
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 16 March 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.633230
 Leila Cheikh Ismail1,2,3
Leila Cheikh Ismail1,2,3 Maysm N. Mohamad4
Maysm N. Mohamad4 Mo'ath F. Bataineh5
Mo'ath F. Bataineh5 Abir Ajab1,3
Abir Ajab1,3 Amina M. Al-Marzouqi3,6
Amina M. Al-Marzouqi3,6 Amjad H. Jarrar4Dima O. Abu Jamous3Habiba I. Ali4
Amjad H. Jarrar4Dima O. Abu Jamous3Habiba I. Ali4 Haleama Al Sabbah7
Haleama Al Sabbah7 Hayder Hasan1,3Lily Stojanovska4,8Mona Hashim1,3
Hayder Hasan1,3Lily Stojanovska4,8Mona Hashim1,3 Reyad R. Shaker Obaid1,3
Reyad R. Shaker Obaid1,3 Sheima T. Saleh1,3Tareq M. Osaili1,3,9
Sheima T. Saleh1,3Tareq M. Osaili1,3,9 Ayesha S. Al Dhaheri4*
Ayesha S. Al Dhaheri4*United Arab Emirates (UAE) has taken unprecedented precautionary measures including complete lockdowns against COVID-19 to control its spread and ensure the well-being of individuals. This study investigated the impact of COVID-19 and societal lockdown measures on the mental health of adults in the UAE. A cross-sectional study was conducted using an English and Arabic online questionnaire between May and June 2020. The psychological impact was assessed by the Impact of Event Scale-Revised (IES-R), and the social and family support impact was evaluated using questions from the Perceived Support Scale (PSS). A total of 4,426 participants (3,325 females and 1,101 males) completed the questionnaire. The mean IES-R score was 28.0 ± 14.6, reflecting a mild stressful impact with 27.3% reporting severe psychological impact. Over 36% reported increased stress from work, home and financial matters. Also, 43–63% of the participants felt horrified, apprehensive or helpless due to COVID-19. Females, younger participants, part-timers, and college or University graduates were more likely to have a high IES-R score (p < 0.05). The majority of participants reported receiving increased support from family members, paying more attention to their mental health, and spending more time to rest and relax. The results of this study demonstrate the impact of the COVID-19 pandemic on mental health among the UAE residents and highlight the need to adopt culturally appropriate interventions for the general population and vulnerable groups, such as females and younger adults.
The novel coronavirus (COVID-19) pandemic has brought about extraordinary challenges in various aspects of life. It is highly expected that outbreaks lead to increase in unemployment and impaired financial status as well as compromised physical and mental health (1, 2). The novel coronavirus emerged initially in Wuhan, China in late December 2019 and surged exponentially across the world leading to the declaration of a global pandemic by the World Health Organization (WHO) on March 11, 2020 (3, 4). More than 105.4 million confirmed cases and over 2.3 million deaths were recorded globally as of 7 February 2021 (5). In the United Arab Emirates (UAE), the first cases of positive coronavirus were diagnosed on January 23, 2020; a Chinese family of four visiting the UAE on holiday (6). To date, there have been over 323 thousand confirmed cases and a total of 914 deaths in the UAE (5).
The alarming spread of the disease and its inevitable health and socioeconomic impact has led to the implementation of serious measures across the world. This was manifested by borders closure, suspension of flights, complete and partial lockdowns, quarantine, physical distancing, and mandating public respiratory hygiene measures (7). During the UAE countrywide lockdown, imposed between mid-March and July 31, 2020, people were instructed to stay at home other than for important individual movement (8). Moreover, the government closed non-essential business (e.g., cafes, gyms, theme parks, salons, and spas), initiated telework and distance learning, improved delivery services like delivering drugs to chronically ill patients and sanitized cities during the night as part of the national disinfection program (9). By the end of the lockdown on early July 2020, reopening of businesses and economic activities was initiated, but with strict preventative and restriction measures including overnight curfews, movement restrictions at the local level, physical distancing and wearing of face covering in public spaces (10).
Quarantine has been historically implemented to control the spread of infectious diseases outbreaks; however, it represents an unfavorable experience for the general population (11). Literature shows that multiple stressors including movement restriction, separation from family and friends, uncertain future, fear of infection, distress, loneliness, boredom, and financial loss are all factors that may exacerbate negative psychological impact and play a role in aggravating poor mental health (12, 13). Several studies have explored mental health problems (emotional disturbance, depression, fear of infection, stress, post-traumatic stress symptoms, and irritability) during other infectious and widespread outbreaks like the Severe Acute Respiratory Syndrome (SARS) epidemic in 2003 and the Middle East respiratory syndrome coronavirus (MERS-CoV) in 2012 (14, 15). However, MERS-CoV was not considered a pandemic because of the low rates of reported cases. Unlike SARS and MERS-CoV the psychological impact of the current pandemic might be more profound due to extensive social media exposure, increased global connectivity, high transmission rates and long duration of quarantine (16, 17).
There is limited research examining mental health in the UAE. However, available studies indicated high prevalence of depression and anxiety among primary health care attenders (18, 19) and social stigma was the main challenge associated with seeking and utilizing psychological services in the UAE (20). Considering the prevalence of mental health disorders in the UAE and in light of the current pandemic, the Ministry of Health and Prevention in the UAE launched a Hayat (life) program from mental health support during the COVID-19 pandemic and a dedicated telephone counseling hotline to help those with psychological concerns or anxiety (10). However, the impact of COVID-19 on mental health status of UAE population has not been investigated to-date.
