 Linda Drozdowicz1
Linda Drozdowicz1 Elisabeth Gordon2
Elisabeth Gordon2 Desiree Shapiro3Sansea Jacobson4Isheeta Zalpuri5Colin Stewart6A. Lee Lewis7Lee Robinson8Myo Thwin Myint9Peter Daniolos10Edwin D. Williamson11Richard Pleak12Ana Soledade Graeff Martins13Mary Margaret Gleason14
Desiree Shapiro3Sansea Jacobson4Isheeta Zalpuri5Colin Stewart6A. Lee Lewis7Lee Robinson8Myo Thwin Myint9Peter Daniolos10Edwin D. Williamson11Richard Pleak12Ana Soledade Graeff Martins13Mary Margaret Gleason14 Cathryn A. Galanter15,16Sarah Miller17Dorothy Stubbe1
Cathryn A. Galanter15,16Sarah Miller17Dorothy Stubbe1 Andrés Martin1,18*
Andrés Martin1,18*- 1Child Study Center, Yale School of Medicine, New Haven, CT, United States
- 2Private Practice, New York, NY, United States
- 3University of California, San Diego, San Diego, CA, United States
- 4Western Psychiatric Hospital, Pittsburgh, PA, United States
- 5Stanford University, Palo Alto, CA, United States
- 6Georgetown University, Washington, DC, United States
- 7Medical University of South Carolina, Charleston, SC, United States
- 8Cambridge Health Alliance, Cambridge, MA, United States
- 9Tulane University, New Orleans, LA, United States
- 10University of Iowa, Iowa City, IA, United States
- 11Vanderbilt University Medical Center, Nashville, TN, United States
- 12Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, United States
- 13Federal University of Rio Grande do Sul, Porto Alegre, Brazil
- 14Children's Hospital of the King's Daughters in Virginia, Norfolk, VA, United States
- 15SUNY Downstate Medical Center, Brooklyn, NY, United States
- 16Kings County Hospital Center, Brooklyn, NY, United States
- 17Temple University, Philadelphia, PA, United States
- 18Standardized Patient Program, Teaching and Learning Center, Yale School of Medicine, New Haven, CT, United States
Objective: Matters of sexuality and sexual health are common in the practice of child and adolescent psychiatry (CAP), yet clinicians can feel ill-equipped to address them with confidence. To address this gap in training and practice, we developed, implemented, and evaluated an educational module enhanced by videotaped depictions of expert clinicians interacting with professional actors performing as standardized patients (SPs).
Methods: We developed an educational resource highlighting common issues of sexual health relevant to CAP practice, including sexual development, psychotropic-related side effects, and sexuality in children with autism. We wrote original scripts, based on which two clinicians interacted with three SPs. Digital recordings were edited to yield 5 clips with a cumulative running time of 20 min. The clips were interspersed during a 90-min session comprising didactic and interactive components. Due to the COVID-19 pandemic, we used synchronous videoconferencing, which allowed content dissemination to several training programs across the country.
Results: We recruited 125 learners from 16 CAP training programs through the American Academy of CAP's Alliance for Learning and Innovation (AALI). Routine inquiry into adolescent patients' sexual function was uncommon, reported by only 28% of participants, with “awkward” and “uncomfortable” the most common terms mentioned in reference to the clinical task. The didactic intervention led to measurable improvements after 2 weeks in skills and knowledge (p = 0.004) and in attitudes (p < 0.001). The three items with the greatest improvement were: (a) availability of developmentally tailored resources; (b) comfort in addressing sexual development with underage patients; and (c) with parents or guardians of neuroatypical or developmentally disabled patients (p < 0.001 for each).
Conclusions: A sexual health curriculum enriched by video-based examples can lead to measurable improvement in outcomes pertinent to the clinical practice of CAP. These educational materials are available for distribution, use and adaptation by local instructors. Our study also provides proof-of-principle for the use of multisite educational initiatives in CAP through synchronized videoconferencing.
Introduction
Sexuality is elemental to the human experience and is engaged in throughout life. Sexual health is a critical element of general health. Defined as a state of physical, emotional, mental, and social wellbeing in relation to sexuality, it is not merely the absence of disease, dysfunction, or infirmity. It requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination, or violence (1).
The relationship between sexual health and general health is extensive. At the individual level, sexual well-being is positively correlated to physical and mental health, while at the community level, sexual health is associated with improved relationships, economic stability, and increased education and employment (2–6). In particular, sexual health and mental health are bidirectionally influential: Depression is the largest single comorbidity for sexual dysfunction, and sexual dysfunction is associated with a 2.3- to 3.1-fold increased risk for developing a major depressive disorder (7). In the context of the practice of medicine, the relationship between sexual and general health is further complicated by the potential for many medications, including psychotropics, to induce sexual dysfunction (8).
Since sexual health has great potential to impact and be impacted by other aspects of health, physicians should address and support the sexual health of their patients, even as the majority do not (9–11). One of the most significant reason physicians fail at this task is the lack of sexual health education in medical education (9–13), which trainees and physicians are overtly aware of.
Medical sexual health education is an ethical imperative. This education teaches physicians to address sexual health and therefore not cause harm by passively perpetuating the stigma surrounding sexuality (10); to initiate the discussion instead of placing the burden on the patient to do so, which can unintentionally limit access to care around a stigmatized topic (11); and to be aware of and minimize or mitigate iatrogenic sexual dysfunction (12). It also allows physicians to support larger public health efforts by destigmatizing sexuality and addressing it as an important component of health. Without this education, many physicians experience considerable levels of discomfort in addressing sexual health and sexuality with their patients (13–15).
