 Raquel Martín Ríos
Raquel Martín Ríos Francisca López-Torrecillas
Francisca López-Torrecillas Ignacio Martín Tamayo
Ignacio Martín Tamayo- 1Department of Personality, Assessment and Psychological Treatment, University of Granada, Granada, Spain
- 2Department of Methodology of Behavioral Sciences, University of Granada, Granada, Spain
There is increasing evidence that executive functions have significative effects on nicotine abuse. An unresolved challenge for smoking cessation interventions is the detection of factors associated with nicotine use. In order to understand how cognition is affected by nicotine abuse, this study was designed to determine the relationship between years of smoking addiction and several variables of executive functions. The sample was composed of 174 smokers, whose age ranged between 27 and 69 years old (M = 47.44; SD = 8.48). Smokers were assessed at baseline with measures of cognitive inhibition [Go/No Go Task and Five Digit Test (FDT)], updating [Visual Search and Attention Test (VSAT) and Letter-Number Sequencing (WAIS IV)] and shifting [Delay Discounting Task (DDT) and Iowa Gambling Task (IGT)] while the outcome measure was years of smoking. The linear regression and correlation analysis highlighting that the variable which has the strongest association with years of smoking is updating. Multivariate analysis of variance (MANCOVA) followed by Tukey post-hoc tests revealed significant differences such that heavy smoking indicated worse performance than light smoking on updating tasks. These findings report the ability of working memory to predict years of smoking and suggest that cigarette packaging warning may experience a loss of effectiveness in heavy smokers.
Introduction
Tobacco use is a major risk factor for cardiovascular and respiratory diseases (1). Smoking is also unfavorable to the immune systems, making smokers more vulnerable to infectious diseases (2). Despite this, the tobacco industry seems unperturbed (3). An unresolved challenge for smoking cessation interventions is the detection of factors associated with nicotine use. In particular, findings in animal models suggest that the underlying reasons for smoking may be quite different across individuals (4).
Several factors are identified to have an impact on smoking addiction: age of initiation (5, 6), negative affective states (7–9), mood disorders (10), psychiatric disorders (11, 12) and executive functioning (8, 13–15). The addiction process elicits neuroadaptations that affect broadly distributed neural circuits involved in cognitive process (16). Indeed, there is increasing evidence that executive functions have significant effects on nicotine dependence. Executive function (EF) refers to a “set of general-purpose control processes that regulate one's thoughts and behaviors” (17). Miyake et al. (18) identified three different components of EF: (1) Inhibitory processes, (2) Updating, and (3) Shifting processes (18). However, studies examining associations between executive measures and clinical aspects of smoking such as years of smoking addiction are reduced and generally limited to predict risk profiles. Also, existing literature examining the effects of EF on substance abuse focuses on inhibition and working memory components (14).
Flaudias et al. (13) evaluated the influence of executive functions (inhibition, updating and shifting) on craving [The Tobacco Craving Questionnaire; (19)] and nicotine dependence [Fagerström Test for Nicotine Dependence, (20)] in a sample of moderate (Fagerström >3) and severe (Fagerström >7) smokers. They used a Stroop task (21) and Hayling's test (22) as measures of inhibition, “Trail Making Test” (23) as a measure of shifting, and the “N-back” test (24) for updating. The dimension of inhibition seems to be a significantly stronger predictor of tobacco dependence than craving or updating abilities (13). Findings are reminiscent of the work of Billieux et al. (25) who has discovered that a poor ability to inhibit evaluated by a go-stop task (26) as well as age are significant predictors of tobacco dependence evaluated by Fagerström Test for Nicotine Dependence, (20). Further, Hu et al. (27) examined the relationship between smoking and cognitive performance in working memory among smokers and non-smokers. All participants were evaluated with the subtests of information, arithmetic and digits (28) and the Dysexecutive Questionnaire (29). In addition, smokers were measured on their level of nicotine dependence (20). Smokers reported lower performance on the arithmetic and digit subtests than non-smokers. There was also a direct correlation between digit scores (reverse order condition) and age of smoking initiation. On the other hand, smokers had higher scores on the dysexecutive questionnaire than non-smokers (27). Taken together, poor executive functions have been linked to nicotine abuse but it is unclear whether such executive components differentially interfere with each stage of addiction. Furthermore, to our knowledge, there are no studies that explore years of smoking addiction as a possible factor linked to executive performance.
