 Natalia Szejko
Natalia Szejko Carolin Fremer1
Carolin Fremer1- 1Clinic of Psychiatry, Social Psychiatry and Psychotherapy, Hannover Medical School, Hannover, Germany
- 2Division of Neurocritical Care & Emergency Neurology, Department of Neurology, Yale School of Medicine, New Haven, CT, United States
- 3Department of Bioethics, Medical University of Warsaw, Warsaw, Poland
- 4Department of Neurology, Medical University of Warsaw, Warsaw, Poland
Although several lines of evidence support the hypothesis of a dysregulation of serotoninergic neurotransmission in the pathophysiology of obsessive-compulsive disorder (OCD), there is also evidence for an involvement of other pathways such as the GABAergic, glutamatergic, and dopaminergic systems. Only recently, data obtained from a small number of animal studies alternatively suggested an involvement of the endocannabinoid system in the pathophysiology of OCD reporting beneficial effects in OCD-like behavior after use of substances that stimulate the endocannabinoid system. In humans, until today, only two case reports are available reporting successful treatment with dronabinol (tetrahydrocannabinol, THC), an agonist at central cannabinoid CB1 receptors, in patients with otherwise treatment refractory OCD. In addition, data obtained from a small open uncontrolled trial using the THC analogue nabilone suggest that the combination of nabilone plus exposure-based psychotherapy is more effective than each treatment alone. These reports are in line with data from a limited number of case studies and small controlled trials in patients with Tourette syndrome (TS), a chronic motor and vocal tic disorder often associated with comorbid obsessive compulsive behavior (OCB), reporting not only an improvement of tics, but also of comorbid OCB after use of different kinds of cannabis-based medicines including THC, cannabis extracts, and flowers. Here we present the case of a 22-year-old male patient, who suffered from severe OCD since childhood and significantly improved after treatment with medicinal cannabis with markedly reduced OCD and depression resulting in a considerable improvement of quality of life. In addition, we give a review of current literature on the effects of cannabinoids in animal models and patients with OCD and suggest a cannabinoid hypothesis of OCD.
Introduction
Obsessive-compulsive disorder (OCD) is characterized by the presence of obsessions and/or compulsions. Obsessions are defined as recurrent and persistent thoughts, urges, or images that are intrusive, unwanted, and cause—in most individuals—marked anxiety and/or distress. Compulsions are repetitive behaviors or mental acts that the person feels driven to perform in response to an obsession or according to the rules that must be applied rigidly (1). OCD is a severe and underdiagnosed mental disorder that causes substantial impairment in quality of life in the majority of patients. The prevalence of OCD is estimated to be around 2% to 3% (2–4). Up to this date, the only treatments approved for alleviation of OCD are cognitive-behavioral therapy (CBT) and pharmacotherapy with (selective) serotonin reuptake inhibitors ((S)SRI) (5). However, about one third of patients does not benefit from these treatment strategies, experiences recurrent episodes, or does not tolerate treatment with SSRI (6, 7). In these otherwise treatment-resistant patients surgical intervention using deep brain stimulation (DBS) has been suggested as an alternative option. Thus, novel treatments and new pharmacological components are urgently needed to improve outcome in patients with OCD.
The pathophysiology of OCD includes the involvement of different neurotransmitter systems, the most important being the serotoninergic system (8, 9). This serotonin hypothesis of OCD is mainly based on beneficial treatment effects of (S)SRI medication. In addition, a number of other pathways such as the GABAergic, glutamatergic, and dopaminergic have been suggested to be involved too (10–12). Accordingly, diverse brain regions have been suggested to be affected (13, 14). Only recently, the ENIGMA-OCD Consortium (15) reported less segregated organization of structural covariance networks in OCD, reorganization of brain hubs as well as a possible signature of altered brain morphometry especially in those regions involved in brain development and maturation such as the cingulate and orbitofrontal areas.
Against the background of increasing acceptance of cannabis-based medicines (CBM) in various diseases (16), increasing evidence for a paramount role of the central endocannabinoid system (ECS) in brain development (17) and stress regulation (18) as well as the fact that the ECS is the most important neuromodulatory system in the brain (19), research was initiated to explore the role of the ECS in the pathophysiology of OCD (20). Although only a small number of studies in animals and humans have been published addressing this topic, most of the data support the hypothesis that CBM might be effective in the treatment of OCD.
The aim of this report is to increase the database by presenting an illustrative case of a patient with severe OCD, who markedly benefitted from treatment with cannabis and, in addition, to summarize available scientific evidence supporting the importance of the ECS in the pathophysiology of OCD.
Case Report
The male patient first presented in our outpatient clinic at the age of 22. Prenatal and perinatal development did not show any abnormalities and his medical history was unremarkable. Family history was negative without neurological and psychiatric diseases. Further history revealed that OCD symptoms already started in kindergarten age. At that time, he suffered from compulsions with the urge to constantly close the door and checking rituals accompanied by a just right feeling. During the following years, obsessions and compulsions exhibited a waxing and waning course without remission at any time. At the age of 17, in parallel to increased OCD symptoms, he developed a depressive episode with suicidal thoughts.
The diagnosis of OCD was made only one year before the first presentation in our clinic at the age of 21, after he had consulted his general practitioner, because his symptoms caused increasing problems in different areas of life, and he was worried that he would not be able to complete his training as animal keeper successfully. Therefore, pharmacotherapy with clomipramine was initiated with a maximal dose 25mg/d. Because of adverse events such as nausea and headache and because he felt no positive effect, he stopped medication after only one week.
