
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 14 January 2020
Sec. Aging Psychiatry
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00953
This article is part of the Research Topic Understanding Brain Aging View all 30 articles
 Stefan Frenzel1*
Stefan Frenzel1* Katharina Wittfeld1,2
Katharina Wittfeld1,2 Mohamad Habes3
Mohamad Habes3 Johanna Klinger-König1Robin Bülow4Henry Völzke5and
Johanna Klinger-König1Robin Bülow4Henry Völzke5and  Hans Jörgen Grabe1,2 for the Alzheimer’s Disease Neuroimaging Initiative†1Department of Psychiatry and Psychotherapy University Medicine Greifswald GreifswaldGermany2German Center for Neurodegenerative Diseases (DZNE) GreifswaldGermany3Center for Biomedical Image Computing and Analytics University of Pennsylvania Philadelphia PAUnited States4Institute of Diagnostic Radiology and Neuroradiology University Medicine Greifswald GreifswaldGermany5Institute for Community Medicine University Medicine Greifswald Greifswald Germany
Hans Jörgen Grabe1,2 for the Alzheimer’s Disease Neuroimaging Initiative†1Department of Psychiatry and Psychotherapy University Medicine Greifswald GreifswaldGermany2German Center for Neurodegenerative Diseases (DZNE) GreifswaldGermany3Center for Biomedical Image Computing and Analytics University of Pennsylvania Philadelphia PAUnited States4Institute of Diagnostic Radiology and Neuroradiology University Medicine Greifswald GreifswaldGermany5Institute for Community Medicine University Medicine Greifswald Greifswald GermanyIntroduction: It has been shown that Alzheimer’s disease (AD) is accompanied by marked structural brain changes that can be detected several years before clinical diagnosis via structural magnetic resonance (MR) imaging. In this study, we developed a structural MR-based biomarker for in vivo detection of AD using a supervised machine learning approach. Based on an individual’s pattern of brain atrophy a continuous AD score is assigned which measures the similarity with brain atrophy patterns seen in clinical cases of AD.
Methods: The underlying statistical model was trained with MR scans of patients and healthy controls from the Alzheimer’s Disease Neuroimaging Initiative (ADNI-1 screening). Validation was performed within ADNI-1 and in an independent patient sample from the Open Access Series of Imaging Studies (OASIS-1). In addition, our analyses included data from a large general population sample of the Study of Health in Pomerania (SHIP-Trend).
Results: Based on the proposed AD score we were able to differentiate patients from healthy controls in ADNI-1 and OASIS-1 with an accuracy of 89% (AUC = 95%) and 87% (AUC = 93%), respectively. Moreover, we found the AD score to be significantly associated with cognitive functioning as assessed by the Mini-Mental State Examination in the OASIS-1 sample after correcting for diagnosis, age, sex, age·sex, and total intracranial volume (Cohen’s f2 = 0.13). Additional analyses showed that the prediction accuracy of AD status based on both the AD score and the MMSE score is significantly higher than when using just one of them. In SHIP-Trend we found the AD score to be weakly but significantly associated with a test of verbal memory consisting of an immediate and a delayed word list recall (again after correcting for age, sex, age·sex, and total intracranial volume, Cohen’s f2 = 0.009). This association was mainly driven by the immediate recall performance.
Discussion: In summary, our proposed biomarker well differentiated between patients and healthy controls in an independent test sample. It was associated with measures of cognitive functioning both in a patient sample and a general population sample. Our approach might be useful for defining robust MR-based biomarkers for other neurodegenerative diseases, too.
Alzheimer’s disease (AD) is a neurodegenerative disorder and accounts for an estimated 60 to 80 percent of cases of dementia (1, 2). Dementia is characterized by memory impairments, disordered cognition, language problems, and changes in behaviour, which seriously impair a person’s ability to live independently. In advanced AD the person loses basic body functions like walking and swallowing and requires around the clock-care. According the World Health Organization (WHO) the incidence of dementia worldwide will reach about 135 million people in 2050 and will become a major challenge for health-care systems of western countries (3).
The hallmark pathology of AD is the progressive accumulation of amyloid beta protein and tau protein in the brain which is accompanied by death of neurons (1, 4). Macroscopically this is reflected in atrophy of specific brain regions which can be assessed via structural magnetic resonance (MR) imaging. At an early stage, the mild cognitive impairment phase, there typically is an atrophy only of the temporal lobe. With progression of the disease other cortical and subcortical regions, notably the hippocampus, become affected too (5–7). These structural changes have been shown to be detectable several years before the clinical diagnosis of AD (8, 9) which led to the development of imaging-based biomarkers of AD based on machine learning (10–16). Biomarkers based on structural MR imaging have been shown to differentiate well between cases of AD and cognitively healthy controls (17) and some of them have been shown to be sensitive at the preclinical stage (18). However, most of these biomarkers have been investigated in single cohorts only.
Since structural brain changes are detectable several years before clinical diagnosis MR-based biomarkers for AD are highly relevant for general population studies, too. However, the investigation of such biomarkers has gained attention only recently within the context of general brain ageing (19–21). In this study, we developed an MR-based biomarker for the in vivo assessment of AD based on a supervised machine learning approach. Based on an individual’s pattern of brain atrophy a continuous score is assigned which measures the similarity with brain atrophy patterns seen in clinical cases of AD. The underlying statistical model is trained using data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (22) and validation is performed in an independent patient sample from the Open Access Series of Imaging Studies (OASIS) (23). Finally, our proposed biomarker is investigated in general population data from the Study of Health in Pomerania (SHIP-Trend) (24).
Data used in the preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The primary goal of ADNI has been to test whether serial magnetic resonance (MR) imaging, positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of mild cognitive impairment (MCI) and early Alzheimer’s disease (AD). For up-to-date information, see www.adni-info.org. T1-weighted structural MR scans from 413 participants of the ADNI-1 screening sample were considered in this study. Images were acquired using multiple scanners with a field strength of 1.5T (25, 26). The detailed MR protocol can be found in the supplement. Since the ADNI scans were used to train the AD classifier additional quality control of the image processing was performed as explained below. The final sample comprised N = 374 individuals with 165 diagnosed with AD and 209 cognitively healthy controls (CN) (see Table 1).
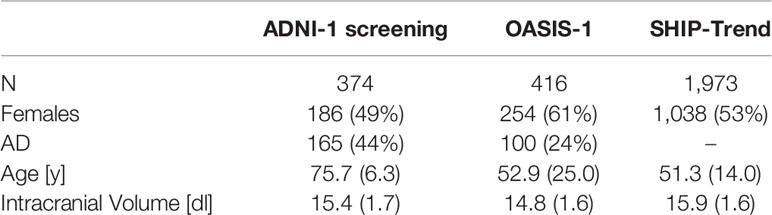
Table 1 Basic demographic characteristics of all three samples.