Studying executive measures together with behavioral aspects of smoking could be of major interest for several reasons. Firstly, smoking cessation therapies are ineffective for most treatment-seeking smokers (30). A better understanding of the underpinnings of nicotine use may help to improve smoking cessation treatment. Secondly, several studies advocate the idea of including further smoking history variables because they would provide possible illustrative predictors of correlates of nicotine dependence (31, 32). Finally, exploring neuropsychological measures among different smoking patterns could lead to potential implications for prevention and treatment (33). In this regard, a comprehensive assessment will help to identify possible inter-subject variables that may be associated with a pattern of sustained tobacco abuse. In response to these limitations, we conducted a naturalistic and cross-sectional study to identify key factors that promote nicotine use. Particularly, this study was designed to determine the effects of several executive control functions. Assuming the three components of the dominant executive functioning model (18), we assessed inhibitory processes, updating and shifting on clinical aspects of smoking. In agreement with existing studies, we hypothesized that inhibition and updating components would be associated with years of addiction. Furthermore, we expected to find that long-term smokers should report more signs of executive dysfunction.
Materials and Methods
The sample consisted of 174 smokers (59% females), whose age ranged between 27 and 69 years old (M = 47.44; SD = 8.48) and they were recruited across 3 years. The average sample score in Fagerström Test for Nicotine Dependence (FTND) was 4.49 (SD=2.32) and they smoked an average of 17.9 (SD=8.94) cigarettes per day. Participants were eligible if they were current smokers and the sample selection criteria were: (1) aged above 18 years old (2) were employed by the University of Granada (Spain). The exclusion criteria were: (1) any illness or mental disorders suggesting possible difficulty in completing the different tasks and (2) current psychotropic medication for psychiatric symptoms, concurrent dependence on other substances (cocaine, heroin, alcohol, etc.). All the participants signed a written consent form. The study protocol was approved by the Bioethics Committee of the University of Granada (Spain) and adhered to the tenets of the Declaration of Helsinki.
Experimental Design
We conducted a naturalistic and cross-sectional study during the course of a smoking cessation treatment intervention. Smokers were invited to participate in a study assessing personality and cognition in relation to smoking behavior. Participants were recruited as they engaged in an occupational health service that provides smoking cessation treatment including pharmacological (varenicline) and behavioral change components. This treatment consisted of three phases: (1) psychoeducation phase to reduce smoking (planning of activities and establishment of objectives), (2) prescription and controlled administration of the drug varenicline a partial agonist and antagonist drug in the presence of nicotine neuronal receptors for nicotine acetylcholine α4β2 and (3) training of relapse prevention strategies.
The program begins with an initial session where a semi-structured interview for smokers is conducted as well as a neuropsychological assessment of all smokers. All measures of this study were collected at baseline. Tests were administered always in a fixed order designed to alternate between easy/difficult tasks. This initial evaluation was conducted in a single session, considering the appropriate breaks to avoid the effect of fatigue. A unique code was assigned to the participants in order to carry out an individual follow-up while safeguarding anonymity.
Measurements
All neuropsychological evaluations were conducted by trained psychologists. Smokers were evaluated at baseline with these assessments:
Semi-structured Interview for Smokers (34)
This survey provides information about socio-demographic data, smoking duration, level of dependence and brand of cigarettes. The primary outcome variable was assessed. Years of smoking addiction were defined as the number of years from the initiation of nicotine use to the initiation of smoking cessation treatment. Another important parameter to consider when evaluating higher prevalence of smoking is the number of cigarettes consumed per smoking day (CPD). CPD was used as a covariate in analyses.
Fagerström Test for Nicotine Dependence (20)
This test was designed to provide an ordinal measure of nicotine dependence related to cigarette smoking. It contains six items that assess the quantity of cigarette consumption, the compulsion to use and dependence. The FTND produces a score from 0 to 10, with higher scores indicating more severe nicotine addiction. The FTND allows classification of nicotine dependence severity into different levels: low (0 to 2 points), moderate (3 to 7 points), and high (>7 points).
Letter-Number Sequencing Task (28)
This task is an attentional subtest of the Wechsler Adult Intelligence Scale. The participant must sequence a random order of numbers and letter. They must say the numbers in ascending order and then the letters in alphabetical order. The dependent variable to be considered in this test would be the total number of hits.
Visual Search and Attention Test (35)
This test consists of four visual cancellation tasks that require the respondent to cross out letters and symbols that are identical to a target. It is an attention task that require visual search based on either a single-feature search or a dual-feature search. The main dependent variable used in this test was number of correctly identified targets.
Go/No Go Task (36)
This task assesses the ability to inhibit a simple motor response. It consisted of 60 trials. In the first 30 trials (pre-switch), participants were asked to press a key as quickly as they could whenever the go stimulus (a letter) was presented, and to withhold the response when the no-go stimulus (a different letter) was presented. In the second 30 trials of the task (post-switch), participants were asked to respond to the previously no-go stimulus and not to respond to the previously go stimulus. The proportion of go vs. no-go trials on both phases (pre- and post-switch) was 7/3. The inter-stimulus interval (ISI) was set at 100 ms, and each stimulus was presented during 1,000 ms. Auditory feedback was provided after each response to indicate whether that response had been right or wrong. Responses were coded as hits (responding in presence the go trial), false alarms (responding in presence of the no-go trial), misses (not responding in presence of the go trial), and correct rejections (not responding in presence of the no-go trial). The main variable from this task was the false alarm rate, computed as the ratio between the number of false alarms and the total number of no-go trials.
