
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 05 March 2021
Sec. Social Psychiatry and Psychiatric Rehabilitation
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.649090
This article is part of the Research Topic Medical Education in Psychiatry View all 12 articles
 Doron Amsalem1,2*
Doron Amsalem1,2* Andrés Martin3,4
Andrés Martin3,4 Mariela Mosheva2,4,5
Mariela Mosheva2,4,5 Omer Soul2,4,5Liran Korotkin4Amitai Ziv2,4,6
Omer Soul2,4,5Liran Korotkin4Amitai Ziv2,4,6 Doron Gothelf5,7
Doron Gothelf5,7 Raz Gross2,4,8
Raz Gross2,4,8Background: Delivering difficult news to individuals diagnosed with mental health disorders and their family members can be challenging. The use of simulated patients (SP) is an effective teaching method to enhance clinical skills, particularly those around communication. We developed, implemented, and evaluated the effectiveness of an SP-based training module to improve psychiatric residents' clinical communication skills in delivering difficult news.
Methods: We conducted 5-h workshops consisting of 3 components: (1) a high-fidelity simulation session with a professional actor; (2) a 30-min lecture; and (3) role-playing of 3 short scenarios, during which residents rotated taking on different roles (as psychiatrist, patient, or family member). We observed through a 1-way mirror and videotaped each resident's simulation session and followed it with personalized debriefing. Following the workshop, each resident received the full-length video of their simulated interview, together with a list of questions as a take-home assignment. Two months after the workshop, the residents were invited to a second SP-based session, during which 2 independent evaluators, each a board-certified psychiatrist with expertise in medical simulation, evaluated the participants' communication skills using a previously validated instrument. To avoid observation bias, the 2 evaluators rated the videotapes blind to the timing of the simulation (pre- vs. post-training). Participants completed self-report questionnaires on satisfaction and self-confidence, before, after, and 2 months following the workshop.
Findings: Of the 28 psychiatric residents who participated in the training day, 24 (86%) completed the post-workshop evaluation. Mean communication score increased from 24.9 to 27.8 (paired t-test: 5.6, p < 0.001). The mean score for the self-confidence questionnaire, calculated on a 1 to 5 Likert scale, increased from 3.4 to 4.0 after the training day, and remained unchanged (4.2) 2 months later (p < 0.001).
Conclusions: An SP-based training module proved useful in improving the objectively measured communication skills of psychiatric residents delivering difficult news. The training further enhanced participants' subjective sense of confidence in those clinical skills.
In psychiatry, sharing diagnoses and other difficult information can be particularly challenging (1). A review of the literature shows that many psychiatrists withhold information due to various reasons (2–4). They assume patients may have restricted ability for information processing due to the nature of psychiatric symptoms, which, by their perspective, can interfere with cognitive and emotional functions as reality testing, lack of insight, and emotional regulation (5). In other studies, mental health providers reported fears about delivering an incorrect diagnosis, the patient's distress, and the stigmatizing impact of using words such as “schizophrenia” (4, 6, 7). Patients and their relatives have expressed dissatisfaction with the way diagnostic and other sensitive information was shared with them (8), and several studies have demonstrated that individuals diagnosed with mental health disorders and their relatives want to be fully informed–and should (9, 10). In sum, there is a need for clear guidelines and proper education to reduce the discomfort and uncertainty associated with sharing difficult information with individuals diagnosed with mental health disorders. In the absence of proper resources and training, psychiatrists may avoid addressing such sensitive content altogether.
Several protocols have been developed to facilitate this complicated process of information disclosure, including the SPIKES (11), and Girgis and Sanson-Fischer (12) protocols. These protocols consistently present similar principles: emotional support; what and how much information to provide; manner of communicating news; and setting (13). A study among 1,337 individuals with life-changing diagnoses showed that the SPIKES protocol largely reflects patients' preferences (14). This study found 83% of the surveyed medical schools in Canada reported using the SPIKES to teach how to disclose difficult news.
The SPIKES (11) protocol includes 6 steps: (1) Setting up the environment; (2) assessing the patient's Perception of his/her condition; (3) Inviting the patient to define which information he/she would like to receive; (4) providing the required Knowledge to the patient; (5) addressing the patient's Emotions with empathic responses; and (6) providing a Summary of treatment options and future plans. SPIKES was originally used in oncology but gradually shifted to other fields of medicine, including infectious diseases, gynecology, neurology, and ophthalmology (11, 15–18). Previous studies have identified the absence of specific guidelines for sharing difficult news in psychiatry (19) and showed the need for such protocols (20), yet the SPIKES model has not yet been empirically studied in psychiatry (21).
