 Kim van der Linden
Kim van der Linden Claudia Simons
Claudia Simons Thérèse van Amelsvoort
Thérèse van Amelsvoort Machteld Marcelis
Machteld Marcelis- 1GGzE, Mental Healthcare Institution Eindhoven, Eindhoven, Netherlands
- 2Department of Psychiatry and Neuropsychology, School for Mental Health and Neuroscience (MHeNS), Maastricht University, Maastricht, Netherlands
Background: Existing research shows that adults with an autism spectrum disorder (ASD) are more vulnerable to develop overt psychosis. However, studies investigating (subclinical) psychotic experiences (PE) in ASD are scarce, and it is unknown if PE are accompanied with more distress in adults with ASD compared to the general population. This study examined lifetime PE and accompanying distress, momentary PE levels, and the impact of daily life stress and negative affect (NA) on momentary PE in males and females with ASD compared to controls.
Methods: In 50 adults with ASD (males N= 26, females N= 24) and 51 adults without ASD (males N= 26, females N= 25), the Community Assessment of Psychic Experiences (CAPE) was used to analyze group differences in frequency and distress of lifetime subclinical positive, negative, and depressive symptoms. The Experience Sampling Method (ESM) was used to measure momentary PE, NA, and stress (activity-related, event-related, and social stress) for 10 days. Multilevel analyses were conducted to test whether stress and NA were associated with momentary PE and whether these associations were modified by group or sex.
Results: Adults with ASD reported more lifetime CAPE negative and depressive symptoms, but similar levels of PE, than controls. Higher levels of accompanying distress were found in participants with ASD for each subscale. With respect to ESM momentary PE, higher levels were reported by adults with ASD and a stronger association between event-related stress and momentary PE was found compared to controls. This was not the case for NA, activity-related, and social stress. Overall, no significant differences between male and female outcomes were found.
Conclusion: Adults with ASD are more prone to encounter lifetime subclinical negative and depressive symptoms and accompanying distress compared to adults without ASD. Similar levels of lifetime PE in both groups were still accompanied with more distress in the ASD group. Furthermore, higher levels of ESM momentary PE were found in participants with ASD. Additionally, event-related stress may act as a risk factor for PE in both females and males with ASD, with a stronger risk-increasing effect than in their control counterparts.
Introduction
Individuals with an autism spectrum disorder (ASD) are more prone to develop overt psychosis relative to those without ASD (1, 2). General population studies have shown that psychotic experiences (PE) are an important risk factor for a psychotic disorder (3, 4), psychopathology (5, 6), and suicidal ideation (7, 8). Still, studies investigating PE in ASD are limited with an inconsistent pattern of results. For example, while two studies found significant associations between childhood autistic traits and PE in adolescence (9, 10), Taylor et al. (11) demonstrated weak or non-significant associations. Given that PE may lead to more severe psychopathology, it is essential to enhance knowledge about its (risk for) occurrence in ASD. Identifying sex differences may be necessary for understanding the underlying mechanisms of PE in ASD, which can lead to effective prevention and better-tailored treatment. Previous studies in general population samples demonstrated significantly higher levels of PE in females than in males (12, 13). However, we only found one study in children with ASD, which showed that 57% of girls with ASD experienced schizophrenia spectrum traits compared with 28% of boys (14).
Stress is a well-known risk factor in the emergence of psychosis. Individuals who have experienced childhood adversity, trauma, or adverse life events have an increased risk of developing subclinical PE (15–20) or a psychotic disorder (21–23). In the last two decades, there has been increased interest in studying the influence of minor daily stressors on momentary PE, also known as psychotic reactivity (24, 25). A widely used method to investigate psychotic reactivity is the Experience Sampling Method (ESM). The ESM is an ecological momentary assessment (EMA) tool to gather information from participants about their experiences in the context of the natural flow of daily life. Typically, multiple times a day, short questionnaires are presented to participants at semi-random moments in time over several consecutive days. This method is less susceptible to recall bias and has been applied to a wide range of psychiatric disorders (26). Although ESM research in ASD is still limited, the feasibility and usefulness of this method have been supported (27–29). Previous ESM studies observed an increased psychotic reactivity in patients at increased risk for psychosis compared with controls (30, 31). Currently, the interplay between stress and momentary PE in ASD has not yet been investigated. However, in another paper on this sample, we reported an increased negative affect (NA) in response to daily stressors in those with ASD relative to controls (submitted for publication). NA may also be directly associated with momentary PE (32–36). More specifically, a recent ESM study demonstrated that NA predicted paranoia, but, conversely, paranoia did not predict changes in NA in patients with a psychotic disorder (35). To date, no study has investigated the association between NA and momentary PE in adults with ASD.
Our first aim was to examine the frequency of experiences related to the extended psychosis phenotype and accompanying distress using the Community Assessment of Psychic Experiences (CAPE, a validated retrospective self-report questionnaire) (37, 38). That is, three individual dimensions (i.e., subclinical positive, negative, and depressive symptoms), as well as the total CAPE score, were investigated. The reason to examine beyond the positive symptom dimension is that the extended psychosis phenotype is multidimensional in nature and complements a general transdiagnostic psychosis factor (6). Our second aim was to investigate the presence and course of ESM momentary subclinical psychotic phenomena in daily life and their association with minor daily stressors and NA. Therefore, the main objectives of the current study were to examine group (ASD versus controls) and sex differences in i) levels of lifetime psychic experiences (positive, negative and depressive symptoms) and accompanying distress, ii) levels of momentary PE, iii) the impact of different types of daily stressors on momentary PE (psychotic reactivity), and iv) the impact of NA on momentary PE.
Method
Sample
The final sample included 50 participants with an ASD diagnosis (N= 26 males, N= 24 females) and 51 controls (N= 26 males, N= 25 females) between 18 and 65 years of age. Participants with ASD were recruited by contacting mental healthcare facilities in the South of the Netherlands, through patient associations, and via social media. The first author (KL) conducted the Autism Diagnostic Observation Schedule II (ADOS-2) (39) module 4 (fluent speech) in all participants of the ASD group to confirm their diagnoses. Only those participants with ASD who had i) a short-term psychological treatment history (maximum 2 years), and ii) no past psychiatric admission were included. Medication use and other psychiatric disorders were no cause for exclusion except in the case of acute psychotic symptoms, suicidal tendencies, or a bipolar disorder. The Mini-International Neuropsychiatric Interview (MINI) (40, 41) was used to assess the presence of psychiatric disorders in participants with ASD. Controls without a developmental or psychiatric disorder were recruited via social media. Participants were excluded if they had a first-degree family member diagnosed with, or suspected of having, ASD. The Autism Spectrum Quotient (AQ) (42, 43) was used to identify the degree of ASD features in controls; a score above 26 led to exclusion (44). The MINI was also used to exclude any control participants with a current psychiatric disorder. General exclusion criteria were i) suffering from known genetic abnormalities, brain injury, epilepsy, or metabolic disorders, and ii) an intelligence quotient (IQ) below 70. The latter was screened with two subtests (matrix reasoning and vocabulary) of the Wechsler Adult Intelligence Scale—Fourth Edition (WAIS-IV) (45). Six participants were excluded during the screening procedure (due to an IQ below 70 or ADOS-2 scores under the threshold for an ASD diagnosis). The sample characteristics are summarized in Table 1.
