interaction study in first episode of psychosis (PEPs). Rev Psiquiatr Salud Ment Engl Ed. (2013) 6:4–16. doi: 10.1016/j.rpsmen.2012.11.001
51. Cuesta MJ, Sánchez-Torres AM, Cabrera B, Bioque M, Merchán-Naranjo J, Corripio I, et al. Premorbid adjustment and clinical correlates of cognitive impairment in first-episode psychosis. The PEPsCog study. Schizophr Res. (2015) 164:65–73. doi: 10.1016/j.schres.2015.02.022
52. Adan A, Capella MDM, Prat G, Forero DA, López-Vera S, Navarro JF. Executive functioning in men with schizophrenia and substance use disorders. Influence of lifetime suicide attempts. PLoS ONE. (2017) 12:e0169943. doi: 10.1371/journal.pone.0169943
53. Keilp JG, Gorlyn M, Russell M, Oquendo MA, Burke AK, Harkavy-Friedman J, et al. Neuropsychological function and suicidal behavior: attention control, memory and executive dysfunction in suicide attempt. Psychol Med. (2013) 43:539–51. doi: 10.1017/S0033291712001419
54. Keilp JG, Gorlyn M, Oquendo MA, Burke AK, Mann JJ. Attention deficit in depressed suicide attempters. Psychiatry Res. (2008)159:7–17. doi: 10.1016/j.psychres.2007.08.020
55. Keilp JG, Wyatt G, Gorlyn M, Oquendo MA, Burke AK, John Mann J. Intact alternation performance in high lethality suicide attempters. Psychiatry Res. (2014) 219:129–36. doi: 10.1016/j.psychres.2014.04.050
56. Richard-Devantoy S, Gorwood P, Annweiler C, Olié J-P, Le Gall D, Beauchet O. Suicidal behaviours in affective disorders: a deficit of cognitive inhibition? Can J Psychiatry Rev Can Psychiatr. (2012) 57:254–62. doi: 10.1177/070674371205700409
57. Castellano S, Torrent C, Petralia MC, Godos J, Cantarella RA, Ventimiglia A, et al. Clinical and neurocognitive predictors of functional outcome in depressed patients with partial response to treatment: one year follow-up study. Neuropsychiatr Dis Treat. (2020) 16:589–95. doi: 10.2147/NDT.S224754
58. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex ‘frontal lobe' tasks: a latent variable analysis. Cognit Psychol. (2000) 41:49–100. doi: 10.1006/cogp.1999.0734
59. Gläscher J, Adolphs R, Damasio H, Bechara A, Rudrauf D, Calamia M, et al. Lesion mapping of cognitive control and value-based decision making in the prefrontal cortex. Proc Natl Acad Sci USA. (2012) 109:14681–6. doi: 10.1073/pnas.1206608109
60. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function. Ann Rev Neurosci. (2001) 24:167–202. doi: 10.1146/annurev.neuro.24.1.167
61. Grissom NM, Reyes TM. Let's call the whole thing off: evaluating gender and sex differences in executive function. Neuropsychopharmacol Off Publ Am Coll Neuropsychopharmacol. (2019) 44:86–96. doi: 10.1038/s41386-018-0179-5
62. Lerner J, Li Y, Valdesolo P, Kassam KS. Emotion and Decision Making. Report No.: ID 2547444 Rochester, NY: Social Science Research Network (2015). Available online at: https://papers.ssrn.com/abstract=2547444 (accessed April 29 2019)
63. Phelps EA, Lempert KM, Sokol-Hessner P. Emotion and decision making: multiple modulatory neural circuits. Annu Rev Neurosci. (2014) 37:263–87. doi: 10.1146/annurev-neuro-071013-014119
64. Bredemeier K, Miller IW. Executive function and suicidality: a systematic qualitative review. Clin Psychol Rev. (2015) 40:170–83. doi: 10.1016/j.cpr.2015.06.005
65. Jiménez E, Arias B, Mitjans M, Goikolea JM, Ruíz V, Brat M, et al. Clinical features, impulsivity, temperament and functioning and their role in suicidality in patients with bipolar disorder. Acta Psychiatr Scand. (2016) 133:266–76. doi: 10.1111/acps.12548
66. Marcus SM, Young EA, Kerber KB, Kornstein S, Farabaugh AH, Mitchell J, et al. Gender differences in depression: findings from the STAR*D study. J Affect Disord. (2005) 87:141–50. doi: 10.1016/j.jad.2004.09.008
67. Riecher-Rössler A. Prospects for the classification of mental disorders in women. Eur Psychiatry J Assoc Eur Psychiatr. (2010) 25:189–96. doi: 10.1016/j.eurpsy.2009.03.002
