 Felipe Cesar de Almeida Claudino1*
Felipe Cesar de Almeida Claudino1* Leonardo Gonçalves1
Leonardo Gonçalves1 Felipe Barreto Schuch2
Felipe Barreto Schuch2 Hugo Roberto Sampaio Martins3
Hugo Roberto Sampaio Martins3 Neusa Sica da Rocha1
Neusa Sica da Rocha1- 1Center of Clinical Research and Center of Experiamental Research, Hospital de Clínicas de Porto Alegre (HCPA), Post-Graduation Program in Psychiatry and Behavioral Sciences, Federal University of Rio Grande do SUl (UFRGS), Porto Alegre, Brazil
- 2Department of Sports Methods and Techniques, Federal University of Santa Maria (UFSM), Santa Maria, Brazil
- 3Department of Internal Medicine, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Brazil
Background: Brain-derived Neurotrophic Factor (BDNF) is considered the main cerebral neurotrophin and is produced in the central neural system and peripherals. Its levels are reduced in patients with several psychiatric disorders, but it is unclear if the response to psychotherapy can alter its concentration.
Objective: To carry out a systematic review evaluating the effects of individual psychotherapy in BDNF levels in patients with mental disorders.
Methods: The databases PubMed, EMBASE, PsycArticles, SciELO, Web of Science, and CENTRAL; the last search was performed on October 2019 for trials evaluating the effects of individual psychotherapy in BDNF levels in adults with mental disorders. PROSPERO registration: CRD42018108144.
Results: Eight of 293 studies were included. A rise in BDNF levels was observed in depressive patients when psychotherapy was combined with medication. Patients with post-traumatic stress disorder (PTSD) who responded to therapy presented a raise in BDNF levels mostly when combined with physical activity. There was a rise in BDNF levels in those who responded to psychotherapy in patients with bulimia, in borderline patients, and in insomniacs.
Conclusions: The BDNF seems to present variations after psychotherapy especially in patients with bulimia, PTSD, insomnia, and borderline. These subjects also have symptom reduction. Thereby, BDNF could be a supplemental tool to analyze the success to psychotherapy. BDNF levels in patients with major depression after therapy are still controversial and the short follow-up of most studies is a limiting factor.
Introduction
Psychotherapy is a well-grounded treatment for mental disorders with outcomes similar to pharmacotherapy (1). Psychotherapeutic interventions consist of exposure to stimuli, content resignification, and behavioral changes via interpersonal interaction (2). It acts on cognition and leads to symptoms remission, the formation of new neural networks, and can consequently lead to changes in demeanor (3). The neurotrophins are peptides in the central nervous system, and the most abundant is brain-derived neurotrophic factor (BDNF) (4), which stands out among the responsible factors in the formation of new neural networks that result in improved symptomatology.
BDNF is a neurotrophin that is more concentrated in certain regions of the brain such as the pre-frontal cortex and the hippocampus (5)—regions where complex cognitive processes occur including memory, personality, and emotional control. Therefore, psychotherapy stimulates these areas (6) reflecting on psychological symptom remission and resulting in a rise in BDNF levels.
Peripheral BDNF concentrations are lower in people with neuropsychiatric and neurodegenerative diseases (7, 8) versus matched controls. There is also signaling interference of this peptide in limbic areas related to emotion such as the hippocampus (9) that may contribute to the maintenance of the diseases.
BDNF levels also rise after antidepressant treatment, and increase in BDNF are associated with symptom improvements (10, 11); thus, it might be a potential mediator of the antidepressant treatment (12). Beyond pharmacological treatment, it is possible to observe increases in this neurotrophin's levels via electroconvulsive therapy (13) and physical activity (14) concurrent to the remission of psychological symptoms. Previous reviews of psychotherapies showed few potential response biomarkers for this treatment in patients diagnosed with PTSD such as the 5-alfa-reductase, heart rate changes (15), glucocorticoid metabolism, gene methylation, (16) and structural brain changes (17).
Despite the promising effects of psychotherapy response biomarkers, there is no systematic review evaluating the effects of individual psychotherapy in BDNF levels. Therefore, the objectives of this study are to: 1) evaluate if there are any changes in BDNF levels in people with mental disorders following individual psychotherapy and 2) evaluate if these changes are associated with symptom improvement.
Methods
Study Eligibility
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (18). The protocol was registered on PROSPERO: CRD42018108144.
Inclusion Criteria
The study population defined: patients over 18 years old, both genders, previously diagnosed with psychiatric disorders and/or mental disorders by qualified professionals and with its pathology described in the Diagnostic and Statistical Manual of Mental Disorders (DSM V).
The interventions of interest for the study: in-person individual psychotherapy: cognitive behavioral therapy, psychoanalysis, eye movement desensitization and reprocessing (EMDR), dialectical behavior therapy, interpersonal psychotherapy, analytically-oriented psychotherapy, and acceptance/commitment therapy, without limit of sessions or length of treatment.
Control groups defined: patients with no mental disorders or patients with psychiatric disorders submitted to other comparative treatments that are not psychotherapy, such as physical activity, meditation, and electroconvulsotherapy.
For the outcome, BDNF levels and disorder symptoms (according to symptom scales) were measured at two different times before and after psychotherapy exposure. Only serum or plasma BDNF levels were considered.
We included longitudinal randomized or non-randomized clinical trials as well as prospective and retrospective cohort studies; there was no language restriction, and any year of publication was considered including studies in progress.
Exclusion Criteria
Patients undergoing only group therapy, online therapy, those without pre and post intervention BDNF serum or plasma levels, and patients who did not have their symptoms evaluated pre and post intervention were not included. Cross-sectional or case reports were not considered.
