 Zhe Li
Zhe Li Xin Yi
Xin Yi Mengting Zhong4
Mengting Zhong4 Zhixiong Li
Zhixiong Li Weiyi Xiang
Weiyi Xiang Shuang Wu
Shuang Wu Zhenzhen Xiong
Zhenzhen Xiong
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 01 June 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.664808
This article is part of the Research TopicBioethics Amidst the COVID-19 PandemicView all 24 articles
Background: The COVID-19 pandemic has had impact that may contribute to a rise in mental health problems. The present study was aimed to better understand psychological status among medical staff and medical students during the early epidemic and to explore the influence factors of psychological distress.
Methods: A cross-sectional survey was conducted online from February 2–14, 2020. We collected general information related to the COVID-19 outbreak. Respondents were assessed using the Kessler-6 Psychological Distress Scale (K6), Social Support Rating Scale (SSRS), Perceived Stress Scale (PSS) and Simplified Coping Style Questionnaire (SCSQ). Stepwise multiple linear regression was performed to identify factors influencing psychological distress.
Results: Five hundred and twenty-eight respondents returned valid questionnaires. Medical staff and Medical students scored averages of 6.77 ± 5.04, 15.48 ± 8.66 on the K6, 37.22 ± 11.39, 22.62 ± 11.25 on the SSRS and 18.52 ± 7.54, 28.49 ± 11.17 on the PSS, respectively. Most medical staff (279, 91.77%) and 148 medical students (66.07%) showed a positive coping style. Social support, perceived stress, hours spent watching epidemic-related information per day and frequency of epidemic-related dreams were identified as factors influencing psychological distress among medical staff and medical students. Coping style emerged as a determinant of psychological distress among medical staff.
Conclusions: In the early stages of the COVID-19 epidemic in China, medical staff and medical students were at moderate to high risk of psychological distress. Our results suggest that psychological interventions designed to strengthen social support, reduce perceived stress and adopt a positive coping style may be effective at improving the mental health of medical staff and medical students.
After being declared an international public health emergency and then an epidemic within <2 months (1, 2), the novel coronavirus disease (COVID-19) epidemic has caused worldwide panic as the numbers of patients, suspected cases and affected regions have increased. As of September 7, 2020, data from the World Health Organization continue to show strong increases in new COVID-19 cases and deaths during the previous week; however, no effective treatment or targeted vaccine is yet available (3).
Many countries have implemented strict control measures in an unprecedented effort to contain the epidemic. Schools and businesses have closed, people have isolated themselves, and personal protective equipment has become scarce, contributing to a global atmosphere of fear, anxiety and depression (4). Overwhelming, sensationalist media coverage has intensified the psychological impact on the public, and may be causing more serious consequences than COVID-19 itself (5). The National Health Commission in China has mandated mental health strategies for patients, medical workers, and people in medical isolation in order to combat the psychological impact of the epidemic (6).
Medical staff, as front-line warriors in epidemic control and prevention, are at high risk of being infected and are continuously exposed to the stresses of providing clinical care under resource-limited conditions. When a new infectious disease outbreak, medical personnel are often at the highest risk of exposure. In the early stages of the epidemic in China, more than 3,000 medical staff in Hubei Province were infected, 40% of which occurred in hospitals (7). Overwork and worry about being infected may increase the risk of psychological distress among medical staff. The prevalence of various negative conditions was higher among medical health workers than among non-medical health workers, including insomnia (38.4 vs. 30.5%), anxiety (13.0 vs. 8.5%), depression (12.2 vs. 9.5%), somatization (1.6 vs. 0.4%), and obsessive-compulsive symptoms (5.3 vs. 2.2%) (8).
Medical students are an important force in the fight against the epidemic in the future, so their mental state when dealing with the epidemic also deserves attention. Studies have confirmed that medical students, in particular because of their professional background, pay close attention to the epidemic, leading them to experience excessive stress and concern (9). For example, in a study at Changzhi Medical College in China, 0.9% of students reported severe anxiety; 2.7%, moderate anxiety; and 21.3%, mild anxiety (9). Studies conducted during epidemics of Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), and Ebola also identified varying degrees of psychological problems among medical staff and students (10–12). Although medical students have some medical training, it is still difficult and stressful for them to make decisions during epidemics due to their lack of clinical experience, particularly during emergency situations (13–15). Therefore, investigating their psychological status during an epidemic may help us better understand and train medical students in the future.
When faced with emerging outbreaks of infectious disease or traumatic experiences, people may respond differently according to their coping style, level of social support or perceived level of stress. This can lead to stronger or weaker psychological distress. Coping strategies refer to the specific efforts, both behavioral and psychological, that people employ to master, tolerate, reduce, or minimize stressful events (16). Coping styles in a disease outbreak are significantly correlated with mental state: positive coping can generate positive emotions and behaviors that lead to improved outcomes, while negative coping styles may be associated with serious psychological distress such as post-traumatic stress disorder (PTSD) (17–19). Among Chinese physicians, coping styles appear to mediate 23–30% of overall psychological distress and its three dimensions (depression, anxiety, reduced self-affirmation) (20). Similarly, negative coping among front-line nurses positively correlates with psychological distress during the COVID-19 epidemic (21). Nevertheless, another study found that negative coping styles may have beneficial effects on relieving stress and temporarily coping with setbacks, suggesting that the difference between the two coping styles may be quantitative (22). It indicates the need to investigate whether these coping styles increase or reduce psychological distress among medical staff and medical students during the COVID-19 epidemic.
The definition of social support is a series of support measures accessible to an individual through their social relationships with other individuals, groups, and the larger community. Social support can be divided into three components: subjective support, objective support, and the utilization of support (23). Social support can influence mental and physical health through two possible mechanisms. One is through main effects: social support is salutary for all individuals independent of the extent of stress that they are currently facing. The other mechanism is a stress-buffering model, in which the social support of others may have an ameliorating effect on life stressors, particularly for individuals under greater stress (24). Effective social support can relieve negative emotions caused by stressors as well as improve self-efficacy, which can increase confidence and courage in fighting against crises such as the COVID-19 epidemic (23). Among Chinese medical workers, lack of support from society and patients was identified as an important factor in the workers' psychological burden (25). However, social support is not always beneficial, as one study indicated that Asians are more likely to benefit from implicit social support (social networking), whereas, Caucasians are more likely to benefit from explicit social support (event-specific advice) (26). The potentially complex effect of social support on psychological distress among medical staff and medical students during the COVID-19 epidemic needs to be investigated.
In the early stage of the COVID-19 epidemic, when little was known about the virus and the disease, the individuals may have suffered psychological stress about becoming infected or spreading the virus to their families, friends, or colleagues (27). Perceived psychological stress may increase risk of mental conditions such as depression, anxiety and PTSD (28, 29). Excessive levels of stress can also affect the work environment and produce long-term psychological consequences, especially during an emergency (30). Therefore, studies of people's coping styles, social support and perceived stress during the present epidemic may help guide psychological screening and intervention.
