 Kwan Woo Choi
Kwan Woo Choi Hong Jin Jeon
Hong Jin Jeon
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Psychiatry , 30 June 2020
Sec. Mood Disorders
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.00607
This article is part of the Research Topic Linking Treatment Target Identification to Biological Mechanisms Underlying Mood Disorders View all 24 articles
Major depressive disorder (MDD) is one of the disabling diseases in the world-wide, and known to increase cardiac morbidity and mortality. Therefore, previous studies related heart rate variability (HRV) have been conducted to evaluate and diagnose MDD, and to predict treatment outcomes in patient with MDD. We reviewed extensively on the previous peer-reviewed publications associated with this issue, using Pub-Med. In this review article, we introduce the basic concept of HRV and HRV measures, and present several important findings associated with diagnosis and treatment prediction in MDD with using HRV parameters. Furthermore, we discuss the possible underlying mechanism of this phenomenon, and suggest several considerations for the future research.
Major depressive disorder (MDD) is one of the most disabling conditions, featured by depressive episodes lasting at least two weeks, over changes in mood, cognition, and vegetative symptoms (1). However, because MDD is a heterogenous condition, and patients with MDD exhibit multiple variable symptoms, which make the correct diagnosis difficult (2). Furthermore, although antidepressant medication has been considered as the first-line treatment for MDD, only 50% of patients are non-responsive to initial treatment, and it is difficult to predict future responsiveness of MDD at the time of beginning treatment (3). Therefore, it is necessary to develop a more reliable method to diagnose MDD and predict treatment responsivity in MDD patients.
Numerous research findings have proven that major depressive disorder (MDD) is strongly associated with elevated risk for the development and progression of cardiovascular diseases (4–13). Autonomic nervous system (ANS) dysfunction is considered one of the pathways linking MDD and negative CVD outcomes (14). Heart rate variability (HRV), levels of variability of the heart beat-to-beat interval over time, has been known to provide an index of ANS functioning including the sympathetic and parasympathetic system (15). In this brief review, we aim to describe a clinical overview of the HRV parameters, methodologic issues, and HRV research which found an association between HRV parameters and MDD diagnosis, and between baseline HRV parameters and MDD treatment responsivity.
We performed a brief review of major publication on the diagnosis for MDD with using HRV use, and predictive value of HRV parameters for treatment response, especially in patients with MDD. A structured literature search was conducted from the PubMed data base until March 2020 (with no publication data limitations) (Arksey and O’Malley, 2005). Search terms and databases were determined in consultation with a health science librarian at Korea University and Samsung Medical Center. Relevant articles which were identified using the following keywords: “heart rate variability” and “major depressive disorder” and “diagnosis”; “heart rate variability” and “major depressive