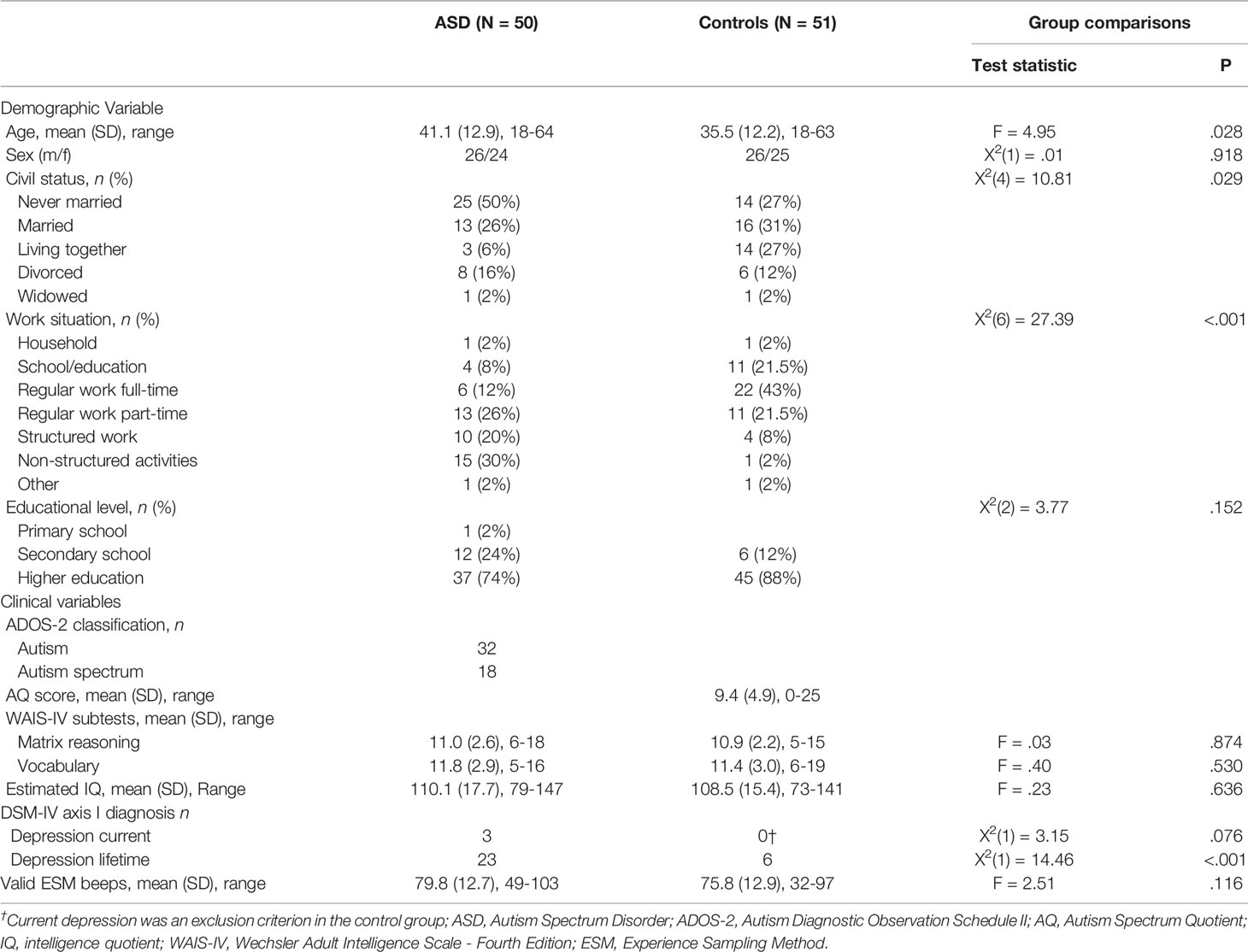
Table 1 Sociodemographic and clinical characteristics of the research sample.
Procedure
This study was approved by the medical ethics committee of Maastricht University (NL51997.068.15) and was carried out in accordance with the Declaration of Helsinki (46). All participants were well informed about the study and gave written informed consent before the first appointment. During the first appointment, participants were screened for meeting the inclusion criteria and they filled in the CAPE. The ESM protocol was explained in a following session.
Daily life assessments were done with the ESM, delivered via the PsyMate™ application. Participants received an iPod or downloaded the app on their smartphone. During 10 days, 10 times a day, the application sent an alert at random moments between 07:30 and 22:30 h. Participants then answered questions about mood, social context, and activities, completing their reports within an allotment of 10 min after the signal. The questionnaire consisted of 7-point Likert scales to capture momentary experiences and categorical questions to capture context (e.g., social context, activities). Participants were encouraged to follow their daily routines. All participants were contacted by telephone after 2 days of sampling to ask if they experienced any problems concerning the protocol. It was also possible for them to contact the researchers, if they had questions or experienced problems with the ESM data collection. Exclusion from the analysis followed in case less than 30% valid reports were acquired (30 out of 100), as previous work has shown that these data are less reliable (47). However, none of the participants were excluded for this reason. After collecting the data, participants were invited for a debriefing session and their experiences were evaluated.
Measures
CAPE—Lifetime Psychic Experiences
The CAPE is a reliable and valid retrospective self-report questionnaire to assess the frequency and distress of a set of different symptom dimensions of the extended psychosis phenotype. The questionnaire consists of 42 items, and the frequency score is measured on a 4-point scale: never (1), sometimes (2), often (3), and nearly always (4). Distress is measured on a 4-point scale: not distressed (1), a bit distressed (2), quite distressed (3), and very distressed (4). For both the frequency scales as well as the distress scales, items are arranged around three dimensions, i.e., positive psychotic experiences (20 items), as well as subclinical negative (14 items), and depressive symptoms (8 items). The internal consistency for this sample was determined by calculating Cronbach’s alpha. Excellent internal consistency was found for the frequency scale (.90) and good internal consistency for the distress scale (.80) in the ASD group. In the control group, a good internal consistency was found for the frequency scale (.83) and an excellent score for the distress scale (.93). The total CAPE scores as well as the three individual dimensions (i.e., positive, negative, and depressive symptoms) were used as outcome measures.
ESM—Momentary Psychotic Experiences
PE were operationalized with four questions (“I feel suspicious”, “I can’t get these thoughts out of my head”, “My thoughts are influenced by others”, and “I hear voices that others don’t”). These questions were scored on 7-point Likert scales (1 = not, 7 = very) and were combined into a mean momentary PE measure.
ESM—Momentary Stress
Stress was conceptualized as subjectively appraised stress after regular daily life encounters or activities. Three different stress measures were obtained: activity-related, event-related, and social stress. Activity-related stress was operationalized, starting with the question “What are you doing?”. Three items followed this question, i.e., “I would rather do something else”; “This is difficult for me”, and “I can do this well”, reverse coded. These questions were scored on 7-point Likert scales (1= not, 7 = very) and were combined into a mean activity-related stress variable. Event-related stress was based on the question “What was the most important event since the last beep?”. Participants subsequently scored how pleasant/unpleasant the event was on a bipolar scale (-3 very unpleasant, 0 neutral, +3 very pleasant). Positive events (scores 1, 2, and 3) were recorded to zero, and negative scores were reverse coded (i.e., higher ratings reflect more stress). Lastly, social stress was operationalized by asking participants if they were in the company of others or alone. If in the company of others, they were asked to rate the item “I would prefer to be alone” (1–7).
ESM—Negative Affect
NA was assessed at each beep with five adjectives (down, insecure, lonely, anxious, irritated) rated on 7-point Likert scales (1 = not, 7 = very). However, detailed factor analyses based on the present ESM data showed that the item ‘irritated’ also had high negative cross-loadings on a positive affect measure (based on the items relaxed, enthusiastic, satisfied, and cheerful). Therefore, the mean of the items “down”, “insecure”, “lonely”, and “anxious” was used as a measure of NA in the analyses.
Statistical Analysis
All analyses were carried out in Stata version 13.1 (48).
CAPE—Lifetime Psychic Experiences
Eight regression analyses were performed to test for differences in frequency of lifetime psychic experiences and degree of distress between adults with ASD and controls. First, two regression analyses were computed with the total CAPE sum scores (on both the frequency and the distress scale) as the dependent variables. Group, sex, and their interaction were added as the independent variables. Second, six regression analyses were performed with the individual CAPE dimensions (positive, negative, and depressive symptoms, again on both the frequency and distress scale) as the dependent variables. Again, group, sex, and their interaction were added as the independent variables. Moreover, previous research showed that young adults are more prone to develop PE than middle-aged and older adults (49), and individuals with depression and lower educational achievement are more vulnerable to develop PE (19, 50, 51). Therefore, we used age, lifetime depression, and education level as covariates, because these variables may partially explain variance in overall and dimensional CAPE scores. Lastly, the predicted marginal means were estimated from these models. In case of a significant two-way interaction, we computed the pairwise differences in simple slopes between the four groups (i.e., males with ASD, females with ASD, control females, and control males). When only a significant main effect for group was found, we estimated the marginal means between ASD and controls.