Despite widespread calls for such research, few epidemiological studies have examined psychological distress among medical staff and students, which might serve as the basis for strategies against current and future mental health challenges. The present study aimed to investigate the psychological status and analyzed risk and protective factors of psychological distress among medical staff and medical students in the early stages of the COVID-19 epidemic. We hypothesized that an active coping style and social support were protective factors against psychological distress. We further hypothesized that perceived stress was risk factor against psychological distress among medical staff and medical students. The goal is to provide a scientific basis for psychological interventions and for targeted training programs to strengthen mental health status when facing the epidemic.
Medical staff and medical students in China were invited by snowball sampling to participate in this study. All invitees completed the questionnaire online using Questionnaire Star (www.wjx.cn). The initial set of invitees (10 medical staff and 10 medical students) was chosen to ensure broad representation of sex, age, education level, academic or medical specialty, medical or academic institution, and city. Then the questionnaire was forwarded by this set of invitees to 10 colleagues and 10 classmates whom they considered suitable for the survey, and this second set forwarded the questionnaire in the same way, and so on (31).
Inclusion criteria for medical staff were: (1) current engagement in clinical work, (2) possession of a valid medical license, and (3) written informed consent. Inclusion criteria for medical students were: (1) current enrollment in a university or medical institution at any educational level, and (2) written informed consent. Respondents would be excluded if they reported ever having been diagnosed with any disorder listed in the Diagnostic and Statistical Manual of Mental Disorders (4th edition).
Given our desire to assess ~20 factors that might influence psychological distress in our sample, we aimed to recruit at least 10 times as many respondents in order to ensure adequate statistical power (32). We increased this number by 20% to allow for drop-outs, giving a minimal sample size of 220.
A cross-sectional, Internet-based survey was conducted during February 2–14, 2020. The study was approved by the Ethics Committee of West China Hospital, Sichuan University (No. 2020–178). The complete description of this survey and informed consent form were set prior to questionnaires. After the participants chose “Yes,” the data collection can be continued. Surveys were prepared and administered using Questionnaire Star.
The following validated surveys were administered to all subjects. In addition, they filled out a custom-made questionnaire, designed based on the literature and expert consultation, that collected data on demographics (gender, age, education state, marriage status), place of residence, quality of family relationships, suspected infection of respondents, suspected infection of their family members, hours per day spent watching media coverage of the epidemic, history of visiting Wuhan or contacting with people from Wuhan in recent month and frequency of epidemic-related dreams.
The 6-item Kessler Psychological Distress Scale (K6) was used to assess the psychological distress of respondents. It asks about six psychological symptoms during the previous 30 days, including feeling “nervous,” “hopeless,” “restless or fidgety,” “depressed,” “everything is an effort,” and “worthless” (33, 34). Responses on a 5-point Likert scale were scored with “0” (none of the time), “1” (seldom), “2” (some of the time), “3” (most of the time), or “4” (all the time). The total score ranges from 0 to 24 (35). Participants in the present study were categorized as being at low risk of psychological distress (total score of 0–12) or high risk of psychological distress (total score of 13 or more) (36). The scale has proven to show cross-cultural reliability and validity (37, 38). The Chinese version of the K6 has shown moderate to high reliability and validity, with the test-retest reliability was 0.79, Cronbach's alpha was 0.84, split-half coefficient was 0.84, and the correlation between K6 and K10 was 0.961 (39–41).
Social support was assessed using the Social Support Rating Scale (SSRS) (42), which consists of 10 items. The scale includes three dimensions: objective support, subjective support and availability of support. The total score is the sum of the scores on each dimension; higher scores reflect more social support. The scale has shown high validity and reliability among Chinese, with a Cronbach's alpha of 0.949 (43).
Perceived stress among medical staff and medical students was assessed using the Perceived Stress Scale (44), which measures extent of self-aware stress and the belief that one's life has been overloaded, unpredictable, or uncontrollable during the previous 30 days. The survey includes two dimensions of loss of control and tension, and the 10 items are answered on a 5-point Likert scale. The total score from 0 to 40 is the sum of the scores on the two dimensions; a higher score indicates greater mental stress. The scale has shown high validity and reliability among Chinese (45), with a Cronbach's alpha of 0.82 (46).
Coping style was measured using the Chinese version of the Simplified Coping Style Questionnaire (SCSQ) (22). The 20-item scale consists of two dimensions, positive and negative coping. The first 12 items cover positive coping, and the latter 8 items cover negative coping. The score is based on a 4-point Likert scale (0 = never, 1 = occasionally, 2 = often, 3 = always), with higher scores representing greater positive or negative coping. In the present study, we determined each respondent's coping style based on the difference between the Z-converted standard score for positive coping and the Z-converted standard score for negative coping. If the difference was higher than 0, we considered that the respondent generally adopted a positive coping strategy; otherwise, we considered that the respondent tended to show a negative coping style (47). The scale has shown high reliability and validity among Chinese, with Cronbach's alpha of 0.916 for positive coping and 0.808 for negative coping (22).
All data were analyzed using SPSS 23.0 (IBM, Chicago, IL, USA). Categorical data were reported as frequencies; continuous data, as mean values. Differences in psychological distress (K6 score) among individuals with different categorical data were assessed for significance using an independent two-samples t-test and analysis of variance, while differences in K6 score among individuals with different continuous data were assessed using linear correlation analysis. Stepwise multiple linear regression was performed to identify correlations of psychological distress with demographic characteristics, epidemic-related variables, social support, perceived stress and coping style. Differences associated with P < 0.05 were considered statistically significant. All statistical tests were two-tailed.
The same IP address could be used only once to complete the questionnaire. The survey did not collect any personal information such as names, in order to ensure anonymity and honest responses.
A total of 331 medical staff and 249 medical students began completing the surveys. After excluding 27 medical staff and 25 medical students who did not complete them, 304 (91.84%) medical staff and 224 (89.96%) students were included in the final analysis.
Among all medical staff, 210 (69.08%) were women and 94 (30.92%) were men. Ages ranged from 21 to 69 years (mean, 37.15; SD, 9.75), and more than half (74.34%) were unmarried. Among all staff, suspected infection of respondents and their family members were 9.54 and 4.93%, respectively. Fifty-six (18.42%) had a history of visiting Wuhan or being in contact with people from Wuhan in recent months, 9.87% lived in Hubei province, 0.66% reported poor family relationships, 15.79% reported frequent epidemic-related dreams, and 13 (4.28%) spent just a few hours per day watching media coverage of the epidemic.