Search Strategy and Study Selection
The titles and/or abstracts were obtained by two independent evaluators (FC and HM) by searching the following databases in October 2019: PubMed, EMBASE, PsycArticles, Scielo, CENTRAL, and Web of Science. The following terms were used for the research in PubMed: (“cognitive behavioral therapy” OR CBT OR “cognitive behavior therapy” OR “cognitive behavior treatment” OR “cognitive-behavioral treatment” OR “cognitive behavior therapy” OR “cognitive behaviour treatment” OR “cognitive behavioral therapy” OR “cognitive behavioural treatment”) OR [(psychotherapy OR “psychotherapeutic processes”) OR “Cognitive Therapy” OR (“psychotherapy, brief” OR “short-duration psychotherapy”) OR “interpersonal therapy” OR “analytical psychotherapy” OR “eye movement desensitization and reprocessing” OR EMDR] AND (“brain derived neurotrophic factor” OR BDNF OR neurotrophin OR neurogenesis OR “nerve cell plasticity” OR “brain plasticity” OR “nerve plasticity” OR “neural plasticity” OR neuroplasticity). The terms were adjusted according to the protocols in each database.The searches in each database were realized twice by two independent evaluators, adapting pre-defined terms following the protocol for each base (such as Mesh terms for PUBMED and thesaurus for Embase, for example). In any divergence regarding the abstracts of each database, an independent third party realized a new search. Independent search results were confronted and divergences were resolved by a third independent party. Abstracts from “grey literature” were only considered if available in the evaluated databases.
The study selection was conducted in two steps. First, the title and abstract of the articles obtained in the search were analyzed by two independent authors (FC and HM) and selected according to the inclusion and exclusion criteria. Next, the remaining articles were read in full. A third reviewer was recruited in case of any disagreement on the inclusion or exclusion of studies at any stage.
Data Extraction and Analysis
Two authors, independently, extracted data on the following metrics, previously defined in pilot forms: year of publication, country, study design, patient precedence, sex, number of participants, disorder type, therapy type, therapy length, total of sessions, BDNF (plasma or serum), mean and standard deviation of BDNF levels (pre and post intervention), symptom measures, and complementary therapies (pharmacotherapy or else).
Assessment of Risk of Bias
Two instruments were used to evaluate the “Assessment of risk of bias”: The New Castle-Ottawa (19) was indicated for longitudinal non-randomized studies. It evaluates aspects such as selection, comparability, and outcome (Table 1). Its scores vary between 0 (highest bias) to 9 points (lowest bias). The Cochrane Collaboration's tool assessed risk of bias for randomized studies (Table 2) (28). This allows evaluation as “high”, “low”, or “unclear” risk of bias for each domain: selection, attrition, detection, performance, reporting, and others. The intra-study risk of bias was also included (Table 3). There was no exclusion of articles, regardless of the score, due to the small number of studies obtained, but the restrictions were considered when analyzing the individual results.
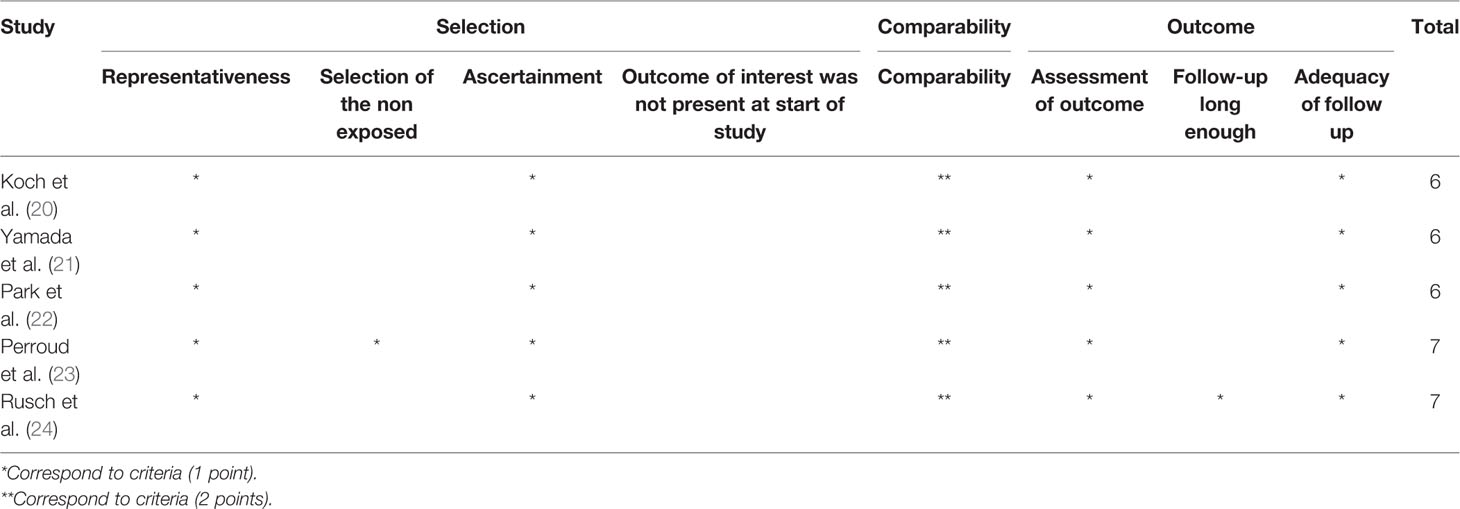
Table 1 Evaluation of the methodological quality of longitudinal studies using the Newcastle-Ottawa scale.

Table 2 Evaluation of the methodological quality of randomized studies using Cochrane Collaboration's tool for assessing risk of bias for studies.
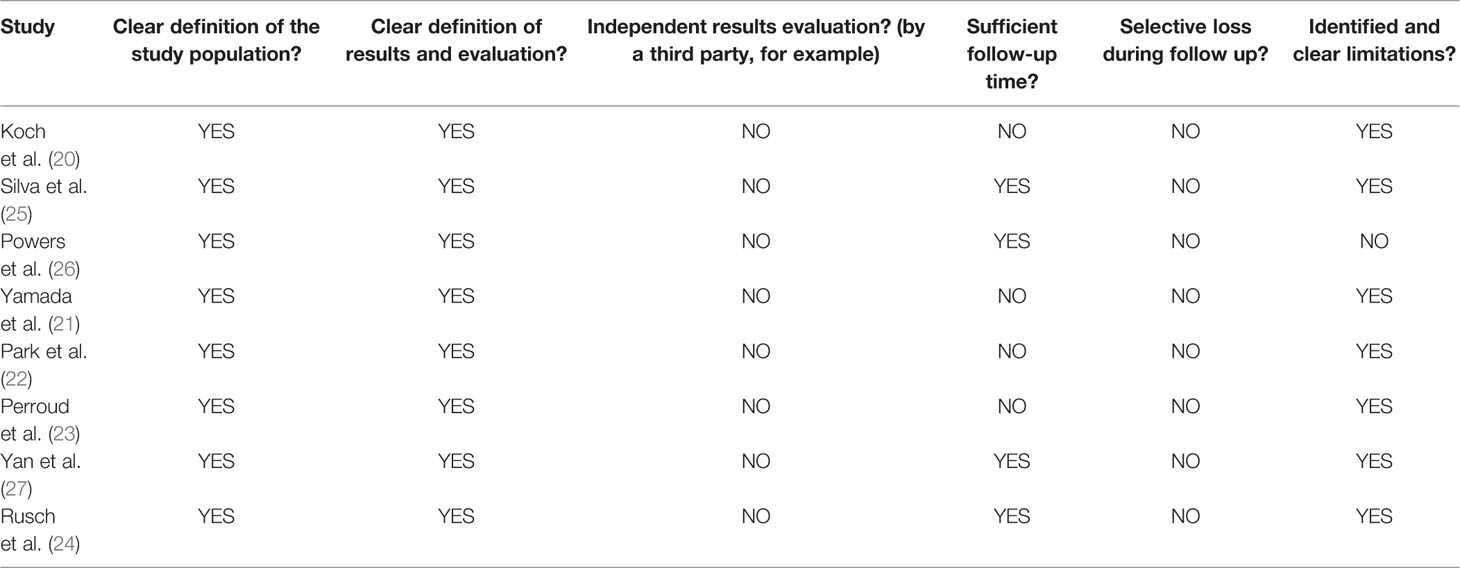
Table 3 Evaluation of Intra-study bias risk of studies included.