During the first presentation in our clinic, the diagnosis of OCD according to DSM-5 was confirmed by one of the authors (KMV). At that time, the patient suffered from compulsions with repeated hand washing (up to 20×/day) and prolonged showering (up to 1h/day) including washing rituals as well as further rituals related to checking, ordering, and cleaning. In addition, he suffered from several obsessions such as contamination fear, sexual obsessions, repetition of same words, and magical thinking. He tried to neutralize these negative thoughts by imagining numbers. Several of these obsessions and compulsions were accompanied by a just right feeling. Altogether, he estimated to spent approximately 4 h a day on obsessive thoughts and compulsive behaviors. Non-surprisingly, OCD symptoms caused relevant problems in social life and at work. In his training as animal keeper, his boss and co-workers often exhorted him, mainly because of slowness due to his compulsions. At vocational school he had difficulties concentrating and learning. Due to his symptoms, he had stopped doing sports, neglected hobbies, avoided social contacts, and withdrew more and more socially. There was no evidence that his symptoms should be attributed to the effects of substance abuse or another medical condition.
The presentation in our clinic was motivated by the fact that he had noticed that use of cannabis alleviated his symptoms. He reported that he had started using cannabis recreationally at age 16. Because his symptoms markedly improved, he started to smoke street cannabis (mixed with tobacco) on a regular basis using 0.5 g cannabis three to four times per week (about 8 g/months). Use of street cannabis resulted in a constant and marked improvement of obsessions and compulsions of about 80% to 90% lasting for 12 to 15 h. In addition, his sleep improved because of a general feeling of relaxation, reduced OCD, and less rumination. No adverse events were reported. Despite these beneficial effects, he decided to stop using street cannabis on a regular basis at the age of 20, because he did not want to do anything illegal and because he was afraid of losing his driver’s license. Beside illegal use of street cannabis, the patient reported that he started smoking tobacco at the age of 15 (approximately 10 cigarettes/day). His further history of substance abuse was unremarkable. He reported not to drink any alcohol for several years.
We decided to initiate treatment with prescribed medicinal cannabis because of the diagnosis of severe OCD, due to the fact that the patient refused pharmacotherapy with (S)SRI as well as psychotherapy, and because of his reports of marked improvement after use of street cannabis. Before first prescription of medicinal cannabis, the patient stated that he has not smoked cannabis for about one year. Because THC content of street cannabis he had used before was unknown, we decided to test two different chemovars: Bedrocan containing 22% THC and <1% cannabidiol (CBD) and Bedrobinol containing 13.5% THC and <1% CBD. Both Bedrocan and Bedrobinol are produced by Bedrocan ® Company in compliance with the European Medicines Agency’s good manufacturing practice (GMP) standards and ISO 9001: 2015 Certificates. Since the patient reported much better effects using Bedrocan, treatment with this chemovar was implemented with a daily dose of 0.2 to 0.3 g. Immediate thereafter, he reported a marked reduction of obsessions and compulsions of about 70% as well as general relaxation, improved sleep, and concentration at school as well as overall improvement of his quality of life resulting in better social functioning and reduced problems at work. For example, he restarted to practice sports. Twenty months after initiation of medicinal cannabis therapy, he passed his final theoretical and practical exams as animal keeper, and his employer offered him a permanent position. During the last months, he slightly increased the daily dose of Bedrocan cannabis up to 0.7 g.
At baseline, before implementation of treatment with medicinal cannabis as well as three, five, and 20 months later, a variety of clinical assessments have been performed by a clinical psychologist and psychotherapist (CF) experienced in this kind of tests. Detailed results are provided in Table 1. During the last follow-up visit, the patient reported an improvement of compulsions and obsessions of 90% to 95%. No side effects were reported. While in the past he had used street cannabis exclusively by smoking mixed with tobacco, after initiation of prescribed therapy with medicinal cannabis, he started inhale cannabis using a vaporizer in parallel. During the last follow-up visit, he reported to vaporize medicinal cannabis during the day and to smoke only once in the evening. However, for smoking he is mixing cannabis only with a small amount of tobacco (which is much smaller than in the past) and completely stopped smoking tobacco cigarettes.
