
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 28 July 2021
Sec. Molecular Psychiatry
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.698257
This article is part of the Research TopicNeuroinflammation, Metabolism, and Psychiatric DisordersView all 12 articles
 Chin-Chuen Lin1†
Chin-Chuen Lin1† Tiao-Lai Huang1,2*†
Tiao-Lai Huang1,2*†Background: Major depressive disorder (MDD) is associated with the activation of the immune/inflammatory system. TNF-α is associated with MDD and poor treatment response. Toll-like receptors (TLR) are responsible in innate immune response, and is associated with MDD and antidepressant response. Some negative regulators of TLR pathway such as SOCS1, TOLLIP, SIGIRR, TNFAIP3, and MyD88s, are reported to be differentially expressed in the peripheral blood samples of patients of MDD.
Methods: We recruited patients with MDD and healthy controls, collect their demographic data, and measured their mRNA levels of negative TLR regulators, using peripheral blood mononuclear cells (PBMC) and isolated TNF-α secreting cells. Clinical symptoms were evaluated using Halmiton Depression Rating Scale (Ham-D). Some patients were evaluated again after 4 weeks of antidepressant treatment.
Results: Forty-seven patients with MDD and 52 healthy controls were recruited. Between the PBMC samples of 37 MDD patients and 42 controls, mRNA levels of SOCS1, SIGIRR, TNFAIP3, and MyD88s were significantly different. Between TNF-α secreting cells of 10 MDD patients and 10 controls, mRNA levels of SIGIRR and TNFAIP3 were significantly different. Change of Ham-D score only correlated significantly with TOLLIP mRNA level after treatment.
Conclusion: SIGIRR and TNFAIP3, two negative regulators of TLR immune response pathways, were differentially expressed in both PBMC and TNF-α secreting cells of patients with MDD as compared to healthy controls. The negative regulations of innate immune response could contribute to the underlying mechanism of MDD.
Major depressive disorder (MDD) has been associated with the activation of the immune/inflammatory system, including changes in serum acute phase protein (1, 2) and cytokine levels (3–5). Antidepressant treatment has also been shown to normalize the inflammatory state, by decreasing serum levels of proinflammatory cytokines such as IL-12 and increasing serum levels of anti-inflammatory cytokines such as IL-4 and TGF-β1 (6). Increased plasma levels of IL-6 and TNF-α before treatment predicted poor antidepressant response (7, 8). A meta-analysis has shown that increased serum levels of TNF-α and IL-6 are the most replicated findings in MDD (9).
Toll-like receptors (TLRs) are the pattern recognition receptors that recognize pathogenic exogenous and endogenous molecular patterns and play an important role in the innate immune system. In humans, 10 TLRs (TLR-1 to 10) were characterized. TLR-1, 2, 4, 5, and 6 are at the cell membrane, detecting bacteria. For example, TLR-4 binds lipopolysaccharide in gram-negative bacteria. TLR-3, 7, 8, and 9 are located on intracellular endosomes, and detect nucleic acids from bacteria and viruses that have penetrated the cell. For example, TLR-7 binds single-stranded RNA from viruses as well as some endogenous proteins. After receptor binding, a cascade is initiated, leading to transcriptions of inflammatory cytokines (10). Prior studies have shown that TLR expressions were associated with MDD diagnosis (11) and depressive symptoms (12). Antidepressant treatment could normalize elevated TLR expressions prior to medications (13). In the recent years, attention has turned to negative regulators of TLR pathway, suggesting that dysfunction in the negative feedback loop could also contribute to the psychopathology of MDD (13, 14). Some of the more frequent investigated negative regulators include suppressor of cytokine signaling 1 (SOCS1), Toll-interacting protein (TOLLIP), single immunoglobulin interleukin-1-related receptor (SIGIRR), TNF-α-induced protein 3 (TNFAIP3), and the short form of MyD88 (MyD88s) (15).
