
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 12 June 2020
Sec. Public Mental Health
Volume 11 - 2020 | https://doi.org/10.3389/fpsyt.2020.00520
 Yifang Zhou1,2†
Yifang Zhou1,2† Yuan Yang3,4,5†Tieying Shi6†
Yuan Yang3,4,5†Tieying Shi6† Yanzhuo Song1Yuning Zhou2Zhibo Zhang1Yanan Guo1Xixi Li2Yongning Liu6Guojun Xu6Teris Cheung7
Yanzhuo Song1Yuning Zhou2Zhibo Zhang1Yanan Guo1Xixi Li2Yongning Liu6Guojun Xu6Teris Cheung7 Yu-Tao Xiang3,4*
Yu-Tao Xiang3,4* Yanqing Tang1,2*
Yanqing Tang1,2*Background: Little empirical evidence is known about the sleep quality of frontline health professionals working in isolation units or hospitals during the novel coronavirus disease (COVID-19) outbreak in China. This study thus aimed to examine the prevalence of poor sleep quality and its demographic and correlates among frontline health professionals.
Methods: This is a multicenter, cross-sectional survey conducted in Liaoning province, China. Sleep quality was measured by the Pittsburgh Sleep Quality Index (PSQI).
Results: A total of 1,931 frontline health professionals were recruited. The prevalence of poor sleep quality was 18.4% (95%CI: 16.6%–20.11%). Multivariate logistic regression analysis found that older age (OR=1.043, 95%CI=1.026–1.061, P < 0.001), being nurse (OR=3.132, 95%CI=1.727–5.681, P < 0.001), and working in outer emergency medical team (OR=1.755, 95%CI=1.029–3.064, P=0.039) were positively associated with poor sleep quality. Participants who were familiar with crisis response knowledge were negatively associated with poor sleep quality (OR=0.70, 95%CI=0.516–0.949, P=0.021).
Conclusion: The prevalence of poor sleep quality was relatively low among frontline health professionals during the COVID-19 epidemic. Considering the negative impact of poor sleep quality on health professionals’ health outcomes and patient outcomes, regularly screening and timely treatments are warranted to reduce the likelihood of poor sleep quality in health professionals.
The novel coronavirus disease (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has aroused enormous attention nationwide (1). This disease was first reported in Wuhan, Hubei province, and then was transmitted to other areas of China (2). As of 1st May, 2020, there have been 82,874 confirmed patients with COVID-19 and 4,633 deaths in China (3).
In order to control the rapid disease transmission, China has suspended public transport and adopted mass quarantine measures in multi-regions since late January, 2020 (2). The National Health Commission of China (NHC) has adopted a range of emergency measures, including the establishment of emergency isolation infectious units and hospitals, and temporary quarantine facilities (“Fang cang” hospitals) (4). External emergency medical teams have also been promptly established nationwide and assigned to provide medical assistance in Hubei province, China. As of 26th February, 2020, more than 178 crisis response teams comprising 32,395 volunteer health professionals have been summoned to Hubei province (5).
Due to insufficient knowledge, awareness and preventive measures in the early stage of the COVID-19 outbreak, a total of 3,387 health professionals in 476 clinical sites have been infected with the disease, of which, 26 died (6). Frontline health professionals, especially those working in Hubei province, and having close contacts with infected patients often reported excessive workload. Due to insufficient supplies of full protective gear, dangerous working environments, and limited clinical experiences in managing the COVID-19, frontline health professionals are extremely vulnerable to experience fatigue, anxiety, depression, emotional breakdown, and sleep disturbance (7).
Sleep problems, such as poor sleep quality, are common in the health care profession due to high level of work-related stress (8, 9). Poor sleep quality could result in serious health consequences, such as hypertension, exhaustion, burnout, and depression (10–13). Health professionals suffering from poor sleep quality were more likely to have poor work performance, which could compromise patient safety and reduce the quality of patient care. In extreme case, health professionals could prescribe inaccurate diagnosis causing potentially fatal medical errors (14–19). Before developing preventive strategies and alleviating the negative outcomes of poor sleep quality, it is pivotal to understand its epidemiology and correlates among health professionals.
Sleep quality could be measured by both objective [e.g., polysomnography (PSG)] and subjective instruments [e.g., sleep diary, and Pittsburgh Sleep Quality Index (PSQI)] (20). The PSQI is the most commonly used subjective assessment tool measuring global sleep quality. A recent meta-analysis (21) showed that the pooled prevalence of poor sleep quality as measured by the PSQI was 61.0% in nurses.