ESM—Momentary Psychotic Experiences
ESM data have a multilevel structure. Therefore, two-level mixed-effects regression models (using the “mixed” command in Stata) were used to analyze data, with observations (level 1) nested within subjects (level 2). The independent variables, their interactions, and the covariates were entered into the models as fixed effects. Random intercepts and random slopes were added at the subject level, using an unstructured covariance matrix for the random effects. Models were fitted using restricted maximum likelihood estimation (REML). Fixed effects were tested via Wald-type tests with α=.05 (two-sided). As a first step, five multilevel models were fitted to test whether momentary PE, NA, and the three stress variables (independent variables) differed between groups (dependent variable: 0 = controls, 1 = ASD). Next, four models were fitted for activity-related stress, event-related stress, social stress, or NA as a continuous predictor and momentary PE as the outcome variable. Age, lifetime depression, and education level were added as covariates in all models as these might explain part of the variance in momentary PE, similar to the lifetime CAPE scores in the previous subsection. We added two-way (stress/NA x group, stress/NA x sex, group x sex) and three-way (stress/NA x group x sex) interactions to test whether associations between stress or NA and PE differed by group or sex. Based on each fitted model, we computed the slopes (of stress or NA on PE) for all four groups (i.e., males with ASD, females with ASD, control females, and control males) with corresponding 95% confidence intervals (CIs). Given that the current sample size was expected to yield limited power to investigate a three-way interaction, we collapsed these to appropriate marginal slopes if the three-way interaction was not significant. Thus, instead, the marginal slopes for the two-way interaction between stress or NA and group were reported. Lastly, we computed, only in case of a significant three-way interaction, the pairwise differences between the simple slopes to investigate the effects of group and sex on PE.
Sensitivity Analysis
To verify whether the results of the main analyses were robust, we performed a sensitivity analysis. First, we excluded the few participants diagnosed with depression (ASD N = 3, controls N = 0). Since depression is known to be associated with perceived stress (52), NA (53), and PE (54) it might explain some variance in the results. Second, the item “I can’t get these thoughts out of my head” was excluded from the repeated analyses since one may argue that this item is related to persistent thinking, a known feature in ASD (55). Thus, for the sensitivity analysis, momentary PE were operationalized as the total sum of the items: “I feel suspicious”, “My thoughts are influenced by others”, and “I hear voices that others don’t”.
Results
CAPE—Lifetime Psychic Experiences
CAPE—Overall Scores
There were no significant effects found in sex or group x sex interaction terms for the overall CAPE scores on frequency and distress (Table 2). Results showed significant group differences in overall CAPE scores. Moreover, the margins demonstrated distinctly higher levels of lifetime CAPE sum scores and accompanying distress in participants with ASD than controls. The estimated marginal means are summarized in Table 3.
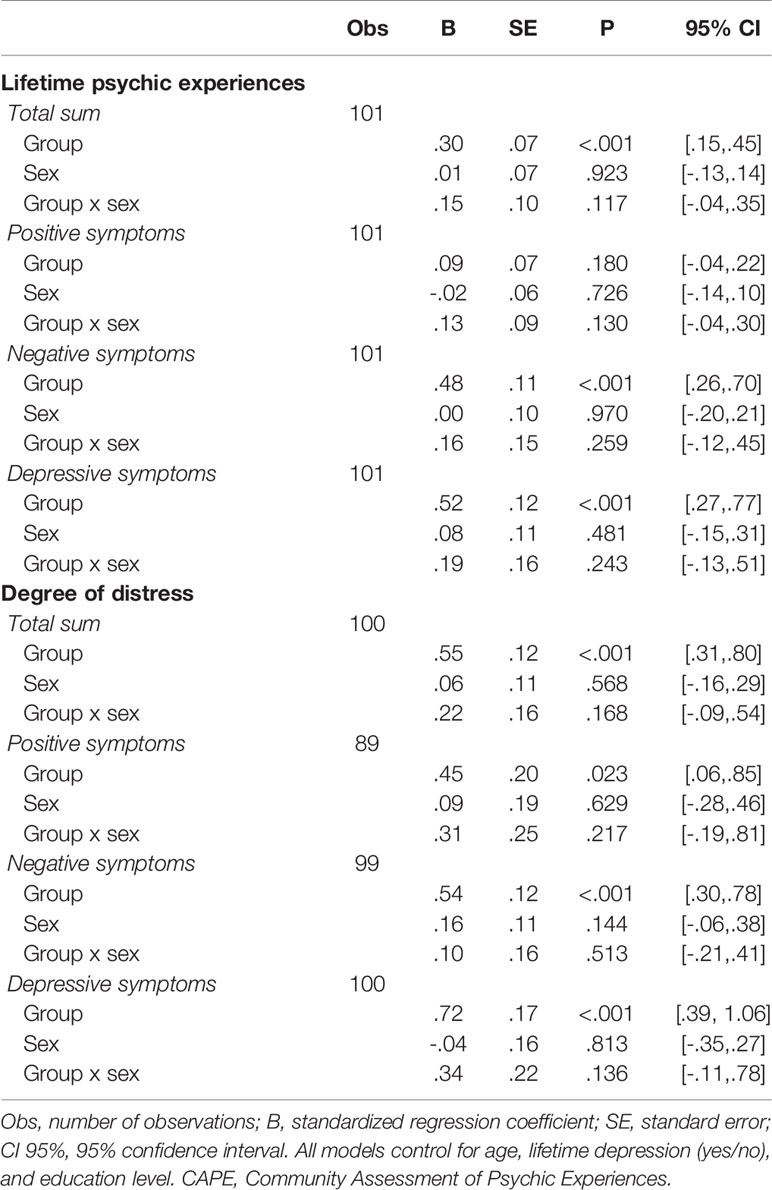
Table 2 Regression estimates of group, sex, and their interaction associated with CAPE overall score and subscale scores.
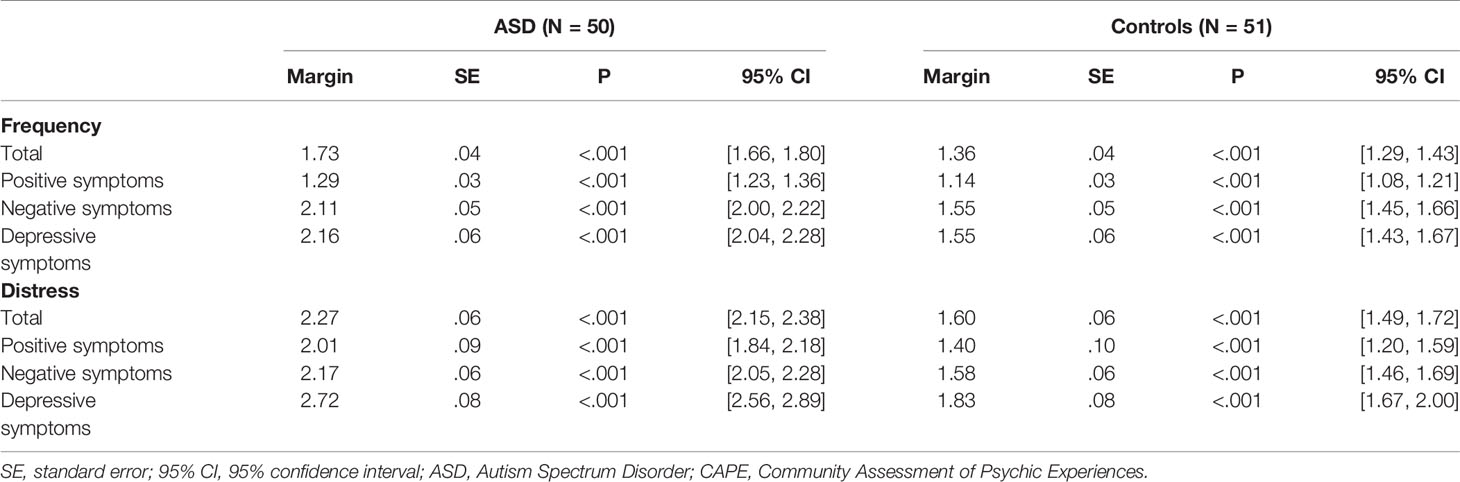
Table 3 Estimated marginal means for the CAPE overall score and subscale scores, per group.
