
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 29 April 2021
Sec. Addictive Disorders
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.639393
This article is part of the Research Topic Opioids in the Time of the COVID-19 Pandemic: From Cellular Mechanisms to Public Health Policy View all 13 articles
 Seyed Ramin Radfar1,2
Seyed Ramin Radfar1,2 Cornelis A. J. De Jong3
Cornelis A. J. De Jong3 Ali Farhoudian4*
Ali Farhoudian4* Mohsen Ebrahimi5,6
Mohsen Ebrahimi5,6 Parnian Rafei7
Parnian Rafei7 Mehrnoosh Vahidi4Masud Yunesian8
Mehrnoosh Vahidi4Masud Yunesian8 Christos Kouimtsidis9
Christos Kouimtsidis9 Shalini Arunogiri10Omid Massah11Abbas Deylamizadeh12Kathleen T. Brady13
Shalini Arunogiri10Omid Massah11Abbas Deylamizadeh12Kathleen T. Brady13 Anja Busse14 ISAM-PPIG Global Survey Consortium
Anja Busse14 ISAM-PPIG Global Survey Consortium Marc N. Potenza15
Marc N. Potenza15 Hamed Ekhtiari16
Hamed Ekhtiari16 Alexander Mario Baldacchino17
Alexander Mario Baldacchino17Background: The coronavirus disease 2019 (COVID-19) pandemic has impacted people with substance use disorders (SUDs) worldwide, and healthcare systems have reorganized their services in response to the pandemic.
Methods: One week after the announcement of the COVID-19 as a pandemic, in a global survey, 177 addiction medicine professionals described COVID-19-related health responses in their own 77 countries in terms of SUD treatment and harm reduction services. The health responses were categorized around (1) managerial measures and systems, (2) logistics, (3) service providers, and (4) vulnerable groups.
Results: Respondents from over 88% of countries reported that core medical and psychiatric care for SUDs had continued; however, only 56% of countries reported having had any business continuity plan, and 37.5% of countries reported shortages of methadone or buprenorphine supplies. Participants of 41% of countries reported partial discontinuation of harm-reduction services such as needle and syringe programs and condom distribution. Fifty-seven percent of overdose prevention interventions and 81% of outreach services were also negatively impacted.
Conclusions: Participants reported that SUD treatment and harm-reduction services had been significantly impacted globally early during the COVID-19 pandemic. Based on our findings, we highlight several issues and complications resulting from the pandemic concerning people with SUDs that should be tackled more efficiently during the future waves or similar pandemics. The issues and potential strategies comprise the following: (1) helping policymakers to generate business continuity plans, (2) maintaining the use of evidence-based interventions for people with SUDs, (3) being prepared for adequate medication supplies, (4) integrating harm reduction programs with other treatment modalities, and (5) having specific considerations for vulnerable groups such as immigrants and refugees.
Coronavirus disease 2019 (COVID-19) was announced as a pandemic by the World Health Organization (WHO) on March 11, 2020 (1). COVID-19 quickly became a global concern given the rapid transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (the infectious agent), lack of a vaccine or evidence-based treatments, person-to-person airborne spread of SARS-CoV-2, and high mortality of COVID-19 in specific populations, especially marginalized groups and/or those with preexisting conditions (2). Lack of capacity to anticipate, cope with, resist, and recover from COVID-19-related health consequences are related to individual vulnerability (3). To manage the current situation successfully, vulnerable groups should be recognized and helped with special considerations by relevant health systems (4).
According to the World Drug Report 2020, among ~269 million people with past-year drug use, over 35 million people experienced substance use disorders (SUDs) (5). People with SUDs (PWSUDs) may be particularly vulnerable to COVID-19 and its complications for multiple reasons (6). PWSUDs are at a higher risk of psychiatric problems such as mixed affective states (7); vice versa, polysubstance use and alcohol use disorder are common among patients with bipolar disorders (8). Moreover, PWSUDs experience underlying diseases that constitute risk factors for COVID-19 infection or can be exacerbated by it; for instance, long-term use of substances may cause cardiovascular problems (9) and chronic obstructive pulmonary disease (10). Such comorbidities may exacerbate superimposed COVID-19 symptoms and lead to higher mortality rates (11). Poor immune system functioning is also prevalent in PWSUDs because of chronic alcohol and drug use and blood-borne or sexually transmitted illnesses (12), poor nutritional status (13), and socioeconomic factors (14). Among PWSUDs, people who inject drugs (PWIDs) are at exceptionally high risk of COVID-19, as well as overdoses, unsafe injections, and risky sex (15).
Psychological conditions (e.g., phobia, anxiety, and panic attacks) during natural disasters and pandemics, which may be precipitated, perpetuated, or exacerbated through social isolation and quarantine, may lead at-risk people to start and/or relapse into drug taking (11, 16). Psychiatric comorbidity has a negative impact on recovery from COVID-19 and may increase the risk of non-fatal and fatal overdoses and suicides (16). In the general population, COVID-19 and related concerns such as potential mortality may act as internal stressors (17) and promote cognitive impairments (18) in domains such as decision making (19), problem solving (20), and attention (21) and thus may increase the incidence and prevalence of psychiatric disorders including PWSUDs (22).
Stigma may undermine social cohesion, contributing to situations in which the virus is more, not less, likely to spread. Such spread may result in more severe health problems and difficulties controlling a disease outbreak (23). There is an elevated likelihood for PWSUDs to be homeless and live in crowded shelters and neighborhoods (24). Synergistically, poor economic status linked to limited access to health care (25) may exacerbate risks for PWSUDs and PWIDs (15). Drug supply chains may be disrupted, and changes in licit and illicit markets may be accompanied by reductions in quality and safety (5, 26).
Furthermore, patients' accessibility to treatment services could be restricted due to lockdown policies (27). Patients receiving opioid agonist treatment (OAT) may not be able to access daily doses of medications (11); spatial distancing may make home detoxification difficult; and closing of non-essential services and utilizing staff and other resources to manage acute COVID-19 cases could result in sudden and uncoordinated closures of services for PWSUDs (26). Individuals who use multiple substances may be particularly impacted (28). Adaptive capacities of systems to epidemic situations that need coordinated responses may relate directly to vulnerabilities of the same systems (29). Accessibility to and equal distribution of wealth (financial and other resources, reliable and correct information and communication channels, appropriate and proportionate working technologies) compounded by reductions in social and relationship capital may impact social resilience to coping with pandemics (30).
To understand better complexities that are challenging addiction treatment and harm reduction services globally, the International Society of Addiction Medicine (ISAM) has been conducting a global longitudinal survey aiming to evaluate rapidly and over time how different countries are maintaining and/or reorganizing their substance use treatment and harm reduction services during the COVID-19 pandemic. This paper will report how different countries have adapted their health system response to emerging needs in the first month after the WHO's official announcement of the pandemic.
Description of the methodology used for this survey has been published as a study protocol (31). Potential respondents were contacted on April 4, 2020 asking about the COVID-19 pandemic impact on PWSUDs in their own countries. Data collection was concluded on May 8, 2020.
The questionnaire consisted of 92 questions in two main areas: (1) situation assessment during the pandemic and (2) health responses to the pandemic. This paper will focus on health responses during the COVID-19 pandemic period (31). Results on the situation assessment are reported in another publication (32).
Questions around health responses to the pandemic were grouped into three categories:
(1) systems available to respond to acute emerging needs due to the COVID-19 pandemic within substance use services;
(2) availability of protocol and/or guidelines around COVID-19 and PWSUDs, and
(3) reduction in face-to-face contacts because of lockdown policies.
To assess respondents' overall views, they were asked to score the “overall situation at a glance” rating scale questions (RSQ) (between 1 and 10 with 1 for the worst situation and 10 for the best situation) based on their opinion regarding the overall quality of the situation of their country for each of the above three sections.
The 2019 statistical annex of World Economic Situation and Prospects (WESP) (33) was used to categorize responding countries. Very low- and low-income categories were merged into one, retaining middle- and upper-income countries designations. In figures, countries' names are sorted alphabetically in each group of high-, middle- and low-income categories. The number of respondents (for countries with more than one respondent) is indicated in front of their names, and numbers in each column represent valid responses from each country.
Statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA) and RStudio (version 1.2.1335). Descriptive data are presented as means and percentages for each country's response mean (percentage), as well as an average to the global responses.
The survey protocols and all materials, including the survey questionnaires, received approval from the University of Social Welfare and Rehabilitation Sciences, an ethics committee in Tehran, Iran (Code: IR.USWR.REC.1399.061).
A total of 177 respondents from 77 countries participated. Figure 1 shows the distribution of the countries and the number of participants from each. Among 177 respondents, 95 (53.7%) were from high-income, 34 (19.2%) from middle-income, and 48 (27.1%) from low-income countries (“World Economic Situation and Prospects 2019,” 2019). Table 1 shows respondents' demographic characteristics classified by their associated countries' income.