Earlier studies regarding TLR expressions and their negative regulators used peripheral blood mononuclear cells (PBMC) as the analyzed sample (14), which contain a variety of cells. Recent advances in technology allowed isolation of specific types of cells, such as monocytes (16) and TNF-α secreting cells (17). As mentioned earlier, TNF-α is an important cytokine in MDD (9). Therefore, in this study, we intended to investigate the mRNA levels of five negative TLR regulators (SOCS1, TOLLIP, SIGIRR, TNFAIP3, and MyD88s) in PBMC and TNF-α secreting cells from patients of MDD, compared to the healthy controls and after antidepressant treatment.
From September 2017 to July 2018, hospitalized patients diagnosed with MDD were recruited at the Chang Gung Memorial Hospital. MDD was diagnosed by a psychiatrist according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Only patients aged between 20 and 65 years old were included. Patients with systemic diseases, such as cardiovascular diseases, liver diseases and thyroid diseases, smokers, or patients with alcohol dependence were excluded. The severity of depression was assessed by the 17-item Halmiton Depression Rating Scale (Ham-D) (18). The choice of antidepressants depended on what the clinicians considered best for the patients. Healthy controls were recruited and assessed by semi-structured interviews to rule out psychiatric disorder according to DSM-5 criteria. Written informed consent was provided by all participants after the content and context of the study was fully explained. The institutional review board (IRB) of Chang Gung Memorial Hospital approved the study design (IRB 201602052B0C501).
Venous blood of 15 ml was drawn from each participant in the morning following a 6-h fast. Peripheral blood mononuclear cells (PBMC) were isolated using Ficoll-Paque medium. TNF-α secreting cells were further isolated from PBMC using TNF-α Secretion Assay-Cell Enrichment and Detection Kit (Miltenyi Biotec, #130-091-269). Isolated cells were stored at −80°C until assay.
Quantitative reverse transcription-polymerase chain reaction (qRT-PCR) was performed using the following sets of primers: SOCS1 5′-GACCCCTTCTCA CCTCTTGA-3′ (sense) and 5′-GTAGGAGGTGCGAGTTCAGG-3′ (antisense); TOLLIP, 5′-GACAACTGTCTCCGTCGCA-3′ (sense) and 5′-CGGGAGCTCACCGATGTA-3′ (antisense); SIGIRR, 5′-CCCAGCTCTTGGATCAGTCT-3′ (sense) and 5′-AGTCAGGGGCCCTATCACAG-3′ (antisense); TNFAIP3, 5′-GGACTT TGCGAAAGGATC G-3′ (sense) and 5′-TCACAGCTTTCCGCATATTG-3′ (antisense); MyD88s, 5′-TCATCGAAAAGAGGTTGGCT-3′(sense) and 5′-GATGGG GATCAGTCGCTTCT-3′ (antisense); glyceraldehyde-3-phosphate dehydrogenase (GAPDH), 5′-TGCACCACC AACTGCTTAGC-3′ (sense) and 5′-GGCATGGACTGTGGTCATGAG-3′ (antisense).
The relative abundance of mRNAs was calculated with the comparative Ct method using GADPH as the housekeeping gene, represented by -ΔCt, to make comparisons with earlier studies possible. Fold changes were calculated with 2∧ − ΔΔCt.
All results are represented as mean ± standard deviation. Comparisons of study groups were calculated using independent t-test, Wilcoxan sign rank test, or Mann-Whitney U-Test. Pearson correlation was used to assess the relationship with the associated parameters. Data analysis was performed using SPSS 19 (Chicago, IL, U.S.A.). p-values of <0.05 were considered statistically significant.
Forty-seven patients with MDD and 52 healthy controls were recruited. Samples of 37 patients and 42 controls were analyzed for PBMC data. Thirteen patients were treated with antidepressants for 4 weeks, and their PBMC data were analyzed both at baseline and after treatment. Samples of 10 patients and 10 controls were analyzed for TNF-α secreting cells. Medications of the 37 MDD patients were summarized in Supplementary Table 1.