The lockdown and quarantine during COVID-19 have resulted major social and psycho-logical impact on the whole population (21). The pandemic has caused changes on societal level as some families experienced conflicts, and instability due to the restriction measures implemented during the outbreak (22). However, many have considered this as an opportunity to establish better support and bonds between family members (23). In countries like the UAE, extended family is considered a pillar of the society and to no doubt have the ability to lessen the negative impacts of such health crisis. Nonetheless, limited research is available on how people are affected by the pandemic and the impact it has on their mental health and living conditions in the UAE. This study aimed to investigate the impact of the COVID-19 outbreak and lockdown measures on mental health and well-being among residents of the UAE. The pandemic is not over yet and restriction measures, teleworking, and home-schooling of children still apply in the UAE. Therefore, it was hypothesized that specific factors related to the implementation of restrictive measures may be associated with the inevitable increase in psychological distress among the general population.
A cross-sectional web-based research study was conducted from May 11, 2020 to June 15, 2020 in the UAE. A total of 4,426 participants were recruited from all the seven emirates in the UAE (Abu Dhabi, Dubai, Sharjah, Ajman, Um Al Quwain, Ras Al-Khaimah, and Fujairah). The study inclusion criteria were, living in the UAE and age ≥18 years. Participants were invited electronically to participate in the study using convenience and snowball sampling methods. These methods guarantee large-scale dissemination and recruitment of participants.
The Impact of Event Scale-Revised (IES-R) was used to assess the psychological impact of the pandemic and the Perceived Support Scale (PSS) was employed to assess the impact on social and family support (24–26). The questionnaire was prepared on Google document forms in English and Arabic, then pilot tested for clarity in a sample of 26 people prior to large-scale launching. Minimal adjustments to the wording were made to guarantee understandability. A uniform resource locator (URL) was retrieved for the survey and was distributed formally (using e-mail invitations) and informally (using social media platforms, e.g., LinkedIn™, Facebook™, and WhatsApp™). The questionnaire included an information sheet on the first page, and the participants were asked to consent before completing the questionnaire. They were free to exit the survey at any point without giving explanations, and no personal identification was requested to retain information confidentiality. Participants were given no incentives for participation in the study. The system of Google Forms only provides responses for questionnaires with 100% completion rate. The responses were downloaded as an Excel file and securely stored using a password protected “Cloud” database.
The present study followed the ethical code for web-based research (27, 28) and conforms to the principles embodied in the Declaration of Helsinki (29). The study protocol was approved by the Social Sciences Research Ethics Committee at United Arab Emirates University (ERS_2020_6115). An electronic informed consent was obtained from all participants.
Socio-demographic characteristics were collected including age, gender, education level, employment status, marital status, and work or study setting.
The scale was used to assess the psychological impact of COVID-19 among adults in the UAE (24). The IES-R is a self-administered questionnaire that includes 22 items and has been previously translated and validated in the English and Arabic languages (30–33). It has been also validated to investigate trauma-related stress symptoms related to the short- and long-term impact of the COVID-19 outbreak (34). Moreover, the IES-R has also been used to measure symptomatology experienced during the COVID-19 pandemic in Saudi Arabia, Egypt, Italy, and China (26, 35–38).
Participants were asked to rate the items based on how distressing the COVID-19 pandemic was for them. Items are rated on a 5-point Likert scale, ranging from 0 (not at all) to 4 (extremely); the response for each question was scored and generated a total score (ranging from 0 to 88). The total IES-R score was considered normal (from 0 to 23); indicative of mild (from 24 to 32); moderate (from 33 to 36); or severe (≥37) psychological impact (35). Three subscale scores were also calculated measuring intrusion (eight items), avoidance (eight items), and hyperarousal (six items) (25).
This section contained six modified and validated questions regarding negative mental health impacts caused by the COVID-19 pandemic (25). Three questions asked if the participants felt horrified, apprehensive, or helpless due to the pandemic. The remaining three questions asked if the participants are experiencing increased stress from work, financial status, and staying at home during the pandemic. The response options were much increased, increased, same as before, decreased, and much decreased.
This section included modified and validated questions from the Perceived Support Scale (PSS) assessing the impact of the COVID-19 pandemic on the support received from family or friends (25, 35). Participants were asked about; support from friends, support from family members, sharing feelings with a family member, sharing feelings with others when in blue, and caring for family members' feelings. The response options were much increased, increased, same as before, decreased, and much decreased.
Participants were asked to rate the frequency of mental health related lifestyle changes that might have affected them during COVID-19 pandemic using modified and validated questions from the Mental Health Lifestyle Scale (MHLSS) (25). This section comprised of four items; attention to mental health, spending enough time to rest, relax, and exercise. The response options were much increased, increased, same as before, decreased, and much decreased.
Normality of data was tested using Kolmogorov-Smirnov test. Categorical variables were presented as frequencies and percentages and continuous variables were presented as mean ± standard deviation (SD). A Chi-square (χ2) test was used to determine the association between IES-R categories with categorical variables. Independent t-test was used to determine differences in IES-R, intrusion, avoidance, and hyperarousal scores between males and females. When significance was detected the effect size (Cohen's effect size, d) was calculated and reported as described previously (39). Moreover, generalized liner model was carried out to determine the confounding effects of sociodemographic factors, negative mental health impact factors, social and family support indicators, and lifestyle factors on continuous IES-R total score. Univariant general linear model with a cut-off value of p < 0.02 was used to select factors to be included in the final regression model. A p-value < 0.05 was considered to be statistically significant. All data were analyzed using Statistical Package for the Social Sciences (SPSS) version 26.0 (IBM, Chicago, IL, USA). The minimum sample size (n = 1,579) was calculated using G*power software, version 3.1.9.4 (HHU, Germany) to detect small effect size (0.02), with a power of 0.95, and alpha 0.05.
The percentage of participants that completed the survey in the Arabic and English languages was 85.0 and 15.0%, respectively. The sociodemographic characteristics of the study population are presented in Table 1. The female to male ratio was almost 3:1, with 24.9% males. The majority of surveyed individuals were aged 36–45 years (33.9%), were married (67.7%), had completed college or University degree of education (64.5%), full-time employed (63.2%), and were working or studying from home (56.2%).