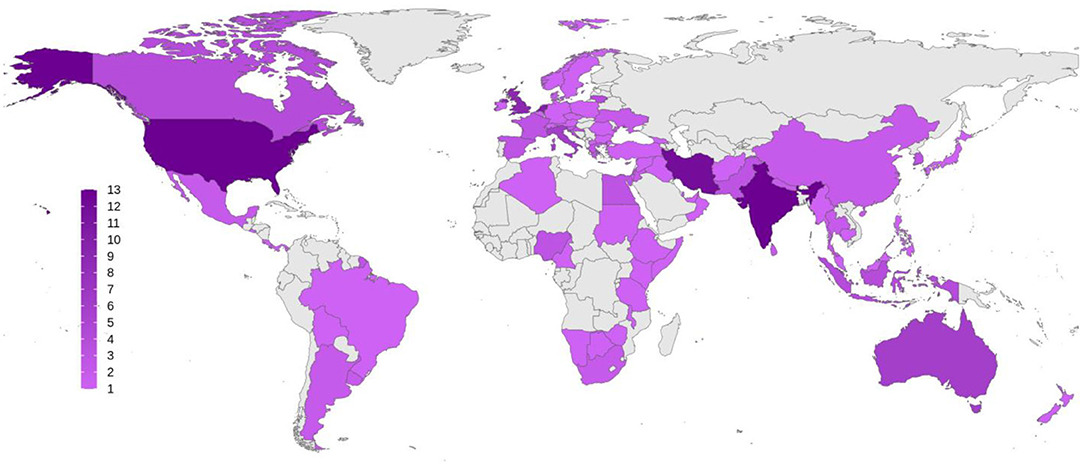
Figure 1. Global distribution of the respondents to the survey. Number of participants from each country is demonstrated as a color spectrum from light to dark purple.
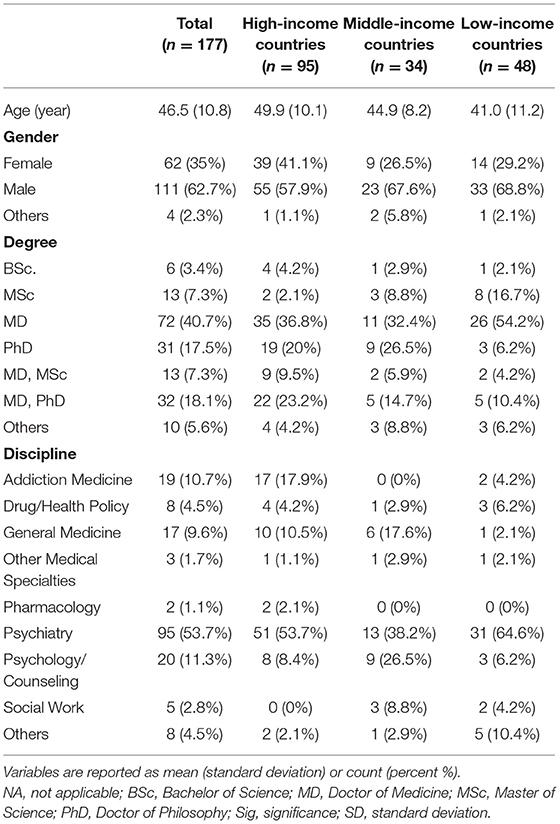
Table 1. Survey respondents' demographic, educational, and professional information classified by their countries' income status.
Among respondents from high-income countries (N = 95), 69% answered that business continuity/contingency plans had been implemented in their countries to make sure that services continued to operate for PWSUDs during the COVID-19 pandemic compared to 40.7% in the middle-income (N = 34) and 53.8% (N = 48) in low-income countries. Overall, respondents from 56% of participating countries reported that business contingency plans had been arranged to help ensure the continuity of services during the pandemic (Figure 2).
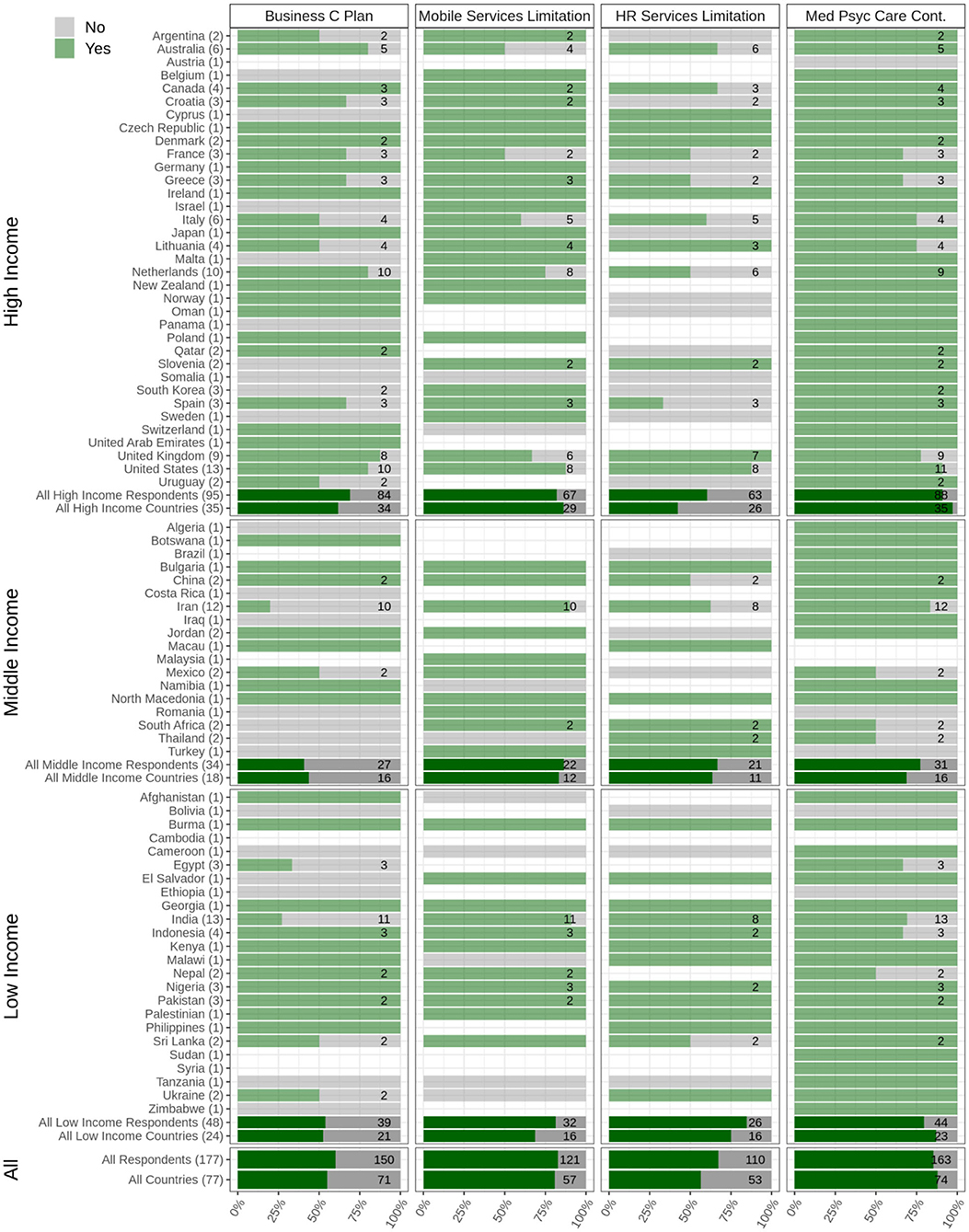
Figure 2. Availability and accessibility of treatment and harm reduction services. Data relating to arranging business continuity plans (Business C Plan), limitations that mobile services faced during the pandemic (mobile services limitation), limitations that harm reduction services faced during the pandemic (HR services limitation), and continuity of other medical and psychiatric necessary care (Med Psyc Care Cont.) are depicted. The Figure shows responses from respondents from 77 countries categorized into low-, middle-, and high-income countries. The light green bars and the numbers associated with each country show the survey respondents who reported having experienced limitations regarding the question in their country (Yes), and the gray bars show the survey respondents who reported having experienced no limitations regarding the question in their country (No). The dark green bars show the overall responses in each category (low, middle, and high income) as well as overall responses.
Among respondents from high-income countries (N = 95), 57% answered that treatment and harm reduction services for PWSUDs had been available and accessible in their countries during the pandemic onset compared to 51.6% in the middle-income (N = 34) and 63% in low-income (N = 48) countries. Overall, respondents from 59% of participating countries reported that treatment and harm reduction services for PWSUDs had been available and accessible during the initial period of the COVID-19 pandemic (Figure 2).
Respondents from over 81% of participating countries (N = 77) reported having experienced limitations in the usage of any outreach services due to lockdown policies for homeless PWSUDs. Furthermore, respondents from 57% of participating countries reported having experienced limitations in their harm reduction overdose services during the initial period of the pandemic. Problems with the distribution of take-home naloxone were reported by respondents from 57% of participating countries. Respondents from 54.8% of the participating countries reported shortages in needle and syringe programs (NSPs) and/or with respect to condom distribution.
Among respondents from high-income countries (N = 95), 90% answered that medical and psychiatric care for PWSUDs had been available during the initial stages of the pandemic compared to 77.4% in middle-income (N = 34) and 79.5% in low-income (N = 48) countries. Overall, respondents in 88% of participating countries reported that necessary medical and psychiatric care for PWSUDs had continued in their countries during this period (Figure 2). However, respondents in 37.5% of participating countries reported having experienced shortages of opioid medications (methadone or Buprenorphine) (Figure 3).