High quality, medically accurate sex education, particularly when started early and provided additively, supports sexual health as children and adolescents develop. It increases empowerment and confidence during a critical period of physical and emotional growth (16) and reduces unprotected sex, pregnancy, and sexually transmitted infections (17). It also improves rates of sexual satisfaction, a key element of sexual health. Yet, many barriers to comprehensive, medically accurate, evidence-based sex education still persist in the US (18). In this context, child and adolescent psychiatrists (CAPs) have an opportunity and duty to intervene and provide relevant sexual health information to patients and families in order to improve their patients' health.
Sex education is often even less accessible to children and adolescents with special needs (19). Reasons range from simply not being provided, to being offered in a way that is inadequate for the individual's learning style or ability (19). This deficiency can have far-reaching effects. In children with autism spectrum disorder (ASD)—a common population in routine CAP practice—good sex education offers benefits beyond those normally expected in the neurotypical population. It provides sexual information directly relevant to physical health, such as how and when to clean one's genitals, menstrual hygiene, and when to seek medical attention—including for sexual symptoms such as loss of libido/desire, erectile dysfunction, or anorgasmia, among others (20). It can help curb the increased risk of sexual victimization for people with ASD (21), and it can also help prevent problematic sexual behaviors, such as public masturbation and unwanted touching, which can have major legal and social ramifications (22).
Moreover, sex education for children and adolescents with ASD or any disability should not be limited to physical health and safety information. Contrary to common assumptions, many people with ASD desire romantic and sexual relationships (23). All children and adolescents deserve and are entitled to the same sexual health education, with the content curated for and presented in a way that is understandable to each individual (23). For those with ASD, this includes concrete teaching about relationships, courtship, and other social skills needed for success—topics that might be picked up from peers in children without ASD, but that may be missed in this population (20).
With this background in mind, we developed, deployed, and evaluated a sexual health educational module specific to the training needs of CAPs. We enhanced our didactic materials with video-based depictions of expert clinicians interacting with professional actors. Due to the COVID-19 pandemic, we provided the training via synchronous videoconferencing, an approach that permitted simultaneous sharing of educational content with several training programs across the country.
Methods
Participants and Synchronized Videoconferencing Delivery
Participants comprised CAP faculty, fellows, and residents at Yale and those recruited through the American Academy of Child and Adolescent Psychiatry's Alliance for Learning and Innovation (AALI). Against the backdrop of the COVID-19 pandemic, the didactic was offered exclusively online, using the videoconferencing platform Zoom (San Jose, CA). This approach permitted the course to be offered virtually with synchronous content delivery and real-time interaction between faculty and learners.
Educational Intervention
We developed the didactic portion of the curriculum under the lead of a psychiatrist with expertise in sex therapy and a CAP with training through NYU's Training Program in Human Sexuality, and with the input of several CAP training directors. We incorporated published recommendations from the Summit on Medical School Education in Sexual Health (24), the needs identified for graduate medical education in sexual health (25), and sexuality matters that are specific to children and adolescents with autism (26–28). For the didactics, we provided basic background education in sexual health, as well as a curated resource list. We focused extensively on those issues of sexual development, health, and management relevant to CAPs. We specifically included information in the didactics on how to address common sexual health issues with patients and their families. The didactics were divided into five parts: (1) Sexual health and sexual development: why it matters and what is normal in childhood; (2) Talking about sexual development in children with autism; (3) Normal sexual development in adolescence, pornography, and “porn literacy;” (4) The management of medication-induced sexual dysfunction; and (5) Special sexuality considerations with autism during adolescence.
To support this content, we developed scripts highlighting common issues of sexuality relevant to CAP, including psychotropic-related side effects and sexuality in children with autism. We made digital recordings of two clinicians interacting with three professional actors, yielding 5 video clips with a cumulative running time of 20 min. The mother in the first scenario, and the adolescent son and his father in the second, are all professional actors hired through the Standardized Patient Program of the Yale School of Medicine's Teaching and Learning Center. The actors are experienced in medical settings and followed standardized patient (SP) best practices (29). The clips outlined in Table 1 were interspersed during a 90-min session comprising didactic and interactive components. We provided a handout with more detail on all didactic components, which also helped accommodate different learning styles. The five video clips and reference handout are included as Supplementary Materials.
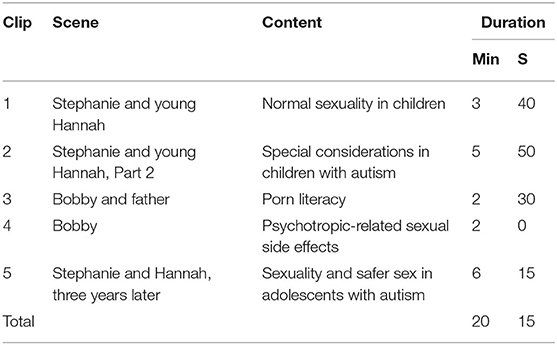
Table 1. Video clips for child and adolescent psychiatry sexual health didactic resource.
Outcome Measures
Participants provided demographic information and repeated a survey at baseline and endpoint. At baseline we asked them to provide the first three words or short phrases “that come to mind when discussing sexuality with your adolescent patients” and the three “when discussing sexuality with their parent(s) or guardian(s).” We adapted the Physician Belief Scale (30) and the Patient-Practitioner Orientation Scale (9) into a 20-item questionnaire tailored to the practice of CAPs. The resulting survey tapped into two common domains in training and education, though is not to be construed as a formal assessment of either: (1) Skills and Knowledge, for which respondents indicated how strongly they agree or disagree with 9 statements using a five-point Likert scale; and (2) Attitudes, a list of 11 statements similarly coded. Some of the items were reverse-coded to prevent response acquiescence bias.
Ethics Approval
Before starting data collection, we obtained institutional review board approval from the Yale Human Investigations Committee (Protocol # 2000027918). The study was deemed exempt, with completion of the survey representing tacit consent. Learners were encouraged to participate, but informed that their responses were neither mandatory nor relevant to their performance evaluation. They were notified that results of the surveys would not be accessible to faculty responsible for their assessment. In order to track individuals' responses over time, each participant provided a de-identified and anonymous study code.