Searches Results
A total of 4,895 references were found. Of these, 1,808 were duplicates and excluded. Thus, 3,087 abstracts were evaluated in terms of title and abstract followed by exclusion of 2,995 by criteria shown in the figure below. At the full-text stage, 92 articles were read in full, and 8 articles were added to the review and inspected followed by two proofreaders (Figure 1).
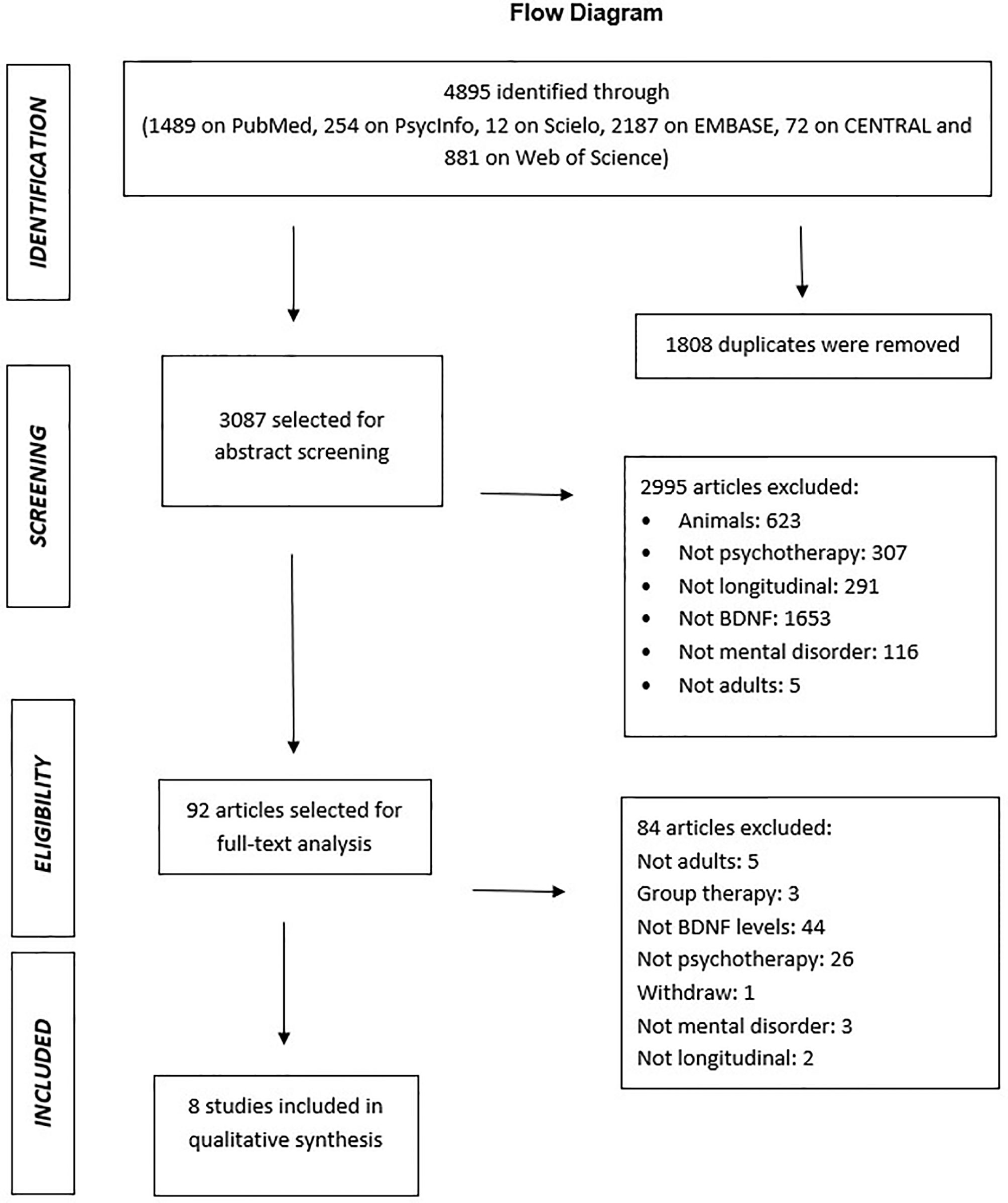
Figure 1 PRISMA flowchart of article selection (18).
Main Mental Disorders Studied
The main features of the studies are detailed in Table 4. We found studies evaluating BDNF levels in people with major depressive disorder (k=3), PTSD (k=2), bulimia (k=1), borderline disorder (k=1), and sleep disorder (K=1) with a predominance in women in five studies (55, 5–100%); three studies have a predominance of male patients. The number of patients varied between n=7 and n=115. Most patients came from outpatient clinics (k=4), and the treatment extent was 4 weeks to 12 months.
