 Amílcar Silva-dos-Santos
Amílcar Silva-dos-Santos Miguel Sales
Miguel Sales Ana Sebastião
Ana Sebastião Ricardo Gusmão
Ricardo Gusmão- 1NOVA Medical School (NMS/FCM) – NOVA University of Lisbon, Lisbon, Portugal
- 2Department of Psychiatry – Hospital Vila Franca de Xira, Vila Franca de Xira, Portugal
- 3Faculty of Medicine and Unit of Neurosciences, Institute of Pharmacology and Neurosciences, Institute of Molecular Medicine, University of Lisbon, Lisbon, Portugal
- 4EPI Unit, Public Health Institute, University of Porto, Porto, Portugal
- 5Departamento de Ciências da Saúde Pública e Forenses, e Educação Médica, Faculdade de Medicina da Universidade do Porto, Porto, Portugal
Journalist:
Aren't you afraid of not feeling human after the implantation of
the deep brain stimulation electrodes to treat your resistant depression?
Patient:
When I was suffering from treatment-resistant depression I was not feeling human!
(A patient of Dr. Helen Mayberg treated with Deep Brain Stimulation).
Introduction
In this opinion article, we humbly propose a new viewpoint on the etiopathogenesis of depression. We base the model on our interpretation of selected recent neurophysiological findings, mainly regarding Deep Brain Stimulation (DBS) to treat Parkinson's Disease and also DBS to treat Treatment-Resistant Depression (TRD). We coin the idea a mental kindling-like mechanism. However, future clinical research, possibly complemented with human laboratory research or animal experiments, will be needed to test the validity of our proposed model. On the current manuscript framework, following the first and introductory section, we will set the stage by presenting selected studies and insights mainly from DBS to treat TRD and PD, on the second and middle section. Finally, we will discuss the proposed viewpoint on the third and last section of the present work.
Selected Neurophysiological Studies and Insights From DBS to Treat Treatment-Resistant Depression and Parkinson's Disease
DBS as a Therapy for PD
DBS was first introduced to medical practice by Benabid et al. (1). They discovered that high-frequency stimulation of the thalamus diminished tremor. Later, guided by the neurophysiological studies of Bergman et al. on the neural circuits involved in PD (2), Benabid stimulated the subthalamic nucleus with high-frequency current and achieved significant improvement of PD symptoms (3). PD has been linked to degeneration of dopaminergic neurons in the substantia nigra (4), which eventually results in an abnormal neuronal activity in the basal ganglia circuitry. This abnormal activity is characterized by synchronous bursts, which resemble epileptiform activity (5). These abnormal bursts affect the activity in the thalamus and cortical areas, causing the symptoms of PD (4). DBS has a therapeutic effect on PD because it disrupts the abnormal bursting in the basal ganglia—corticothalamic loops (6).
DBS as a Therapy for Depression
In 2005, Mayberg's group reported that DBS was effective for the treatment of patients with depression who were resistant to medication and/or electroconvulsive therapy (ECT) (7). The idea of such treatment was based on neuroimaging studies that revealed, in some patients with depression, abnormal hyperactivity of the subcallosal cingulate cortex (SCC) also known by area 25 of Broadman (BA25) or subgenual cingulated (Cg25). Mayberg et al. hypothesized that this hyperactivity detected in neuroimaging studies could be reduced by DBS. Indeed, DBS of the area 25 reduced depression symptoms in patients with abnormal neural activity (7). After this work, other studies have been published regarding the stimulation of area 25 of Broadman in depression making this area the most targeted in DBS for treatment-resistant depression (7–12). The lateral habenula is another area targeted in depression. It has been reported that the hyperactivity in this area can be ameliorated with DBS (13). Contrarily to the hyperactivation in the area 25 of Broadman and in the lateral habenula, there is hypoactivity in the nucleus accumbens (NAcc) that can be reverted by DBS in patients with treatment-resistant depression (14, 15). Other areas that have been stimulated in DBS are the ventral capsule and ventral striatum (16, 17), the internal capsule (18), the medial forebrain bundle (19), and the inferior thalamic peduncle (20). As it can be noted, there are different areas with distinct type of neural activity (hypo/hyperactivity) in treatment-resistant depression and DBS with high frequency stimulation can bring those activity to normal.
