 Stefan Sondermann
Stefan Sondermann Jörg Stahl1
Jörg Stahl1 Steffen Moritz
Steffen Moritz Jan Philipp Klein
Jan Philipp Klein
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 08 July 2020
Sec. Psychological Therapies
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.00652
This article is part of the Research Topic CBASP in the Treatment of Persistent Depressive Disorder View all 14 articles
Background: Deficits in social cognition, referred to as preoperational thinking, are assumed to play a key role in the pathogenesis of persistent depression. The aim of this study was to explore the effect of preoperational thinking on the two-year course of depressive symptoms in a sample of persistently depressed, episodically depressed as well as healthy participants.
Methods: We recruited 43 persistently depressed participants, 26 episodically depressed participants and 16 healthy control participants. Preoperational thinking was assessed at baseline with the Luebeck Questionnaire for Recording Preoperational Thinking. Over the period of two years, the course of depressive symptom severity was measured every three months using the Inventory of Depressive Symptomatology.
Results: Using linear mixed model analysis we found a significant effect for the influence of preoperational thinking on the severity of depressive symptoms in the observation period. We found a non-significant statistical trend for an association of preoperational thinking with the change of depressive symptom severity.
Conclusion: Our analyses suggest that a high degree of preoperational thinking is associated with a higher severity of depressive symptoms and possibly less symptom improvement. These findings support the notion that preoperational thinking is a relevant factor for the further course of depression and might indeed contribute to the maintenance of persistent depression.
Depressive disorders are frequent mental disorders and one of the main causes of years lived with disability (YLDs), implicating a high burden of disease (1). Approximately 20% of all patients with a depressive disorder develop a persistent depressive disorder (2, 3), with some studies even suggesting rates of up to 30% (4, 5). The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) summarizes the different forms of persistent depression under the diagnosis of persistent depressive disorder (PD). A common feature of all these subgroups is a duration of more than two years (6). A recent systematic review comparing patients with PD to patients with nonpersistent depression (ED) found more comorbidities, more suicide attempts and higher number of previous in- and outpatient treatments in patients with PD (7).
The European Psychiatric Association recommends the Cognitive–Behavioral Analysis System of Psychotherapy (CBASP) as first line psychotherapeutic treatment for persistent depression (8). CBASP was specifically developed for persistent depression (9) combining elements of cognitive behavioral therapy and interpersonal strategies. CBASP assumes that patients with early-onset PD have deficits in social cognition which emerge as a result of adverse childhood experiences (9). It has been observed that patients with PD show higher levels of alexithymia as well as more emotional and behavioral avoidance compared to patients with ED (7, 10), they have more interpersonal fears (11) and are perceived to be more hostile and submissive compared to a normative group as well as in comparison to patients with ED (12).
McCullough (9) suggests that deficits in social cognition should be the target of therapy for PD to improve patients’ ability to predict and learn from the consequences of their interpersonal behavior. To conceptualize this, the term preoperational thinking was coined, based on Piaget’s theory of cognitive development in children (13, 14). According to observations made by McCullough the cognitive style of patients with PD is similar to preoperational children between the age of two to seven years (9). He describes their thinking as prelogical and precausal, with them being caught in the assumption that all others will respond to them in the same way and in their view, they will always feel like they feel in the present (9). The loss of perspective, to see responses of others as one among many types, is part of the experience that current events are a mere replay of the past. These characteristics are aptly summarized in a patient statement that says: “Whatever I do, nothing will ever change.” (9, 11). Another illustration is given by McCullough, who reports a dialog between therapist and patient about an interpersonal conflict, which resulted in the patients statement: “Why are you taking his side? You`re just like all the others—no one understands me.” (9). This preoperational thinking is assumed to be the reason for the interpersonal problems in patients with PD because it makes it difficult for them to learn from the actual experience of interpersonal encounters.
Studies that used theory of mind exercises to capture this deficit in social cognition did not find these deficits in patients with persistent depression. In conclusion, Köhler et al. (7) describe the evidence as scarce, with only some evidence for differences between depressed patients in general compared to healthy controls (15–17). Our study aims to provide a more detailed view of social cognition by using a measure developed specifically for preoperational thinking and examining its association with the long-term course of depressive symptoms both in patients and healthy controls. Previous studies using this measure have shown higher levels of preoperational thinking in patients with PD compared to patients with ED or healthy controls (11, 18, 19). Preoperational thinking was also linked to childhood maltreatment with a mediating effect of interpersonal fears (11), as well as mediating the association of childhood maltreatment and a hostile interpersonal style (20).
We did not find existing studies that analyzed the association of preoperational thinking with the course of persistent depression over time. We have therefore conducted a longitudinal study to test the association between baseline preoperational thinking and the two-year course of depressive symptoms. Based on the observation that patients with PD exhibit a higher level of preoperational thinking we hypothesized that preoperational thinking negatively affects the course of depressive symptoms. We were interested if preoperational thinking was associated to the mean levels of depressive symptoms as well as to the change in depressive symptoms in this period.
We present a prospective, observational, longitudinal study comparing three groups of participants who were matched for age and sex: participants with PD, participants with ED and participants as healthy controls (HC). This study sample was put together from two cross-sectional studies. The first of these (21) recruited depressed participants from in- and outpatient settings, as well as healthy controls via local advertisements. The second study (22, 23) recruited patients with depression in a day clinic setting. All participants provided informed consent before enrolling. The ethics committee at the University of Lübeck (Germany) approved the study.
General inclusion criteria were the same as in the underlying studies: Age between 18 and 65 years and adequate proficiency of the German language. Exclusion criteria were somatic conditions requiring acute treatment as well as diagnoses of schizophrenia, schizotypal disorder, bipolar disorder, delusional disorder or substance use disorder. Further criteria for the group of HCs were absence of current mental disorder and no history of psychiatric treatment.