Liaoning province is located in northern China. As of 1st May, 2020, there had been 146 COVID-19 patients in Liaoning province, of which, two died (3). During the COVID-19 outbreak, frontline health professionals experienced high work-related stress, which could lead to psychological distress, burnout, and sleep problems. To date, little has been known about the prevalence of sleep quality among frontline health professionals in areas of China which were less affected by the COVID-19. This gap gave us the impetus to examine the prevalence of poor sleep quality and its associated factors in this population. We hypothesized that frontline health professionals working in Liaoning province were less likely to experience poor sleep quality compared to their counterparts working in Hubei province—the epicenter of the COVID-19 outbreak.
This was a cross-sectional study conducted between February 21 and 23, 2020 in Liaoning province, China using convenience snowball sampling. During the COVID-19 outbreak, frontline health professionals were managed by hospital authorities using the WeChat in Liaoning province, China. Data collection was executed using the Wenjuanxing program which is an application embedded with WeChat (https://www.wjx.cn/app/survey.aspx). WeChat is the most popular social media platform in China used by over one billion people (i.e., more than 70% of Chinese population) (22). The Wenjuanxing program has been widely used in epidemiological surveys (23, 24). Inclusion criteria included 1) adults aged 18 years or above; 2) frontline health professionals (i.e., doctors and nurses) working in isolation unit/hospitals, or fever clinics established for the COVID-19 outbreak in either outer emergency medical team from Liaoning in Wuhan or in Liaoning province; 3) ability to read Chinese and provide written informed consent. This study was approved by the clinical research ethics committee of the First Hospital of China Medical University.
Participant’s basic sociodemographic characteristics, such as gender, age, educational level, marital status, occupation, living circumstances, current smoking and drinking behaviors, current working status, previous working experience, and perceived family support, were collected using a data collection form designed for this study. Participant’s working status was assessed by four questions using a dichotomous response (“Yes/No”): 1) “Do you have direct contact with SARS-CoV-2 infected patient in daily clinical practice?”; 2) “Are you currently working in the COVID-19 outer emergency medical team in Wuhan, Hubei province?”; 3) “Are you familiar with the crisis response protocols and with relevant knowledge?”; and 4) “Have you ever attended any crisis response/rescue work previously?” Information on current drinking and smoking habits was solicited by the following questions: “Did you drink alcoholic beverage at least once per month (Yes/No)” (25), “Did you smoke at least one cigarette per day (Yes/No)” (26). Those who answered “Yes” to these questions were considered as current alcohol drinker or current smoker. ‘Perceived family support’ was measured by a single dichotomous question (Yes/No): “Do you think you had good familial support during the COVID-19 outbreak?”
The Chinese version of the PSQI is a 19-item instrument consisting of seven domains (subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, daytime dysfunction, and use of sleep medications). PSQI is a widely used self-administered questionnaire to assess sleep quality (27). The psychometric properties of the Chinese version of the PSQI was satisfactory, with the Cronbach’s alpha of 0.734 (28). The PSQI total score ranges from 0 to 21, with higher scores indicating poorer sleep quality. The cut-off value for poor sleep quality is 7 in Chinese populations (28).
Data analyses were conducted using SPSS Analytics software Version 21.0. Kolmogorov-Smirnov test was performed to test the normal distribution of continuous variables. Comparisons between good and poor sleep quality groups in terms of basic demographic and clinical characteristics were conducted using Chi-square test, and two independent samples t-test, as appropriate. Multivariate logistic regression analysis with the “enter” method (i.e., entering all the independent variables in the model simultaneously) was used to further identify significant independent demographic and clinical correlates associated with poor sleep quality. Poor sleep quality was the dependent variable, while all sociodemographic and clinical variables were entered as the independent variables. Significant level was set as P < 0.05 for all tests (two-sided).
A total of 1,931 health professionals participated in this study; of which, 355 (18.4%, 95%CI=16.6%–20.11%) reported poor sleep quality (PSQI total score of ≥7). Table 1 shows the basic sociodemographic and clinical characteristics of participants by sleep quality. The mean PSQI total scores and component scores of the whole sample separated by good and poor sleep quality groups are shown in Table 2.