To validate the AD classifier we used data from the Open Access Series of Imaging Studies (OASIS-1) which is a cross-sectional collection of MR scans of N = 416 individuals aged 18 to 96 (23) (see Table 1). One hundred of the participants older than 60 have been clinically diagnosed with very mild to moderate AD. More information can be found at www.oasis-brains.org. Details of the MR protocol can be found in the supplement. All images were screened for artefacts, acquisition problems, and processing errors and images with severe flaws were excluded by the OASIS investigators. No additional quality control was performed by the authors. 235 participants (100 AD, 135 CN) completed the Mini-Mental State Examination (MMSE). The MMSE is a 30-point questionnaire that is used extensively to screen for dementia (27).
The Study of Health in Pomerania (SHIP) was designed to assess the prevalence of common risk factors and diseases in a population of northeast Germany randomly drawn from local registers (24). 4,308 subjects participated at baseline between 1997 and 2001. In parallel to the original SHIP study a new independent sample was drawn and examinations of similar extent were undertaken (SHIP-Trend). In this study, T1-weighted structural MR images of the head from 2,154 participants of SHIP-Trend were considered (28). Details of the MR protocol can be found in the supplement. Scans with very poor technical quality, (e.g. frontal darkening) were excluded (N = 84). In addition, scans showing structural abnormalities (e.g. tumors, cysts) and cases of cerebral stroke were excluded as well (N = 93). The image processing pipeline (see below) failed to process 4 scans. The final sample comprised N = 1973 individuals (see Table 1).
Of those, 1,955 participants completed a word list recall (WLR) test during the face-to-face interview as part of the standard SHIP-Trend protocol. The WLR test consists of eight items which needed to be recalled immediately (immediate WLR, 0 to 8 points) and after a 20 min delay (delayed WLR with distractor words, -8 to 8 points). The total WLR score was computed as sum of both tests. The WLR is part of the Nuremberg Gerontopsychological Inventory (29).
Cortical reconstruction and volumetric segmentation of all three data sets were performed with the FreeSurfer image analysis suite version 5.3 (“recon-all”), which is documented and freely available for download online (http://surfer.nmr.mgh.harvard.edu).
Briefly, this processing includes removal of non-brain tissue using a hybrid watershed/surface deformation procedure (30), automated Talairach transformation, segmentation of subcortical white matter and deep gray matter volumetric structures (including hippocampus, amygdala, caudate, putamen, ventricles) (31–33), intensity normalization (34), tessellation of the gray matter white matter boundary, automated topology correction (35, 36), and surface deformation following intensity gradients to optimally place the gray/white and gray/cerebrospinal fluid borders at the location where the greatest shift in intensity defines the transition to the other tissue class (37–39).
Once the cortical models are complete, individual images are being registered to a spherical atlas which is based on individual cortical folding patterns to match cortical geometry across subjects (40), and the cerebral cortex is being parcelled into 68 units with respect to gyral and sulcal structure (41, 42). Cortical white matter, i.e. white matter up to 5mm below the gray matter boundary, is also being parcelled into 68 units by assigning each white matter voxel the label of the closest cortical voxel (43). FreeSurfer also gives an estimate of the total intracranial volume (eTIV) which was not used to train the AD classifier but as a covariate in subsequent statistical analyses.
Although being part of the standard FreeSurfer output several brain regions were excluded from the analyses. The 5th ventricle was excluded because it was not detected in all scan (zero volume). In addition, the brain stem and optic chiasm were excluded as well. In total, 169 out of 172 brain regions of gray matter, white matter, and the ventricular system were considered (see Figure 1). The complete list of regions can be found in the Supplementary Material.
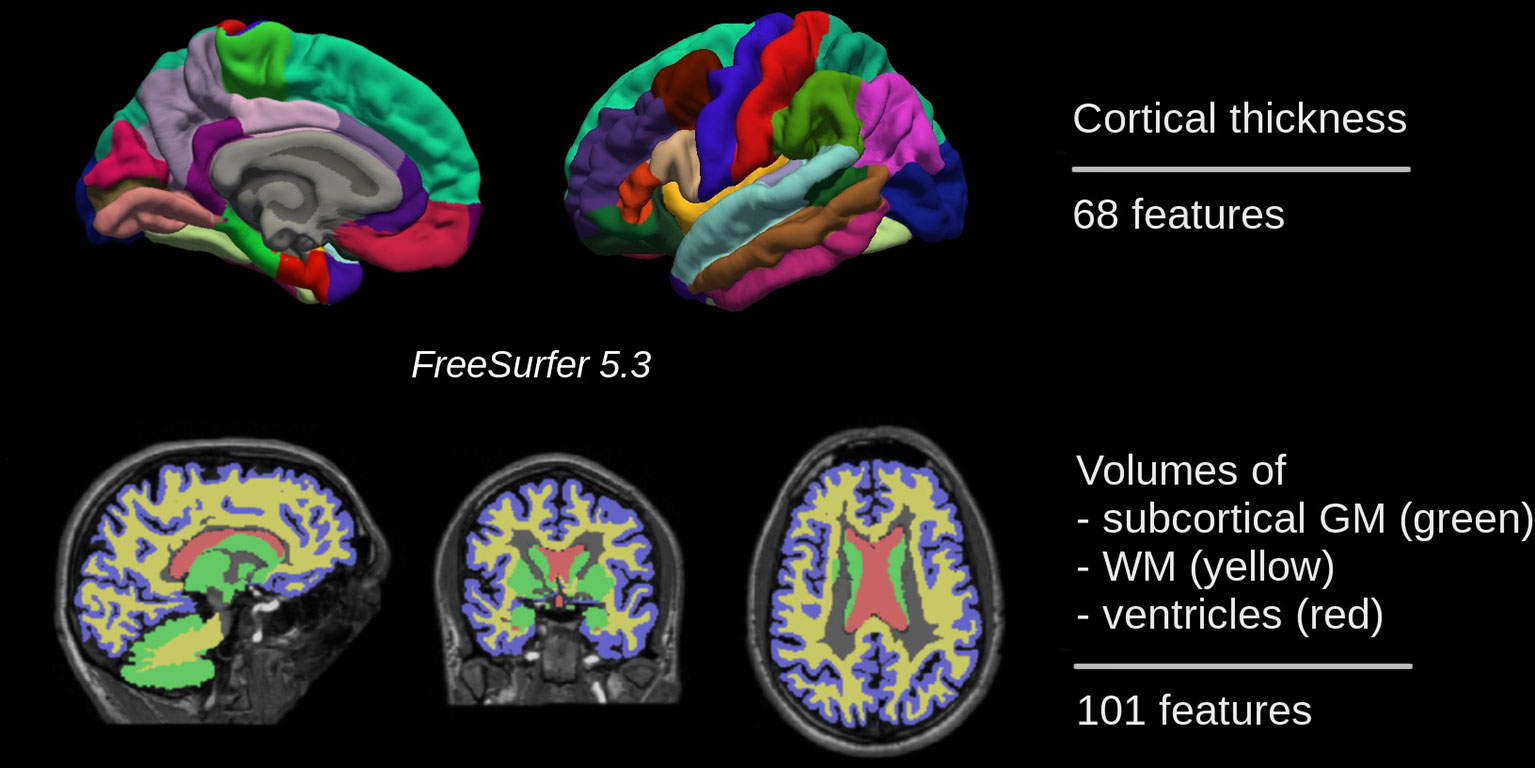
Figure 1 In total, 169 features of gray matter, white matter, and the ventricular system were used for training a binary classifier which distinguishes between individuals with Alzheimer’s disease and cognitively normal ones.