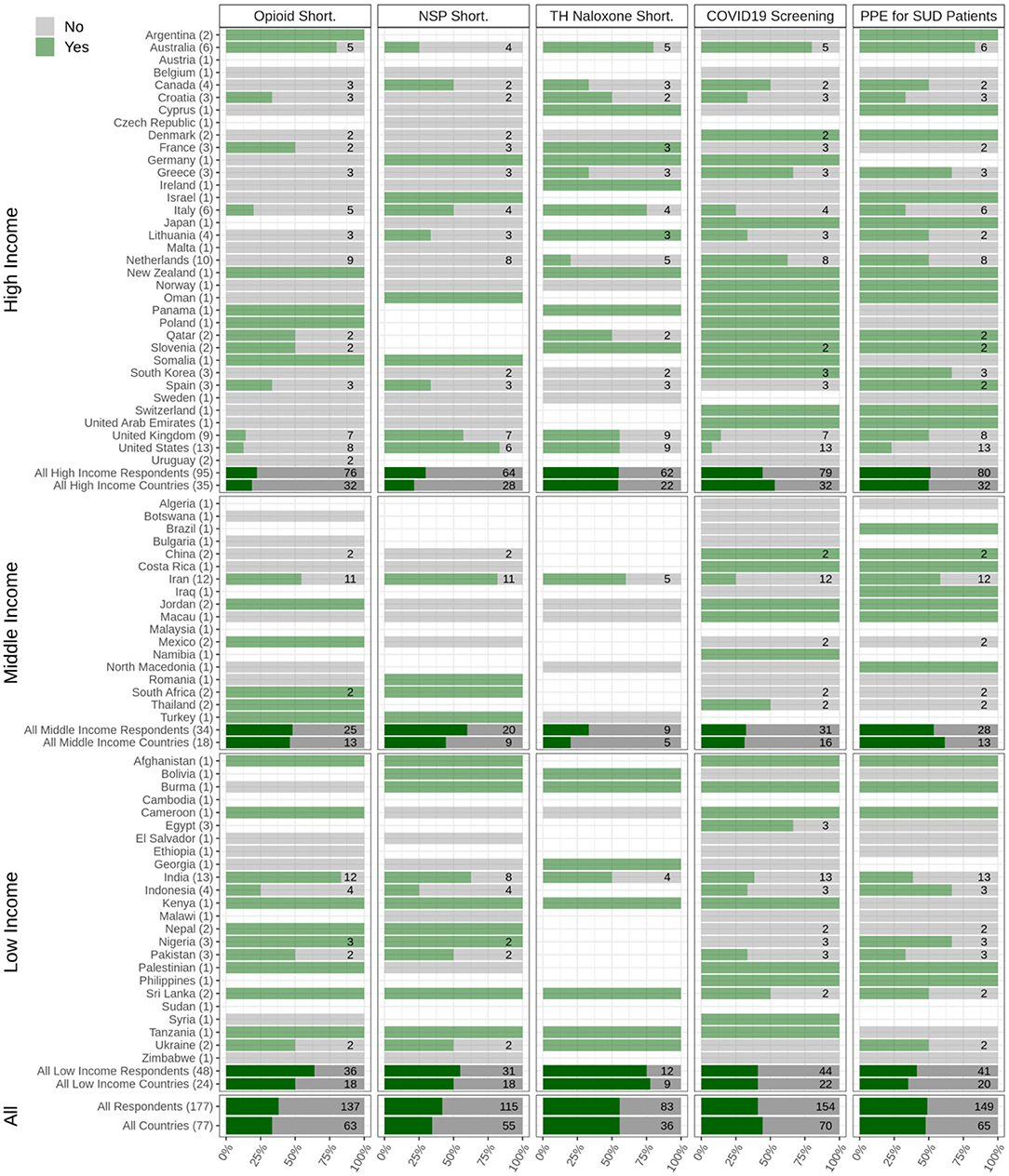
Figure 3. Medical services for people with substance use disorders during the pandemic. The responses of respondents from 77 countries are shown, categorized into low-, middle-, and high-income countries to the questions related to the shortages in opioid medication (opioid short.), disruption in needle and syringe and/or condom distribution services (NSP Short.), availability or shortages in take-home naloxone services (TH Naloxone short.), availability of COVID-19 screening kits and equipment for people with substance use disorders (PWSUDs) in their countries (COVID-19 screening), and personal protective equipment provision to PWSUDs (PPE for SUD patients).
Only 44.3% of respondents from high-income (N = 95), 32.2% from middle-income (N = 34), and 40.1% from low-income (N = 48) countries reported that COVID-19 screening and/or diagnosis test kits based on local/national guidelines for PWSUD had been available in their country. Overall, respondents from only 48% of the participating countries reported that there had been enough personal protective equipment (PPE) available for PWSUDs during the initial stage of the pandemic. Respondents from 77.7% of participating countries reported SUD health workers' safety as a concern for employers in the outpatient treatment centers, 66.4% had received training regarding their safety, and 72.9% reported that they had had access to enough PPE (Figure 3).
The distribution of other responses on the effect of COVID-19 on substance use treatment and/or harm reduction services to vulnerable groups such as children, women, pregnant women, and immigrants or refugees can be seen in Table 2 and Figure 4. Table 2 shows the existence of services for children, women, pregnant women, and refugees or immigrants among the countries based on their income group.
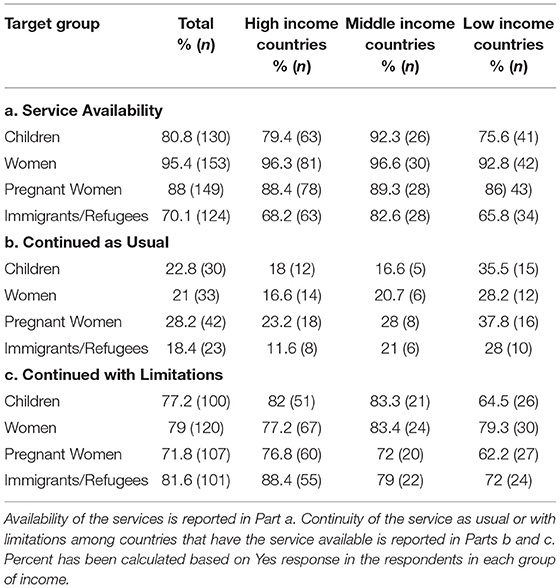
Table 2. Services for children, women, pregnant women, and refugees or immigrants among the countries based on their income group.
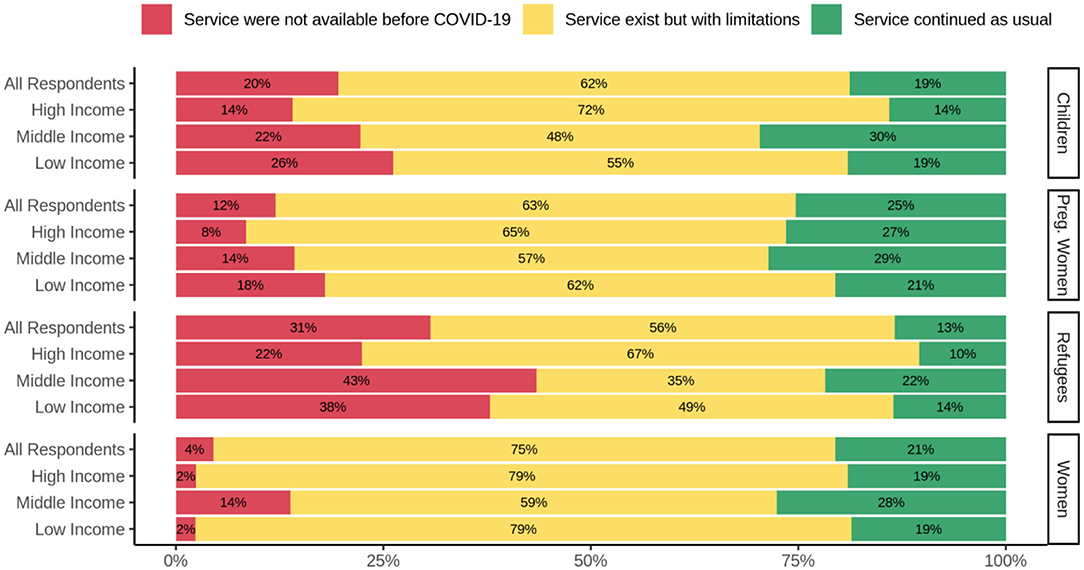
Figure 4. Effects of COVID-19 on substance use treatment and/or harm reduction services for vulnerable groups. Services for children, pregnant women, refugees, and women, in high-, middle-, and low-income countries are depicted. The red, yellow, and green bars depict the responses indicating lack of availability of services during the COVID-19 pandemic, the existence of limited services, and usual service provision, respectively.
Overall, 22.8% of all respondents replied that service for children continued as usual compared to 77.2% that replied service for children continued but with limitations. According to the responses, in all three groups of income countries, treatment and/or harm reduction services for pregnant women were a group with minimum impact from COVID-19. Refugees and the immigrant population was the group that their services impacted more than other groups due to COVID-19. Only 18.4% replied that service for refugees and/or immigrants population continued as usual, and 81.6% replied that this service continued but with limitations.
Overall, respondents from 48% of the participating countries reported the presence of local and/or national guidelines tailored to be used during the initial stage of the pandemic (60.2% in high-income, 57.1% in middle-income, and 29% in low-income countries). Among respondents from high-income countries, 65.7% answered that there had been a protocol available for COVID-19 screening in various treatment sectors for PWSUDs or harm reduction facilities compared to 60% in middle-income and 82.3% in low-income countries.