Between the PBMC samples of 37 MDD patients (12 males and 25 females) and 42 controls (18 males and 24 females), mRNA levels of SOCS1, SIGIRR, TNFAIP3, and MyD88s were significantly different, using independent t-test (p = 1.1 × 10−5, 2.0 × 10−8, 6.0 × 10−14, and 7.2 × 10−12, respectively). Their demographic data and mRNA levels were summarized in Table 1. Fold changes of MDD group were relative to the controls. No significant difference in GPDPH expression was found between MDD patients and controls. SOCS1 level correlated significantly with levels of TNFAIP3 and MyD88s (p = 0.001 and 0.014, respectively). SIGIRR level correlated significantly with BMI, Ham-D score, TNFAIP3 level, and MyD88s level (p = 0.026, 0.000, 0.000, and 0.000, respectively). TNFAIP3 level correlated significantly with BMI, SOCS level, SIGIRR level, and MyD88s level (p = 0.011, 0.001, 0.000, and 0.000, respectively). MyD88s level correlated significantly with BMI, Ham-D score, SOCS level, SIGIRR level, and TNFAIP3 level (p = 0.010, 0.000, 0.014, 0.000, and 0.000, respectively).
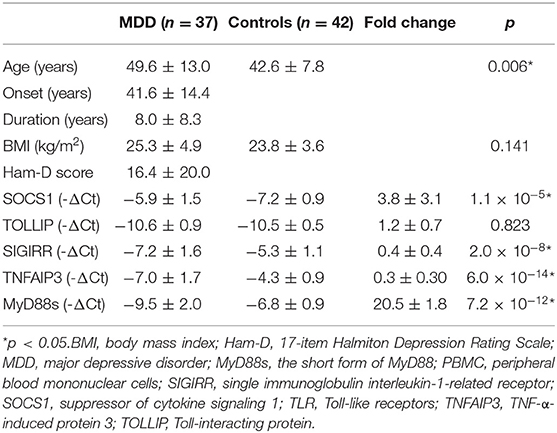
Table 1. Demographic data and mRNA levels of PBMC.
In the 13 treatment completers (1 male and 12 females), mRNA levels of PBMC did not differ significantly before and after treatment using Wilcoxan sign rank test, despite the significant decrease of Ham-D score. Their demographic data and mRNA levels were summarized in Table 2. Fold changes of post-treatment group were relative to the baseline. No significant difference in GPDPH expression was found before and after treatment. The demographic data of the treatment completers do not differ significantly from the 37-patient group, though the treatment completers had more severe depression at baseline. Change of Ham-D score only correlated significantly with TOLLIP mRNA level after treatment (p = 0.021).
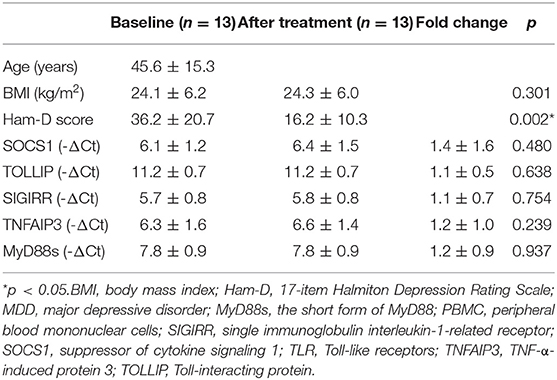
Table 2. Demographic data and mRNA levels of PBMC before and after antidepressant treatment.
Between TNF-α secreting cells of 10 MDD patients (1 male and 9 females) and 10 controls (2 males and 8 females), mRNA levels of SIGIRR and TNFAIP3 were significantly different, using Mann-Whitney U Test (p = 0.023 and 3.2 × 10−4, respectively). Their demographic data and mRNA levels were summarized in Table 3. Fold changes of MDD group were relative to the controls. No significant difference in GPDPH expression was found between MDD patients and controls. SIGIRR level correlated significantly with SOCS1 level and TNFAIP3 level (p = 0.000 and 0.001, respectively). TNFAIP3 level correlated significantly with SOCS1 level, SIGIRR level, and MyD88s level (p = 0.042, 0.001, and 0.004, respectively).