Delay Discounting Task (37)
This task is a monetary-choice questionnaire asking for individual preferences between smaller, immediate rewards and larger, delayed rewards varying on their value and time to be delivered. The questionnaire is composed of a fixed set of 27 choices. We calculated the area under the curve (AUC) (38). The AUC was calculated for the range of reward magnitudes included in the questionnaire (small –Euro 25 to 35; medium –Euro 50 to 60; and large –Euro 75 to 85), according to the formula (x2–x1) [(y1–y2)/2], where x1 and x2 are successive delays, and y 1 and y 2 are the subjective values associated with these delays.
Iowa Gambling Task (39)
The task is a computerized measure of decision-making abilities. The participants attempt to win as much play money as possible by selecting cards from four decks (A, B, C, and D). Each time a participant selects a card, a specified amount of play money is awarded. However, interspersed among these rewards, there are probabilistic punishments (monetary losses). Two of the decks of cards (A and B) produce high immediate gains; however, in the long run, they will take more money than they give, and are thus considered disadvantageous. The other two decks (C and D) are considered advantageous, as they result in small, immediate gains, but will yield more money than they take in the long run. The decisive dependent measure for this task was the difference in the number of cards selected from the advantageous vs. disadvantageous decks across five block of 20 trials.
Five Digit Test (40)
This test is a numerical Stroop task divided into four components. The first component demands participants to name numbers from 1 to 5 as fast as they can. On the second component, participants must describe quantities from 1 to 5. The third component involves a selective attention trial, they must not read the numbers but rather tell how many numbers are present in each stimulus. Finally, on the fourth component participants must read the stimulus numbers. We recorded the total time for each component. The main dependent variable used in this test was the time required to complete each task.
Statistical Analysis
We presented sociodemographic data as percentages and frequencies. In addition, we tested the association of years of smoking with other neuropsychological tests using Spearman rank-order correlations. Firstly, we performed a linear regression analyses including the following predictors: Letter-Number Sequencing Task total score, Visual Search and Attention Test total stimulus score, Go/No Go false alarms, Delay Discounting area under the curve, Iowa Gambling Task net score and Five Digit Test score. The dependent variable was the years of smoking addiction. Secondly, we performed a multivariate analysis of variance (MANCOVA) to determine whether there are any differences between performance in cognitive tasks and relevant aspect of smoking. Although there is not a consensus on how to best define smoking (31), different variables collected by smoking history were considered to provide a broader assessment of smoking (32). In consequence, smokers were coded as either “light smoking” (0–24 years) or “heavy smoking” (≥ 25 years) on the results of smoking behavior self-reports. Nicotine dependence level as measured by FTND were coded as high level of dependence (>7 points) and moderate level of dependence (3 to 7 points) (20). Finally, according to the number of cigarettes per day, it has been proposed that smokers can be divided into three levels (CPD: 5–14, CPD: 15–24, ≥25 CPD) (41).
All statistical tests were performed using the software package SPSS version 25.0 (42). We performed an analysis on all the participants simultaneously. For all analyses, p = 0.05 was adopted as the significance criterion.
Results
The means and standard deviations of clinical aspects of smoking and neuropsychological measures are provided in Table 1. The mean sample score on the Fagerström test for nicotine dependence (FNDT) was moderate (M = 4.49, SD = 2.32). The sample had an average of 17.9 cigarettes per day (SD = 8.94) with an average nicotine level per cigarette of 0.99 mg (SD=.13). Besides, participants showed a low level of previous attempts to quit smoking (M = 1.27, SD = 1.35) during their years of addiction. Men smokers reported a significantly higher level of both nicotine dependence on the FTND overall (M = 5.05, SD = 2.51) and cigarettes per day (M = 20.96, SD = 10.02) that did woman smokers (M = 4.19, SD = 2.05; M = 16.20, SD = 7.92).