Over 76% of respondents from high-income, 63.3% from middle-income, and 63% from low-income countries reported that there had been guidelines available that helped service providers in the management and/or referral of PWSUDs with symptoms of COVID-19.
Most respondents replied that there had been plans to restrict personal contacts and decrease patients' commutes for treatment in their countries (86, 90, and 86.6% in high-, middle- and low-income countries, respectively, and 85% overall) due to their national and regional lockdown policies.
As a result, respondents from 80% of the participating countries reported that clinicians had been prescribing longer-period prescriptions (e.g., 28 days rather than weekly) to PWSUDs during the onset of the pandemic (Figure 5).
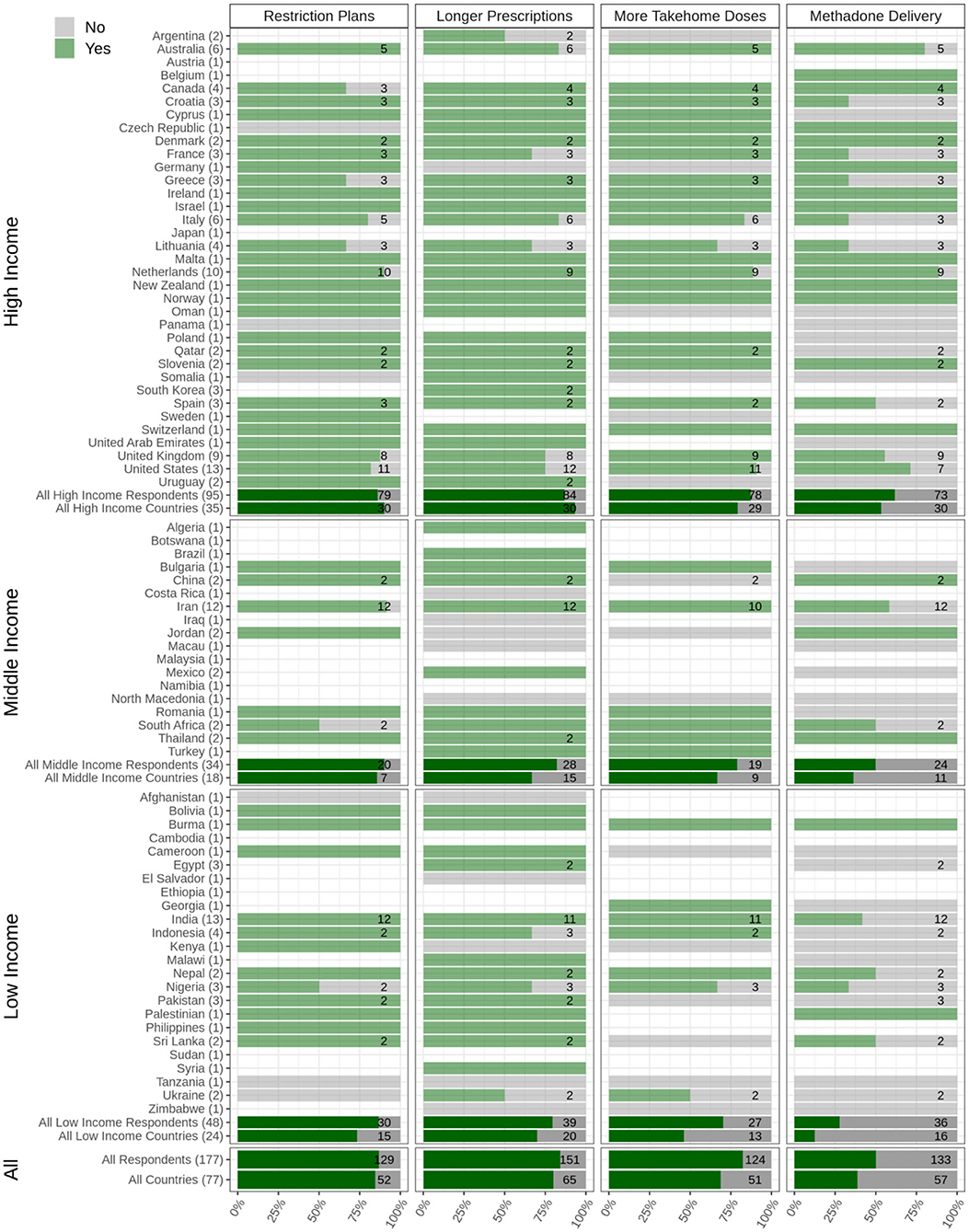
Figure 5. Health policies for COVID-19 among people with substance use disorders (PWSUDs). Plans to restrict any personal contact, provision of prescriptions of longer durations, provision of more take-home doses of opioids drugs, and availability of any program for delivering opioid drugs to patients' homes are depicted. The Figure shows responses from 77 countries, which are categorized into low, middle, and high income. The light green bars and the numbers associated with each country show the survey respondents who reported having experienced limitations regarding the question in their country (Yes), and the gray bars show the survey respondents who reported having experienced no limitations regarding the question in their country (No). The dark green bars show the overall responses in each category (low, middle, and high income) as well as overall responses.
Additionally, around 69% of participating countries reported that clinicians within OAT programs had provided more take-home doses of methadone and/or Buprenorphine during the onset of the pandemic. Regionally, 61.6% of respondents from high-income, 50% from middle-income, and 27.7% from low-income countries reported that this approach had been used in their countries (Figure 5).
Respondents from high-income countries most frequently reported having had the availability of long-acting injectable Buprenorphine (34.9%; n = 63). Overall, respondents from 22% of participating countries reported that long-acting injectable Buprenorphine had been available as a therapeutic option.
Figure 6 shows the average score of each question based on income categorization. The maximum contrast between high- and low-income countries was seen in the availability and access to treatment and harm reduction services. Maximum and minimum differences between high- and middle-income countries were observed in flexibility in service provision and countries' reactions to the COVID-19 pandemic, respectively.
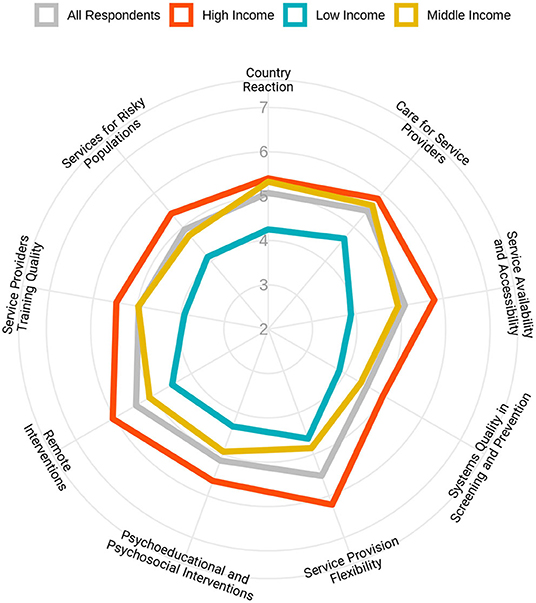
Figure 6. Flexibility of health responses for people with substance use disorders in response to the pandemic in different domains based on the income levels of the countries. Respondents were asked to rate the overall flexibility of their health system in nine different domains, from 1 (extremely poor) to 10 (extremely good).
An average for all rating scale questions in different domains has been calculated, and Figure 7 shows the results in a global map format.
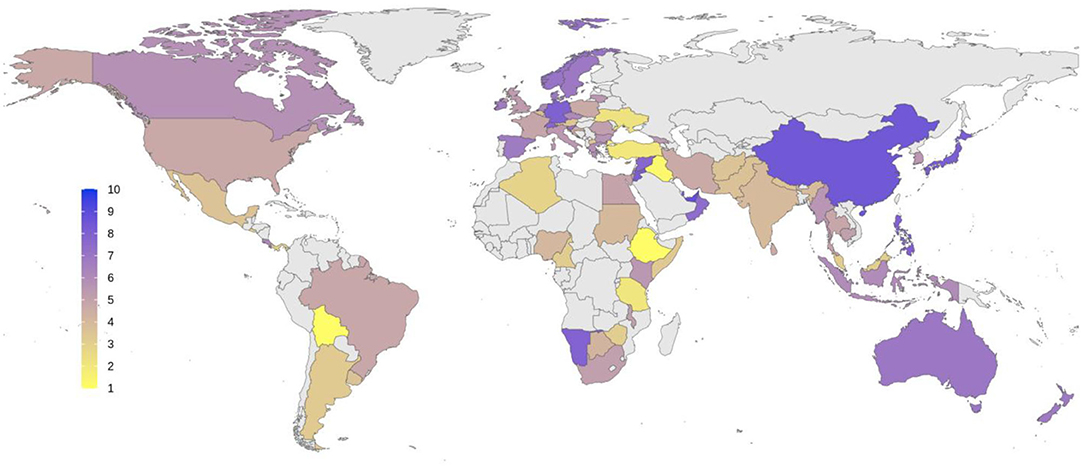
Figure 7. The overall quality of health response to COVID-19 pandemic based on the subjective ratings by respondents from different countries. Average scores were measured based on responses in nine domains depicted in Figure 6. Score 1 represents the worst quality in response, and 10 represents the best situation in favor of health services. Average scores for each country are shown using a color spectrum from yellow to blue.