Among all medical students, 134 (66.67%) were women. Ages ranged from 18 to 32 years (mean, 20.34; SD, 2.41), 95.54% reported good family relationship, suspected infection of respondents and their family members were 64.29% for both. and 148 (66.07%) had a history of visiting Wuhan or being in contact with people from Wuhan in recent months, while 27.86% lived in Hubei province, 144 (64.29%) had frequent epidemic-related dreams, and 7 (3.10%) spent just a few hours each day watching media coverage of the epidemic (Table 1).
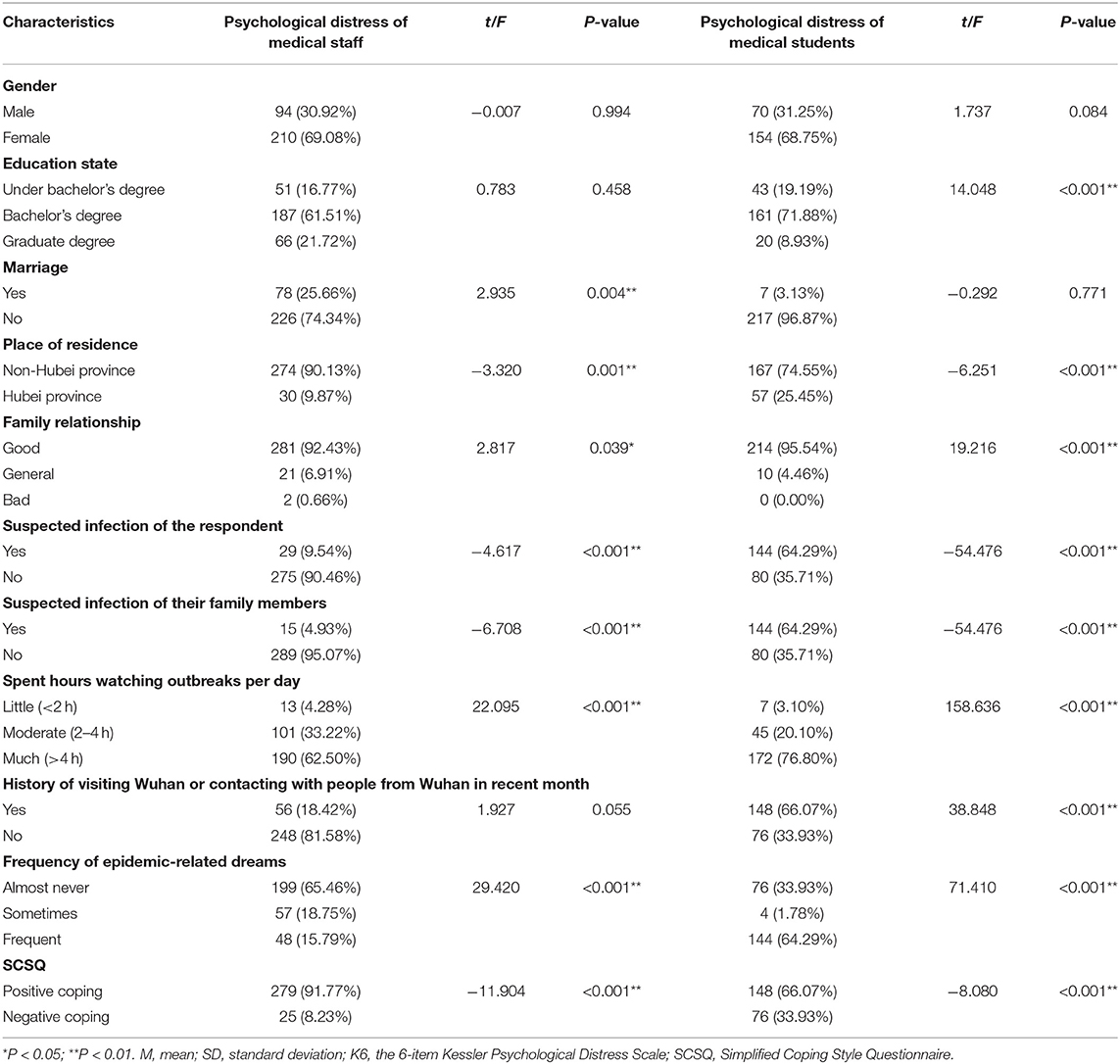
Table 1. Univariate analysis of factors associated with psychological distress among medical staff and medical students.
Medical staff scored a median of 6.77 on the K6, and individuals who scored higher were more likely to develop psychological distress. Average SSRS score was 37.22 ± 11.39, and average PSS score was 18.52 ± 7.54 (Table 2). Most staff (279, 91.77%) showed a positive coping style. Factor values are listed in Table 3. Multivariate analysis identified the following factors as significantly associated with psychological distress among medical staff (Table 4): hours per day spent watching media coverage of the epidemic (β = 1.003, P = 0.003), frequent epidemic-related dreams (β = 0.575, P = 0.032), social support (β = −0.104, P < 0.001), perceived stress (β = 0.285, P < 0.001) and coping style (β = 2.520, P = 0.004).

Table 2. Correlation analysis between factors and psychological distress among medical staff and medical students.

Table 3. Variables assessed in the analysis of risk factors for psychological distress among medical staff and medical students.
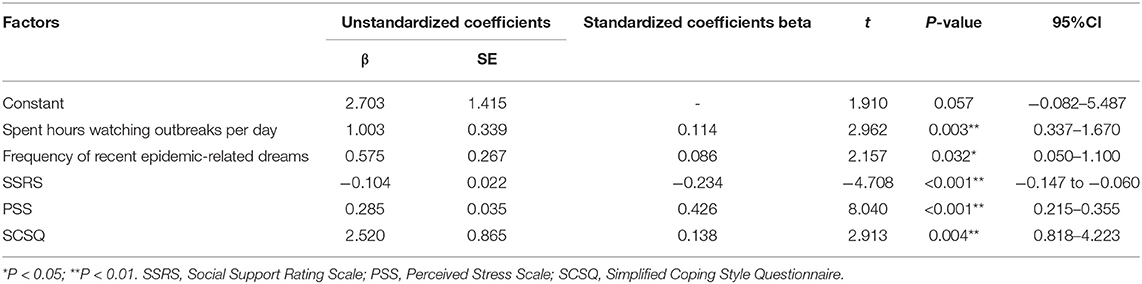
Table 4. Analysis of independent risk factors for psychological distress among medical staff.
Medical students scored a mean of 15.48 on the K6; their average SSRS score was 22.62 ± 11.25, and their average PSS score was 28.49 ± 11.17 (Table 2). A small majority (148, 66.07%) showed a positive coping style. Multivariate analysis identified the following factors as significantly associated with psychological distress among students (Table 5): hours per day spent watching media coverage of the epidemic (β = 1.679, P < 0.001), frequent epidemic-related dreams (β = 3.745, P < 0.001), social support (β = −0.135, P < 0.001), and perceived stress (β = 0.256, P < 0.001).
