
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 21 September 2021
Sec. Psychopharmacology
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.699748
This article is part of the Research TopicNeurobiological Underpinnings of Cognitive Impairment and Pharmacological TreatmentsView all 6 articles
 Amber N. Edinoff1*
Amber N. Edinoff1* Prithvi K. Doppalapudi1Claudia Orellana1
Prithvi K. Doppalapudi1Claudia Orellana1 Caroline Ochoa2Shelby Patti2Yahya Ghaffar2
Caroline Ochoa2Shelby Patti2Yahya Ghaffar2 Elyse M. Cornett3Aaron J. Kaye4Omar Viswanath5,6,7
Elyse M. Cornett3Aaron J. Kaye4Omar Viswanath5,6,7 Ivan Urits3,8
Ivan Urits3,8 Adam M. Kaye9Alan D. Kaye3
Adam M. Kaye9Alan D. Kaye3Given the typical age onset of schizophrenia, there are tremendous economic and social impacts that extend beyond the person and their families. One critical determinant of the diseases' impact is the patient's adherence to antipsychotic drug treatment. Approved in 2015 for the treatment of schizophrenia, paliperidone palmitate (Invega Trinza, a 3-month injection, noted as PP3M) is a second-generation long-acting injectable antipsychotic medication. Among the different formulations offered for palmitate paliperidone, including the 1 and 3-month formulations, the longer duration 3-month formulation was better at preventing relapse in schizophrenic patients. To date, different formulations of palmitate paliperidone that have been studied on relapse episodes of schizophrenia include once-daily extended-release oral paliperidone (ORAL paliperidone), once-monthly paliperidone palmitate (PP1M), and once-every-3-months paliperidone palmitate (PP3M). Post-hoc analyses show that patients who were withdrawn from PP1M paliperidone had the least risk of relapse, followed by patients withdrawn from PP3M and patients withdrawn from ORAL paliperidone. PP3M was better at preventing relapse compared to ORAL paliperidone. The results demonstrated that 50% of patients who were withdrawn from ORAL paliperidone, PP1M, or PP3M remained relapse-free for ~2, 6, and 13 months, respectively. Compared to PP1M, PP3M is just as safe and effective and has the added advantage of increased adherence related to a longer dose interval, decreasing the risk of relapse.
Schizophrenia is a complex and often misunderstood mental illness that can be severely debilitating if left untreated (1). First characterized around the mid-to-late- 19th century, schizophrenia was initially described as an early form of dementia and was called “dementia praecox,” meaning “early dementia” (2). In the early 20th century, the term “schizophrenia” was used instead to distinguish mental illness from dementia and other neuropsychiatric disorders (2). Since then, technological and psychosocial advancements such as genetic testing and cognitive-behavioral therapy have drastically improved the way we understand and treat schizophrenia. However, certain aspects of the disease remain a mystery (3, 4).
Affecting ~1% of the world's population, roughly 78 million people worldwide and 2.4 million in the US, schizophrenia is one of the top 15 leading causes of disability worldwide (5). The disease often presents in early adulthood between the ages of 20 and 45, with men exhibiting symptoms in their early 20's and women in their mid-twenties to early 30's (6, 7). For affected people, all aspects of their daily lives are affected, and they have a lower life expectancy and overall quality of life (1, 8). Given the young age of onset in schizophrenia and the type of care required for patients, there are remarkable economic and social impacts that extend beyond the person and their families (9). For example, it was estimated that in 2013, ~$155 billion was spent on direct and indirect costs associated with schizophrenia, which is 2.5 times more than the approximate $62 billion spent in 2002 (8, 9). One critical determinant of the diseases' impact is the patient's adherence to antipsychotic drug treatment, which can be complicated by a number of isolated and interrelated factors such as access to care and socioeconomic status (10). Consequently, vulnerable patient populations such as low-income, minorities, and the homeless are most at risk for relapses in treatment related to lower medication adherence, resulting in uncontrolled symptoms and ultimately poorer health outcomes (9).
The use of long acting injectables (LAI) is a debated topic in the field of psychiatry. It is argued that the use of LAIs very early in the course of treatment can be very desirable as an estimated half of patients hospitalized for a first episode of psychosis discontinue their medication after being discharged (11). A study performed by Bartzokis et. al looked at the use of oral risperidone and the use of an LAI on the impact of intracortical myelination (ICM) trajectory in the first episode of schizophrenia. The authors found the ICM volume increased significantly in the LAI group and non-significantly in the oral risperidone group (12). The authors suggest that using a LAI may modify the ICM volume due to either better adherence to the medications or a different pharmacokinetic profile. Another study compared paliperidone palmitate, a 1-month LAI, with oral antipsychotic therapy. The study found that paliperidone palmitate was associated with a significant delay in time to first treatment failure vs. oral antipsychotics with overall treatment failure over 15 months being 38.8 vs. 53.7% (13). This study illustrated the real world management of schizophrenia using a 1-month LAI which demonstrated a longer time to treatment failure when compared to oral antipsychotics (13).
PP3M has shown a longer time to relapse and good safety and tolerability in many studies (14). However, its approval was met with resistance which highlighted concerns that this dosing interval would lead to less frequent doctor visits which could negatively affect the therapeutic relationship (15). This report also argued that the longer dosing interval would actually lower adherence to treatment as a whole (15). They concluded that more clinical studies should be conducted prior to the approval of PP3M to assess its safety and efficacy.