The emergence of COVID-19 in early 2020 raised considerable challenges for substance use treatment and harm reduction programs worldwide, as reflected in this global survey. The need for effective spatial distancing and isolation to protect patients, the treatment workforce, and people in contact with patients and health workers have placed increased demands on treatment services provision, with potential imbalances in impact on particularly vulnerable patient populations (28). Here, in this global survey, we have explored different challenges and health responses in 77 countries. Our findings showed that respondents from 56% of participating countries reported business contingency plans had been arranged to help ensure that services would continue to operate during the pandemic, which is compatible with responses to another question indicating that 41% of respondents believed there had not been sufficient availability and accessibility of treatment and harm reduction services during the onset of the pandemic in their countries at the time of survey completion.
As a preventative measure to reduce COVID-19 spread, all international and national published guidelines advised limited but effective ways regarding how to initiate treatment, support stabilization, and maintenance and continue to provide harm reduction measures to treatment-seeking and other populations with substance use problems (4, 34). These recommendations often included extending flexibility in OAT services with reduced supervision of doses and increased home delivery (35). Another step taken to adjust to the present situation included expanding telemedicine and teletherapy services (5, 28, 34).
The COVID-19 pandemic is synergistically interacting with a substance use epidemic globally, creating a syndemic [defined as a synergistic epidemic, the aggregation of two or more concurrent or sequential epidemics, which exacerbate the prognosis and burden of disease (36)]. During the COVID-19 pandemic, marginalized people, including PWSUDs, are at greater risk of increased morbidity and mortality (37). These syndemic disadvantaged populations may be more likely to experience disparate, possibly substandard, service provision in systems prioritizing resource needs around a pandemic response (Inverse Response Law and Inverse Care Law) (38). Such inequities may present at macrolevels around effective and appropriate policymaking at national, organizational, and local levels (38) and at microlevels around areas of access to resources, social services, public health benefits of medical treatments, pharmacies, healthcare facilities, and provision of medical equipment (39).
Proactive business continuity plans for PWSUDs are important for all governments as part of COVID-19 remobilization plans and possible future responses to similar pandemics to support and avert delays and inequities in responses. Overall, PWSUDs are at risk for a negative impact of COVID-19 (6); it is also essential to mention that gender differences play a substantial role in the vulnerabilities of PWSUDs (40). Our findings showed that 88% of respondents reported continuity of other necessary medical and psychiatric care compared to <60% who reported the existence of business continuity/contingency plans and enough availability and accessibility of treatment and harm reduction services for PWSUDs. These findings suggest that policymakers and health authorities in each country could have possibly made more appropriate decisions in order to protect at-risk and marginalized PWSUDs including those who may be homeless, have HIV/AIDS, hepatitis, or multiple and complex morbidities. Such decisions may involve considering how to subtly provide scheduled and new appointments and prescription medications in the circumstances of lockdowns.
This study has multiple limitations that have been described in detail in the study protocol of the survey (31). The responses obtained were intentionally based around personal opinions of addiction medicine experts to help understand the “state of things in real life” rather than objective epidemiological data, which would have been considerably delayed. Therefore, ethical approval has not been taken from each of the countries that participated in the survey. The limited number of respondents makes this information non-representative and possibly biased. In other words, the survey results might be subject to bias and not demonstrate a true reflection of addiction services in their countries. Hence, the findings (opinions) have a high chance of subjective biasing. Sampling bias is another limitation, and indeed due to sampling methodology, the participants were not necessarily oriented to all domains of the questionnaire.
Given the urgency of the COVID-19 pandemic, the paper aims to alert and inform colleagues around the world and facilitate collaboration. Due to the time limitations, the questionnaire was circulated only in English. Therefore, some experts may have withdrawn from the survey for lingual reasons, and others may have answered questions less precisely.
Based on our findings in this global survey, we conclude that the addiction medicine systems in all countries, regardless of income level, have been affected to some degree by the COVID-19 pandemic. Depending on the different domains and the ability of countries to adapt to existing conditions, these effects may differ across jurisdictions. Income level may relate importantly to responses and impact vulnerable groups like PWSUDs. Although this survey's findings should be interpreted with caution, the translation of our study results as recommendations for addiction medicine services, and policymakers would hopefully support a more resilient system of care that improves responses to future COVID-19 waves and other pandemics.
Continuity of services, especially in crises, needs certain evidence-based and locally tailored protocols and guidelines. In our study, addiction medicine professionals reported that most of their countries did not provide early guidelines or protocols to tailor their services to the pandemic. It is important to consider that respondents in only one-third of low-income countries reported the availability of such guidelines compared to respondents in half of the high-income countries. Another survey (41) conducted in four high-income regions (New South Wales, Ireland, Scotland, New York State, and British Columbia) found that special guidelines in response to the new situation and assurance of continuity of the services were available very soon after the start of lockdown, which is consistent with our findings that high-income countries had a more timely response in this domain. In the absence of guidelines and protocols, clinicians and service providers may not effectively balance various competing ethical and professional issues when they are making clinical and operational decisions when many things may be happening that could potentially be conflicting in nature (e.g., maintaining stability but reducing therapeutic contacts). Guidelines also allow stakeholders to improvise and identify innovative ways through evidence-based solutions to decrease the dual burden of substance use and COVID-19 infection (42). International organizations such as the WHO and United Nations Office of Drug Control (UNODC) and other related groups such as the International Society of Addiction Medicine (ISAM), International Society of Substance Use Professionals (ISSUP), and World Federation Against Drugs (WFAD) should provide adequate support to raise policymakers' knowledge in the area of addiction medicine on how to establish business continuity committees during initial stages of pandemics in order to make advanced care planning decisions through effective leadership.
Additionally, our results showed that respondents reported the shortage of opioid medication for maintenance treatment from about 40% of participating countries. Lack of opioid medications in patients undergoing maintenance treatment is a risk factor for a lapse, relapse, and/or overdoses. This situation may become more severe when transport and other supply chains are disrupted, compounded with the reduced provision by pharmacies and other dispensing outlets either due to spatial distancing, and reduced hours of service and/or closing during the pandemic.
According to this finding, we recommend that governments and local authorities be cognizant that an effective response system is based on a well-informed and supportive environment. Available and communicated international and national clinical guidelines are pivotal in future responses to similar pandemics when supporting PWSUDs.
The World Drug Report 2020 stated that “If Governments respond the same way to the current economic slump, interventions such as prevention of drug use and related risk behaviors and drug treatment services could be hard hit” (43). Substance use accounts for ~11% of the global health burden (44). Treatment is a critical strategy for reducing the burden of the disease. A study of World Mental Health Surveys (45) found that only 7.1% of PWSUDs had received at least minimally adequate treatment in the past year (10.3, 4.3, and 1.0%, respectively, in high-, upper-middle, and low/lower-middle-income countries) (46). Poor access to treatment, awareness/perceived treatment need, and compliance (on the part of both provider and client) have been reported to be the main barriers to substance use treatment (46).
Our results also show that harm reduction services seem to be among the most affected during the initial stages of the COVID-19 pandemic. Eighty-one percent of participating countries reported limitations in usage of any mobile and other outreach services due to lockdown policies for homeless PWSUDs, with respondents from 57% of participating countries reporting limitations in their harm reduction overdose services during the initial period of the pandemic. This was compounded with reported problems with the distribution of take-home naloxone as reported by respondents from 57% of participating countries. Finally, respondents from 54.8% of participating countries reported that there had been shortages at needle and syringe programs and/or of condom distribution. International organizations with regional and local government structures should create contingencies around adequate supplies of medications such as methadone and Buprenorphine. Harm reduction services, especially outreach services, are among the most effective strategies for preventing HIV, hepatitis C virus (HCV), and hepatitis B virus (HCV) transmission among the most at-risk populations (47).
Pregnant women and immigrants/refugees with SUDs are particularly among vulnerable groups. According to our survey responses, pregnant women were perceived as relatively less impacted during the initial period of the pandemic. This is reassuring, as discontinuity of treatment services could place not only a pregnant woman at high risk but also the developing fetus. However, refugee and immigrant populations were reported as having had their services impacted more than other groups due to the pandemic. Only 12.9% of respondents replied that service for refugees and/or immigrants population continued as usual, and 57.3% replied that this service continued but with severe limitations (48).
These findings highlight the fact that harm reduction initiatives should be seen as an integral part of an evidence-based treatment program and not as an adjunct to failed treatment and/or solely as a public health response to reduce blood-borne diseases. Service providers should be considering identifying person-centered, continuous care provision in all therapeutic options available (harm reduction initiatives included), especially during pandemic situations.
Lastly, our findings suggest that, in general, in multiple domains of countries' reactions to the pandemic (e.g., availability of and access to treatment and harm reduction, screening and early interventions, flexibility in service provision and services for special and high-risk populations), the COVID-19 pandemic has had a more negative impact that is linked to the income level of countries. Vulnerable groups such as immigrants and refugees with SUDs should have access to all possible therapeutic options available as described in the UN charter in the Human Rights Convention (“International Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families”). Appropriate evidence-based services must be designed and implemented by health authorities for such vulnerable groups. Availability of all relevant resources is essential in the delivery of quality services.
Due to the methodological limitations of the study, the findings of this survey might not demonstrate the exact situation of the countries. AB is a staff member of UNODC. The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the decisions or policies of the UNODC or other organizations.
The raw data supporting the conclusions of this article will be made available by the authors upon request.