Delivering the diagnosis of a serious illness is an important skill in all fields of medicine, and residents consistently identify a desire and need for further education (22–24). Among various training approaches, the use of simulated patients (SPs) offers numerous advantages in medical education, which have been well-reviewed in the literature (25–27). Practicing specific skills in a supportive space without risk of harm to patients by someone inexperienced, allows for educators and trainees to focus their attention on the complexities of the skills at hand, such as delivering difficult news (28, 29). However, while SP-based methodology is widely used in medical education, its use in the psychiatric field has emerged only recently (30–32). In psychiatry, as in other fields, assisting residents to acquire skills in delivering diagnosis is pivotal (33, 34). Similar to oncology and palliative care, there are complexities and potential harm that can emerge from poorly shared information, yet in psychiatry, the use of simulation to practice communication skills has been minimally studied.
Most studies on SP-based training in delivering difficult news in medicine have focused on self-efficacy and satisfaction outcomes to address communication skills, providing findings that are solely based on the learner's subjective perceptions (35). There are only a few studies that have attempted to examine objective changes in learner performance through the use of SPs and external evaluators (36–38): a study of 38 residents in family medicine and internal medicine (37); a study of 34 residents in pediatric emergency medicine (38); and a study of 98 residents, mainly in surgery-related specialties (36). However, such an approach is yet to be undertaken in psychiatry.
We developed an SP-based workshop to enhance psychiatric residents' clinical and communication skills in delivering difficult news to patients and their families. We hypothesized that following participation in the workshop, psychiatry residents would improve their abilities to communicate difficult news as demonstrated by measurable increases in: (1) objective performance as assessed by external evaluators, and (2) self-confidence.
Participants were psychiatry residents recruited from 3 free-standing psychiatric hospitals and one general hospital. All training sites were located in the center of Israel and academically affiliated with Tel-Aviv University. The Sheba Medical Center Institutional Review Board approved the study (Protocol #SMC5912-19). All participants signed an informed consent form. The study was conducted between March 2019 and January 2020.
In partnership with the Israel Center for Medical Simulation (MSR), Tel Aviv University, and Yale School of Medicine, we developed a 5-h workshop designed to teach psychiatry residents how to communicate difficult information to patients or their family members. During the course of the study, we delivered the workshop 5 times, with a maximum of 6 psychiatric residents each time, in order to provide each participant with the opportunity to interact with an SP. For consistency, the same SPs attended all the workshops and played the same role each time. The workshop consisted of 3 components: (1) High-fidelity simulation: each participant had a 15-min interaction with an SP depicting one of two scenarios described below, followed by a small-group debriefing session. Video cameras recorded the encounters for further analysis, feedback, and reflection in the debriefing sessions. Each participant encountered one SP and then observed other participants through a 1-way mirror. Debriefings were led by two psychiatrists (DA and RG) with expertise in video-based debriefing, who highlighted core elements of delivering difficult news and communication skills. All participants were encouraged to reflect and share their feelings and thoughts, and to make suggestions for improvement; (2) SPIKES protocol: a 60-min presentation focusing on aspects unique to psychiatry. The SPIKES tool was chosen following a literature review because of its wide use, simplicity, and applicability for delivering difficult information to patients and their relatives (11, 39). Participants were invited to discuss their own issues and concerns regarding the delivery of difficult information; and (3) Role-playing: a 90-min session with 3 short scenarios, during each of which 2 residents rotated taking on different roles (as psychiatrist, patient, or family member). At the end of the training day, each resident received the full-length video of their simulated interview, together with a list of questions as a take-home assignment. Two months after the training day, each resident was invited to a second videotaped SP-based session.
We created two scenarios for SPs, each based on different psychiatric vignettes of a patient and a family member. The first scenario describes a discussion with the mother of an 18-year-old patient recently admitted to a locked inpatient unit due to a first psychotic episode. The second scenario describes a hospitalized patient with bipolar disorder being recommended long-term use of lithium.
Scenarios for role plays included 3 different discussions between a psychiatrist and a patient or family member. For each scenario, we provided 2 summary cards: one for the resident who role played the psychiatrist, another for the one who played the patient or family member. During each conversation, the practicing residents rotated between roles to experience the entire spectrum of the interaction. The first scenario describes a mother being given an autism diagnosis for her 3-year-old son. The second scenario describes a 36-year-old woman with schizoaffective disorder who during an outpatient visit updates her psychiatrist on her efforts to conceive, while on treatment with valproate, a potentially teratogenic medication. The third scenario describes a 43-year-old man diagnosed with bipolar disorder being informed that his driver's license will be suspended following a recent psychotic episode.