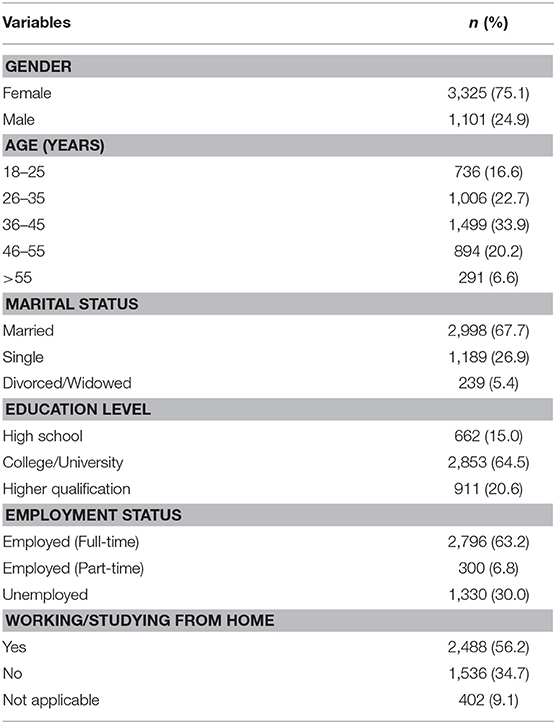
Table 1. Sociodemographic characteristics of participants (n = 4,426) using Chi-square test.
The overall mean IES-R score was 28.0 ± 14.6 (range 0–84), reflecting a mild stressful impact of the COVID-19 pandemic on the surveyed participants (Table 2). For 41.7% of the participants, the IES-R score was in the normal range (0–23). Over 27% of the participants had a score reflecting severe psychological impact (≥37), with a higher mean IES-R score among females (28.6 ± 14.9) compared to males (25.9 ± 13.7) (p < 0.001; with a small Cohen's effect size).
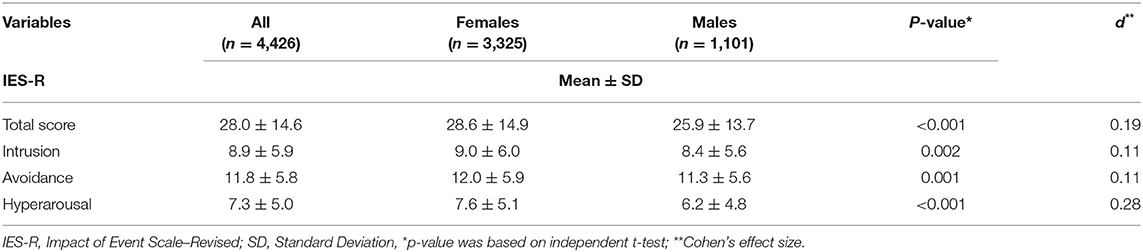
Table 2. Psychological impact of COVID-19 on participants by gender (n = 4,426).
The overall means for intrusion, avoidance and hyperarousal scales in participants were 8.9 ± 5.9, 11.8 ± 5.8, and 7.3 ± 5.0, respectively. The mean scores for all subscales in females were significantly higher compared with males (p < 0.001; with a small Cohen's effect size).
Table 3 presented the association of IES-R scores with sociodemographic factors. A Chi-square analysis revealed significant association between IES-R categories with gender (p < 0.001), age (p < 0.001), education level (p = 0.002), and employment status (p = 0.02). Multivariate regression analysis revealed that females (p < 0.001), younger participants (age groups 18–25, 26–35, and 36–45; p < 0.001), college/University graduate (p = 0.004), and part-timers (p = 0.033) were more likely to have higher IES-R scores.
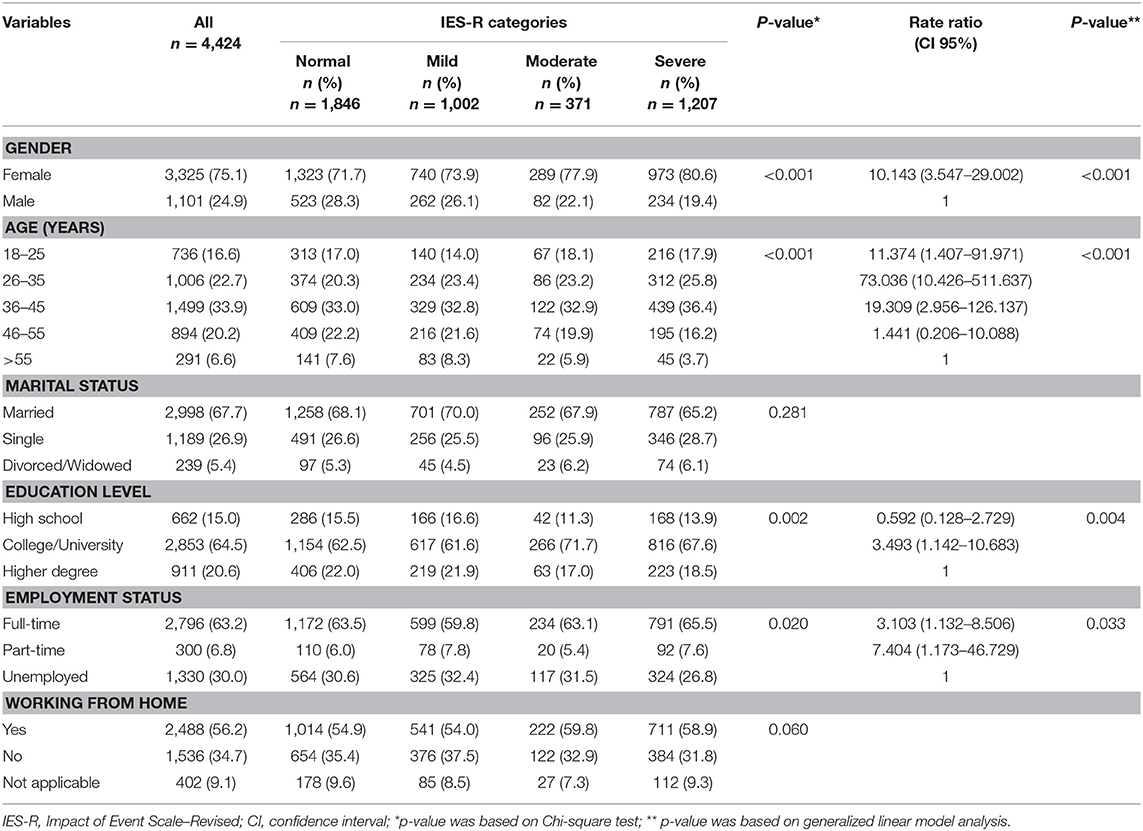
Table 3. Association of IES-R scores with sociodemographic factors (n = 4,426).