Two randomized control trials (RTCs) were used to elevate the authorization of the 3-month injection of paliperidone palmitate (PP3M). The first was by Berwaerts et al. which looked at PP3M vs. placebo for relapse prevention in schizophrenia. This study showed that the time to first relapse was significantly different in the PP3M group when compared to placebo (16). The second study was by Savitz et al. in 2016. This study was a double blind, paraellel-group multicenter phase 3 trial that was designed to test PP3M to the currently available 1-month formulation. The patients in this study were previously stabilized on the 1-month formulation. The authors found no clinically relevant differences in pharmacokinetic exposures and that PP3M was non-inferior to the 1-month with similar relapse rates (17). The authors concluded that the PP3M could offer a unique dosing option for relapse prevention in some patients. This manuscript examines the use of PP3M which shows promise in preventing relapse rates with its longer dosing interval and aims to examine the studies regarding its safety, efficacy, and clinical utility as a narrative review with the more current studies available.
There is also an increased risk for future schizophrenia diagnosis after a presentation of an unspecified psychosis. According to Hensel et al., 1 in 4 persons diagnosed with unspecified psychotic disorder will receive a schizophrenia diagnosis after 2 years (18). Also, once patients have already been diagnosed with schizophrenia and have begun treatment, relapse is a possibility when patients are non-adherent to their regimens (19, 20).
There are three classes of findings used to diagnose schizophrenia: positive symptoms, negative symptoms, and cognitive impairment (21). Positive symptoms are also referred to as psychotic symptoms and are generally episodic in nature. They include the presence of hallucinations, delusions, or bizarre behaviors and/or beliefs. There are various classifications of hallucinations and delusions, but the common denominator is they all indicate a loss of contact with reality. According to the DSM 5, hallucinations or delusions must be present to indicate a diagnosis of schizophrenia. Negative symptoms, on the other hand, are more consistent over time and are all strongly associated with poor psychosocial functioning. These symptoms include a diminish or absence of basic emotional and behavioral states. For instance, monotonous vocal tone, immobile facial expressions, and quality of speech are examples of negative symptoms. The last set of findings in a patient with schizophrenia, the presence of cognitive impairment, are relatively intuitive. These symptoms consist of difficulties with learning, memory, attention, concentration, abstract thinking, and problem-solving (21).
Existing medications for the treatment of schizophrenia work by improving only positive symptoms such as agitation, hallucinations, delusions, and aggression (22). However, these medications are not as effective at preventing negative symptoms (23). Table 1 discusses antipsychotics.
Table 1. Basic mechanism of action of antipsychotics.
The only known mechanism of action of medications that are approved for the treatment of schizophrenia is the blocking of dopaminergic neurotransmission (24). This has been seen in studies looking at PET studies in patients with first break schizophrenia. Kapur et al. looked at patients prior to receiving haloperidol and 2 weeks after starting treatment. They found patients showed a wide range of D2 occupancy and the greater degree of receptor occupancy predicted clinical improvement as well as such as hyperprolactinemia and extrapyramidal side effects (25). This is consistent with the theory of a dysfunction in dopaminergic neurotransmission.
Evidence suggests that not only is the dysfunction of dopaminergic receptors responsible for the symptoms of schizophrenia, but the pathogenesis of schizophrenia also involves dysfunction of multiple signaling systems outside of the dysfunction in dopaminergic signaling (26). These systems mainly include glutamatergic, serotonergic, adrenergic, and cholinergic signaling systems (23). Therefore, new medications are being tested in Phase II and Phase III clinical trials that work on serotonin, glutamate, adrenergic, and acetylcholinergic receptors (23).
Examples of these drugs include brexpiprazole, RP-5063, and eltroprazine, which work on the malfunctioning serotonergic system (22). ADX-7114 modulates the glutamate system (26), Neboglamine modulates the adrenergic system, and ABT-126 and encenicline modulate the cholinergic system (22).
The rationale behind inhibiting the dopaminergic neurotransmission for the treatment of schizophrenia is by inhibiting the dopamine D2 receptor in the mesolimbic pathway, the psychotic symptoms of schizophrenia can be inhibited (23). On the other hand, blocking the transmission of serotonin can increase the release of dopamine in the prefrontal cortex and improve negative symptoms and cognitive impairment associated with schizophrenia (27). The agonism of the cholinergic system by nicotinic a-7 receptors is used in the control of cognitive functions associated with schizophrenia (22). Therefore, nicotinic a-7 agonists have been suggested as adjuncts to treatments that improve cognitive impairment associated with schizophrenia (23). Nicotinic agonists are used mainly for controlling the cognitive symptoms associated with schizophrenia, whereas muscarinic agonists are used to control the positive symptoms (22). The dysfunction of the glutamatergic system contributes to the development of schizophrenia in terms of negative symptoms, cognitive deficits and, possibly also positive symptoms (23). Therefore, pharmacologic modulation of this system is of great recent interest (27).
One question that can arise is, which drugs are more effective at preventing relapses and treating schizophrenia as compared to other drugs (28)? A nationwide cohort of ~30,000 patients with schizophrenia showed that clozapine and long-acting injectable antipsychotic medications prevented relapse most effectively (28).