Based on the ADNI-1 screening sample a binary classifier was trained with diagnoses as dependent variable. In order to minimize the influence of image segmentation errors on the classifier, we performed an additional statistical quality control of each feature. More specifically, we removed all scans with brain measurements deviating more than four standard deviations from the mean value after adjusting for age, sex, age·sex, eTIV, and diagnosis (N = 39). All features were standardized to zero mean and unit variance. We then used L2-penalized (ridge) logistic regression to train the binary classifier which optimally separates individuals with AD from CN (44). The AD score was defined as the linear predictors of the logistic model, i.e. it is given by log[p/(1-p)] with p denoting the probability of having AD.
Prediction of AD scores in OASIS-1 and SHIP-Trend were based on a classifier trained on the whole ADNI-1 sample. The corresponding model coefficients can be found in the supplement. The penalization parameter λ was selected from the set {2-8, 2-7, …, 2} by 20-fold cross-validation with 20 repetitions (λ = 0.125) anduni-modality of the tuning curve was checked by visual inspection (see Supplementary Material). In order to assess the classification accuracy within ADNI-1 we used leave-one-out cross-validation, i.e. each individual’s AD score was calculated using a model trained on all others. The optimal λ was estimated within a second loop in order to strictly separate training and test data (again by 20-fold cross-validation with 20 repetitions).
For SHIP-Trend we additionally performed voxel-based morphometry (VBM) analyses with SPM12 (Welcome Trust Centre for Neuroimaging, University College London) and CAT12 [developed by Christian Gaser, University of Jena, Germany, http://www.neuro.uni-jena.de, e.g. (45)] in order to map the contribution of distinct brain regions to the AD score.
All images were bias-corrected, spatially normalized by using the high-dimensional DARTEL normalization, segmented into the different tissue classes, modulated for non-linear warping and affine transformations, and smoothed by a Gaussian kernel of 8 mm FWHM. The homogeneity of gray matter images was checked using the covariance structure of each image with all other images (outliers ≥3 standard deviations from the mean), as implemented in the check data quality function in the CAT12 toolbox. To mask irrelevant brain areas of the smoothed gray and white matter segmentations we used the Masking Toolbox from Gerard Ridgway to define explicit masks for the gray and white matter VBM analyses. Specifically, we used the MATLAB script “make_majority_mask.m” to generate a gray matter mask with an absolute threshold of 0.1 and a consensus fraction of 80% and a white matter mask with an absolute threshold of 0.2 and a consensus fraction of 90%.
The statistical threshold for significant voxels was set to a family-wise error (FWE) corrected peak-level p-values Ppeak,FWE < 0.025 as we conducted a two-sided test and looked at positive and negative associations with the FSAD score while correcting for age, sex, age·sex, and total intracranial volume. Again, age was modeled by restricted cubic splines with four knots located at the 0.05, 0.33, 0.66, and 0.95 age quantiles.
All statistical analyses were performed with R 3.6 (46). The classifier was implemented using the glmnet package (47). Association analyses of the AD score with the basic covariates age, sex, age·sex, eTIV, and diagnosis were performed by ordinary least-squares multivariable regression. For SHIP-Trend we used restricted cubic splines (48) with four knots located at the 0.05, 0.33, 0.66, and 0.95 quantile in order to account for the non-linear dependency of the AD score on chronological age. Effects of single variables were assessed either by t-tests with robust variance estimates or ANOVA of type 2.
Prior to training the AD classifier we checked the ADNI-1 screening sample for possible imbalances with respect to age, sex, and intracranial volume. We did not find significant differences between patients and controls with respect to age (t = -0.55, P = 0.58), sex (Fisher’s Exact Test, P = 0.84), and estimated intracranial volume (t = 0.15, P = 0.88).
At first, classification performance within the ADNI-1 screening sample was investigated. Classification accuracy was assessed by leave-one-out cross-validation, i.e. each individual’s AD score was calculated using a model trained on all others. The resulting scores are shown in Figure 2A. Individuals with an AD score larger than zero and smaller than zero were classified as AD and CN, respectively, and these classifications were compared with the known diagnoses. The overall accuracy was 89% with the 95% confidence interval (CI) (85.7%, 92.2%). Sensitivity (true positive rate) and specificity (true negative rate) was 91% and 87%, respectively. The receiver operating characteristic (ROC) curves were obtained by systematic variation of the classification threshold and area under the curve (AUC) was calculated as 95% with 95% CI (93.5%, 97.6%).