Two independent evaluators (MM and OS), each a board-certified psychiatrist with expertise in medical simulation, evaluated the participants' communication skills. To avoid observation bias, the 2 evaluators rated the videotapes blind to the timing of the simulation (pre-workshop vs. two-month post-workshop). The communication tool was developed by Kurtz et al. (40) and was previously used (41) to evaluate residents' communications skills. The communication tool is based on the SPIKES protocol and includes 17 items, such as “Introduces themselves and their roles” to examine the Setting step, or “Assesses the patient's starting point” to assess the Perception step. Response options were: 0 = “not done or inadequate,” 1 = “adequate,” and 2 = “good.” The scale's Cronbach's alpha was 0.93 for this study; inter-rater agreement was moderate (kappa = 0.58, p < 0.001).
Participants completed self-report questionnaires on their confidence in delivering difficult news before, after, and 2 months following the workshop. The questionnaire was previously used by Tobler et al. (41) and included 13 items such as “I feel confident in my ability to listen to patients' concerns,” or “I feel confident in my ability to summarize information in a way that is easy to understand.” Response choices ranged from 1 (“strongly disagree”) to 5 (“strongly agree”) on a Likert scale. The questionnaire was translated into Hebrew and then back-translated to English by 2 bilingual authors (DA and LK). The 2 translators and a third author (DG) discussed and resolved discrepancies in the translation. The scale's Cronbach alpha for this study was 0.81. In addition, a 6-item questionnaire was used to measure the participant's self-efficacy and satisfaction at the end of the workshop. Response choices ranged from 1 (“not at all”) to 5 (“very much”) on a Likert scale. The scale's Cronbach alpha was 0.92 for this study.
We calculated mean scores and standard deviations for each of the questionnaires. We used the Shapiro Wilk-test to evaluate for normal distribution. We then used paired t-tests to compare change in communication skills mean scores before and 2 months after the workshop. We also used paired t-tests to compare change in resident self-assessment mean scores between pre- and post-workshop time points, and between pre- and 2-months post-workshop. We used a two-tailed p-value of 0.05 as threshold for significance. We conducted all statistical analyses using IBM SPSS software, version 26.0 (Armonk, NY).
Our study sample consisted of 28 psychiatric residents (17 females, 11 males) who participated in the study and completed the pre- and post-workshop evaluations, 24 (86%) of whom also completed the two-month post-workshop evaluation. Participants' age distribution was as follows: under 25 (n = 2, 7%); 25 to 30 (n = 11, 39%); and 30 to 35 (n = 15, 54%). Distribution according to years in residency training was as follows: under 2 years (n = 16, 57%); more than 2 years (n = 12; 43%). Across all time points, independent t-tests showed no differences in total mean scores between females and males, or between residents in general or psychiatric hospitals, or between more- and less-experienced residents.
In Table 1 we summarize mean scores for the 17-item communication skills assessment, as rated by the 2 independent evaluators blind to time period (pre- or 2 months post-workshop). Mean scores increased from 24.9 to 27.8 (t = 5.55, p < 0.001) between pre- and 2-month post-workshop, reflecting improvement in residents' performance. We also found improvement from pre- to 2-month post-workshop in 5 of the 17 items.