CAPE—Symptom Dimensions
None of the individual CAPE symptom dimensions were significantly associated with the interaction between group and sex, and no significant effects were found for sex (all P >.05) (Table 2). The results showed significant group differences for all three symptom dimensions of frequency and distress (see Tables 2 and 3) except for the positive symptom frequency scale. Thus, adults with ASD reported higher levels of negative and depressive symptoms on the CAPE frequency scale and higher levels of accompanying distress on all three symptom dimensions.
ESM—Momentary Psychotic Experiences
Higher levels of momentary PE were found in adults with ASD relative to controls (Table 4).
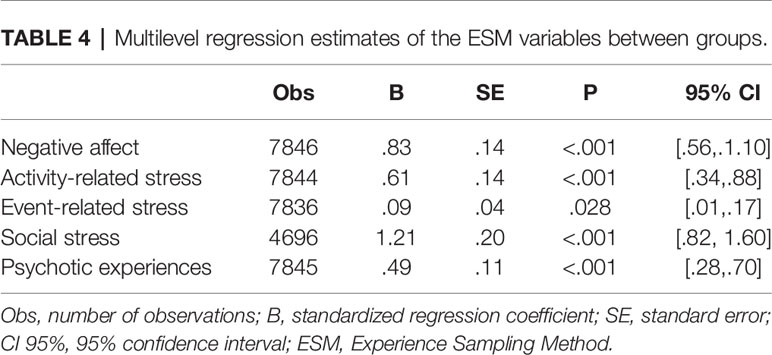
Table 4 Multilevel regression estimates of the ESM variables between groups.
ESM—Momentary Stress and Negative Affect
The ASD group reported significantly higher levels of NA, activity-related, event-related, and social stress than controls (Table 4). Note that the number of observations of the social stress variable was lower than for the other predictors because social stress was only measured in situations where participants reported being in the company of others.
ESM—the Impact of Daily Life Stressors on Momentary Psychotic Experiences
Activity-Related Stress
The interaction between activity-related stress, group, and sex in the model of momentary PE was not significant; neither was the two-way interaction between group and activity-related stress. There were significant main effects of both activity-related stress and group (Table 5).
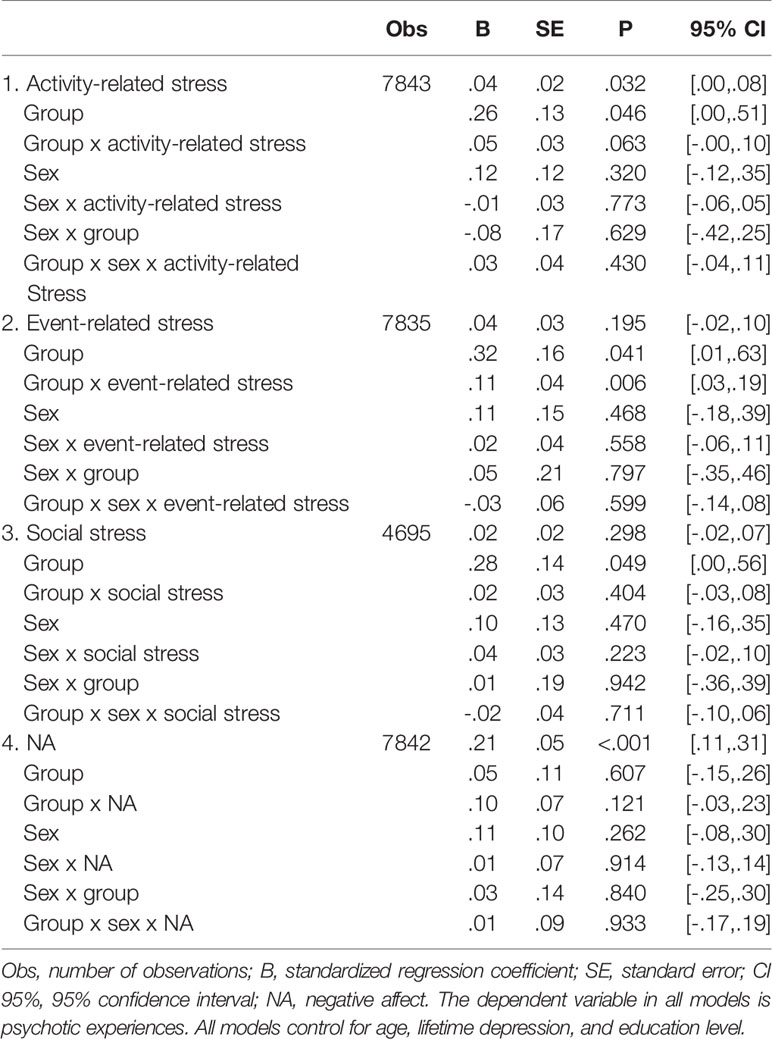
Table 5 Multilevel regression estimates of stress, group, sex, and their interactions in the model of momentary psychotic experiences.
Event-Related Stress
The analyses showed no significant three-way interaction. As shown in Table 5, a significant two-way interaction was found between group and event-related stress in the model of momentary PE. The results of the simple slopes showed a stronger association between event-related stress and PE in the ASD group (B = .15, S.E. = .02, P <.001, 95% CI [.11,.19]) than in controls (B = .05, S.E. = .02, P = .016, 95% CI [.01/.09]) (see Figure 1).
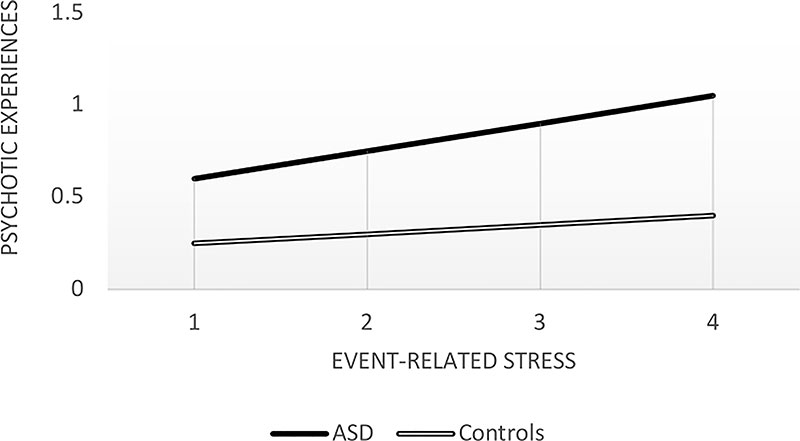
Figure 1 Associations between event-related stress scores and psychotic experiences. ASD, Autism spectrum disorder.
Social Stress
No significant interaction was found between group, sex, and social stress nor between group and social stress in the model of momentary PE. Results demonstrated a trend-significant main effect for group.
ESM—the Impact of Negative Affect on Momentary Psychotic Experiences
The results showed a non-significant three-way interaction (group x sex x NA), and two-way interaction (group x NA) in the model of momentary PE. The analyses showed a significant effect of NA on momentary PE (Table 5).
Sensitivity Analysis
Additional analyses were carried out, excluding participants diagnosed with depression from the sample (ASD: N = 3, controls: N = 0), and with momentary PE as the total sum of three items instead of four (the item “I can’t get these thoughts out of my head” was excluded). All analyses were repeated within the new sample (ASD N = 47, controls N = 51). The results remained similar for all analyses except one: a significant two-way interaction was found between activity-related stress and group on momentary PE (B = .05, S.E. = .02, P = .019, 95% CI [.01,.08]). Marginal effects of the interaction term showed that activity-related stress was significantly associated with momentary PE in the ASD group (B = .07, S.E. = .01, P <.001, 95% CI [.05,.08]) but not in the control group (B = .02, S.E. = .01, P = .094, 95% CI [-.00,.04]). All results are presented in Supplementary Tables S1 and S2.