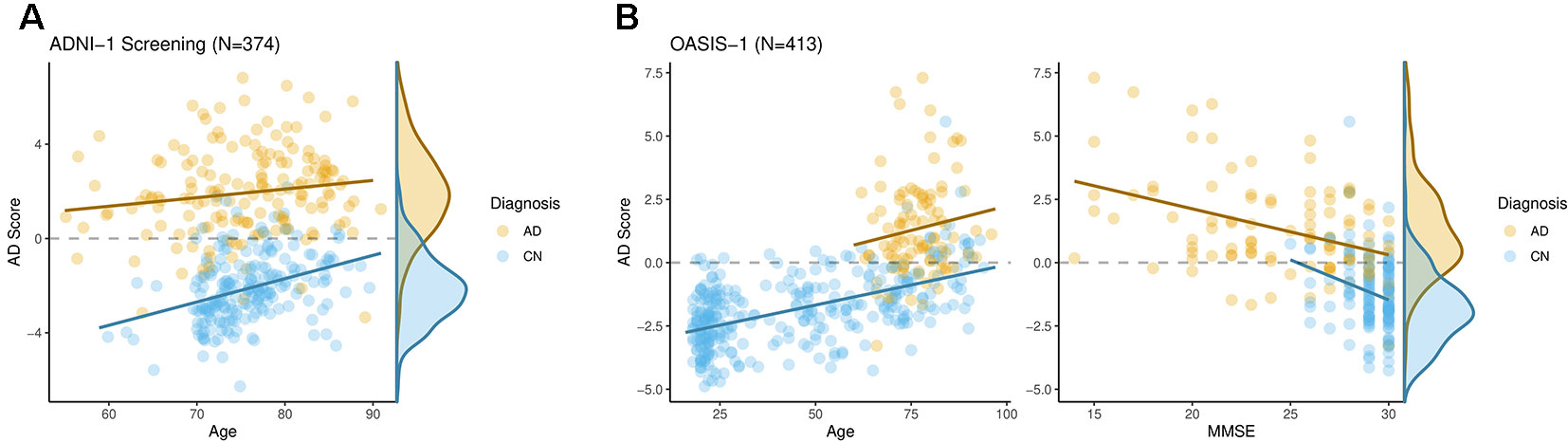
Figure 2 The AD score differentiated well individuals with Alzheimer’s disease from cognitively normal ones both in ADNI-1 (A) and OASIS-1 (B). Moreover, it was significantly associated with cognitive functioning as assessed by the Mini-Mental State Examination within both groups in OASIS-1.
Using the ADNI-1 sample a model was trained and AD scores were calculated for the OASIS-1 sample. The resulting scores are shown in Figure 2B, left panel. Again, individuals with an AD score larger than zero and smaller than zero were classified as AD and CN, respectively. The overall accuracy was 87% with 95% CI (83.2%, 90.0%). Sensitivity and specificity were 89% and 79%, respectively. The AUC was calculated as 93% with 95% CI (90.0%, 95.7%).
We performed association analyses of the AD score with the basic covariates diagnosis, age, sex, age·sex, and intracranial volume by means of multivariable regression. For the ADNI-1 sample the percentage of variation explained (R2) was 72%. As expected, the AD score was significantly larger in those diagnosed with AD (t = 30, P < 2·10-16, see Figure 2A). In addition, there was a significant effect of age (t = 2.5, P = 0.012). No significant effects of sex (t = 1.1, P = 0.29), age·sex (t = -0.89, P = 0.37), or intracranial volume (t = 1.4, P = 0.17) were found.
For the OASIS-1 sample the multivariable regression of the AD score yielded R2 = 55%. Again, we found a significant effect of diagnosis of AD (t = 9.7, P < 2·10-16), and age (t = 8.5, P = 4.9·10-16). In addition, there was a significant effect of sex with females having slightly larger AD scores (t = 2.2, P = 0.025). No significant effects of age·sex (t = -0.75, P = 0.45), or intracranial volume (t = 0.55, P = 0.57) were found.
When analyzing the OASIS-1 subsample with MMSE scores available (N = 235, 100 AD, 135 CN) we again found significant effects of diagnosis (t = 9.3, P < 2.2·10-16), and age (t = 5.7, P = 3.9·10-8). No significant effects were found for sex (t = 0.97, P = 0.33), age·sex (t = -0.61, P = 0.54), and intracranial volume (t = 0.80, P = 0.42). The total R2 was 45%. Adding the MMSE score to the model increased the R2 to 51% and the corresponding marginal effect was significant (t = -4.1, P = 4.9·10-5, Cohen’s f2 = 0.13), i.e. on average individuals with low MMSE scores had larger AD scores when correcting for all basic covariates including diagnosis.
In order to compare the diagnostic utility of the AD score with the MMSE we aimed to predict diagnoses in the OASIS-1 subsample with MMSE scores available. For this we used standard logistic regression models with different sets of predictors and compared the corresponding classification accuracies. Note that we did not separate the training and test set since we aimed to compare different sets of predictors rather than obtaining objective accuracy estimates. Using a basic model containing age, sex, and its interaction, we were able to predict AD diagnoses with an accuracy of 61% (AUC = 70%). Adding either the MMSE score or the AD score improved the accuracy to 82% (AUC = 91%) and 82% (AUC = 90%), respectively. When adding both the MMSE score and the AD score the resulting accuracy improved even further to 87% (AUC = 94%). The accuracy of the combined model was significantly better than one of the two previous ones (χ12 = 29, P = 8·10-8; χ12 = 53, P = 3·10-13).
AD scores were calculated for the SHIP-Trend sample (N = 1973, see Table 1) using a model trained on the whole ADNI-1 screening sample. Again, we performed association analyses of the AD score with the basic covariates age, sex, age·sex, and intracranial volume by means of multivariable regression. Since the AD score was clearly non-linearly related to age (see Figure 3A) we decided to include age by restricted cubic splines. ANOVA of type 2 was used to assess the effects of each variable. We found significant associations with age (F = 170, P < 2·10-16) and age·sex (F = 3.7, P = 0.010). No significant effects of sex (F = 0.40, P = 0.53), or intracranial volume (t = 2.5, P = 0.11) were found. The R2 was 22%.