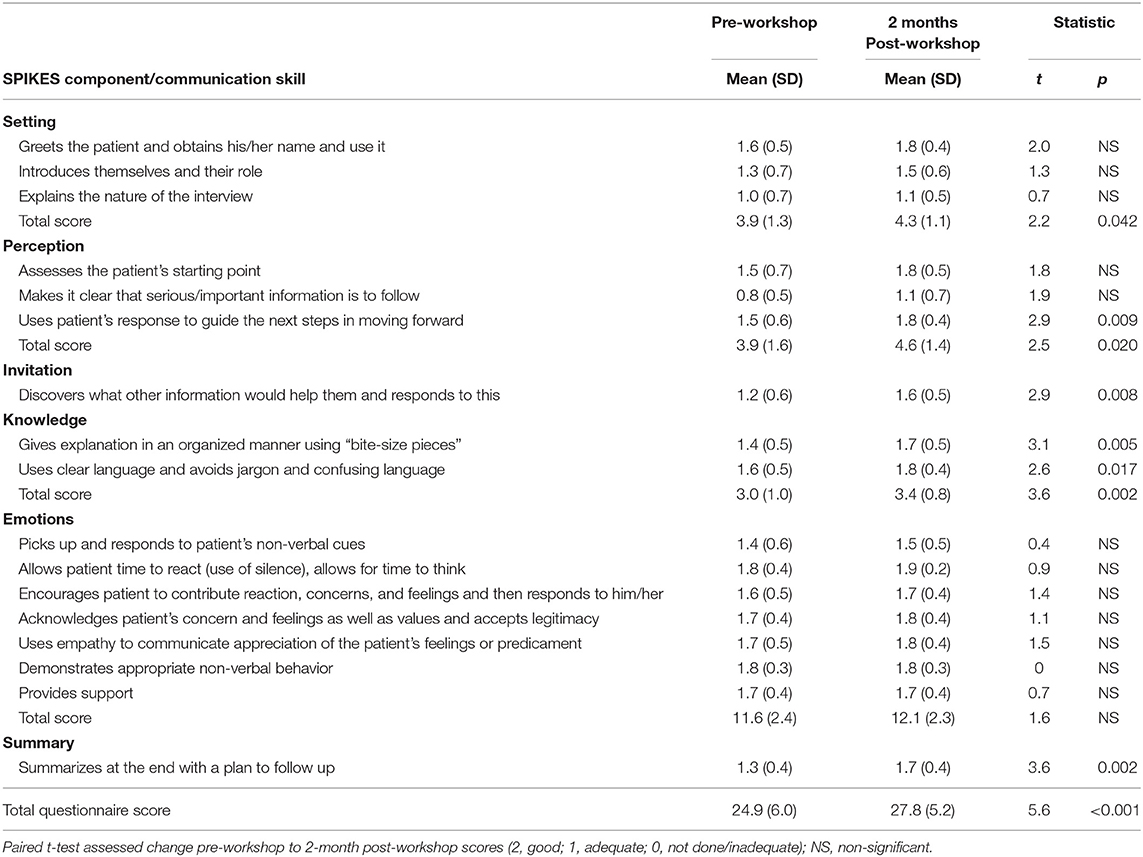
Table 1. Evaluators' scores on communication skills, blinded to the time period (before the workshop and 2 months after).
In Table 2 we summarize mean scores of residents' self-confidence in their ability to communicate difficult news before, immediately after, and 2-months after the workshop. Mean questionnaire scores increased from 3.6 to 4.0 (t = 7.3, p < 0.001) between pre- and post-workshop, reflecting an improvement in residents' confidence. Mean scores remained high after 2 months (mean score 4.2, t = 5.2, p < 0.001), showing an enduring effect for the workshop. Paired t-tests also showed significant change between pre- and post-workshop, and between pre- and 2-month post-workshop for 11 (85%) of the 13 questionnaire items. The mean total score for the 6-item self-report satisfaction questionnaire was 4.4 ± 0.7, indicating high satisfaction with the workshop (see Table 3).
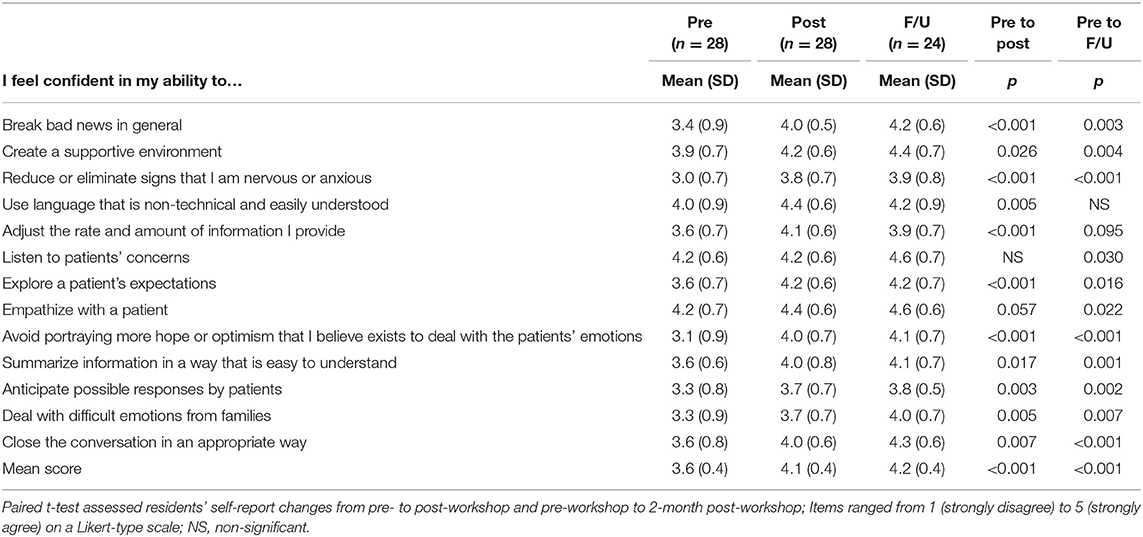
Table 2. Residents' self-ratings for confidence in their ability to communicate before, immediately after, and 2 months after the workshop.