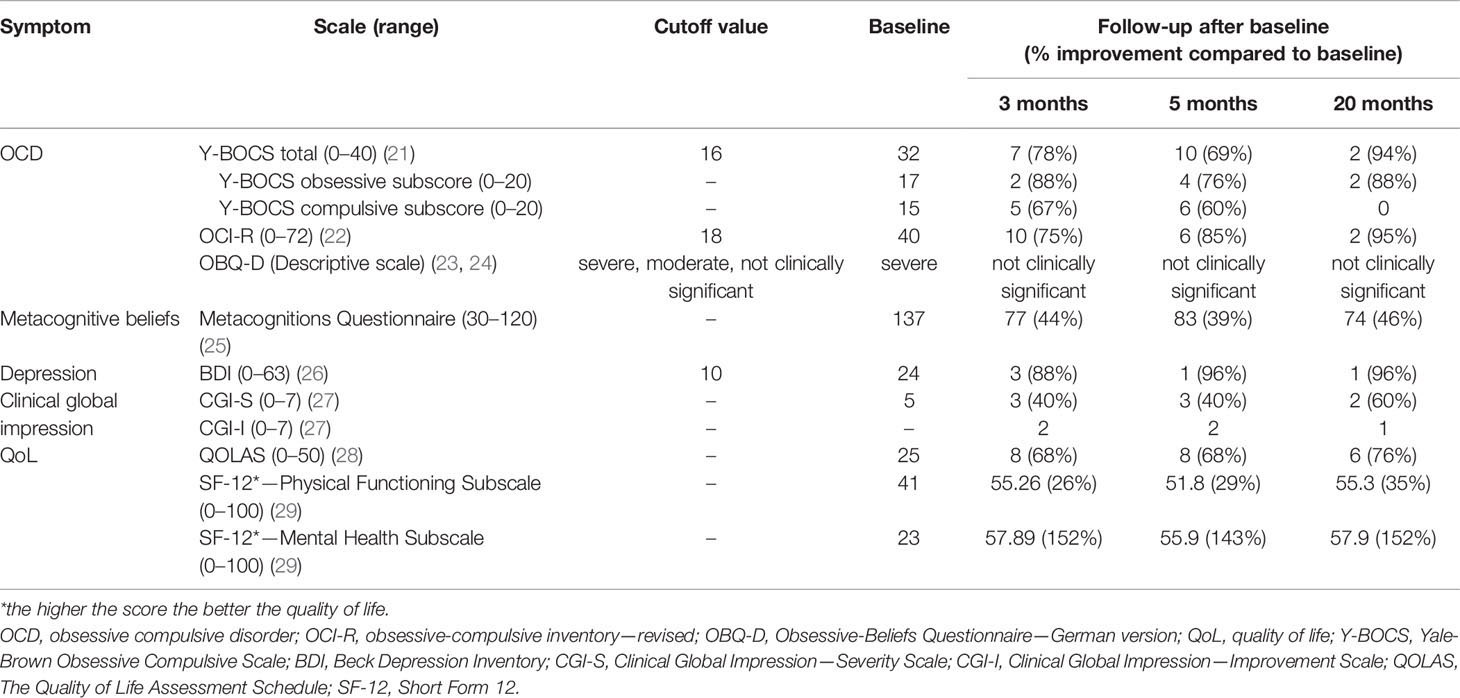
Table 1 Clinical assessments at baseline and at different time points after treatment with medicinal cannabis.
Evidence Supporting the Role of the ECS in the Pathophysiology of OCD: Data Obtained From Animal Studies
Most robust data suggesting an involvement of the ECS in the pathophysiology of OCD comes from animal studies. Although the most widely used animal model for OCD is marble burying based on the observation that rats and mice will bury either harmful or harmless objects in their bedding, this model is not ideal. Critics point out that the marble burying test reacts to two types of drugs, (S)SRIs and benzodiazepines, although benzodiazepines have no effects in patients suffering from OCD. Therefore, findings from this animal model should be interpreted with caution. Rueda-Orozco et al. (30) showed that administration of the anandamide receptor antagonist AM251 delays extinction of OCD-like behavior in a procedural memory task in rats presumably caused by impaired endocannabinoid activity in the dorsolateral striatum. Gomes et al. (31) used a mouse model and demonstrated that activation of CB1 receptors using WIN55.212-2 results in reduced OCD-like behavior as indicated by a significant decrease in the number of buried marbles. They also applied an inhibitor of the anandamide hydrolysis that led to decreased marble burying. Nardo et al. (32) described attenuating influence of CBD on marble-burying behavior in mice. After administration of meta-chloro-phenyl-piperazine (mCPP), a substance that enhances OCD, animals were treated either with CBD (30 mg/kg) or the SSRI fluoxetine (10 mg/kg) resulting in similar reducing effects on marble burying. In contrast, Umathe et al. (33) reported increased marble-burying behavior in mice after use of high doses of the endocannabinoid anandamide and its analogues AM404 or URB597, while low doses of these substances decreased marble-burying. Deiana et al. (34) determined pharmacokinetic profiles of several phytocannabinoids after acute single-dose intraperitoneal and oral administration in mice and rats. The pharmacodynamic-pharmacokinetic relationship of CBD (120 mg/kg, intraparenchymal and oral) was further assessed using a marble burying test in mice. All phytocannabinoids penetrated similarly the blood-brain barrier. In rats, oral administration of CBD inhibited marble burying matching its pharmacokinetic profile. Casarotto et al. (35) also showed inhibitory effects of CBD on marble burying behavior in C57BL/6J mice. Varvel et al. (36) conducted an interesting experiment aiming to test the hypothesis that elevated brain levels of anandamide may potentiate extinction in a fixed platform water maze task. They used mice genetically deprived of the enzyme fatty acid amide hydrolase (FAAH) that inactivates anandamide. Accordingly, mice treated with the FAAH inhibitor OL-135 did not display any memory impairment or motor disruption but did exhibit a significant increase in the rate of extinction. FAAH compromised mice exhibited a significant increase in acquisition rate. The authors concluded, that endogenous anandamide facilitates extinction through a CB1 receptor mechanism of action and FAAH inhibition represents a promising pharmacological approach to treat disorders such as OCD. Further evidence from the field of genetics was published by Imperatore et al. (37), who used a monoacylglycerol lipase (MAGL) knock-out mouse as a genetic model of congenital and sustained elevation of 2-arachidonoylglycerol (2-AG) levels in the brain. MAGL(−) mice demonstrated impaired CB1 signaling and anxiety-like behavior. Finally, Kinsey et al. (38) showed that inhibition of the endocannabinoid catabolic enzymes FAAH and MAGL elicits anxiolytic-like effects in the marble burying assay.