Data Collection and Statistical Analysis
Participants completed surveys through their preferred, WiFi-enabled personal devices during dedicated time on two dates in May and June 2020. We collected information securely through Qualtrics (Provo, UT), and analyzed data using SPSS version 25 (Armonk, NY).
We compared differences before and after the didactic intervention using paired-t-tests and Cohen's d effect sizes for continuous variables (global scores on Skills and Knowledge, and on Attitudes). We next compared the survey's 20 individual items using chi square-tests for the 20 categorical items, relying on McNemar's-test to examine changes before and after the intervention. McNemar's-test was used to determine differences on a dichotomous dependent variable between two related groups, and is commonly used to analyze pre-post study designs (31). Finally, we used word cloud generator software (wordclouds.com; Zygomatic Inc., Vianen, The Netherlands) to visually depict students' word choices at baseline.
Results
We approached 20 training programs associated with the AALI network; 15 agreed to participate in one of the dates offered (14 in the US, one in Brazil). Two hundred and nine learners participated in one of the two sessions, and 166 of them (80%) consented to participate and completed the baseline assessment. Some of these learners did not complete the endpoint survey (n = 23) or failed to provide a matching unique identifier (n = 18). This resulted in a final working sample of 125 participants, yielding a total usable completion rate of 75% (125/143). We compared baseline demographic characteristics between endpoint survey completers (n = 125) and non-completers (n = 41). Finding no differences (p > 0.05 for all contrasts), we restricted analyses to the completer group.
Table 2 summarizes characteristics of these 125 participants and their clinical practice routines regarding sexual health. There was a weak correlation between the overall composite score and years in clinical practice (r = 0.3, p = 0.01), but not with self-rated views on sexuality. Of note, over two thirds of participants acknowledged inquiring about sexual health only “occasionally,” “rarely,” or “never.” Safer sex practices, sexual activity, pregnancy prevention, and sexually transmitted infections were more commonly addressed than masturbation or specific sexual dysfunctions. Addressing patients' sexual activity with parents or guardians was challenging, particularly for patients who are neuro-atypical or have developmental delays. Figure 1 provides a visual depiction of participants' perceptions on addressing sexuality with their patients and guardians, with “awkward” and “uncomfortable” leading the way.
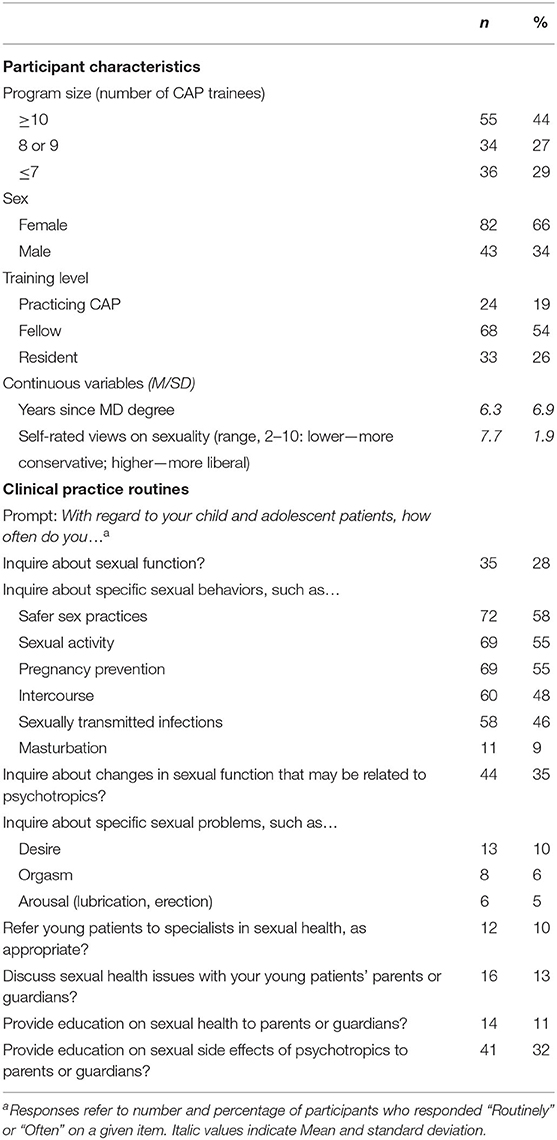
Table 2. Descriptive characteristics and clinical practice routines of study participants (n = 125).