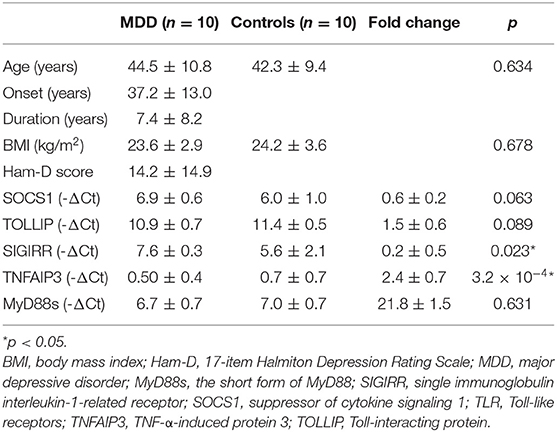
Table 3. Demographic data and mRNA levels from TNF-α secreting cells.
The most important finding of this study is that SIGIRR and TNFAIP3, two negative regulators of TLR immune response pathways, were differentially expressed in both PBMC and TNF-α secreting cells of patients with MDD as compared to healthy controls. While both SIGIRR and TNFAIP3 mRNA levels had been investigated in the PBMC of patients with MDD in the past (14), only TNFAIP3 mRNA level was reported in TNF-α secreting cells of patients with MDD before (17). To our knowledge, this is the first study to report the differential expression of SIGIRR in TNF-α secreting cells of patients with MDD as compared to healthy controls.
SIGIRR is a transmembrane TLR regulator, which binds to TLR4 and interleukin-1 receptor associated kinase (IRAK) to inhibit the downstream TLR signal pathways (15). In this study, SIGIRR were significantly lower in patients in MDD whether the samples were PBMC or TNF-α secreting cells. Previously, lower SIGIRR was found in PBMC in patients with MDD, but not statistically significant (14). In another study analyzing SIGIRR in monocyte sample of patients of MDD, significantly higher level of SIGIRR was found (16). We speculate that the lower SIGIRR in PBMC and TNF-α secreting cells indicate a deficiency to prevent TLR inflammation. Given most of the studies, including our own, had limited sample size, further investigations would be needed to confirm the significance of SIGIRR in TLR regulation in MDD.
TNFAIP3, also known as A20, is an intracellular TLR regulator, which deubiquitylates tumor-necrosis factor-receptor-associated factor 6 (TRAF6), thus inhibiting the downstream activation of NF-κB inflammatory pathway (15). TNFAIP3 is a potent regulator of dendritic spine remodeling and synapse efficacy in neurons (19). TNFAIP3 had been investigated in various samples from patients of MDD in the past, including PBMC, monocytes, and TNF-α secreting cells (14, 16, 17). In this finding, we found significantly lower TNFAIP3 mRNA level in patients with MDD, which was in line with earlier studies on PBMC (14) and monocytes (16). However, in the TNF-α secreting cells, we found significantly higher mRNA levels of TNFAIP3 in patients of MDD, while an earlier study also found higher TNFAIP levels, no statistical significance was found (17). While lower TNFAIP3 levels in PBMC and monocytes in patients of MDD could indicate a failed defense against TLR inflammation, the higher level found in TNF-α secreting cells in this study might also be an exaggerated response from the overall inflammatory state in patients of MDD. There had also been reports of abnormalities of TNFAIP3 in other psychiatric disorders. In the PBMC of adolescents diagnosed bipolar I disorder, TNFAIP3 mRNA level correlated with pediatric inpatient aggression prediction score, as well as functional brain activations of right anterior part of anterior cingulate gyrus, a part of aggression pathway (20). Significantly higher levels TNFAIP3 mRNA levels were found in the monocytes of patients of bipolar disorder (21). The abnormalities of TLR pathway negative regulators could also be found in psychiatric disorders other than MDD.