Group assignment was based on a diagnostic interview according to DSM-5 criteria (24) conducted by a trained psychologist for all patients. The group of PD was composed of participants who met the criteria of persistent depressive disorder with: (1) major depressive episode longer than two years without remission; (2) dysthymia; (3) intermittent major depressive episodes with current episode; (4) intermittent major depressive episodes, without current episodes. The group of ED included participants with: (1) a major depressive episode less than 2 years; or (2) a major depressive episode, currently in remission.
Recruitment of study 1 took place between November 2014 and May 2016, while participants in study 2 were recruited between May 2016 and July 2016. In summary, 144 participants of study one and two were invited to participate in this follow-up study; of these, 85 consented to take part (Figure 1). The group sizes were 43 participants in group PD, 26 participants in group ED and 16 participants as healthy controls. To test for a systemic bias caused by participants who did not participate, lost to follow-up analyses were performed. Lost to follow-up was defined as a participant who took part less than two times (participation ≤1) after baseline testing. In this analysis all patients who were asked to participate (N = 144) were included. The resulting groups showed no significant differences in the baseline variables of age, diagnosis, gender, secondary education, IDS score and LQPT score (all p-values ≥0.21). For full detail of lost to follow-up analysis see Supplementary Table 1.

Figure 1 Participant flow with participation rates for each point in time. ED, Episodic depression; HC, Healthy controls; PD, Persistent depression.
The Luebeck Questionnaire for Recording Preoperational Thinking (LQPT;19) was used to measure preoperational thinking. Following the description of a short social situation, the participants should respond how they would react in the given situation. It presents a choice between two responses: either indicating a high or a low level of preoperational thinking. For example, in item number 14 a meeting with a new acquaintance is cancelled on short notice by another person. The participant is asked how they would respond to the given situation; they can chose between the following responses: “The acquaintance wouldn’t have liked me anyway” indicates a higher level of preoperational thinking while “Too bad it was cancelled, I will call again another time” is indicative of a lower level of preoperational thinking. The LQPT contains 20 items, a low total score shows a high level of preoperational thinking. Recent studies reported the LQPT to be a reliable and valid measure with an excellent internal consistency [Cronbach’s alpha 0.901 (19, 21, 25)].
As measurement of the severity of depressive symptoms the Inventory of Depressive Symptomatology, Self-Report (IDS-SR, subsequently abbreviated as IDS (26); was used in its German version (27). It was chosen due to its psychometric properties and its easy administration (26, 28, 29). Multiple studies reported the IDS to be a reliable instrument with Cronbach’s alpha coefficients between 0.79 and 0.94 (26, 28, 30).
Further measures used included the DSM-5 based diagnostic interview (24), a demographic questionnaire on age, gender and education, and a short questionnaire about past health care utilization. All measures were used at baseline testing. Subsequently, all participants were notified every three months via email over a course of two years to complete the IDS and the questionnaire about health care utilization. In total, this resulted in eight time points of data collection beyond baseline assessment.
All data analyses were performed using SPSS 26 (IBM Corporation, Armonk, NY, USA). Significance levels for all statistical tests were set at p ≤.05. Group comparisons are conducted using ANOVAs and t-tests for data with normal distribution and for non-normalized distributed data Kruskal–Wallis tests and Mann–Whitney U tests. The main hypothesis was tested using linear-mixed models (LMM) as they have the advantage of using all available data of each participant. LMM analyses also offer the opportunity to choose an appropriate covariance structure reflecting the potential dependence due to repeated measurements (31). No missing values were substituted in any of the statistical analyses as mixed model analyses based on all observed data are valid and unbiased methods for data missing at random (MAR) (32). In the first analysis, the IDS total score served as dependent variable and was analyzed with time and baseline LQPT as fixed effect. A first order autoregressive structure with homogeneous variances (AR1) was chosen based on Akaike’s Information Criterion (AIC) from a fixed set of candidate structures, namely a first order autoregressive (AR1) with either homogeneous or heterogeneous variances; diagonal or scaled identity structure. In a subsequent analysis, we entered time, baseline LQPT, and group as fixed effects with the IDS total score serving as dependent variable. We conducted a third analysis with IDS change at outcome corrected for baseline IDS score as dependent variable and time, baseline LQPT and baseline IDS as fixed effects.
Demographics and baseline characteristics are shown in Table 1. Participants did not differ significantly in age or gender across groups. HC participants had a higher secondary education than participants of the other groups. Significant group differences between all groups were found in LQPT scores, as well as IDS results with mostly large effect sizes. Health care utilization differed between groups with HC participants having lower utilization in comparison to the other groups except for doctor visits of other, non-specified specialties.
