 Morgane Gindt1,2*
Morgane Gindt1,2* Susanne Thümmler1,2
Susanne Thümmler1,2 Andréa Soubelet1,2
Andréa Soubelet1,2 Fabian Guenolé3Michèle Battista1Florence Askenazy1,2
Fabian Guenolé3Michèle Battista1Florence Askenazy1,2- 1Hôpitaux Pédiatriques de Nice CHU-Lenval, Nice, France
- 2Université Côte d’Azur, Nice, France
- 3Centre Hospitalier Universitaire de Caen, Caen, France
Introduction: After a traumatic event, children and adolescents may present several clinical consequences, the most common being Post-Traumatic Stress Disorder (PTSD). Most children and adolescents with PTSD have comorbid disorders, such Attention Deficit Hyperactivity Disorder, depression, attachment and anxiety disorders, sleep disturbances and behavior problems. However, epidemiological studies on the development of PTSD and other psychiatric disorders in children and adolescents as a consequence of a terrorist attack and mass murder are lacking. Long-term follow-up of exposed children and adolescents will help identify risk and protective factors of developing psychiatric and psychological conditions after exposure to traumatic events or situations. The main objective of this article is to present the methodology of “14–7” program. The aim of “14–7” program is to characterize the risk and protective psychosocial factors affecting the clinical evolution of a pediatric population sample, exposed to the terrorist attack of July 14th, 2016 in Nice.
Method and Analysis: “14–7” program is a multicentre longitudinal cohort study. Major inclusion criteria are children and adolescents exposed to the terrorist attack and aged under 18 years on July 14th, 2016. These children and adolescents will be compared to a non-exposed to the “14–7” terrorist attack group, matched on age and gender. Participants will be assessed at baseline (T1), 2 years (T2) and 5 years (T3) after the initial assessment (T1), and every 5 years until they are 25 years old. Multiple domains are assessed: 1) mental health disorders, 2) intensity of PTSD symptoms, 3) intensity of comorbid symptoms, 4) quality of the parent–child relationship, 5) intelligence quotient, 6) parental symptoms. We will also establish a biological collection of saliva samples, magnetic resonance imaging (MRI) and actigraphy data collection. Main analyses comprise analyses of variance and regression analyses of predictors of clinical evolution over time.
Ethics and Dissemination: The National Ethics Committee “NORD OUEST III” approved the “14–7” Program protocol (number 2017-A02212-51). All patients and their caregivers signed informed consent on enrolment in the “14–7” Program. Inclusions started on November 21st, 2017. Three hundred thirty-five individuals have been included (191 children and adolescents, 144 parents).
Clinical Trial Registration: www.ClinicalTrials.gov, identifier NCT03356028
Background
On 14 July 2016 in Nice, celebration day in France, a terrorist attack happened. Many children and their families were impacted physically and psychologically. At least 30,000 people were present on the Promenade des Anglais (the attack site). This is the most important terrorist attack against families and children in France.
Eighty-six people died in the attack, including 10 children, the youngest being 4 years old. At least 55 children and adolescents were bereaved because of this crime. From 14th 2016 to the beginning of the “14–7” Program (November 21st, 2017), 827 outpatients children, aged less than 18 years old, have consulted the child and adolescent psychiatry service as results of clinical consequences of this attack (1).
After being exposed to a traumatic event, children and adolescents may suffer from several clinical conditions (2). Among them, the most common is post-traumatic stress disorder (PTSD) (2). PTSD includes four main clinical symptoms: flashbacks of the event, avoidance behaviors, alteration of cognition and mood, and neurovegetative overactivation (3). Moreover, children and adolescents have specific clinical symptoms, such as general fears, developmental regression or traumatic re-enactment through play (4).
PTSD contributes to the development of many other mental disorders (5, 6). Around 75% of children and adolescents with PTSD have comorbid disorders. The main comorbidities identified in the pediatric populations are anxiety disorders, attention-deficit-hyperactivity disorder and depression (7, 8, 9). In addition, children and adolescents might present reactive attachment disorder, sleep disturbances and behavior problems (such as oppositional defiant disorder) (8).
Rates of PTSD in children and adolescents exposed to a potentially traumatic event have been shown to vary between 6% and 20% depending on several factors (10). That is, trauma history and exposure, sociodemographic, psychiatric, psychologic, environmental, and biological factors may modulate the development of PTSD.
Concerning trauma history and exposition, it has been reported that individuals who experience multiple trauma are at higher risk of developing chronic PTSD (11). In addition, the degree of violence, the individual experiences during the exposition, is known to influence the development of PTSD (12). However, whether the exposure is direct or indirect does not seem to have an impact on PTSD development, but it may have an effect on its chronicity (13). Repeated trauma cause more PTSD in children and adolescents than single events [35% (14) vs. 18% (15)]. The prevalence of PTSD after a human attack (more than 50% (16, 17) might be much higher than after other traumas [23% to 30%, after a natural disaster (18, 19), 17% after road accidents (15, 20)]. A higher prevalence of PTSD after a mass attack compared to other types of trauma is also described in adults [39% vs 10% (21, 22)].