The studies involving human participants were reviewed and approved by The University of Social Welfare and Rehabilitation Sciences ethics committee, Tehran, Iran (Code: IR.USWR.REC.1399.061). The patients/participants provided their written informed consent to participate in this study.
SRR, AF, HE, CD, and AMB conceived and designed the study. SRR, AF, PR, MV, HE, CD, and AMB conducted the survey and collected the data. ME and PR analyzed the data and ran the statistical analyses. SRR, AF, HE, CD, MY, and AMB supervised the analysis and gave conceptual advice. SRR, AF, PR, MV, HE, CD, and AMB contributed to drafting the manuscript. CK, SA, AB, and MP edited the manuscript. All authors discussed the results and implications and commented on the final manuscript.
Adrian Octavian Abagiu1, Franck David Noel Abouna2, Mohamed Hassan Ahmed3, Basma Al-ansari4, Feda Mahmmoud Abu Al-khair5, Mandhar Humaid Almaqbali6, Atul Ambekar7, Hossein Mohaddes Ardabili8, Sidharth Arya9, Victor Olufolahan Lasebikan10, Murad Ali Ayasreh11, Debasish Basu12, Zoubir Benmebarek13, Roshan Bhad7, Mario Blaise14, Nicolas Bonnet15, Jennifer Brasch16, Barbara Broers17, Jenna L. Butner18, Moses Camilleri19, Giovanna Campello 20, Giuseppe Carra21, Ivan Celic22, Fatemeh Chalabianloo23, Abhishek Chaturvedi24, José de Jesús Eduardo Noyola Cherpitel25, Kelly J. Clark26, Melissa Anne Cyders27, Ernesto de Bernardis28, John Edward Derry29, Naveen Kumar Dhagudu30, Pavla Dolezalova31, Geert Dom32, Adrian John Dunlop33, Mahmoud Mamdouh Elhabiby34, Hussien Elkholy35, Nsidibe Francis Essien36, Ghandi Ilias Farah37, Marica Ferri38, Georgios D Floros39, Catherine Friedman40, Clara Hidalgo Fuderanan41, Gilberto Gerra17, Abhishek Ghosh12, Maka Gogia42, Ilias A. Grammatikopoulos43, Paolo Grandinetti44, Amira Guirguis45, David Gutnisky46, Paul Steven Haber47, Peyman Hassani-Abharian48, Zahra Hooshyari49, Islam Ibrahim Mokhtar Ibrahim34, Hada Fong-ha Ieong50, Regina Nova Indradewi51, Shelly Iskandar52, Shobhit Jain53, Sandi James54, Seyyed Mohammad hossein Javadi55, Keun Ho Joe56, Darius Jokubonis57, Acka Tushevska Jovanova58, Rama Mohamed Kamal59, Alexander Ivanov Kantchelov60, Preethy Kathiresan7, Gary Katzman61, Paul Kawale62, Audrey Margaret Kern63, Felix Henrique Paim Kessler64, Sung-Gon Sue Kim65, Ann Marie Kimball66, Zeljko Kljucevic67, Kristiana Siste68, Roneet Lev69, Hae Kook Lee70, Aiste Lengvenyte71, Shaul Lev-ran72, 73, Geni Seseja Mabelya74, Mohamed Ali El Mahi75, J. Maphisa Maphisa76, Icro Maremmani77, Laura Masferrer78, Orlagh McCambridge79, Garrett Gregory McGovern80, Aung Kyi Min81, Amir Moghanibashi-Mansourieh56, Jazman Mora-Rios82, Indika Udaya Kumara Mudalige83, Diptadhi Mukherjee84, Pejic Munira Munira85, Bronwyn Myers86, Jayakrishnan Menon T N87, Venkata Lakshmi Narasimha88, Nkemakolam Ndionuka89, Ali-Akbar Nejatisafa90, Kamran Niaz20, Asad Tamizuddin Nizami91, Jan H. Nuijens92, Laura Orsolini93, Vantheara Oum94, Adegboyega Adekunle Oyemade95, Irena Rojnia Palavra96, Sagun Ballav Pant97, Joselyn Paredes98, Eric Peyron99, Randall Alberto Quirós100, Rouhollah Qurishi101, Noor ul Zaman Rafiq102, Ranjini Raghavendra Rao103, Woraphat Ratta-apha104, Karren-Lee Raymond105, Jens Reimer106, Eduardo Renaldo107, Tara Rezapour108, James Roy Robertson109, Carlos Roncero110, Fazle Roub111, Elizabeth Jane Rubenstein112, Claudia Ines Rupp113, Elizabeth Saenz20, Mohammad Salehi114, Lampros Samartzis115, Laura Beatriz Sarubbo116, Nusa Segrec117, Bigya Shah118, Hongxian Shen119, Tomohiro Shirasaka120, Steve Shoptaw121, Fransiskus Muronga Sintango122, Veronica Andrea Sosa123, Emilis Subata124, Norberto Sztycberg125, Fatemeh Taghizadeh126, Joseph Brian Tay Wee Teck127, Christian Tjagvad128, Marta Torrens129, Judith Meme Twala130, Ramyadarshni Vadivel131, Joseph Robert Volpicelli132, Jelmer Weijs133, Steven Michael Wintoniw134, Apisak Wittayanookulluk135, Marcin Wojnar136, Sadia Yasir91, Yimenu Yitayih137, Min Zhao138 and Arash Khojasteh Zonoozi139
1 Prof. Dr. Matei Bals- Arena OMT Department, National Institute for Infectious Diseases, Bucharest, Romania
2 Faculty of Medicine and Biomedical Sciences, University of Yaoundé 1, Yaoundé, Cameroon
3 Alamal psychiatric hospital, Dubai, United Arab Emirates
4 Sydney Medical School, University of Sydney, Sydney, NSW, Australia
5 Al Ahliyya Amman University, Amman, Jordan
6 Ministry of Health, Muscat, Oman
7 Department of Psychiatry and National Drug Dependence Treatment Center (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi, India
8 Faculty of Medicine, Psychiatry and Behavioral Sciences Research Center, Ibn-e-Sina Hospital, Mashhad University of Medical Sciences, Mashhad, Iran
9 State Drug Dependence Treatment Center, Institute of Mental Health, Pt BDS University of Health Sciences, Rohtak, India
10 Department of Psychiatry, College of Medicine, University of Ibadan, Ibadan, Nigeria
11 Addiction medicine clinic, Amman, Jordan
12 Department of Psychiatry, Drug De-addiction & Treatment Center, Postgraduate Institute of Medical Education & Research, Chandigarh, India
13 Addiction medicine clinic, Mila, Algeria
14 Center medical Marmottan, Paris, France
15 Réseau de Prévention des Addictions (RESPADD), Paris, France
16 Department of Psychiatry and Behavioral Neurosciences, Michael DeGroote School of Medicine, McMaster University, Hamilton, ON, Canada
17 Geneva University Hospitals, Geneva, Switzerland
18 CUNY School of Medicine, New York, NY, United States
19 Aġenzija Sedqa, Santa Venera, Malta
20 United Nations Office on Drugs and Crime (UNODC), Vienna, Austria
21 Department of Medicine and Surgery, University Milan-Bicocca, Milan, Italy
22 University Psychiatric Hospital Vrapce, Zagreb, Croatia
23 Department of Addiction Medicine, Haukeland University Hospital, Bergen, Norway
24 Department of Biochemistry, Melaka Manipal Medical College, Manipal Academy of Higher Education, Manipal, India
25 Addiction medicine clinic, Mexico City, Mexico
26 Addiction Crisis Solutions, Louisville, KY, United States
27 Department of Psychology, Indiana University Purdue University - Indianapolis, Indianapolis, IN, United States
28 SerT Lentini, ASP Siracusa, Syracuse, Italy
29 Serenity Vista Addiction Treatment Center, Jaramillo, Panama
30 Department of Psychiatry, ESIC Medical College, Hyderabad, India
31 National Institute of Mental Health, Klecany, Czechia
32 Collaborative Antwerp Psychiatric Research Institute (CAPRI), Antwerp University (UA), Antwerp, Belgium
33 Drug & Alcohol Clinical Services, Hunter New England Local Health District, New Lambton, NSW, Australia
34 Ain Shams University, Cairo, Egypt
35 Department of Neurology and Psychiatry, Faculty of Medicine, Ain Shams University, Cairo, Egypt
36 Center for Research and Information on Substance Abuse, Jos, Nigeria
37 Addiction Medicine Clinic, Damascus, Syria
38 European Monitoring Center for Drugs and Drug Addiction (EMCDDA), Lisbon, Portugal
39 2nd Department of Psychiatry, Aristotle University of Thessaloniki, Thessaloniki, Greece
40 Brown University and Lifespan Health System, Providence, RI, United States
41 Fuderanan Mental Health Clinic, Manila, Philippines
42 Georgian Harm Reduction Network, Tbilisi, Georgia
43 Organization Against Drugs, Primary Care Health Center, Veria, Greece
44 Addictions Services (Ser.D.), Department of Territorial Assistance, ASL Teramo, Teramo, Italy
45 Swansea University Medical School, Institute of Life Sciences 2, Sketty, United Kingdom
46 Hospital Borda, Universidad de Buenos Aires, Buenos Aires, Argentina
47 University of Sydney, Sydney, NSW, Australia
48 Institutes for Cognitive Science Studies (IRICSS), Brain and Cognition Clinic, Tehran, Iran
49 Tehran University of Medical Sciences, Tehran, Iran
50 Department of Anesthesiology, Yale University, New Haven, CT, United States
51 Drugs Rehabilitation Center, National Narcotics Board of Indonesia, East Jakarta, Indonesia
52 Department of Psychiatry, Universitas Padjadjaran, Bandung, Indonesia
53 Department of Psychiatry, Heritage Institute of Medical Sciences (HIMS), Varanasi, India
54 Univeristi Malaysia Sabah, Sabah, Malaysia
55 Department of Social Work, University of Social Welfare & Rehabilitation Sciences, Tehran, Iran