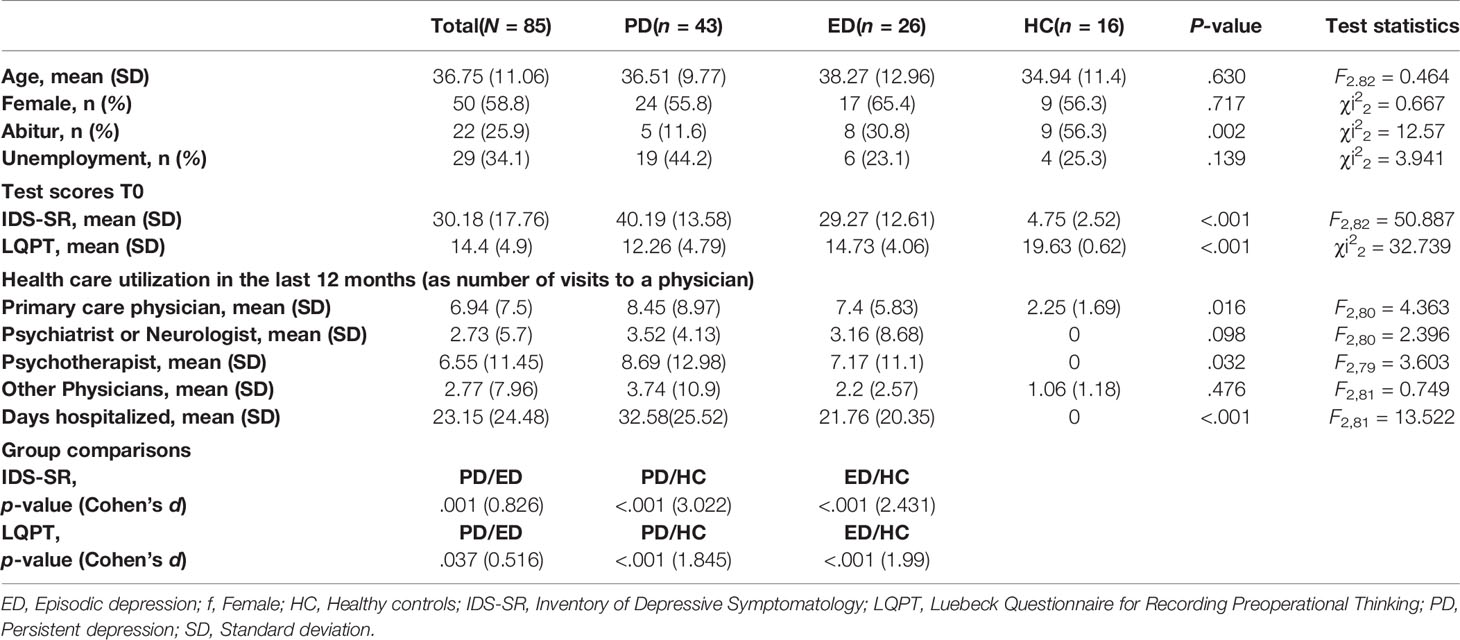
Table 1 Sociodemographic data and Baseline test scores with group comparisons.
Participation rate of 56.2% was achieved. Initially at three months (T1) participation rate was 68.2% which decreased over time to a participation rate of 48.2% at the last time point after two years (T8). For full details of participation refer to Figure 1. Data from two participants were excluded because of double participation (one instance at T5 and a separate instance at T6). In these cases, only the results of the first participation at each date were considered.
Figure 2 shows the course of depressive symptoms for each group. At all points in time, patients with PD showed higher scores than those with ED who in turn had higher scores than HCs. In multigroup comparisons via ANOVA, significant group differences were found for all time points (for time points T5 and T7, Kruskal–Wallis tests were calculated because the normality assumption was violated). In post-hoc analyses, we found that each of the groups (PD, ED, HC) differed from all the others, except for non-significant differences between PD and ED at T4 (t(35) = 1.875, p = .069), T5 (Mann–Whitney U test: U = 83,000, p = .109) and T8 (t(28) = 1.738, p = .093).
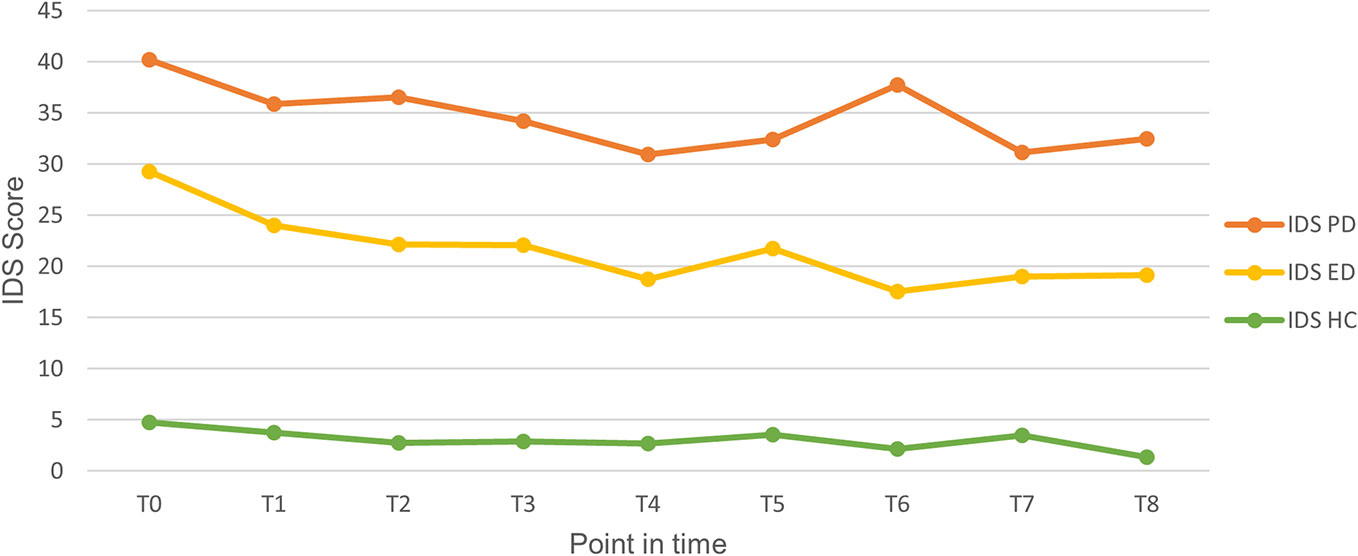
Figure 2 Course of depressive symptom severity for each point in time in the period of two years. ED, Episodic depression; HC, Healthy controls; IDS, Inventory of Depressive Symptomatology; PD, Persistent depression.