Discussion
The current study aimed at acquiring more insight into (subclinical) psychotic symptom expression and potential contributing risk factors in adults with ASD. Participants with ASD reported significantly higher lifetime CAPE sum scores (reflecting the extended psychosis phenotype), as well as higher lifetime subclinical negative and depressive symptom scores, all accompanied with higher levels of distress than controls. Although no significant group differences were found in lifetime CAPE PE scores, the ASD group reported more accompanying distress than controls. Adults with ASD reported more ESM momentary PE than controls and event-related stress was associated with increased momentary PE in adults with ASD. There was no moderating effect of group on the associations between either activity-related stress, social stress, or NA, and the outcome variable momentary PE. Overall, no significant differences between male and female outcomes were found.
CAPE—Lifetime Psychic Experiences
Adults with ASD reported significantly more lifetime experiences related to the extended psychosis phenotype, including higher levels of distress. Analyses of the sub-dimensions showed that adults with ASD reported higher levels of negative and depressive symptoms compared to controls, but not higher levels of PE. Although the latter finding differs from previous literature, current results are in line with studies that found a stronger association between autistic features and negative, rather than positive, symptoms (56, 57). Moreover, this is the first ASD study to investigate distress related to symptoms of the extended psychosis phenotype. Higher levels of distress were found in the ASD group compared with controls, for the total scale and all three sub-dimensions. Thus, even though no evidence was found that individuals with ASD have more lifetime PE, they experienced more distress from those experiences than controls. These findings are (clinically) informative since previous studies showed that distress related to PE, rather than frequency of PE, is associated with a higher risk of developing clinical need (58–61). The increased frequency and distress levels of negative and depressive symptoms also point out that clinicians and caregivers should be alerted for a transdiagnostic approach in the mental health care of individuals with ASD, encompassing support and treatment interventions for these extended psychosis phenotype features. Moreover, higher levels of distress related to lifetime experiences may suggest that stress sensitivity plays a role in the emergence of PE (62, 63) in adults with ASD. More specifically, previous research has demonstrated that early trauma and adverse life events can result in altered stress sensitivity, which in turn may lead to a higher frequency and intensity of PE later in life. This pathway has been described as the “affective pathway towards psychosis” (34, 62). An increased stress sensitivity in adults with ASD may be due to a higher vulnerability for childhood adversities, e.g., family and neighborhood adversities (64), and peer victimization (65, 66).
No sex differences were found with respect to lifetime psychic experiences. Given that there is no previous research available, it is not possible to make direct comparisons. However, our results seem to be in contrast with the replicated finding from general population studies that males experience more negative symptoms while females experience more positive symptoms (67, 68). Although there is one general population study that showed higher levels of the CAPE total frequency scale in females (69), this study did not provide data on the subscales. The current results suggest that negative and depressive symptoms are related to ASD in general instead of being sex-dependent. Still, since this is the first study investigating lifetime experiences in adult males and females with ASD, more studies are warranted to further examine this topic. Future studies should aim for larger sample sizes since the current sample was relatively small to investigate sex differences. Furthermore, previous studies examining sex differences in co-occurring symptoms (e.g., anxiety) found significant differences in children and adolescents with ASD (70–72), but not in adults (73–75). Therefore, the results of the present study may not be illustrative of the complete lifespan.
ESM—Momentary Psychotic Experiences
Levels of Momentary Psychotic Experiences
Despite the absence of group differences in frequency levels of CAPE PE, higher levels of ESM momentary PE were demonstrated in ASD. This may indicate that real-time, real-world, daily life monitoring can signal (small changes in) PE, whereas a retrospective instrument may lack the sensitivity to do so. This urges the need for the combination of well-validated (retrospective and EMA) instruments to investigate transdiagnostic phenomenological features in ASD, as the different approaches may be (partly) complementary. Of note, concerning affect, the two instruments yielded overlapping results. As no questions on negative symptoms were included in the ESM questionnaire for this study, this may be a consideration for future research on ASD. In summary, the present study showed the feasibility and relevance of studying momentary PE in a naturalistic environment.
The Impact of Daily Stressors on Momentary Psychotic Experiences
The ASD group showed higher PE levels in association with event-related stress than the control group. Another paper on this sample demonstrated that adults with ASD report higher levels of NA associated with event-related stress, i.e., increased stress-reactivity (submitted for publication). Findings seem to concur with research reporting on unpleasant events as an important stressor in individuals with ASD (76, 77). The absence of a moderating effect of sex could be related to a lack of power. Still, it may also indicate that an increased psychotic reactivity associated with event-related stress is characteristic of ASD in general. Group and sex had no significant effect on the association between activity-related stress and momentary PE. Although, the interaction between group and activity-related stress did reach significance in the sensitivity analysis. No significant moderation effects of group and sex on social stress in the association with momentary PE were found. This was unexpected, especially since problems in social functioning and communication have been found in ASD as well as in individuals who are at clinical high risk for psychosis and individuals with a first psychotic episode (78). The results may comply with a longitudinal study of Bevan Jones et al. (10), which observed that maternal concerns about social interaction in childhood were not significantly associated with increased PE in adolescence. The present findings show that even though adults with ASD reported an increased desire to be alone when in the company of others, momentary PE levels associated with social stress were comparable in both groups. A possible explanation for these findings may be that adults with ASD do experience benefits of social contact (79, 80). It may be that the presence of social support provides a feeling of safety and improves quality of life (81). Thus social support may be a protective factor for momentary PE in ASD, in agreement with the results of a recent longitudinal cohort study in the general population (82).
The Impact of Negative Affect on Momentary Psychotic Experiences
Results showed a significant association between NA and momentary PE but no significant effect of sex and group. Despite the lack of significant group differences, these findings are in line with research that demonstrated an association between NA and momentary PE (34, 36). Moreover, although adults with ASD reported significantly higher levels of NA than controls, the current findings implicate that NA is not a specific risk factor for momentary PE. Nevertheless, in line with the affective pathway to psychosis as described in subsection CAPE—Lifetime Psychic Experiences, research has shown that increased NA in response to daily stress is associated with higher levels of lifetime CAPE scores in the general population (83). Therefore, it may be suggested that NA should not be viewed as a separate risk factor, but may lie on the causal pathway between stress and momentary PE.
Clinical Implications
Present findings highlight the critical role of stress with the emergence of PE in ASD. Results demonstrated that adults with ASD not only experience higher levels of distress in response to (lifetime) PE, but also that stressful events in daily life may increase momentary PE. This may lead to a vicious cycle where adults with ASD may feel distressed by their PE, which, in turn, increases the frequency and intensity of PE. Stress prevention may be one way to disrupt this cycle. Although research on treatment interventions in adults with ASD is limited, some studies demonstrated that cognitive-behavioral therapy (84), acceptance and commitment therapy (85), and dog-assisted therapy (86) led to a significant stress reduction in this population.
Strengths and Limitations
Previous research mainly investigated PE in the ASD population using standard clinical measures. We have tried to bridge the gap in the present literature by examining both self-reported lifetime experiences and momentary assessment of PE in a naturalistic environment. Another strength is that this study included an equal number of males and females, while most research in ASD is focused on male children and adolescents. Furthermore, an ASD group with minimal treatment history was included, and therefore it was possible to examine psychotic reactivity minimally influenced by prior treatment. Although we included a relatively large sample and a sufficient number of self-reports, a lack of power may have affected the three-way interactions. Furthermore, it may be questioned whether all the items used to investigate momentary PE were suitable for the ASD group. A previous study (87) from our department showed, however, that these momentary PE were strongly associated with the positive symptom items of the Positive and Negative Symptom Scale (PANSS) (88) in patients with a psychotic disorder. Lastly, a high functioning group was included, and therefore results may not be generalized to the whole ASD spectrum.
Conclusion
Current results underline that adults with ASD are more prone to encounter lifetime extended psychosis phenotype features, i.e., subclinical negative and depressive symptoms, accompanied with more distress. Even though no group differences were found in the frequency of lifetime PE, these symptoms were accompanied with greater distress in ASD. Results showed higher levels of momentary PE in adults with ASD compared to controls. Furthermore, event-related stress was associated with increased levels of momentary PE, indicating increased psychotic reactivity, in participants with ASD. No significant differences between males and females were found.
Data Availability Statement
The datasets presented in this article are not readily available because of patient confidentiality and participant privacy. Requests to access the datasets should be directed to MM (bS5tYXJjZWxpc0BtYWFzdHJpY2h0dW5pdmVyc2l0eQ==).