68. Giltay EJ, Enter D, Zitman FG, Penninx BWJH, van Pelt J, Spinhoven P, et al. Salivary testosterone: associations with depression, anxiety disorders, and antidepressant use in a large cohort study. J Psychosom Res. (2012) 72:205–13. doi: 10.1016/j.jpsychores.2011.11.014
69. Kumsar S, Kumsar NA, Saglam HS, Köse O, Budak S, Adsan Ö. Testosterone levels and sexual function disorders in depressive female patients: effects of antidepressant treatment. J Sex Med. (2014) 11:529–35. doi: 10.1111/jsm.12394
70. Zagni E, Simoni L, Colombo D. Sex and gender differences in central nervous system-related disorders. Neurosci J. (2016) 2016:2827090. doi: 10.1155/2016/2827090
71. Labaka A, Goñi-Balentziaga O, Lebeña A, Pérez-Tejada J. Biological sex differences in depression: a systematic review. Biol Res Nurs. (2018) 20:383–92. doi: 10.1177/1099800418776082
72. Alexopoulos GS, Manning K, Kanellopoulos D, McGovern A, Seirup JK, Banerjee S, et al. Cognitive control, reward-related decision making and outcomes of late-life depression treated with an antidepressant. Psychol Med. (2015) 45:3111–20. doi: 10.1017/S0033291715001075
73. Cotrena C, Branco LD, Kochhann R, Shansis FM, Fonseca RP. Quality of life, functioning and cognition in bipolar disorder and major depression: a latent profile analysis. Psychiatry Res. (2016) 241:289–96. doi: 10.1016/j.psychres.2016.04.102
74. Bahk Y-C, Jang S-K, Choi K-H, Lee S-H. The relationship between childhood trauma and suicidal ideation: role of maltreatment and potential mediators. Psychiatry Investig. (2017) 14:37–43. doi: 10.4306/pi.2017.14.1.37
75. Jiménez-Treviño L, Saiz PA, García-Portilla MP, Blasco-Fontecilla H, Carli V, Iosue M, et al. 5-HTTLPR-brain-derived neurotrophic factor (BDNF) gene interactions and early adverse life events effect on impulsivity in suicide attempters. World J Biol Psychiatry Off J World Fed Soc Biol Psychiatry. (2019) 20:137–49. doi: 10.1080/15622975.2017.1376112
76. Zelazny J, Melhem N, Porta G, Biernesser C, Keilp JG, Mann JJ, et al. Childhood maltreatment, neuropsychological function and suicidal behavior. J Child Psychol Psychiatry. (2019) 60:1085–93. doi: 10.1111/jcpp.13096
77. O'Brien BS, Sher L. Child sexual abuse and the pathophysiology of suicide in adolescents and adults. Int J Adolesc Med Health. (2013) 25:201–5. doi: 10.1515/ijamh-2013-0053
78. Carvalho JN, Renner AM, Donat JC, de Moura TC, Fonseca RP, Kristensen CH. Executive functions and clinical symptoms in children exposed to maltreatment. Appl Neuropsychol Child. (2020) 9:1–12. doi: 10.1080/21622965.2018.1497989
79. Dannehl K, Rief W, Euteneuer F. Childhood adversity and cognitive functioning in patients with major depression. Child Abuse Negl. (2017) 70:247–54. doi: 10.1016/j.chiabu.2017.06.013
80. Salagre E, Solé B, Tomioka Y, Fernandes BS, Hidalgo-Mazzei D, Garriga M, et al. Treatment of neurocognitive symptoms in unipolar depression: a systematic review and future perspectives. J Affect Disord. (2017) 221:205–21. doi: 10.1016/j.jad.2017.06.034
81. Miret M, Ayuso-Mateos JL, Sanchez-Moreno J, Vieta E. Depressive disorders and suicide: epidemiology, risk factors, and burden. Neurosci Biobehav Rev. (2013) 37:2372–4. doi: 10.1016/j.neubiorev.2013.01.008
Keywords: suicide, major depressive disorders, cognition, executive function, trauma
Citation: Fernández-Sevillano J, Alberich S, Zorrilla I, González-Ortega I, López MP, Pérez V, Vieta E, González-Pinto A and Saíz P (2021) Cognition in Recent Suicide Attempts: Altered Executive Function. Front. Psychiatry 12:701140. doi: 10.3389/fpsyt.2021.701140
Received: 27 April 2021; Accepted: 01 June 2021;
Published: 22 July 2021.
Edited by:
Javier Ortuño Sierra, University of La Rioja, SpainReviewed by:
Adriana Díez-Gómez, University of La Rioja, SpainCopyright © 2021 Fernández-Sevillano, Alberich, Zorrilla, González-Ortega, López, Pérez, Vieta, González-Pinto and Saíz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana González-Pinto, YW5hbWFyaWEuZ29uemFsZXotcGludG9hcnJpbGxhZ2FAb3Nha2lkZXR6YS5ldXM=
†These author contributed equally and share last and senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.