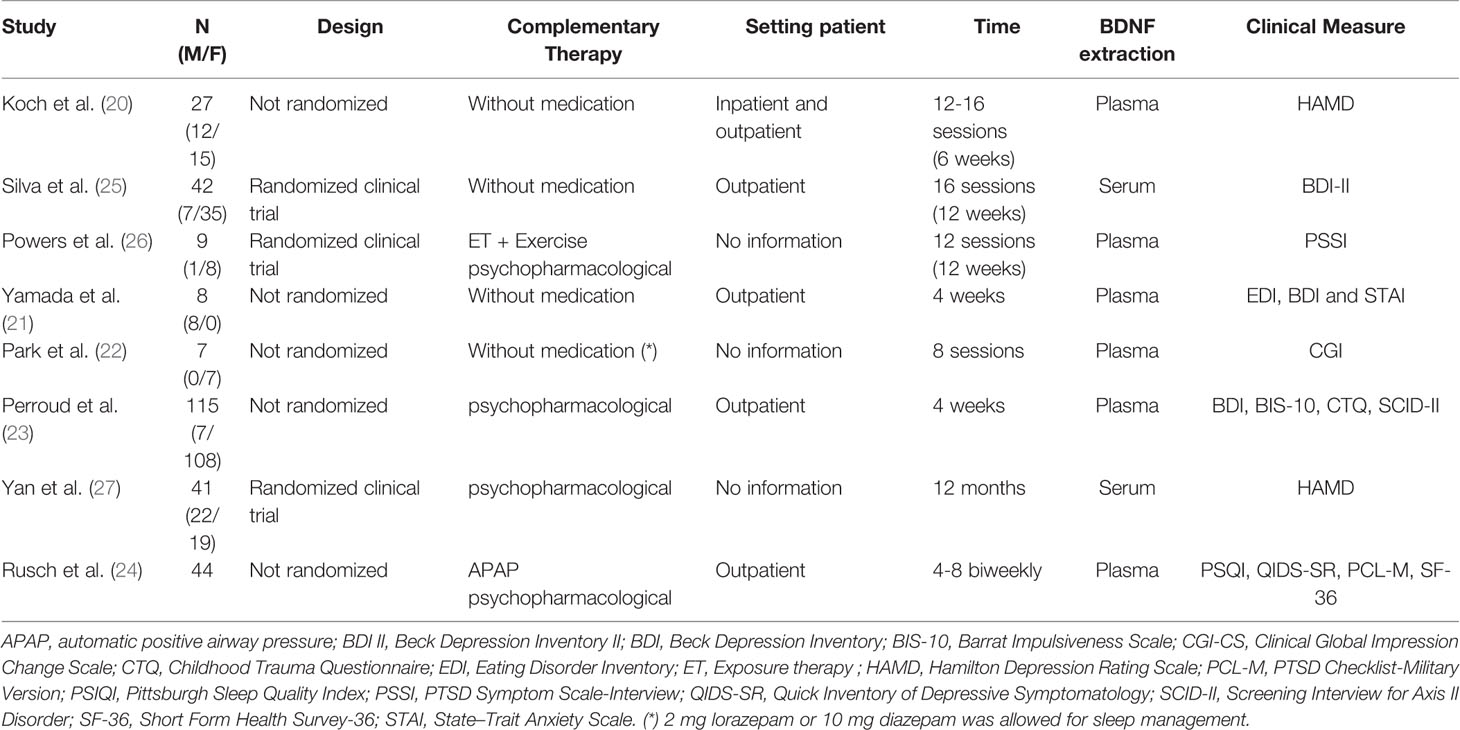
Table 4 Characteristics of included studies.
Main Clinical Measures Evaluated and Diagnosis Criteria
The diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders IV (29, 30) (k=3), SIDES (Structured Interviews for Disorders of Extreme Stress) (31) (k=1), Mini International Neuropsychiatric Interview (MINI-PLUS) (32) (k=1), Classification and Diagnostic Criteria for Mental Disorder in China 3 (CCMD-3) (33), and Epworth Sleepiness Scale (ESS) (34) were used. Different scales were used for the symptom evaluation: Hamilton Depression Rating Scale (35), (BDI) Beck Depression Inventory (36, 37), PTSD Symptom Scale-Interview Version (38), State–Trait Anxiety Scale (39), Clinical Global Impression Change Scale (CGI-CS) (40), (BIS-10): Barrat Impulsiveness Scale (41), (CTQ): Childhood Trauma Questionnaire (42), (SCID-II): Screening Interview for Axis II Disorder (43), (PSIQI): Pittsburgh Sleep Quality Index (44), (QIDS-SR): Quick Inventory of Depressive Symptomatology (45), (PCL-M): PTSD Checklist-Military Version (46), and (SF-36): Short From Health Survey-36 (47).
All studies presented symptom reduction on these scales. Three articles branched the patients into responders depending on the reduction of 50% of the HAMD (20) or BDI (23). baseline and CGI-C scores above the “much improved” level after therapy (22)
Complementary Psychopharmacotherapy
Three of the articles included psychopharmacotherapy as a complementary therapy. Those diagnosed with insomnia could use automatic positive airway pressure (APAP). Only one study included physical activity versus complementary therapy (19). Six of the eight studies analyzed plasma levels of BDNF, and two opted for serum levels.
Psychotherapy, Scales, and BNDF Levels
The main results of individual studies are described in Table 5. No significant changes in BDNF levels were observed in depressive patients and those who submitted to interpersonal therapy: [baseline responders (mean ±SD): 3.3±.3.7 x non-responders 2.8±1.3 p=0.68; Day 21-responders: 3.4 ±3.6 x non-responders 3.1±2.3 p=0.97] (17) or Cognitive-Behavioral Therapy [pre-treatment (mean ±SD) 1.387±0.26; post-treatment 1.328±0.3, p= 0.294] (18). However, the responders initially had a higher level of neurotrophin and a higher increase versus non-responders (17). In a study of medication associated with therapy, the group using only vortioxetine had a significant difference in BDNF levels between intervention and control groups in baseline and after. The group who underwent CBT associated with medication had a significant increase versus the control group (p<0.001) (27).