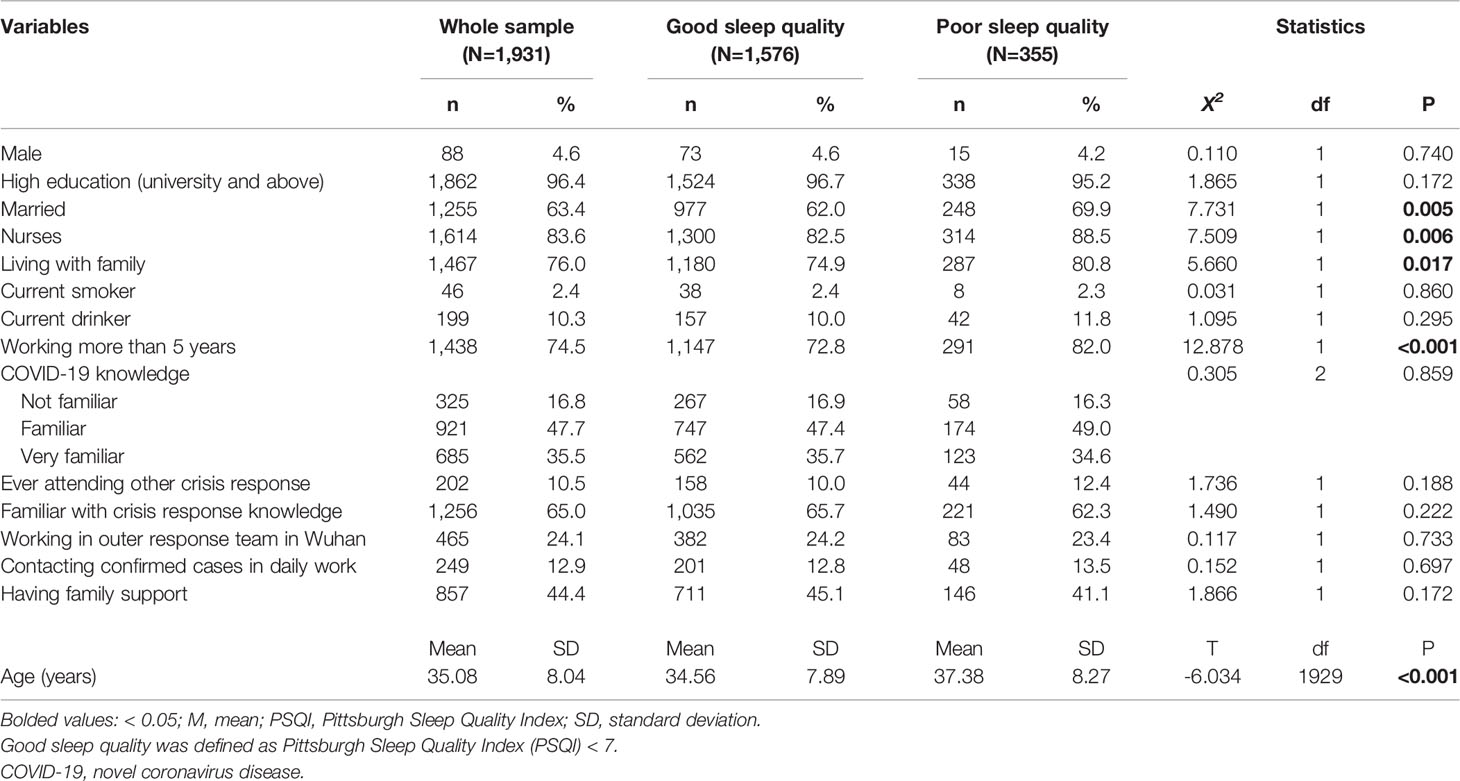
Table 1 Demographic characteristics of the study sample (N=1,931).
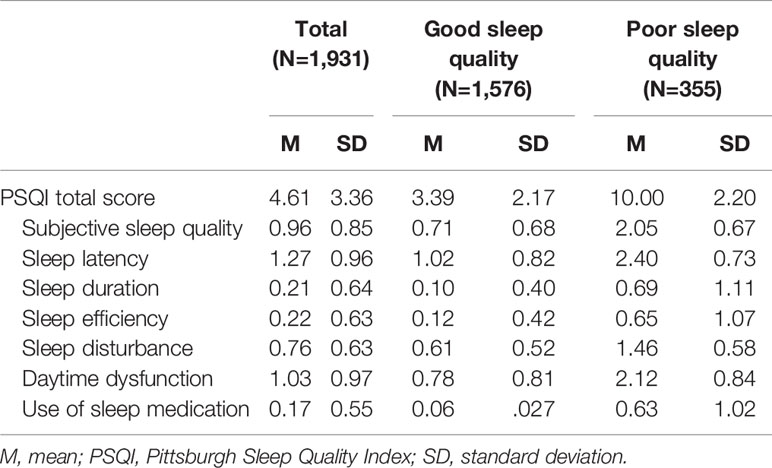
Table 2 PSQI total and component scores in all participants.