At all follow-up assessment time points, participants were asked to report their utilization of health care resources in the last three months. At nearly all time points, the three groups differed in the number of visits to a primary care physician (all p-values <.011, except for T2, T5, T7 and T8), to a neurologist or psychiatrist (all p-values <.045, except for T2, T4, and T8) and to a psychotherapist (all p-values <.041). For all the analyses with a significant global effect, post-hoc testing revealed that patients with PD had the highest number of visits (except for the category “neurologist or psychiatrist” at T1; here, patients with ED had more visits than patients with PD). Patients with PD were the only group reporting hospitalizations after the second assessment. The visits at physicians of other specialties showed heterogeneous results.
In our first LMM analysis, we found a significant effect of the LQPT on IDS (F1,94 = 96.886, p <.001), and of time on the IDS (F1,318 = 17.534, p <.001). This implies that preoperational thinking is associated with the severity of depressive symptoms in the observation period. In the second LMM analysis we added diagnosis group to the fixed effects. We found significant effects of diagnosis (F2,101 = 18.003, p <.001), time (F1,288 = 15.811, p <.001) and LQPT (F1,108 = 28.192, p <.001) on the IDS. Average IDS-scores over the observation period were 1.46 points higher (CI: 0.91, 2.00) for each point decrease in the LQPT-Score. This shows that level of preoperational thinking at baseline is associated to average symptom severity over the observation period even after correcting for diagnosis. In our third analysis, we found a statistical trend for the association of LQPT to change in IDS corrected for baseline IDS (F1,78 = 3.344, p = .071) and significant effects of time (F1,232 = 8.259, p = .004) and baseline IDS (F1,75 = 14.228, p <.001). The estimated effects of the LQPT are a 0.66 (CI: −0.06, 1.38) higher change in IDS score for each point increase in LQPT score and are higher but with wider confidence intervals than those of the baseline IDS on IDS change (0.36 (CI:0.17, 0.55)).
Table 2 shows the full results of the statistical analyses. For a graphical illustration of the analysis, please refer to Figure 3 where we have plotted a separate line for the course of depressive symptom severity for each participant with color coding dependent on LQPT scores.
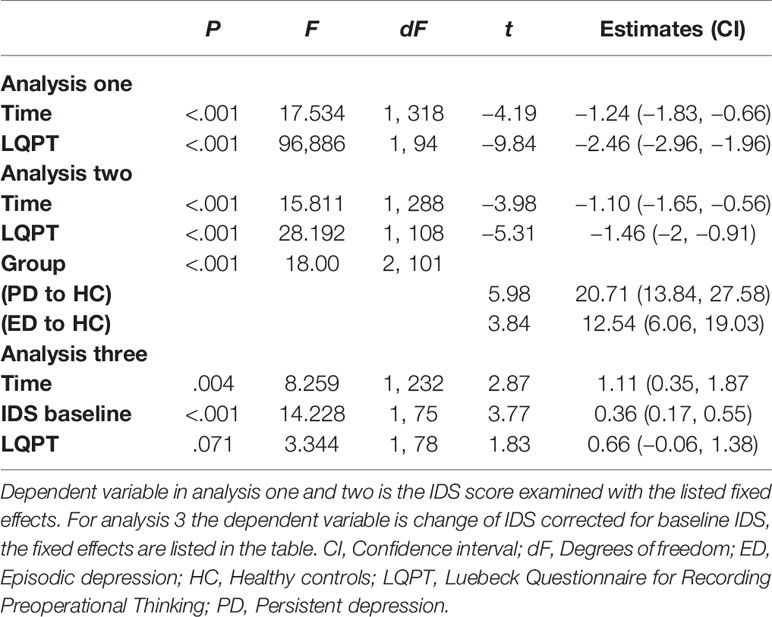
Table 2 Results of linear mixed model analyses.
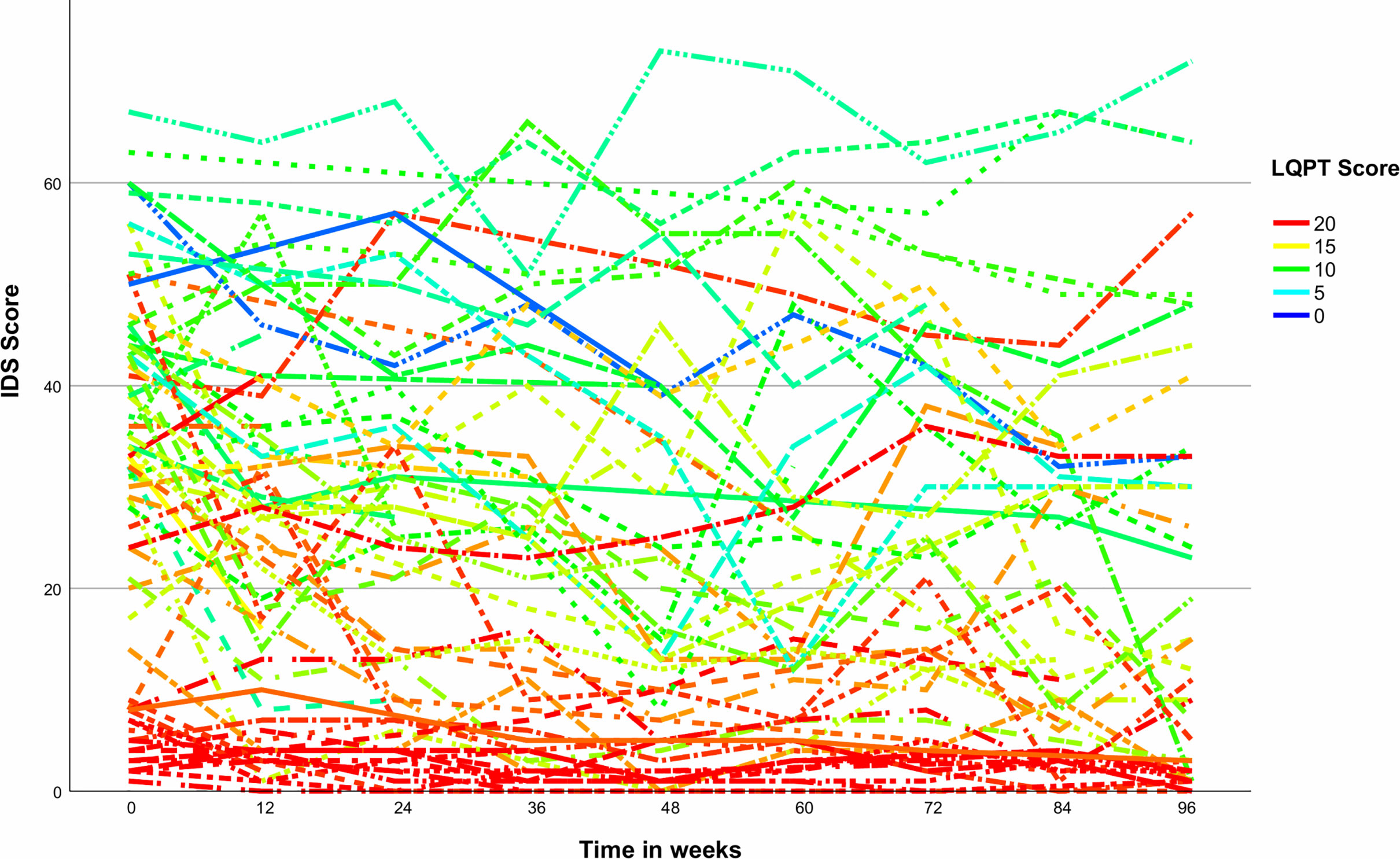
Figure 3 Individual courses of depressive symptoms over time with color coding dependent on level of preoperational thinking. IDS, Inventory of Depressive Symptomatology; LQPT, Luebeck Questionnaire for Recording Preoperational Thinking.
In this study, we examined the influence of preoperational thinking on depressive symptom severity over two years. We found that participants with higher levels of preoperational thinking had a higher baseline symptom severity than participants with lower levels of preoperational thinking. This effect was independent of the diagnosis of PD, suggesting that it might indeed be preoperational thinking and not only a baseline diagnosis of PD that contributes to higher depressive symptoms over the observation period. While we did find a statistical trend, we did not find a significant effect of preoperational thinking on the change of depressive symptom severity over the course of two years. This could suggest that baseline preoperational thinking helps explain changes of depressive symptoms, with higher levels of preoperational thinking leading to less symptom improvement.
Depressive symptoms declined most sharply between baseline and three months later. Reductions in depressive symptoms were modest after that period. This observation is in keeping with previous studies (33, 34), in particular Spijker et al. (35) who showed that rates of remission were highest within the first three months following therapy. As expected, the group of healthy controls exhibited no symptom severity that would indicate depression.