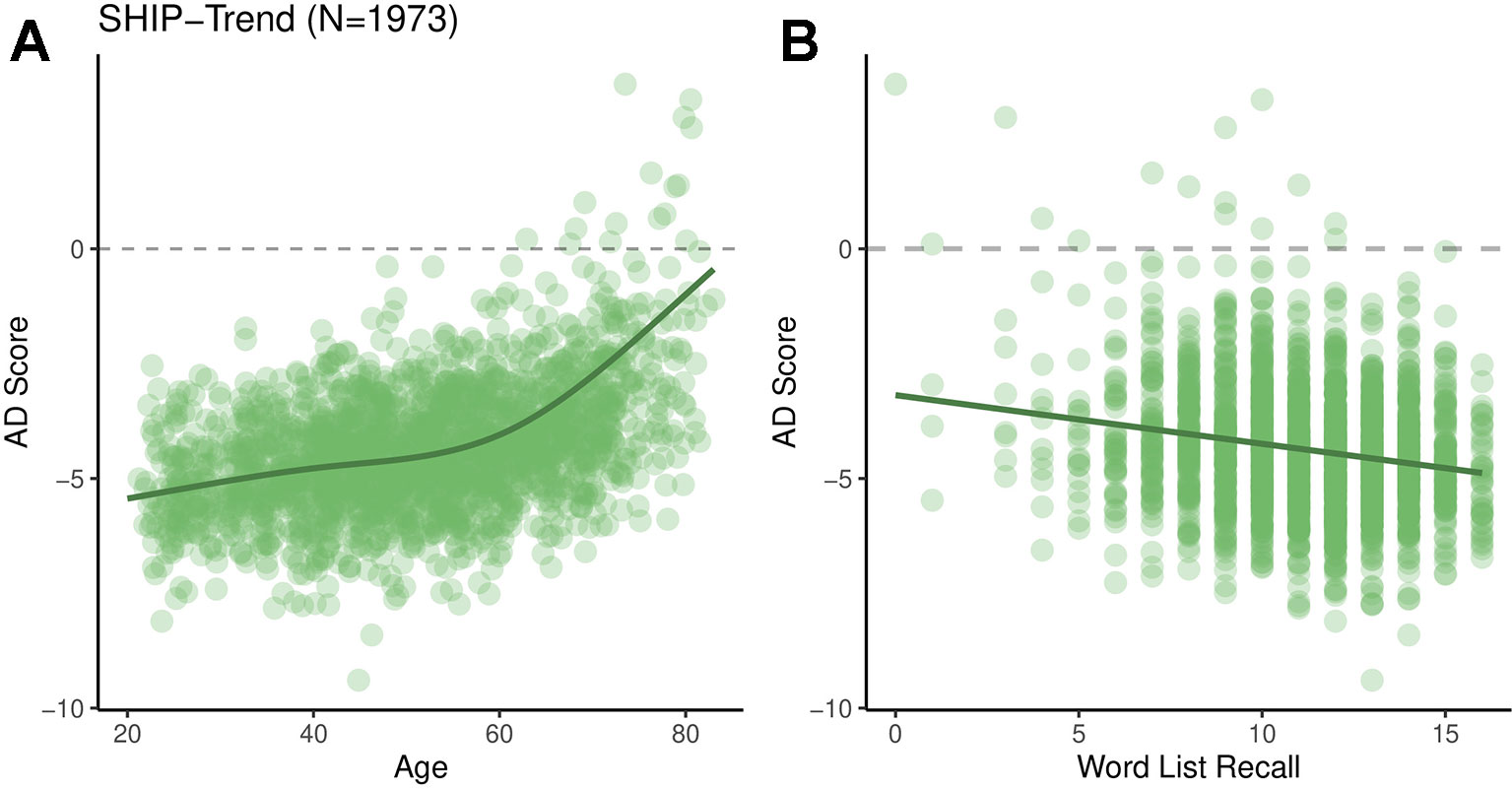
Figure 3 AD scores for the SHIP-Trend sample plotted against chronological age (A) and the overall word list recall score (B).
The AD score was significantly associated with the total WLR score (F = 4.1, P = 0.037, Cohen’s f2 = 0.009, adjusted for all basic covariates, see Figure 3B). Additional analyses showed that the AD score was more strongly associated with the immediate WLR score (F = 4.9, P = 0.026) than the delayed WLR recall (F = 1.8, P = 0.17).
In order to map the contributions of distinct brain regions to the AD score in greater detail we performed VBM analyses with both gray and white matter segmentations in SHIP-Trend. The results are visualized in Figure 4. Using the gray matter segmentation we found a large cluster that was negatively associated with the AD score. The peak voxel was located in the left medial temporal gyrus. The cluster stretched over the medial temporal gyrus, the inferior temporal gyrus, the fusiform gyrus, and the precuneus in both hemispheres, among others. Using the white matter segmentation we also found a large cluster that was negatively associated with the AD score. It comprised the medial temporal lobe, the periventricular area, and the corpus callosum, among others. Interestingly, it also includes a large portion of the brain stem which was not included in the feature set used for constructing the AD score.
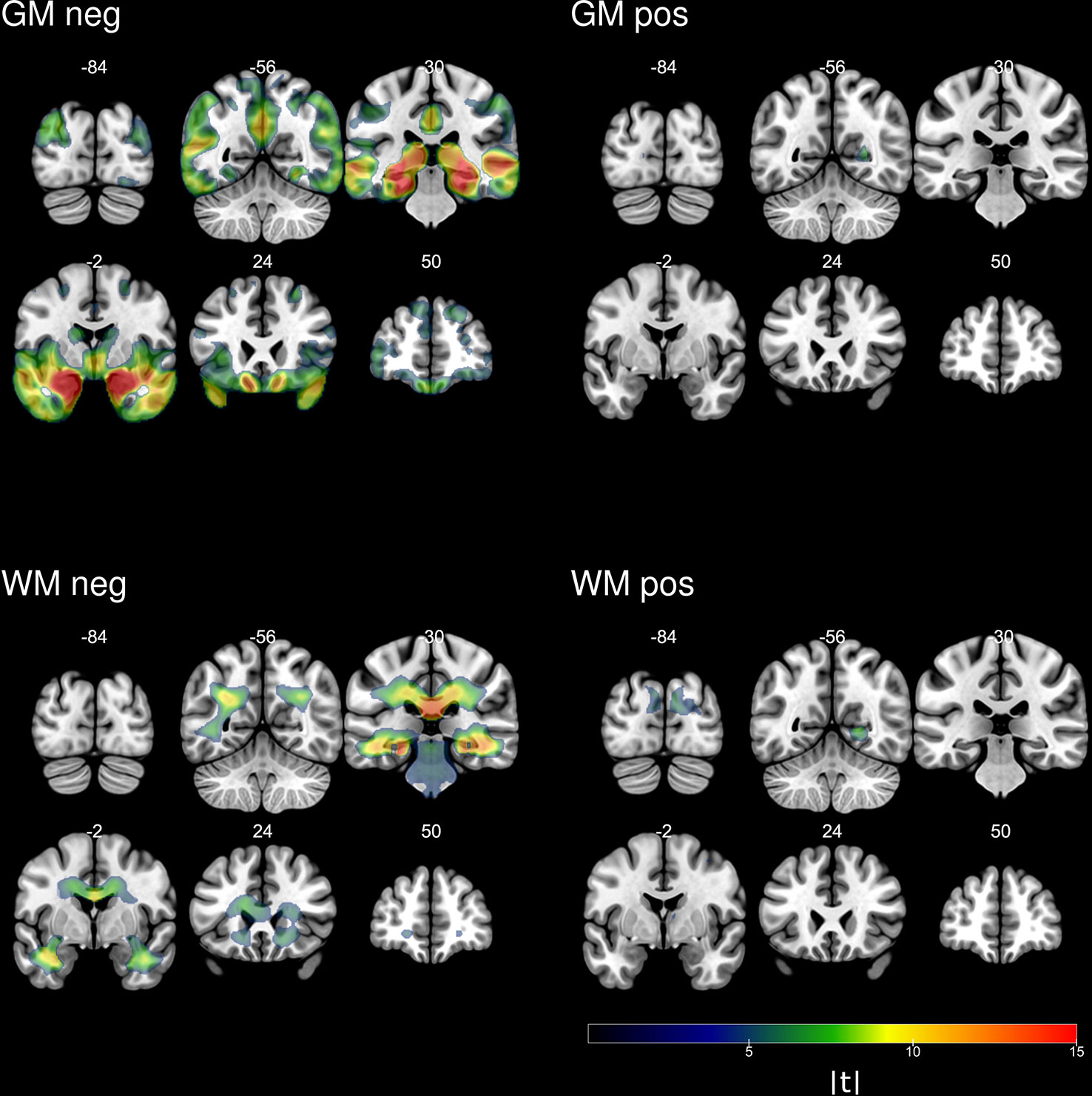
Figure 4 Absolute values of the t-statistics of voxel-based analyses of the AD score in SHIP-Trend.