Table 3. Residents' self-efficacy and satisfaction ratings at the end of the workshop.
The purpose of this study was to test the efficacy of a 5-h simulation-enhanced workshop in improving psychiatric residents' self-confidence and communication skills sharing difficult news with patients and their family members. As hypothesized, we found an increase in communication skills as evaluated by external evaluators blind to the timing of simulated interactions (before or 2 months after the training). We also found an increase in residents' self-confidence after attending the workshop, a change that endured 2 months later. Our findings strengthen the existing knowledge (42, 43) on the positive effect of SP-based training in psychiatry, and expand it by demonstrating objective and subjective improvements that persist 2 months after training.
Our simulation-enhanced workshop differs from previous efforts in other areas of medicine. Other workshops have focused mainly on “breaking bad news” (28, 37), whereas we attempted to address a wider spectrum of difficult news, as specifically pertinent to psychiatry. In addition to sharing new diagnoses (schizophrenia or autism), the scenarios and role play vignettes we developed included discussions about involuntary hospitalization, the need for chronic medication use, considerations around medication use during pregnancy and, a driver's license suspension due to a psychotic episode.
Unlike other fields in medicine with more discrete diagnostic criteria, sharing diagnoses in psychiatry can be a continuous and iterative process, often requiring more than one session (6). Sharing information about diagnosis of a serious mental illness is particularly challenging, as the nature of mental illness is often difficult to explain, since there may be no clear etiology and treatment options and prognosis may vary widely. In addition, newly diagnosed individuals with mental health disorders often may not accept their diagnosis due to lack of insight, impaired reality testing or cognition, or stigma related to their condition (44). Moreover, diagnostic information is not the only difficult information that a psychiatrist is likely to share with patients or family members. We addressed this variability through a range of different SP scenarios, discussions, and role plays.
Our main finding was a significant increase in the total mean scores of communication skills at two-months follow-up. This finding is in line with a previous study (41) among 39 pediatric residents, which showed a similar effect in improving residents' communication skills. However, and in contrast to that study, we found that even though residents' self-confidence improved across all self-rated domains, blinded evaluators found no change on items assessing the way the residents addressed the SP's Emotions. This finding was inconsistent with other studies showing a change across all SPIKES domains (41, 45). Three possible explanations may address this discrepancy: First, our study assessed a 2-month follow-up interval, compared to an immediate change in other studies. Second, the pre- and post-workshop mean scores were both relatively high for these items, indicating a possible ceiling effect. Third, the lack of change may be attributed to differences between the simulated environment and the residents' daily clinical reality, as some simulated scenarios may not represent the full complexity of real patients.
We have recently described a new model of SP-based learning that can help address the last of these three possibilities. In this model, termed Co-constructive Patient Simulation (CCPS) (46), a designated learner creates a case script based on a challenging encounter faced during clinical practice. Together with an instructor, the learner is then involved in creating, editing, and practicing role play of the simulated case with an SP. After the creation of the simulated environment, fellow learners with no prior knowledge of the case interview the SP. The educational encounter is followed by a group debriefing. We piloted the CCPS model with 11 trainees in child and adolescent psychiatry throughout a full academic year. The topics chosen by the 6 designated learners included: medical errors and error disclosure, racial tensions and overt racism, interprofessional conflicts, transphobia, patient-on-provider violence, and sexual health. The residents, who rated the model highly, shared that they were engaged and could openly discuss emotionally challenging topics. In sum, it seems that for the unique challenges of sharing difficult news in psychiatry, a learner-centered simulation approach may create even more meaningful and relevant learning opportunities.