Univariate analyses revealed five correlates that were significantly associated with poor sleep quality (i.e., being nurses, older age, married, living with family, and > 5 years working experience), while the remaining were not associated with poor sleep quality. Multivariate logistic regression analysis revealed that nurses (OR=3.132, 95%CI=1.727–5.681, P < 0.001), older age (OR=1.043, 95%CI=1.026–1.061, P < 0.001), and health professionals who were working in outer emergency medical team in Hubei province (OR=1.755, 95%CI=1.029–3.064, P=0.039) were more likely to report poor sleep quality. Those who were familiar with crisis response protocols and with relevant knowledge were less likely to report poor sleep quality (OR=0.700, 95%CI=0.516–0.949, P=0.021) (Table 3).
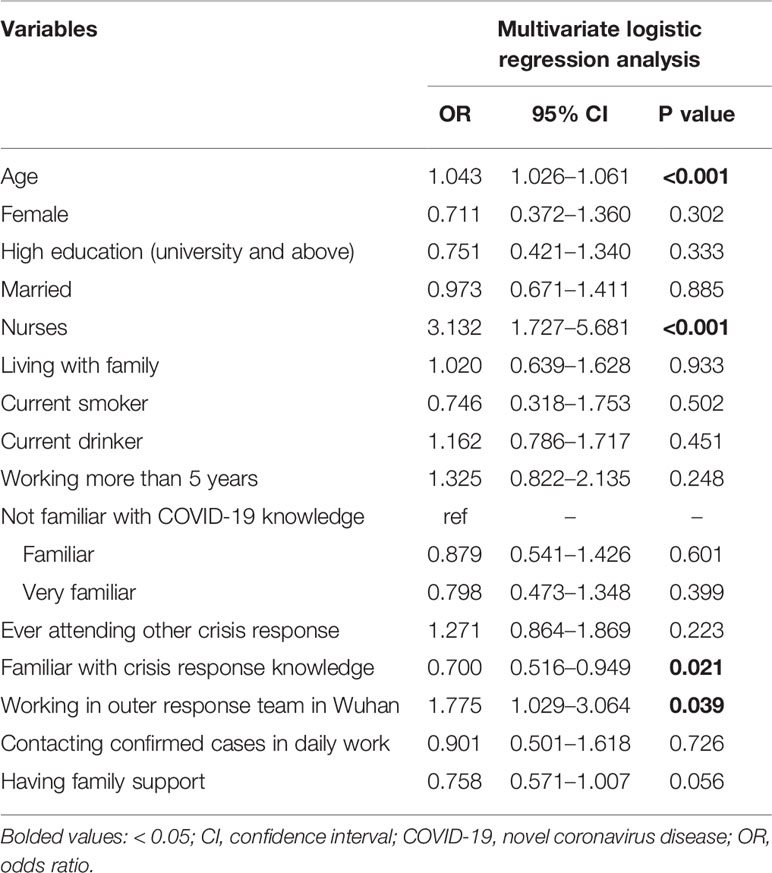
Table 3 Independent correlates of poor sleep quality by multivariate logistic regression analysis.
This was the first study to examine sleep quality among frontline health professionals using the PSQI during the outbreak of the COVID-19 in areas less affected by COVID-19 in China. Using the cut-off value of 7, the prevalence of poor sleep quality was 18.4% (95%CI=16.6%–20.11%) among frontline health professionals in Liaoning province. This prevalence rate was lower than most of the previous findings in similar studies. For example, a recent cross-sectional study in China reported that 36.1% of frontline health professionals suffered from sleep disturbance using the Insomnia Severity Index (ISI) in early stage of the COVID-19 epidemic in China (i.e., late January, 2020) (7). A recent systematic review and meta-analysis found that the pooled prevalence of sleep disturbances among Chinese healthcare professionals was 39.2% (95%CI=36.0%–42.7%), using the PSQI (29). Machi et al. reported that the prevalence of poor sleep quality was 31.0% in US doctors working in emergency departments using the PSQI with the cut-off value of 6 (30), while Surani et al., reported that the prevalence of poor sleep quality was 36.8% in Pakistani physicians using the PSQI cut-off value of 5 (31). In contrast, the prevalence of poor sleep quality was 35.21% (95%CI=33.08%–37.35%) using the cut-off of 5, while the corresponding figure was 26.41% (95%CI=24.44%–28.38%) using the cut-off of 6 in this study.