We found higher symptom severity in the group PD at all points in time which ties in well with other studies reporting a higher symptom severity in patients with PD (36, 37). A review comparing PD to non-PD patients concludes that available studies show inconsistent results with about one third of the sources showing higher symptom severity in PD, only a minority showing higher symptom severity in ED but many studies reporting no differences in symptom severity (7). Use of healthcare resources differed across groups with group PD having higher utilization mostly in the categories of visits at a primary care physician, at a neurologist or psychiatrist and visits at a psychotherapist compared to participants of group ED and HC. This higher utilization is consistent with previous studies indicating more treatment as well as longer history of treatment in patients with PD (7).
The differences in level of preoperational thinking at baseline for the groups PD and ED are consistent with other studies (18, 19). We did find a significant group difference, with the group PD showing higher levels of preoperational thinking than the other groups, whereas the group of ED showed significant higher levels of preoperational thinking in comparison to the group HC. Our results show that higher levels of preoperational thinking are associated with higher depressive symptom severity over time. These results are consistent with the view that deficits in social cognition are relevant for the course of depression. The trend we found for the association of baseline LQPT with change in IDS (corrected for baseline IDS) should be examined further by subsequent studies. Our effect estimates suggest a small effect that appears to be stronger than the effect of baseline IDS score on the IDS change. Considering the wider confidence intervals, the true effect size could be weaker or stronger.
Other studies have already demonstrated that social cognition may be associated with symptom severity in episodic depression. In a recent meta-analysis by Bora and Berk patients with ED differed in theory of mind skills from healthy controls; the level of impairment was related to symptom severity (38). Our results are consistent with the assumptions of CBASP about persistent depression, in particular, that preoperational thinking is a factor contributing to the maintenance of depression and thus plays a key role in its formation. Constantino et al. observed in a study of persistently depressed patients that a decrease of hostile-submissive interpersonal impact messages under therapy was associated with a greater reduction of depressive symptoms over time (39). These findings are consistent with recent results by Klein et al. showing that the association between treatment and outcome was mediated through the reduction of interpersonal problems, in their study measured as change in social inhibition and the improvement of the therapeutic alliance (40). This implies that treatment-induced improvements in interpersonal skills positively affect the course of depression.
The association of preoperational thinking with depressive symptom severity was not specific to patients with PD. Further studies should measure the levels of preoperational thinking repeatedly in addition to depressive symptom severity. This may help to confirm that higher levels of preoperational thinking are associated with higher depressive symptom severity over time in both patients with PD and ED. That approach with a larger sample size would also allow to examine if the statistical trend for association of baseline LQPT to change in IDS is replicable. A possible design could follow the approach of Faissner et al., who used a latent growth model with repeated measurement of cognitive and metacognitive maladaptive beliefs (41). Furthermore, the role of other variables possibly associated with preoperational thinking could also be addressed in a further study. These additional variables include alexithymia (42), because alexithymia has also been associated with interpersonal problems in depression (43). Another potential variable is attachment because both alexithymia and attachment styles (44, 45) have been shown to mediate the association between childhood maltreatment and depression in separate studies (44).