Ethics Statement
The studies involving human participants were reviewed and approved by Medisch-ethische toetsingscommissie azM/UM, Maastricht, the Netherlands. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors contributed to conception and design of the study. KL organized the database, performed the statistical analysis, and wrote the first draft of the manuscript. CS, TA, and MM critically reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Geestelijke Gezondheidszorg Eindhoven (GGzE) and Maastricht University. The open access publication fees were supported by Maastricht University.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank the participants, centrum autisme GGzE, GGz Breburg, Apanta GGz and “Nederlandse Vereniging voor autisme (NVA)”. Additionally, we would like to thank Jeroen van Oosterhout, Truda Driesen, Emmy Ottenheijm, Mario Meulendijks, Taco Hübner, Richard van Roy, Jeanine van der Meijden, Kees Spitters, Peggy Gevers, Debora Op ‘t Eijnde, Dafne Op ‘t Eijnde, Sana Erabti, Karel Borkelmans, and Ron Mengelers for their input, management, and assistance in data collection, analysis, proofreading, and technical support.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00766/full#supplementary-material
References
1. Selten JP, Lundberg M, Rai D, Magnusson C. Risks for nonaffective psychotic disorder and bipolar disorder in young people with autism spectrum disorder: a population-based study. JAMA Psychiatry (2015) 72(5):483–9. doi: 10.1001/jamapsychiatry.2014.3059
2. Marín JL, Rodríguez-Franco MA, Chugani VM, Maganto MM, Villoria ED, Bedia RC. Prevalence of schizophrenia spectrum disorders in average-IQ adults with autism spectrum disorders: a meta-analysis. J Autism Dev Disord (2018) 48(1):239–50. doi: 10.1007/s10803-017-3328-5
3. Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry (2000) 57(11):1053–8. doi: 10.1001/archpsyc.57.11.1053
4. Dominguez MD, Wichers M, Lieb R, Wittchen HU, van Os J. Evidence that onset of clinical psychosis is an outcome of progressively more persistent subclinical psychotic experiences: an 8-year cohort study. Schizophr Bull (2011) 37(1):84–93. doi: 10.1093/schbul/sbp022
5. Downs JM, Cullen AE, Barragan M, Laurens KR. Persisting psychotic-like experiences are associated with both externalising and internalising psychopathology in a longitudinal general population child cohort. Schizophr Res (2013) 144(1-3):99–104. doi: 10.1016/j.schres.2012.12.009
6. van Os J, Reininghaus U. Psychosis as a transdiagnostic and extended phenotype in the general population. World Psychiatry (2016) 15(2):118–24. doi: 10.1002/wps.20310
7. DeVylder JE, Thompson E, Reeves G, Schiffman J. Psychotic experiences as indicators of suicidal ideation in a non-clinical college sample. Psychiatry Res (2015) 226(2-3):489–93. doi: 10.1016/j.psychres.2015.02.007
8. Núñez D, Fresno A, van Borkulo CD, Courtet P, Arias V, Garrido V, et al. Examining relationships between psychotic experiences and suicidal ideation in adolescents using a network approach. Schizophr Res (2018) 201:54–61. doi: 10.1016/j.schres.2018.05.020
9. Sullivan S, Rai D, Golding J, Zammit S, Steer C. The association between autism spectrum disorder and psychotic experiences in the avon longitudinal study of parents and children (ALSPAC) birth cohort. J Am Acad Child Adolesc Psychiatry (2013) 52(8):806–14. doi: 10.1016/j.jaac.2013.05.010
10. Bevan Jones R, Thapar A, Lewis G, Zammit S. The association between early autistic traits and psychotic experiences in adolescence. Schizophr Res (2012) 135(1-3):164–9. doi: 10.1016/j.schres.2011.11.037
11. Taylor MJ, Robinson EB, Happé F, Bolton P, Freeman D, Ronald A. A longitudinal twin study of the association between childhood autistic traits and psychotic experiences in adolescence. Mol Autism (2015) 6:44–56. doi: 10.1186/s13229-015-0037-9
12. Zammit S, Kounali D, Cannon M, David AS, Gunnell D, Heron J, et al. Psychotic experiences and psychotic disorders at age 18 in relation to psychotic experiences at age 12 in a longitudinal population-based cohort study. Am J Psychiatry (2013) 170(7):742–50. doi: 10.1176/appi.ajp.2013.12060768
13. Sieradzka D, Power RA, Freeman D, Cardno AG, McGuire P, Plomin R, et al. Are genetic risk factors for psychosis also associated with dimension-specific psychotic experiences in adolescence? PloS One (2014) 9(4):e94398. doi: 10.1371/journal.pone.0094398
14. Gadow KD, DeVincent CJ. Comparison of children with autism spectrum disorder with and without schizophrenia spectrum traits: gender, season of birth, and mental health risk factors. J Autism Dev Disord (2012) 42(11):2285–96. doi: 10.1007/s10803-012-1473-4
15. Rössler W, Hengartner MP, Ajdacic-Gross V, Haker H, Angst J. Impact of childhood adversity on the onset and course of subclinical psychosis symptoms — Results from a 30-year prospective community study. Schizophr Res (2014) 153(1-3):189–95. doi: 10.1016/j.schres.2014.01.040
16. Rössler W, Ajdacic-Gross V, Rodgers S, Haker H, Müller M. Childhood trauma as a risk factor for the onset of subclinical psychotic experiences: Exploring the mediating effect of stress sensitivity in a cross-sectional epidemiological community study. Schizophr Res (2016) 172(1-3):46–53. doi: 10.1016/j.schres.2016.02.006
17. Trotta A, Murray RM, Fisher HL. The impact of childhood adversity on the persistence of psychotic symptoms: a systematic review and meta-analysis. Psychol Med (2015) 45(12):2481–98. doi: 10.1017/S0033291715000574
18. McGrath JJ, Saha S, Lim CCW, Aguilar-Gaxiola S, Alonso J, Andrade LH, et al. Trauma and psychotic experiences: transnational data from the World Mental Health Survey. Br J Psychiatry (2017) 211(6):373–80. doi: 10.1192/bjp.bp.117.205955
19. Johns LC, Cannon M, Singleton N, Murray RM, Farrell M, Brugha T, et al. Prevalence and correlates of self-reported psychotic symptoms in the British population. Br J Psychiatry (2004) 185(4):298–305. doi: 10.1192/bjp.185.4.298
20. Wiles NJ, Zammit S, Bebbington P, Singleton N, Meltzer H, Lewis G. Self-reported psychotic symptoms in the general population. Results from the longitudinal study of the British National Psychiatric Morbidity Survey. Br J Psychiatry (2006) 8(6):519–26. doi: 10.1192/bjp.bp.105.012179
21. Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull (2012) 38(4):661–71. doi: 10.1093/schbul/sbs050
22. Beards S, Gayer-Anderson C, Borges S, Dewey ME, Fisher HL, Morgan C. Life events and psychosis: a review and meta-analysis. Schizophr Bull (2013) 39(4):740–7. doi: 10.1093/schbul/sbt065
23. Bonoldi I, Simeone E, Rocchetti M, Codjoe L, Rossi G, Gambi F, et al. Prevalence of self-reported childhood abuse in psychosis: A meta-analysis of retrospective studies. Psychiatry Res (2013) 210(1):8–15. doi: 10.1016/j.psychres.2013.05.003