disorder” and “treatment”; “heart rate variability” and “major depressive disorder” and “treatment response”; “heart rate variability” and “depression” and “remission”. The retrieved title and abstracts were investigated for relevance for two reviewers (Kwan Woo Choi [KWC], and Hong Jin Jeon [HJJ]) using the following inclusion criteria: 1) the study focused on heart rate variability as the main outcome; 2) the study mainly focused on the diagnosis or treatment response of major depressive disorder (MDD); 3) the population of the study targeted adult people, who are older than 18 years old; 4) the article is written in English. In reviewing abstracts, citations were excluded from the review using the following criteria: 1) the study does not deal with specific HRV parameters; 2) the study was not written in English. The initial database search returned 155 database citations. 155 abstracts were selected to review for inclusion in the scoping review and 27citations qualified for full paper review. Following full paper review, seven articles were excluded as they did not meet inclusion criteria. The final set of 13 studies included (Figure 1).
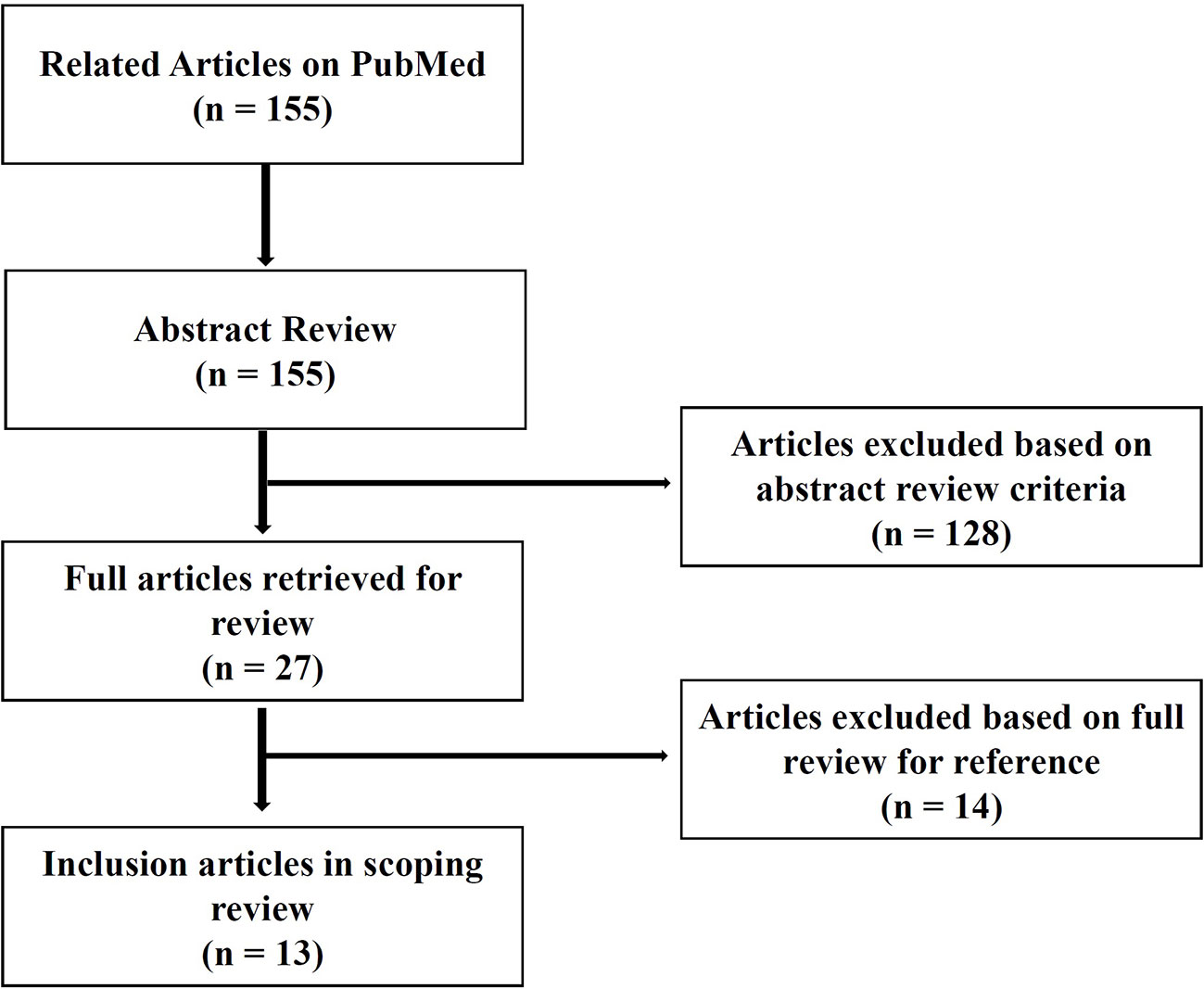
Figure 1 Flow chart of review selection process.
HRV is defined as fluctuation of the heart beat interval over time (16). Since the heart is dually innervated by the sympathetic and parasympathetic branches of the autonomous nervous system (ANS), subtle moment-to-moment changes in heart rate (HR) are qualitative indicators of ANS function (17). According to the reliable international guidelines, HRV parameters could be divided into two domains; frequency domain (spectral analysis) and time domain (non-spectral analysis) (Table 1) (15, 18).
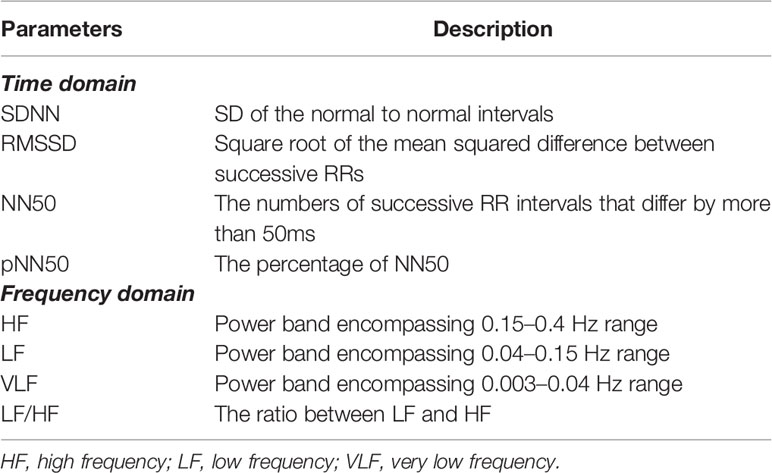
Table 1 A brief description of the most relevant measures of heart rate variability.
Time domain HRV features are calculated with simple mathematical methods to measure the amount of variability present in a specific time period in a continuous ECG signal (19). These parameters are based on the time series of R to R interval (RRI) from the ECG signals. The standard deviation of average normal to normal (NN) intervals (SDNN), the root mean square of successive differences (RMSSD), and the percentage of absolute differences in successive NN values greater than 50ms (pNN50) are widely utilized as time-domain HRV indicators. SDNN is known to reflect both sympathetic and parasympathetic functioning, whereas RMSSD and pNN50 are related to parasympathetic functioning (20–22).
Frequency domain provides an assessment of vagal modulation of the RRI, extracted from the ECG. Frequency domain is mostly commonly acquired by fast Fourier transformation to separate RRI into characteristic very low frequency (VLF, 0.003–0.04 Hz), low frequency (LF, 0.04–0.15 Hz), and high frequency (HF, 0.15–0.4 Hz) band (20). Spectral measures are acquired over different time intervals (approximately 2.5 to 15 min), depending on the frequency being analyzed (20). According to previous studies, LF is influenced by both sympathetic and parasympathetic activities, and HF is affected by mostly parasympathetic activities (23, 24). LF/HF ratio is ratio of LF and HF, and it implicates the sympathetic predominance compared to parasympathetic activities (21, 22).