DBS Mechanisms
The exact mechanisms by which DBS works are not fully understood. In particular, it may seem paradoxical that DBS inhibits neural activity in the stimulated area instead of stimulating the neurons, therefore acting in a similar way to an ablation (6). One explanation for the inhibitory effect of DBS is that in the thalamus it induces a release of inhibitory neurotransmitters such as the homeostatic neuromodulator adenosine that causes a decrease in the excitatory neurotransmission and a reduction of tremor via Adenosine A1 receptors activation (21, 22). Inhibition is not the only mechanism by which DBS alleviates symptoms of PD and depression. Other mechanisms have been suggested and reviewed elsewhere (23), such as replacement of pathological bursting by neuronal patterns driven by DBS (24).
The correction of abnormal brain activity is another proposed DBS mechanism of action. Since, on the one hand, there is abnormal brain oscillation in PD (25) that is similar to the neural activity observed in some models of seizures and epilepsy (26, 27), and on the other hand, it has also been reported abnormal brain oscillation between some areas in depressive animals, it was considered that, at least in part, some abnormal epileptiform oscillation might be an electrophysiologic trait of some neurologic and psychiatric disorders. The origin of some abnormal brain oscillations is at the core of our proposed mental kindling-like mechanism and it will be addressed in the third part of the current manuscript.
DBS Works by Stimulating a Specific Brain Area. Why Do Therapies Such as Electroconvulsive Therapy (ECT) and Repetitive Transcranial Magnetic Stimulation (rTMS) Do Not Target a Specific Brain Area?
DBS of the subcallosal cingulated cortex (SCC) is effective in the treatment of depression. However, a patient-personalized protocol must be applied in order to be effective. Neuroimaging and electrophysiological studies during DBS surgery allow the determination of the exact and most adequate area to stimulate. It seems that SCC resembles a crossroad of different projections and the best effect is achieved by stimulating the exact crossing point (28). DBS targets specific areas that are functionally impaired in Depression. Some therapies such as the well-known ECT and the more recent TMS (initially applied to treat depression and then extended to other psychiatric disorders) (29–31), act in broader way. The duration of the effect varies among the different approaches: DBS only works when the stimulation is on, ECT's effects are more sustained (although requiring maintenance sessions), while TMS requires multiple sessions during weeks before achieving clinical results. The reason for these discrepancies is not known. A possible explanation could be that unlike DBS, that is more efficient locally, the other techniques could simultaneously modulate several regions and be more effective targeting the systemic/circuitries changes or, at least in part, the broad stimulation can reaches the more deep and specific areas through white matters pathways.
Other Selected Neuroanatomical and Neurophysiological Findings Relevant to Our Viewpoint
Psychiatric or mental disorders are some of the most difficult diseases to understand. Unlike the diseases that can be explained by a single gene mutation, specific lesions or microorganisms, mental disorders usually have multiple causes. As it has been stated in this paper, there are several areas with distinct neural activities (hypo/hyperactivity) that can be targeted in DBS for depression. Besides the local abnormal neural activity observed in neuroimaging techniques, there are abnormal oscillations between different regions that can be recorded with non-invasive electrophysiological tools and that might be used as potential biomarkers to evaluate neuromodulation success (32). To simplify our perspective about depression, we will focus on a particular brain area, but we consider that the mechanism we propose can, possibly, be applied to different areas of the brain. Several studies suggest that the chronic hyperactivation of area 25 is one of the neural mechanisms of depression. Functional neuroanatomy studies demonstrated that simply thinking about sad life events causes hyperactivity of the area 25 (33). This hyperactivity can be reduced by several types of treatment: selective serotonin reuptake inhibitor (8), transcranial magnetic stimulation (TMS) (34) and electroconvulsive therapy (ECT) (35). Several studies reported that depression is a multifactorial disease. From a pragmatic point of view, in psychiatry we observe a frequent pattern in clinical practice: a typical depressive patient has familiar history of depression or other mental illness, and has experienced one or few severe life stress, or accumulated many mild/moderate adverse life events during weeks, months to few years before the depressive episode. A typical sequence that triggers depression is: first the patient voluntarily thinks about the stressors, but later this remembrance became automatic or involuntarily (independent of the patient's will) and eventually the patient becomes clinically depressed. It remains unknown how the psychological, environmental and biological/genetic factors interact together with a cognitive style to cause a chronic hyperactivation of area 25. It has been reported that there is abnormal brain oscillations in PD such as low-frequency rhythmic bursting in the basal ganglia (5, 25, 36) that are similar to epileptic activity. It has also been reported abnormal brain oscillations between some areas in depressive animals (37). Furthermore, it was suggested that this epileptiphorm abnormal oscillation can be an electrophysiologic trait of several neurologic and psychiatric disorders (26). A possible phenomena that we call mental kindling-like mechanism (Figure 1A) may cause such abnormal brain oscillation in some types of depression associated with significant live events and/or stressors.