Studies in Patients With Pure OCD
Until today, only two case studies and one small controlled trial have been published reporting effects of CBM in a total of 14 patients with OCD (39–42). In 2008, Schindler et al. (41) described two patients with otherwise treatment-resistant OCD, who improved after adding dronabinol to preexisting treatments. The first patient was a 38-year-old woman with severe OCD and recurrent major depression, who had been treated with paroxetine (60 mg/d) and CBT with no improvement. Later on, therapy with clomipramine (300 mg/d) was initiated, which resulted only in a “partial response.” By chance, she discovered that smoking street cannabis improved her symptoms. Therefore, combined treatment with clomipramine and dronabinol (30 mg/per day) was started. After 10 days, OCD symptoms decreased by 50% (from 20 to 10 as measured by Yale-Brown Obsessive-Compulsive Scale, Y-BOCS). The second patient was a 36-year-old man with schizophrenia and OCD, who was admitted to hospital due to deterioration of psychotic and obsessive symptoms. The patient was previously treated with various antipsychotics such as haloperidol, olanzapine, risperidone, quetiapine, and aripiprazole as well as (S)SRIs without relevant effects. Even electroconvulsive therapy was performed without relevant improvement. After initiation of combined therapy with dronabinol (10 mg/d), clomipramine (150 mg/d) and clozapine (400 mg/d), OCD symptoms markedly improved within two weeks (from 23 to 15 according to Y-BOCS). Both patients reported no side effects.
In 2017, Cooper and Grant (40) reported about a 24-year-old male, who suffered a lacunar infarct of the left thalamus and thereafter developed persistent, repetitive, unwanted thoughts primarily related to doing unintentional harm or engaging in sexual acts with others. He had also a 10-year history of insulin-dependent diabetes and bipolar I disorder since age 16, which was stable on ziprasidone. His obsessions remained refractory to various agents used in monotherapy or combination (fluvoxamine, clomipramine, mirtazapine, risperidone, olanzapine, clozapine, ziprasidone, haloperidol, quetiapine, memantine, ondansetron, intravenous ketamine, N-acetylcysteine, gabapentin, clonazepam, plus mood stabilizing agents). Combination with dronabinol (20 mg/d) resulted in a marked improvement after two weeks of treatment (Y-BOCS score declined from 39 to 10) resulting in an amelioration of quality of life. In addition, for the first time he was able to tolerate CBT.
In 2020, the results of a trial were published using cannabinoid augmentation of exposure-based psychotherapy (EX) (39). Eleven unmedicated outpatients (18–60 years), who met DSM-5 criteria for OCD with at least moderate severity of symptoms (Y-BOCS ≥16), were assigned to either treatment with the synthetic THC analogue nabilone alone or a combination of nabilone+EX for 4 weeks. All participants received 1 mg nabilone twice a day orally. Nabilone was well tolerated, and no severe side effects occurred, but three participants withdrew because of increased anxiety. While monotherapy with nabilone resulted only in little symptom change (Y-BOCS decrease of 2.5 ± 3.6 after 4 months), combined treatment with nabilone+EX significantly improved the therapeutic effect of EX (Y-BOCS decrease of 11.2 ± 3.4) suggesting that nabilone can be used to augment treatment effects of EX in patients with OCD.
Studies in Patients With Tourette Syndrome and Comorbid Obsessive-Compulsive Behavior
Further evidence supporting beneficial effects of CBM in OCD comes from clinical studies in patients with Tourette syndrome (TS), a complex spectrum disorder characterized by motor and vocal tics. Up to 80% of patients with TS, in addition, suffer from psychiatric comorbidities, most frequently obsessive-compulsive behavior (OCB) and attention deficit/hyperactivity disorder (ADHD). While there is increasing evidence from retrospective surveys, case studies, and small randomized controlled trials (RCTs) that different CBM improve tics in patients with TS, in some of these studies, an improvement of OCB has also been described (43–48).
In a case study in a 16-year-old male with TS and comorbid OCB, rage attacks, sleeping problems, anxiety, and depression treatment with dronabinol (up to 33.6 mg/d) resulted in an improvement of both tics and psychiatric comorbidities including OCB (37). In a survey among adult patients with TS (39), 17 of 64 patients reported use of marijuana. Of these, 14 reported a reduction of tics and one a remission of OCB after use of cannabis. In a retrospective analysis efficacy and safety of smoked cannabis was investigated in 19 adults with TS (36). Of these, 15 patients were also diagnosed with comorbid OCD. In all of them, OCD improved according to Y-BOCS after starting treatment with cannabis. Only recently, results of a retrospective analysis (n=98) and an online survey (n=40) have been published in patients with TS, who had used different kinds of CBM including street cannabis, the cannabis extract nabiximols, dronabinol, and medicinal cannabis (38). In patients with comorbid OCD, improvement of OCD symptoms of 15% to 42% was reported.
In a single-dose RCT (n=12) using 5.0, 7.5, or 10 mg THC, a significant improvement of OCB was found compared to placebo (mean reduction of 4.83 ± 5.59 according to the Tourette Syndrome Symptom List (TSSL), p=0.041) (47). In contrast, in an RCT using up to 10 mg THC/d over 6 weeks in 24 patients no improvement of OCD was found (48). A summary of all studies in animal and humans is shown in Table 2.