We also found SOCS1 to be statistically higher and MyD88s to be statistically lower in PBMC of patients of MDD, though no statistical significance was found in TNF-α secreting cells. SOCS1 suppresses IRAK to prevent inflammatory response initiated by TLR 4 and 9 (15, 22, 23). In our study, significantly higher SOCS1 level was found in PBMC of patients with MDD. Previously, significantly higher SOCS1 was also found in the monocytes of patients of MDD (16), but not in PBMC (14). SOCS1 had also been investigated in other mood disorder, namely bipolar disorder. SOCS1 mRNA levels were also significantly higher in patients with bipolar disorder, but this finding remained positive in male patients only if different genders were analyzed separately (24). SOCS1 could also contribute to the innate immune responses associated with MDD.
MyD88s is the short form of MyD88, which is the most crucial adaptor in TLR signaling (15). MyD88s antagonizes MyD88 functions, preventing IRAK4 to phosphorylate IRAK1, thus halting the inflammatory pathway. In our study, we found significantly lower MyD88s mRNA levels in the PBMC in patients with MDD, similar to past findings in PBMC (14) and monocytes (16). The negative regulators of TLR signaling could form a complex web, and further investigations are warranted. The recent findings of negative TLR regulators of MDD are summarized in Table 4.
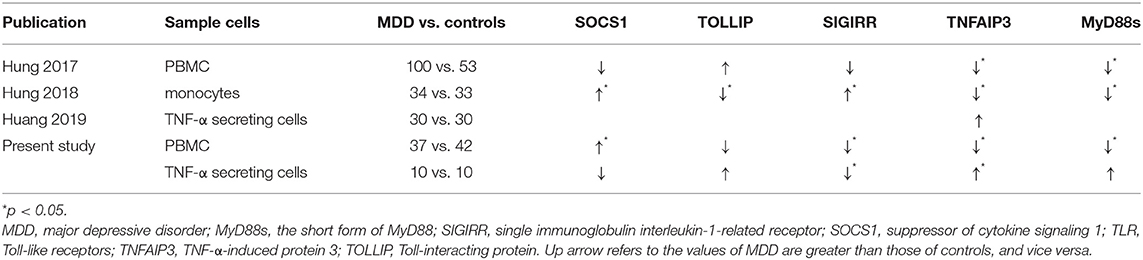
Table 4. Summary of recent findings of negative regulators of TLR pathway (-ΔCt).
In the patients treated with antidepressants for 4 weeks, we did not find significant changes in the levels of those negative regulator mRNA. Earlier studies could not find significant changes in levels of SOCS1, TOLLIP, SIGIRR, or MyD88s in PBMC or monocytes of patients with MDD, but TNFAIP3 levels showed significant increase after treatment (14, 16). TNFAIP3 level is also associated with psychological anxiety in MDD (25), baseline Ham-D score (14), and decreases in Ham-D score (14). While in another study, SOCS1 level correlated with changes in Ham-D score (16). In our study, only TOLLIP mRNA levels after treatment correlated significantly with changes in Ham-D score. The exact mechanism of how those regulators contribute to clinical symptoms remained elusive.
There are several limitations in this study. The sample sizes of both PBMC and TNF-α secreting cells investigations were small. The antidepressants were not controlled. Different classes of antidepressants could interact with the targeted outcomes in various ways. The treatment duration was merely 4 weeks, which is relatively short compared to other studies involving antidepressant treatment, which usually lasted 8–12 weeks. Due to limited fund, we were unable to analyze negative TLR regulators of TNF-α secreting cells after antidepressant treatment. Lastly, TNF-α-secreting cells include several cell types, such as monocytes, macrophages, and T cells, which could confound the findings. The readers are warned against over-interpret our study results because of those limitations, and a larger sample size with more controlled variables will be needed before a firm conclusion could be made.