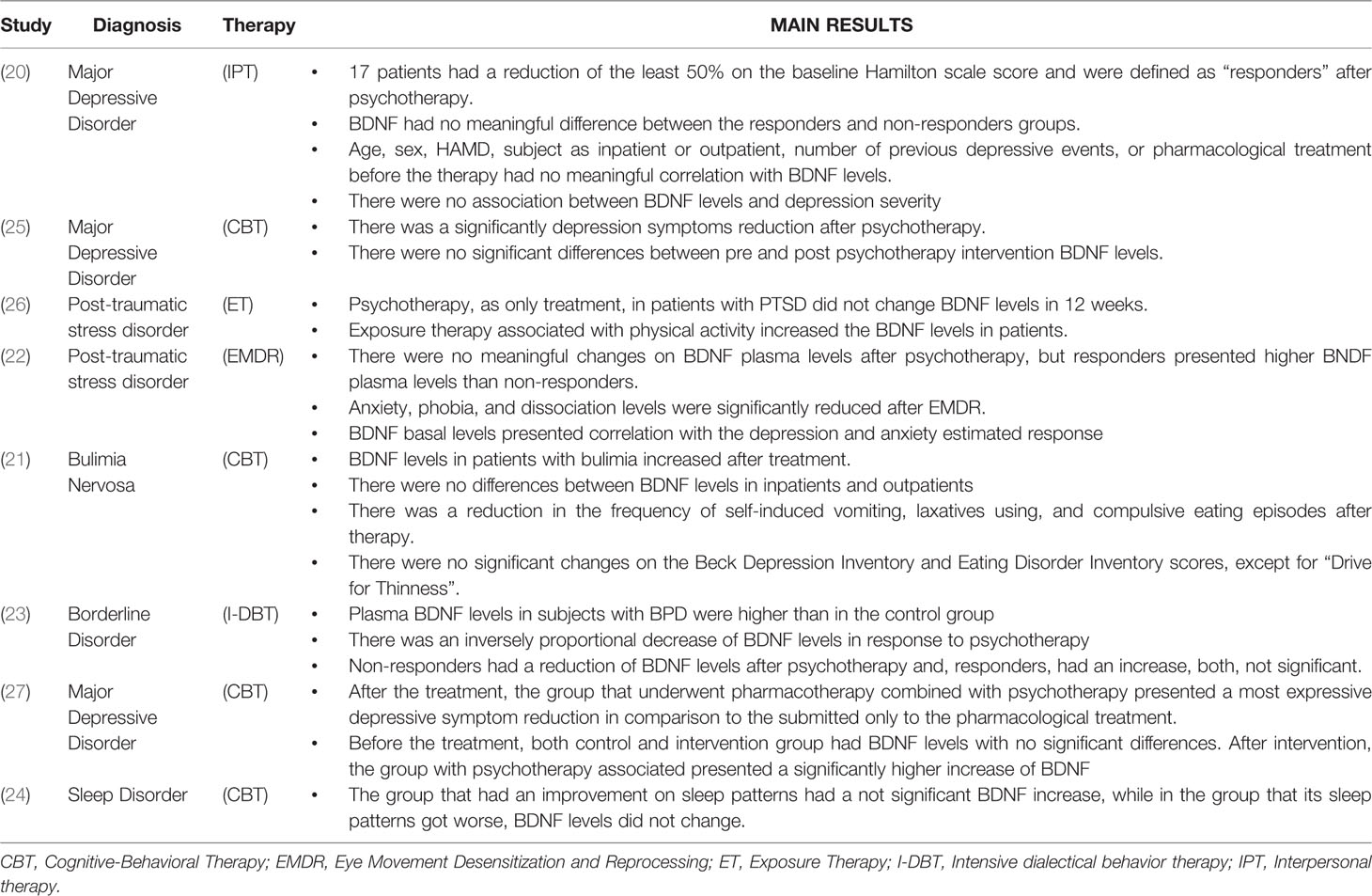
Table 5 Main results.
Two studies (19, 28) in PTSD patients have shown increased levels of BDNF after intervention in different modalities: exposure therapy (19) and eye movement desensitization and reprocessing (28). The first study related elevation of neurotrophin when psychotherapy was associated with physical activity (mean ±SD) (pre: 1.38 x post: 3.73). Their values were not expressive in isolation (pre: 1.77 x post: 1.75) and PSSI: PE (prolonged exposure therapy): (mean ±SD) 37.00 (8.25); PE+ Exercise: 42.00 (5.2) (19). However, the second study indicated that patients who presented a clinical response or symptom remission symptoms had higher increases in BDNF than those who did not respond to treatment [responders: (mean ±SD 4435.6±1273.4; non-responders 2789±643.2; p 0.025)]. There was an association between the increase of BDNF levels and symptoms reduction such as anxiety, phobia, and dissociation after EMDR in patients with PTSD (19).
At baseline, patients with bulimia nervosa undergoing eye movement desensitization and reprocessing had reduced BDNF values versus controls (p = 0.02)—this has been established in previous studies. This sample presented elevation of BDNF levels which were more expressive among responders than non-responders. The pre and post therapy scale scores of responders are listed here: BDI pre (mean ±SD) 22±11.9, post: 17.4±15.2, p=0.22, STAI-state pre: 56±12.9, post 50±17.7, p=0.07, STAI-trait pre: 65.8±10.1, post: 55.2±18.5, p 0.08 (13).
Borderline personality diagnosed patients had a higher BDI mean than the healthy control group (mean ± SD 34.10±11.8) similar to other symptom scales. Responders had an insignificant increase in plasma BDNF levels (p=0.062), as non-responders had insignificant reduction (p=0.78) (23).
Finally, patients with sleep disorders were divided between those who presented an improved sleep pattern and those who got worse. The first group presented an insignificant BDNF increase (pre: 80.2± 28.6; post 89.1±36.3; p =0.089). BDNF levels were stable in the group with no improvement (pre: 91.7±38.1; post 100.2±44.4; p=0.155) (27).
Discussion
To the best of our knowledge, this is the first systematic review to evaluate the relation between BDNF levels in response to psychotherapies. The results showed that, in general, there was a reduction of clinical symptoms in patients with mental disorders that went through different kinds of psychotherapies. In most cases, there was also a concurrent rise in BDNF levels.
In central nervous system, the levels of BDNF are higher in structures of the limbic system, such as the hippocampus (48) and, in patients with mental disorders, the neurotrophin concentration in this region is reduced (49). Meanwhile, the psychotherapy has the potential for stimulation of the limbic system and (50), although the physiology is not clear until this moment, we can assume que psychotherapies act in this system, stimulating a higher BDNF production, reducing psychiatric symptoms.
While this present review showed that there is no absolute consensus regarding BDNF levels rise after psychotherapy, there is meta-analysis that shows evidence of the increase of BDNF after pharmacological treatment (51, 52). Although both treatments are recognized as effective, this difference can be explained by the short follow-up time of the patients. The response to pharmacological therapy tends to occur faster (53), while the response to psychotherapy may take months (54), depending on factors such as therapeutic relation, for example (55).