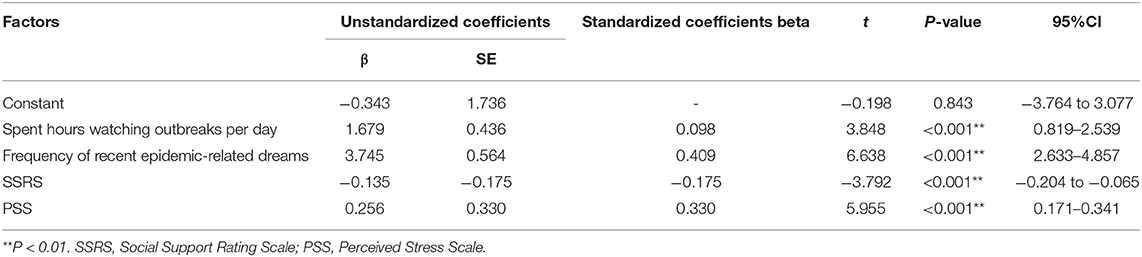
Table 5. Analysis of independent risk factors for psychological distress among medical students.
The current study assessed the prevalence of psychological distress among Chinese medical workers and medical students during the early stages of the COVID-19 epidemic, and it explored potential correlations of that distress with social support, perceived stress, and coping style. Similar to previous bio-disasters including SARS, Ebola, H1N1 influenza and MERS epidemics, the COVID-19 epidemic appears to have strongly adverse psychological effects on medical staff, such as depression, anxiety and insomnia (48).
The present results about psychological distress among medical staff are consistent with a previous study among Chinese medical staff (48). The study among healthcare workers in Ireland reflected that 42.6% for depression and 45.1% for both anxiety and stress (49). Also, there were study indicated that during the outbreak, the prevalence of depressive was in 27.5–50.7%, insomnia was in 34–36.1%, and severe anxiety in 45% among Italian healthcare workers (50). However, a study on Singapore healthcare workers revealed a lower prevalence with a proportion of 5.3 on depression and 8.7 on anxiety, 3.8% of them screened for moderate to severe levels of psychological distress during the COVID-19 epidemic (51). The discrepancy of psychological impact of COVID-19 on healthcare workers may reflect the different epidemic situation in different counties in the early stages of COVID-19 outbreak.
The present study further showed that a substantial proportion of medical students also experienced psychological distress during the initial stages of the COVID-19 epidemic. Previous studies found prevalence of anxiety to be 24.9% and prevalence of depression to be 40.5% among medical students during the COVID-19 epidemic (52, 53). These prevalence are much higher than those in the general Chinese population (54). A survey on Australian medical students revealed a mean K10 score of 20.6 indicating moderate psychological distress (55). As reported in a study on Iranian medical students, the prevalence of anxiety was 38.1% and depression was 27.6% (56). Also, a previous study on home-quarantined Bangladeshi students reflected that, 28.5% of them had stress, 33.3% had anxiety and 46.92% had depression from mild to extremely severe (57). These higher prevalence may reflect that, because schools have been closed, medical students tend to receive COVID-19 information more from social media rather than from scientific sources (58), which may lead to inaccurate assessment of the epidemic situation, leading in turn to excessive stress and concern that compromises their ability to gain professional knowledge in school (12).
Our results are consistent with the idea that the COVID-19 epidemic has placed a substantial burden on the mental health of medical staff and medical students in China. Therefore, psychological interventions should be provided urgently not only for medical staff but also for medical students, who are the reserve forces for medical staff. Such interventions should aim to enhance mental health during the COVID-19 epidemic.
Multilinear regression identified social support, perceived stress, hours per day spent watching media coverage of the epidemic, and frequency of recent epidemic-related dreams as factors significantly influencing psychological distress among medical staff and medical students. Coping style was identified as another influencing factor among medical staff.
Social support was identified as a factor influencing psychological distress in medical staff and medical students. Individuals who reported more social support were less likely to develop psychological distress. This is consistent with previous studies of Chinese medical workers (42, 59). Several studies have emphasized the role of social support in protecting mental health of various populations, including medical students (52, 60, 61). For example, inadequate support from family and friends has been associated with significantly greater risk of depression among US medical students (61), and a study of Australian medical students found similar results (62). Social support from friends or family can help medical staff reduce anxiety and stress, by reducing the perceived threat and inappropriate behavior that can result from stress events (63, 64). Social support can also improve self-efficacy, leading to more understanding, encouragement, courage, and a sense of professional achievement, resulting in increased confidence and optimism, which improves positive coping when facing stress (65, 66).
Psychological resilience may partially mediate the effects of social support on mental health, as suggested by a study of Chinese health care workers during the peak of the COVID-19 epidemic (59). Resilience has been positively associated with social support during the aftermath of major disasters: a study of adolescent survivors of the Wenchuan earthquake found that resilience can help protect individuals against mental illness (67, 68). This positive correlation has been observed across different populations faced with different disasters (69–72). Therefore, institutions should pay more attention to providing their staff with support that complements the social support they receive from families and healthcare authorities. More importantly, medical schools can embed training in emotional resilience into the curriculum in order to reduce psychological distress among medical students in daily life and emergency events (62).
In the present study, a higher level of perceived stress among medical staff or medical students was associated with greater likelihood of developing psychological distress. A study of medical staff in Guangdong, China found that individuals with moderate-to-severe anxiety or depressive symptoms were more likely to perceive higher stress (73), and perceived stress has been shown to predict anxiety among the general Chinese population during COVID-19 (46). A study of women in the US found that stressful life events were significantly associated with depression (74). Our results with medical students are consistent with a previous study suggesting that anxiety and depression among medical students are significantly related to their stress (75). Perceived stress reflects one's psychological experience after the self-interpretation of stressful event (76). A higher score is associated with higher risk of developing mental illness. Psychological stress may weaken immunity, resulting in a higher risk of infection and mental illness (77, 78).
In addition to the social support mentioned above, resilience can also alleviate the adverse effects of stress on medical workers and students (79, 80). For example, resilience negatively correlates with perceived stress among Chinese medical staff during COVID-19 (81). A study of medical staff during the SARS epidemic found that measures to increase resilience reduced perceived stress among medical staff (82). Another study found that resilience among medical students can protect them from stress (83). This protective role of resilience may help guide the design of measures to alleviate the stress of medical workers and medical students during the COVID-19 epidemic as well as during normal professional and personal life (84).
Medical staff and medical students in our study who spent more time daily watching media coverage of the epidemic were more likely to develop psychological distress. Similar results were reported in a study of the general Chinese population (85). During the early stage of the epidemic, media reports may have caused intense worry and panic by highlighting the government's efforts to fight against the outbreak, protective interventions, numbers of suspected infections and confirmed cases every day, while also highlighting the lack of effective treatments (85). At the same time, medical staff are concerned about their own health and about the risk of transmitting infection to their families. The more time they spend on searching for information about the epidemic, the more anxiety, stress or fear they report (86–88).