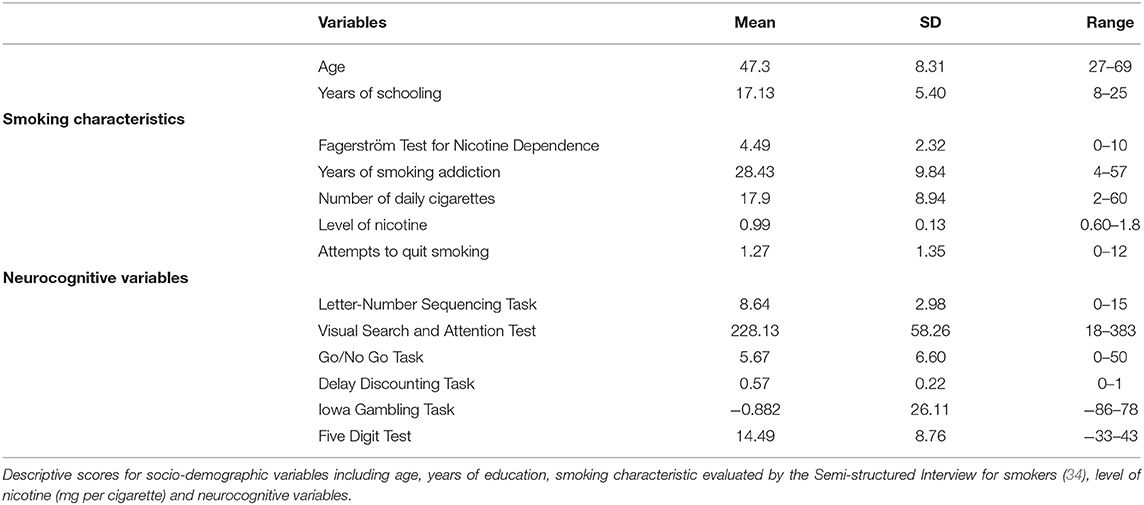
Table 1. Baseline demographic and smoking characteristics of the participants (n = 174).
Table 2 shows the pattern of correlations between Years of smoking addiction and neuropsychological measures. Moderate correlations were found between Years of smoking and measures of working memory (VSAT), inhibitory control (GNG) and cognitive flexibility (IGT), ranging from −0.119 to −0.425. The strongest association was with the working memory score (VSAT). We also found a differential pattern of association of the variable outcome with Letter-Number Sequencing Task, Delay Discounting Task and Five Digit test (ranging from −0.011 to 0.078).
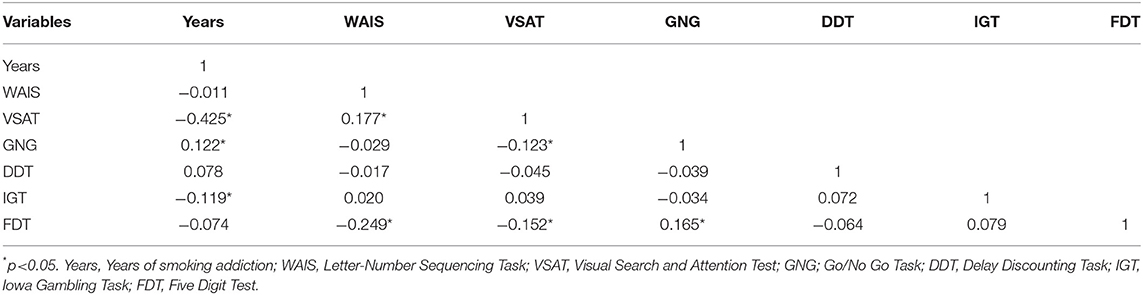
Table 2. Pearson correlation analysis between cognitive variables and Years of smoking (n = 174).
After bivariate correlation analysis, multiple regression analyses were used to identify predictors of years of smoking addiction in current smokers. The model including neurocognitive scores showed satisfactory fit explaining 22.2% of variance, F (6, 167) = 7.893; p < 0.000. Inspection of parameter estimates showed that the dimension of working memory (VSAT) was significantly and inversely associated with Years of smoking (β = −0.434, p < 0.000). However, none of the others neurocognitive tasks were significantly associated with the primary outcome variable (see Table 3).
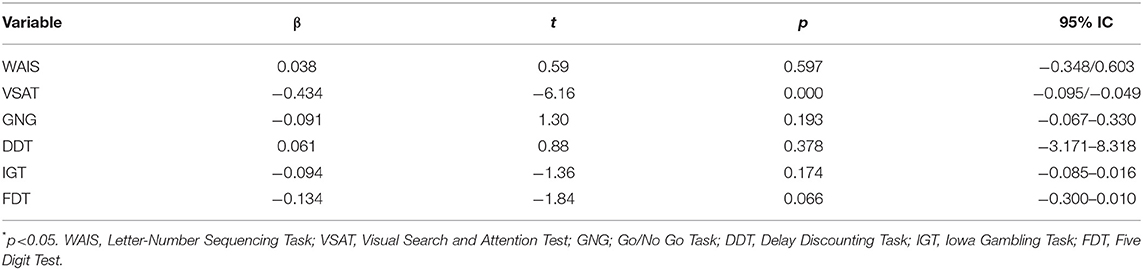
Table 3. Multiple linear regression analysis (n = 174).