These findings showed initial evidence that BDNF could be a potential tool to evaluate the effect of psychotherapies on patients with mental disorders. The BDNF levels could be used with symptom evaluation and other tools such as clinical symptom scales to confirm that there is a satisfactory response to therapy. Furthermore, BDNF levels tend to be stable over time (56), and psychotherapy can be a variable course. Thus, such levels might change at a different rate versus those observed here. Only one of our manuscripts had a follow-up longer than 12 weeks. Prior reviews and meta-analyses have shown that there is an increase in BDNF levels in depressive patients treated with pharmacologically (57) or with physical activity (58). Healthy patients have stable BDNF levels over time, which favors the theory that patients with mental disorders submitted to therapies have an increase in neurotrophins as an outcome. However, in this review, only patients using medication associated with psychotherapy had an increased BDNF.
Although there is initial evidence for the role of BDNF as an individual psychotherapy response biomarker, the heterogeneity across the studies limit the conclusions of this meta-analysis—the groups had different disorders, types of therapies, therapy exposure times, and others boundary conditions that may affect the results. The literature is restricted to depression, PTSD, bulimia, insomnia, and borderline disorders. Thus, the conclusions cannot be extended to other disorders like bipolar disorder and anxiety disorders.
We also cannot disregard the relevance of polymorphism knowledge in response to psychotherapies. A biological response marker could also be expanded to other biomarkers. Longitudinal studies evaluating BDNF levels in response to psychotherapy could facilitate the performance of a meta-analysis of such candidate biomarkers.
Limitations
The conclusions of this review must be cautious because the studies included in this review are small, most of which with a short follow up period. As to BDNF values, the included studies quantified serum and plasma BDNF levels and there is evidence that the levels of these molecules change according to analyzed tissue and organs (59, 60) Also, it isn't possible to quantify the proBDNF precursor and its derivatives values: mature BDNF and pro-peptide BDNF. It is relevant to know this data, for there is evidence that they have different effects in the physiopathology of psychiatric disorder (61). As well, age (62) and ethnicity (63) may interfere in BDNF levels and also were not considered while quantifying the neurotrophin.
Conclusion
In conclusion, there is a nascent body of evidence evaluating the effects of individual psychotherapies on BDNF. These neurotrophins seem to present variations after psychotherapy especially in patients with bulimia, PTSD, insomnia, and borderline personality, and that show reductions in symptoms. In patients with depression, those who submitted only to psychotherapy had no increase in BDNF levels while patients with associated medicine usage showed an obviously higher increase versus those who submitted solely to pharmacological treatment. There is only one study with a higher than 12-week follow-up period, which suggests that a longer follow-up time is needed for BDNF levels. BDNF could supplement symptom scales to analyze the effects of psychotherapy.
Data Availability Statement
The data set obtained for this study are available from corresponding author on request.
Author Contributions
FC: preparation and registration of the review protocol, extraction of articles in the databases, selection of articles, analysis of results, and article production. LG: protocol production, results analysis, and article production. FS: protocol production, results analysis, and article production. HM: preparation of the review protocol, extraction of articles in the databases, selection of articles, analysis of results, and article production. NR: main orientation, protocol production, review of articles in case of divergence, analysis of results, and article production.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brasil (CAPES)—Finance Code 001 and by Hospital de Clínicas de Porto Alegre Research Incentive Fund (FIPE).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
FC is supported by a doctoral scholarship from Coordenacão de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil.
References
1. Huhn M, Tardy M, Spineli L, Kissling W, Förstl H, Pitschel-Walz G, et al. Efficacy of Pharmacotherapy and Psychotherapy for Adult Psychiatric Disorders. JAMA Psychiatry (2014) 71(6):706–15. doi: 10.1001/jamapsychiatry.2014.112
3. Leeman E, Leeman S. Elements of Dynamics IV: Neuronal Metaphors—Probing Neurobiology for Psychodynamic Meaning. J Am Acad Psychoanal Dyn Psychiatry (2004) 32(4):645–59. doi: 10.1521/jaap.32.4.645.53837
4. Neves C, Lacerda A, Lima L, Lage V, Balthazar C, Leite H, et al. Different levels of brain-derived neurotrophic factor and cortisol in healthy heavy smokers. Braz J Med Biol Res (2017) 50(12):1–5. doi: 10.1590/1414-431x20176424
5. Pezawas L. The Brain-Derived Neurotrophic Factor val66met Polymorphism and Variation in Human Cortical Morphology. J Neurosci (2004) 24(45):10099–102. doi: 10.1523/JNEUROSCI.2680-04.2004
6. Ritchey M, Dolcos F, Eddington K, Strauman T, Cabeza R. Neural correlates of emotional processing in depression: Changes with cognitive behavioral therapy and predictors of treatment response. J Psychiatr Res (2011) 45(5):577–87. doi: 10.1016/j.jpsychires.2010.09.007
7. Boulle F, van den Hove D, Jakob S, Rutten B, Hamon M, van Os J, et al. Epigenetic regulation of the BDNF gene: implications for psychiatric disorders. Mol Psychiatry (2011) 17(6):584–96. doi: 10.1038/mp.2011.107
8. Zuccato C, Cattaneo E. Brain-derived neurotrophic factor in neurodegenerative diseases. Nat Rev Neurol (2009) 5(6):311–22. doi: 10.1038/nrneurol.2009.54
9. Smith M, Makino S, Kvetnanský R, Post R. Effects of Stress on Neurotrophic Factor Expression in the Rat Brain. Ann New York Acad Sci (1995) 771(1 Stress):234–9. doi: 10.1111/j.1749-6632.1995.tb44684.x