Association of IES-R categories with negative mental health indicators are displayed in Table 4. Over 43% of the participants reported increased stress from work during the outbreak, 36.5% felt an increased level of stress from financial matters, and 55.7% of the participants reported increased stress at home during the pandemic. Moreover, around 43–63% of participants felt horrified, apprehensive or helpless due to the pandemic. Chi-square analysis and multivariate regression analysis both revealed that increased stress and negative feelings were strongly associated with higher IES-R scores (p <0.001).
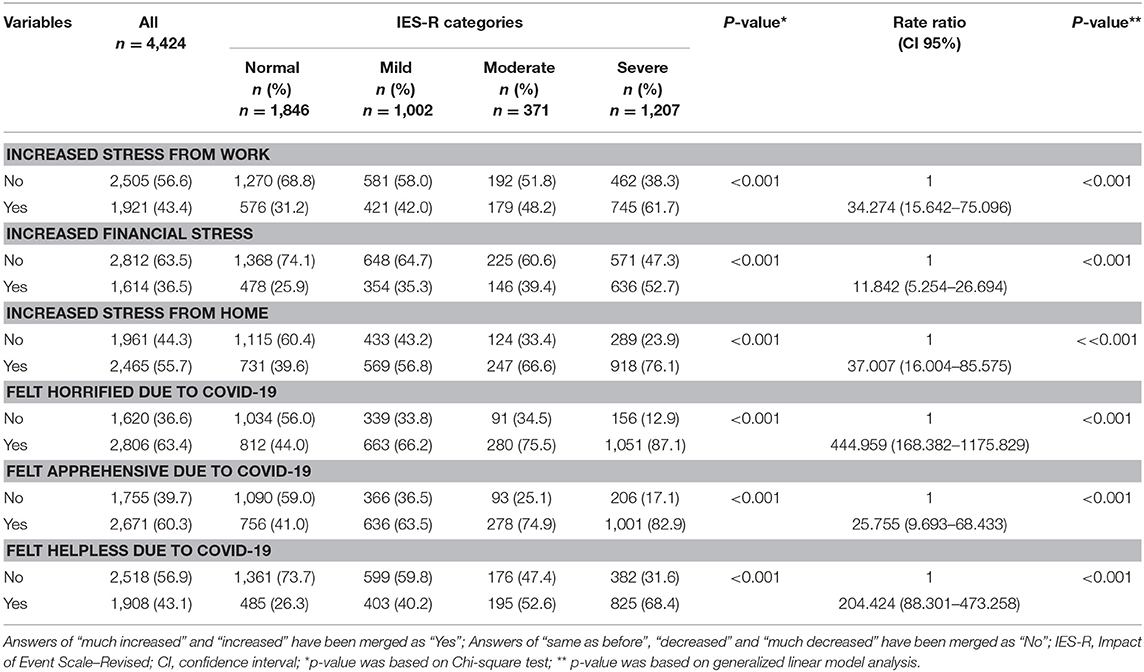
Table 4. Association of IES-R scores with negative mental health indicators (n = 4,426).
As expected, Table 5 showed that 45.1% of the participants reported receiving increased support from family members, 52.8% reported increased shared feelings with their family members and 71.8% cared more about their family members' feelings during the pandemic. In contrast, only 27% had increased support from friends. However, participants with increased support from family and friends, who shared feelings with family members, and caring about family members were more likely to report higher IES-R scores (P <0.001).
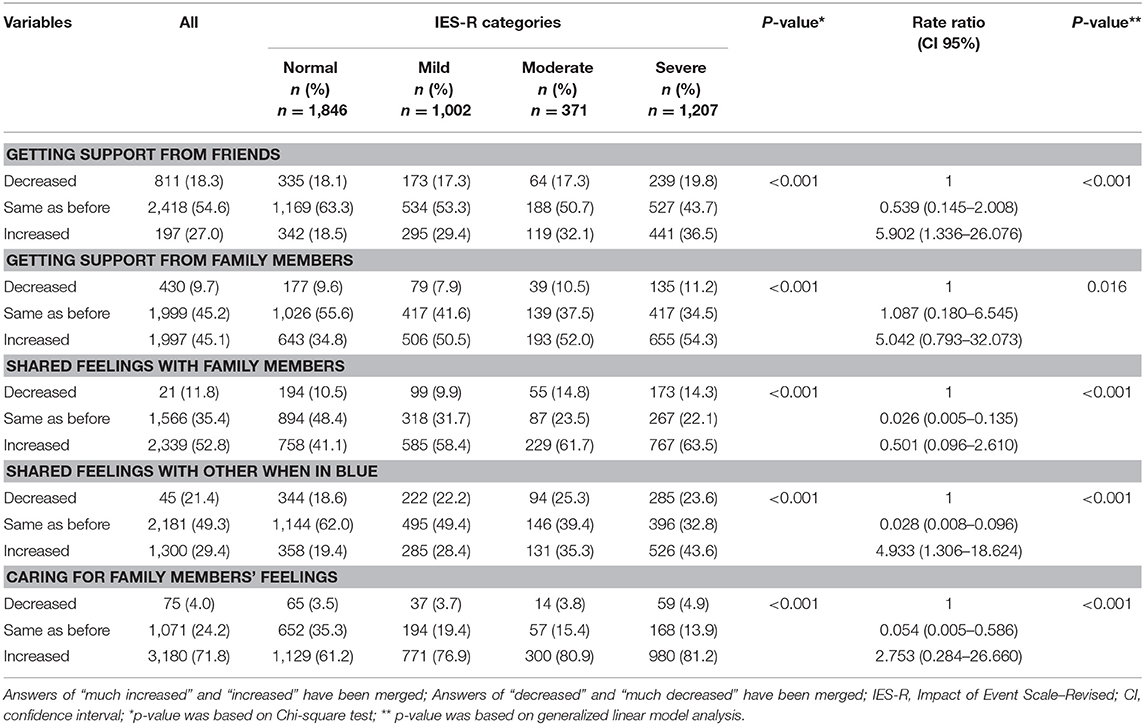
Table 5. Association of IES-R scores with impact on family and social support (n = 4,424).