Years of addiction (0–24 years; ≥ 25 years) x FTND level (moderate level of dependence or high level of dependence) x cigarettes per day (CPD: 5–14, CPD: 15–24, ≥ 25 CPD) multivariate analysis of covariance (MANCOVA) was conducted on the WAIS subscale, the VSAT test, the GNG task, the DDT task, the IGT and the FDT with age as the covariate. According to Pillai's Trace multivariate effects were highly significant for the FTND F(7, 156) = 2.107, p < 0.041, partial η2 = 0.086. Univariate effects on VSAT was significant F(11, 156) = 8.455, p < 0.000, and also on WAIS, F(11, 156) = 1.877, p < 0.046 (Table 4). To further clarify the findings, Tukey post-hoc test (p < 0.05) indicated that long-term smokers (≥25 years) scored significantly lower (indicated worse functioning) on VSAT task. In addition, both smokers with higher levels of dependence on FNDT (>7 points) and smokers with higher rates of cigarettes per day (≥25 CPD) score worse on WAIS task.
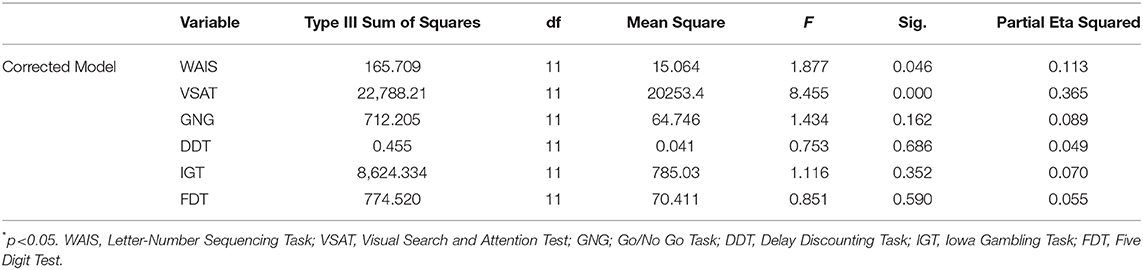
Table 4. Tests of between-subjects effects.
Discussion
Through this behavioral research, we intend to explore possible individual differences that may be linked to an executive pattern attributable to sustained smoking abuse. The aim of this study was to identify predictors of years of smoking addiction in a sample of current smokers. Specifically, we investigated the influence of neurocognitive variables such as updating, inhibitory control and cognitive flexibility ability. Results from the analysis revealed that the regression model including neurocognitive scores showed satisfactory fit explaining 22.2% of variance. However, an inspection of parameter estimates showed that the dimension of working memory (VSAT)was significantly and inversely associated with Years of smoking addiction. In consequence, the main finding of this study was that a poorer performance in working memory predicts the primary outcome variable. These results are in line with some previous scientific studies which examined the relationship between smoking and cognitive performance in working memory. Sutherland et al. (43) analyzed the effect of nicotine on EF performance through a working memory task based on the continuous-counting paradigm that required maintenance and simultaneous shifting in a sample of smokers and non-smokers. The findings suggest that smokers showed increased sustained activation in the medial and lateral prefrontal cortex during task execution. Smokers were also less effective in mobilizing the cognitive resources required to perform tasks that require recruitment and control of working memory. Thus, the increase in frontal activity recorded in smokers represents the need to increase cognitive resources to guide behavior during task execution (43). Recent data suggest that smokers performed worse on some cognitive tasks (arithmetic and digits subtests) (28) than nonsmokers. In addition, working memory (scores on digit subtest) was related to the age of starting smoking (27). In contrast, the lack of findings among others neuropsychological measures could be attributed to the fact that executive components such as inhibition and change are involved in other aspect of nicotine addiction such as relapse or initiation. For example, López-Torrecillas et al. (44) analyzed the predictive capacity of different temperamental measures [Barratt Impulsiveness Scale (44)], temperamental dimensions [Temperament and Character Inventory Revised; (45)], and neurocognitive tasks: Go/NoGo task (36), a delayed discount task (37) and decision making [Iowa Gambling Task; (39)] to predict smoking relapse. The results showed that poorer performance on the Gambling Task predicted greater relapse (44). Besides, a recent study (46) examined the predictive ability of delayed discounting to predict relapses after six months of tobacco cessation. The logistic regression model reported that longer discount delay, younger age, more previous quit attempts and higher dependence (FTND) were associated with higher risk of relapse at the 6-month follow-up.