24. Hernaus D, Collip D, Lataster J, Viechtbauer W, Myin E, Ceccarini J, et al. Psychotic reactivity to daily life stress and the dopamine system: a study combining experience sampling and [18F]fallypride positron emission tomography. J Abnorm Psychol (2015) 124(1):27–37. doi: 10.1037/abn0000010
25. Glaser JP, Van Os J, Thewissen V, Myin-Germeys I. Psychotic reactivity in borderline personality disorder. Acta Psychiatr Scand (2010) 121(2):125–34. doi: 10.1111/j.1600-0447.2009.01427.x
26. Myin-Germeys I, Oorschot M, Collip D, Lataster J, Delespaul P, van Os J. Experience sampling research in psychopathology: opening the black box of daily life. Psychol Med (2009) 39(9):1533–47. doi: 10.1017/S0033291708004947
27. Chen Y-W, Bundy A, Cordier R, Chien Y-L, Einfeld S. The experience of social participation in everyday contexts among individuals with autism spectrum disorders: an experience sampling study. J Autism Dev Disord (2016) 46(4):1403–14. doi: 10.1007/s10803-015-2682-4
28. Kovac M, Mosner M, Miller S, Hanna EK, Dichter GS. Experience sampling of positive affect in adolescents with autism: Feasibility and preliminary findings. Res Autism Spectr Disord (2016) 29-30:57–65. doi: 10.1016/j.rasd.2016.06.003
29. Hintzen A, Delespaul P, van Os J, Myin-Germeys I. Social needs in daily life in adults with Pervasive Developmental Disorders. Psychiatry Res (2010) 179(1):75–80. doi: 10.1016/j.psychres.2010.06.014
30. Myin-Germeys I, Delespaul P, van Os J. Behavioural sensitization to daily life stress in psychosis. Psychol Med (2005) 35(5):733–41. doi: 10.1017/S0033291704004179
31. van der Steen Y, Gimpel-Drees J, Lataster T, Viechtbauer W, Simons CJP, Lardinois M, et al. Clinical high risk for psychosis: the association between momentary stress, affective and psychotic symptoms. Acta Psychiatr Scand (2017) 136(1):63–73. doi: 10.1111/acps.12714
32. Garety PA, Kuipers E, Fowler D, Freeman D, Bebbington P. A cognitive model of the positive symptoms of psychosis. Psychol Med (2001) 31(2):189–95. doi: 10.1017/S0033291701003312
33. Jaya ES, Ascone L, Lincoln TM. A longitudinal mediation analysis of the effect of negative-self-schemas on positive symptoms via negative affect. Psychol Med (2018) 48(8):1299–307. doi: 10.1017/S003329171700277X
34. Kramer I, Simons CJP, Wigman JTW, Collip D, Jacobs N, Derom C, et al. Time-lagged moment-to-moment interplay between negative affect and paranoia: new insights in the affective pathway to psychosis. Schizophr Bull (2014) 40(2):278–86. doi: 10.1093/schbul/sbs194
35. So SH-W, Chau AKC, Peters ER, Swendsen J, Garety PA, Kapur S. Moment-to-moment associations between negative affect, aberrant salience, and paranoia. Cognit Neuropsychiatry (2018) 23(5):299–306. doi: 10.1080/13546805.2018.1503080
36. Thewissen V, Bentall RP, Oorschot M, AC J, van Lierop T, van Os J, et al. Emotions, self-esteem, and paranoid episodes: an experience sampling study. Br J Clin Psychol (2011) 50(2):178–95. doi: 10.1348/014466510X508677
37. Konings M, Bak M, Hanssen M, Van Os J, Krabbendam L. Validity and reliability of the CAPE: a self-report instrument for the measurement of psychotic experiences in the general population. Acta Psychiatr Scand (2006) 114(1):55–61. doi: 10.1111/j.1600-0447.2005.00741.x
38. Stefanis N, Hanssen M, Smirnis N, Avramopoulos D, Evdokimidis I, Stefanis C, et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med (2002) 32(2):347–58. doi: 10.1017/S003329170100514
39. Lord C, Rutter M, DiLavore P, Risi S, Gotham K, Bishop S. Autism Diagnostic Observation Schedule Second Edition (ADOS-2) Manual (Part 1): Modules 1–4. Torrance, CA: Western Psychological Services (2012).
40. Lecrubier Y, Sheehan DV, Weiller E, Amorim P, Bonora I, Harnett Sheehan K, et al. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. Eur Psychiatry (1997) 12(5):224–31. doi: 10.1016/S0924-9338(97)83296-8
41. van Vliet I, de Beurs E. The MINI-International Neuropsychiatric Interview. A brief structured diagnostic psychiatric interview for DSM-IV en ICD-10 psychiatric disorders. Tijdschrift voor Psychiatr (2007) 49(6):393–97.
42. Hoekstra RA, Bartels M, Cath DC, Boomsma DI. Factor structure, reliability and criterion validity of the Autism-Spectrum Quotient (AQ): a study in Dutch population and patient groups. J Autism Dev Disord (2008) 38(8):1555–66. doi: 10.1007/s10803-008-0538-x
43. Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The Autism-Spectrum Quotient (AQ): evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord (2001) 31(1):5–17. doi: 10.1023/A:1005653411471
44. Woodbury-Smith MR, Robinson J, Wheelwright S, Baron-Cohen S. Screening adults for Asperger syndrome using the AQ: A preliminary study of its diagnostic validity in clinical practice. J Autism Dev Disord (2005) 35(3):331–5. doi: 10.1007/s10803-005-3300-7
45. Wechsler D. Wechsler Adult Intelligence Scale–Fourth Edition (WAIS–IV). San Antonio, TX: The Psychological Corporation (2008).
46. World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull World Health Organ (2001) 79(4):373–4. doi: 10.4414/fms.2001.04031
47. Delespaul P. Assessing schizophrenia in daily life: the experience sampling method. Maastricht, the Netherlands (1995).
49. McGrath JJ, Saha S, Al-Hamzawi AO, Alonso J, Andrade L, Borges G, et al. Age of onset and lifetime projected risk of psychotic experiences: cross-national data from the World Mental Health Survey. Schizophr Bull (2016) 42(4):933–41. doi: 10.1093/schbul/sbw011
50. van Os J, Hanssen M, Bijl RV, Ravelli A. Strauss (1969) revisited: a psychosis continuum in the general population? Schizophr Res (2000) 45(1-2):11–20. doi: 10.1016/S0920-9964(99)00224-8
51. van Rossum I, Dominguez MD, Lieb R, Wittchen HU, van Os J. Affective dysregulation and reality distortion: a 10-year prospective study of their association and clinical relevance. Schizophr Bull (2011) 37(3):561–71. doi: 10.1093/schbul/sbp101
52. Bergdahl J, Bergdahl M. Perceived stress in adults: prevalence and association of depression, anxiety and medication in a Swedish population. Stress Health (2002) 18(5):235–41. doi: 10.1002/smi.946
53. Forbes EE, Williamson DE, Ryan ND, Dahl RE. Positive and negative affect in depression: Influence of sex and puberty. Ann N Y Acad Sci (2004) 1021(1):341–7. doi: 10.1196/annals.1308.042
54. Smith B, Fowler DG, Freeman D, Bebbington P, Bashforth H, Garety P, et al. Emotion and psychosis: Links between depression, self-esteem, negative schematic beliefs and delusions and hallucinations. Schizophr Res (2006) 86(1):181–8. doi: 10.1016/j.schres.2006.06.018
55. Russell A, Brosnan M. Habits and Autism: Restricted, Repetitive Patterns of Behaviour and Thinking in Autism. The psychology of habit: theory, mechanisms, change, and contexts. Cham: Springer International Publishing: Springer (2018) p. 343–61.