MDD is assoicated with the increased risk of cardiovascular morbidity and mortality (4, 5), and also known to be associated with reduced HRV (25, 26). For these reasons, there have been numerous studies to find the neurobiological biomarkers of MDD related to HRV parameters (Table 2).
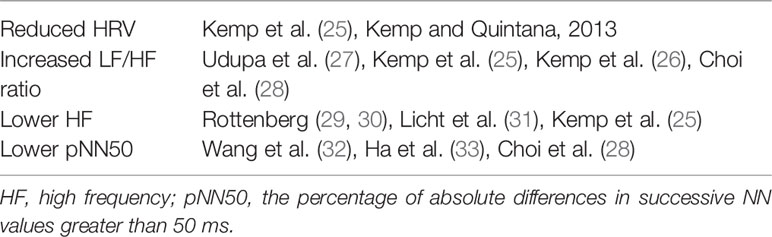
Table 2 Heart rate variability for the diagnosis of major depressive disorder.
Consistently, there have been many reports which showed an increased LF/HF ratio in patients with MDD compared to HCs (25–28). According to the previous meta-analysis by Kemp et al. which compared 673 depressed patients and 407 healthy controls (HCs) with using 18 articles (25), depressed patients without cardiovascular disease showed reduced time domain HRV, HF HRV, and increased LF/HF ratio than HCs. Udupa et al. also found that 40 patients with MDD showed a more increased LF/HF ratio than 40 age matched HCs (27). More recently, Choi et al. found that patients with MDD showed an elevated LF/HF ratio especially after the stress induction compared HCs (28). The LF/HF ratio is associated with sympathetic predominance (34), which could be related to the increased sympathetic modulation or disrupted ANS modulation in MDD.
As well as LF/HF ratio, decreased HF has also been one of the consistent HRV parameters which were significantly associated with MDD (25, 29, 30, 35, 36). In one meta-analysis, patients with MDD had lower resting levels of HRV than HCs (25). According the large-scale prospective Netherland Study of Depression and Anxiety (NESDA), Licht et al. also showed that remitted and current MDD patients had a lower HF compared to HCs, although they concluded the association appeared to be mainly associated with the effect of antidepressants (36). Rottenberg et al. also found significantly reduced HF in patients with MDD, however the overall effect size was relatively small according to their meta-analysis (29). In reviewing previous reports, HF could be particularly related with anxious depression. Reduction in HF might have significant relations with anxiety according to neurovisceral integration (NVI) model studies (37, 38). Moreover, various anxiety disorders were associated with reduced HRV (39, 40). Some investigators found that low HF in MDD is driven or exacerbated by co-occurring anxiety (26, 31, 41, 42). HF is associated with the parasympathetic tone (43, 44). Relatively high HF is known to reflect adaptive functioning, and neural activity in the prefrontal cortex related to emotional, cognitive, and autonomic regulation (38, 44). Further studies will be needed to evaluate the relationship between HF and MDD.
The pNN50 is known to be associated with HF, which reflects the activity level of the parasympathetic nervous system (15, 28). There have been several reports which showed reduced pNN50 in patients with MDD compared to HCs (28, 32, 33). Especially, Ha et al. showed that reduced in pNN50 in the medication-naïve, and newly diagnosed with elderly MDD patients who were older than 60 years old (33). Choi et al. also revealed a lower value of pNN50 compared to HCs at the stress phase, and recovery phase (28).
Antidepressants have been utilized as a front-line treatment of MDD, whereas only one-third to one-half MDD patients who take a complete initial course of antidepressants achieve remission (45, 46). Whereas there are consistent findings that tricyclic antidepressants reduce HRV, it is controversial whether selective serotonin reuptake inhibitors (SSRIs) alters HRV (25, 47). Although there have been studies which found increases in HRV or stability after successful antidepressant treatment in patients with MDD (48, 49), there has been paucity of research which found specific baseline HRV parameters, which could predict treatment responsivity in patients with MDD. Table 3 summarizes previous HRV findings associated with MDD.
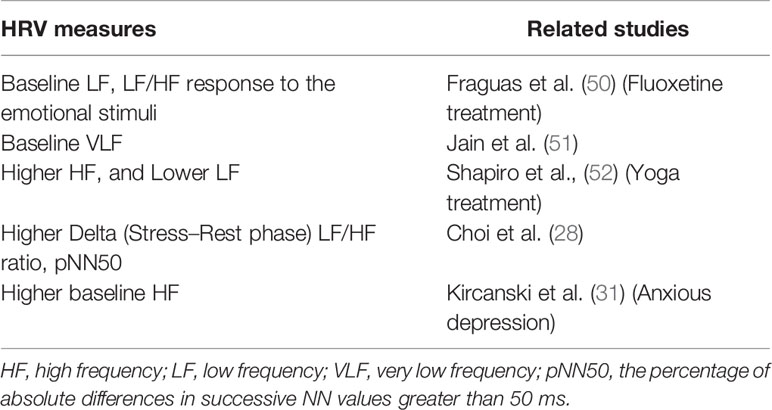
Table 3 Heart rate variability for the prediction of better or worse treatment response in MDD.