Our study has several limitations. First, lacking a comparison to other teaching methods or a non-training control group, we conducted within-group pre- and post-workshop tests. Consequently, improvement in communication and clinical skills could be attributed in part to other factors, such as site-specific training opportunities, given that residents continued their training and had other psychiatric learning experiences during the 2-month interval between the pre- and post-workshop assessments. Second, our sample consisted of only 24 residents who completed the study, thus limiting generalizability and statistical power. Third, our study included residents in different training years, introducing heterogeneity to the study sample, even though we found no differences in outcomes between more and less experienced residents. Finally, given the small sample size and exploratory nature of our study, we recognize that our item-level findings would have been more modest had we made corrections for multiple comparisons. For example, in the case of Table 1, the Bonferroni significance threshold would have been a more conservative 0.0038 (i.e., 0.05/13). Nevertheless, an approach of not adjusting for multiple comparisons is preferable as it leads to fewer errors of interpretation when the data under evaluation are not random numbers but actual observations (47).
This study presented and evaluated the efficacy of a model for teaching psychiatric residents how to better communicate diagnostic and other difficult information. Participants found the simulation-enriched workshop to be useful and demonstrated objective improvements in their abilities to deliver difficult news. The training further enhanced participants' subjective sense of confidence and competence in those communication skills. Sharing diagnoses and other difficult information in psychiatry is challenging, and future studies should focus on developing and investigating ways to facilitate this clinical process.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Sheba Medical Center Institutional Review Board approved the study (Protocol #SMC5912-19). The patients/participants provided their written informed consent to participate in this study.
DA and AM developed the study design. DA and LK performed the analytic calculations. MM and OS performed the evaluations. RG supervised the project. All authors contributed to the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Del Piccolo L, Danzi O, Fattori N, Mazzi MA, Goss C. How psychiatrist's communication skills and patient's diagnosis affect emotions disclosure during first diagnostic consultations. Patient Educ Couns. (2014) 96:151–8. doi: 10.1016/j.pec.2014.06.001
3. Mitchell AJ. Reluctance to disclose difficult diagnoses: a narrative review comparing communication by psychiatrists and oncologists. Support Care Cancer. (2007) 15:819–28. doi: 10.1007/s00520-007-0226-y
4. Paccaloni M, Moretti F, Zimmermann C. Giving information and involving in treatment: what do psychiatrists think? A review. Epidemiol Psychiatr Sci. (2005) 14:198–216. doi: 10.1017/S1121189X00007958
5. Moran GS, Oz G, Karnieli-Miller O. Psychiatrists' challenges in considering disclosure of schizophrenia diagnosis in israel. Qual Health Res. (2014) 42:1368–80. doi: 10.1177/1049732314547085
6. Cleary M, Hunt GE, Horsfall J. Delivering difficult news in psychiatric settings. Harv Rev Psychiatry. (2009) 17:315–21. doi: 10.3109/10673220903271780
7. Outram S, Harris G, Kelly B, Cohen M, Sandhu H, Vamos M, et al. Communicating a schizophrenia diagnosis to patients and families: a qualitative study of mental health clinicians. Psychiatr Serv. (2014) 65:551–4. doi: 10.1176/appi.ps.201300202
8. Amsalem D, Hasson-Ohayon I, Gothelf D, Roe D. How do patients with schizophrenia and their families learn about the diagnosis? Psychiatry. (2018) 81:283–7. doi: 10.1080/00332747.2018.1443676
9. Fisher M. Telling patients with schizophrenia their diagnosis. Patients expect a diagnosis. BMJ. (2000) 321:385. doi: 10.1136/bmj.321.7257.385
10. Clafferty RA, McCabe E, Brown KW. Conspiracy of silence? Telling patients with schizophrenia their diagnosis. Psychiatr Bull. (2001) 25:336–39. doi: 10.1192/pb.25.9.336
11. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES—A six-step protocol for deliveringbBad news: application to the patient with cancer. Oncologist. (2000) 5:302–11. doi: 10.1634/theoncologist.5-4-302
12. Girgis A, Sanson-Fisher RW. Breaking bad news 1: current best advice for clinicians. Behav Med. (1998) 24:53–9. doi: 10.1080/08964289809596381
13. Fujimori M, Uchitomi Y. Preferences of cancer patients regarding communication of bad news: a systematic literature review. Jpn J Clin Oncol. (2009) 39:201–16. doi: 10.1093/jjco/hyn159
14. Mirza RD, Ren M, Agarwal A, Guyatt GH. Assessing patient perspectives on receiving bad news: a survey of 1337. Patients with life-changing diagnoses. AJOB Empir Bioeth. (2019) 10:36–43. doi: 10.1080/23294515.2018.1543218
15. Hilkert SM, Cebulla CM, Jain SG, Pfeil SA, Benes SC, Robbins SL. Breaking bad news: a communication competency for ophthalmology training programs. Surv Ophthalmol. (2016) 61:791–8. doi: 10.1016/j.survophthal.2016.04.005
16. McCluskey L, Casarett D, Siderowf A. Breaking the news: a survey of ALS patients and their caregivers. Amyotroph Lateral Scler Other Mot Neuron Disord. (2004) 5:131–5. doi: 10.1080/14660820410020772
17. Greiner AL, Conklin J. Breaking bad news to a pregnant woman with a fetal abnormality on ultrasound. Obstet Gynecol Surv. (2015) 70:39–44. doi: 10.1097/OGX.0000000000000149
18. Koochak HE, Yazdi F, Abdolbaghi MH, Salehi MR, Shadloo B, Rahimi-Movaghar A. Breaking HIV news to clients: SPIKES strategy in post-test counseling session. Acta Med Iran. (2016) 54:313–7.