56. Esterberg ML, Trotman HD, Brasfield JL, Compton MT, Walker EF. Childhood and current autistic features in adolescents with schizotypal personality disorder. Schizophr Res (2008) 104(1-3):265–73. doi: 10.1016/j.schres.2008.04.029
57. Spek AA, Wouters SGM. Autism and schizophrenia in high functioning adults: Behavioral differences and overlap. Res Autism Spectr Disord (2010) 4(4):709–17. doi: 10.1016/j.rasd.2010.01.009
58. Bak M, Myin-Germeys I, Delespaul P, Vollebergh W, de Graaf R, van Os J. Do different psychotic experiences differentially predict need for care in the general population? Compr Psychiatry (2005) 46(3):192–9. doi: 10.1016/j.comppsych.2004.08.003
59. Peters E, Ward T, Jackson M, Morgan C, Charalambides M, McGuire P, et al. Clinical, socio-demographic and psychological characteristics in individuals with persistent psychotic experiences with and without a “need for care”. World Psychiatry (2016) 15(1):41–52. doi: 10.1002/wps.20301
60. Jacobs N, Myin-Germeys I, Derom C, Vlietinck R, Os J. Deconstructing the familiality of the emotive component of psychotic experiences in the general population. Acta Psychiatr Scand (2005) 112(5):394–401. doi: 10.1111/j.1600-0447.2005.00588.x
61. Martin G, Thomas H, Andrews T, Hasking P, Scott JG. Psychotic experiences and psychological distress predict contemporaneous and future non-suicidal self-injury and suicide attempts in a sample of Australian school-based adolescents. Psychol Med (2015) 45(2):429–37. doi: 10.1017/S0033291714001615
62. Myin-Germeys I, van Os J. Stress-reactivity in psychosis: evidence for an affective pathway to psychosis. Clin Psychol Rev (2007) 27(4):409–24. doi: 10.1016/j.cpr.2006.09.005
63. DeVylder JE, Koyanagi A, Unick J, Oh H, Nam B, Stickley A. stress sensitivity and psychotic experiences in 39 low- and middle-Income countries. Schizophr Bull (2016) 42(6):1353–62. doi: 10.1093/schbul/sbw044
64. Berg KL, Shiu CS, Acharya K, Stolbach BC, Msall ME. Disparities in adversity among children with autism spectrum disorder: a population-based study. Dev Med Child Neurol (2016) 58(11):1124–31. doi: 10.1111/dmcn.13161
65. Ung DPD, McBride NBA, Collier ABA, Selles RPD, Small BPD, Phares VPD, et al. The relationship between peer victimization and the psychological characteristics of youth with autism spectrum disorder. Res Autism Spectr Disord (2016) 32:70–9. doi: 10.1016/j.rasd.2016.09.002
66. Sreckovic MA, Brunsting NC, Able H. Victimization of students with autism spectrum disorder: A review of prevalence and risk factors. Res Autism Spectr Disord (2014) 8(9):1155–72. doi: 10.1016/j.rasd.2014.06.004
67. Bora E, Baysan Arabaci L. Effect of age and gender on schizotypal personality traits in the normal population Schizotypy and age. Psychiatry Clin Neurosci (2009) 63(5):663–9. doi: 10.1111/j.1440-1819.2009.02011.x
68. Maric N, Krabbendam L, Vollebergh W, de Graaf R, van Os J. Sex differences in symptoms of psychosis in a non-selected, general population sample. Schizophr Res (2003) 63(1-2):89–95. doi: 10.1016/S0920-9964(02)00380-8
69. Armando M, Nelson B, Yung AR, Ross M, Birchwood M, Girardi P, et al. Psychotic-like experiences and correlation with distress and depressive symptoms in a community sample of adolescents and young adults. Schizophr Res (2010) 119(1):258–65. doi: 10.1016/j.schres.2010.03.001
70. Solomon M, Miller M, Taylor SL, Hinshaw SP, Carter CS. Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders. J Autism Dev Disord (2012) 42(1):48–59. doi: 10.1007/s10803-011-1215-z
71. May T, Cornish K, Rinehart N. Does Gender Matter? A one year follow-up of autistic, attention and anxiety symptoms in high-functioning children with autism spectrum disorder. J Autism Dev Disord (2014) 44(5):1077–86. doi: 10.1007/s10803-013-1964-y
72. Rynkiewicz A, Łucka I. Autism spectrum disorder (ASD) in girls. Co-occurring psychopathology. Sex differences in clinical manifestation. Psychiatr Pol (2018) 52(4):629–39. doi: 10.12740/PP/OnlineFirst/58837
73. Lugnegård T, Hallerbäck MU, Gillberg C. Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res Dev Disabil (2011) 32(5):1910–7. doi: 10.1016/j.ridd.2011.03.025
74. Lai M-C, Lombardo MV, Pasco G, Ruigrok AN, Wheelwright SJ, Sadek SA, et al. A behavioral comparison of male and female adults with high functioning autism spectrum conditions. PloS One (2011) 6(6):e20835. doi: 10.1371/journal.pone.0020835
75. Hofvander BR, Delorme R, Chaste P, Nydén A, Wentz E, Ståhlberg O, et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry (2009) 9:35–44. doi: 10.1186/1471-244X-9-35
76. Hess KL. Stress for Individuals with Autism Spectrum Disorders: Effects of Age, Gender, and Intelligence Quotient. Dissertation, Georgia State University (2009).
77. Corbett BA, Schupp CW, Levine S, Mendoza S. Comparing cortisol, stress, and sensory sensitivity in children with autism. Autism Res (2009) 2(1):39–49. doi: 10.1002/aur.64
78. Solomon M, Olsen E, Niendam T, Ragland JD, Yoon J, Minzenberg M, et al. From lumping to splitting and back again: Atypical social and language development in individuals with clinical-high-risk for psychosis, first episode schizophrenia, and autism spectrum disorders. Schizophr Res (2011) 131(1-3):146–51. doi: 10.1016/j.schres.2011.03.005
79. Gantman A, Kapp SK, Orenski K, Laugeson EA. Social kkills training for young adults with high-functioning autism spectrum disorders: A randomized controlled pilot study. J Autism Dev Disord (2012) 42(6):1094–103. doi: 10.1007/s10803-011-1350-6
80. Renty J, Roeyers H. Individual and marital adaptation in men with autism spectrum disorder and their spouses: The Role of social support and coping strategies. J Autism Dev Disord (2007) 37(7):1247–55. doi: 10.1007/s10803-006-0268-x
81. Tobin MC, Drager KDR, Richardson LF. A systematic review of social participation for adults with autism spectrum disorders: Support, social functioning, and quality of life. Res Autism Spectr Disord (2014) 8(3):214–29. doi: 10.1016/j.rasd.2013.12.002
82. Crush E, Arseneault L, Moffitt TE, Danese A, Caspi A, Jaffee SR, et al. Protective factors for psychotic experiences amongst adolescents exposed to multiple forms of victimization. J Psychiatr Res (2018) 104:32–8. doi: 10.1016/j.jpsychires.2018.06.011
83. Collip D, Wigman JT, Myin-Germeys I, Jacobs N, Derom C, Thiery E, et al. From epidemiology to daily life: linking daily life stress reactivity to persistence of psychotic experiences in a longitudinal general population study. PloS One (2013) 8(4):e62688. doi: 10.1371/journal.pone.0062688
84. McGillivray JA, Evert HT. Group cognitive behavioural therapy program shows potential in reducing symptoms of depression and stress among young people with ASD. J Autism Dev Disord (2014) 44(8):2041–51. doi: 10.1007/s10803-014-2087-9
85. Pahnke J, Bjureberg J, Bohman B, Lundgren T, Hirvikoski T, Bolte S, et al. Acceptance and commitment therapy for autistic adults: An open pilot study in a psychiatric outpatient context. J Contextual Behav (2019) 13:34–41. doi: 10.1016/j.jcbs.2019.04.002
86. Wijker C, Leontjevas R, Spek A, Enders-Slegers M-J. Effects of dog assisted therapy for adults with autism spectrum disorder: An exploratory randomized controlled trial. J Autism Dev Disord (2019) 50(6):2153–63. doi: 10.1007/s10803-019-03971-9
87. van Os J, Lataster T, Delespaul P, Wichers M, Myin-Germeys I, Jiménez-Murcia S. Evidence that a psychopathology interactome has diagnostic value, predicting clinical needs: An experience sampling study. PloS One (2014) 9(1):e86652. doi: 10.1371/journal.pone.0086652
Keywords: autism spectrum disorder, stress, psychotic experiences, negative affect, momentary assessment
Citation: van der Linden K, Simons C, van Amelsvoort T and Marcelis M (2020) Lifetime and Momentary Psychotic Experiences in Adult Males and Females With an Autism Spectrum Disorder. Front. Psychiatry 11:766. doi: 10.3389/fpsyt.2020.00766
Received: 25 April 2020; Accepted: 20 July 2020;
Published: 03 August 2020.
Edited by:
Tim Ziermans, University of Amsterdam, NetherlandsReviewed by:
Anja Vaskinn, Oslo University Hospital, NorwayYu-Wei Ryan Chen, The University of Sydney, Australia
Copyright © 2020 van der Linden, Simons, van Amelsvoort and Marcelis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kim van der Linden, S2ltLnZhbmRlcmxpbmRlbkBtYWFzdHJpY2h0dW5pdmVyc2l0eS5ubA==