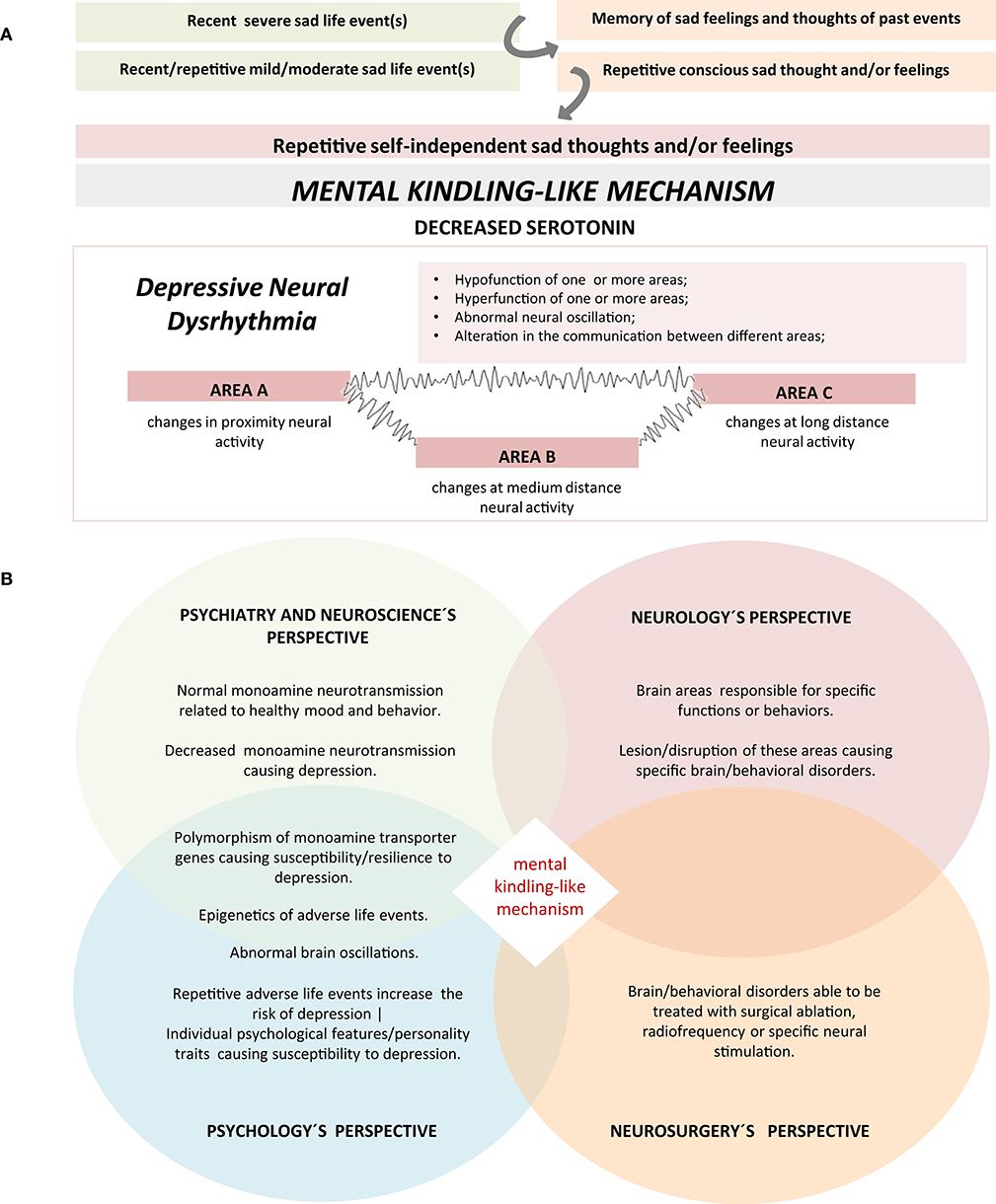
Figure 1. (A) A schematic of the hypothesis of the mental kindling-like mechanism in the etiopathogenesis of Depression. Repetitive sad life events, whether mild, moderate, or severe cause not only repetitive conscious thoughts and/or feelings, but also recall memories of sad feelings and thoughts. This pattern starts as a conscious process but can later become an independent or involuntarily process that can self-perpetuate and eventually cause the mental kindling-like mechanism. The mechanism may cause the depletion of serotonin and/or work as a trigger to dysregulate the neural nucleus and networks of emotion, resulting in the hypofunction/hyperfunction of different areas as well as abnormal communication between areas. (B) An hypothetical integrative physiopathological perspective of treatment-resistant major depression. A change in the neuronal activity of a brain region associated with depressive symptoms, decreased monoamine neurotransmission and abnormal neural activity caused, at least in part, by a possible mental kindling-like mechanism triggered by repetitive adverse live events in patients with genetic and/or psychological predisposition to depression. Due to the complexity and the multifactorial causes of depression, a single perspectives are not enough to understand the mechanisms of this disorder. A global and a more integrative perspective with the contribution of different disciplines can help understanding the mechanisms of depression.
Discussion
According to our interpretation of the studies presented above, we propose that a severe adverse life event, or repetitive mild/moderate chronic negative life events can initially lead, at least in part, to conscious and transient hyperactivation of area 25 and then an automatic/involuntary processing of this information contribute to its chronic hyperactivation. From a clinical perspective, depressive patients often have constant, repetitive, involuntary thoughts that they not regularly pay attention to. They also say that recent sad life events triggers the memories of previous sad thoughts and feelings, which amplify the currents ones. Often, they recognize this pattern if the clinician asks them what are the content of their thoughts and feeling, at night when they are in the bed awaiting to fall asleep, or when they are not occupied with day to day tasks. Similarly to the kindling experimental model of epilepsy (38), in which repetitive external electric brain