Another important consideration is how long should the treatment be continued (29)? Relapse rates are extremely high when antipsychotic treatment is discontinued, even when the patient has suffered only a single episode of psychosis (30). Even though relapse poses serious psychological and biological consequences, there are currently no reliable predictors of relapse (29). However, treatment continued for too long leads to a poorer long-term outcome (31). Overall, whichever treatment is used for the patient, it is still best for clinicians to maintain patients on a constant low-dose, well-tolerated antipsychotic than stopping patients completely (29).
The negative symptoms associated with schizophrenia strongly affect functional outcomes; hence research and development of new drugs are important (22). However, attempts at developing anti-schizophrenia medications have had limited progress in treating negative symptoms (26). Further research is being conducted to elucidate how to improve medications to better control these symptoms (22).
Although the exact mechanism of action of paliperidone is unclear, it is in a pathway similar to risperidone (32). That is because paliperidone is the active metabolite of risperidone. The difference between the two is the addition of a hydroxyl group in paliperidone (32). Both risperidone and paliperidone have similar binding affinities for certain receptor subtypes, there are several distinctions that are pharmacological meaningful. The differences are in the 5HT2A/D2 affinity and it is hypothesized that this difference can affect mitochondrial movement and therefore calcium homeostasis, synaptic plasticity, and neuronal firing (32). In addition to these receptors, there is differential binding to histamine, adrenergic, and cholinergic receptors. Risperidone is thought to have antagonism at the alpha 1 and alpha 2 adrenergic and H1 receiptors which may contribute to the therapeutic response as well as its adverse effects (32). Paliperidone, on the other hand, is thought to exhibit weaker affinity for the alpha 1 and alpha 2 adrenergic receptors when compared to risperidone. Other studies suggest that there is no affinity of cholinergic, muscarinic, and beta 1 and beta 2 adrenergic receptors. Paliperidone has an affinity for 5HT1D, 5HT2B, 5HT7 and D3 receptors, however, the inhibition constant values for binding to D2 and 5HT2A receptors are lower than for risperidone (32). The PP3M formulation uses NanoCrystal technology similar to its predecessor, the PP1M, but is superior in its extended sustained release capability due to an increased particle size (33).
Paliperidone palmitate (Invega Trinza, a 3-month injection, noted as PP3M) was approved by the U.S. Food and Drug Administration (FDA) in 2015 for the treatment of schizophrenia and is a second-generation (atypical) long-acting injectable (LAI) antipsychotic medication (34). Its active ingredient is paliperidone, an atypical antipsychotic that is the metabolite of risperidone, another first-generation antipsychotics (9). At the time of FDA approval, PP3M was the only antipsychotic LAI with a 3-month interval and, in addition to treating schizophrenia, is used for schizoaffective disorder and as an adjunct to mood stabilizers or antidepressants in adults (34, 35).
Patients taking PP3M must be closely monitored for changes such as cognitive and/or motor impairment, weight, blood levels, and decreased cardiovascular function, among others (12). Atypical antipsychotics, in general, have a degree of metabolic complications such as hyperlipidemia, hyperglycemia, and QT prolongation. Additionally, certain populations are at a greater risk for complications or death while using these medications, including elderly patients with dementia-related psychosis and with renal or hepatic impairment, Parkinson's dementia, or Lewy body dementia (35, 36). The safety and effectiveness in children under 18 have not been established, and pregnant women should be advised of the potential fetal risk (36).
There is a transition period before starting PP3M to safely introduce the medication to the patient (36). First, the patient must be started on a trial of oral risperidone or paliperidone to ensure tolerability and to monitor for potential side effects before being transitioned to a LAI. Once an LAI is started, patients must be stabilized on Invega Sustenna (PP1M), the 1-month version of paliperidone palmitate, for at least 4 months, with the last 2 months at the same dose (35). Only then may patients be converted to PP3M at a dose about 3.5 times higher than the last administered dose of PP1M (35, 36). PP3M is then administered in place of the next scheduled monthly injection, then every 3 months thereafter (35). The injection can be given either 1 week early or 1 week late due to scheduling issues with the patient. However, it is not approved for early injection due to treatment failure or due to the drug “wearing-off” early.
PP3M can only be administered by a healthcare professional and only using the thin wall needles provided in the INVEGA TRINZA® or INVEGA SUSTENNA® kits (35, 36). One dose is meant for a single intramuscular injection, and the syringe must be shaken within 5 min of injection to prevent an incomplete administration (35). If a patient misses an injection, they have up to 2.5 and 3.5 months to receive their dose (36). For missed doses of 3.5–4 months, the previously administered dose should be given immediately and then continue with the 3-month injections following this dose (36). For a missed dose of 4–9 months, they should not receive the next dose and must start a re-initiation regimen, and for missed doses that are >9 months, the patient will re-initiate treatment with PP1M before starting again with PP3M (36).
Recently, Janssen submitted a supplemental New Drug Application (sNDA) to the FDA for a 6-month formulation of Paliperidone Palmitate (PP6M) and will submit a Marketing Authorization Application extension to the European Medicines Agency (EMA) later this year (37). With an increased dosing regimen interval, the PP6M formulation hopes to offer greater flexibility and control to patients and providers for schizophrenia treatment (37). Similar to the PP3M formulation, there will be a transition period, and patients will have to be stabilized on the PP1M and/or PP3M formulations (37).