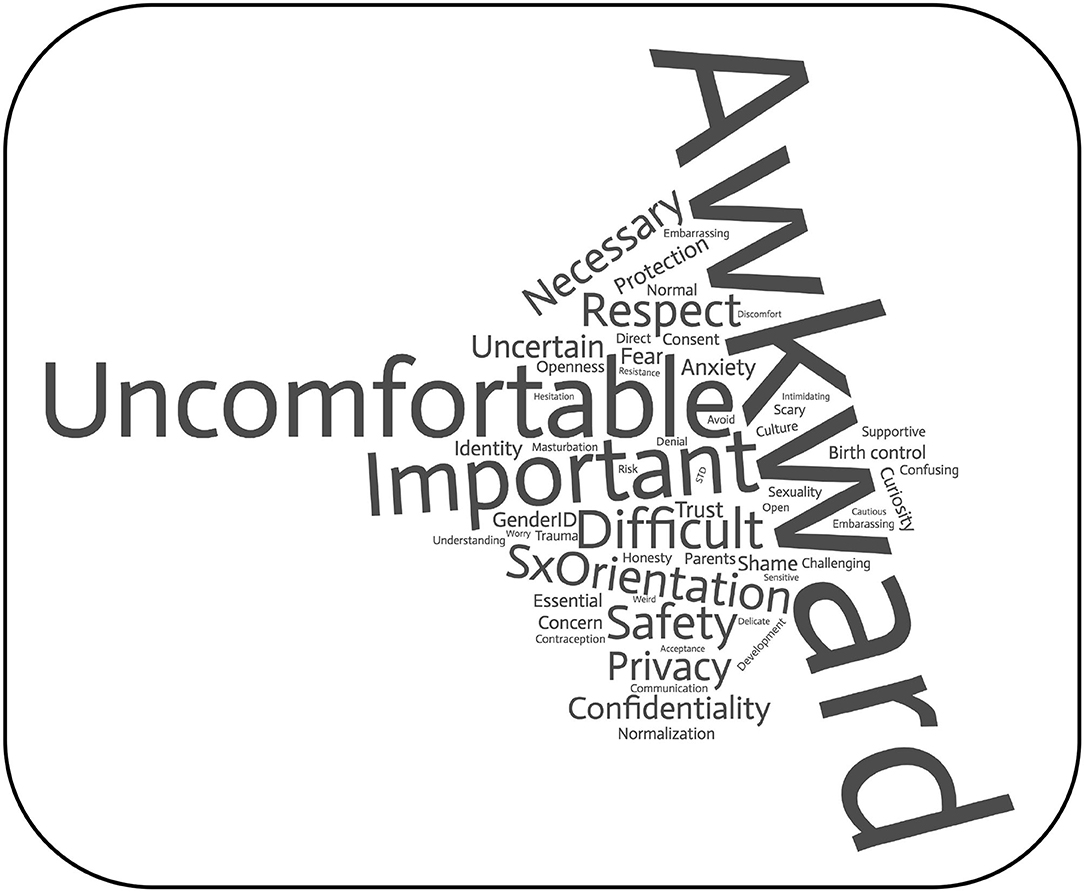
Figure 1. Word cloud based on the prompt “please list words or short phrases that come to mind when discussing sexuality with your adolescent patients [3 words] and/or their parents” [3 words]. n = 628 entries, comprising 58 words with 4 or more occurrences each.
The didactic intervention led to measurable improvements after 2 weeks in Skills and Knowledge (p = 0.004), Attitudes (p < 0.001), and in the overall composite score (p < 0.001; Table 3). Although statistically and clinically significant, effect sizes were small (Cohen's d ≤ 0.35). In order to better understand the specific components driving these changes, we conducted a secondary item-level analysis. Table 4 summarizes these findings, rank ordered by the degree of change from baseline to endpoint. The three items with the greatest improvement were: (a) Availability of developmentally tailored resources; (b) Comfort in addressing sexual development with underage patients; and (c) with parents or guardians of neuroatypical or developmentally disabled patients (p < 0.001 for each).
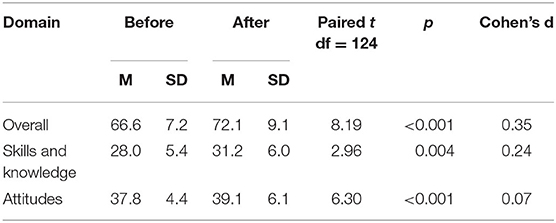
Table 3. Outcome change after didactic intervention: sexual health skills and attitudes in child and adolescent psychiatry practice (n = 125).
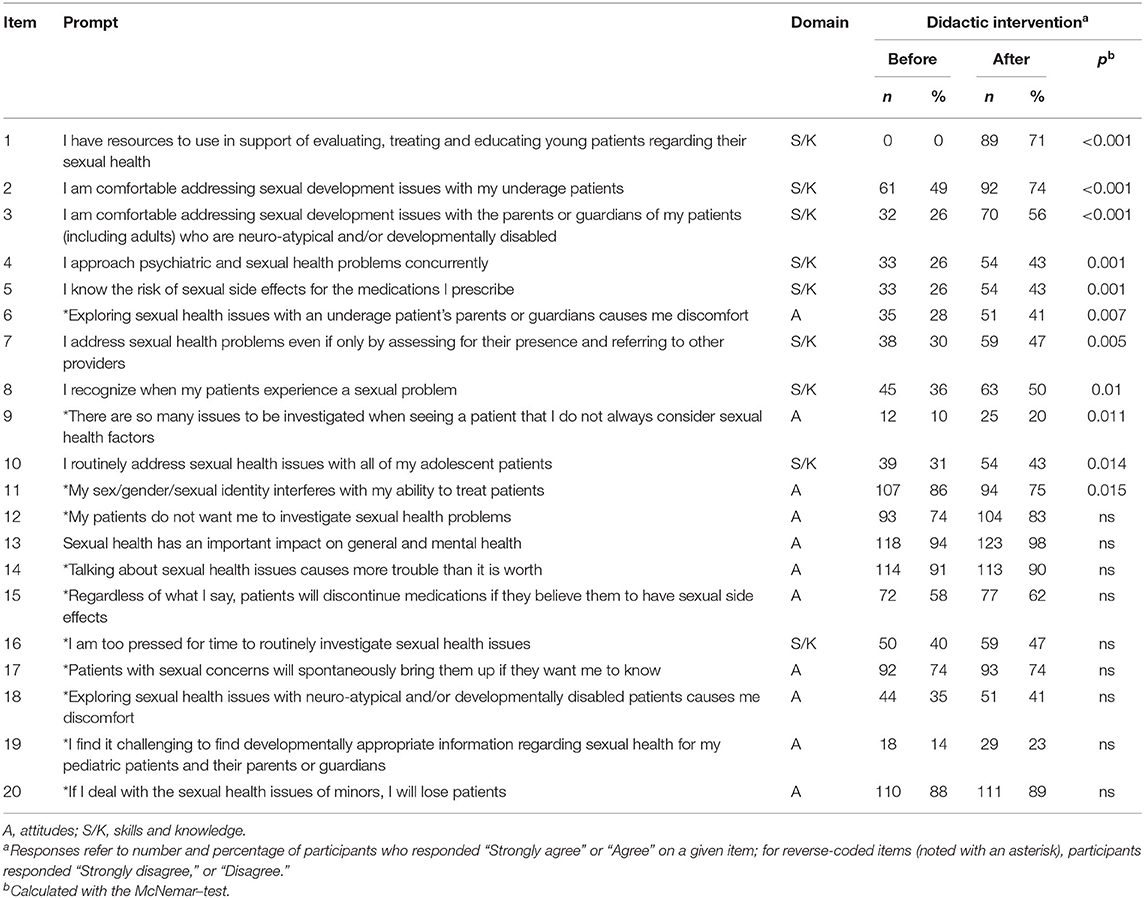
Table 4. Item analysis: sexual health skills and attitudes in child and adolescent psychiatry practice (n = 125).