Medical students, in contrast, have tended to depend more on social media rather than scientific sources to obtain information about the epidemic and prevention measures, which may lead to inaccurate assessment of the epidemic situation (58). The frequent mention of the outbreak in the media and excessive attention paid to it may also aggravate their concerns and fears, compromising their ability to learn professionally about it (12, 89). Our results support the idea that medical students' self-confidence in coping with COVID-19 can be increased by giving priority to traditional national media directly connected to trustworthy medical decision-makers (90).
Frequency of epidemic-related dreams was significantly associated with psychological distress among medical staff and medical students in our study. Similar results have been reported in a study of the general Chinese population (54). Sleep problems, especially dreams in which the content relates directly to the traumatic event, are core symptoms of PTSD (91). This suggests that Chinese medical staff and medical students may have experienced PTSD symptoms in the early stages of the COVID-19 epidemic.
Multivariate analysis also showed that coping style was an important factor influencing psychological distress among the medical staff in our study. Medical staff with a positive coping style were less likely to report psychological distress. Several studies have linked negative coping style with subsequent mental illness, and positive coping style with better mental health (20, 92, 93). Indeed, these results have been reported for the general Chinese population during COVID-19 (54), as well as for Romanian healthcare workers (94). Therefore, appropriate psychological interventions should be urgently provided to medical workers with negative coping styles during COVID-19.
Among medical students in our study, coping style did not emerge from multivariate analysis as significantly associated with psychological distress, although it was significant in single-factor analysis (see Table 1). These results suggest that coping style may not be a major determinant of psychological distress among medical students. It is also possible that our sample was too small to detect an association.
This study was conducted during the early stages of the COVID-19 epidemic, only a few days after the entire city of Wuhan was placed under quarantine. While it may give a reasonably accurate view of the situation early in the epidemic, our results should be interpreted with caution given several limitations. One is the on-line format, necessary in large part because of the inability for us to interact face-to-face with potential respondents. So it is unclear whether our results can be generalized to people without Internet access. Secondly, the snowball sampling method may cause selection bias which may reduce the generalizability of our study. Thirdly, we did not assess whether and how respondents were engaging in prevention, as preventive behaviors can also play a role in mediating stress levels (95). Fourthly, the influence factors related to COVID-19 epidemic would change and the starting situations were different in different counties. However, our study may benefit to develop targeted training programs to strengthen mental health status of medical staffs and students when facing the similar infectious disease epidemic in the future in different countries. Finally, our cross-sectional study could not capture changes in psychological distress or identify its predictors during the course of the COVID-19 epidemic. Therefore, future studies would be to convey a follow-up for the current situation and engage in a more consistent analysis about the long-term psychological effects of the COVID-19 epidemic among medical staff and medical students. Such work should also further explore the ability of social support and coping strategies to mediate the effects of the COVID-19 epidemic on psychological distress and mental health more generally.
The COVID-19 epidemic in China has substantially affected the mental health of medical staff and medical students. Urgent mental health interventions should be implemented in a timely manner in order to prevent psychological distress and promote recovery. Our study has associated higher social support, lower perceived stress and less time spent daily watching media coverage of the epidemic with lower psychological distress among medical staff and medical students in the early stages of the COVID-19 epidemic. Medical staff with a positive coping style may also have lower psychological distress. Our results have several practical implications. Medical staff and medical students may benefit from being taught positive coping strategies and being encouraged to seek and maintain social support. Such interventions may help protect their mental health not only during the current COVID-19 epidemic but also during future public health emergencies. Most importantly, they should regularly receive comprehensive, systematic training in order to be more resilient to the daily pressures of their work. To benefit medical students, who are the reserve forces supporting medical staff, medical schools should use social media more frequently to disseminate knowledge and develop training plans (53). Medical schools should also consider adding training in mental resilience for emergency events into their curricula (61).
The raw data supporting the conclusions of this article will be made available by the corresponding authors on reasonable request.
The studies involving human participants were reviewed and approved by the Ethics Committee of West China Hospital, Sichuan University and run in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent to participate in this study was obtained from all individual participants included in this study through the Web-based surveys.
ZheL and XY developed concept, study design, and wrote the original paper. MZ, ZhiL, and WX collected and analyzed the data. SW and ZX made critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
This study was sponsored by the Science and Technology project of Health Commission of Sichuan Province (20PJ027, ZheL), Applied Psychology Research Center of Sichuan Province (CSXL-202A08, ZheL), the Department of Human Resources and Social Security of Sichuan Province [(2020) 291-20, ZheL], the special project of Aging Career and Industrial Research Center in 2020, Key Research Base of Social Sciences in Sichuan Province XJLL2020002, ZX).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank all the medical staff and medical students participated in the study.
1. World Health Organization. WHO Director-General's statement on IHR Emergency Committee on Novel Coronavirus (2019)nCoV. Geneva (2020). Available online at: https://apps.who.int (accessed December 17, 2020).
2. World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19. Geneva (2020). Available online at: https://apps.who.int (accessed December 17, 2020).
3. World Health Organization. WHO Coronavirus Disease 2019 (Covid-19) Situation Report-205. Geneva: World Health Organization (2020). Available online at: https://apps.who.int (accessed December 17, 2020).
4. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. (2020) 49:155–60. doi: 10.47102/annals-acadmedsg.202043
5. Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry Clin Neurosci. (2020) 74:281–2. doi: 10.1111/pcn.12988
6. National Health Commission of the People's Republic of China. Guideline for Psychological Crisis Intervention During 2019-nCoV. Beijing: National Health Commission of the People's Republic of China (2020).
7. Beijing Daily. National Support Wuhan Medical Staff “Zero Infection” New Crown Pneumonia. Beijing: Beijing Daily (2020).
8. Zhang WR, Wang K, Yin L, Zhao WF, Xue Q, Peng M, et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother Psychosom. (2020) 89:242–50. doi: 10.1159/000507639
9. Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. (2020) 287:112934. doi: 10.1016/j.psychres.2020.112934
10. Lee SM, Kang WS, Cho AR, Kim T, Park JK. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr Psychiatry. (2018) 87:123–7. doi: 10.1016/j.comppsych.2018.10.003
11. Ji D, Ji YJ, Duan XZ, Li WG, Sun ZQ, Song XA, et al. Prevalence of psychological symptoms among Ebola survivors and healthcare workers during the 2014-2015 Ebola outbreak in Sierra Leone: a cross-sectional study. Oncotarget. (2017) 8:12784–91. doi: 10.18632/oncotarget.14498
12. Patil NG, Chan Y, Yan H. SARS and its effect on medical education in Hong Kong. Med Educ. (2003) 37:1127–8. doi: 10.1046/j.1365-2923.2003.01723.x
13. Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin Med Res. (2016) 14:7–14. doi: 10.3121/cmr.2016.1303
14. Loh LC, Ali AM, Ang TH, Chelliah A. Impact of a spreading epidemic on medical students. Malays J Med Sci. (2005) 12:43–9.