The prospective longitudinal design of this study enabled us to examine the relationship between the interindividual differences at baseline and the intraindividual changes in depressive symptom severity over two years. The recruitment of two groups with different forms of depression and a group of healthy controls is another strength of this study. Lost to follow-up analyses did not indicate a systematic bias. A possible source of heterogeneity in the group PD relates to group assignment. In our study we divided depressive participants in persistent versus episodic depression based on DSM-5 criteria (6); the group of persistent depression thus included participants with dysthymia alongside participants with PD with current major depressive episode. In line with observations by Klein et al. (42, 46) we decided to use the DSM-5 based assignment because of the similarities between the subgroups of dysthymic and persistent depression with major depressive disorder over the course of time. A possible problem based in the study design is that we did not test for transition of an episodic depression into a persistent depression. The rate of chronification is estimated to be around 15 to 20% (3), with some studies suggesting even higher rates of around 30% (4). This could potentially skew our results and minimize the differences of the depressive groups, if some participants of the group ED had developed a persistent depression across the observation period. Contrary to this we did find significant differences between the group’s PD and ED at six out of nine points in time.
Main limitations of this study are the small group size and the low participation rate of the included participants. One of the possible causes for this is the non-personal approach via E-Mail. Fricker et al. (43, 47) showed higher participation rates with telephone surveys in comparison to internet survey even if higher incentives where offered in the internet survey. Another possible problem of E-Mail based data collection is failed contacting due to anti-spam procedures of providers. Advantages of an internet survey and in this case contacting via E-Mail is the direct acquisition of data which prevents transmission errors and the flexibility and time savings for participant and investigator. As Weightman et al. (48) mention, a problem in studies on social cognition is the multitude of different tools and constructs which lead to a limited comparability across different studies. To the best of our knowledge only Ladegaard et al. (49) examined the course of social cognition abilities in depression. In a sample of patients with a first episode of major depression, they found an improvement of these skills with symptom remission (49). Another limitation is the unbalanced number of participants in the three groups, which was probably a result of already imbalanced group sizes in the two studies from which the participants were recruited. Still, lost to follow-up rates were similar across groups. It is also unclear to what extent the treatment received by study participants affected the course of their depression.
Our study suggests that preoperational thinking is associated with symptom severity across the course of depression and possibly with the change of symptom severity, further supporting the evidence for the role of social cognition in the pathogenesis of persistent depression. Other studies should try to verify this association to give a better understanding of social cognition, the extent of its effects on depressive disorders and help identify what kind of deficits distinguish patients with depressive disorders from others.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics committee University of Lübeck. The patients/participants provided their written informed consent to participate in this study.
Conception and design: JK with support from SS. Acquisition of data: Study 1—JS and SS, Study 2—UG and JO. Follow-up study: SS with support from SM and JK. Analysis and interpretation of data: SS and JK. Drafting of manuscript: SS with support from JK and SM. All authors contributed to the article and approved the submitted version.
We acknowledge financial support by Land Schleswig-Holstein within the funding programme Open Access Publikationsfonds. No other funding was received.
JK received funding for clinical trials (German Federal Ministry of Health, Servier), payments for lectures on Internet interventions (Servier) and payment for workshops and books (Beltz, Elsevier, Hogrefe, Springer) on psychotherapy of chronic depression and psychiatric emergencies.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank all participants for their participation in the study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00652/full#supplementary-material
CBASP, Cognitive–Behavioral Analysis System of Psychotherapy; CI, Confidence interval; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ED, Episodic depression; HC, Healthy controls; IDS-SR, Inventory of Depressive Symptomatology—Self-rated version; LMM, Linear-mixed models; LQPT, Luebeck Questionnaire for Recording Preoperational Thinking; PD, Persistent depression.
1. GBD. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (Lond Engl) (2018) 392(10159):1789–858. doi: 10.1016/S0140-6736(18)32279-7
2. Gilmer WS, Trivedi MH, Rush AJ, Wisniewski SR, Luther J, Howland RH, et al. Factors associated with chronic depressive episodes: a preliminary report from the STAR-D project. Acta Psychiatr Scand (2005) 112(6):425–33. doi: 10.1111/j.1600-0447.2005.00633.x
3. DGPPN B, KBV AWMF. (Hrsg.). S3-Leitlinie / Nationale VersorgungsLeitlinie Unipolare Depression. Vol. 2. Auflage. DGPPN, BÄK, KBV, AWMF. (2015). https://www.awmf.org/leitlinien/detail/ll/nvl-005.html; https://www.leitlinien.de/mdb/downloads/nvl/depression/depression-2aufl-vers5-lang.pdf
4. Murphy JA, Byrne GJ. Prevalence and correlates of the proposed DSM-5 diagnosis of Chronic Depressive Disorder. J Affect Disord (2012) 139(2):172–80. doi: 10.1016/j.jad.2012.01.033
5. Satyanarayana S, Enns MW, Cox BJ, Sareen J. Prevalence and correlates of chronic depression in the Canadian Community Health Survey: Mental health and well-being. Can J Psychiatry (2009) 54(6):389–98. doi: 10.1177/070674370905400606
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Arlington, Virginia: American Psychiatric Association (2013).
7. Köhler S, Chrysanthou S, Guhn A, Sterzer P. Differences between chronic and nonchronic depression: Systematic review and implications for treatment. Depress Anxiety (2019) 36(1):18–30. doi: 10.1002/da.22835
8. Jobst A, Brakemeier EL, Buchheim A, Caspar F, Cuijpers P, Ebmeier KP, et al. European Psychiatric Association Guidance on psychotherapy in chronic depression across Europe. Eur Psychiatry (2016) 33(1):18–36. doi: 10.1016/j.eurpsy.2015.12.003
9. McCullough JP. Treatment for chronic depression: cognitive behavioral analysis system of psychotherapy (CBASP) Vol. 326. New York: Guilford Press (2000).