SIGIRR and TNFAIP3, two negative regulators of TLR immune response pathways, were differentially expressed in both PBMC and TNF-α secreting cells of patients with MDD as compared to healthy controls. The negative regulations of innate immune response could contribute to the underlying mechanism of MDD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board of Chang Gung Memorial Hospital. The patients/participants provided their written informed consent to participate in this study.
T-LH contributed substantially to conception, design, and approved the final draft. C-CL and T-LH contributed to acqusition of data, helped with analysis, and interpretation of data. C-CL drafted the article and revised it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
This work was supported by the research Grants of Ministry of Science and Technology (MOST 106-2314-B-182A-106 and MOST 107-2314-B-182A-130).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We like to thank Dr. Yi-Yung Hung and Professor Hong-Yo Kang for their pioneer works in this area as well as their help in experimental design and methodology.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.698257/full#supplementary-material
1. Maes M, Delange J, Ranjan R, Meltzer HY, Desnyder R, Cooremans W, et al. Acute phase proteins in schizophrenia, mania and major depression: modulation by psychotropic drugs. Psychiatry Res. (1997) 66:1–11. doi: 10.1016/S0165-1781(96)02915-0
2. Song C, Dinan T, Leonard BE. Changes in immunoglobulin, complement and acute phase protein levels in the depressed patients and normal controls. J Affect Disord. (1994) 30:283–8. doi: 10.1016/0165-0327(94)90135-X
3. Maes M, Bosmans E, Suy E, Vandervorst C, DeJonckheere C, Raus J. Depression-related disturbances in mitogen-induced lymphocyte responses and interleukin-1 beta and soluble interleukin-2 receptor production. Acta Psychiatr Scand. (1991) 84:379–86. doi: 10.1111/j.1600-0447.1991.tb03163.x
4. Seidel A, Arolt V, Hunstiger M, Rink L, Behnisch A, Kirchner H. Cytokine production and serum proteins in depression. Scand J Immunol. (1995) 41:534–8. doi: 10.1111/j.1365-3083.1995.tb03604.x
5. Chang TT, Yen YC. Cytokines and major psychiatric disorders. Taiwanese J Psychiatry (Taipei). (2010) 24:257–68. Available online at: http://www.sop.org.tw/sop_journal/pastIssues/info.asp?/1635.html
6. Sutcigil L, Oktenli C, Musabak U, Bozkurt A, Cansever A, Uzun O, et al. Pro- and anti-inflammatory cytokine balance in major depression: effect of sertraline therapy. Clin Dev Immunol. (2007) 2007:76396. doi: 10.1155/2007/76396
7. O'Brien SM, Scully P, Fitzgerald P, Scott LV, Dinan TG. Plasma cytokine profiles in depressed patients who fail to respond to selective serotonin reuptake inhibitor therapy. J Psychiatr Res. (2007) 41:326–31. doi: 10.1016/j.jpsychires.2006.05.013
8. Lanquillon S, Krieg JC, Bening-Abu-Shach U, Vedder H. Cytokine production and treatment response in major depressive disorder. Neuropsychopharmacology. (2000) 22:370–9. doi: 10.1016/S0893-133X(99)00134-7
9. Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. (2010) 67:446–57. doi: 10.1016/j.biopsych.2009.09.033
10. Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell. (2010) 140:805–20. doi: 10.1016/j.cell.2010.01.022
11. Hung YY, Kang HY, Huang KW, Huang TL. Association between toll-like receptors expression and major depressive disorder. Psychiatry Res. (2014) 220:283–6. doi: 10.1016/j.psychres.2014.07.074