On the other hand, multivariate analyses of covariance (MANCOVA) revealed highly significant differences between heavy smokers and light smokers on both VSAT and WAIS tasks after controlling for age via covariate analysis. When age scores were added as covariate in the MANCOVA, the observed differences between light and heavy smokers seemed potentially attributable to the higher levels of nicotine dependence in the heavy smokers. In particular, nicotine dependence level as measured by FTND significantly interacted with updating measures. Sensitivity analyses further showed that long-term smokers (≥25 years) scored significantly lower on the VSAT task. Besides, groups with both highest levels of dependence on FNDT (>7 points) and highest rates of cigarettes per day (≥25 CPD) showed worse scores on WAIS task. Group differences in working memory may reflect the injurious effects of smoking. Also, these results indicate that updating measures could be useful to prospectively predict years of addiction, such that they could be utilized to identify potential heavy smokers. Consequently, based on human neuroimaging evidence, the insula is critically involved in maintaining cigarette smoking (47). Recently, Li et al. (48) investigated the differences in insular morphometry between smokers and non-smokers. The authors explained that the insula had a trend to be negatively correlated (not significant) with pack-years. However, they found decreased cortical thickness of insula in smokers compared to non-smokers (48).
The analyses presented in this article emphasize the need to include a comprehensive smoking assessment, which contains variables of smoking behavior, to examine the effects of nicotine consumption on cognition. As mentioned before, the diverse behavioral effects of nicotine on different aspects of cognition suggest that there is considerable heterogeneity in the underlying causes of smoking (4). Taken together, the results highlight key factors that promote nicotine use. Smoking behavior may reflect a decrease in working memory and attention span that requires a visual search. Following Kübler et al. (49), we hypothesize that smokers with a long history of tobacco addiction show poor performance in working memory and attention tasks then it predisposes them to ruminative and craving thoughts, conventionally linked to addiction (49, 50).
This study has some important limitations that should be considered for an appropriate interpretation of its findings. First of all, participants were all employees of the same institution and there may be a concern because the sample is not representative of clinical populations but sufficiently diverse to be representative of the general population. Secondly, the cross-sectional nature of this study makes it difficult to obtain the inferred causal relationship between the variables. However, to our knowledge, this is the first study to show that a cognitive measure (attention task that requires visual search) is significantly associated with years of smoking. Despite these limitations, these findings have important public health implications and suggest that interventions designed for smoking cessation should focus not only on reducing relapses but also on improving executive functions such as working memory and attentional bias to smoking cues. In addition, these findings suggest that cigarette packaging warning (51) may experience a loss of effectiveness in long-term smokers as well as high levels of dependence. In this sense, behavioral approaches that recover cognitive functions help to improve theoretical support (33). Future studies in this area will have critical value toward reducing deficits in executive control functions, resulting in public health benefits.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Bioethics Committee of the University of Granada (Spain). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RMR and FLT: conceived, designed, and performed the experiments and wrote the paper. RMR, FLT, and IMT: analyzed the data. RMR: guarantor for this paper. All authors: read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank the research participants for their time and dedication.
References
1. World Health Organization. WHO Report on Global Tobacco Epidemic. Geneva: World Health Organization (2019).
2. Zhou Z, Chen P, Peng H. Are healthy smokers really healthy? Tob Induced Dis. (2016) 14:35. doi: 10.1186/s12971-016-0101-z
3. Hefler M, Gartner CE. The tobacco industry in the time of COVID-19: time to shut it down? Tob Control. (2020) 29:245–6. doi: 10.1136/tobaccocontrol-2020-055807
4. Hall FS, Der-Avakian A, Gould TJ, Markou A, Shoaib M, Young JW. Negative affective states and cognitive impairments in nicotine dependence. Neurosci Biobehav Rev. (2015) 58:168–85. doi: 10.1016/j.neubiorev.2015.06.004
5. Rupprecht LE, Smith TT, Schassburger RL, Buffalari DM, Sved AF, Donny EC. Behavioral mechanisms underlying nicotine reinforcement. Curr Top Behav Neurosci. (2015) 24:19–53. doi: 10.1007/978-3-319-13482-6_2
6. de Kloet SF, Mansvelder HD, De Vries TJ. Cholinergic modulation of dopamine pathways through nicotinic acetylcholine receptors. Biochem Pharmacol. (2015) 97:425–38. doi: 10.1016/j.bcp.2015.07.014
7. Lyvers M, Carlopio C, Bothma V, Edwards MS. Mood, mood regulation expectancies and frontal systems functioning in current smokers versus never-smokers in China and Australia. Addict Behav. (2013) 38:2741–50. doi: 10.1016/j.addbeh.2013.07.002
8. Lyvers M, Carlopio C, Bothma V, Edwards MS. Mood, mood regulation, and frontal systems functioning in current smokers, long-term abstinent ex-smokers, and never-smokers. J Psychoactive Drugs. (2014) 46:133–9. doi: 10.1080/02791072.2013.876522
9. Perkins KA, Karelitz JL, Giedgowd GE, Conklin CA. Negative mood effects on craving to smoke in women versus men. Addict Behav. (2013) 38:1527–31. doi: 10.1016/j.addbeh.2012.06.002
10. Kutlu MG, Gould TJ. Nicotine modulation of fear memories and anxiety: implications for learning and anxiety disorders. Biochem Pharmacol. (2015) 97:498–511. doi: 10.1016/j.bcp.2015.07.029
11. McCorkindale AN, Sheedy D, Kril JJ, Sutherland GT. The effects of chronic smoking on the pathology of alcohol-related brain damage. Alcohol. (2016) 53:35–44. doi: 10.1016/j.alcohol.2016.04.002
12. Molero Chamizo A, Muñoz Negro JE. Psicofarmacología de la nicotina y conducta adictiva. Trastornos Adictivos. (2005) 7:137–52. doi: 10.1016/S1575-0973(05)74521-9
13. Flaudias V, Picot MC, Lopez-Castroman J, Llorca P-M, Schmitt A, Perriot J, et al. Executive functions in tobacco dependence: importance of inhibitory capacities. PLoS ONE. (2016) 11:e0150940. doi: 10.1371/journal.pone.0150940
14. Kim-Spoon J, Kahn RE, Lauharatanahirun N, Deater-Deckard K, Bickel WK, Chiu PH, et al. Executive functioning and substance use in adolescence: Neurobiological and behavioral perspectives. Neuropsychologia. (2017) 100:79–92. doi: 10.1016/j.neuropsychologia.2017.04.020
15. Kluwe-Schiavon B, Sanvicente-Vieira B, Viola TW, Moustafa AA. Executive Functioning and Substance Use Disorders. Cognitive, Clinical, and Neural Aspects of Drug Addiction. Oxford: Elsevier (2020). p. 3–20.