In 2014, 32 out of ~11,000 patients in Japan died shortly after taking Xeplion, the brand name for PP1M in that country, during post-marketing monitoring (38, 39). The reported causes of death include sudden death (most cardiac in nature), suicide, neuroleptic malignant syndrome, and other diseases such as cancer (38, 40). An analysis of these deaths, funded by Janssen Research & Development LLC., found that although there was an increased mortality reporting rate in this population, there was no significant difference in the mortality incidence rates compared to those in interventional clinical studies in Japan and in observational patient cohorts (39). Additionally, this analysis found that more than 50% of those patients were of advanced age (50+), more than 70% were at an increased risk for cardiovascular disease, and many were taking multiple antipsychotics (39). Therefore, the study concluded that the observed death rate could not be definitively attributed to Xeplion (39). However, the warning was given to not use this LAI with other antipsychotics or in a mix that could be seen as polypharmacy.
Furthermore, a meta-analysis conducted in 2016 reviewed 52 random control trials of various LAI antipsychotics (LAI-APs) to assess the safety of LAIs and found no significant difference in the incidence of death between LAI-APs and oral antipsychotics or placebo treatment groups (40). When comparing the pooled LAI-APs group to the placebo group within the first 13 weeks of treatment, there was a downward trend in the mortality rate, but the authors noted this trend with caution due to a small sampling size (40). People with schizophrenia have an increased risk of cardiovascular disease (CDV), and a significant number of deaths result from CDV (41). This increased risk has been long established, but numerous genetic, environmental, and pharmacological factors complicate this relationship (42). In view of this and the study's results, it can be concluded that there is no significant increased risk in the mortality rate while on LAI-APs (40).
Following injection, PP3M dissolves slowly due to it being water-insoluble (36). After dissolving, paliperidone palmitate is hydrolyzed to paliperidone and absorbed into the bloodstream. The FDA reports that once in the bloodstream, the drug reaches maximum plasma concentrations after a median of 30–33 days (36). The distribution of the drug once in circulation varies depending on injection site. Deltoid muscle injections showed an 11–12% higher maximum serum concentration on average than gluteal muscle injections (36). In the same way, deltoid muscle injections had a mean steady-state ratio of 1.7, with gluteal muscle injections having a mean peak-to-trough ratio of 1.6 (36). Overall, the drug has shown to have a volume of distribution of about 1,960 L.
Similarly, half-life has proved to differ based on injection site. The FDA reports a median half-life of 84–95 days with deltoid administration and 118–139 days with gluteal administration (36). One possible explanation for this extended half-life is that the drug is not greatly metabolized by the liver. If the provider notices that it seems to be “wearing-off” early, they should consider gluteal over deltoid injections for the previously stated reasons. The FDA demonstrated that 59% of an oral immediate-release paliperidone is excreted unchanged a week after administration, insinuating that there are no liver isozymes, largely impacting the metabolism of the drug (36).
PP1M (Invega Sustenna) and PP3M (Invega Trinza) are both intramuscular injections of paliperidone palmitate used for long-lasting treatment of Schizophrenia. PP3M is a 3-month injection, meaning it is administered once every 3 months, while PP1M is administered once a month (11). PP3M is indicated for treatment only after patients have been treated with PP1M for 4 months, and it has shown to be effective and tolerated (43). The key advantage of either paliperidone palmitate injection is that they assist with non-compliance. Inconsistency with or absence of maintenance therapy is a key factor related to relapse in schizophrenia patients (19). Furthermore, up to 80% of patients with schizophrenia do not adhere to medication regimens. This can lead to hospitalization, episodes of psychotic behavior, and overall negative burdens on not only patients but also their families and society (20). Having long-lasting treatment options available helps to alleviate some of the non-compliant aspects of the patient population (20). PP3M has the added convenience of only being required every third month as opposed to monthly. Even when comparing the pharmacokinetics of the two, the exposure for a 3.5-fold higher dose of PP3M is similar to the corresponding dose of PP1M (36).
Clinical studies have been conducted recently to highlight the safety and efficacy of different medications used in the treatment of schizophrenia, especially in scenarios of non-adherence and lack of access (44). Of the many medications that have been studied, the most extensively studied medication is palmitate paliperidone, as it can be given in the injectable form and can be given for a long period of time (33). One such study compared the medication aripiprazole once-monthly 400 mg and paliperidone palmitate once-monthly on the Heinrichs–Carpenter Quality-of-Life Scale (QLS) (45). QLS is an accepted health-related quality of life measurement in schizophrenic patients (45). This study, conducted over a period of 28 weeks, showed that patients who had taken aripiprazole 400 mg had significant improvements in the metrics measured in QLS as compared to schizophrenic patients who were administered paliperidone palmitate (45).
Another similar study conducted demonstrated that among the different formulations offered for palmitate paliperidone, including the 3-month formulation and 1-month formulation, the 3-month formulation was better at preventing relapse in schizophrenic patients (44). Furthermore, another study conducted to compare the prevention in relapse in schizophrenic patients offered palmitate paliperidone 3-month formulation compared to placebo treatment showed that palmitate paliperidone 3-month formulation was better at preventing relapse (46). Moreover, schizophrenic patients who had been administered PP3M had fewer reported hospitalizations for psychiatric and social reasons as compared to patients who were given placebo (47).
It is interesting to note that the efficacy of palmitate paliperidone 3-month formulation was noted not only in the American population but was also noted in the Latin American population. A study conducted showed that Latin American patients administered palmitate paliperidone showed no new adverse effects as compared to American patients and patients from all over the world (17).