The discrepancy in the prevalence of sleep quality in health professionals across studies could be partly explained by different population characteristics and the use of assessment tools. Since 25th January, 2020, 30 provinces, municipalities, and autonomous regions covering over 1.3 billion Chinese population have initiated first-level responses to major public health emergencies. A range of measures, including establishment of emergency isolation infectious units and hospitals, have been urgently adopted (32, 33). However, compared to Hubei province, the epicenter of the COVID-19 in China, the disease epidemic was not as serious as in other areas of China. Liaoning province is a good example. Based on previous experience learned in the 2003 SARS epidemic that frontline health professionals were more likely to suffer from psychological problems (2), the authorities in Liaoning province have thus undertaken certain preventive interventions to relieve stress among frontline health professionals, such as timely provision of financial and material supports, mass education on pressure control, online psychological counseling service (e.g., 24-h hotlines), and on-site psychological guidance. These measures could reduce the risk of poor sleep quality (34).
As expected, older age was positively associated with poor sleep quality. Compared to their younger counterparts, older adults usually have more household responsibilities, and economic burdens (35, 36). Older adults are also prone to experience negative life events, such as divorce and bereavement, and suffer from physical discomforts and chronic physical diseases (37, 38), which could contribute to poor sleep quality (39). In this study, nurses were more likely to report poor sleep quality when compared with other health professionals (e.g., doctors and medical technicians). A vast majority of the nursing sample were females (95.4%). Some studies found that women were approximately 1.5 times more likely to report sleep problems than their male counterparts (30, 31, 40). Similar gender difference was also found in other neuropsychiatric diseases, such as headache, depression, and anxiety (40). In this light, generic factor could be one possible reason to explain the gender difference in sleep quality (41). It is also evident that anxiety and depression are more common in women, which could increase the risk of poor sleep quality (42–44). Besides, women tend to have greater bodily vigilance and awareness of physical symptoms than men. The societal norms and cultural context are more receptive for women to express their psychological distress and somatic symptoms (45), which may, perhaps, increase their likelihood of reporting poor sleep quality in survey studies.
Apart from female nurses, health professionals working in external emergency medical team in Hubei province, China were also more likely to experience poor sleep quality. In early February, 2020, emergency medical teams in Liaoning, China were urgently summoned to assist in Hubei province. Compared to those working in local isolation hospitals in Liaoning province, the external emergency medical teams need to adapt to unfamiliar living environment and work settings, and could experience heavy clinical workload, burnout, loneliness, homesickness, and fear of infection. All these bio-psycho-social factors could affect their sleep quality (46). Health professionals who were familiar with crisis response protocols/knowledge, however, were less likely to report poor sleep quality in this study. We speculate that receiving good training and learning relevant knowledge of crisis response for infectious diseases could be a protective factor and effectively reduce the extent of fear, anxiety, and uncertainty.
The strengths of this study include large sample size, and the use of standardized measurements. There are several methodological limitations that need to be acknowledged. First, this was a cross-sectional study, therefore, the causal relationships between demographic and clinical variables, and poor sleep quality could not be established. Second, most participants were female nurses, which could lead to potential selection bias. Third, sleep quality was assessed by only one self-administered instrument and thus, recall bias may exist. Finally, due to logistical reasons and risk of cross-infection, random sampling cannot be used in most studies on frontline health professionals during the COVID-19 outbreak. Thus, convenience sampling has been widely used (47, 48), which limits the generalizability of the findings. In addition, some variables associated with sleep quality, such as economic status, interpersonal relationship and psychiatric diagnoses (e.g., major depression and anxiety disorder), were not examined in this study.
In conclusion, it is encouraging to note that the prevalence of poor sleep quality was relatively low among frontline health professionals in Liaoning province during the COVID-19 epidemic. Nonetheless, considering the negative impact of poor sleep quality on health, wellbeing and daily clinical practice, regularly screening and timely treatments are warranted in frontline health professionals during the COVID-19 outbreak.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by clinical research ethics committee of the First Hospital of China Medical University. The patients/participants provided their written informed consent to participate in this study.