Among sociodemographic factors, age, sex, socio-economic status (15) and psychosocial resources (23) have been associated with different varying risks of PTSD. Some studies assumed that being a woman or a girl has been found associated with higher risk of PTSD development after a traumatic event (24). Younger children might have a higher prevalence of PTSD compared to older ones [39% for under 6 years versus 33% for 6–11 or 27% 12 years and older (9)]. People with lower socioeconomic status (15) and with depleted psychosocial resources (23) seem at greater risk of PTSD development. Consistent effects were found for these variables in PTSD severity (9.2% more) and PTSD onset (8.75% more), while the results are less obvious concerning racial/ethnic differences in PTSD persistence (5.40% more).
Among psychiatric factors, having anterior mental disorders, and in particular depression, anxious disorders, or PTSD (25) is associated with higher intensity of acute stress reaction and higher risk of peri-traumatic dissociation (26). Moreover, the risk of PTSD chronicization is increased when the child develops PTSD comorbidities (27).
Concerning psychological factors that have been found related to PTSD, the feeling of fear, during trauma and in the first month after the exposition to the traumatic event, is a risk factor implicated in the PTSD development (28). In a similar way, guilt and shame after the event predict the development of this disorder (29). Finally, cognitive alterations, that is, alterations of working memory and executive functioning and attentional biases are correlated with the occurrence and the risk of transition to PTSD chronic state symptoms (30).
Among environmental factors, family reactions during and after the trauma modulate the risk of PTSD development (31). Parental distress as well as parental PTSD and other parental mental disorders conduct to a higher risk of PTSD in children and adolescents (32, 33). On the contrary, quality of familial and social support, available psychological health care, recognition of traumatic impact by the society (31) have been identified as protective factors of PTSD development.
Finally, researches on adults have shown three biological markers of PTSD development: low cortisol 24 h after trauma (34), reduction of the volume of the hippocampus (35) and prefrontal dysfunction (36). Studies underlined that individuals with decreased hippocampus volume and prefrontal dysfunction following exposure displayed more PTSD-related symptoms 1 month after. In contrast, initial smaller hippocampus volume pre-exposure did not have an effect on PTSD-related symptoms (35).
Although several risk factors of PTSD in both children and adults have been documented, most research on risk factors of PTSD development in children and adolescents has focused on a small number of factors. Therefore, there is to date no integrative model of the PTSD development, and of risk of chronicity or relapse. Research on adult PTSD attempts to demonstrate the existence of different PTSD patterns consistent with symptoms, trauma and comorbidity (37) and to understand the temporal courses of PTSD (38). These results have not yet been replicated in children and adolescents.
Because both children and parents were exposed to the event and because of the nature of traumatic event, the prevalence of PTSD in the pediatric population implicated in the Nice attack may be very important.
The primary objective of the “14–7” Program is to characterize the risk and/or protective psychosocial factors affecting the clinical evolution of a pediatric population sample exposed to the terrorist attack of July 14th, 2016 in Nice.
Secondary objectives of the “14–7” Program are to examine efficacy of clinical treatments as a function of the developmental age of the child, and to develop recommendations for treatments and therapies.
Methods/Design
Ethical Consideration, Funding, and Registration
The “14–7” Program protocol was approved by the National Ethics Committee “NORD OUEST III” (number 2017-A02212-51).
All patients and their legal caregivers signed informed written consent upon enrolment in the study. The “14–7” Program has also been registered with ClinicalTrials.gov (number NCT03356028). Inclusions started on November 21st, 2017.
Objectives
The main objective of “14–7” Program is to characterize the risk and/or protective psychosocial factors affecting the clinical evolution of a pediatric population sample, after the “14–7” terrorist attack.
Secondary objectives are: 1) assessment of the prevalence and incidence of mental health disorders, 2) assessment of the intensity of PTSD symptoms, 3) assessment of the intensity of comorbid symptoms, 4) assessment of the quality of the parent–child relationship, 5) assessment of the intelligence quotient, 6) assessment of parental symptoms 7) establishment of a biological collection of saliva samples, and 8) establishment of a magnetic resonance imaging (MRI) and actigraphy data collection.
Study Design
“14–7” is a longitudinal research involving human beings (i.e., French Law: category 2), with minimal risk and constraints, not involving health products. This search is a longitudinal follow-up study until participants reach the age of 25 years old. Participants will be assessed at baseline (T1), 2 years (T2), and 5 years (T3) after the initial assessment (T1), and every 5 years until they are 25 years old (Figure 1). During T1, T2, and T3 salivary samples will be taken from the included children and their parents, for all participants. At T1 and T2, actigraphy and MRI will be proposed for all participants.