15. Wong JG, Cheung EP, Cheung V, Cheung C, Chan MT, Chua SE, et al. Psychological responses to the SARS outbreak in healthcare students in Hong Kong. Med Teach. (2004) 26:657–9. doi: 10.1080/01421590400006572
16. Noorbakhsh SN, Besharat MA, Zarei J. Emotional intelligence and coping styles with stress. Proc Soc Behav Sci. (2010) 5:818–22. doi: 10.1016/j.sbspro.2010.07.191
17. Affinito J, Louie K. Positive coping and self-assessed levels of health and burden in unpaid caregivers of patients with end stage renal disease receiving hemodialysis therapy. Nephrol Nurs J. (2018) 45:373–9.
18. Huang J, Liu Q, Li J, Li X, You J, Zhang L, et al. Post-traumatic stress disorder status in a rescue group after the Wenchuan earthquake relief. Neural Regen Res. (2013) 8:1898–906. doi: 10.3969/j.issn.1673-5374.2013.20.009
19. Folkman S. Personal control and stress and coping processes: a theoretical analysis. J Pers Soc Psychol. (1984) 46:839–52. doi: 10.1037/0022-3514.46.4.839
20. Wang Y, Wang P. Perceived stress and psychological distress among Chinese physicians: the mediating role of coping style. Medicine (Baltimore). (2019) 98:e15950. doi: 10.1097/MD.0000000000015950
21. Nie A, Su X, Zhang S, Guan W, Li J. Psychological impact of COVID-19 outbreak on frontline nurses: a cross-sectional survey study. J Clin Nurs. (2020) 12: 15454. doi: 10.1111/jocn.15454
22. Xie YN. A preliminary study of the reliability and validity of the simplified coping style questionnaire (in Chinese). Chin J Clin Psychol. (1998) 6:114–5.
23. Berkman LF, Glass T. Social integration, social networks, social support, and health. Soc Epidemiol. (2000) 1:137–73.
24. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
25. Cai Z, Zheng S, Huang Y, Zhang X, Qiu Z, Huang A, et al. Emotional and cognitive responses and behavioral coping of Chinese medical workers and general population during the pandemic of COVID-19. Int J Environ Res Public Health. (2020) 17:6198. doi: 10.3390/ijerph17176198
26. Taylor SE, Welch WT, Kim HS, Sherman DK. Cultural differences in the impact of social support on psychological and biological stress responses. Psychol Sci. (2007) 18:831–7. doi: 10.1111/j.1467-9280.2007.01987.x
27. Maunder R, Hunter J, Vincent L, Bennett J, Peladeau N, Leszcz M, et al. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ. (2003) 168:1245–51.
28. Salim S. Oxidative stress and psychological disorders. Curr Neuropharmacol. (2014) 12:140–7. doi: 10.2174/1570159X11666131120230309
29. Ma X, Liu X, Hu X, Qiu C, Wang Y, Huang Y, et al. Risk indicators for post-traumatic stress disorder in adolescents exposed to the 5.12 Wenchuan earthquake in China. Psychiatry Res. (2011) 189:385–91. doi: 10.1016/j.psychres.2010.12.016
30. Müller MP, Hänsel M, Fichtner A, Hardt F, Weber S, Kirschbaum C, et al. Excellence in performance and stress reduction during two different full scales simulator training courses: a pilot study. Resuscitation. (2009) 80:919–24. doi: 10.1016/j.resuscitation.2009.04.027
31. Wu S, Li Z, Li ZX, Xiang W, Yuan Y, Liu Y, et al. The mental state and risk factors of Chinese medical staff and medical students in early stages of the COVID-19 epidemic. Compr Psychiatry. (2020) 102:152202. doi: 10.1016/j.comppsych.2020.152202
32. Wang JL. Clinical Epidemiology-Clinical Research Design, Measurement and Evaluation, Shanghai. Shanghai: The Science and Technology Press (2001).
33. Matud MP, Garcia MC. Psychological distress and social functioning in elderly Spanish people: a gender analysis. Int J Environ Res Public Health. (2019) 16:341. doi: 10.3390/ijerph16030341
34. Xu H, Xiong HY, Chen YH, Wang L, Liu T, Kang YK, et al. Comparative study of the Kessler 10 and Kessler 6 scales on Chinese university students' mental health (in Chinese). Modern Prev Med. (2013) 24:4493–6.
35. Lee S, Oh ST, Lee H, Lee JS, Pak H, Choi WJ, et al. Associated risk factors for psychological distress in patients with gastric epithelial neoplasm undergoing endoscopic submucosal dissection. Medicine. (2018) 97:e13912. doi: 10.1097/MD.0000000000013912
36. Franz M, Lensche H, Schmitz N. Psychological distress and socioeconomic status in single mothers and their children in a German city. Soc Psychiatry Psychiatr Epidemiol. (2003) 38:59–68. doi: 10.1007/s00127-003-0605-8
37. Kessler RC, Green JG, Gruber MJ, Sampson NA, Bromet E, Cuitan M, et al. Screening for serious mental illness in the general population with the K6 screening scale: results from the WHO World Mental Health (WMH) survey initiative. Int J Methods Psychiatr Res. (2010) 19(Suppl. 1):4–22. doi: 10.1002/mpr.333
38. Mohammed A, Sheikh TL, Gidado S, Poggensee G, Nguku P, Olayinka A, et al. An evaluation of psychological distress and social support of survivors and contacts of Ebola virus disease infection and their relatives in Lagos, Nigeria: a cross sectional study−2014. BMC Public Health. (2015) 15:824. doi: 10.1186/s12889-015-2167-6
39. Kang YK, Guo WJ, Xu H, Chen YH, Li XJ, Tan ZP, et al. The 6-item Kessler psychological distress scale to survey serious mental illness among Chinese undergraduates: psychometric properties and prevalence estimate. Compr Psychiatry. (2015) 63:105–12. doi: 10.1016/j.comppsych.2015.08.011
40. Sing L, Adley T, King LN, Yee LM, Wanjun G, Arthur M, et al. Performance of the 6-item Kessler scale for measuring serious mental illness in Hong Kong. Compr Psychiatry. (2012) 53:584–92. doi: 10.1016/j.comppsych.2011.10.001
41. Zhou C, Chu J, Wang T, Peng Q, He J, Zheng W, et al. Evaluation of reliability and validity of the Chinese version of simple psychological assessment scale Kessler 10 (in Chinese). Chin J Clin Psych. (2008) 16:627–9.