19. Seeman M V. Breaking bad news: schizophrenia. J Psychiatr Pract. (2010) 16:269–76. doi: 10.1097/01.pra.0000386915.62311.4d
20. Milton AC, Mullan B. Views and experience of communication when receiving a serious mental health diagnosis: satisfaction levels, communication preferences, and acceptability of the SPIKES protocol. J Ment Health. (2017) 26:395–404. doi: 10.1080/09638237.2016.1207225
21. Amsalem D, Hasson-Ohayon I, Roe D, Gothelf D. The SPIKES protocol is not applied in the process of breaking bad news to patients with schizophrenia. Isr J Psychiatry. (2019) 56:28–32.
22. Orlander JD, Graeme Fincke B, Hermanns D, Johnson GA. Medical residents' first clearly remembered experiences of giving bad news. J Gen Intern Med. (2002) 17:825–31. doi: 10.1046/j.1525-1497.2002.10915.x
23. Kolarik RC, Walker G, Arnold RM. Pediatric resident education in palliative care: a needs assessment. Pediatrics. (2006) 117:1949–54. doi: 10.1542/peds.2005-1111
24. Meyer EC, Sellers DE, Browning DM, McGuffie K, Solomon MZ, Truog RD. Difficult conversations: Improving communication skills and relational abilities in health care. Pediatr Crit Care Med. (2009) 10:352–9. doi: 10.1097/PCC.0b013e3181a3183a
25. Schlegel C, Woermann U, Rethans JJ, Van Der Vleuten C. Validity evidence and reliability of a simulated patient feedback instrument. BMC Med Educ. (2012) 12:6. doi: 10.1186/1472-6920-12-6
26. Wallace J, Rao R, Haslam R. Simulated patients and objective structured clinical examinations: review of their use in medical education. Adv Psychiatr Treat. (2002) 8:342–8. doi: 10.1192/apt.8.5.342
27. Ryall T, Judd BK, Gordon CJ. Simulation-based assessments in health professional education: a systematic review. J Multidiscip Healthc. (2016) 9:69–82. doi: 10.2147/JMDH.S92695
28. Nellis M, Howell J, Ching K, Bylund C. The use of simulation to improve resident communication and personal experience at end-of-life care. J Pediatr Intensive Care. (2016) 6:91–7. doi: 10.1055/s-0036-1584684
29. Back AL, Arnold RM, Baile WF, Fryer-Edwards KA, Alexander SC, Barley GE, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med. (2007) 167:453–60. doi: 10.1001/archinte.167.5.453
30. Abdool PS, Nirula L, Bonato S, Rajji TK, Silver IL. Simulation in undergraduate psychiatry: exploring the depth of learner engagement. Acad Psychiatry. (2017) 41:251–61. doi: 10.1007/s40596-016-0633-9
31. McNaughton N, Ravitz P, Wadell A, Hodges BD. Psychiatric education and simulation: a review of the literature. Can J Psychiatry. (2008) 53:85–93. doi: 10.1177/070674370805300203
32. Amsalem D, Gothelf D, Soul O, Dorman A, Ziv A, Gross R. Single-day simulation-based training improves communication and psychiatric skills of medical students. Front Psychiatry. (2020) 11:221. doi: 10.3389/fpsyt.2020.00221
33. Loughland C, Kelly B, Ditton-Phare P, Sandhu H, Vamos M, Outram S, et al. Improving clinician competency in communication about schizophrenia: a pilot educational program for psychiatry trainees. Acad Psychiatry. (2015) 39:160–4. doi: 10.1007/s40596-014-0195-7
34. Ditton-Phare P, Loughland C, Duvivier R, Kelly B. Communication skills in the training of psychiatrists: a systematic review of current approaches. Aust N Z J Psychiatry. (2017) 7:675–92. doi: 10.1177/0004867417707820
35. Kowalski C, Sathanandan S. The use of simulation to develop advanced communication skills relevant to psychiatry. BMJ Simul Technol Enhanc Learn. (2015) 1:29–32. doi: 10.1136/bmjstel-2014-000006