16. Zarrindast M-R, Khakpai F. The modulatory role of nicotine on cognitive and non-cognitive functions. Brain Res. (2019) 1710:92–101. doi: 10.1016/j.brainres.2018.12.002
17. Miyake A, Friedman NP. The nature and organization of individual differences in executive functions. Curr Dir Psychol Sci. (2012) 21:8–14. doi: 10.1177/0963721411429458
18. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. (2000) 41:49–100. doi: 10.1006/cogp.1999.0734
19. Berlin I, Singleton EG, Heishman SJ. Validity of the 12-item French version of the tobacco craving questionnaire in treatment-seeking smokers. Nicotine Tob Res. (2010) 12:500–7. doi: 10.1093/ntr/ntq039
20. Fagerstrom KO, Schneider NG. Measuring nicotine dependence: a review of the Fagerstrom Tolerance Questionnaire. J Behav Med. (1989) 12:159–82. doi: 10.1007/BF00846549
21. Golden CJ. Identification of brain disorders by the stroop color and word test. J Clin Psychol. (1976) 32:654–8. doi: 10.1002/1097-4679(197607)32:3<654::AID-JCLP2270320336>3.0.CO;2-Z
22. Burgess PW, Shallice T. Response suppression, initiation and strategy use following frontal lobe lesions. Neuropsychologia. (1996) 34:263–72. doi: 10.1016/0028-3932(95)00104-2
23. Vickers D, Vincent N, Medvedev A. The geometric structure, construction, and interpretation of path-following (trail-making) tests. J Clin Psychol. (1996) 52:651–61. doi: 10.1002/(SICI)1097-4679(199611)52:6<651::AID-JCLP7>3.0.CO;2-N
24. Kirchner WK. Age differences in short-term retention of rapidly changing information. J Exp Psychol. (1958) 55:352–8. doi: 10.1037/h0043688
25. Billieux J, Gay P, Rochat L, Khazaal Y, Zullino D, Van der Linden M. Lack of inhibitory control predicts cigarette smoking dependence: evidence from a non-deprived sample of light to moderate smokers. Drug Alcohol Depend. (2010) 112:164–7. doi: 10.1016/j.drugalcdep.2010.06.006
26. Dougherty DM, Mathias CW, Marsh DM, Jagar AA. Laboratory behavioral measures of impulsivity. Behav Res Methods. (2005) 37:82–90. doi: 10.3758/BF03206401
27. Hu P, Huang L, Zhou S, Shi Q, Xiao D, Wang C. Smoking status and cognitive performance among vocational school students in Beijing, China. Respir Med. (2018) 135:8–11. doi: 10.1016/j.rmed.2017.12.008
29. Bodenburg S, Dopslaff N. The dysexecutive questionnaire advanced. J Nerv Ment Dis. (2008) 196:75–8. doi: 10.1097/NMD.0b013e31815faa2b
30. Schuit E, Panagiotou OA, Munafò MR, Bennett DA, Bergen AW, David SP. Pharmacotherapy for smoking cessation: effects by subgroup defined by genetically informed biomarkers. Cochrane Database Syst Rev. (2017) 2017:CD011823. doi: 10.1002/14651858.CD011823.pub2
31. Husten CG. How should we define light or intermittent smoking? Does it matter? Nicotine Tob Res. (2009) 11:111–21. doi: 10.1093/ntr/ntp010
32. Colby SM, Tiffany ST, Shiffman S, Niaura RS. Measuring nicotine dependence among youth: a review of available approaches and instruments. Drug Alcohol Depend. (2000) 59(Suppl 1):23–39. doi: 10.1016/S0376-8716(99)00163-5
33. Valentine G, Sofuoglu M. Cognitive effects of nicotine: recent progress. Curr Neuropharmacol. (2018) 16:403–14. doi: 10.2174/1570159X15666171103152136
34. López-Torrecillas F. Estrés, afrontamiento, variables de personalidad y consumo de drogas. Granada: Universidad de Granada (1996). Available online at: http://hdl.handle.net/10481/14874
35. Trenerry MR, Crosson B, Deboe J, Leber WR. Visual Search and Attention Test. Odessa: Psychological assessment resources, Inc. (1990).