Previously, in response to the emotional stimulus, baseline changes in LF and LF/HF ratio were positively associated with the decrease level in MDD symptoms during fluoxetine treatment (50). More recently, Jain et al. found that baseline VLF was negatively correlated with symptom improvement in depression (51). Shapiro et al. showed that remitters in MDD had significantly more increased HF, and decreased LF than non-remitters during yoga treatment (52). Choi et al. found that delta LF/HF ratio (Stress phase–Rest phase), and delta pNN50 (Stress phase–Rest phase) were significantly positively associated with treatment response (after 12 weeks) in patients with MDD (28). Regarding types of MDD, Kircanski et al. recently showed that patients with higher HRV, or HF had better treatment outcomes especially in anxious depression (31). However, in non-anxious depression, patients with lower HRV had better outcomes (31). Their study implicates that there might be subtype-specific treatment biomarkers in patients with MDD. A similar study. attempted to differentiate treatment response group from non-response group using EEG and HRV (53). However, the researchers did not predict treatment responsivity in depression using HRV parameters, while they could predict treatment outcome in MDD only using the EEG parameter (53). Despite focusing on PTSD diagnosis other than MDD, Minassian et al. showed that high LF/HF ratio (>6.7) before deployment was significantly associated with post-deployment post-traumatic stress disorder (PTSD) in active-duty marines (54).
Disrupted autonomic function may be regarded as a serious pathophysiological candidate for elevated risk of cardiovascular mortality in patients with MDD. Thayer and Lane suggested a neurovisceral integration (NVI) model in the context of emotional regulation (55). According to the NVI model, decreased activation of the central autonomic network (CAN) may affect the decreased level of HRV. CAN is known to be the constellation of brain areas responsible for the neurobiological and physiological regulation of affect and attendant behaviors. According to the NVI modes, the CAN modulates the neuroendocrine, visceromotor, and even behavioral systems (37, 56). Furthermore, the CAN has connection with the sinoatrial node of the heart via the stellate ganglion through vagus nerve (57). Therefore, HRV is a widely utilized biomarkers of CAN regulatory functioning and considered an informative indicator of brain–body integration, and concomitant health or pathological states (58, 59). CAN is known to consist with the anterior cingulate cortex, insular cortex, ventromedial prefrontal cortex, and the various subcortical structures such as amygdala, hypothalamus, periaqueductal gray matter, parabrachial plexus, and etc. (55–57). Both direct and indirect links between frontal cortex and autonomic motor circuits have been known to be responsible for both the sympathetic and parasympathetic effects on the heart (21, 37, 56). Previous brain imaging studies found that brain regions such as right superior prefrontal, right dorsolateral prefrontal, right dorsolateral prefrontal and left rostral anterior cingulate cortices showed significantly functional decrease concomitantly with decreased HRV (37, 60–62). According to the Thayer and Lane, prefrontal top-down inhibitory and regulatory processes might influence on subcortical emotion regulation centers (37). MDD can be related to the prefrontal hypoactivation and the loss of inhibitory neural functioning with poor affective information processing and regulation (21, 37, 55, 56, 63). Prefrontal hypoactivity might be associated with altered cardiac function in MDD patients, specifically for treatment non-responders.
Although HRV is a non-invasive, pain free, economic and simple technique and one of the easily accessible modalities measuring ANS profiles (18), it is important to consider several important potential confounding factors for the future research.
Due to circadian variation in autonomic cardiac function and HRV (64, 65), it should be recommended to evaluate HRV parameters at about the same time of the day. Furthermore, participants should be recommended to have a normal sleep routine, no intense physical training, and no alcohol the day before the measurement (66–70).
According to the previous research, HRV decreases with aging (71), or HRV parameters changes with a trend toward a decrease in autonomous cardiac function (72, 73). HRV parameters are also known to have different profiles between male and female population (71, 72, 74). In the recent meta-analysis, Koenig and Thayer showed that females had a significantly lower mean RR interval, lower SDNN, lower LF power, lower LF/HF ratio and greater HF power, which implied more increased parasympathetic activity than males (74). Alcohol use is also associated with altered HRV parameters (69, 70). According to the meta-analytic study by Quintana et al., alcohol dependence patients showed reduced HRV compared to nondependent controls (69). On the contrary, the researchers found that habitual, and moderate alcohol drinkers showed increased levels of HF compared to nonhabitual drinkers in their other original study (70). It might be associated with a J-shaped curve that moderate alcohol use is related to a protective effect compared to alcohol dependence or abstinence (69, 70). Smoking is also associated with reduced HRV levels according to previous studies (75, 76). Recent studies also reported that even e-cigarette use decreased HF component, and increased LF and LF/HF ratio compared to controls (77, 78). Weight, height, and waist-to-hip ratio are also considered as potential confounding factors (79). Yi et al. recently showed that waist-to-hip ratio was more strongly correlated with HRV indices and more likely predict reduced HRV compared to body mass index (BMI), and percentage of body fat mass. However, although the previous study indicated no correlation between HRV and BMI (80), BMI should be considered as one of the confounding factors since it is still controversial (79, 81). Therefore, above-mentioned demographic factors should be considered to conduct future research related to HRV.
Previous studies suggest HRV alterations related to antidepressant medication. According to 2010 Kemp et al.’s meta-analysis, they showed that tricyclic antidepressant (TCA) decreased HRV whereas SSRI nefazedone, and mirtazapine did not have any significant effect on HRV (25). On the contrary, their large-scale longitudinal study showed that SSRI, and serotonin and norepinephrine reuptake inhibitors decreased HRV parameters (82). More recently, without TCA and clozapine, there were no significant effect on HRV parameters associated with SSRI treatment (83). Futures studies will be needed to clarify relationships between specific treatment regimen and HRV parameters.