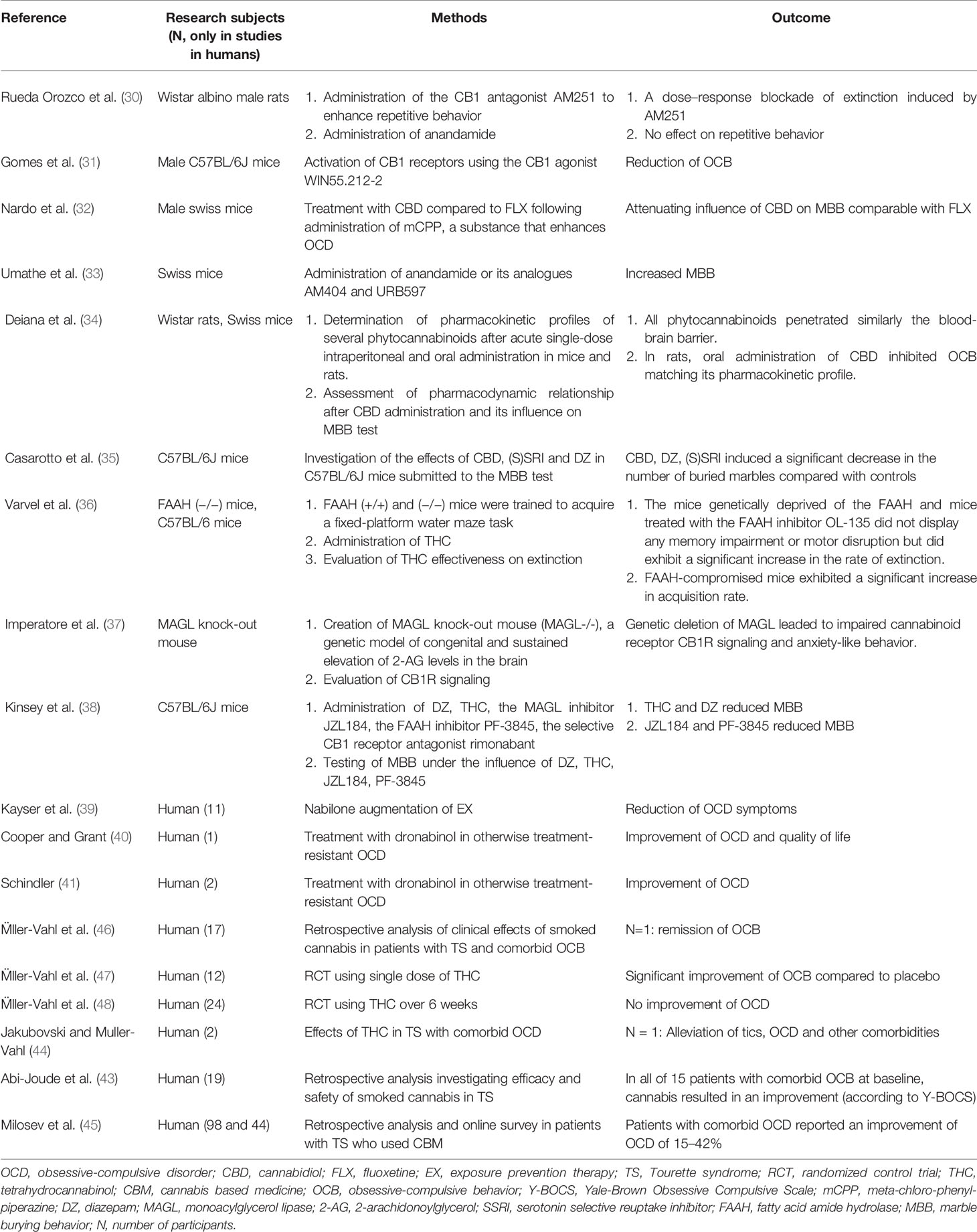
Table 2 Studies in animals and humans investigating the role of the endocannabinoid system (ESC) in OCD.
Discussion
The presented case report adds evidence to the hypothesis that modulation of the ECS by activating central CB1 receptors may improve OCD. Although in general our findings are in line with previous case reports (39–42), there are also some relevant differences: (i) while in all previous studies pure THC (dronabinol) or the synthetic analogue of THC, nabilone, have been used, our patient was treated with medicinal cannabis including more than 100 different cannabinoids; (ii) in previous case studies, preexisting treatment was augmented with CBM, while we used medicinal cannabis as monotherapy; and (iii) while all previously described patients were treatment resistant, in this case, the patient refused treatment with psychotherapy and had stopped medication with an (S)SRI due to adverse events after only one week. Thus, currently it is not only unclear whether CBM in general might be effective in the treatment of OCD, but also which cannabinoid or combinations of cannabinoids—and in particular the ratio of THC to CBD—is most effective and whether treatment with CBM should be used in monotherapy or in combination with (S)SRI or behavioral therapy.
Interestingly, neither our patient, nor those OCD patients described in the literature reported about clinically relevant adverse events. Most frequent adverse events associated with medically supervised treatment with THC and medicinal cannabis are dizziness, somnolence, drowsiness, problems with concentration, and tiredness, while severe adverse events occur only rarely. In general, CBM are well-tolerated, particularly when up-titrated slowly (49). It should be noted that our patient had used street cannabis (without negative effects) for several years, before treatment with medicinal cannabis was initiated. Thus, it cannot be excluded that CBM might be effective only in a subgroup of patients with OCD, who tolerate this kind of treatment well. In any case, before initiating treatment with CBM contraindications such as psychosis must be excluded, and patients must be informed about potential adverse events.
Currently, possible underling mechanisms of beneficial effects of CBM in OCD are unknown. However, it can be speculated that positive effects might be related to the well-known complex interplay between cannabinoids and serotonin (5-HT) function. In in vivo and in vitro studies, it has been demonstrated that cannabinoids modulate the activity of the 5-HT system at several levels. For example, it has been shown that activation of CB1 receptors affects the synthesis and release of 5-HT and that CB1 receptor agonists—depending on dose and duration of administration—either reduce or increase firing activity in 5-HT cells in the dorsal raphe nucleus [for review see: (50)]. Thus, based on the serotonin hypothesis of OCD, it can be speculated that CBM improves OCD by modulating the serotoninergic system. However, one might also speculate that OCD is caused by a dysfunction within the ECS. Accordingly, CBM might ameliorate OCD via direct activation of the ECS or indirectly by reducing anxiety (51) and stress (52). In line with this hypothesis, it has been demonstrated that chronic stress leads to a downregulation of CB1 receptor signaling in brain regions involved in OCD such as hippocampus, striatum, nucleus accumbens, prefrontal cortex, dorsal raphe nucleus, amygdala, and hypothalamus [for review see (18)]. Furthermore, an endogenous molecular mechanism has been identified in a specific cortico-striatal pathway that mediates the transition between goal-directed and habitual action strategies (53). Deletion of CB1 receptors from orbital frontal cortex neurons projecting to the dorsal striatum prevents mice from shifting from goal-directed to habitual action control suggesting that the emergence of habits depends on endocannabinoid-mediated attenuation.