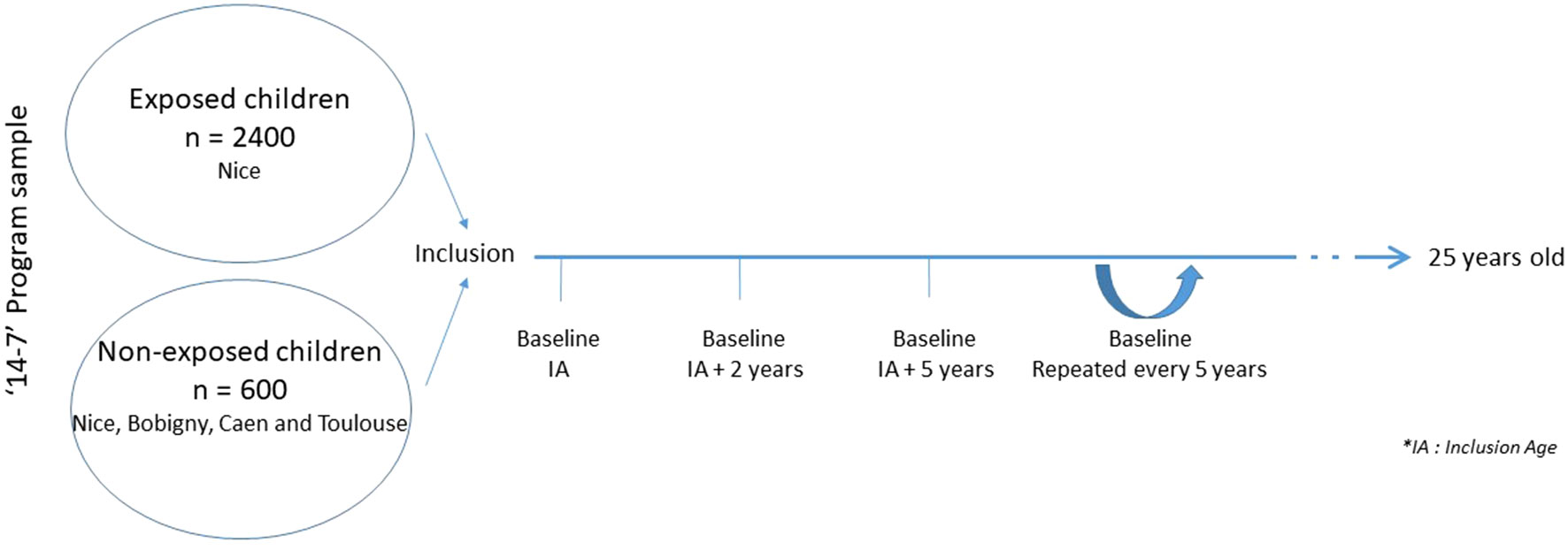
Figure 1 Study design and participants of “14–7” Program.
Each measurement occasion includes four visits. Measures administered at visits 1, 2, 3, and 4 are summarized in Table 1. Assessment will be performed by investigators [child and adolescent psychiatrists, (neuro)psychologists] specifically trained in psychotrauma and child psychiatry.
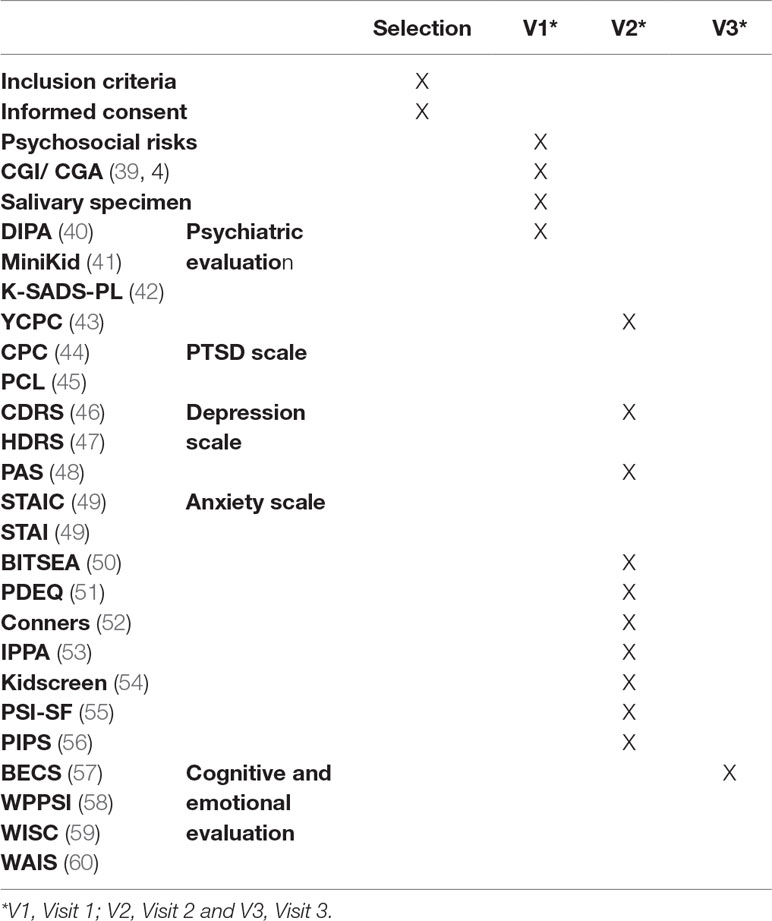
Table 1 “14-7” Program procedure and evaluation criteria for the first study times.