10. Brunoni A, Lopes M, Fregni F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: implications for the role of neuroplasticity in depression. Int J Neuropsychopharmacol (2008) 11(8):1169–80. doi: 10.1017/S1461145708009309
11. Sen S, Duman R, Sanacora G. Serum Brain-Derived Neurotrophic Factor, Depression, and Antidepressant Medications: Meta-Analyses and Implications. Biol Psychiatry (2008) 64(6):527–32. doi: 10.1016/j.biopsych.2008.05.005
12. Kurita M, Nishino S, Kato M, Numata Y, Sato T. Plasma Brain-Derived Neurotrophic Factor Levels Predict the Clinical Outcome of Depression Treatment in a Naturalistic Study. PloS One (2012) 7(6):e39212. doi: 10.1371/journal.pone.0039212
13. Brunoni A, Baeken C, Machado-Vieira R, Gattaz W, Vanderhasselt M. BDNF blood levels after electroconvulsive therapy in patients with mood disorders: A systematic review and meta-analysis. World J Biol Psychiatry (2014) 15(5):411–8. doi: 10.3109/15622975.2014.892633
14. Phillips C. Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection. Neural Plast (2017) 2017:1–17. doi: 10.1155/2017/7260130
15. Gonçalves R, Lages A, Rodrigues H, Pedrozo A, Coutinho E, Neylan T, et al. Potenciais biomarcadores da terapia cognitivo-comportamental para o transtorno de estresse pós-traumático: uma revisão sistemática. Arch Clin Psychiatry (São Paulo) (2011) 38(4):155–60. doi: 10.1590/S0101-60832011000400008
16. Colvonen P, Glassman L, Crocker L, Buttner M, Orff H, Schiehser D, et al. Pretreatment biomarkers predicting PTSD psychotherapy outcomes: A systematic review. Neurosci Biobehav Rev (2017) 75:140–56. doi: 10.1016/j.neubiorev.2017.01.027
17. Linden D. How psychotherapy changes the brain – the contribution of functional neuroimaging. Mol Psychiatry (2006) 11(6):528–38. doi: 10.1038/sj.mp.4001816
18. Liberati A, Altman D, Tetzlaff J, Mulrow C, Gøtzsche P, Ioannidis J, et al. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
19. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
20. Koch J, Hinze-Selch D, Stingele K, Huchzermeier C, Göder R, Seeck-Hirschner M, et al. Changes in CREB Phosphorylation and BDNF Plasma Levels during Psychotherapy of Depression. Psychother Psychosom (2009) 78(3):187–92. doi: 10.1159/000209350
21. Yamada H, Yoshimura C, Nakajima T, Nagata T. Recovery of low plasma BDNF over the course of treatment among patients with bulimia nervosa. Psychiatry Res (2012) 198(3):448–51. doi: 10.1016/j.psychres.2011.12.015
22. Park S, Park Y, Lee M, Chang H. Plasma brain-derived neurotrophic factor level may contribute to the therapeutic response to eye movement desensitisation and reprocessing in complex post-traumatic stress disorder: a pilot study. Acta Neuropsychiatr (2012) 24(6):384–6. doi: 10.1111/j.1601-5215.2011.00623.x
23. Perroud N, Salzmann A, Prada P, Nicastro R, Hoeppli M, Furrer S, et al. Response to psychotherapy in borderline personality disorder and methylation status of the BDNF gene. Trans Psychiatry (2013) 3(1):e207–7. doi: 10.1038/tp.2012.140
24. Rusch H, Guardado P, Baxter T, Mysliwiec V, Gill J. Improved Sleep Quality is Associated with Reductions in Depression and PTSD Arousal Symptoms and Increases in IGF-1 Concentrations. J Clin Sleep Med (2015) 11(6):615–23. doi: 10.5664/jcsm.4770
25. da Silva S, Wiener C, Ghisleni G, Oses J, Jansen K, Molina M, et al. Effects of cognitive-behavioral therapy on neurotrophic factors in patients with major depressive disorder. Rev Bras Psiquiatr (2018) 40(4):361–6. doi: 10.1590/1516-4446-2017-2357
26. Powers M, Medina J, Burns S, Kauffman B, Monfils M, Asmundson G, et al. Exercise Augmentation of Exposure Therapy for PTSD: Rationale and Pilot Efficacy Data. Cogn Behav Ther (2015) 44(4):314–27. doi: 10.1080/16506073.2015.1012740
27. Yan G, Zhang M, Liu Y, Yin M. Efficacy of vortioxetine combined cognitive behaviour intervention therapy on brain-derived neurotrophic factor level on depressive patients. Psychogeriatrics (2019) 19(5):475–81. doi: 10.1111/psyg.12426
28. Higgins J, Altman D, Gotzsche P, Juni P, Moher D, Oxman A, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ (2011) 343(oct18 2):d5928–8. doi: 10.1136/bmj.d5928
29. Takahashi S, Kitamura T, Okano T, Tomita T, Kikuchi A. Japanese Version of Structured Clinical Interview for DSM-VI Axis I Disorders. Tokyo, Japan: Nihon Hyoronsha; (2003).
30. American Psychiatric Association. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington: American Psychiatric Association; (1994).
31. Pelcovitz D, van der Kolk B, Roth S, Mandel F, Kaplan S, Resick P. Development of a Criteria Set and a Structured Interview for Disorders of Extreme Stress (SIDES). J Trauma Stress (1997) 10(1):3–16. doi: 10.1023/A:1024800212070
32. Sheehan D, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J Clin Psychiatry (1998) 59(20):22–33. doi: 10.1037/t18597-000
33. Chinese Society of Psychiatry. The Chinese Classification and Diagnostic Criteria of Mental Disorders Version 3 (CCMD-3). Jinan: Chinese Society of Psychiatry (2001).
34. Johns M. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep (1991) 14(6):540–5. doi: 10.1093/sleep/14.6.540
35. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry (1960) 23(1):56–62. doi: 10.1136/jnnp.23.1.56
38. Foa E, Riggs D, Dancu C, Rothbaum B. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Trauma Stress (1993) 6(4):459–73. doi: 10.1002/jts.2490060405
39. Spielberger C, Gorsuch R, Lushene H. Stai manual for the State-Trait Anxiety Inventory. Palo Alto: CA Consulting Psychologist Press; (1970).
40. Guy W, Clinical global impression (CGI). ECDEU Assessment Manual for Psychopharmacology. US Department of Health and Human Services, Public Health Service, Alcohol Drug Abuse and Mental Health Administration, NIMH Psychopharmacology Research branch. Rockville, MD: National Institute of Mental Health; (1976) p. 218–22-1.
41. Baylé F, Bourdel M, Caci H, Gorwood P, Chignon J, Adés J, et al. Structure factorielle de la traduction française de l'échelle d'impulsivité de Barratt (BIS-10). Can J Psychiatry (2000) 45(2):156–65. doi: 10.1177/070674370004500206
42. Bernstein DP, Fink L. Childhood Trauma Questionnaire. A Retrospective Self-Report. San Antonio;: The Psychological Corporation (1998).