Other studies done on palmitate paliperidone are concerned with the half-life of the drug and relapse (48). The major concern is if different formulations of the drug with different half-lives affect schizophrenic patients who have discontinued the medication (49). The different formulations of palmitate paliperidone that have been studied to examine the effect of half-lives on relapse episodes of schizophrenia include once-daily extended-release oral paliperidone (ORAL paliperidone), once-monthly paliperidone palmitate (PP1M), and once-every-3-months paliperidone palmitate (PP3M) (48). Post-hoc analyses have shown that patients who were withdrawn from PP1M paliperidone had the least risk of relapse, followed by patients withdrawn from PP3M and patients withdrawn from ORAL paliperidone (48). PP3M was better at preventing relapse compared to ORAL paliperidone. The results demonstrated that 50% of patients who were withdrawn from ORAL paliperidone, PP1M, or PP3M remained relapse-free for ~2, 6, and 13 months, respectively (48).
Studies that have assessed and compared the pharmacokinetics, safety, and tolerability of PP3M with PP1M have shown that the overall difference between the two in these parameters is negligible (33, 50). Studies have also interestingly shown no difference in injection site pain between the two formulations regardless of dosage difference and volume difference (51). The studies also clarify that giving these medications once every 3 months is the best way to prevent relapse in schizophrenic patients (33). PP3M is still preferable as it has a longer dosing interval and thus can provide a unique treatment option to help patients achieve improvement in symptoms (52).
Retrospective analyses of population pharmacokinetics of paliperidone using a one-compartment model have shown the apparent clearance (CL), apparent volume of distribution (V), and a fraction of the absorbed dose (F3) to be approximately around 3.84 l/h, 1,960 L and 20.9%, respectively (53). These parameters change accordingly if there is rapid or slow absorption (53). Hence, this study supports the two saturable absorption hypothesis to be applicable for paliperidone after intramuscular administration of its long-acting 3-month formulation, palmitate ester (53). This study was also crucial as it highlighted that factors such as age, race, sex, body mass index, and injection site do not affect the pharmacokinetics and steady-state of paliperidone in patients undergoing such treatment (53). However, the study did show that the renal status of the patient did affect how well the drug was cleared (53). Table 2 summarizes the studies discussed in this section.
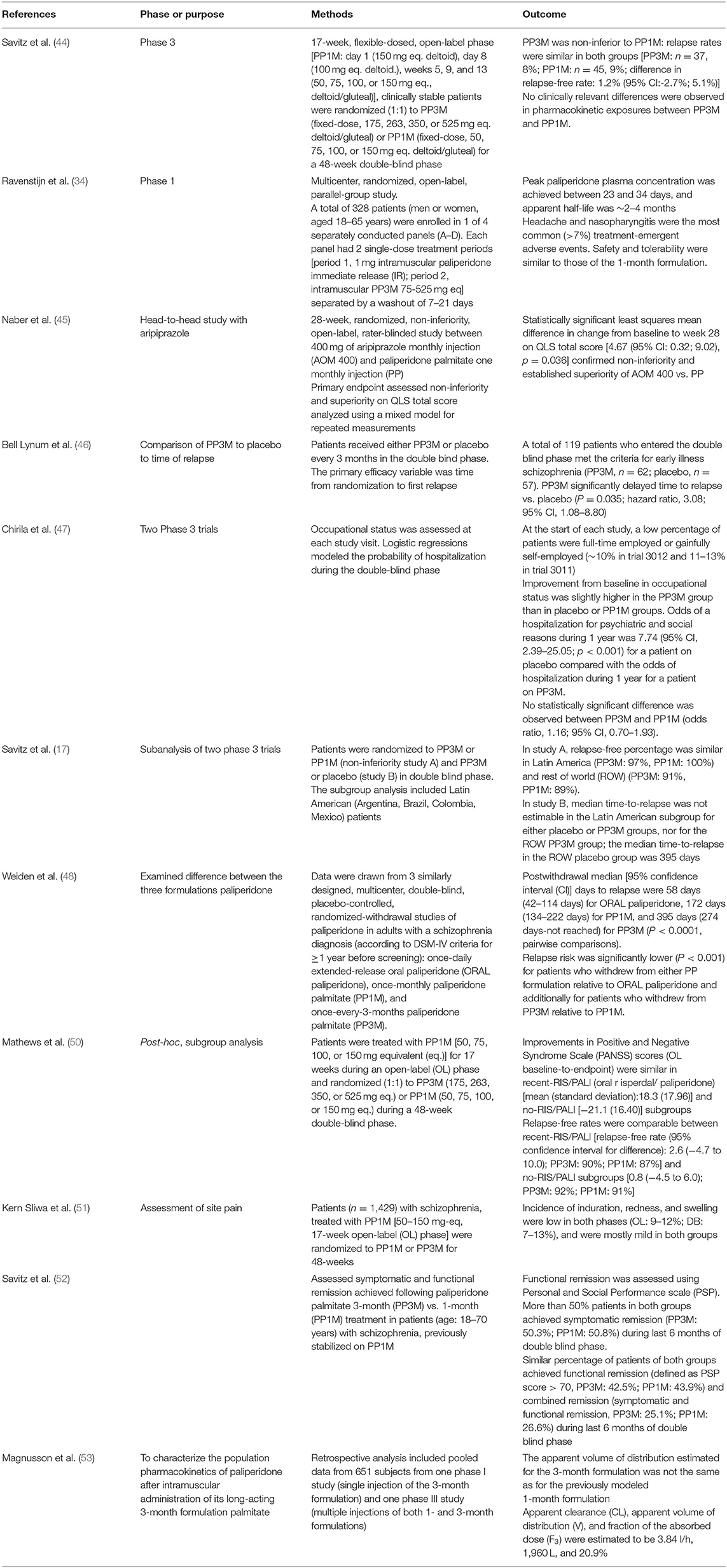
Table 2. Summary of clinical studies.