insults lead to abnormal automatic activity and hence to seizures/epilepsy, repetitive exposure to sad thought can lead to self-independent chronic abnormal brain activity and hence depression (abnormal brain epileptiform-like activity triggered by repetitive automatic or self-amplifying thoughts in the areas linked to emotions). However, some patients exposed to several life stressors do not develop symptoms of depression. This might be related to a resilience effect. As an example, Caspi et al. found that patients with the long allele of the serotonin transporter (causing better serotoninergic activity) are more resilient to stressful life events and hence less susceptible to develop depression than patient with the short allele of the same gene (39). In the context, we can speculate that life events triggered kindling-like mechanism or mental kindling-like mechanism will disrupt the neural activity, in susceptible patients, either locally in some brain areas (such as the 25) or more broadly in other emotion circuitries. According to this perspective to understand depression, the final endpoint of depression could be explained as a brain dysrhythmia (depressive neural dysrhythmia), either locally (one nucleus) or systemically (circuitries, different nuclei), in which genetic and neurochemical mechanism would play important roles. This perspective that we call integrative perspective to understand mental disorders (Figure 1B) can integrate different scientific points of view to understand psychiatric disorders: (1) Neurosurgery—functional neurosurgery, to ablate the abnormal area (excision, ablation, applying radiofrequency or the new electric stimulation approach); (2) Neurology: specific brain areas have specific functions. Some brain areas are involved in healthy emotions. A lesion on these areas could cause depression; (3) Psychiatry and Neuroscience: Monoamine theory. Decreased serotonin and/or noradrenalin neurotransmission can cause depression. Treatment of depression can be achieved by restoring the monoamine neurotransmission, epigenetic, and changes in brain oscillation. Also specific personalities have specific cognitive styles that confers susceptibility to specific disorders (ex. patients with ruminative tendency are prone to depression); (4) Psychology/psychotherapy: Repetitive mild/moderate life traumas or severe life trauma can increase the risk of depression. Applying a new psychological style can help to address and deal with specific adverse life events.