Participants
Two groups were defined:
● Group 1: children exposed to the “14–7” terrorist attack;
● Group 2: children non-exposed to the “14–7” terrorist attack.
Patient selection and recruitment:
Exposed children are recruited by consultation registry of the Nice CHU Lenval, ORSAN database (a national list of victims from terrorist attack). Controls will be matched on age and sex. Moreover, participants will be recruited via press advertisements and National Education. For the control group, categorical screening criteria were used to estimate the number of subjects necessary to reach a statistical power of 80% with a risk of type-I error (α) of 5% for the main outcome variable. Assuming a frequency of development of PTSD of 20% in the general population, to demonstrate a 40% increase in incidence (incidence rate found during violent and intentional traumatic events), it is necessary to include 1,122 participants; that is, 561 child controls. We will then include 600 children (150 per centre) matched on age and sex to the group of exposed children.
Inclusion Criteria
Exposed group:
● Children, adolescents, and young adults of the Nice region exposed by the terrorist attack and aged under 18 years on July 14th, 2016, according to DSM 5.
● Children of pregnant women at the time of the Nice attack.
● Affiliated to a social security scheme;
● Fluent in French;
● Informed written consent of legal guardians and child/adolescent.
Non-exposed group:
● Children, adolescents and young adults, matched in age and gender to exposed group;
● Non-exposed to the “14–7” terrorist attack;
● Affiliated to a social security scheme
● Fluent in French;
● Informed written consent of legal guardians and child/adolescent.
Non-Inclusion and Exclusion Criteria
Non-inclusion criteria for the Nice cohort and control group were children, adolescents and/or young adults with average intellectual disability (IQ below 50), persons deprived of freedom after judicial or administrative decision, and persons subject to an exclusion period due to participation in other research.
Concerning the exclusion criteria, a request made by the child/adolescent/young adult or his/her parent for no longer participating to the “14–7” Program.
Measures
Quantitative and qualitative measures are administered to the participants (summarized in Table 1):
● Questionnaires regarding psychosocial risks (socio-demographic information; exposure to the traumatic event; care immediately after exposure; current care; social support, media exposure; legal procedure and assistance),
● Semi-structured interviews to assess the main diagnosis in children: MiniKid, Diagnostic Infant and Preschool Assessment (DIPA) or Kiddie—Schedule for Affective Disorders and Schizophrenia (K SADS),
● Salivary specimens for the construction of a biological DNA and RNA database,
● Clinical scales to assess PTSD: Young Child PTSD Checklist (YCPC), Child PTSD Checklist (CPC), or PTSD checklist (PCL),
● Clinical scales to assess anxiety: Preschool Anxiety Scale (PAS), Situational-Trait Anxiety Inventory for children (STAIC), or Situational-Trait Anxiety Inventory (STAI),
● Clinical scales to assess depression: Children’s Depression Rating Scale (CDRS) or Hamilton Depression Rating Scale (HDRS),
● Clinical scales to assess ADH/D (Conners),
● Clinical scales to assess dissociative experiences: Peri-traumatic Dissociation Experiences Questionnaire (PDEQ),
● Evaluation of social aspects: Brief Infant-Toddler Social and Emotional Assessment (BITSEA), Inventory of Parenting and Peer Attachment (IPPA), Kidscreen, parental stress index—short form (PSI-SF), or Post-Trauma Inventory of Parental Style (PIPS),
● Cognitive and socio-affective development for the youngest patients (Cognitive and Socio-Emotional Evaluation Battery: BECS) and intelligence quotient: Wechsler Preschool and Primary Scale of Intelligence (WPPSI), Wechsler Intelligence Scale for Children (WISC), or Wechsler Adult Intelligence Scale (WAIS).
● Parents’ clinical symptoms are also evaluated with the Clinical Global Impression (CGI), Clinical Global Assessment Scale (CGA), PCL, HDRS, STAI, PDEQ, PSI-SF and PIPS.
Clinical scales are all based on DSM-5 classification. They are scientifically validated assessment tools and are often used in clinical settings.
Data Collection Process
Each investigator at the different study centers is responsible for collecting and entering data on the electronic CRF (Case Report Form) at the time of the visit. The Child and Adolescent Psychiatry University Unit (SUPEA) and the Research Center (Epidemiology and Population Health (INSERM U1018)) will perform data analysis of the database.
Statistical Analysis
Statistical analyses will be run with R, SPSS, and AMOS softwares.
Descriptive analyses of all the parameters collected at baseline and during follow-up will be conducted.
Correlations will be carried out to examine associations between trauma history and exposition, sociodemographic, psychiatric, environmental, psychological and biological data.
Analyses of variance will be conducted to test the differences between the exposed group and the control group on trauma history and exposition, sociodemographic, psychiatric, environmental, psychological and biological data.