Table 6 showed the association of IES-R scores with lifestyle indicators during the pandamic. A significat percentage of participants reported increased attention to their mental health (45.5%) and spending more time to rest and relax (41.2 and 38.7%, respectively). In contrast, 41.0% of the participants reported spending less time exercising. The multivariate regression analysis showed that participants who had increased attention to mental health (p <0.001) and decreased time spent on resting (p = 0.002), relaxing (p <0.001), and exersicing (p < 0.001), were more likely to report higher IES-R scores compared with particpants reporting no change.
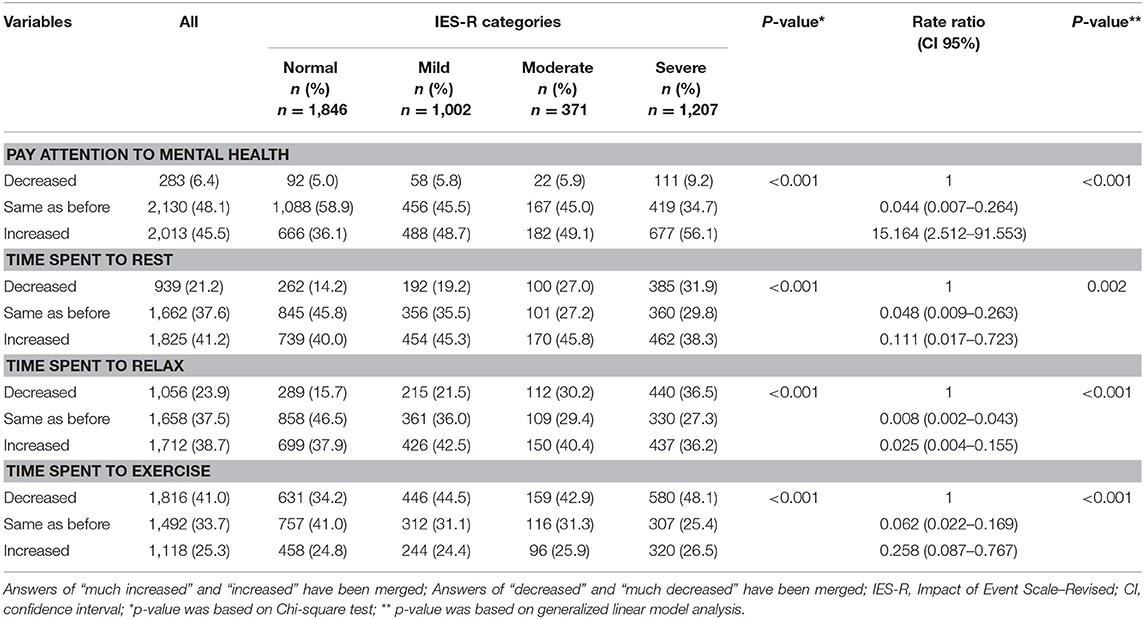
Table 6. Association of IES-R scores with lifestyle changes (n = 4,424).
The results of this study showed that over one third of the participants in the UAE had an IES-R score indicating moderate to severe disturbance due to the COVID-19 pandemic. Similarly, in neighboring gulf countries, an online survey conducted among Saudi adults during the pandemic reported mild to moderate rates of anxiety among the general population and a significantly higher level of anxiety was observed among married respondents (40). In Bahrain, an online Depression Anxiety and Stress Scale-21 (DASS-21) showed that one third of the participants had depressive and stress symptoms (41). Likewise, Lebanese citizens have also reported an increase of Post-traumatic Stress Disorder (PTSD) symptomatology during the fourth week of the COVID-19 quarantine (42). However, levels in the current study were lower than those reported in China, which revealed that over half (53.8%) of the general population had a moderate-to-severe psychological impact during the outbreak (13). Similar to China, results from Egypt indicated high IES-S mean score (34.3 ± 15.0), and more than half of the participants (52%) showed moderate and severe psychological impact due to the pandemic (38). Different populations in the world have been experiencing different pandemic fear depending on the speed of spreading, regulations adopted by the governments or previous experiences of outbreaks like those caused by SARS, Ebola, and MERS-CoV, such factors could contribute to heightening the impact of the present pandemic (43). The majority of the participants in the current study reported feeling horrified, apprehensive or helpless due to the pandemic. Existing evidence suggests a link between hopelessness and depression and highlights the unique sensory processing patterns of depressed individuals in determining unfavorable outcomes (44).
In the current study, females, younger participants, part-timers and University or college educated participants were more likely to have higher stress scores. The process underlying gender differences in the susceptibility to psychological disorders have not yet been fully understood. However, some evidence suggests that fluctuations in ovarian hormone levels and greater brainstem activation among women may contribute to greater PTSD prevalence and higher emotional stimuli (45–47). Moreover, the literature suggested that greater access to information through social media could be triggering stress and anxiety amongst the younger population (48, 49). Conflicting results about the potential relationship between education level and PTSD were reported in the literature. Some evidence suggests that individuals with a higher level of education might use better coping strategies and ultimately be less impacted by the environmental disaster (50, 51). Others suggested that highly educated people might be more stressed due to higher self-awareness and discernment of the pandemic severity (48, 52).