In this study, we developed a structural MR imaging-based biomarker for the in vivo detection of Alzheimer’s disease. It was based on 169 regional brain features of gray matter, white matter, and the ventricular system derived from the image processing pipeline FreeSurfer. L2-penalized logistic regression was used to define a binary classifier which optimally separates individuals with AD from cognitively normal ones. For the ADNI-1 screening sample the cross-validated classification accuracy was 89% and AUC was 95%. These results are on par with other classification studies involving structural MR images (17). However, most classification studies were based on only one sample. Here, the classifier was trained using the ADNI-1 screening sample and AD scores were predicted in the independent sample OASIS-1. We found our classifier to also perform well with an accuracy of 87% and AUC being 93%.
For obtaining regional brain features we used the freely available image segmentation pipeline FreeSurfer. FreeSurfer has been shown to give reliable volumetric estimates independent of scanner platforms and protocols with the exception of the magnetic field strength which has been found to introduce additional bias (49). In our study, however, all scans were acquired with 1.5T. Since FreeSurfer is available under an open source license for the GNU/Linux operating system it can be run within typical high performance computing environments with little to no additional adaptations. This facilitates the application to large imaging data sets which are being used increasingly for the investigation of neurodegenerative disorders. Moreover, future improvements of the image processing algorithms used within FreeSurfer will likely improve any derived biomarkers, too.
On the other hand there is strong evidence for at least three distinct subtypes of AD with respect to regional brain atrophy (50, 51). Hence, it is unclear whether further improvements of the classification accuracy of structural MRI markers with respect a single diagnostic category (AD diagnosis) can be expected. Instead, the relation of MRI markers measures and measures of cognitive functioning, which ultimately impairs the affected individual’s quality of life, seems to be more appropriate. Here, we studied the association of the AD score with MMSE scores in a subsample of OASIS-1. We found a significant association after correcting for diagnosis, age, sex, age·sex, and total intracranial volume (Cohen’s f2 = 0.13, see Figure 2B). The AD score was associated with cognitive functioning in AD patients (adjusted for age, sex, and intracranial volume) which indicates it to be a measure of the progression of AD. Interestingly, it was also associated with the MMSE in cognitive normal individuals after correcting for age, sex, and intracranial volume, indicating that it captures subclinical pathology (atrophy), too.
This was supported by the association analyses in the general population sample SHIP-Trend where we found the AD score to be significantly associated with the WLR consisting of an immediate and a delayed recall (again after correcting for age, sex, age·sex, and total intracranial volume, Cohen’s f2 = 0.009). This association was mainly driven by the immediate recall. Indeed, there seems to be a deficit in semantic memory years before AD diagnosis while AD patients show impairments in multiple cognitive domains (52). Such a deficit in semantic memory could explain the association with the WLR performance in SHIP-Trend.
However, the association between the AD score and cognitive functioning in non-demented individuals could also be partially driven by other psychiatric diseases. One example for this is depression which is known to be associated with decreased hippocampal volume and impaired memory. Since depression has a much higher life-time prevalence than AD it is potentially highly relevant for population-based studies. Whether the AD score proposed here is indeed associated with a specific profile of cognitive dysfunction in non-demented individuals needs to be investigated in future studies.
One limitation of our method is that AD scores of single individuals can only be interpreted within populations after adjusting for confounding variables like age. In all data sets the AD score was positively associated with age. In SHIP-Trend this association was non-linear with the slope increasing around the age of 60 (see Figure 3A). However, this should not be interpreted as progression of some sort of AD-related subclinical pathology, but rather statistical artefact of the spatial overlap of general age-related atrophy and AD-related atrophy. Even if the model coefficients of the AD classifier were randomly drawn there would still be a significant association of the resulting AD score with chronological age. Since age is a potential confounding variable thorough adjustment of the analyses is needed. Most of the time this requires non-linear modelling with polynomials or splines.
In summary, our proposed AD score well differentiated between patients and healthy controls in an independent test sample. It was associated with measures of cognitive functioning both in a patient sample and a general population sample. Thus, our approach might be useful for defining robust MR-based biomarkers for other neurodegenerative diseases, too.
Data used in the preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu) and the Open Access Series of Imaging Studies. Request should be made to the corresponding author: c3RlZmFuLmZyZW56ZWxAdW5pLWdyZWlmc3dhbGQuZGU=.
The studies involving human participants were reviewed and approved by Institutional Review Board of University Medicine Greifswald (“Ethikkomission an der Universitätsmedizin Greifswald”). The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SF performed all statistical analysis, and wrote the manuscript. SF, JK-K, MH, and HG designed the study. SF, MH, and KW processed the MR imaging data. KW conducted the VBM analyses. RB and HV contributed essentially to the data collection.
HG has received travel grants and speakers honoraria from Fresenius Medical Care and Janssen Cilag. He has received research funding from the German Research Foundation (DFG), the German Ministry of Education and Research (BMBF), the DAMP Foundation, Fresenius Medical Care, the EU “Joint Programme Neurodegenerative Disorders (JPND)”.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer XH declared a shared affiliation, with no collaboration, with one of the authors MH to the handling editor.