Although we formulated our opinion based on the interpretation of recent and relevant scientific data and clinical studies, we acknowledge that future research will be needed to test the validity of our proposed model.
Author Contributions
AS-d-S wrote the first draft. All the authors edited and reviewed the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Benabid AL, Pollak P, Louveau A, Henry S, de Rougemont J. Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Appl Neurophysiol. (1987) 50:344–6. doi: 10.1159/000100803
2. Bergman H, Wichmann T, DeLong MR. Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science. (1990) 249:1436–8. doi: 10.1126/science.2402638
3. Limousin P, Pollak P, Benazzouz A, Hoffmann D, Le Bas JF, Broussolle E, et al. Effect of parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. (1995) 345:91–5. doi: 10.1016/S0140-6736(95)90062-4
4. Wichmann T, DeLong MR, Guridi J, Obeso JA. Milestones in research on the pathophysiology of Parkinson's disease. Mov Disord. (2011) 26:1032–41. doi: 10.1002/mds.23695
5. Santana MB, Halje P, Simplício H, Richter U, Freire MAM, Petersson P, et al. Spinal cord stimulation alleviates motor deficits in a primate model of parkinson disease. Neuron. (2014) 84:716–22. doi: 10.1016/j.neuron.2014.08.061
6. Lozano A, Dostrovsky J, Chen R, Ashby P. Deep brain stimulation for Parkinson's disease: disrupting the disruption. Lancet Neurol. (2002) 1:225–31. doi: 10.1016/S1474-4422(02)00101-1
7. Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C, et al. Deep brain stimulation for treatment-resistant depression. Neuron. (2005) 45:651–60. doi: 10.1016/j.neuron.2005.02.014
8. Kennedy SH, Evans KR, Kruger S, Mayberg HS, Meyer JH, McCann S, et al. Changes in regional brain glucose metabolism measured with positron emission tomography after paroxetine treatment of major depression. Am J Psychiatry. (2001) 158:899–905. doi: 10.1176/appi.ajp.158.6.899
9. Puigdemont D, Pérez-Egea R, Portella MJ, Molet J, de Diego-Adeliño J, Gironell A, et al. Deep brain stimulation of the subcallosal cingulate gyrus: further evidence in treatment-resistant major depression. Int J Neuropsychopharmacol. (2012) 15:121–33. doi: 10.1017/S1461145711001088
10. Puigdemont D, Portella M, Pérez-Egea R, Molet J, Gironell A, de Diego-Adeliño J, et al. A randomized double-blind crossover trial of deep brain stimulation of the subcallosal cingulate gyrus in patients with treatment-resistant depression: a pilot study of relapse prevention. J Psychiatry Neurosci. (2015) 40:224–31. doi: 10.1503/jpn.130295
11. Lozano AM, Giacobbe P, Hamani C, Rizvi SJ, Kennedy SH, Kolivakis TT, et al. A multicenter pilot study of subcallosal cingulate area deep brain stimulation for treatment-resistant depression. J Neurosurg. (2012) 116:315–22. doi: 10.3171/2011.10.JNS102122
12. Holtzheimer PE, Kelley ME, Gross RE, Filkowski MM, Garlow SJ, Barrocas A, et al. Subcallosal cingulate deep brain stimulation for treatment-resistant unipolar and bipolar depression. Arch Gen Psychiatry. (2012) 69:150–8. doi: 10.1001/archgenpsychiatry.2011.1456
13. Kiening K, Sartorius A. A new translational target for deep brain stimulation to treat depression. EMBO Mol Med. (2013) 5:1151–3. doi: 10.1002/emmm.201302947