Findings of the current study were in agreement with results from Saudi Arabia, as health care workers, students and females had higher levels of stress, anxiety and depression symptoms (37). Likewise, females, younger persons, students, those with chronic illnesses and people with low income reported higher psychological impacts due to COVID-19 in Egypt and Bahrain (38, 41). Findings from Tunisia identified females, people who reported exposure to confirmed COVID-19 case, those who felt deprived of essential resources, and those exposed to 2 or more hours per day of media coverage of COVID-19 as vulnerable groups (53). These subgroups are considered at higher risk for adverse psychological effects during such crisis. Therefore, clinical interventions targeted toward vulnerable groups are needed to mitigate the influence of the ongoing pandemic and alleviate triggers of distress, such as low social, financial, and emotional support, feelings of fear, isolation and uncertainty, and threats to health and well-being (54). Telehealth counseling helplines have been shown useful to provide support to the vulnerable groups and appropriate for the delivery of mental health services (55). Likewise, awareness about self-relaxation and self-care measures can lessen feelings of social isolation (56).
The study showed that over one-third of participants experienced increased stress from work, home and financial matters during the COVID-19 pandemic. The results were comparable to reports among Egyptian adults (38). Contributing factors may include effects of COVID-19 and the associated lockdowns on daily life and routine, work-family balance, and lack of financial support for those who need it (57). Moreover, COVID-19 associated lockdowns required many working parents to do a full-time job from home and care for the family simultaneously. Findings also suggested that females were more likely to have experienced an increased level of stress from work while males experienced an increased level of stress from financial matters. Considering the long-standing role expectations of females as caregivers and males as breadwinners, it is usually working mothers, who need to adjust their work patterns to meet the needs of the family and the household (58). A study among Australian working parents revealed that active care and household management rose by an hour and a half for fathers and by 2 h and a half for mothers (57). Demonstrating that both genders were dissatisfied with their work-family balance and facing increased stress from home matters during the COVID-19 pandemic, which was also shown in the current study. Besides, families were affected by prolonged school closure, requiring online education support and uncertainty about examinations and enrolment arrangements (59). Governments and workplace policies could support work-family balance by allowing the right to request part-time work, flexible working hours, and the option to work from home (60).
The majority of participants reported getting increased support from other family members as well as caring more about the feelings of family as a whole during the pandemic. Apparently, such acts have had a positive impact on mental health and may have helped the participants to cope with other negative feelings during the pandemic. Similarly, a study from Egypt confirmed that family and friends were much valued in a time of crisis (38). On the other hand, domestic violence reports have increased during the pandemic in many parts of the world. The World Health Organization Europe member states have reported a 60% increase in emergency calls from women subjected to violence by their intimate partner during the pandemic (61). Reasons could include job losses, rising alcohol-based harm and drug use, stress and fear (61).
Current results revealed strong association between decreased time spent on physical activity and likelihood of scoring higher on IES-R scale, suggesting that lower levels of physical activity during the pandemic are more likely to increase impact of the event in a negative manner. These results are in agreement with the results reported by a study among Arab adults that investigated the influence of home confinement during the pandemic and reported significant relationship between higher levels of physical activity and better mental well-being (62). The authors of the latter study suggested that higher levels of physical activity are associated with positive hormonal status, therefore, favoring improved mood and mental health (62). Moreover, physical activity has been recommended as a form of therapy to counteract the expected negative impact of quarantine on mental and physical factors (63). The authors of the current study suggest that home-based physical activities could be employed to overcome the closure of training facilities and public parks during lockdown to improve mental status.
This study has several strengths, including the large sample size and the use of validated questionnaires that provide the ability to compare the findings with previous studies. Moreover, due to the strict quarantine measures in place, using an online survey allowed data collection from various cities and guaranteed the anonymity of the participants. However, there were some limitations; the use of a self-reported questionnaire which might cause some respondent bias or misreporting of data. Also, the snowballing sampling strategy which may limit the representativeness of the UAE population. Furthermore, the use of an online survey limited the reach to non-social media users which led to less generalizable results. The cross-sectional study design may limit the causal interpretation, and a longitudinal study on the psychological impact in the UAE is recommended.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study protocol was reviewed and approved by the Social Sciences Research Ethics Committee at United Arab Emirates University (ERS_2020_6115). An electronic informed consent was obtained from all participants.
ASA, MB, and LC: conceptualization. ASA, MB, MM, AA, LS, MH, SS, and LC: methodology. ASA, MM, SS, and LC: formal analysis and writing—original draft preparation. ASA, MB, MM, AA, AAM, AJ, DA, HIA, HA, HH, LS, MH, RS, SS, TO, and LC: investigation and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185. doi: 10.1016/j.ijsu.2020.04.018
2. Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned? Int J Epidemiol. (2020) 49:717–26. doi: 10.1093/ije/dyaa033
3. WHO. Pneumonia of Unknown Cause – China. World Health Organization (2020). Available online at: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/
4. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed Atenei Parmensis. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
5. WHO. Weekly Epidemiological Update – 9 February 2021. World Health Organization (2020). Available online at: https://www.who.int/publications/m/item/weekly-epidemiological-update—9-february-2021
6. The-National-News. Coronavirus: UAE Records First Case 2020. (2020). Available online at: https://www.thenationalnews.com/uae/health/coronavirus-uae-records-first-case-1.971253
7. Bedford J, Enria D, Giesecke J, Heymann DL, Ihekweazu C, Kobinger G, et al. COVID-19: towards controlling of a pandemic. Lancet. (2020) 395:1015–8. doi: 10.1016/S0140-6736(20)30673-5
8. Koh D. COVID-19 lockdowns throughout the world. Occupat Med. (2020) 70:322. doi: 10.1093/occmed/kqaa073
9. Bloukh SH, Shaikh A, Pathan HM, Edis Z. Prevalence of COVID-19: A Look Behind the Scenes From the UAE and India (2020). doi: 10.20944/preprints202004.0179.v2
10. UAE.Government. Handling the COVID-19 Outbreak in the UAE. The United Arab Emirates' Government Portal (2020). Available online at: https://u.ae/en/information-and-services/justice-safety-and-the-law/handling-the-covid-19-outbreak
11. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
12. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int J Med. (2020) 113:531–7. doi: 10.1093/qjmed/hcaa201
13. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
14. Lee AM, Wong JG, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. (2007) 52:233–40. doi: 10.1177/070674370705200405
15. Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin Med Res. (2016) 14:7–14. doi: 10.3121/cmr.2016.1303
16. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE. (2020) 15:e0231924. doi: 10.1371/journal.pone.0231924
17. Depoux A, Martin S, Karafillakis E, Preet R, Wilder-Smith A, Larson H. The pandemic of social media panic travels faster than the COVID-19 outbreak. J Travel Med. (2020) 27:taaa031. doi: 10.1093/jtm/taaa031
18. Daradkeh TK, Eapen V, Ghubash R. Mental morbidity in primary care in Al Ain (UAE): Application of the Arabic translation of the PRIME-MD (PHQ) version. German J Psychiatry. (2005) 8:32–5.