12. Wu MK, Huang TL, Huang KW, Huang YL, Hung YY. Association between toll-like receptor 4 expression and symptoms of major depressive disorder. Neuropsychiatr Dis Treat. (2015) 11:1853–7. doi: 10.2147/NDT.S88430
13. Hung YY, Huang KW, Kang HY, Huang GY, Huang TL. Antidepressants normalize elevated Toll-like receptor profile in major depressive disorder. Psychopharmacology (Berl). (2016) 233:1707–14. doi: 10.1007/s00213-015-4087-7
14. Hung YY, Lin CC, Kang HY, Huang TL. TNFAIP3, a negative regulator of the TLR signaling pathway, is a potential predictive biomarker of response to antidepressant treatment in major depressive disorder. Brain Behav Immun. (2017) 59:265–72. doi: 10.1016/j.bbi.2016.09.014
15. Liew FY, Xu D, Brint EK, O'Neill LA. Negative regulation of toll-like receptor-mediated immune responses. Nat Rev Immunol. (2005) 5:446–58. doi: 10.1038/nri1630
16. Hung YY. Antidepressants improve negative regulation of toll-like receptor signaling in monocytes from patients with major depression. Neuroimmunomodulation. (2018) 25:42–8. doi: 10.1159/000489562
17. Huang KW, Wu MK, Hung YY. Elevated TNIP3 mRNA expression in TNF-alpha-secreting cells from patients with major depressive disorder. Neuroimmunomodulation. (2019) 26:153–8. doi: 10.1159/000501083
18. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. (1967) 6:278–96. doi: 10.1111/j.2044-8260.1967.tb00530.x
19. Mei S, Ruan H, Ma Q, Yao WD. The ubiquitin-editing enzyme A20 regulates synapse remodeling and efficacy. Brain Res. (2020) 1727:146569. doi: 10.1016/j.brainres.2019.146569
20. Barzman D, Eliassen J, McNamara R, Abonia P, Mossman D, Durling M, et al. Correlations of inflammatory gene pathways, corticolimbic functional activities, and aggression in pediatric bipolar disorder: a preliminary study. Psychiatry Res. (2014) 224:107–11. doi: 10.1016/j.pscychresns.2014.07.009
21. Padmos RC, Hillegers MH, Knijff EM, Vonk R, Bouvy A, Staal FJ, et al. A discriminating messenger RNA signature for bipolar disorder formed by an aberrant expression of inflammatory genes in monocytes. Arch Gen Psychiatry. (2008) 65:395–407. doi: 10.1001/archpsyc.65.4.395
22. Nakagawa R, Naka T, Tsutsui H, Fujimoto M, Kimura A, Abe T, et al. SOCS-1 participates in negative regulation of LPS responses. Immunity. (2002) 17:677–87. doi: 10.1016/S1074-7613(02)00449-1
23. Kinjyo I, Hanada T, Inagaki-Ohara K, Mori H, Aki D, Ohishi M, et al. SOCS1/JAB is a negative regulator of LPS-induced macrophage activation. Immunity. (2002) 17:583–91. doi: 10.1016/S1074-7613(02)00446-6
24. Keshavarzi A, Eftekharian MM, Komaki A, Omrani MD, Kholghi Oskooei V, Taheri M, et al. Sexual dimorphism in up-regulation of suppressors of cytokine signaling genes in patients with bipolar disorder. BMC Psychiatry. (2019) 19:402. doi: 10.1186/s12888-019-2396-9
Keywords: MDD, SIGIRR, TLR, TNFAIP3, TNF-α secreting cells
Citation: Lin C-C and Huang T-L (2021) SIGIRR and TNFAIP3 Are Differentially Expressed in Both PBMC and TNF-α Secreting Cells of Patients With Major Depressive Disorder. Front. Psychiatry 12:698257. doi: 10.3389/fpsyt.2021.698257
Received: 28 April 2021; Accepted: 30 June 2021;
Published: 28 July 2021.
Edited by:
Chad A. Bousman, University of Calgary, CanadaReviewed by:
Zulqarnain Baloch, Kunming University of Science and Technology, ChinaCopyright © 2021 Lin and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tiao-Lai Huang, YTU0MDUyMEBhZG0uY2dtaC5vcmcudHc=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.