The session was rated highly on a five-point Likert scale (4.6 +/− 0.7; Table 5. Finally, 116 participants (93%) provided responses to our optional question about the session in general, and about its video-based component in particular. Comments were generally positive, with representative verbatim quotes including the following: “We were very impressed by the quality of the talk, the videos were amazing for our modeling on how to approach sexual issues. I am very glad that we could take part in this class and hope we can keep participating in the future;” “This online multisite approach is a unique and effective contribution to training, particularly given the recent pandemic. Thank you for including our program;” and “The video interactions were particularly helpful in making the concepts ‘come alive' and providing actionable clinical examples to emulate and learn from: I will for sure be using your ‘electric/mechanical/plumbing' analogies [which refer to arousal/erection//ejaculation] in my own practice, and for that I thank you.” There were over a dozen requests to make the teaching materials available, including this representative one: “Videos were great, and it would be useful to have access to them along with a facilitator's guide [a la NNCI (National Neuroscience Curriculum Initiative)], so programs could develop their own seminars based off of this one.” There were several suggestions for future enhancements, most consistently the use of small break-out groups to increase interactivity. The use of synchronized videoconferencing had the lowest rating on the session evaluation, and the poor phrasing of our question may have introduced too high a threshold to overcome, as we inquired about “Zoom contributing to or enhancing the training in some way.” Despite this, ratings were still on average above 4 (“somewhat agree”), and textual comments were largely positive, noting more of its advantages, particularly the opportunity to interact with learners across institutions: “Loved having multiple sites; think this is great early move toward harnessing this technology.”
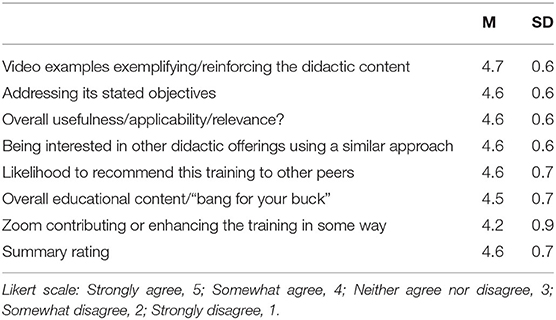
Table 5. Session evaluation (n = 125).
Discussion
This study was designed to examine: (1) a specialized educational resource on sexual health and its impact on learners' knowledge, skills, and attitudes; (2) the use of videotaped depictions of clinical interactions to complement the module's content; and (3) the deployment of educational content through a multisite initiative using synchronized videoconferencing. The results of our study support the utility of each of the three components.
Sex Ed 201: An Educational Resource Tailored for Child and Adolescent Psychiatrists
In keeping with experiences reported in the medical education literature in medicine (9–13), including psychiatry (32, 33), the CAP participants in our study felt uneasy and insufficiently prepared to address issues of sexuality in their clinical practice. Although realizing how “important” and “necessary” the topic was, they almost universally felt “awkward” or “uncomfortable” in broaching it directly with patients and families. We found that a one-time education session of 90 min led to improvements in knowledge, skills and attitudes measurable after 2 weeks.
We developed the education module mindful of the specialty's specific needs, and in particular that of presenting information in an appropriate way to children and adolescents of different ages and developmental needs, and with their parents or guardians as clinically indicated. We found wide variability in clinicians' prior knowledge and education regarding sexual health, and inconsistency in the resources available to them. Indeed, we found particular improvement after the training on concrete knowledge about the availability of developmentally tailored materials, including books, websites, trainings, and others such as those we curated. This finding highlights the need to incorporate easily accessible and up to date resources into sexual health curricula to the extent possible. This is especially relevant for CAPs, who routinely interface with children, adolescents and adults with a broad array of age, language abilities, and developmental differences. We emphasized that addressing sexual health is important for all child and adolescent patients, no matter what diagnosis or (dis)ability they may have, but given time constraints, chose to provide more in-depth education on only one diagnosis. We decided on and incorporated autism-specific content given the growing (and overdue) attention to the importance of sexual health among youth and young adults on the autism spectrum (28, 34).
The CAP training competencies, as outlined by the American Board of Psychiatry and Neurology (35) and by the Accreditation Council for Graduate Medical Education's program requirements (36) include several aspects relevant to sexuality, including among others: psychosexual development, disorders of sexual development, sexual abuse, and sexual orientation. However, sexual function, sexual health, and common sexual dysfunctions tend to be sparely addressed, when addressed at all. There are no clear parameters on what a comprehensive curriculum would entail, or how it could be incorporated into an already overflowing set of training requirements. Moreover, there is a dearth of CAP educators appropriately trained in sexual health. To that end, our initiative provides a concrete step toward greater standardization in education and training (37), as well as material that can be incorporated and adapted “off the shelf” by end users who may otherwise not have ready access to content experts.
Making It Real: Incorporating Simulation With Standardized Patients Into CAP
Simulation with SPs offers learners an opportunity to gain exposure to a wide range of patients and clinical scenarios, and to practice and refine clinical skills in a safe and supportive environment (38). Although widely used in undergraduate medical education, simulation-based training in post-graduate psychiatric training is considerably more limited (39–41). SP use in CAP training is virtually non-existent, partly because of the additional practical, legal, and ethical considerations inherent to working with underage actors (42). Still, there are several informative examples of simulation-based psychiatric training using SPs in other fields. For example, performance on adolescent suicide risk assessment among residents in pediatrics objectively improved after using an SP-based learning module (43).