Multivariate models (linear and non-linear regression models, mediation and moderated mediation models) will be carried out to:
1. examine associations between clinical conditions (trauma history and exposition, sociodemographic, psychiatric, environmental, psychological, and biological data), at baseline in children and parents,
2. predict clinical evolution over time with trauma history and exposition, sociodemographic, psychiatric, environmental, psychological and biological variables. Significant predictors from bivariate analysis (at p < 0.05) will then be included in a multivariate regression model. Owing to overlap of assessments, multicollinearity of predictors will be tested and addressed in multivariable models.
Each individual hypothesis will be tested at a significance level of 0.05. However, in order to compensate for the likelihood of incorrectly rejecting a null hypothesis when testing multiple hypotheses (i.e., making a Type I error), methods such as the Bonferroni correction will be used to reduce the likelihood of Type I error when testing multiple comparisons.
These statistics will be conducted on data from the whole cohort and from single groups (i.e., group of exposed children and non-exposed group) and on data from all collection waves.
Outcomes
The main objective of “14–7” Program is to characterize the risk and/or protective psychosocial factors affecting the clinical evolution to the age of 25 years old of a pediatric population sample exposed to the mass trauma of 14 July 2016 in Nice.
Knowledge concerning risk and/or protective factors will help practitioners to detect children and adolescents at high risk of mental disorders in order to provide efficient follow-up and therapy.
Secondary objectives of the “14–7” Program are to examine efficacy of clinical treatments as a function of the developmental age of the child, and to develop recommendations for treatments and therapies. Results will therefore help future clinicians make evidence-based decisions on which treatment to use, depending on the developmental age of the child, and then help reduce the costs of trauma consequences.
Finally, in France, “14–7” Program should rapidly provide clinicians with adapted and standardized assessment tools validated in the pediatric population of all ages in the French language (e.g., DIPA, YCPC, CPC).
Discussion
It has been reported that psychiatric disorders such as PTSD have a high prevalence in war-exposed children (61), and more generally in intentional trauma (62). However, research on psychotrauma in terrorism context on pediatric population is rare and/or very fragmented, and there are few reliable data in children and adolescents exposed to traumatic events (63).
Most epidemiological studies have involved either small samples of number of participants or very heterogeneous samples. For example, in some studies, participants have experienced different types of trauma and in other studies, a very small number of factors related to PTSD have been investigated [for a meta-analysis, see Ref. (31)]. In others, very few factors related to PTSD have been investigated such as quality of life [Ref. (31); see also Ref. (18)]. Then, one of the main advantages of the “14–7” Program is that it includes multiple assessments (psychiatric, psychological, psychosocial, biological, and cognitive), on a population of children having experienced the same traumatogenic event. The interest of “14–7” Program is to understand better clinical and cognitive specificities of trauma in pediatric population. Moreover, “14–7” Program integrates a developmental and biological approach.
Children and adolescents are also vulnerable for conduct, attention, and others psychiatric disorders after a PTSD development (8). An acute understanding of the clinical, cognitive, social, and biological consequences of trauma are necessary to orient specific follow up and treatments of the impacted pediatric population.
The main strength of the “14–7” Program is the standardized evaluation and follow-up of a large number of children and adolescents impacted by a terrorist attack in a country in peace, with assessments until the young adult age (25 years).
The American Academy of Child and Adolescent Psychiatry (AACAP) recommends early interventions for children and adolescents to reduce clinical manifestations of trauma (64). AACAP also suggests that relying on the support of the young patient’s family, school, and friends is important, and that psychotherapies should allow the child to talk about the traumatic event in a safe space by speaking, drawing, playing, or writing. Unfortunately, no recommendation on the types of therapies to use and on their duration has been provided so far (64).
Limitations of the Study
The main limitation of the “14–7” program might be the risk of non-representability of the entire pediatric population impacted by the terrorist attack.
First, individuals exposed to this attack and leaving outside the Nice region will be very difficult to be included. Second, children’ and/or parents’ avoidance behaviour might limit participation to the study. Third, the time lapse between the attack and the start of “14–7” Program does not permit to prospectively analyze clinical manifestations and PTSD during the first year. Nevertheless, questionnaires and diagnostic assessments include retrospective and lifetime evaluations. Finally, participant drop-out occurs in all prospective and longitudinal studies. Attrition not only causes loss of power because of diminishing numbers of participants, but if systematic, this may lead to selection biases and erroneous conclusions being drawn from a study. To prevent attrition, call phoning and newsletters are regularly realized for all participants.
Ethics Statement
The studies involving human participants were reviewed and approved by National Ethics Committee “NORD OUEST III.” Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
MG wrote the manuscript. ST, AS, FG, and MB are the proofreaders. FA is the writer and the coordinator.
Funding
This work has been supported by the Université Côte d’Azur.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
“14–7” Program is funded by Fondation de France, Promenade des Anges, Conseil Départemental 06, Société Française de Psychiatrie de l’Enfant et de l’Adolescent et des Disciplines Associés and Rotary Club.