Schizophrenia is a complex and challenging psychiatric disorder involving a number of dysfunctions with interplaying biological and environmental factors (3, 20). Since its first description in the 19th century, the understanding of schizophrenia has vastly improved and expanded thanks to technological advancements such as gene linkage studies and diagnostic tools such as the DSM (54). Conversely, as research progresses in the classification and treatment of schizophrenia, certain aspects (i.e., treatment options) of the disease remain limited, and more unknowns persist, such as the etiopathogenesis (54).
Pharmacotherapy remains the key treatment for schizophrenia despite only treating the positive and not the negative symptoms (22, 23). However, the use of antipsychotic treatments is necessary to correct the dopamine imbalance, which will yield better results in psychosocial rehabilitation (20). Difficulty in medication management can affect and even derail long-term treatment goals for patients (9, 19). However, PP3M, and potentially the PP6M formulation, offers hope in treatment management. Compared to PP1M, PP3M is just as safe and effective but with the added advantage of increased adherence due to a longer dose interval, decreasing the risk of relapse (19, 44, 48). Despite some safety concerns regarding LAIs and PP3M, the data does not show a significant risk of death in patients taking PP3M or LAIs (38–40). Additionally, many confounding variables contributing to the lowered life spans of individuals with schizophrenia must be taken into account (8). Nevertheless, PP3M is an effective, long-acting treatment option that is enabling patients and providers to focus less on medication adherence and more on the treatment plan and long-term goals (34). Prescribers must consider that not all patients will respond to a LAI and may have to consider other atypical medication trials if the symptoms are not able to be controlled with the PP3M. More research should be done to assess the long term effects of the use of LAIs and to either confirm or refute PP3M, as well as other LAIs, as being a way to prevent disease relapse.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Schultz SK, Andreasen NC. Schizophrenia. Lancet. (1999) 353:1425–30. doi: 10.1016/S0140-6736(98)07549-7
2. Jablensky A. The diagnostic concept of schizophrenia: its history, evolution, and future prospects. Dialogues Clin Neurosci. (2010) 12:271–87. doi: 10.31887/DCNS.2010.12.3/ajablensky
3. Vértes PE, Seidlitz J. Towards a natural history of schizophrenia. Brain J Neurol. (2019) 142:3669–71. doi: 10.1093/brain/awz353
4. Tandon R, Gaebel W, Barch DM, Bustillo J, Gur RE, Heckers S, et al. Definition and description of schizophrenia in the DSM-5. Schizophrenia Res. (2013) 150:3–10. doi: 10.1016/j.schres.2013.05.028
5. Global regional and national incidence prevalence and years lived with disability for 328 diseases and injuries for 195 countries 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1211–59. doi: 10.1016/S0140-6736(17)32154-2
6. Messias EL, Chen CY, Eaton WW. Epidemiology of schizophrenia: review of findings and myths. Psychiatr Clin North Am. (2007) 30:323–38. doi: 10.1016/j.psc.2007.04.007
7. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. (2008) 30:67–76. doi: 10.1093/epirev/mxn001
8. Cloutier M, Aigbogun MS, Guerin A, Nitulescu R, Ramanakumar AV, Kamat SA, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. (2016) 77:764–71. doi: 10.4088/JCP.15m10278
9. Wander C. Schizophrenia: opportunities to improve outcomes and reduce economic burden through managed care. Am J Managed Care. (2020) 26 (3 Suppl.):S62–8. doi: 10.37765/ajmc.2020.43013
10. Bera RB. Patient outcomes within schizophrenia treatment: a look at the role of long-acting injectable antipsychotics. J Clin Psychiatry. (2014) 75 (Suppl. 2):30–3. doi: 10.4088/JCP.13065su1c.07
11. Watts V. Some experts urge more use of long-acting, injectable antipsychotics. Psychiatr News. (2014) 49:1–1. doi: 10.1176/appi.pn.2014.12a8
12. Bartzokis G, Lu PH, Raven EP, Amar CP, Detore NR, Couvrette AJ, et al. Impact on intracortical myelination trajectory of long acting injection versus oral risperidone in first-episode schizophrenia. Schizophrenia Res. (2012) 140:122–8. doi: 10.1016/j.schres.2012.06.036
13. Alphs L, Benson C, Cheshire-Kinney K, Lindenmayer JP, Mao L, Rodriguez SC, et al. Real-world outcomes of paliperidone palmitate compared to daily oral antipsychotic therapy in schizophrenia: a randomized, open-label, review board-blinded 15-month study. J Clin Psychiatry. (2015) 76:554–61. doi: 10.4088/JCP.14m09584
14. Role of 3-Monthly Long-Acting Injectable Paliperidone in the Maintenance of Schizophrenia. PsycNET. Available online at: https://psycnet.apa.org/record/2017-54225-001 (accessed August 1, 2021).