In conclusion, there have been several attempts to diagnose MDD, and to predict treatment responsiveness in patients with MDD with using baseline HRV parameters. We should consider methodological issues and potential confounding factors to examine relationships between MDD and HRV parameters. Furthermore, it will be needed to have larger sample size, prospective and longitudinal study design, and related other regimen such as neuroimaging, inflammatory markers, and so on for the more refined future research.
KC and HJ: Writing and reviewing the whole manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This research was supported by the Original Technology Research Program for Brain Science through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (No. NRF-2016M3C7A1947307; PI HJ), and by the Bio & Medical Technology Development Program of the NRF funded by the Korean government, MSIT (No. NRF-2017M3A9F1027323; PI HJ). This research was also supported by Healthcare AI Convergence Research & Development Program through the National IT Industry Promotion Agency of Korea (NIPA) funded by the Ministry of Science and ICT(No. S1601-20-1041). This work was supported and funded by Korea University (No. K1922891; KWC). The NRF of Korea, NIPA and Korea University had no further role in study design; collection, analysis, and interpretation of data; writing of the report; or in the decision to submit the study for publication.
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association (2013).
2. Baldessarini RJ, Forte A, Selle V, Sim K, Tondo L, Undurraga J, et al. Morbidity in Depressive Disorders. Psychother Psychosom (2017) 86:65–72. doi: 10.1159/000448661
3. Cleare A, Pariante CM, Young AH, Anderson IM, Christmas D, Cowen PJ, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: A revision of the 2008 British Association for Psychopharmacology guidelines. J Psychopharmacol (2015) 29:459–525. doi: 10.1177/0269881115581093
4. Barth J, Schumacher M, Herrmann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med (2004) 66:802–13. doi: 10.1097/01.psy.0000146332.53619.b2
5. Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J (2006) 27:2763–74. doi: 10.1093/eurheartj/ehl338
6. Barefoot JC, Schroll M. Symptoms of depression, acute myocardial infarction, and total mortality in a community sample. Circulation (1996) 93:1976–80. doi: 10.1161/01.cir.93.11.1976
7. Carney RM, Blumenthal JA, Catellier D, Freedland KE, Berkman LF, Watkins LL, et al. Depression as a risk factor for mortality after acute myocardial infarction. Am J Cardiol (2003) 92:1277–81. doi: 10.1016/j.amjcard.2003.08.007
8. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosis after myocardial infarction. Circulation (1995) 91:999–1005. doi: 10.1161/01.cir.91.4.999
9. Freedland KE, Rich MW, Skala JA, Carney RM, Davila-Roman VG, Jaffe AS. Prevalence of depression in hospitalized patients with congestive heart failure. Psychosom Med (2003) 65:119–28. doi: 10.1097/01.psy.0000038938.67401.85
11. Lett HS, Blumenthal JA, Babyak MA, Sherwood A, Strauman T, Robins C, et al. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med (2004) 66:305–15. doi: 10.1097/01.psy.0000126207.43307.c0
12. Penninx BW, Beekman AT, Honig A, Deeg DJ, Schoevers RA, van Eijk JT, et al. Depression and cardiac mortality: results from a community-based longitudinal study. Arch Gen Psychiatry (2001) 58:221–7. doi: 10.1001/archpsyc.58.3.221
13. Zellweger MJ, Osterwalder RH, Langewitz W, Pfisterer ME. Coronary artery disease and depression. Eur Heart J (2004) 25:3–9. doi: 10.1016/j.ehj.2003.09.009
14. Stapelberg NJ, Hamilton-Craig I, Neumann DL, Shum DH, McConnell H. Mind and heart: heart rate variability in major depressive disorder and coronary heart disease - a review and recommendations. Aust N Z J Psychiatry (2012) 46:946–57. doi: 10.1177/0004867412444624