36. Verdejo-García AJ, Perales JC, Pérez-García M. Cognitive impulsivity in cocaine and heroin polysubstance abusers. Addict Behav. (2007) 32:950–66. doi: 10.1016/j.addbeh.2006.06.032
37. Kirby KN, Petry NM, Bickel WK. Heroin addicts have higher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol. (1999) 128:78–87. doi: 10.1037/0096-3445.128.1.78
38. Myerson J, Green L, Warusawitharana M. Area under the curve as a measure of discounting. J Exp Anal Behav. (2001) 76:235–43. doi: 10.1901/jeab.2001.76-235
39. Bechara A. Decision making, impulse control and loss of willpower to resist drugs: a neurocognitive perspective. Nat Neurosci. (2005) 8:1458–63. doi: 10.1038/nn1584
40. Sedó MA. The five digit test: a color-free non reading alternative to the stroop. Int Neuropsychol Soc Liaison Commit Newsl. (2004) 13:6–7.
41. Cui Y, Robinson JD, Versace F, Lam CY, Minnix JA, Karam-Hage M, et al. Differential cigarette-related startle cue reactivity among light, moderate, and heavy smokers. Addict Behav. (2012) 37:885–9. doi: 10.1016/j.addbeh.2012.02.003
43. Sutherland MT, Ross TJ, Shakleya DM, Huestis MA, Stein EA. Chronic smoking, but not acute nicotine administration, modulates neural correlates of working memory. Psychopharmacology. (2011) 213:29–42. doi: 10.1007/s00213-010-2013-6
44. López-Torrecillas F, Perales JC, Nieto-Ruiz A, Verdejo-García A. Temperament and impulsivity predictors of smoking cessation outcomes. PLoS ONE. (2014) 9:e112440. doi: 10.1371/journal.pone.0112440
45. Cloninger CR. A psychobiological model of temperament and character. Arch Gen Psychiatry. (1993) 50:975. doi: 10.1001/archpsyc.1993.01820240059008
46. González-Roz A, Secades-Villa R, Pericot-Valverde I, Weidberg S, Alonso-Pérez F. Effects of delay discounting and other predictors on smoking relapse. Spanish J Psychol. (2019) 22:E9. doi: 10.1017/sjp.2019.11
47. Sutherland MT, Stein EA. Functional neurocircuits and neuroimaging biomarkers of tobacco use disorder. Trends Mol Med. (2018) 24:129–43. doi: 10.1016/j.molmed.2017.12.002
48. Li Y, Yuan K, Cai C, Feng D, Yin J, Bi Y, et al. Reduced frontal cortical thickness and increased caudate volume within fronto-striatal circuits in young adult smokers. Drug Alcohol Depend. (2015) 151:211–9. doi: 10.1016/j.drugalcdep.2015.03.023
49. Kübler A, Murphy K, Garavan H. Cocaine dependence and attention switching within and between verbal and visuospatial working memory. Eur J Neurosci. (2005) 21:1984–92. doi: 10.1111/j.1460-9568.2005.04027.x
50. Hester R, Garavan H. Neural mechanisms underlying drug-related cue distraction in active cocaine users. Pharmacol Biochem Behav. (2009) 93:270–7. doi: 10.1016/j.pbb.2008.12.009
Keywords: smoking, neuropsychologial assessment, executive function, working memory, tobacco
Citation: Martín Ríos R, López-Torrecillas F and Martín Tamayo I (2021) Executive Functions in Tobacco Use Disorder: New Challenges and Opportunities. Front. Psychiatry 12:586520. doi: 10.3389/fpsyt.2021.586520
Received: 31 August 2020; Accepted: 18 February 2021;
Published: 15 March 2021.
Edited by:
Marc N. Potenza, Yale University, United StatesReviewed by:
Danielle Davis, School of Medicine Yale University, United StatesAnthony Gianni Vaccaro, University of Southern California, United States
Copyright © 2021 Martín Ríos, López-Torrecillas and Martín Tamayo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Martín Ríos, cm1hcnRpeEBjb3JyZW8udWdyLmVz