56 National Center for Mental Health of Korea, Seoul, South Korea
57 Republican Center for Addictive Disorders, Vilnius, Lithuania
58 Addiction medicine clinic, Skopje, North Macedonia
59 Naufar Institute, Doha, Qatar
60 The Kantchelov Clinic, Sofia, Bulgaria
61 Mount Sinai Medical Center, New York, NY, United States
62 African Institute for Development Policy, Lilongwe, Malawi
63 Sobriety Centers of New Hampshire, Antrim, NH, United States
64 Federal University of Rio Grande do Sul, Porto Alegre, Brazil
65 Department of Neuropsychiatry, Pusan National University Yangsan Hospital, YangsanSouth Korea
66 Chatham House, Washington, United States
67 Institute for Public Health of Split-Dalmatia County, Split, Croatia
68 Faculty of Medicine, Universitas Indonesia-Ciptomangunkusumo Hospital, Jakarta, Indonesia
69 Scripps Mercy Hospital, San Diego, CA, United States
70 Department of Psychiatry, The Catholic University of Korea, Seoul, South Korea
71 Faculty of Medicine, Institute of Clinical Medicine, Psychiatric Clinic, Vilnius University, Vilnius, Lithuania
72 Tel Aviv University, Tel Aviv, Israel
73 Israel Center on Addiction, Netanya, Israel
74 Community Health Work, Dar es Salaam, Tanzania
75 Hayat Center for Treatment and Psycho-social Rehabilitation, Khartoum, Sudan
76 University of Botswana, Gaborone, Botswana
77 V.P. Dole, Dual Disorder Unit, Santa Chiara University Hospital, University of Pisa, Pisa, Italy
78 CAS Girona, Department of Psychology, University of Girona, Girona, Spain
79 Community addiction team, Southern Health and Social Care Trust, Craigavon, United Kingdom
80 Priority Medical Clinic, Dublin, Ireland
81 Save the Children International, Yangon, Myanmar
82 Dirección de Investigaciones Epidemiológicas y Sociales, Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz, Mexico City, México
83 Department of Psychiatry, Faculty of Medicine, Sir John Kotelawala Defense University, Colombo, Sri Lanka
84 Center for Addiction Medicine, NIMHANS, Bangalore, India
85 Kleopatra Kodric, Irena Nisic, Ljubljana, Slovenia
86 Alcohol Tobacco and Other Drug Research Unit, South African Medical Research Council, Cape Town, South Africa
87 NIMHANS, Bangalore, India
88 Department of Psychiatry, Center for Addiction Medicine, National Institute of Mental Health and Neurosciences, Bengaluru, India
89 Federal Neuropsychiatric Hospital, Calabar, Nigeria
90 Department of Psychiatry, Psychosomatic Research Center, Tehran University of Medical Sciences, Tehran, Iran
91 Institute of Psychiatry, WHO Collaborating Center for Mental Health, Rawalpindi, Pakistan
92 Brijder Addiction Care, Zaandam, Netherlands
93 Department of Clinical Neurosciences/DIMSC, Unit of Clinical Psychiatry, School of Medicine, Polytechnic University of Marche, Ancona, Italy
94 Koh Kong Provincial Hospital, Phoumin, Cambodia
95 Kaiser Permanente, Oakland, CA, United States
96 Psychiatric hospital Sveti Ivan, Zagreb, Croatia
97 Department of Psychiatry and mental health, Institute of Medicine, Tribhuvan University, Kirtipur, Nepal
98 Universidad de El Salvador, San Salvador, El Salvador
99 AddiPsy, Lyon, France
100 Addiction medicine clinic, San José, Costa Rica
101 Novadic-Kentron Addiction Care Network, Vught, Netherlands
102 Phoenix Foundation for Research and Development, Lahore, Pakistan
103 Barwon Health, Geelong, VIC, Australia
104 Faculty of Medicine Siriraj Hospital, Mahidol University, Salaya, Thailand
105 University of the Sunshine Coast (USC), Queensland, QLD, Australia
106 Center for Interdisciplinary Addiction Research, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
107 Drugs Rehabilitation Center, National Narcotics Board of Indonesia, East Jakarta, Indonesia
108 Department of Cognitive Psychology, Institute for Cognitive Science Studies, Tehran, Iran
109 Usher Institute, University of Edinburgh, Edinburgh, United Kingdom
110 Psychiatry Service, University of Salamanca Health Care Complex, School of Medicine, University of Salamanca, Salamanca, Spain
111 PGIMER, Chandigarh, India
112 Street Health Center, Kingston, ON, Canada
113 Department of Psychiatry, Psychotherapy, and Psychosomatics, Medical University Innsbruck, Innsbruck, Austria
114 Department of Neurosciences and Addiction Studies, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran
115 Medical School, University of Cyprus, Cyprus
116 Clínica Psiquiátrica de la Facultad de Medicina, Uruguay
117 Center for Treatment of Drug addiction, University Psychiatric Clinic, Ljubljana, Slovenia
118 Department of Psychiatry, Patan Academy of Health Sciences, School of Medicine, Lagankhel, Nepal
119 Department of Psychiatry, Second Xiangya Hospital, Central South University, Changsha, China
120 Department of Psychiatry, Teine Keijinkai Medical Center, Sapporo, Hokkaido, Japan
121 Department of Family Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
122 Health Professions Councils of Namibia, Windhoek, Namibia
123 Addiction medicine clinic, Montevideo, Uruguay
124 Republican Center for Addictive Disorders, Vilnius, Lithuania
125 Asociasion Programa Andres Argentina, Santa Fe, Argentina
126 Mazandaran University of Medical Sciences, Mazandaran, Iran
127 MRC/CSO SPHSU, University of Glasgow, Glasgow, United Kingdom
128 Gladsaxe Substance Use Disorder Treatment Center, Gladsaxe, Denmark
129 Institut de Neuropsiquiatria i Addiccions, IMIM-Hospital del Mar, Medical Research Barcelona, Spain
130 NACADA, Nairobi, Kenya
131 Waikato District Health Board (WDHB) Hamilton, Hamilton, New Zealand
132 Institute of Addiction Medicine, Plymouth Meeting, PA, United States
133 Jellinek, Amsterdam, Netherlands
134 Addictions Foundation of Manitoba, Manitoba, Canada
135 Thanyarak Chiangmai hospital, Khilek, Thailand
136 Medical University of Warsaw, Warsaw, Poland
137 Jimma University, Jimma, Ethiopia
138 Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China
139 Student Research Committee, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
2. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. (2020) 323:1775–6. doi: 10.1001/jama.2020.4683
3. Adger WN. Social vulnerability to climate change and extremes in coastal Vietnam. World Dev. (1999) 27:249–69. doi: 10.1016/S0305-750X00136-3
4. Marsden J, Darke S, Hall W, Hickman M, Holmes J, Humphreys K, et al. Mitigating and learning from the impact of COVID-19 infection on addictive disorders. Addiction. (2020) 115:1007–10. doi: 10.1111/add.15080
5. Knopf A. Addiction telemedicine comes into its own with COVID-19. Alcohol Drug Abuse Weekly. (2020) 32:5–6. doi: 10.1002/adaw.32673
6. Volkow ND. Collision of the COVID-19 and addiction epidemics. Am Coll Phys. (2020) 173:61–2. doi: 10.7326/M20-1212
7. Di Nicola M, Pepe M, Modica M, Lanzotti P, Panaccione I, Moccia L, et al. Mixed states in patients with substance and behavioral addictions. Psychiatr Clin. (2020) 43:127–37. doi: 10.1016/j.psc.2019.10.012
8. Janiri D, Di Nicola M, Martinotti G, Janiri L. Who's the leader, mania or depression? Predominant polarity and alcohol/polysubstance use in bipolar disorders. Curr Neuropharmacol. (2017) 15:409–16. doi: 10.2174/1570159X14666160607101400
9. Havakuk O, Rezkalla SH, Kloner RA. The cardiovascular effects of cocaine. J Am Coll Cardiol. (2017) 70:101–13. doi: 10.1016/j.jacc.2017.05.014
10. Riezzo I, Fiore C, De Carlo D, Pascale N, Neri M, Turillazzi E, et al. Side effects of cocaine abuse: multiorgan toxicity and pathological consequences. Curr Med Chem. (2012) 19:5624–46. doi: 10.2174/092986712803988893
11. Arya S, Gupta R. COVID-19 outbreak: challenges for addiction services in India. Asian J Psychiatry. (2020) 51:102086. doi: 10.1016/j.ajp.2020.102086
12. Szabo G, Mandrekar P. A recent perspective on alcohol, immunity, and host defense. Alcohol Clin Exp Res. (2009) 33:220–32. doi: 10.1111/j.1530-0277.2008.00842.x
13. Bhaskaram P. Micronutrient malnutrition, infection, and immunity: an overview. Nutr Rev. (2002) 60(Suppl. 5):S40–5. doi: 10.1301/00296640260130722
14. Spooner C, Hetherington K. Social Determinants of Drug Use. National Drug and Alcohol Research Center, University of New South Wales (2005).