14. Bewernick BH, Hurlemann R, Matusch A, Kayser S, Grubert C, Hadrysiewicz B, et al. Nucleus accumbens deep brain stimulation decreases ratings of depression and anxiety in treatment-resistant depression. Biol Psychiatry. (2010) 67:110–6. doi: 10.1016/j.biopsych.2009.09.013
15. Bewernick BH, Kayser S, Sturm V, Schlaepfer TE. Long-term effects of nucleus accumbens deep brain stimulation in treatment-resistant depression: evidence for sustained efficacy. Neuropsychopharmacology. (2012) 37:1975–85. doi: 10.1038/npp.2012.44
16. Malone DA, Dougherty DD, Rezai AR, Carpenter LL, Friehs GM, Eskandar EN, et al. Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol Psychiatry. (2009) 65:267–75. doi: 10.1016/j.biopsych.2008.08.029
17. Dougherty DD, Rezai AR, Carpenter LL, Howland RH, Bhati MT, O'Reardon JP, et al. A randomized sham-controlled trial of deep brain stimulation of the ventral capsule/ventral striatum for chronic treatment-resistant depression. Biol Psychiatry. (2015) 78:240–8. doi: 10.1016/j.biopsych.2014.11.023
18. Van Der Wal JM, Bergfeld IO, Lok A, Mantione M, Figee M, Notten P, et al. Long-term deep brain stimulation of the ventral anterior limb of the internal capsule for treatment-resistant depression. J Neurol Neurosurg Psychiatry. (2020) 91:189–95. doi: 10.1136/jnnp-2019-321758
19. Schlaepfer TE, Bewernick BH. Deep brain stimulation for major depression. Handb Clin Neurol. (2013) 116:235–43. doi: 10.1016/B978-0-444-53497-2.00018-8
20. Jiménez F, Velasco F, Salin-Pascual R, Hernández JA, Velasco M, Criales JL, et al. A patient with a resistant major depression disorder treated with deep brain stimulation in the inferior thalamic peduncle. Neurosurgery. (2005) 57:585–92. doi: 10.1227/01.NEU.0000170434.44335.19
21. Sebastiao AM, Ribeiro JA. Adenosine receptors and the central nervous system. Handb Exp Pharmacol. (2009) 193:471–534. doi: 10.1007/978-3-540-89615-9_16
22. Bekar L, Libionka W, Tian GF, Xu Q, Torres A, Wang X, et al. Adenosine is crucial for deep brain stimulation-mediated attenuation of tremor. Nat Med. (2008) 14:75–80. doi: 10.1038/nm1693
23. Benabid AL, Chabardes S, Mitrofanis J, Pollak P. Deep brain stimulation of the subthalamic nucleus for the treatment of Parkinson's disease. Lancet Neurol. (2009) 8:67–81. doi: 10.1016/S1474-4422(08)70291-6
24. McIntyre CC, Savasta M, Kerkerian-Le Goff L, Vitek JL. Uncovering the mechanism(s) of action of deep brain stimulation: activation, inhibition, or both. Clin Neurophysiol. (2004) 115:1239–48. doi: 10.1016/j.clinph.2003.12.024
25. Fuentes R, Petersson P, Siesser WB, Caron MG, Nicolelis MAL. Spinal cord stimulation restores locomotion in animal models of Parkinson's disease. Science. (2009) 323:1578–82. doi: 10.1126/science.1164901
26. Pais-Vieira M, Yadav AP, Moreira D, Guggenmos D, Santos A, Lebedev M, et al. A closed loop brain-machine interface for epilepsy control using dorsal column electrical stimulation. Sci Rep. (2016) 6:32814. doi: 10.1038/srep32814
27. Silva-dos-Santos A. The hypothesis of connecting two spinal cords as a way of sharing information between two brains and nervous systems. Front Psychol. (2017) 8:105. doi: 10.3389/fpsyg.2017.00105