42. Xiao H, Zhang Y, Kong D, Li S, Yang N. The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February 2020 in China. Med Sci Monit. (2020) 26:e923549. doi: 10.12659/MSM.923549
43. Liu JW, Li FY, Lian YL. Reliability and validity of social support rating scale (in Chinese). J Xinjiang Med Univ. (2008) 1:4–6.
44. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
45. Huang F, Wang H, Wang Z, Zhang J, Du W, Su C, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. (2020) 20:130. doi: 10.1186/s12888-020-02520-4
46. Zhao X, Lan M, Li H. Perceived stress and sleep quality among the non-diseased general public in China during the 2019 coronavirus disease: a moderated mediation model. Sleep Med. (2020) 21:339–45. doi: 10.1016/j.sleep.2020.05.021
47. Li X, Guan L, Chang H, Zhang B. Core self-evaluation and burnout among nurses: the mediating role of coping styles. PLoS ONE. (2014) 9:e115799. doi: 10.1371/journal.pone.0115799
48. Liu CY, Yang YZ, Zhang XM, Xu X, Dou QL, Zhang WW. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiol Infect. (2020) 148:e98. doi: 10.1017/S0950268820001107
49. Ali S, Maguire S, Marks E, Doyle M, Sheehy C. Psychological impact of the COVID-19 pandemic on healthcare workers at acute hospital settings in the South-East of Ireland: an observational cohort multicentre study. BMJ Open. (2020) 10:e042930. doi: 10.1136/bmjopen-2020-042930
50. Preti E, Di MV, Perego G, Ferrari F, Mazzetti M, Taranto P, et al. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: rapid review of the evidence. Curr Psychiatry Rep. (2020) 22:43. doi: 10.1007/s11920-020-01166-z
51. Chew NWS, Lee GKH, Tan BYQ, Jing M, Goh Y, Ngiam NJH, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. (2020) 88:559–65. doi: 10.1016/j.bbi.2020.04.049
52. Cao X, Yang C, Wang D. The impact on mental health of losing an only child and the influence of social support and resilience. Omega. (2020) 80:666–84. doi: 10.1177/0030222818755284
53. Liang SW, Chen RN, Liu LL, Li XG, Chen JB, Tang SY, et al. The psychological impact of the COVID-19 epidemic on Guangdong college students: the difference between seeking and not seeking psychological help. Front Psychol. (2020) 11:2231. doi: 10.3389/fpsyg.2020.02231
54. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
55. Lyons Z, Wilcox H, Leung L, Dearsley O. COVID-19 and the mental well-being of Australian medical students: impact, concerns and coping strategies used. Aust Psychiatry. (2020) 28:649–52. doi: 10.1177/1039856220947945
56. Nakhostin-Ansari A, Sherafati A, Aghajani F, Khonji MS, Aghajani R, Shahmansouri N. Depression and anxiety among iranian medical students during COVID-19 pandemic. Iran J Psychiatry. (2020) 15:228–35. doi: 10.18502/ijps.v15i3.3815
57. Khan AH, Sultana MS, Hossain S, Hasan MT, Ahmed HU, Sikder MT. The impact of COVID-19 pandemic on mental health & wellbeing among home-quarantined Bangladeshi students: a cross-sectional pilot study. J Affect Disord. (2020) 277:121–8. doi: 10.1016/j.jad.2020.07.135
58. Khasawneh AI, Humeidan AA, Alsulaiman JW, Bloukh S, Ramadan M, Al-Shatanawi TN, et al. Medical students and COVID-19: knowledge, attitudes, and precautionary measures. A descriptive study from Jordan. Front Public Health. (2020) 8:253. doi: 10.3389/fpubh.2020.00253
59. Hou T, Zhang T, Cai W, Song X, Chen A, Deng G, et al. Social support and mental health among health care workers during coronavirus disease 2019 outbreak: a moderated mediation model. PLoS ONE. (2020) 15:e0233831. doi: 10.1371/journal.pone.0233831
60. Koelmel E, Hughes AJ, Alschuler KN, Ehde DM. Resilience mediates the longitudinal relationships between social support and mental health outcomes in multiple sclerosis. Arch Phys Med Rehabil. (2017) 98:1139–48. doi: 10.1016/j.apmr.2016.09.127
61. Rothon C, Goodwin L, Stansfeld S. Family social support, community “social capital” and adolescents' mental health and educational outcomes: a longitudinal study in England. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:697–709. doi: 10.1007/s00127-011-0391-7
62. Bore M, Kelly B, Nair B. Potential predictors of psychological distress and well-being in medical students: a cross-sectional pilot study. Adv Med Educ Pract. (2016) 7:125–35. doi: 10.2147/AMEP.S96802
63. Yang N, Xiao H, Wang W, Li S, Yan H, Wang Y. Effects of doctors' empathy abilities on the cellular immunity of patients with advanced prostate cancer treated by orchiectomy: the mediating role of patients' stigma, self-efficacy, and anxiety. Patient Prefer Adherence. (2018) 12:1305–14. doi: 10.2147/PPA.S166460
64. Adamczyk K, Segrin C. Perceived social support and mental health among single vs. partnered polish young adults. Curr Psychol. (2015) 34:82–96. doi: 10.1007/s12144-014-9242-5
65. Glozah FN. Exploring Ghanaian adolescents' meaning of health and wellbeing: a psychosocial perspective. Int J Qual Stud Health Well Being. (2015) 10:26370. doi: 10.3402/qhw.v10.26370
66. Segrin C, Passalacqua SA. Functions of loneliness, social support, health behaviors, and stress in association with poor health. Health Commun. (2010) 25:312–22. doi: 10.1080/10410231003773334
67. Bao Y. The path analysis of the impact of competency, job burnout and social support on the psychological resilience of nurses (in Chinese). Gen Pract Nurs. (2017) 15:3844–7.