Study design: YT and Y-TX. Data collection, analysis, and interpretation: YiZ, YY, TS, YS, YuZ, ZZ, YG, XL, YL, and GX. Drafting of the manuscript: YY, Y-TX, and YT. Critical revision of the manuscript: TC. Approval of the final version for publication: all co-authors.
The study was supported by the University of Macau (MYRG2019-00066-FHS), and the National Key R&D Program of China (Grant #2018YFC1311600 and 2016YFC1306900).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. New Engl J Med (2020) 382(13):1199–1207 doi: 10.1056/NEJMoa2001316
2. Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry (2020b) 7(3):228–9. doi: 10.1016/S2215-0366(20)30046-8
3. Health Emergency Office. Update on the epidemic situation of new coronavirus pneumonia as of 24:00 on February 25 (in Chinese). (2020). http://fmsnewscn/swf/2020_sjxw/2_1_xgyq/indexhtml (access Feb 25th, 2020).
4. Li W, Yang Y, Liu ZH, Zhao YJ, Zhang QE, Zhang L, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci (2020) 16(10):1732–8. doi: 10.7150/ijbs.45120
5. National Health Commission. (2020). Transcript of the press conference on February 20, 2020 (in Chinese). http://wwwnhcgovcn/xcs/fkdt/202002/526411b8aa6143a487a6827aaa2f40acshtml (access Feb 25th 2020).
6. Dingxiangyuan. (2020). Epidemic Daily on February 25th: Remember these 22 medical staff (in Chinese). http://wwwdxycn/bbs/topic/42850513?keywords=%E8%AF%B7%E8%AE%B0%E4%BD%8F%E8%BF%9922%E4%BD%8D (access Feb 25th 2020).
7. Liu S, Yang LL, Zhang CX, Xiang YT, Liu Z, Hu S, et al. 2019 novel coronavirus: online mental health services. Lancet Psychiatry (2020) 7(4):e17–8. doi: 10.1016/S2215-0366(20)30077-8
8. Thichumpa W, Howteerakul N, Suwannapong N, Tantrakul V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol Health (2018) 40:e2018018. doi: 10.4178/epih.e2018018
9. Sagayadevan V, Abdin E, Binte Shafie S, Jeyagurunathan A, Sambasivam R, Zhang Y, et al. Prevalence and correlates of sleep problems among elderlySingaporeans. Psychogeriatrics (2017) 17(1):43–51. doi: 10.1111/psyg.12190
10. Kunert K, King ML, Kolkhorst FW. Fatigue and sleep quality in nurses. J Psychosoc Nurs Ment Health Serv (2007) 45(8):30–7. doi: 10.3928/02793695-20070801-07
11. Giorgi F, Mattei A, Notarnicola I, Petrucci C, Lancia L. Can sleep quality and burnout affect the job performance of shift-work nurses? A hospital cross-sectional study. J Advanced Nurs (2018) 74(3):698–708. doi: 10.1111/jan.13484
12. Liu RQ, Qian Z, Trevathan E, Chang JJ, Zelicoff A, Hao YT, et al. Poor sleep quality associated with high risk of hypertension and elevated blood pressure in China: results from a large population-based study. Hypertens Res (2016) 39(1):54–9. doi: 10.1038/hr.2015.98
13. Tsuno N, Besset A, Ritchie K. Sleep and depression. J Clin Psychiatry (2005) 66(10):1254–69. doi: 10.4088/JCP.v66n1008
14. Park E, Lee HY, Park CS. Association between sleep quality and nurse productivity among Korean clinical nurses. J Nurs Manage (2018) 26(8):1051–8. doi: 10.1111/jonm.12634
15. Barbe T, Kimble LP, Rubenstein C. Subjective cognitive complaints, psychosocial factors and nursing work function in nurses providing direct patient care. J Advanced Nurs (2018) 74(4):914–25. doi: 10.1111/jan.13505
16. Rogers AE. (2008). “The effects of fatigue and sleepiness on nurse performance and patient safety,” Patient safety and quality: An evidence-based handbook for nurses. Agency for Healthcare Research and Quality (US) (2008).