References
1. Askenazy F, Gindt M, Chauvelin L, Battista M, Guenolé F, Thummler S. Early phase psychiatric response for children and adolescents after mass trauma: lessons learned from the truck-ramming attack in nice on July 14th, 2016. Front Psychiatry (2019) 10:1–9. doi: 10.3389/fpsyt.2019.00065
2. Hornor G. Posttraumatic stress disorder. J Pediatr Health Care (2013) 27(3): e29–e38. doi: 10.1016/j.pedhc.2012.07.020
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorder-5. Arlington, VA, American Psychiatric Association (2013) doi: 10.1176/appi.books.9780890425596
4. Terr L. Childhood traumas: an outline and overview. Am J Psychiat (1991) 148:1020. doi: 10.1176/ajp.148.1.10
5. La Greca A, Silverman W, Wasserstein S. Children’s predisaster functioning as a predictor of posttraumatic stress following Hurricane Andrew. J Consult Clin Psychol (1998) 66(6):883–92. doi: 10.1037//0022-006X.66.6.883
6. Lai B, La Greca A, Auslander B, Short M. Children’s symptoms of posttraumatic stress and depression after a natural disaster: comorbidity and risk factors. J Affect Disord (2013) 146(1):71–78. doi: 10.1016/j.jad.2012.08.041
7. Ardino V. Post-Traumatic syndromes in childhood and adolescence: a handbook of research and practice. UK: John Wiley & Sons, Ltd. (2011). doi: 10.1002/9780470669280
8. Davis L, Siegel L. Posttraumatic stress disorder in children and adolescents: a review and analysis. Clin Child Fam Psychol (2000) 3:135–54. doi: 10.1023/A:1009564724720
9. Salmon K, Bryant R. Posttraumatic stress disorder in children: the influence of develop-mental factors. Clin Psychol Rev (2002) 22:163–88. doi: 10.1016/S0272-7358(01)00086-1
10. Berkowitz S, Stover C, Marans S. The child and family traumatic stress intervention: secondary prevention for youth at risk of developing PTSD. J Child Psychol Psychiatry (2011) 52(6):676–85. doi: 10.1111/j.1469-7610.2010.02321.x
11. Radnitz C, Schlein I, Hsu L. The effect of prior trauma exposure on the development of PTSD following spinal cord injury. J Anxiety Disord (2000) 14(3):313–24. doi: 10.1016/S0887-6185(00)00025-6
12. Ma X, Liu X, Hu X. Risk indicators for posttraumatic stress disorder in adolescents exposed to the 5.12 Wenchuan earthquake in China. Psychiatry Res (2011) 189(3):385–91. doi: 10.1016/j.psychres.2010.12.016
13. Scrimin S, Moscardino U, Capello F, Alto G, Steinberg A, Pynoos R. Trauma reminders and PTSD symptoms in children three years after a terrorist attack in Beslan. Soc Sci Med (2011) 72(5):694–700. doi: 10.1016/j.socscimed.2010.11.030
14. Huemer J, Erhart F, Steiner H. Posttraumatic stress disorder in children and adolescents: a review of psychopharmacological treatment. Child Psychiatry Hum Dev (2010) 41:624–40. doi: 10.1007/s10578-010-0192-3
15. Chossegros L, Hours M, Charnay P. Predictive factors of chronic post-traumatic stress disorder 6 months after a road traffic accident. Accid Anal Prev (2011) 43(1):471–7. doi: 10.1016/j.aap.2010.10.004
16. Feldman R, Vengrober A. Posttraumatic stress disorder in infants and young children exposed to war-related trauma. J Am Acad Child Psy (2011) 50(7):645–58. doi: 10.1016/j.jaac.2011.03.001
17. Harjai M, Chandrashekhar N, Raju U, Jog S. Terrorism, trauma and children. Med J Armed Forces India (2005) 61(4):330–2. doi: 10.1016/S0377-1237(05)80056-5
18. Ularntinon S, Piyasil V, Ketumarn P. Assessment of psychopathological consequences in children at 3 years after tsunami disaster. J Med Assoc Thai (2008) 91(3):S69–75.