15. Vasylyeva TI, Smyrnov P, Strathdee S, Friedman SR. Challenges posed by COVID-19 to people who inject drugs and lessons from other outbreaks. J Int AIDS Soc. (2020) 23:e25583. doi: 10.1002/jia2.25583
16. Nobles J, Martin F, Dawson S, Moran P, Savovic J. The Potential Impact of COVID-19 on Mental Health Outcomes and the Implications for Service Solutions. Bristol: National Institute for Health Research, University of Bristol (2020).
17. Liu CH, Doan SN. Psychosocial stress contagion in children and families during the COVID-19 pandemic. Clin Pediatr. 2020:0009922820927044. doi: 10.1177/0009922820927044
18. Zarrabian S, Hassani-Abharian P. Covid-19 pandemic and the importance of cognitive rehabilitation. Basic Clin Neurosci. (2020) 11:129–32. doi: 10.32598/bcn.11.covid19.194.5
19. Starcke K, Brand M. Decision making under stress: a selective review. Neurosci Biobehav Rev. (2012) 36:1228–48. doi: 10.1016/j.neubiorev.2012.02.003
20. Cheng SK, Lam DJ. Relationships among life stress, problem solving, self-esteem, and dysphoria in Hong Kong adolescents: test of a model. J Soc Clin Psychol. (1997) 16:343–55. doi: 10.1521/jscp.1997.16.3.343
21. Dutra SJ, Marx BP, McGlinchey R, DeGutis J, Esterman M. Reward ameliorates posttraumatic stress disorder-related impairment in sustained attention. Chronic Stress. (2018) 2:2470547018812400. doi: 10.1177/2470547018812400
22. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. (2020) 63:e32. doi: 10.1192/j.eurpsy.2020.35
23. Ren S-Y, Gao R-D, Chen Y-L. Fear can be more harmful than the severe acute respiratory syndrome coronavirus 2 in controlling the corona virus disease 2019 epidemic. World J Clin Cases. (2020) 8:652. doi: 10.12998/wjcc.v8.i4.652
24. Coetzee BJs, Kagee A. Structural barriers to adhering to health behaviours in the context of the COVID-19 crisis: considerations for low-and middle-income countries. Global Public Health. (2020) 151093–102. doi: 10.1080/17441692.2020.1779331
25. O'Sullivan T, Bourgoin M. Vulnerability in an influenza pandemic: looking beyond medical risk. Behaviour. (2010) 11:16. Available online at: https://homelesshub.ca/resource/vulnerability-influenza-pandemic-looking-beyond-medical-risk
26. COVID-19 Resources Page for People Who Use Drugs and Drug Service Providers. EMCDDA (2020). Available online at: https://www.emcdda.europa.eu/publications/ad-hoc/covid-19-resources_en
27. Bojdani E, Rajagopalan A, Chen A, Gearin P, Olcott W, Shankar V, et al. COVID-19 pandemic: impact on psychiatric care in the united states, a review. Psychiatry Res. (2020) 289:113069. doi: 10.1016/j.psychres.2020.113069
28. Mellis AM PM, Hulsey J. COVID-19-related treatment service disruptions among people with single- and poly-substance use concerns. J Subst Abuse Treat. (2021) 121:108180. doi: 10.1016/j.jsat.2020.108180
29. Smit B, Wandel J. Adaptation, adaptive capacity and vulnerability. Global Environ Change. (2006) 16:282–92. doi: 10.1016/j.gloenvcha.2006.03.008
30. Dolan AH, Walker IJ. Understanding vulnerability of coastal communities to climate change related risks. J Coastal Res. (2006) 1316–23. Available online at: www.jstor.org/stable/25742967 (accessed April 9, 2021).
31. Baldacchino A, Radfar SR, De Jong C, Rafei P, Yunesian M, Gerra G, et al. COVID-19 and substance use disorder: study protocol for the International Society of Addiction Medicine Practice and Policy Interest Group Global survey. Basic Clin Neurosci. (2020) 11:155–62. doi: 10.32598/bcn.11.covid19.2545.1
32. Farhoudian A, Radfar SR, Mohaddes Ardabili H, Rafei P, Ebrahimy M, Khojasteh Zonoozi A, et al. A global survey on changes in the supply, price and use of illicit drugs and alcohol, and related complications during the 2020 COVID-19 pandemic. medRxiv [Preprint]. (2020). doi: 10.1101/2020.07.16.20155341
33. World Economic Situation and Prospects 2019. United Nations (2019). Available online at: https://www.un.org/development/desa/dpad/publication/world-economic-situation-and-prospects-2019/
34. Farhoudian A, Baldacchino A, Clark N, Gerra G, Ekhtiari H, Dom G, et al. COVID-19 and substance use disorders: recommendations to a comprehensive healthcare response. An International Society of Addiction Medicine (ISAM) practice and policy interest group position paper. Auton Neurosci Basic Clin. (2020) 11:129–46. doi: 10.32598/bcn.11.covid19.1
35. Dunlop A, Lokuge B, Masters D, Sequeira M, Saul P, Dunlop G, et al. Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic. Harm Reduct J. (2020) 17:1–7. doi: 10.1186/s12954-020-00370-7
36. Singer M, Bulled N, Ostrach B, Mendenhall E. Syndemics and the biosocial conception of health. Lancet. (2017) 389:941–50. doi: 10.1016/S0140-673630003-X
37. Dorahy MJ, Rowlands A, Renouf C, Hanna D, Britt E, Carter JD. Impact of average household income and damage exposure on post-earthquake distress and functioning: a community study following the February 2011 Christchurch earthquake. Br J Psychol. (2015) 106:526–43. doi: 10.1111/bjop.12097
38. Phibbs S, Kenney C, Rivera-Munoz G, Huggins TJ. The inverse response law: theory and relevance to the aftermath of disasters. Int J Environ Res Public Health. (2018) 15:916. doi: 10.3390/ijerph15050916
39. Runkle JD, Brock-Martin A, Karmaus W, Svendsen ER. Secondary surge capacity: a framework for understanding long-term access to primary care for medically vulnerable populations in disaster recovery. Am J Public Health. (2012) 102:e24–32. doi: 10.2105/AJPH.2012.301027
40. Leone B, Di Nicola M, Moccia L, Pettorruso M, De Risio L, Nucara G, et al. Gender-related psychopathology in opioid use disorder: results from a representative sample of Italian addiction services. Addict Behav. (2017) 71:107–10. doi: 10.1016/j.addbeh.2017.03.010
41. Mongan D, Galvin B, Farragher L, Dunne M, Nelson M. Impact of COVID-19 on drug services in four countries. Dublin: Health Research Board (2020). Available online at: https://www.drugsandalcohol.ie/32296
42. Sokol R, Gupta A, Powers S, Hoffman L, Meza J. Guidance for Treating Patients with Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (B/N) in the COVID-19 Era via Telehealth: a review of previous evidence, new COVID-19 OUD treatment guidelines, and a case report of their application (2020). Available online at: https://deepblue.lib.umich.edu/handle/2027.42/155566
44. Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1659–724. doi: 10.1016/S0140-673631679-8
45. World Health Organization. Atlas on Substance Use 2010: Resources for the Prevention and Treatment of Substance Use Disorders. World Health Organization (2010).
46. Degenhardt L, Glantz M, Evans-Lacko S, Sadikova E, Sampson N, Thornicroft G, et al. Estimating treatment coverage for people with substance use disorders: an analysis of data from the World Mental Health Surveys. World Psychiatry. (2017) 16:299–307. doi: 10.1002/wps.20457
47. Nazari SSH, Noroozi M, Soori H, Noroozi A, Mehrabi Y, Hajebi A, et al. The effect of on-site and outreach-based needle and syringe programs in people who inject drugs in Kermanshah, Iran. Int J Drug Policy. (2016) 27:127–31. doi: 10.1016/j.drugpo.2015.10.011
Keywords: COVID-19 pandemic, substance use disorder, public health, drug policy, opioid agonist treatment, addiction services, harm reduction
Citation: Radfar SR, De Jong CAJ, Farhoudian A, Ebrahimi M, Rafei P, Vahidi M, Yunesian M, Kouimtsidis C, Arunogiri S, Massah O, Deylamizadeh A, Brady KT, Busse A, ISAM-PPIG Global Survey Consortium, Potenza MN, Ekhtiari H and Baldacchino AM (2021) Reorganization of Substance Use Treatment and Harm Reduction Services During the COVID-19 Pandemic: A Global Survey. Front. Psychiatry 12:639393. doi: 10.3389/fpsyt.2021.639393
Received: 08 December 2020; Accepted: 27 February 2021;
Published: 29 April 2021.
Edited by:
David Richard Walwyn, University of Pretoria, South AfricaReviewed by:
Marco Di Nicola, Catholic University of the Sacred Heart, ItalyCopyright © 2021 Radfar, De Jong, Farhoudian, Ebrahimi, Rafei, Vahidi, Yunesian, Kouimtsidis, Arunogiri, Massah, Deylamizadeh, Brady, Busse, ISAM-PPIG Global Survey Consortium, Potenza, Ekhtiari and Baldacchino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ali Farhoudian, ZmFyaG91ZGlhbkB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.