17. Lockley SW, Barger LK, Ayas NT, Rothschild JM, Czeisler CA, Landrigan CP. Effects of health care provider work hours and sleep deprivation on safety and performance. Joint Commission J Qual Patient Safety (2007) 33(11):7–18. doi: 10.1016/S1553-7250(07)33109-7
18. Caruso CC. Negative impacts of shiftwork and long work hours. Rehabil Nurs (2014) 39(1):16–25. doi: 10.1002/rnj.107
19. Stimpfel AW, Sloane DM, Aiken LH. The longer the shifts for hospital nurses, the higher the levels of burnout and patient dissatisfaction. Health Affairs (2012) 31(11):2501–9. doi: 10.1377/hlthaff.2011.1377
20. Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res (1989) 28(2):193–213. doi: 10.1016/0165-1781(89)90047-4
21. Zeng LN, Yang Y, Wang C, Li XH, Xiang YF, Hall BJ, et al. Prevalence of Poor Sleep Quality in Nursing Staff: A Meta-Analysis of Observational Studies. Behav Sleep Med (2019), 1–14. doi: 10.1080/15402002.2019.1677233
22. Wechat. (2020). Wechat, a new lifestyle (in Chinese) 2020 [20th Feb 2020]. Available from: https://weixin.qq.com/.
23. Xi X, Liu YF. The appliation of Wechat platform and Wenjuanxing in cognitive training among psychiatric nurse, cleaning staff and patients (in Chinese). Nurs Pract Res (2017) 14(21):114–7.
24. Li F, Wu JF, Mai XH, Ning K, Chen KY, Chao L, et al. Internalized Homophobia and Depression in Homosexuals: The Role of Self-concept Clarity (in Chinese). Chin J Clin Psychol (2016) 24(3):475–9.
25. Xiang YT, Ma X, Lu JY, Cai ZJ, Li SR, Xiang YQ, et al. Alcohol-related disorders in Beijing, China: prevalence, socio-demographic correlates, and unmet need for treatment. Alcohol Clin Exp Res (2009) 33(6):1111–8. doi: 10.1111/j.1530-0277.2009.00933.x
26. Zeng LN, Zong QQ, Zhang JW, An FR, Xiang YF, Ng CH, et al. Prevalence of smoking in nursing students worldwide: A meta-analysis of observational studies. Nurse Educ Today (2020) 84:104205. doi: 10.1016/j.nedt.2019.104205
27. Becker NB, Jesus SN, Joao K, Viseu JN, Martins RIS. Depression and sleep quality in older adults: a meta-analysis. Psychol Health Med (2017) 22(8):889–95. doi: 10.1080/13548506.2016.1274042
28. Zheng B, Li M, Wang KL, Lv J. Analysis of the reliability and validity of the Chinese version of Pittsburgh sleep quality index among medical college students (in Chinese). Beijing Da Xue Xue Bao Yi Xue Ban (2016) 48(3):424–8.
29. Qiu D, Yu Y, Li RQ, Li YL, Xiao SY. Prevalence of sleep disturbances in Chinese healthcare professionals: a systematic review and meta-analysis. Sleep Med (2020) 67:258–66. doi: 10.1016/j.sleep.2019.01.047
30. Machi MS, Staum M, Callaway CW, Moore C, Jeong K, Suyama J, et al. The relationship between shift work, sleep, and cognition in career emergency physicians. Acad Emerg Med (2012) 19(1):85–91. doi: 10.1111/j.1553-2712.2011.01254.x
31. Surani AA, Surani A, Zahid S, Ali S, Farhan R, Surani S. To Assess Sleep Quality among Pakistani Junior Physicians (House Officers): A Cross−sectional Study. Ann Med Health Sci Res (2015) 5(5):329–33. doi: 10.4103/2141-9248.165246
32. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet (2020). doi: 10.1016/S0140-6736(20)30185-9
33. Wang X. (2020). Coronavirus outbreak: 444 new cases added on Friday. 2020: http://www.chinadaily.com.cn/a/202001/25/WS5e2bad63a310128217273336.html (access January 25, 2020).