19. Yang P, Wu M, Hsu C, Ker J. Evidence of early neurobiological alternations in adolescents with posttraumatic stress disorder: a functional MRI study. Neurosci Lett (2004) 370:13–8. doi: 10.1016/j.neulet.2004.07.033
20. Meiser-Stedman R, Dalgleish T, Glucksman E, Yule W, Smith P. Maladaptive cognitive appraisals mediate the evolution of posttraumatic stress reactions: a 6-month follow-up of child and adolescent assault and motor vehicle accident survivors. J Abnorm Psychol (2009) 118(4):778–87. doi: 10.1037/a0016945
21. Jehel L, Paterniti S, Brunet A, Duchet C, Guelfi JD. Prediction of the occurrence and intensity of post-traumatic stress disorder in victims 32 months after bomb attack. Eur Psychiatry (2003) 18:172–6. doi: 10.1016/S0924-9338(03)00043-9
22. Rosendal S, Salcioğlu E, Andersen H, Mortensen E. Exposure characteristics and peri-trauma emotional reactions during the 2004 tsunami in Southeast Asia, what predicts posttraumatic stress and depressive symptoms? Compr Psychiatry (2011) 52(6):630–7. doi: 10.1016/j.comppsych.2010.12.004
23. Alcantara C, Casement M, Lewis-Fernandez R. Conditional risk for PTSD among Latinos: a systematic review of racial/ethnic differences and sociocultural explanations. Clin Psychol Rev (2013) 33(1):107–19. doi: 10.1016/j.cpr.2012.10.005
24. Yang P, Yen C, Tang T. Posttraumatic stress disorder in adolescents after typhoon Morakot associated mudslides. J Anxiety Disord (2011) 25(3. 2–8. doi: 10.1016/j.janxdis.2010.10.010
25. Stein N, Dickstein B, Schuster J, Litz B, Resick P. Trajectories of response to treatment for posttraumatic stress disorder. Behav Ther (2012) 43(4):790–800. doi: 10.1016/j.beth.2012.04.003
26. Wolf E, Miller M, Reardon A, Ryabchenko K, Castillo D, Freund R. A latent class analysis of dissociation and posttraumatic stress disorder. Arch Gen Psychiatry (2012) 69(7):698–705. doi: 10.1001/archgenpsychiatry.2011.1574
27. Back S, Sonne S, Killeen T, Dansky B, Brady K. Comparative profiles of women with PTSD and comorbid cocaine or alcohol dependence. Am J Drug Alcohol Abuse (2003) 29(1):169–89. doi: 10.1081/ADA-120018845
28. Holbrook T, Hoyt D, Coimbra R, Potenza B, Sise M, Anderson J. Long-term posttraumatic stress disorder persists after major trauma in adolescents: new data on risk factors and functional outcome. J Trauma (2005) 58:764–71. doi: 10.1097/01.TA.0000159247.48547.7D
29. Brewin C, Holmes E. Psychological theories of posttraumatic stress disorder. Clin Psychol Rev (2003) 23(3):339–76. doi: 10.1016/S0272-7358(03)00033-3
30. Bomyea J, Risbrough V, Lang A. A consideration of select pre-trauma factors as key vulnerabilities in PTSD. Clin Psychol Rev (2012) 32(7):630–41. doi: 10.1016/j.cpr.2012.06.008
31. Alisic E, Jongmans M, van Wesel F, Kleber R. Building child trauma theory from longitudinal studies: a meta-analysis. Clin Psychol Rev (2011) 31(5):736–47. doi: 10.1016/j.cpr.2011.03.001
32. Bluestone N, Roberts A, Paradis A, Miller A, Saxe G, Koenen K. Parental sensitivity to child distress accurately predicts PTSD symptom severity in children. Compr Psychiatry (2011) 52(6):E2–3. doi: 10.1016/j.comppsych.2011.04.012
33. Morris A, Gabert-Quillen C, Delahanty D. The ASSOCIATION between parent PTSD/depression symptoms and child PTSD symptoms: a meta-analysis. J Pediatr Psychol (2012) 37(10):1076–88. doi: 10.1093/jpepsy/jss091
34. Bryant R. Early predictors of posttraumatic stress disorder. Biol Psychiatry (2003) 53(9):789–95. doi: 10.1016/S0006-3223(02)01895-4
35. Admon R, Leykin D, Lubin G. Stress-induced reduction in hippocampal volume and connectivity with the ventromedial prefrontal cortex are related to maladaptive responses to stressful military service. Hum Brain Mapp (2012) 34(11):2808–2816. doi: 10.1002/hbm.22100
36. Jovanovic T, Norrholm S, Blanding N. Impaired fear inhibition is a biomarker of PTSD but not depression. Depress Anxiety (2010) 27(3):244–51. doi: 10.1002/da.20663
37. Muller M, Vandeleur C, Rodgers S. Factors associated with comorbidity patterns in full and partial PTSD: findings from the PsyCoLaus study. Compr Psychiatry (2014) 55(4):837–848. doi: 10.1016/j.comppsych.2014.01.009
38. Rona R, Jones M, Sundin J. Predicting persistent posttraumatic stress disorder (PTSD) in UK military personnel who served in Iraq: a longitudinal study. J Psychiatry Res (2012) 46(9):1191–8. doi: 10.1016/j.jpsychires.2012.05.009
39. Guy W, National Institute of Mental Health (U. S.). Psychopharmacology research branch. division of extramural research programs. ECDEU assessment manual for psychopharmacology. Rockville, Md. : U.S. Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs. Consulté à l’adresse. (1976). http://archive.org/details/ecdeuassessmentm1933guyw.
40. Scheeringa MS, Haslett N. The reliability and criterion validity of the diagnostic infant and preschool assessment: a new diagnostic instrument for young children. Child Psychiatry Hum Dev (2010) 41(3):299–312. doi: 10.1007/s10578-009-0169-2
41. Sheehan DV, Sheehan KH, Shytle RD. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J Clin Psychiatry (2010) 71(3):313–26. doi: 10.4088/JCP.09m05305whi
42. Kaufman J, Birmaher B, Axelson DA, Perepletchikova F, Brent D, Ryan N. K-SADS-PL DSM 5. In: Child and Adolescent Research and Education. Pittsburgh: Western Psychiatric Institute and Clinic. (2016).