15. Malik M. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J (1996) 17:354–81.
16. Roy-Byrne PP, Stang P, Wittchen HU, Ustun B, Walters EE, Kessler RC. Lifetime panic-depression comorbidity in the National Comorbidity Survey. Association with symptoms, impairment, course and help-seeking. Br J Psychiatry (2000) 176:229–35. doi: 10.1192/bjp.176.3.229
17. Bilchick KC, Berger RD. Heart rate variability. J Cardiovasc Electrophysiol (2006) 17:691–4. doi: 10.1111/j.1540-8167.2006.00501.x
18. Laborde S, Mosley E, Thayer JF. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research - Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front Psychol (2017) 8:213. doi: 10.3389/fpsyg.2017.00213
19. Sgoifo A, Carnevali L, Alfonso Mde L, Amore M. Autonomic dysfunction and heart rate variability in depression. Stress (2015) 18:343–52. doi: 10.3109/10253890.2015.1045868
20. Kidwell M, Ellenbroek BA. Heart and soul: heart rate variability and major depression. Behav Pharmacol (2018) 29:152–64. doi: 10.1097/FBP.0000000000000387
21. Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol (2010) 141:122–31. doi: 10.1016/j.ijcard.2009.09.543
22. Kuang D, Yang R, Chen X, Lao G, Wu F, Huang X, et al. Depression recognition according to heart rate variability using Bayesian Networks. J Psychiatr Res (2017) 95:282–7. doi: 10.1016/j.jpsychires.2017.09.012
23. Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger AC, Cohen RJ. Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science (1981) 213:220–2. doi: 10.1126/science.6166045
24. Billman GE. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front Physiol (2013) 4:26. doi: 10.3389/fphys.2013.00026
25. Kemp AH, Quintana DS, Gray MA, Felmingham KL, Brown K, Gatt JM. Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biol Psychiatry (2010) 67:1067–74. doi: 10.1016/j.biopsych.2009.12.012
26. Kemp AH, Quintana DS, Felmingham KL, Matthews S, Jelinek HF. Depression, comorbid anxiety disorders, and heart rate variability in physically healthy, unmedicated patients: implications for cardiovascular risk. PloS One (2012) 7:e30777. doi: 10.1371/journal.pone.0030777
27. Udupa K, Sathyaprabha TN, Thirthalli J, Kishore KR, Lavekar GS, Raju TR, et al. Alteration of cardiac autonomic functions in patients with major depression: a study using heart rate variability measures. J Affect Disord (2007) 100:137–41. doi: 10.1016/j.jad.2006.10.007
28. Choi KW, Jang EH, Kim AY, Fava M, Mischoulon D, Papakostas GI, et al. Heart rate variability for treatment response between patients with major depressive disorder versus panic disorder: A 12-week follow-up study. J Affect Disord (2019) 246:157–65. doi: 10.1016/j.jad.2018.12.048
29. Rottenberg J. Cardiac vagal control in depression: a critical analysis. Biol Psychol (2007) 74:200–11. doi: 10.1016/j.biopsycho.2005.08.010
30. Rottenberg J, Wilhelm FH, Gross JJ, Gotlib IH. Respiratory sinus arrhythmia as a predictor of outcome in major depressive disorder. J Affect Disord (2002) 71:265–72. doi: 10.1016/s0165-0327(01)00406-2
31. Kircanski K, Williams LM, Gotlib IH. Heart rate variability as a biomarker of anxious depression response to antidepressant medication. Depress Anxiety (2019) 36:63–71. doi: 10.1002/da.22843
32. Wang Y, Zhao X, O’Neil A, Turner A, Liu X, Berk M. Altered cardiac autonomic nervous function in depression. BMC Psychiatry (2013) 13:187. doi: 10.1186/1471-244X-13-187
33. Ha JH, Park S, Yoon D, Kim B. Short-term heart rate variability in older patients with newly diagnosed depression. Psychiatry Res (2015) 226:484–8. doi: 10.1016/j.psychres.2015.02.005
34. Reyes del Paso GA, Langewitz W, Mulder LJ, van Roon A, Duschek S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: a review with emphasis on a reanalysis of previous studies. Psychophysiology (2013) 50:477–87. doi: 10.1111/psyp.12027
35. Rottenberg J, Salomon K, Gross JJ, Gotlib IH. Vagal withdrawal to a sad film predicts subsequent recovery from depression. Psychophysiology (2005) 42:277–81. doi: 10.1111/j.1469-8986.2005.00289.x
36. Licht CM, de Geus EJ, Zitman FG, Hoogendijk WJ, van Dyck R, Penninx BW. Association between major depressive disorder and heart rate variability in the Netherlands Study of Depression and Anxiety (NESDA). Arch Gen Psychiatry (2008) 65:1358–67. doi: 10.1001/archpsyc.65.12.1358
37. Thayer JF, Lane RD. Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev (2009) 33:81–8. doi: 10.1016/j.neubiorev.2008.08.004
38. Thayer JF, Ahs F, Fredrikson M, Sollers JJ. 3rd, Wager TD. A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci Biobehav Rev (2012) 36:747–56. doi: 10.1016/j.neubiorev.2011.11.009
39. Licht CM, de Geus EJ, van Dyck R, Penninx BW. Association between anxiety disorders and heart rate variability in The Netherlands Study of Depression and Anxiety (NESDA). Psychosom Med (2009) 71:508–18. doi: 10.1097/PSY.0b013e3181a292a6
40. Chalmers JA, Quintana DS, Abbott MJ, Kemp AH. Anxiety Disorders are Associated with Reduced Heart Rate Variability: A Meta-Analysis. Front Psychiatry (2014) 5:80. doi: 10.3389/fpsyt.2014.00080
41. Chang HA, Chang CC, Tzeng NS, Kuo TB, Lu RB, Huang SY. Generalized anxiety disorder, comorbid major depression and heart rate variability: a case-control study in taiwan. Psychiatry Invest (2013) 10:326–35. doi: 10.4306/pi.2013.10.4.326
42. Watkins LL, Grossman P, Krishnan R, Blumenthal JA. Anxiety reduces baroreflex cardiac control in older adults with major depression. Psychosom Med (1999) 61:334–40. doi: 10.1097/00006842-199905000-00012
43. Berntson GG, Bigger JT Jr., Eckberg DL, Grossman P, Kaufmann PG, Malik M, et al. Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology (1997) 34:623–48. doi: 10.1111/j.1469-8986.1997.tb02140.x
44. Porges SW. Orienting in a defensive world: mammalian modifications of our evolutionary heritage. A Polyvagal Theory. Psychophysiology (1995) 32:301–18. doi: 10.1111/j.1469-8986.1995.tb01213.x
45. Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry (2006) 163:28–40. doi: 10.1176/appi.ajp.163.1.28
46. Saveanu R, Etkin A, Duchemin AM, Goldstein-Piekarski A, Gyurak A, Debattista C, et al. The international Study to Predict Optimized Treatment in Depression (iSPOT-D): outcomes from the acute phase of antidepressant treatment. J Psychiatr Res (2015) 61:1–12. doi: 10.1016/j.jpsychires.2014.12.018
47. Licht CM, de Geus EJ, van Dyck R, Penninx BW. Longitudinal evidence for unfavorable effects of antidepressants on heart rate variability. Biol Psychiatry (2010) 68:861–8. doi: 10.1016/j.biopsych.2010.06.032
48. Balogh S, Fitzpatrick DF, Hendricks SE, Paige SR. Increases in heart rate variability with successful treatment in patients with major depressive disorder. Psychopharmacol Bull (1993) 29:201–6.