By incorporating videotaped depictions of experienced clinicians interacting with SPs, we were able to offer realistic portrayals of encounters likely to be faced by CAPs in their clinical practice. Learners were able to see the techniques and actual words used to demystify sexual health and turn it into a routine part of outpatient visits. In an ideal setting, learners would be able to practice these skills during face-to-face interactions with SPs. However, such an approach would be logistically taxing, particularly for as many participants and given the challenges to provide SPs around as many sites with varying levels of local resources and expertise. Instead, the availability of enduring learning materials such as ours allows for a series of consistent and standardized stimuli, which can then be adapted locally and incorporated into practice by individual learners or training programs.
We consider that the availability of such resources, especially if part of broader materials, could strengthen learning opportunities across the discipline. For example, curated content incorporating SP depictions could be useful to ensure consistent training across training sites, regardless of their size or local resources. Aspects of clinical practice with high public health impact and limited local expertise (such as adolescent substance abuse) could be natural topics to consider as next steps. The challenges to incorporate underage SPs notwithstanding, we are committed to expanding simulation in CAP. We are not alone in seeing the potential that could be unleashed: “The ability of mental health simulation to bridge the gap between education and clinical practice, alongside its potential for interprofessional education and initial evidence supporting its effectiveness, merit its inclusion as a key educational tool in providing better care for mental health needs…Mental health simulation is poised to have a positive effect should the necessary support, funding, and progressive thinking be applied” (44).
The Zoom Where It Happens: Leveraging a New Technology to Enhance CAP Training
The timing of our scheduled training session vis-á-vis the COVID-19 pandemic forced us to move from what had initially been designed as a single site initiative to one that incorporated 15 peer institutions. Were it not for the pandemic, it is unlikely that we would have conceptualized this effort as one delivered through synchronous videoconferencing. The approach provided several unique advantages: a broader reach in the number and geographic extraction of participants; training consistency across sites; interaction in real time with content experts and fellow learners; and logistic ease in securing curricular content and experienced faculty. Our resort to this means of content delivery is not new (45), and we are in good company with other medical specialties that adapted rapidly to the limitations brought on by the pandemic [e.g., (46)].
Apart from those aspects of sexual health we set out to study, we consider this report a proof of principle for a novel education model in CAP. The combination of a secure virtual platform for synchronous videoconferencing, and the recruitment reach available through a network such as AALI, together offer entirely new opportunities. Given the relatively small size of the field, and the limited number of faculty experienced in a range of subspecialized topics, we believe that CAP could stand to benefit from similar efforts focused on strategic content areas.
Limitations
We recognize several limitations to our study. First, our sample was modest in size and varied in its characteristics, which may limit its representativeness and generalizability to other training programs within, and particularly outside of the US; second, we recognize the possibility of a social desirability bias: learners may have answered the surveys more favorably at the second time point; third, we did not have a control group, such as of learners exposed to the lecture content but not to the videos, which could have helped identify active components of the intervention; fourth, we recognize that even as we measured changes in attitudes and knowledge 2 weeks after the intervention, we do not know whether effects will prove to be durable, or whether they will translate into actual clinical practice. A single exposure may not be sufficient to have an enduring effect; a spiral curriculum could be beneficial, wherein repeat encounters with sexual health content as relevant to CAP would reinforce previous learning. Compounding these measurement limitations is the fact that our primary outcome measure is a practical adaptation that does not have the strong empirical validation and support we would have optimally worked with. Finally, in harnessing Zoom at the early stages of the pandemic, we had much to learn. As aptly noted by one of the participants: “We have miles to go before we sleep regarding taking optimal advantage of this approach, which we absolutely should.” In particular, future iterations of this approach should carefully balance how best to incorporate interactive components, including optimal use of break-out rooms.
In summary, our study shows that a sexual health curriculum enriched by video-based examples can lead to measurable improvement in outcomes pertinent to the clinical practice of CAP. These educational materials are available for distribution, use and adaptation by local instructors. Our study also provides proof-of-principle for the use of multisite educational initiatives through synchronized videoconferencing.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
This study was approved by The Yale Human Investigations Committee (Protocol # 2000027918). It was deemed exempt, with survey completion standing for tacit consent. Written informed consent was not required for this study, in accordance with national legislation and institutional requirements.
Author Contributions
LD and EG designed the sexual health curriculum and wrote the scripts. LD, EG, and AM worked with standardized patients in developing the videotaped depictions, designed the study, and drafted the first version of the manuscript. AM took the lead in analyzing the data and is responsible for the integrity of the data and analyses. All authors recruited learners at their respective training sites and participated in the education module, reviewed and contributed to working drafts, and approved the final, submitted version.
Funding
Supported by the Riva Ariella Ritvo Endowment at Child Study Center, Yale School of Medicine, and by NIMH R25 MH077823, Research Education for Future Physician-Scientists in Child Psychiatry.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We appreciate the professional actors' contributions and the learners' engaged participation. We are grateful to Barbara Hildebrand of the Standardized Patient Program, Teaching and Learning Center, and Zsofia Leranth-Nagy of the Youth Standardized Patient Program, Child Study Center, Yale School of Medicine.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.593101/full#supplementary-material
References
1. WHO. Defining Sexual Health. WHO. (2002). Available online at: https://www.who.int/reproductivehealth/publications/sexual_health/defining_sh/en/ (accessed July 6, 2020).
2. Office of the Surgeon General (US), Office of Population Affairs (US). The Surgeon General's Call to Action to Promote Sexual Health and Responsible Sexual Behavior. Rockville, MD: Office of the Surgeon General (2001). (Publications and Reports of the Surgeon General). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK44216/ (accessed July 6, 2020).