10. van Randenborgh A, Hüffmeier J, Victor D, Klocke K, Borlinghaus J, Pawelzik M. Contrasting chronic with episodic depression: An analysis of distorted socio-emotional information processing in chronic depression. J Affect Disord (2012) 141(2–3):177–84. doi: 10.1016/j.jad.2012.02.039
11. Klein JP, Stahl J, Hüppe M, McCullough JP, Schramm E, Ortel D, et al. Do interpersonal fears mediate the association between childhood maltreatment and interpersonal skills deficits? A matched cross-sectional analysis. Psychother Res (2020) 30(2):267–78. doi: 10.1080/10503307.2018.1532125
12. Bird T, Tarsia M, Schwannauer M. Interpersonal styles in major and chronic depression: A systematic review and meta-analysis. J Affect Disord (2018) 239:93–101. doi: 10.1016/j.jad.2018.05.057
13. Piaget J. The Language and Thought of the Child. London: Kegan Paul, Trench, Trubner & co, ltd. (1926). p. 246.
14. Piaget J. Part I: Cognitive development in children: Piaget development and learning. J Res Sci Teach (1964) 2(3):176–86. doi: 10.1002/tea.3660020306
15. Wilbertz G, Brakemeier EL, Zobel I, Härter M, Schramm E. Exploring preoperational features in chronic depression. J Affect Disord (2010) 124(3):262–9. doi: 10.1016/j.jad.2009.11.021
16. Zobel I, Werden D, Linster H, Dykierek P, Drieling T, Berger M, et al. Theory of mind deficits in chronically depressed patients. Depress Anxiety (2010) 27(9):821–8. doi: 10.1002/da.20713
17. Wolkenstein L, Schönenberg M, Schirm E, Hautzinger M. I can see what you feel, but i can’t deal with it: Impaired theory of mind in depression. J Affect Disord (2011) 132(1–2):104–11. doi: 10.1016/j.jad.2011.02.010
18. Klein JP, Kensche M, Becker-Hingst N, Stahl J, Späth C, Mentler T, et al. Development and psychometric evaluation of the Interactive Test of Interpersonal Behavior (ITIB): A pilot study examining interpersonal deficits in chronic depression. Scand J Psychol (2016) 57(1):83–91. doi: 10.1111/sjop.12222
19. Kühnen T, Knappke F, Otto T, Friedrich S, Klein JP, Kahl KG, et al. Chronic depression: Development and evaluation of the luebeck questionnaire for recording preoperational thinking (LQPT). BMC Psychiatry (2011) 11(1):199. doi: 10.1186/1471-244X-11-199
20. Klein JP, Grasshoff L, Hermanns R, Haeger S, Sondermann S, Kühnen T, et al. Präoperatorisches Denken bei Patienten mit Angststörung oder Chronischem Rückenschmerz: Zwei Querschnittsstudien zum besseren Verständnis des Cognitive Behavioral Analysis System of Psychotherapy (CBASP). Z für Psychiatr Psychol und Psychother (2020) 68(3):1–9. doi: 10.1024/1661-4747/a000418
21. Stahl J. Evaluation eines interaktiven Testsystems zur Erfassung interpersonellen Verhaltens „ Interactive Test of Interpersonal B ehaviour “ ITIB. [thesis]. University of Lübeck (2018). p. 155.
22. Outzen J. Changes in Interpersonal and Metacognitive Skills during a Day Clinic Treatment in Patients with Depression [master’s thesis]. Universität zu Lübeck (2016). p. 149.
23. Grave U. Depressionsrelevante Fertigkeitsdefizite bei chronischer Depression Depressionsrelevante Fertigkeitsdefizite bei chronischer Depression [master’s thesis]. Universität zu Lübeck (2016). p. 23.