36. Liénard A, Merckaert I, Libert Y, Bragard I, Delvaux N, Etienne AM, et al. Is it possible to improve residents breaking bad news skills: a randomised study assessing the efficacy of a communication skills training program. Br J Cancer. (2010) 103:171–7. doi: 10.1038/sj.bjc.6605749
37. Gorniewicz J, Floyd M, Krishnan K, Bishop TW, Tudiver F, Lang F. Breaking bad news to patients with cancer: a randomized control trial of a brief communication skills training module incorporating the stories and preferences of actual patients. Patient Educ Couns. (2017) 100:655–66. doi: 10.1016/j.pec.2016.11.008
38. Yuan YY, Scott S, Van Horn N, Oke O, Okada P. Objective evaluation of a simulation course for residents in the pediatric emergency medicine department: breaking bad news. Cureus. (2019) 11:e3903. doi: 10.7759/cureus.3903
39. Smith RC, Marshall-Dorsey AA, Osborn GG, Shebroe V, Lyles JS, Stoffelmayr BE, et al. Evidence-based guidelines for teaching patient-centered interviewing. Patient Educ Couns. (2000) 39:37–36. doi: 10.1016/S0738-3991(99)00088-9
40. Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in Medicine. 2nd ed. Oxford: Radcliffe Medical Press.
41. Tobler K, Grant E, Marczinski C. Evaluation of the impact of a simulation-enhanced breaking bad news workshop in pediatrics. Simul Healthc. (2014) 9:213–9. doi: 10.1097/SIH.0000000000000031
42. Ditton-Phare P, Sandhu H, Kelly B, Kissane D, Loughland C. Pilot evaluation of a communication skills training program for psychiatry residents using standardized patient assessment. Acad Psychiatry. (2016) 40:768–75. doi: 10.1007/s40596-016-0560-9
43. Fallowfield L, Jenkins V, Farewell V, Solis-Trapala I. Enduring impact of communication skills training: results of a 12-month follow-up. Br J Cancer. (2003) 89:1445–9. doi: 10.1038/sj.bjc.6601309
44. Farooq S, Johal RK, Ziff C, Naeem F. Different communication strategies for disclosing a diagnosis of schizophrenia and related disorders. Cochrane Database Syst Rev. (2017) 10:CD011707. doi: 10.1002/14651858.CD011707.pub2
45. Burg LB, Daetwyler CJ, Filho GRO, Del Castanhel F, Grosseman S. What skills really improve after a flipped educational intervention to train medical students and residents to break bad news? J Educ Learn. (2019) 8:35. doi: 10.5539/jel.v8n3p35
46. Martin A, Weller I, Amsalem D, Duvivier R, Jaarsma D, de Carvalho Filho M. Co-constructive patient simulation: a learner-centered method to enhance communication and reflection skills. Simul Healthc. (2020). doi: 10.1097/SIH.0000000000000528. [Epub ahead of print].
Keywords: simulation, residents, medical education, delivering difficult news, psychiatry
Citation: Amsalem D, Martin A, Mosheva M, Soul O, Korotkin L, Ziv A, Gothelf D and Gross R (2021) Delivering Difficult News: Simulation-Enhanced Training Improves Psychiatry Residents' Clinical Communication Skills. Front. Psychiatry 12:649090. doi: 10.3389/fpsyt.2021.649090
Received: 03 January 2021; Accepted: 10 February 2021;
Published: 05 March 2021.
Edited by:
Armida Mucci, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Stefano Barlati, University of Brescia, ItalyCopyright © 2021 Amsalem, Martin, Mosheva, Soul, Korotkin, Ziv, Gothelf and Gross. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Doron Amsalem, ZG9yb24uYW1zYWxlbUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.