19. Eapen V, El-Rufaie O. United Arab Emirates (UAE). Int Psychiatry. (2008) 5:38–40. doi: 10.1192/S1749367600005580
20. Al-Darmaki F. The status of counseling in the United Arab Emirates. In: Mental Health and Psychological Practice in the United Arab Emirates. New York, NY: Palgrave Macmillan (2015). 105–16. doi: 10.1057/9781137558237_10
21. Sameer A, Khan MA, Nissar S, Banday MZ. Assessment of mental health and various coping strategies among general population living under imposed COVID-lockdown across world: a cross-sectional study. Ethics Med Public Health. (2020) 15:100571. doi: 10.1016/j.jemep.2020.100571
22. Sharma A, Borah SB. Covid-19 and domestic violence: an indirect path to social and economic crisis. J Fam Violence. (2020) 1–7. doi: 10.1007/s10896-020-00188-8
23. Ahmen D, Buheji M, Fardan SM. Re-emphasising the future family role in “care economy” as a result of covid-19 pandemic spillovers. Am J Econ. (2020) 10:332–8. doi: 10.5923/j.economics.20201006.03
24. Weiss DS. The impact of event scale: revised. In: Cross-Cultural Assessment of Psychological Trauma and PTSD. International and Cultural Psychology Series. Boston, MA: Springer (2007). 219–38. doi: 10.1007/978-0-387-70990-1_10
25. Lau JT, Yang X, Tsui H, Pang E, Wing YK. Positive mental health-related impacts of the SARS epidemic on the general public in Hong Kong and their associations with other negative impacts. J Infect. (2006) 53:114–24. doi: 10.1016/j.jinf.2005.10.019
26. Ma ZF, Zhang Y, Luo X, Li X, Li Y, Liu S, et al. Increased stressful impact among general population in mainland China amid the COVID-19 pandemic: a nationwide cross-sectional study conducted after Wuhan city's travel ban was lifted. Int J Soc Psychiatry. (2020) 66:770–9. doi: 10.1177/0020764020935489
27. Franzke A, Bechmann A, Zimmer M, Ess C. Internet Research: Ethical Guidelines 3.0. San Francisco, CA: Association of Internet Researchers (2019).
28. Holmes S. Methodological and ethical considerations in designing an Internet study of quality of life: a discussion paper. Int J Nurs Stud. (2009) 46:394–405. doi: 10.1016/j.ijnurstu.2008.08.004
29. WMA. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
30. Agostini T, Grassi M, Pellizzoni S, Murgia M editors. The arabic impact of event scale-revised: psychometric properties in a sample of Syrian refugees. In: 13th Alps Adria Psychology Conference, Ljubljana: Horizons of Psychology (2018) 27:86.
31. Brunet A, St-Hilaire A, Jehel L, King S. Validation of a French version of the impact of event scale-revised. Can J Psychiatry. (2003) 48:56–61. doi: 10.1177/070674370304800111
32. Christianson S, Marren J. The impact of event scale-revised (IES-R). Medsurg Nurs. (2012) 21:321–2.
33. Beck JG, Grant DM, Read JP, Clapp JD, Coffey SF, Miller LM, et al. The impact of event scale-revised: psychometric properties in a sample of motor vehicle accident survivors. J Anxiety Disord. (2008) 22:187–98. doi: 10.1016/j.janxdis.2007.02.007
34. Association AD. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes–2020. Diabetes Care. (2020) 43:S14–31. doi: 10.2337/dc20-S002
35. Davico C, Ghiggia A, Marcotulli D, Ricci F, Amianto F, Vitiello B. Psychological Impact of the COVID-19 Pandemic on Adults and Their Children in Italy. The Lancet. (2020). doi: 10.2139/ssrn.3576933
36. Zhang Y, Ma ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: a cross-sectional study. Int J Environ Res Public health. (2020) 17:2381. doi: 10.3390/ijerph17072381
37. Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. (2020) 102:152192. doi: 10.1016/j.comppsych.2020.152192
38. El-Zoghby SM, Soltan EM, Salama HM. Impact of the COVID-19 pandemic on mental health and social support among adult Egyptians. J Commun Health. (2020) 45:689–95. doi: 10.1007/s10900-020-00853-5
39. Cohen J. Some statistical issues in psychological research. In: Wolman BB, editors. Handbook of Clinical Psychology. New York, NY: McGraw-Hill (1965). p. 95–121.