43. First M, Gibbon M, Spitzer R, Williams JBW, Smith Benjamin L. Structured Clinical Interview for DSM-IV Personality Disorders (SCID-II). Washington DC;: American Psychiatric Association (1994).
44. Buysse D, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res (1989) 28(2):193–213. doi: 10.1016/0165-1781(89)90047-4
45. Rush A, Trivedi M, Ibrahim H, Carmody T, Arnow B, Klein D, et al. The 16-Item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry (2003) 54(5):573–83. doi: 10.1016/S0006-3223(02)01866-8
46. Weathers F, Keane T, Davidson J. Clinician-administered PTSD scale: A review of the first ten years of research. Depression Anxiety (2001) 13(3):132–56. doi: 10.1002/da.1029
47. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care (1992) 30(6):473–83. doi: 10.1097/00005650-199206000-00002
48. Hofer M, Pagliusi SR, Hohn A, Leibrock J, Barde YA. Regional distribution of brain-derived neurotrophic factor mRNA in the adult mouse brain. EMBO J (1990) 9:2459–64. doi: 10.1002/j.1460-2075.1990.tb07423.x)
49. Reinhart V, Bove SE, Volfson D, Lewis DA, Kleiman RJ, Lanz TA. Evaluation of TrkB and BDNF transcripts in prefrontal cortex, hippocampus, and striatum from subjects with schizophrenia, bipolar disorder, and major depressive disorder. Neurobiol Dis (2015) 77:220–7. doi: 10.1016/j.nbd.2015.03.011)
50. Goldapple K, Segal Z, Garson C, Lau M, Bieling P, Kennedy S, et al. Modulation of cortical-limbic pathways in major depression: treatment-specific effects of cognitive behavior therapy. Arch Gen Psychiatry (2004) 61:34–41. doi: 10.1001/archpsyc.61.1.34
51. Zhou C, Zhong J, Zou B, Fang L, Chen J, Deng X, et al. Meta-analyses of comparative efficacy of antidepressant medications on peripheral BDNF concentration in patients with depression. PLoS One (2017) 12(2):e0172270. doi: 10.1371/journal.pone.0172270
52. Polyakova M, Stuke K, Schuemberg K, Mueller K, Schoenknecht P, Schroeter ML. BDNF as a biomarker for successful treatment of mood disorders: a systematic & quantitative meta-analysis. J Affect Disord (2015) 174:432–40. doi: 10.1016/j.jad.2014.11.044
53. Machado-Vieira R, Baumann J, Wheeler-Castillo C, Latov D, Henter ID, Salvadore G, et al. The Timing of Antidepressant Effects: A Comparison of Diverse Pharmacological and Somatic Treatments. Pharma (Basel) (2010) 3(1):19–41. doi: 10.3390/ph3010019
54. Hansen NB, Lambert MJ, Forman EM. The Psychotherapy Dose-Response Effect and Its Implications for Treatment Delivery Services. Clin Psychol: Sci Pract (2006) 9(3):329–43. doi: 10.1093/clipsy.9.3.329
55. Ardito RB, Rabellino D. Therapeutic alliance and outcome of psychotherapy: historical excursus, measurements, and prospects for research. Front Psychol (2011) 2:270. doi: 10.3389/fpsyg.2011.00270
56. Naegelin Y, Dingsdale H, Säuberli K, Schädelin S, Kappos L, Barde Y. Measuring and Validating the Levels of Brain-Derived Neurotrophic Factor in Human Serum. eneuro (2018) 5(2):1–9. doi: 10.1523/ENEURO.0419-17.2018
57. Seligman M. The effectiveness of psychotherapy: The Consumer Reports study. Am Psychol (1995) 50(12):965–74. doi: 10.1037/0003-066X.50.12.965
58. Dinoff A, Herrmann N, Swardfager W, Liu C, Sherman C, Chan S, et al. The Effect of Exercise Training on Resting Concentrations of Peripheral Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis. PLoS One (2016) 11(9):e0163037. doi: 10.1371/journal.pone.0163037
59. Yang B, Ren Q, Zhang J, Chen Q-X, Hashimoto K. Altered expression of BDNF, BDNF pro-peptide and their precursor proBDNF in brain and liver tissues from psychiatric disorders: rethinking the brain–liver axis. Trans Psychiatry (2017) 7(5):e1128. doi: 10.1038/tp.2017.95
60. Hashimoto K. Brain-derived neurotrophic factor (BDNF) and its precursor proBDNF as diagnostic biomarkers for major depressive disorder and bipolar disorder. Eur Arch Psychiatry Clin Neurosci (2014) 265(1):83–4. doi: 10.1007/s00406-014-0557-x
61. Södersten K, Pålsson E, Ishima T, Funa K, Landén M, Kenji H, et al. Abnormality in serum levels of mature brain-derived neurotrophic factor (BDNF) and its precursor proBDNF in mood-stabilized patients with bipolar disorder: A study of two independent cohorts. J Affect Disord (2014) 160:1–9. doi: 10.1016/j.jad.2014.01.009
62. Lommatzsch M, Zingler D, Schuhbaeck K, Schloetcke K, Zingler C, Schuff-Werner P, et al. The impact of age, weight and gender on BDNF levels in human platelets and plasma. Neurobiol Aging (2005) 26(1):115–23. doi: 10.1016/j.neurobiolaging.2004.03.002
Keywords: psychotherapy, brain derived neurotrophic factor, BDNF, mental disorders, systematic review
Citation: Claudino FCA, Gonçalves L, Schuch FB, Martins HRS and Rocha NS (2020) The Effects of Individual Psychotherapy in BDNF Levels of Patients With Mental Disorders: A Systematic Review. Front. Psychiatry 11:445. doi: 10.3389/fpsyt.2020.00445
Received: 29 March 2020; Accepted: 01 May 2020;
Published: 19 May 2020.
Edited by:
Takeshi Terao, Oita University, JapanReviewed by:
Kenji Hashimoto, Chiba University, JapanReiji Yoshimura, University of Occupational and Environmental Health Japan, Japan
Copyright © 2020 Claudino, Gonçalves, Schuch, Martins and Rocha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felipe Cesar de Almeida Claudino, ZmVsaXBlYWNsYXVkaW5vQGdtYWlsLmNvbQ==