68. Hourani L, Bender RH, Weimer B, Peeler R, Bradshaw M, Lane M, et al. Longitudinal study of resilience and mental health in Marines leaving military service. J Affect Disord. (2012) 139:154–65. doi: 10.1016/j.jad.2012.01.008
69. Perlman D, Taylor E, Molloy L, Brighton R, Patterson C, Moxham L. A path analysis of self-determination and resiliency for consumers living with mental illness. Community Ment Health J. (2018) 54:1239–44. doi: 10.1007/s10597-018-0321-1
70. Gloria CT, Steinhardt MA. Relationships among positive emotions, coping, resilience and mental health. Stress Health. (2016) 32:145–56. doi: 10.1002/smi.2589
71. Hu TQ, Zhang DJ, Wang JL. A meta-analysis of the trait resilience and mental health. Pers Indiv Differ. (2015) 76:18–27. doi: 10.1016/j.paid.2014.11.039
72. Tol WA, Song S, Jordans MJ. Annual research review: resilience and mental health in children and adolescents living in areas of armed conflict–a systematic review of findings in low- and middle-income countries. J Child Psychol Psychiatry. (2013) 54:445–60. doi: 10.1111/jcpp.12053
73. Wang H, Huang D, Huang H, Zhang J, Guo L, Liu Y, et al. The psychological impact of COVID-19 pandemic on medical staff in Guangdong, China: a cross-sectional study. Psychol Med. (2020) 6:1–9. doi: 10.1017/S0033291720002561
74. Kendler KS, Thornton LM, Gardner CO. Stressful life events and previous episodes in the etiology of major depression in women: an evaluation of the “kindling” hypothesis. Am J Psychiatry. (2000) 157:1243–51. doi: 10.1176/appi.ajp.157.8.1243
75. Moutinho IL, Maddalena NC, Roland RK, Lucchetti AL, Tibiriçá SH, Ezequiel OD, et al. Depression, stress and anxiety in medical students: a cross-sectional comparison between students from different semesters. Rev Assoc Med Bras (1992). (2017) 63:21–8. doi: 10.1590/1806-9282.63.01.21
76. Boals A, Banks JB. Effects of traumatic stress and perceived stress on everyday cognitive functioning. Cogn Emot. (2012) 26:1335–43. doi: 10.1080/02699931.2011.651100
77. Cruz-Pereira JS, Rea K, Nolan YM, O'Leary OF, Dinan TG, Cryan JF. Depression's unholy trinity: dysregulated stress, immunity, and the microbiome. Annu Rev Psychol. (2020) 71:49–78. doi: 10.1146/annurev-psych-122216-011613
78. Dhabhar FS, Saul AN, Holmes TH, Daugherty C, Neri E, Tillie JM, et al. High-anxious individuals show increased chronic stress burden, decreased protective immunity, and increased cancer progression in a mouse model of squamous cell carcinoma. PLoS ONE. (2012) 7:e33069. doi: 10.1371/journal.pone.0033069
79. Thompson G, Wrath A, Trinder K, Adams GC. The roles of attachment and resilience in perceived stress in medical students. Can Med Educ J. (2018) 9:69–77. doi: 10.36834/cmej.43204
80. Brennan EJ. Towards resilience and wellbeing in nurses. Br J Nurs. (2017) 26:43–7. doi: 10.12968/bjon.2017.26.1.43
81. Huang L, Wang Y, Liu J, Ye P, Cheng B, Xu H, et al. Factors associated with resilience among medical staff in radiology departments during the outbreak of 2019 novel coronavirus disease (COVID-19): a cross-sectional study. Med Sci Monit. (2020) 26:e925669. doi: 10.12659/MSM.925669
82. Maunder RG, Leszcz M, Savage D, Adam MA, Peladeau N, Romano D, et al. Applying the lessons of SARS to pandemic influenza: an evidence-based approach to mitigating the stress experienced by healthcare workers. Can J Public Health. (2008) 99:486–8. doi: 10.1007/BF03403782
83. Lin YK, Lin CD, Lin BY, Chen DY. Medical students' resilience: a protective role on stress and quality of life in clerkship. BMC Med Educ. (2019) 19:473. doi: 10.1186/s12909-019-1912-4
84. O'Dowd E, O'Connor P, Lydon S, Mongan O, Connolly F, Diskin C, et al. Stress, coping, and psychological resilience among physicians. BMC Health Serv Res. (2018) 18:730. doi: 10.1186/s12913-018-3541-8
85. Yu H, Li M, Li Z, Xiang W, Yuan Y, Liu Y, et al. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry. (2020) 20:426. doi: 10.1186/s12888-020-02826-3
86. Mobaraki K, Ahmadzadeh J. Current epidemiological status of Middle East respiratory syndrome coronavirus in the world from 1.1.2017 to 17.1.2018: a cross-sectional study. BMC Infect Dis. (2019) 19:351. doi: 10.1186/s12879-019-3987-2
87. Nickell LA, Crighton EJ, Tracy CS, Al-Enazy H, Bolaji Y, Hanjrah S, et al. Psychosocial effects of SARS on hospital staff: survey of a large tertiary care institution. CMAJ. (2004) 170:793–8. doi: 10.1503/cmaj.1031077
88. Chong M, Wang W, Hsieh W, Lee CY, Chiu NM, Yeh WC, et al. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital, Br J Psychiatry. (2004) 185:127–33. doi: 10.1192/bjp.185.2.127
89. Young ME, Norman GR, Humphreys KR. Medicine in the popular press: the influence of the media on perceptions of disease. PLoS ONE. (2008) 3:e3552. doi: 10.1371/journal.pone.0003552
90. Wang PW, Lu WH, Ko NY, Chen YL, Li DJ, Chang YP, et al. COVID-19-related information sources and the relationship with confidence in people coping with COVID-19: facebook survey study in Taiwan. J Med Internet Res. (2020) 22:e20021. doi: 10.2196/20021
91. First MB. Diagnostic and statistical manual of mental disorders, 5th edition, and clinical utility. J Nerv Ment Dis. (2013) 201:727–9. doi: 10.1097/NMD.0b013e3182a2168a
92. Hollifield M, Hewage C, Gunawardena CN, Kodituwakku P, Bopagoda K, Weerarathnege K. Symptoms and coping in Sri Lanka 20-21 months after the 2004 tsunami. Br J Psychiatry. (2008) 192:39–44. doi: 10.1192/bjp.bp.107.038422
93. Dave C, Tanya G. The mediating effects of coping strategies in the relationship between automatic negative thoughts and depression in a clinical sample of diabetes patients. Pers Indiv Differ. (2008) 46:460–4. doi: 10.1016/j.paid.2008.11.014
94. Man MA, Toma C, Motoc NS, Necrelescu OL, Bondor CI, Chis AF, et al. Disease perception and coping with emotional distress during COVID-19 pandemic: a survey among medical staff. Int J Environ Res Public Health. (2020) 17:4899. doi: 10.3390/ijerph17134899
Keywords: COVID-19, psychological distress, social support, coping style, stress, medical staff, medical students
Citation: Li Z, Yi X, Zhong M, Li Z, Xiang W, Wu S and Xiong Z (2021) Psychological Distress, Social Support, Coping Style, and Perceived Stress Among Medical Staff and Medical Students in the Early Stages of the COVID-19 Epidemic in China. Front. Psychiatry 12:664808. doi: 10.3389/fpsyt.2021.664808
Received: 06 February 2021; Accepted: 28 April 2021;
Published: 01 June 2021.
Edited by:
Thalia A. Arawi, American University of Beirut Medical Center, LebanonReviewed by:
Danilo Forghieri Santaella, University of São Paulo, BrazilCopyright © 2021 Li, Yi, Zhong, Li, Xiang, Wu and Xiong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhenzhen Xiong, eHp6NjIzMDg2MzFAMTYzLmNvbQ==; Shuang Wu, d3M5MTA5MDJAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.