40. Alkwiese M, Alsaqri SH, Aldalaykeh M, Hamzi M, Mahdi M, Shafie Z. Anxiety among the general population during coronavirus-19 disease in Saudi Arabia: implications for a mental support program. medRxiv. (2020) 2020.05.07.20090225. doi: 10.1101/2020.05.07.20090225
41. Alsalman A, Mubarak H, Aljabal M, Abdulnabi M, Ishaq A, Yusuf A, et al. The Psychological Impact of COVID-19 Pandemic on the Population of Bahrain. SSRN. (2020). doi: 10.2139/ssrn.3660648
42. Fawaz M, Samaha A. COVID-19 quarantine: Post-traumatic stress symptomatology among Lebanese citizens. Int J Soc Psychiatry. (2020) 66:666–74. doi: 10.1177/0020764020932207
43. Tee ML, Tee CA, Anlacan JP, Aligam KJG, Reyes PWC, Kuruchittham V, et al. Psychological impact of COVID-19 pandemic in the Philippines. J Affect Disord. (2020) 277:379–91. doi: 10.1016/j.jad.2020.08.043
44. Serafini G, Gonda X, Canepa G, Pompili M, Rihmer Z, Amore M, et al. Extreme sensory processing patterns show a complex association with depression, and impulsivity, alexithymia, and hopelessness. J Affect Disord. (2017) 210:249–57. doi: 10.1016/j.jad.2016.12.019
45. Soni M, Curran VH, Kamboj SK. Identification of a narrow post-ovulatory window of vulnerability to distressing involuntary memories in healthy women. Neurobiol Learn Mem. (2013) 104:32–8. doi: 10.1016/j.nlm.2013.04.003
46. Felmingham K, Williams LM, Kemp AH, Liddell B, Falconer E, Peduto A, et al. Neural responses to masked fear faces: sex differences and trauma exposure in posttraumatic stress disorder. J Abnorm Psychol. (2010) 119:241–7. doi: 10.1037/a0017551
47. Maeng LY, Milad MR. Sex differences in anxiety disorders: Interactions between fear, stress, and gonadal hormones. Horm Behav. (2015) 76:106–17. doi: 10.1016/j.yhbeh.2015.04.002
48. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatry. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
49. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatry. (2020) 52:102066. doi: 10.1016/j.ajp.2020.102066
50. Tang B, Deng Q, Glik D, Dong J, Zhang L. A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. Int J Environ Res Public Health. (2017) 14:1537. doi: 10.3390/ijerph14121537
51. Di Crosta A, Palumbo R, Marchetti D, Ceccato I, La Malva P, Maiella R, et al. Individual differences, economic stability, and fear of contagion as risk factors for PTSD symptoms in the COVID-19 emergency. Front Psychol. (2020) 11:2329. doi: 10.3389/fpsyg.2020.567367
52. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health. (2020) 16:57. doi: 10.1186/s12992-020-00589-w
53. Fekih-Romdhane F, Ghrissi F, Abbassi B, Cherif W, Cheour M. Prevalence and predictors of PTSD during the COVID-19 pandemic: findings from a Tunisian community sample. Psychiatry Res. (2020) 290:113131. doi: 10.1016/j.psychres.2020.113131
54. Slepski LA. Pandemic planning. In: Daily E, Powers R, editors. International Disaster Nursing. Cambridge: Cambridge University Press (2010). p. 397–426. doi: 10.1017/CBO9780511841415.027
55. Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S, Bai X, et al. The role of telehealth in reducing the mental health burden from COVID-19. Telemed e-Health. (2020) 26:377–9. doi: 10.1089/tmj.2020.0068
56. Banerjee D. The COVID-19 outbreak: crucial role the psychiatrists can play. Asian J Psychiatry. (2020) 50:102014. doi: 10.1016/j.ajp.2020.102014
57. Craig L, Churchill B. Dual-earner parent couples' work and care during COVID-19. Gender Work Organ. (2020) 28:514–27. doi: 10.1111/gwao.12497
58. Powell A, Craig L. Gender differences in working at home and time use patterns: evidence from Australia. Work Employm Soc. (2015) 29:571–89. doi: 10.1177/0950017014568140
59. Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. (2020) 87:40–8. doi: 10.1016/j.bbi.2020.04.028
60. Ranson G. Men, paid employment and family responsibilities: conceptualizing the ‘working father'. Gender Work Organ. (2012) 19:741–61. doi: 10.1111/j.1468-0432.2011.00549.x
61. Mahase E. Covid-19: EU states report 60% rise in emergency calls about domestic violence. Br Med J. (2020) 369:m1872. doi: 10.1136/bmj.m1872
62. Kilani HA, Bataineh MF, Al-Nawayseh A, Atiyat K, Obeid O, Abu-Hilal MM, et al. Healthy lifestyle behaviors are major predictors of mental wellbeing during COVID-19 pandemic confinement: a study on adult Arabs in higher educational institutions. PLoS ONE. (2020) 15:e0243524. doi: 10.1371/journal.pone.0243524
Keywords: psychological impact, mental health, COVID-19, United Arab Emirates, well-being
Citation: Cheikh Ismail L, Mohamad MN, Bataineh MF, Ajab A, Al-Marzouqi AM, Jarrar AH, Abu Jamous DO, Ali HI, Al Sabbah H, Hasan H, Stojanovska L, Hashim M, Shaker Obaid RR, Saleh ST, Osaili TM and Al Dhaheri AS (2021) Impact of the Coronavirus Pandemic (COVID-19) Lockdown on Mental Health and Well-Being in the United Arab Emirates. Front. Psychiatry 12:633230. doi: 10.3389/fpsyt.2021.633230
Received: 24 November 2020; Accepted: 16 February 2021;
Published: 16 March 2021.
Edited by:
Daniel Bressington, Charles Darwin University, AustraliaReviewed by:
Gianluca Serafini, San Martino Hospital (IRCCS), ItalyCopyright © 2021 Cheikh Ismail, Mohamad, Bataineh, Ajab, Al-Marzouqi, Jarrar, Abu Jamous, Ali, Al Sabbah, Hasan, Stojanovska, Hashim, Shaker Obaid, Saleh, Osaili and Al Dhaheri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ayesha S. Al Dhaheri, YXllc2hhX2FsZGhhaGVyaUB1YWV1LmFjLmFl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.