24. Klein JP, Belz M. Psychotherapie Chronischer Depression. Praxisleitfaden CBASP. Göttingen: Hogrefe (2014).
25. Sargin AE, Uca O, Kose S, Türkçapar H. Reliability, validity, and factorial structure of the Turkish version of the Luebeck questionnaire for recording preoperational thinking (Turkish LQPT). Psychiatry Clin Psychopharmacol (2018) 28(2):191–8. doi: 10.1080/24750573.2017.1411575
26. Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive Symptomatology (IDS): psychometric properties. Psychol Med (1996) 26(3):477–86. doi: 10.1017/S0033291700035558
27. Drieling T, Schärer LO, Langosch JM. The Inventory of Depressive Symptomatology: German translation and psychometric validation. Int J Methods Psychiatr Res (2007) 16(4):230–6. doi: 10.1002/mpr.226
28. Trivedi MH, Rush AJ, Ibrahim HM, Carmody TJ, Biggs MM, Suppes T, et al. The Inventory of Depressive Symptomatology, Clinician Rating (IDS-C) and Self-Report (IDS-SR), and the Quick Inventory of Depressive Symptomatology, Clinician Rating (QIDS-C) and Self-Report (QIDS-SR) in public sector patients with mood disorders: a psych. Psychol Med (2004) 34(1):73–82. doi: 10.1017/S0033291703001107
29. Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry (2003) 54(5):573–83. doi: 10.1016/S0006-3223(02)01866-8
30. Corruble E, Legrand JM, Duret C, Charles G, Guelfi JD. IDS-C and IDS-SR: Psychometric properties in depressed in-patients. J Affect Disord (1999) 56(2–3):95–101. doi: 10.1016/S0165-0327(99)00055-5
31. Gueorguieva R, Krystal JH. Move over ANOVA: Progress in Analyzing Repeated-Measures Data and Its Reflection in Papers Published in the Archives of General Psychiatry. Arch Gen Psychiatry (2004) 61(3):310–7. doi: 10.1001/archpsyc.61.3.310
32. Bell ML, Fiero M, Horton NJ, Hsu C-H. Handling missing data in RCTs; a review of the top medical journals. BMC Med Res Methodol (2014) 14(1):118. doi: 10.1186/1471-2288-14-118
33. Stegenga BT, Kamphuis MH, King M, Nazareth I, Geerlings MI. The natural course and outcome of major depressive disorder in primary care: The PREDICT-NL study. Soc Psychiatry Psychiatr Epidemiol (2012) 47(1):87–95. doi: 10.1007/s00127-010-0317-9
34. Comijs HC, Nieuwesteeg J, Kok R, van Marwijk HW, van der Mast RC, Naarding P, et al. The two-year course of late-life depression; results from the Netherlands study of depression in older persons. BMC Psychiatry (2015) 15(1):1–9. doi: 10.1186/s12888-015-0401-5
35. Spijker J, de Graaf R, Bijl RV, Beekman ATF, Ormel J, Nolen WA. Duration of major depressive episodes in the general population: results from The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Br J Psychiatry (2002) 181(Cidi):208–13. doi: 10.1192/bjp.181.3.208
36. Köhler S, Wiethoff K, Ricken R, Stamm T, Baghai TC, Fisher R, et al. Characteristics and differences in treatment outcome of inpatients with chronic vs. episodic major depressive disorders. J Affect Disord (2015) 173:126–33. doi: 10.1016/j.jad.2014.10.059
37. Wiersma JE, van Oppen P, van Schaik DJF, van der Does AJW, Beekman ATF, Penninx BWJH. Psychological Characteristics of Chronic Depression. J Clin Psychiatry (2011) 72(03):288–94. doi: 10.4088/JCP.09m05735blu
38. Bora E, Berk M. Theory of mind in major depressive disorder: A meta-analysis. Vol. 191. J Affect Disord (2016) 191:49–55. doi: 10.1016/j.jad.2015.11.023
39. Constantino MJ, Laws HB, Arnow B, Klein DN, Rothbaum BO, Manber R. The relation between changes in patients’ interpersonal impact messages and outcome in treatment for chronic depression. J Consult Clin Psychol (2012) 80(3):354–64. doi: 10.1037/a0028351
40. Klein JP, Probst T, Kriston L, Assmann N, Bailer J, Eich H, et al. Changes in Therapeutic Alliance and in Social Inhibition as Mediators of the Effect of the Cognitive Behavioral Analysis System of Psychotherapy: A Secondary Analysis from a Randomized Clinical Trial. Psychother Psychosom (2020) 19:1–2. doi: 10.1159/000506082
41. Faissner M, Kriston L, Moritz S, Jelinek L. Course and stability of cognitive and metacognitive beliefs in depression. Depress Anxiety (2018) 35(12):1239–46. doi: 10.1002/da.22834
42. Li S, Zhang B, Guo Y, Zhang J. The association between alexithymia as assessed by the 20-item Toronto Alexithymia Scale and depression: A meta-analysis. Psychiatry Res (2015) 227(1):1–9. doi: 10.1016/j.psychres.2015.02.006
43. Spitzer C, Siebel-Jürges U, Barnow S, Grabe HJ, Freyberger HJ. Alexithymia and interpersonal problems. Psychother Psychosom (2005) 74(4):240–6. doi: 10.1159/000085148
44. Thomas R, DiLillo D, Walsh K, Polusny MA. Pathways from child sexual abuse to adult depression: The role of parental socialization of emotions and alexithymia. Psychol Violence (2011) 1(2):121–35. doi: 10.1037/a0022469
45. Taubner S, Kessler H, Buchheim A, Kächele H, Staun L. The Role of Mentalization in the Psychoanalytic Treatment of Chronic Depression. Psychiatry Interpers Biol Process (2011) 74(1):49–57. doi: 10.1521/psyc.2011.74.1.49
46. Klein DN, Shankman SA, Rose S. Ten-Year Prospective Follow-Up Study of the Naturalistic Course of Dysthymic Disorder and Double Depression. Am J Psychiatry (2006) 163(5):872–80. doi: 10.1176/ajp.2006.163.5.872
47. Fricker S. An Experimental Comparison of Web and Telephone Surveys. Public Opin Q (2005) 69(3):370–92. doi: 10.1093/poq/nfi027
48. Weightman MJ, Air TM, Baune BT. A Review of the Role of Social Cognition in Major Depressive Disorder. Front Psychiatry (2014) 11:5(NOV). doi: 10.3389/fpsyt.2014.00179
Keywords: depression, social cognition, preoperational thinking, persistent depressive disorder, Cognitive–Behavioral Analysis System of Psychotherapy, interpersonal behavior
Citation: Sondermann S, Stahl J, Grave U, Outzen J, Moritz S and Klein JP (2020) Preoperational Thinking as a Measure of Social Cognition Is Associated With Long-Term Course of Depressive Symptoms. A Longitudinal Study Involving Patients With Depression and Healthy Controls. Front. Psychiatry 11:652. doi: 10.3389/fpsyt.2020.00652
Received: 22 April 2020; Accepted: 23 June 2020;
Published: 08 July 2020.
Edited by:
Cynthia H. Y. Fu, University of East London, United KingdomReviewed by:
Loredana Lucarelli, University of Cagliari, ItalyCopyright © 2020 Sondermann, Stahl, Grave, Outzen, Moritz and Klein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefan Sondermann, c3RlZmFuLnNvbmRlcm1hbm5AdWtzaC5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.