15. Ostuzzi G, Papola D, Gastaldon C, Barbui C. New EMA report on paliperidone 3-month injections: taking clinical and policy decisions without an adequate evidence base. Epidemiol Psychiatr Sci. (2017) 26:231. doi: 10.1017/S2045796016001025
16. Berwaerts J, Liu Y, Gopal S, Nuamah I, Xu H, Savitz A, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. (2015) 72:830–9. doi: 10.1001/jamapsychiatry.2015.0241
17. Savitz AJ, Xu H, Gopal S, Nuamah I, Mathews M, Soares B. Efficacy and safety of paliperidone palmitate 3-month formulation in latin american patients with schizophrenia: a subgroup analysis of data from two large phase 3 randomized, double-blind studies. Braz J Psychiatry. (2019) 41:499–510. doi: 10.1590/1516-4446-2018-0153
18. Hensel JM, Chartier MJ, Ekuma O, MacWilliam L, Mota N, Tachere RO, et al. Risk and associated factors for a future schizophrenia diagnosis after an index diagnosis of unspecified psychotic disorder: a population-based study. J Psychiatr Res. (2019) 114:105–12. doi: 10.1016/j.jpsychires.2019.04.019
19. Porcelli S, Bianchini O, De Girolamo G, Aguglia E, Crea L, Serretti A. Clinical factors related to schizophrenia relapse. Int J Psychiatry Clin Pract. (2016) 20:54–69. doi: 10.3109/13651501.2016.1149195
20. Daghistani N, Rey JA. Invega trinza: the first four-times-a-year, long-acting injectable antipsychotic agent. P T. (2016) 41:222–7.
21. Mueser KT, Mcgurk SR. Schizophrenia. Lancet. (2004) 363:2063–72. doi: 10.1016/S0140-6736(04)16458-1
22. Köster LS, Carbon M, Correll CU. Emerging drugs for schizophrenia: an update. Expert Opin Emerging Drugs. (2014) 19:511–31. doi: 10.1517/14728214.2014.958148
23. Yang AC, Tsai SJ. New targets for schizophrenia treatment beyond the dopamine hypothesis. Int J Mol Sci. (2017) 18:1689. doi: 10.3390/ijms18081689
24. Maric NP, Jovicic MJ, Mihaljevic M, Miljevic C. Improving current treatments for schizophrenia. Drug Dev Res. (2016) 77:357–67. doi: 10.1002/ddr.21337
25. Kapur S, Zipursky R, Jones C, Remington G, Houle S. Relationship between dopamine D(2) occupancy, clinical response, and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry. (2000) 157:514–20. doi: 10.1176/appi.ajp.157.4.514
26. Meltzer HY. New trends in the treatment of schizophrenia. CNS Neurol Disord Drug Targets. (2017) 16:900–6. doi: 10.2174/1871527316666170728165355
27. Stepnicki P, Kondej M, Kaczor AA. Current concepts and treatments of schizophrenia. Molecules. (2018) 23:2087. doi: 10.3390/molecules23082087
28. Tiihonen J, Mittendorfer-Rutz E, Majak M, Mehtälä J, Hoti F, Jedenius E, et al. Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29 823 patients with schizophrenia. JAMA Psychiatry. (2017) 74:686–93. doi: 10.1001/jamapsychiatry.2017.1322
29. Emsley R, Kilian S, Phahladira L. How long should antipsychotic treatment be continued after a single episode of schizophrenia? Curr Opin Psychiatry. (2016) 29:224–9. doi: 10.1097/YCO.0000000000000249
30. Kishimoto T, Agarwal V, Kishi T, Leucht S, Kane JM, Correll CU. Relapse prevention in schizophrenia: a systematic review and meta-analysis of second-generation antipsychotics versus first-generation antipsychotics. Mol Psychiatry. (2013) 18:53–66. doi: 10.1038/mp.2011.143
31. Alphs L, Nasrallah HA, Bossie CA, Fu DJ, Gopal S, Hough D, et al. Factors associated with relapse in schizophrenia despite adherence to long-acting injectable antipsychotic therapy. Int Clin Psychopharmacol. (2016) 31:202–9. doi: 10.1097/YIC.0000000000000125
32. Corena-McLeod M. Comparative pharmacology of risperidone and paliperidone. Drugs R D. (2015) 15:163–74. doi: 10.1007/s40268-015-0092-x
33. Ravenstijn P, Remmerie B, Savitz A, Samtani MN, Nuamah I, Chang C-T, et al. Pharmacokinetics, safety, and tolerability of paliperidone palmitate 3-month formulation in patients with schizophrenia: a phase-1, single-dose, randomized, open-label study. J Clin Pharmacol. (2016) 56:330–9. doi: 10.1002/jcph.597
34. Johnson & Johnson. U.S. FDA Approves INVEGA TRINZATM, First and Only Four-Times-A-Year Treatment for Schizophrenia (New Brunswick, NJ). (2015). p. 1–7.
35. Invega Trinza (Paliperidone Palmitate) Prescribing Information. Washington, DC. (2006). p. 1–14.
36. FDA Label. INVEGA TRINZA® (Paliperidone Palmitate) Extended-Release Injectable Suspension, for Intramuscular Use. Washington, DC. (2017). p. 1–55.