Data collection and sharing for this project was in part funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.;Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
For this study, we also used data from the Open Access Series of Imaging Studies (OASIS) Cross-Sectional: Principal Investigators: D. Marcus, R, Buckner, J, Csernanskny J. Morris; P50 AG05681, P01 AG03991, P01 AG026276, R01 AG021910, P20 MH071616, U24 RR021382.
The Study of Health in Pomerania (SHIP) is part of the Community Medicine Research net (CMR) (http://www.medizin.uni-greifswald.de/icm) of the University Medicine Greifswald, which is supported by the German Federal State of Mecklenburg- West Pomerania. MRI scans in SHIP-Trend have been supported by a joint grant from Siemens Healthineers, Erlangen, Germany, and the Federal State of Mecklenburg-West Pomerania.
This study was further supported by the EU-JPND Funding for BRIDGET (FKZ:01ED1615).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00953/full#supplementary-material
1. Alzheimer’s Association. 2016 Alzheimer’s disease facts and figures. Alzheimers Dement (2016) 12:459–509. doi: 10.1016/j.jalz.2016.03.001
2. Barker WW, Luis CA, Kashuba A, Luis M, Harwood DG, Loewenstein D, et al. Relative frequencies of alzheimer disease, lewy body, vascular and frontotemporal dementia, and hippocampal sclerosis in the State of Florida brain bank. Alzheimer Dis Assoc Disord (2002) 16:203. doi: 10.1097/00002093-200210000-00001
3. Prince MJ, Guerchet MM, Prina M. The Epidemiology and Impact of Dementia: Current State and Future Trends. Geneva, Switzerland: WHO Thematic Briefing (2015).
4. Hardy JA, Higgins GA. Alzheimer’s disease: the amyloid cascade hypothesis. Science (1992) 256(5054):184–5. doi: 10.1126/science.1566067
5. Frisoni GB, Fox NC, Jack CR Jr., Scheltens P, Thompson PM. The clinical use of structural MRI in Alzheimer disease. Nat Rev Neurol (2010) 6:67–77. doi: 10.1038/nrneurol.2009.215
6. Thompson PM, Hayashi KM, Zubicaray G, de, Janke AL, Rose SE, Semple J, et al. Dynamics of gray matter loss in Alzheimer’s Disease. J Neurosci (2003) 23:994–1005. doi: 10.1523/JNEUROSCI.23-03-00994.2003
7. Tondelli M, Wilcock GK, Nichelli P, De Jager CA, Jenkinson M, Zamboni G. Structural MRI changes detectable up to ten years before clinical Alzheimer’s disease. Neurobiol Aging (2012) 33, 825:e25–825.e36.
8. Jack CR, Shiung MM, Weigand SD, O’Brien PC, Gunter JL, Boeve BF, et al. Brain atrophy rates predict subsequent clinical conversion in normal elderly and amnestic MCI. Neurology (2005) 65:1227–31.
9. Twamley EW, Ropacki SAL, Bondi MW. Neuropsychological and neuroimaging changes in preclinical Alzheimer’s disease. J Int Neuropsychol Soc (2006) 12:707–35. doi: 10.1017/S1355617706060863
10. Beheshti I, Demirel H. Feature-ranking-based Alzheimer’s disease classification from structural MRI. Magnet Resonance Imaging (2016) 34:252–63. doi: 10.1016/j.mri.2015.11.009
11. Davatzikos C, Xu F, An Y, Fan Y, Resnick SM. Longitudinal progression of Alzheimer’s-like patterns of atrophy in normal older adults: the SPARE-AD index. Brain (2009) 132:2026–35.
12. Duchesne S, Caroli A, Geroldi C, Barillot C, Frisoni GB, Collins DL. MRI-based automated computer classification of probable AD versus normal controls. IEEE Trans Med Imaging (2008) 27:509–20.
13. Fan Y, Resnick SM, Wu X, Davatzikos C. Structural and functional biomarkers of prodromal Alzheimer’s disease: a high-dimensional pattern classification study. NeuroImage (2008) 41:277–85.
14. Klöppel S, Stonnington CM, Chu C, Draganski B, Scahill RI, Rohrer JD, et al. Automatic classification of MR scans in Alzheimer’s disease. Brain (2008) 131:681–9.
15. Li H, Habes M, Wolk DA, Fan Y, Alzheimer’s Disease Neuroimaging Initiative and the Australian Imaging Biomarkers and Lifestyle Study of Aging. A deep learning model for early prediction of Alzheimer’s disease dementia based on hippocampal magnetic resonance imaging data. Alzheimers Dement (2019) 15:1059–70.
16. Salvatore C, Cerasa A, Battista P, Gilardi MC, Quattrone A, Castiglioni I. Magnetic resonance imaging biomarkers for the early diagnosis of Alzheimer’s disease: a machine learning approach. Front Neurosci (2015) 9:307.
17. Rathore S, Habes M, Iftikhar MA, Shacklett A, Davatzikos C. A review on neuroimaging-based classification studies and associated feature extraction methods for Alzheimer’s disease and its prodromal stages. NeuroImage (2017) 155:530–48.
18. Davatzikos C, Bhatt P, Shaw LM, Batmanghelich KN, Trojanowski JQ. Prediction of MCI to AD conversion, via MRI, CSF biomarkers, and pattern classification. Neurobiol Aging (2011) 32, 2322:e19–27.
19. Cole JH, Ritchie SJ, Bastin ME, Valdés Hernández MC, Muñoz Maniega S, Royle N, et al. Brain age predicts mortality. Mol Psychiatry (2018) 23:1385–92. doi: 10.1038/mp.2017.62
20. Habes M, Janowitz D, Erus G, Toledo JB, Resnick SM, Doshi J, et al. Advanced brain aging: relationship with epidemiologic and genetic risk factors, and overlap with Alzheimer disease atrophy patterns. Trans Psychiatry (2016) 6:e775. doi: 10.1038/tp.2016.39
21. Janowitz D, Habes M, Toledo JB, Hannemann A, Frenzel S, Terock J, et al. Inflammatory markers and imaging patterns of advanced brain aging in the general population. Brain Imaging Behav (2019).
22. Petersen RC, Aisen PS, Beckett LA, Donohue MC, Gamst AC, Harvey DJ, et al. Alzheimer’s Disease Neuroimaging Initiative (ADNI). Neurology (2010) 74:201–9.
23. Marcus DS, Wang TH, Parker J, Csernansky JG, Morris JC, Buckner RL. Open Access Series of Imaging Studies (OASIS): cross-sectional MRI data in young, middle aged, nondemented, and demented older adults. J Cognit Neurosci (2007) 19:1498–507.