However, we cannot entirely exclude that beneficial effects in the presented case are only caused by placebo effects and positive expectations or other possible confounders such as environmental, emotional or psychological factors that might have influenced OCD. It also cannot be ruled out that treatment with medicinal cannabis only indirectly influenced OCD symptoms by reducing stress or improving other symptoms such as anxiety, depression or sleeping problems.
Conclusion
There is increasing evidence that the ECS might be involved in the pathophysiology of OCD. In line with this hypothesis, from a limited number of case studies it is suggested that CBM might be effective in the treatment of OCD. However, so far it is unclear, which cannabinoids—in monotherapy of combination with other treatments—might be most effective and which patients might respond best.
Data Availability Statement
All datasets presented in this study are included in the article/supplementary material.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author Contributions
KM-V and CF conceived and designed the study and acquired data. CF set up the electronic database. KM-V, NS and CF interpreted the data and reviewed and edited the manuscript. KM-V and NS wrote the original draft of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: Classification and criteria changes. World Psychiatry (2013) 12(2):92–8. doi: 10.1002/wps.20050
2. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry (2010) 15(1):53–63. doi: 10.1038/mp.2008.94
3. Scahill L, Specht M, Page C. The Prevalence of Tic Disorders and Clinical Characteristics in Children. J Obsessive Compuls Relat Disord (2014) 3(4):394–400. doi: 10.1016/j.jocrd.2014.06.002
4. Mahjani B, Dellenvall K, Grahnat AS, Karlsson G, Tuuliainen A, Reichert J, et al. Cohort profile: Epidemiology and Genetics of Obsessive-compulsive disorder and chronic tic disorders in Sweden (EGOS). Soc Psychiatry Psychiatr Epidemiol (2020) 1–11. doi: 10.1007/s00127-019-01822-7
5. Del Casale A, Sorice S, Padovano A, Simmaco M, Ferracuti S, Lamis DA, et al. Psychopharmacological Treatment of Obsessive-Compulsive Disorder (OCD). Curr Neuropharmacol (2019) 17(8):710–36. doi: 10.2174/1570159X16666180813155017
6. Naguy A, Alamiri B. Treatment-resistant OCD—A psychopharmacological ‘touche d’art’. Asian J Psychiatr (2018) 34:98–9. doi: 10.1016/j.ajp.2018.04.025
7. Bloch MH, Green C, Kichuk SA, Dombrowski PA, Wasylink S, Billingslea E, et al. Long-term outcome in adults with obsessive-compulsive disorder. Depress Anxiety (2013) 30(8):716–22. doi: 10.1002/da.22103
8. Aouizerate B, Guehl D, Cuny E, Rougier A, Burbaud P, Tignol J, et al. Updated overview of the putative role of the serotoninergic system in obsessive-compulsive disorder. Neuropsychiatr Dis Treat (2005) 1(3):231–43. doi: 10.1016/j.pneurobio.2004.02.004
9. Boloc D, Mas S, Rodriguez N, Ortiz AE, Morer A, Plana MT, et al. Genetic Associations of Serotoninergic and GABAergic Genes in an Extended Collection of Early-Onset Obsessive-Compulsive Disorder Trios. J Child Adolesc Psychopharmacol (2019) 29(2):152–7. doi: 10.1089/cap.2018.0073
10. Winter L, Heitland I, Saryyeva A, Lutjens G, Schwabe K, Heissler HE, et al. Acute Effects of Electrical Stimulation of the Bed Nucleus of the Stria Terminalis/Internal Capsule in Obsessive-Compulsive Disorder. World Neurosurg (2018) 111:e471–e7. doi: 10.1016/j.wneu.2017.12.084
11. Simpson HB, Kegeles LS, Hunter L, Mao X, Van Meter P, Xu X, et al. Assessment of glutamate in striatal subregions in obsessive-compulsive disorder with proton magnetic resonance spectroscopy. Psychiatry Res (2015) 232(1):65–70. doi: 10.1016/j.pscychresns.2015.01.009
12. Bellini S, Fleming KE, De M, McCauley JP, Petroccione MA, D’Brant LY, et al. Neuronal Glutamate Transporters Control Dopaminergic Signaling and Compulsive Behaviors. J Neurosci (2018) 38(4):937–61. doi: 10.1523/JNEUROSCI.1906-17.2017
13. Ahmari SE, Spellman T, Douglass NL, Kheirbek MA, Simpson HB, Deisseroth K, et al. Repeated cortico-striatal stimulation generates persistent OCD-like behavior. Science (2013) 340(6137):1234–9. doi: 10.1126/science.1234733
14. Carmi L, Alyagon U, Barnea-Ygael N, Zohar J, Dar R, Zangen A. Clinical and electrophysiological outcomes of deep TMS over the medial prefrontal and anterior cingulate cortices in OCD patients. Brain Stimul (2018) 11(1):158–65. doi: 10.1016/j.brs.2017.09.004
15. Yun J-Y, Boedhoe PSW, Vriend C, Jahanshad N, Abe Y, Ameis SH, et al. Brain structural covariance networks in obsessive-compulsive disorder: a graph analysis from the ENIGMA Consortium. Brain J Neurol (2020) 143(2):684–700. doi: 10.1093/brain/awaa001
16. Abrams DI. The therapeutic effects of Cannabis and cannabinoids: An update from the National Academies of Sciences, Engineering and Medicine report. Eur J Intern Med (2018) 49:7–11. doi: 10.1016/j.ejim.2018.01.003
17. Meyer HC, Lee FS, Gee DG. The Role of the Endocannabinoid System and Genetic Variation in Adolescent Brain Development. Neuropsychopharmacology (2018) 43(1):21–33. doi: 10.1038/npp.2017.143
18. Lutz B, Marsicano G, Maldonado R, Hillard CJ. The endocannabinoid system in guarding against fear, anxiety and stress. Nat Rev Neurosci (2015) 16(12):705–18. doi: 10.1038/nrn4036
19. Garcia C, Palomo-Garo C, Gomez-Galvez Y, Fernandez-Ruiz J. Cannabinoid-dopamine interactions in the physiology and physiopathology of the basal ganglia. Br J Pharmacol (2016) 173(13):2069–79. doi: 10.1111/bph.13215
20. Casarotto P, Gomes F, Guimarães F. “Cannabinoids and obsessive-compulsive disorder", in Cannabinoids in Neurologic and Mental Disease. Elsevier (2015) pp. 365–87.
21. Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, et al. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen Psychiatry (1989) 46(11):1006–11. doi: 10.1001/archpsyc.1989.01810110048007
22. Foa EB, Kozak MJ, Salkovskis PM, Coles ME, Amir N. The validation of a new obsessive-compulsive disorder scale: The obsessive-compulsive inventory. Psychol Assess (1998) 10(3):206–14. doi: 10.1037/1040-3590.10.3.206
23. Obsessive Compulsive Cognitions Working Group. Psychometric validation of the Obsessive Beliefs Questionnaire and the Interpretation of Intrusions Inventory: Part I. Behav Res Ther (2003) 41(8):863–78. doi: 10.1016/S0005-7967(02)00099-2
24. Obsessive Compulsive Cognitions Working Group. Psychometric validation of the obsessive belief questionnaire and interpretation of intrusions inventory–Part 2: Factor analyses and testing of a brief version. Behav Res Ther (2005) 43(11):1527–42. doi: 10.1016/j.brat.2004.07.010
25. Wells A, Cartwright-Hatton S. A short form of the metacognitions questionnaire: properties of the MCQ-30. Behav Res Ther (2004) 42(4):385–96. doi: 10.1016/S0005-7967(03)00147-5
26. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
27. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont) (2007) 4(7):28–37. doi: 10.1016/S0300-7073(07)71474-3
28. Elstner K, Selai CE, Trimble MR, Robertson MM. Quality of Life (QOL) of patients with Gilles de la Tourette’s syndrome. Acta Psychiatr Scand (2001) 103(1):52–9. doi: 10.1111/j.1600-0447.2001.00147.x
29. Ware J Jr., Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care (1996) 34(3):220–33. doi: 10.1097/00005650-199603000-00003
30. Rueda-Orozco PE, Montes-Rodriguez CJ, Soria-Gomez E, Mendez-Diaz M, Prospero-Garcia O. Impairment of endocannabinoids activity in the dorsolateral striatum delays extinction of behavior in a procedural memory task in rats. Neuropharmacology (2008) 55(1):55–62. doi: 10.1016/j.neuropharm.2008.04.013
31. Gomes FV, Casarotto PC, Resstel LB, Guimaraes FS. Facilitation of CB1 receptor-mediated neurotransmission decreases marble burying behavior in mice. Prog Neuropsychopharmacol Biol Psychiatry (2011) 35(2):434–8. doi: 10.1016/j.pnpbp.2010.11.027
32. Nardo M, Casarotto PC, Gomes FV, Guimaraes FS. Cannabidiol reverses the mCPP-induced increase in marble-burying behavior. Fundam Clin Pharmacol (2014) 28(5):544–50. doi: 10.1111/fcp.12051
33. Umathe SN, Manna SS, Jain NS. Endocannabinoid analogues exacerbate marble-burying behavior in mice via TRPV1 receptor. Neuropharmacology (2012) 62(5-6):2024–33. doi: 10.1016/j.neuropharm.2011.12.030
34. Deiana S, Watanabe A, Yamasaki Y, Amada N, Arthur M, Fleming S, et al. Plasma and brain pharmacokinetic profile of cannabidiol (CBD), cannabidivarine (CBDV), Δ9;-tetrahydrocannabivarin (THCV) and cannabigerol (CBG) in rats and mice following oral and intraperitoneal administration and CBD action on obsessive-compulsive behaviour. Psychopharmacol (Berl) (2012) 219(3):859–73. doi: 10.1007/s00213-011-2415-0
35. Casarotto PC, Gomes FV, Resstel LB, Guimarães FS. Cannabidiol inhibitory effect on marble-burying behaviour: involvement of CB1 receptors. Behav Pharmacol (2010) 21(4):353–8. doi: 10.1097/FBP.0b013e32833b33c5
36. Varvel SA, Wise LE, Niyuhire F, Cravatt BF, Lichtman AH. Inhibition of Fatty-Acid Amide Hydrolase Accelerates Acquisition and Extinction Rates in a Spatial Memory Task. Neuropsychopharmacology (2007) 32(5):1032–41. doi: 10.1038/sj.npp.1301224
37. Imperatore R, Morello G, Luongo L, Taschler U, Romano R, De Gregorio D, et al. Genetic deletion of monoacylglycerol lipase leads to impaired cannabinoid receptor CB₁R signaling and anxiety-like behavior. J Neurochem (2015) 135(4):799–813. doi: 10.1111/jnc.13267
38. Kinsey SG, O’Neal ST, Long JZ, Cravatt BF, Lichtman AH. Inhibition of endocannabinoid catabolic enzymes elicits anxiolytic-like effects in the marble burying assay. Pharmacol Biochem Behav (2011) 98(1):21–7. doi: 10.1016/j.pbb.2010.12.002