37. Johnson & Johnson. Janssen Submits Paliperidone Palmitate 6-Month (PP6M) Supplemental New Drug Application to US FDA for Treatment of Schizophrenia in Adults. New Brunswick, NJ. (2020). p. 13.
38. Fujii Y. What lessons should we learn from the death of patients on xeplion?. Seishin Shinkeigaku Zasshi. (2015) 117:132–45. (Japanese).
39. Pierce P, Gopal S, Savitz A, Qiu H, Hino T, Busch M, et al. Paliperidone palmitate: Japanese postmarketing mortality results in patients with schizophrenia. Curr Med Res Opin. (2016) 32:1671–9. doi: 10.1080/03007995.2016.1198755
40. Kishi T, Matsunaga S, Iwata N. Mortality risk associated with long-acting injectable antipsychotics: a systematic review and meta-analyses of randomized controlled trials. Schizophrenia Bull. (2016) 42:1438–45. doi: 10.1093/schbul/sbw043
41. Hennekens CH, Hennekens AR, Hollar D, Casey DE. Schizophrenia and increased risks of cardiovascular disease. Am Heart J. (2005) 150:1115–21. doi: 10.1016/j.ahj.2005.02.007
42. Jindal R, MacKenzie EM, Baker GB, Yeragani VK. Cardiac risk and schizophrenia. J Psychiatry Neurosci. (2005) 30:393–5.
43. National Drug Monograph. Paliperidone Palmitate (Invega Sustenna and Trinza). Washington, DC: National Drug Monograph. (2015) p. 1–17.
44. Savitz AJ, Xu H, Gopal S, Nuamah I, Ravenstijn P, Janik A, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. (2016) 19:pyw018. doi: 10.1093/ijnp/pyw018
45. Naber D, Hansen K, Forray C, Baker RA, Sapin C, Beillat M, et al. Qualify: a randomized head-to-head study of aripiprazole once-monthly and paliperidone palmitate in the treatment of schizophrenia. Schizophrenia Res. (2015) 168:498–504. doi: 10.1016/j.schres.2015.07.007
46. Bell Lynum KS, Turkoz I, Kim E. Paliperidone palmitate once-every-3-months in adults with early illness schizophrenia. Early Intervention Psychiatry. (2018) 13:667–72. doi: 10.1111/eip.12685
47. Chirila C, Nuamah I, Woodruff K. Health care resource use analysis of paliperidone palmitate 3 month injection from two phase 3 clinical trials. Curr Med Res Opin. (2017) 33:1083–90. doi: 10.1080/03007995.2017.1300144
48. Weiden PJ, Kim E, Bermak J, Turkoz I, Gopal S, Berwaerts J. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. (2017) 78:e813–20. doi: 10.4088/JCP.16m11308
49. Morris MT, Tarpada SP. Long-acting injectable paliperidone palmitate: a review of efficacy and safety. Psychopharmacol Bull. (2017) 47:42–52.
50. Mathews M, Pei H, Savitz A, Nuamah I, Hough D, Alphs L, et al. Paliperidone palmitate 3-monthly versus 1-monthly injectable in patients with schizophrenia with or without prior exposure to oral risperidone or paliperidone: a post hoc, subgroup analysis. Clin Drug Investig. (2018) 38:695–702. doi: 10.1007/s40261-018-0647-z
51. Kern Sliwa J, Savitz A, Nuamah I, Mathews M, Gopal S, Elefant E, et al. An assessment of injection site reaction and injection site pain of 1-month and 3-month long-acting injectable formulations of paliperidone palmitate. Perspect Psychiatr Care. (2018) 54:530–8. doi: 10.1111/ppc.12267
52. Savitz AJ, Xu H, Gopal S, Nuamah I, Hough D, Mathews M. Paliperidone palmitate 3-month treatment results in symptomatic remission in patients with schizophrenia: a randomized, multicenter, double-blind, and noninferiority study. Int Clin Psychopharmacol. (2017) 32:329–36. doi: 10.1097/YIC.0000000000000190
53. Magnusson MO, Samtani MN, Plan EL, Jonsson EN, Rossenu S, Vermeulen A, et al. Population pharmacokinetics of a novel once-every 3 months intramuscular formulation of paliperidone palmitate in patients with schizophrenia. Clin Pharmacokinetics. (2017) 56:421–33. doi: 10.1007/s40262-016-0459-3
Keywords: paliperidone, long-acting injectable, antipsychotic, schizophrenia, Invega Trinza
Citation: Edinoff AN, Doppalapudi PK, Orellana C, Ochoa C, Patti S, Ghaffar Y, Cornett EM, Kaye AJ, Viswanath O, Urits I, Kaye AM and Kaye AD (2021) Paliperidone 3-Month Injection for Treatment of Schizophrenia: A Narrative Review. Front. Psychiatry 12:699748. doi: 10.3389/fpsyt.2021.699748
Received: 24 April 2021; Accepted: 23 August 2021;
Published: 21 September 2021.
Edited by:
Wen Wang, Fourth Military Medical University, ChinaReviewed by:
Adele Stewart, Florida Atlantic University, United StatesCopyright © 2021 Edinoff, Doppalapudi, Orellana, Ochoa, Patti, Ghaffar, Cornett, Kaye, Viswanath, Urits, Kaye and Kaye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amber N. Edinoff, YWVkaW5vQGxzdWhzYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.