28. Riva-Posse P, Choi KS, Holtzheimer PE, McIntyre CC, Gross RE, Chaturvedi A, et al. Defining critical white matter pathways mediating successful subcallosal cingulate deep brain stimulation for treatment-resistant depression. Biol Psychiatry. (2014) 76:963–9. doi: 10.1016/j.biopsych.2014.03.029
29. Sokhadze E, Baruth J, Tasman A, Mansoor M, Ramaswamy R, Sears L, et al. Low-frequency repetitive transcranial magnetic stimulation (rTMS) affects event-related potential measures of novelty processing in autism. Appl Psychophysiol Biofeedback. (2010) 35:147–61. doi: 10.1007/s10484-009-9121-2
30. Freitas C, Mondragon-Llorca H, Pascual-Leone A. Noninvasive brain stimulation in Alzheimer's disease: systematic review and perspectives for the future. Exp Gerontol. (2011) 46:611–27. doi: 10.1016/j.exger.2011.04.001
31. Levkovitz Y, Isserles M, Padberg F, Lisanby SH, Bystritsky A, Xia G, et al. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. (2015) 14:64–73. doi: 10.1002/wps.20199
32. Smart OL, Tiruvadi VR, Mayberg HS. Multimodal approaches to define network oscillations in depression. Biol Psychiatry. (2015) 77:1061–70. doi: 10.1016/j.biopsych.2015.01.002
33. Liotti M, Mayberg HS, Brannan SK, McGinnis S, Jerabek P, Fox PT. Differential limbic–cortical correlates of sadness and anxiety in healthy subjects: implications for affective disorders. Biol Psychiatry. (2000) 48:30–42. doi: 10.1016/S0006-3223(00)00874-X
34. Nahas Z, Teneback CC, Kozel A, Speer AM, DeBrux C, Molloy M, et al. Brain effects of TMS delivered over prefrontal cortex in depressed adults: role of stimulation frequency and coil-cortex distance. J Neuropsychiatry Clin Neurosci. (2001) 13:459–70. doi: 10.1176/jnp.13.4.459
35. Nobler MS, Oquendo MA, Kegeles LS, Malone KM, Campbell CC, Sackeim HA, et al. Decreased regional brain metabolism after ect. Am J Psychiatry. (2001) 158:305–8. doi: 10.1176/appi.ajp.158.2.305
36. Bevan MD, Magill PJ, Terman D, Bolam JP, Wilson CJ. Move to the rhythm: oscillations in the subthalamic nucleus-external globus pallidus network. Trends Neurosci. (2002) 25:525–31. doi: 10.1016/S0166-2236(02)02235-X
37. Dzirasa K, Kumar S, Sachs BD, Caron MG, Nicolelis MAL. Cortical-amygdalar circuit dysfunction in a genetic mouse model of serotonin deficiency. J Neurosci. (2013) 33:4505–13. doi: 10.1523/JNEUROSCI.4891-12.2013
38. Goddard GV, McIntyre DC, Leech CK. A permanent change in brain function resulting from daily electrical stimulation. Exp Neurol. (1969) 25:295–330. doi: 10.1016/0014-4886(69)90128-9
Keywords: deep brain stimulation, etiopathogenesis, Parkinson's disease, treatment-resistant depression, depression, mental kindling-like mechanism
Citation: Silva-dos-Santos A, Sales M, Sebastião A and Gusmão R (2021) A New Viewpoint on the Etiopathogenesis of Depression: Insights From the Neurophysiology of Deep Brain Stimulation in Parkinson's Disease and Treatment-Resistant Depression. Front. Psychiatry 12:607339. doi: 10.3389/fpsyt.2021.607339
Received: 18 September 2020; Accepted: 18 February 2021;
Published: 09 April 2021.
Edited by:
Alireza Mohammadi, University of Tabriz, IranReviewed by:
Ossama Yassin Mansour, Alexandria University, EgyptCopyright © 2021 Silva-dos-Santos, Sales, Sebastião and Gusmão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amílcar Silva-dos-Santos, YW1pbGNhcnNzQGdtYWlsLmNvbQ==