39. Kayser RR, Raskin M, Snorrason I, Hezel DM, Haney M, Simpson HB. Cannabinoid Augmentation of Exposure-Based Psychotherapy for Obsessive-Compulsive Disorder. J Clin Psychopharmacol (2020) 40(2):207–10. doi: 10.1097/JCP.0000000000001179
40. Cooper JJ, Grant J. Refractory OCD Due to Thalamic Infarct With Response to Dronabinol. J Neuropsychiatry Clin Neurosci (2017) 29(1):77–8. doi: 10.1176/appi.neuropsych.16030053
41. Schindler F, Anghelescu I, Regen F, Jockers-Scherubl M. Improvement in refractory obsessive compulsive disorder with dronabinol. Am J Psychiatry (2008) 165(4):536–7. doi: 10.1176/appi.ajp.2007.07061016
42. Kayser RR, Snorrason I, Haney M, Lee FS, Simpson HB. The Endocannabinoid System: A New Treatment Target for Obsessive Compulsive Disorder? Cannabis Cannabinoid Res (2019) 4(2):77–87. doi: 10.1089/can.2018.0049
43. Abi-Jaoude E, Chen L, Cheung P, Bhikram T, Sandor P. Preliminary Evidence on Cannabis Effectiveness and Tolerability for Adults With Tourette Syndrome. J Neuropsychiatry Clin Neurosci (2017) 29(4):391–400. doi: 10.1176/appi.neuropsych.16110310
44. Jakubovski E, Muller-Vahl K. Speechlessness in Gilles de la Tourette Syndrome: Cannabis-Based Medicines Improve Severe Vocal Blocking Tics in Two Patients. Int J Mol Sci (2017) 18(8):1–6. doi: 10.3390/ijms18081739
45. Milosev LM, Psathakis N, Szejko N, Jakubovski E, Muller-Vahl KR. Treatment of Gilles de la Tourette Syndrome with Cannabis-Based Medicine: Results from a Retrospective Analysis and Online Survey. Cannabis Cannabinoid Res (2019) 4(4):265–74. doi: 10.1089/can.2018.0050
46. Muller-Vahl KR, Kolbe H, Schneider U, Emrich HM. Cannabinoids: possible role in patho-physiology and therapy of Gilles de la Tourette syndrome. Acta Psychiatr Scand (1998) 98(6):502–6. doi: 10.1111/j.1600-0447.1998.tb10127.x
47. Muller-Vahl KR, Schneider U, Koblenz A, Jobges M, Kolbe H, Daldrup T, et al. Treatment of Tourette’s syndrome with Delta 9-tetrahydrocannabinol (THC): a randomized crossover trial. Pharmacopsychiatry (2002) 35(2):57–61. doi: 10.1055/s-2002-25028
48. Muller-Vahl KR, Schneider U, Prevedel H, Theloe K, Kolbe H, Daldrup T, et al. Delta 9-tetrahydrocannabinol (THC) is effective in the treatment of tics in Tourette syndrome: a 6-week randomized trial. J Clin Psychiatry (2003) 64(4):459–65. doi: 10.4088/JCP.v64n0417
49. MacCallum CA, Russo EB. Practical considerations in medical cannabis administration and dosing. Eur J Intern Med (2018) 49:12–9. doi: 10.1016/j.ejim.2018.01.004
50. Cohen K, Weizman A, Weinstein A. Modulatory effects of cannabinoids on brain neurotransmission. Eur J Neurosci (2019) 50(3):2322–45. doi: 10.1111/ejn.14407
51. Hill MN, Sun JC, Tse MT, Gorzalka BB. Altered responsiveness of serotonin receptor subtypes following long-term cannabinoid treatment. Int J Neuropsychopharmacol (2006) 9(3):277–86. doi: 10.1017/S1461145705005651
52. Haring M, Grieb M, Monory K, Lutz B, Moreira FA. Cannabinoid CB(1) receptor in the modulation of stress coping behavior in mice: the role of serotonin and different forebrain neuronal subpopulations. Neuropharmacology (2013) 65:83–9. doi: 10.1016/j.neuropharm.2012.09.002
Keywords: obsessive-compulsive disorder, OCD, cannabinoids, cannabis-based medicine, endocannabinoid system, cannabis, depression
Citation: Szejko N, Fremer C and Müller-Vahl KR (2020) Cannabis Improves Obsessive-Compulsive Disorder—Case Report and Review of the Literature. Front. Psychiatry 11:681. doi: 10.3389/fpsyt.2020.00681
Received: 04 April 2020; Accepted: 29 June 2020;
Published: 21 July 2020.
Edited by:
Roberto Ciccocioppo, University of Camerino, ItalyReviewed by:
Kurt Leroy Hoffman, Autonomous University of Tlaxcala, MexicoAntonio Ferragud, University of Cambridge, United Kingdom
Copyright © 2020 Szejko, Fremer and Müller-Vahl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natalia Szejko, bmF0YWxpYS5zemVqa29Ad3VtLmVkdS5wbA==