44. Scheeringa MS. child PTSD checklist — parent version (CPC - P). New Orleans: Tulane University. (2014).
45. Weathers F, Litz B, Keane T, Palmieri P, Marx BP, Schnurr P. The PTSD checklist for DSM-5 (PCL-5). National Center for PTSD (2013).
46. Posnanski EO, Grossman RN, Buchsbaum Y, Banegas M, Freeman L, Gibbons R. Preliminary studies of reliability and validity of the children’s depression scale. J Am Acad Child Psychiatry (1984) 23(2):191–7. doi: 10.1097/00004583-198403000-00011
47. Guelfi J, Criquillion-Doublet S. Dépression et syndromes anxio-dépressifs. Neuilly-sur-Seine: Ardix Medical. (1993).
48. Spence SH, Rapee R, McDonald C, Ingram M. The structure of anxiety symptoms among preschoolers. Behav Res Ther (2001) 39(11):1293–316. doi: 10.1016/S0005-7967(00)00098-X
49. Spielberger D, Gorsuch R, Lushene R, Vagg P, Jacobs G. Manual for the state-trait anxiety inventory. Palo Alto: CA: Consulting Psychologist Press (1983).
50. Wendland J, Danet M, Gacoin E. French version of the Brief Infant-Toddler Social and Emotional Assessment questionnaire — BITSEA. J Pediatr Psychol (2014) 39(5):562–75. doi: 10.1093/jpepsy/jsu016
51. Bui E, Brunet A, Allenou C. Peritraumatic reactions and posttraumatic stress symptoms in school-aged children victims of road traffic accident. Gen Hosp Psychiatry (2010) 32(3):330–3. doi: 10.1016/j.genhosppsych.2010.01.014
52. Egeland J, Kovalik-Gran I. Validity of the factor structure of Conners’ CPT. J Atten Disord (2010) 13(4):347–57. doi: 10.1177/1087054709332477
53. Gullone E, Robinson K. The inventory of parent and peer attachment-revised (IPPA-R) for children: a psychometric investigation. Clin Psychol Psychother (2005) 12(1):67–79. doi: 10.1002/cpp.433
54. Ravens-Sieberer U, Gosch A, Rajmil L. KIDSCREEN-52 quality-of-life measure for children and adolescents. Expert Rev Pharmcoecon Outcomes Res (2005) 5(3):353–64. doi: 10.1586/14737167.5.3.353
55. Abidin R. Parenting stress index, short form: professional manual. In: Parenting Stress Index., 3rd ed. Odessa, FL: Psychological Assessment Resources, Inc. (1995).
56. Scheeringa MS. Posttrauma Inventory of Parental Style (PIPS). New Orleans: Tulane University. (2002).
57. Adrien JL, Blanc R, Thiebaut E. Etude préliminaire de la validation d’un nouvel instrument, la BECS (Batterie d’Evaluation Cognitive et Socio émotionnelle), pour l’évaluation du développement psychologique d’enfants à autisme. ANAE (2005) 83(84):165–8.
58. Wechsler D. Wechsler preschool and primary scale of intelligence. 4th edition (WPPSI -4TM). NY: Pearson. (2012).
61. Halevi G, Djalovski A, Vengrober A, Feldman R. Risk and resilience trajectories in war-exposed children across the first decade of life. J Child Psychol Psychiatry (2016) 57(10):1183–93. doi: 10.1111/jcpp.12622
62. Kessler RC, Sonnega A, Bomet E, Hughes M, Nelson CB, Breslau N. Epidemiological risk factors for trauma and PTSD. In: Yehuda R, editor. Risk factors for posttraumatic stress disorder. Washington DC: American Psychiatric Press (1999). p. 23–59.
63. Josse E. Le traumatisme psychique: Chez le nourrisson, l’enfant et l’adolescent. Bruxelles: De Boeck Supérieur (2011). doi: 10.3917/dbu.josse.2011.01
Keywords: post-traumatic stress disorder, children, longitudinal studies, cohort, psychiatry
Citation: Gindt M, Thümmler S, Soubelet A, Guenolé F, Battista M and Askenazy F (2019) Methodology of “14–7” Program: A Longitudinal Follow-Up Study of the Pediatric Population and Their Families Exposed to the Terrorist Attack of Nice on July 14th, 2016. Front. Psychiatry 10:629. doi: 10.3389/fpsyt.2019.00629
Received: 29 May 2019; Accepted: 05 August 2019;
Published: 12 September 2019.
Edited by:
Jonathan Lachal, INSERM U1018 Centre de recherche en Épidémiologie et Santé des Populations, FranceReviewed by:
Silke Schauder, University of Picardie Jules Verne, FranceLayla Tarazi-sahab, Saint Joseph University, Lebanon
Copyright © 2019 Gindt, Thümmler, Soubelet, Guenolé, Battista and Askenazy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Morgane Gindt, Z2luZHQubUBwZWRpYXRyaWUtY2h1bGVudmFsLW5pY2UuZnI=