49. Glassman AH, Bigger JT, Gaffney M, Van Zyl LT. Heart rate variability in acute coronary syndrome patients with major depression: influence of sertraline and mood improvement. Arch Gen Psychiatry (2007) 64:1025–31. doi: 10.1001/archpsyc.64.9.1025
50. Fraguas R Jr., Marci C, Fava M, Iosifescu DV, Bankier B, Loh R, et al. Autonomic reactivity to induced emotion as potential predictor of response to antidepressant treatment. Psychiatry Res (2007) 151:169–72. doi: 10.1016/j.psychres.2006.08.008
51. Jain FA, Cook IA, Leuchter AF, Hunter AM, Davydov DM, Ottaviani C, et al. Heart rate variability and treatment outcome in major depression: a pilot study. Int J Psychophysiol (2014) 93:204–10. doi: 10.1016/j.ijpsycho.2014.04.006
52. Shapiro D, Cook IA, Davydov DM, Ottaviani C, Leuchter AF, Abrams M. Yoga as a complementary treatment of depression: effects of traits and moods on treatment outcome. Evid Based Complement Alternat Med (2007) 4:493–502. doi: 10.1093/ecam/nel114
53. Pawlowski MA, Gazea M, Wollweber B, Dresler M, Holsboer F, Keck ME, et al. Heart rate variability and cordance in rapid eye movement sleep as biomarkers of depression and treatment response. J Psychiatr Res (2017) 92:64–73. doi: 10.1016/j.jpsychires.2017.03.026
54. Minassian A, Maihofer AX, Baker DG, Nievergelt CM, Geyer MA, Risbrough VB, et al. Association of Predeployment Heart Rate Variability With Risk of Postdeployment Posttraumatic Stress Disorder in Active-Duty Marines. JAMA Psychiatry (2015) 72:979–86. doi: 10.1001/jamapsychiatry.2015.0922
55. Thayer JF. Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord (2000) 61:201–16. doi: 10.1016/S0165-0327(00)00338-4
56. Smith R, Thayer JF, Khalsa SS, Lane RD. The hierarchical basis of neurovisceral integration. Neurosci Biobehav Rev (2017) 75:274–96. doi: 10.1016/j.neubiorev.2017.02.003
57. Benarroch EE. The central autonomic network: functional organization, dysfunction, and perspective. Mayo Clin Proc (1993) 68:988–1001. doi: 10.1016/S0025-6196(12)62272-1
58. Beissner F, Meissner K, Bar KJ, Napadow V. The autonomic brain: an activation likelihood estimation meta-analysis for central processing of autonomic function. J Neurosci (2013) 33:10503–11. doi: 10.1523/JNEUROSCI.1103-13.2013
59. McCraty R, Shaffer F. Heart Rate Variability: New Perspectives on Physiological Mechanisms, Assessment of Self-regulatory Capacity, and Health risk. Glob Adv Health Med (2015) 4:46–61. doi: 10.7453/gahmj.2014.073
60. Gianaros PJ, Van Der Veen FM, Jennings JR. Regional cerebral blood flow correlates with heart period and high-frequency heart period variability during working-memory tasks: Implications for the cortical and subcortical regulation of cardiac autonomic activity. Psychophysiology (2004) 41:521–30. doi: 10.1111/1469-8986.2004.00179.x
61. Lane RD. Neural substrates of implicit and explicit emotional processes: a unifying framework for psychosomatic medicine. Psychosom Med (2008) 70:214–31. doi: 10.1097/PSY.0b013e3181647e44
62. Lane RD, McRae K, Reiman EM, Chen K, Ahern GL, Thayer JF. Neural correlates of heart rate variability during emotion. Neuroimage (2009) 44:213–22. doi: 10.1016/j.neuroimage.2008.07.056
63. Beauchaine TP, Thayer JF. Heart rate variability as a transdiagnostic biomarker of psychopathology. Int J Psychophysiol (2015) 98:338–50. doi: 10.1016/j.ijpsycho.2015.08.004
64. van Eekelen AP, Houtveen JH, Kerkhof GA. Circadian variation in cardiac autonomic activity: reactivity measurements to different types of stressors. Chronobiol Int (2004) 21:107–29. doi: 10.1081/cbi-120027983
65. Massin MM, Maeyns K, Withofs N, Ravet F, Gerard P. Circadian rhythm of heart rate and heart rate variability. Arch Dis Child (2000) 83:179–82. doi: 10.1136/adc.83.2.179
66. Stein PK, Pu Y. Heart rate variability, sleep and sleep disorders. Sleep Med Rev (2012) 16:47–66. doi: 10.1016/j.smrv.2011.02.005
67. Stanley J, Peake JM, Buchheit M. Cardiac parasympathetic reactivation following exercise: implications for training prescription. Sports Med (2013) 43:1259–77. doi: 10.1007/s40279-013-0083-4