3. Hogben M, Ford J, Becasen JS, Brown KF. A systematic review of sexual health interventions for adults: narrative evidence. J Sex Res. (2015) 52:444–69. doi: 10.1080/00224499.2014.973100
4. Information NC for B, Pike USNL of M 8600 R, MD B, USA 20894. Sexual health interventions: a meta-analysis. Database of Abstracts of Reviews of Effects (DARE): Quality-assessed Reviews. Centre for Reviews and Dissemination (2014). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK292511/ (accessed July 26, 2020).
5. Ford JV, Ivankovich MB, Douglas JM, Hook EW, Barclay L, Elders J, et al. The need to promote sexual health in America: a new vision for public health action. Sex Transm Dis. (2017) 44:579–85. doi: 10.1097/OLQ.0000000000000660
6. Swartzendruber A, Zenilman JM. A national strategy to improve sexual health. JAMA. (2010)304:1005–6. doi: 10.1001/jama.2010.1252
7. Atlantis E, Sullivan T. Bidirectional association between depression and sexual dysfunction: a systematic review and meta-analysis. J Sex Med. (2012) 9:1497–507. doi: 10.1111/j.1743-6109.2012.02709.x
8. Ishak W, editor. The Textbook of Clinical Sexual Medicine. Springer International Publishing (2017). p. 347–9 (Evaluation and treatment of substance-/medication-induced sexual dysfunction). Available online at: https://www.springer.com/gp/book/9783319525389 (accessed August 8, 2020).
9. Tsimtsiou Z, Hatzimouratidis K, Nakopoulou E, Kyrana E, Salpigidis G, Hatzichristou D. Original research—education: predictors of physicians' involvement in addressing sexual health issues. J Sex Med. (2006) 3:583–8. doi: 10.1111/j.1743-6109.2006.00271.x
10. Merrill J, Laux L, Thornby J. Why doctors have difficulty with sex histories. South Med J. (1990) 83:613–7. doi: 10.1097/00007611-199006000-00004
11. Rubin ES, Rullo J, Tsai P, Criniti S, Elders J, Thielen JM, et al. Best practices in North American pre-clinical medical education in sexual history taking: consensus from the summits in medical education in sexual health. J Sex Med. (2018) 15:1414–25. doi: 10.1016/j.jsxm.2018.08.008
12. Faulder GS, Riley SC, Stone N, Glasier A. Teaching sex education improves medical students' confidence in dealing with sexual health issues. Contraception. (2004) 70:135–9. doi: 10.1016/j.contraception.2004.03.010
13. Shindel AW, Baazeem A, Eardley I, Coleman E. Sexual health in undergraduate medical education: existing and future needs and platforms. J Sex Med. (2016) 13:1013–26. doi: 10.1016/j.jsxm.2016.04.069
14. Skelton JR, Matthews PM. Teaching sexual history taking to health care professionals in primary care. Med Educ. (2001) 35:603–8. doi: 10.1046/j.1365-2923.2001.00926.x
15. Shindel AW, Ando KA, Nelson CJ, Breyer BN, Lue TF, Smith JF. Medical student sexuality: how sexual experience and sexuality training impact U.S. and Canadian medical students' comfort in dealing with patients' sexuality in clinical practice. Acad Med. (2010) 85:1321–30. doi: 10.1097/ACM.0b013e3181e6c4a0
16. Goldman JDG. An exploration in health education of an integrated theoretical basis for sexuality education pedagogies for young people. Health Educ Res. (2011) 26:526–41. doi: 10.1093/her/cyq084
17. Chin HB, Sipe TA, Elder R, Mercer SL, Chattopadhyay SK, Jacob V, et al. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: two systematic reviews for the Guide to Community Preventive Services. Am J Prev Med. (2012) 42:272–94. doi: 10.1016/j.amepre.2011.11.006
18. Hall KS, Sales JM, Komro KA, Santelli J. The state of sex education in the United States. J Adolesc Health. (2016) 58:595–7. doi: 10.1016/j.jadohealth.2016.03.032
19. Holland-Hall C, Quint EH. Sexuality and disability in adolescents. Pediatr Clin North Am. (2017) 64:435–49. doi: 10.1016/j.pcl.2016.11.011
20. Loftin R. Sex education, sexual health, and autism spectrum disorder. Pediatr Ther. (2015) 5:1. doi: 10.4172/2161-0665.1000230
21. Brown-Lavoie SM, Viecili MA, Weiss JA. Sexual knowledge and victimization in adults with autism spectrum disorders. J Autism Dev Disord. (2014) 44:2185. doi: 10.1007/s10803-014-2093-y
22. Gill M. Sex can wait, masturbate: the politics of masturbation training. Sexualities. (2012) 15:472–93. doi: 10.1177/1363460712439655
23. Murphy NA, Elias ER. Sexuality of children and adolescents with developmental disabilities. Pediatrics. (2006) 118:398–403. doi: 10.1542/peds.2006-1115
24. University of Minnesota Program in Human Sexuality. Summit on Medical School Education in Sexual Health, Papers. Program in Human Sexuality, University of Minnesota (2018). Available online at: https://www.sexualhealth.umn.edu/education-and-training/summit-medical-school-education-sexual-health/papers (accessed August 3, 2020).