24. Völzke H, Alte D, Schmidt CO, Radke D, Lorbeer R, Friedrich N, et al. Cohort profile: the study of health in Pomerania. Int J Epidemiol (2011) 40:294–307.
25. Jack CR, Bernstein MA, Fox NC, Thompson P, Alexander G, Harvey D, et al. The Alzheimer’s disease neuroimaging initiative (ADNI): MRI methods. J Magnet Resonance Imaging (2008) 27:685–91.
26. Wyman BT, Harvey DJ, Crawford K, Bernstein MA, Carmichael O, Cole PE, et al. Standardization of analysis sets for reporting results from ADNI MRI data. Alzheimer’s Dementia: J Alzheimer’s Assoc (2013) 9:332–7.
27. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res (1975) 12:189–98.
28. Hegenscheid K, Kühn JP, Völzke H, Biffar R, Hosten N, Puls R. Whole-body magnetic resonance imaging of healthy volunteers: pilot study results from the population-based SHIP study. Rofo (2009) 181:748–59.
29. Oswald WD, Fleischmann UM. Psychometrics in aging and dementia: advances in geropsychological assessments. Arch Gerontol Geriatr (1985) 4:299–309.
30. Ségonne F, Dale AM, Busa E, Glessner M, Salat D, Hahn HK, et al. A hybrid approach to the skull stripping problem in MRI. Neuroimage (2004) 22:1060–75.
31. Fischl B, Salat DH, Busa E, Albert M, Dieterich M, Haselgrove C, et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron (2002) 33:341–55.
32. Fischl B, Salat DH, van der Kouwe AJW, Makris N, Ségonne F, Quinn BT, et al. Sequence-independent segmentation of magnetic resonance images. Neuroimage (2004a) 23 Suppl 1:S69–84.
33. Han X, Fischl B. Atlas renormalization for improved brain MR image segmentation across scanner platforms. IEEE Trans Med Imaging (2007) 26:479–86.
34. Sled JG, Zijdenbos AP, Evans AC. A nonparametric method for automatic correction of intensity nonuniformity in MRI data. IEEE Trans Med Imaging (1998) 17:87–97.
35. Fischl B, Liu A, Dale AM. Automated manifold surgery: constructing geometrically accurate and topologically correct models of the human cerebral cortex. IEEE Trans Med Imaging (2001) 20:70–80.
36. Ségonne F, Pacheco J, Fischl B. Geometrically accurate topology-correction of cortical surfaces using nonseparating loops. IEEE Trans Med Imaging (2007) 26:518–29.
37. Dale AM, Sereno MI. Improved localizadon of cortical activity by combining EEG and MEG with MRI cortical surface reconstruction: a linear approach. J Cognit Neurosci (1993) 5:162–76.
38. Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage (1999) 9:179–94.
39. Fischl B, Dale AM. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc Natl Acad Sci USA (2000) 97:11050–5. doi: 10.1073/pnas.200033797
40. Fischl B, Sereno MI, Tootell RBH, Dale AM. High-resolution intersubject averaging and a coordinate system for the cortical surface. Hum Brain Mapp (1999) 8:272–84. doi: 10.1002/(SICI)1097-0193(1999)8:4<272::AID-HBM10>3.0.CO;2-4
41. Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage (2006) 31:968–80.
42. Fischl B, van der Kouwe A, Destrieux C, Halgren E, Ségonne F, Salat DH, et al. Automatically parcellating the human cerebral cortex. Cereb Cortex (2004b) 14:11–22.
43. Salat DH, Greve DN, Pacheco JL, Quinn BT, Helmer KG, Buckner RL, et al. Regional white matter volume differences in nondemented aging and Alzheimer’s disease. Neuroimage (2009) 44:1247–58. doi: 10.1016/j.neuroimage.2008.10.030
44. Hastie T, Tibshirani R, Friedman JH. The Elements of Statistical Learning: Data Mining, Inference, and Prediction. Berlin, Germany: Springer Science & Business Media (2001).
45. Penny WD, Friston KJ, Ashburner JT, Kiebel SJ, Nichols TE. Statistical Parametric Mapping: The Analysis of Functional Brain Images. Amsterdam, Netherlands: Elsevier (2011).
46. Team T. (2008). The R project for statistical computing. http://www.r-Project.Org.
47. Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Softw (2010) 33:1–22. doi: 10.18637/jss.v033.i01
48. Harrell F. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis. Basel, Switzerland: Springer International Publishing (2015).
49. Han X, Jovicich J, Salat D, van der Kouwe A, Quinn B, Czanner S, et al. Reliability of MRI-derived measurements of human cerebral cortical thickness: the effects of field strength, scanner upgrade and manufacturer. Neuroimage (2006) 32:180–94. doi: 10.1016/j.neuroimage.2006.02.051
50. Varol E, Sotiras A, Davatzikos C, the Alzheimer’s Disease Neuroimaging Initiative. HYDRA: revealing heterogeneity of imaging and genetic patterns through a multiple max-margin discriminative analysis framework. Neuroimage (2017) 145:346–64. doi: 10.1016/j.neuroimage.2016.02.041
51. Whitwell JL, Dickson DW, Murray ME, Weigand SD, Tosakulwong N, Senjem ML, et al. Neuroimaging correlates of pathologically defined subtypes of Alzheimer’s disease: a case-control study. Lancet Neurol (2012) 11:868–77.
Keywords: Alzheimer's disease, machine learning, dementia, magnetic resonance imaging, FreeSurfer
Citation: Frenzel S, Wittfeld K, Habes M, Klinger-König J, Bülow R, Völzke H and Grabe HJ (2020) A Biomarker for Alzheimer’s Disease Based on Patterns of Regional Brain Atrophy. Front. Psychiatry 10:953. doi: 10.3389/fpsyt.2019.00953
Received: 21 October 2019; Accepted: 03 December 2019;
Published: 14 January 2020.
Edited by:
Gabriele Sani, Sapienza University of Rome, ItalyReviewed by:
Xiaosong He, University of Pennsylvania, United StatesCopyright © 2020 Frenzel, Wittfeld, Habes, Klinger-König, Bülow, Völzke and Grabe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefan Frenzel, c3RlZmFuLmZyZW56ZWxAdW5pLWdyZWlmc3dhbGQuZGU=
†Data used in preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). As such, the investigators within the ADNI contributed to the design and implementation of ADNI and/or provided data but did not participate in analysis or writing of this report. A complete listing of ADNI investigators can be found at: http://adni.loni.usc.edu/wp-content/uploads/how_to_apply/ADNI_Acknowledgement_List.pdf
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.