68. Quintana DS, Heathers JA. Considerations in the assessment of heart rate variability in biobehavioral research. Front Psychol (2014) 5:805. doi: 10.3389/fpsyg.2014.00805
69. Quintana DS, McGregor IS, Guastella AJ, Malhi GS, Kemp AH. A meta-analysis on the impact of alcohol dependence on short-term resting-state heart rate variability: implications for cardiovascular risk. Alcohol Clin Exp Res (2013) 37 Suppl 1:E23–9. doi: 10.1111/j.1530-0277.2012.01913.x
70. Quintana DS, Guastella AJ, McGregor IS, Hickie IB, Kemp AH. Moderate alcohol intake is related to increased heart rate variability in young adults: implications for health and well-being. Psychophysiology (2013) 50:1202–8. doi: 10.1111/psyp.12134
71. Umetani K, Singer DH, McCraty R, Atkinson M. Twenty-four hour time domain heart rate variability and heart rate: relations to age and gender over nine decades. J Am Coll Cardiol (1998) 31:593–601. doi: 10.1016/s0735-1097(97)00554-8
72. Kuo TB, Lin T, Yang CC, Li CL, Chen CF, Chou P. Effect of aging on gender differences in neural control of heart rate. Am J Physiol (1999) 277:H2233–9. doi: 10.1152/ajpheart.1999.277.6.H2233
73. Fukusaki C, Kawakubo K, Yamamoto Y. Assessment of the primary effect of aging on heart rate variability in humans. Clin Auton Res (2000) 10:123–30. doi: 10.1007/bf02278016
74. Koenig J, Thayer JF. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci Biobehav Rev (2016) 64:288–310. doi: 10.1016/j.neubiorev.2016.03.007
75. Sjoberg N, Saint DA. A single 4 mg dose of nicotine decreases heart rate variability in healthy nonsmokers: implications for smoking cessation programs. Nicotine Tob Res (2011) 13:369–72. doi: 10.1093/ntr/ntr004
76. Hayano J, Yamada M, Sakakibara Y, Fujinami T, Yokoyama K, Watanabe Y, et al. Short- and long-term effects of cigarette smoking on heart rate variability. Am J Cardiol (1990) 65:84–8. doi: 10.1016/0002-9149(90)90030-5
77. Moheimani RS, Bhetraratana M, Peters KM, Yang BK, Yin F, Gornbein J, et al. Sympathomimetic Effects of Acute E-Cigarette Use: Role of Nicotine and Non-Nicotine Constituents. J Am Heart Assoc (2017) 6(9):e006579. doi: 10.1161/JAHA.117.006579
78. Moheimani RS, Bhetraratana M, Yin F, Peters KM, Gornbein J, Araujo JA, et al. Increased Cardiac Sympathetic Activity and Oxidative Stress in Habitual Electronic Cigarette Users: Implications for Cardiovascular Risk. JAMA Cardiol (2017) 2:278–84. doi: 10.1001/jamacardio.2016.5303
79. Yi SH, Lee K, Shin DG, Kim JS, Kim HC. Differential association of adiposity measures with heart rate variability measures in Koreans. Yonsei Med J (2013) 54:55–61. doi: 10.3349/ymj.2013.54.1.55
80. Antelmi I, de Paula RS, Shinzato AR, Peres CA, Mansur AJ, Grupi CJ. Influence of age, gender, body mass index, and functional capacity on heart rate variability in a cohort of subjects without heart disease. Am J Cardiol (2004) 93:381–5. doi: 10.1016/j.amjcard.2003.09.065
81. Gulgun M, Fidanci MK. Body mass index may be an influential factor in heart rate variability. Rev Port Cardiol (2015) 34:789. doi: 10.1016/j.repc.2015.03.029
82. Kemp AH, Brunoni AR, Santos IS, Nunes MA, Dantas EM, Carvalho de Figueiredo R, et al. Effects of depression, anxiety, comorbidity, and antidepressants on resting-state heart rate and its variability: an ELSA-Brasil cohort baseline study. Am J Psychiatry (2014) 171:1328–34. doi: 10.1176/appi.ajp.2014.13121605
Keywords: heart rate variability, major depressive disorder, antidepressant treatment, treatment, diagnosis
Citation: Choi KW and Jeon HJ (2020) Heart Rate Variability for the Prediction of Treatment Response in Major Depressive Disorder. Front. Psychiatry 11:607. doi: 10.3389/fpsyt.2020.00607
Received: 17 April 2020; Accepted: 11 June 2020;
Published: 30 June 2020.
Edited by:
J. John Mann, Columbia University, United StatesReviewed by:
Gianna Sepede, University of Studies G. d'Annunzio Chieti and Pescara, ItalyCopyright © 2020 Choi and Jeon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Jin Jeon, amVvbmhqQHNra3UuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.