25. Parish SJ, Clayton AH. Continuing medical education: sexual medicine education: review and commentary (CME). J Sex Med. (2007) 4:259–68. doi: 10.1111/j.1743-6109.2007.00430.x
26. Chan J, John RM. Sexuality and sexual health in children and adolescents with autism. J Nurse Pract. 8:306–15. doi: 10.1016/j.nurpra.2012.01.020
27. Lehan Mackin M, Loew N, Gonzalez A, Tykol H, Christensen T. Parent perceptions of sexual education needs for their children with autism. J Pediatr Nurs. (2016) 31:608–18. doi: 10.1016/j.pedn.2016.07.003
28. Pugliese CE, Ratto AB, Granader Y, Dudley KM, Bowen A, Baker C, et al. Feasibility and preliminary efficacy of a parent-mediated sexual education curriculum for youth with autism spectrum disorders. Autism. (2020) 24:64–79. doi: 10.1177/1362361319842978
29. Lewis KL, Bohnert CA, Gammon WL, Hölzer H, Lyman L, Smith C, et al. The association of standardized patient educators (ASPE) standards of best practice (SOBP). Adv Simul. (2017) 2:10. doi: 10.1186/s41077-017-0043-4
30. Ashworth CD, Williamson P, Montano D. A scale to measure physician beliefs about psychosocial aspects of patient care. Soc Sci Med. (1984) 19:1235–8. doi: 10.1016/0277-9536(84)90376-9
31. Adedokun OA, Burgess WD. Analysis of paired dichotomous data: a gentle introduction to the McNemar test in SPSS. J MultiDisc Eval. (2011) 8:125–31. Available online at: https://journals.sfu.ca/jmde/index.php/jmde_1/article/view/336 (accessed October 21, 2020).
32. Rele K, Wylie K. Management of psychosexual and relationship problems in general mental health services by psychiatry trainees. Int J Clin Pract. (2007) 61:1701–4. doi: 10.1111/j.1742-1241.2007.01455.x
33. Hegde D, Sreedaran P, Pradeep J. Challenges in taking sexual history: a qualitative study of Indian postgraduate psychiatry trainees. Indian J Psychol Med. (2018) 40:356–63. doi: 10.4103/IJPSYM.IJPSYM_64_18
34. Cheak-Zamora NC, Teti M, Maurer-Batjer A, O'Connor KV, Randolph JK. Sexual and relationship interest, knowledge, and experiences among adolescents and young adults with autism spectrum disorder. Arch Sex Behav. (2019) 48:2605–15. doi: 10.1007/s10508-019-1445-2
35. American Board of Psychiatry and Neurology. Child and Adolescent Psychiatry Core Competencies Outline. (2011). Available online at: https://www.abpn.com/wp-content/uploads/2015/02/2011_core_CAP_MREE.pdf (accessed August 2, 2020).
36. Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Child and Adolescent Psychiatry. (2020). Available online at: https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/405_ChildAdolescentPsychiatry_2020_TCC.pdf?ver=2020-06-19-130559-823 (accessed August 2, 2020).
37. Jannini EA, Reisman Y. Medicine without sexual medicine is not medicine: an MJCSM and ESSM petition on sexual health to the political and university authorities. J Sex Med. (2019) 16:943–5. doi: 10.1016/j.jsxm.2019.04.001
38. Rosen KR. The history of medical simulation. J Crit Care. (2008) 23:157–66. doi: 10.1016/j.jcrc.2007.12.004
39. Brenner AM. Uses and limitations of simulated patients in psychiatric education. Acad Psychiatry. (2009) 33:112–9. doi: 10.1176/appi.ap.33.2.112
40. Hodges BD, Hollenberg E, McNaughton N, Hanson MD, Regehr G. The psychiatry OSCE: a 20-year retrospective. Acad Psychiatry. (2014) 38:26–34. doi: 10.1007/s40596-013-0012-8
41. Plakiotis C. Objective structured clinical examination (OSCE) in psychiatry education: a review of its role in competency-based assessment. Adv Exp Med Biol. (2017) 988:159–80. doi: 10.1007/978-3-319-56246-9_13
42. Budd N, Andersen P, Harrison P, Prowse N. Engaging children as simulated patients in healthcare education. Simul Healthc. (2020) 15:199–204. doi: 10.1097/SIH.0000000000000452
43. Fallucco EM, Hanson MD, Glowinski AL. Teaching pediatric residents to assess adolescent suicide risk with a standardized patient module. Pediatrics. (2010) 125:953–9. doi: 10.1542/peds.2009-2135
44. Attoe C, Kowalski C, Fernando A, Cross S. Integrating mental health simulation into routine health-care education. Lancet Psychiatry. (2016) 3:702–3. doi: 10.1016/S2215-0366(16)30100-6
45. Chipps J, Brysiewicz P, Mars M. A systematic review of the effectiveness of videoconference-based tele-education for medical and nursing education. Worldviews Evid Based Nurs. (2012) 9:78–87. doi: 10.1111/j.1741-6787.2012.00241.x
Keywords: child and adolescence psychiatry, sexual education, standardized patient, simulation, training and education
Citation: Drozdowicz L, Gordon E, Shapiro D, Jacobson S, Zalpuri I, Stewart C, Lewis AL, Robinson L, Myint MT, Daniolos P, Williamson ED, Pleak R, Graeff Martins AS, Gleason MM, Galanter CA, Miller S, Stubbe D and Martin A (2020) Sexual Health in Child and Adolescent Psychiatry: Multi-Site Implementation Through Synchronized Videoconferencing of an Educational Resource Using Standardized Patients. Front. Psychiatry 11:593101. doi: 10.3389/fpsyt.2020.593101
Received: 10 August 2020; Accepted: 05 October 2020;
Published: 17 November 2020.
Edited by:
Hector Wing Hong Tsang, Hong Kong Polytechnic University, Hong KongReviewed by:
Devashish Konar, Mental Health Care Centre, IndiaBhing-Leet Tan, Singapore Institute of Technology, Singapore
Copyright © 2020 Drozdowicz, Gordon, Shapiro, Jacobson, Zalpuri, Stewart, Lewis, Robinson, Myint, Daniolos, Williamson, Pleak, Graeff Martins, Gleason, Galanter, Miller, Stubbe and Martin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrés Martin, YW5kcmVzLm1hcnRpbkB5YWxlLmVkdQ==