34. Rawtaer I, Mahendran R, Chan HY, Lei F, Kua EH. A nonpharmacological approach to improve sleep quality in older adults. Asia Pac Psychiatry (2018) 10(2):e12301. doi: 10.1111/appy.12301
35. Dai J, Chiu HF, Xiang Y-T, Chan SS, Yu X, Hou Z-J, et al. The prevalence of insomnia and its socio-demographic and clinical correlates in older adults in rural China: a pilot study. Aging Ment Health (2013) 17(6):761–5. doi: 10.1080/13607863.2013.781117
36. Dzaja A, Arber S, Hislop J, Kerkhofs M, Kopp C, Pollmächer T, et al. Women’s sleep in health and disease. J Psychiatr Res (2005) 39(1):55–76. doi: 10.1016/j.jpsychires.2004.05.008
37. Jeong HG, Han C, Park MH, Ryu SH, Pae CU, Lee JY, et al. Influence of the number and severity of somatic symptoms on the severity of depression and suicidality in community-dwelling elders. Asia Pac Psychiatry (2014) 6(3):274–83. doi: 10.1111/appy.12138
38. Lin X, Haralambous B, Pachana NA, Bryant C, LoGiudice D, Goh A, et al. Screening for depression and anxiety among older Chinese immigrants living in Western countries: The use of the Geriatric Depression Scale (GDS) and the Geriatric Anxiety Inventory (GAI). Asia Pac Psychiatry (2016) 8(1):32–43. doi: 10.1111/appy.12191
39. Xiang Y-T, Ma X, Cai Z-J, Li S-R, Xiang Y-Q, Guo H-L, et al. The prevalence of insomnia, its sociodemographic and clinical correlates, and treatment in rural and urban regions of Beijing, China: a general population-based survey. Sleep (2008) 31(12):1655–62. doi: 10.1093/sleep/31.12.1655
40. Li RH, Wing YK, Ho SC, Fong SY. Gender differences in insomnia–a study in the Hong Kong Chinese population. J Psychosom Res (2002) 53(1):601–9. doi: 10.1016/S0022-3999(02)00437-3
41. Zhang J, Lam SP, Li SX, Tang NL, Yu MW, Li AM, et al. Insomnia, sleep quality, pain, and somatic symptoms: sex differences and shared genetic components. Pain (2012) 153(3):666–73. doi: 10.1016/j.pain.2011.12.003
42. Zhang B, Wing YK. Sex differences in insomnia: a meta-analysis. Sleep (2006) 29(1):85–93. doi: 10.1093/sleep/29.1.85
43. Suh S, Cho N, Zhang J. Sex Differences in Insomnia: from Epidemiology and Etiology to Intervention. Curr Psychiatry Rep (2018) 20(9):69. doi: 10.1007/s11920-018-0940-9
44. Chung MS, Chiu HJ, Sun WJ, Lin CN, Kuo CC, Huang WC, et al. Association among depressive disorder, adjustment disorder, sleep disturbance, and suicidal ideation in Taiwanese adolescent. Asia Pac Psychiatry (2014) 6(3):319–25. doi: 10.1111/appy.12112
45. Barsky AJ, Peekna HM, Borus JF. Somatic symptom reporting in women and men. J Gen Intern Med (2001) 16(4):266–75. doi: 10.1046/j.1525-1497.2001.016004266.x
46. Xiang Y, Jin Y, Wang Y, Zhang QE, Zhang L, Cheung T. Tribute to health workers in China: a group of respectable population during the outbreak of the COVID-19. Int J Biol Sci (2020a). doi: 10.7150/ijbs.45135
47. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open (2020) 3(3):e203976. doi: 10.1001/jamanetworkopen.2020.3976
Keywords: COVID-19, China, health professionals, sleep quality, Pittsburgh Sleep Quality Index
Citation: Zhou Y, Yang Y, Shi T, Song Y, Zhou Y, Zhang Z, Guo Y, Li X, Liu Y, Xu G, Cheung T, Xiang Y-T and Tang Y (2020) Prevalence and Demographic Correlates of Poor Sleep Quality Among Frontline Health Professionals in Liaoning Province, China During the COVID-19 Outbreak. Front. Psychiatry 11:520. doi: 10.3389/fpsyt.2020.00520
Received: 24 March 2020; Accepted: 21 May 2020;
Published: 12 June 2020.
Edited by:
Ahmed S. BaHammam, King Saud University, Saudi ArabiaReviewed by:
Haitham Jahrami, Arabian Gulf University, BahrainCopyright © 2020 Zhou, Yang, Shi, Song, Zhou, Zhang, Guo, Li, Liu, Xu, Cheung, Xiang and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu-Tao Xiang, eHl1dGx5QGdtYWlsLmNvbQ==; Yanqing Tang, dGFuZ3lhbnFpbmdAY211LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.