 Marta Sancho1,2*
Marta Sancho1,2* Marta de Gracia2
Marta de Gracia2 Roser Granero3,4
Roser Granero3,4 Sara González-Simarro1
Sara González-Simarro1 Isabel Sánchez2,3
Isabel Sánchez2,3 Fernando Fernández-Aranda2,3,5
Fernando Fernández-Aranda2,3,5 Joan Trujols1,6
Joan Trujols1,6 Núria Mallorquí-Bagué1,2,3
Núria Mallorquí-Bagué1,2,3 Gemma Mestre-Bach2,3
Gemma Mestre-Bach2,3 Amparo del Pino-Gutiérrez2,3,7Teresa Mena-Moreno2Cristina Vintró-Alcaraz2
Amparo del Pino-Gutiérrez2,3,7Teresa Mena-Moreno2Cristina Vintró-Alcaraz2 Trevor Steward2,3
Trevor Steward2,3 Neus Aymamí2Mónica Gómez-Peña2
Neus Aymamí2Mónica Gómez-Peña2 José Manuel Menchón2,5,6
José Manuel Menchón2,5,6 Susana Jiménez-Murcia2,3,5*
Susana Jiménez-Murcia2,3,5*- 1Department of Psychiatry, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 2Department of Psychiatry, Bellvitge University Hospital-IDIBELL, L’Hospitalet de Llobregat, Spain
- 3CIBER Fisiopatología Obesidad y Nutrición (CIBERobn), Instituto de Salud Carlos III, Madrid, Spain
- 4Department of Psychobiology and Methodology, Autonomous University of Barcelona, Barcelona, Spain
- 5Department of Clinical Sciences, School of Medicine, University of Barcelona, Barcelona, Spain
- 6CIBER Salud Mental (CIBERsam), Instituto de Salud Carlos III, Madrid, Spain
- 7Nursing Department of Mental Health, Public Health, Maternal and Child Health, Nursing School of the University of Barcelona, Barcelona, Spain
Introduction: Impairments in emotion regulation are understood to be a transdiagnostic risk factor of suffering from compulsive and addictive behaviors. The aim of this study was to investigate the role of emotion regulation deficits in gambling disorder and to analyze these differences taking gender, age, and gambling activity preferences into account. Methods: The sample included n = 484 patients seeking treatment for gambling disorder at a specialized outpatient service. Main outcomes were sociodemographic variables, emotion regulation, and gambling severity. Results: Differences between sexes were found in non-acceptance of emotions. Older patients obtained higher levels in non-acceptance of emotions, lack of emotion regulation strategies, emotional clarity, and global emotion regulation scores. No differences were found in emotion scores considering gambling preferences (non-strategic versus strategic). Path analysis showed that emotion regulation scores and age had a direct effect on gambling disorder severity, while emotion regulation and gambling preference were not mediational variables in the relationships of gender and age with gambling severity. Conclusions: Emotion regulation impairments differ in patients seeking treatment for gambling problems. Early prevention and intervention programs should incorporate the different dimensions of this process, taking into account clinical phenotypes.
Introduction
Impairments in emotion regulation (ER) are understood to be a transdiagnostic risk factor for the onset and maintenance of addictions (1–5). According to Gross (6, p. 275), ER refers to “those processes for which individuals exert an influence on their emotions, when have them and how experience and express them.” Other models such as that by Gratz and Roemer (7) focus on difficulties in ER, underlying that healthy ER should consist in the capacity to modulate rather than suppress negative emotional states (8). These authors name several components of emotional dysregulation, such as impaired awareness of emotions or an inability to refrain from impulsive behavior when experiencing negative emotions. Studies focusing on clinical samples have shown that individuals with ER deficits often engage in maladaptive behaviors to downregulate or to escape from their emotions (1, 5, 9). These difficulties in managing emotions can lead to a lack of coping skills and bring about errors in self-regulation and impulse control, which constitute a risk factor for several disorders such as behavioral addictions (5, 10, 11).
Concerning gambling disorder (GD; 12), although different subgroups can be identified, with differentiated clinical, psychopathological, and personality characteristics, ER problems are usually present in most people affected by this disorder (13–15). Rogier and Velotti (8) conceptualize this addiction in a model that integrates ER components described in Gratz and Roemer’s model and the timeline model by Sheppes et al. (16) of healthy ER processing. In this way, these authors refer to difficulties in ER processes among the individuals with GD. For instance, pathological gamblers show deficits in identifying emotions because of a failure in emotional awareness, a difficulty in accepting emotional states, and poor ER self-efficacy. In line with these results, Williams et al. (1) found a lack of emotional clarity and emotional awareness as well as a high impulsivity in a sample with GD. Other authors reported greater difficulties in describing feelings as well as higher scores in externally oriented thinking in this population compared to healthy controls (17–19). Orlowski et al. (20) associated a lack of reappraisal or an accepting attitude toward negative emotions with the number of Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) symptoms, indicating a greater GD severity. Consistent with previous studies, GD is defined as an affect regulation disorder in which the gambling serves as a coping strategy (21). These findings emphasize the role that emotion dysregulation and other related constructs, such as alexithymia, play in the vulnerability to GD (9).
A potentially addictive behavior like gambling could be used as a coping strategy in the presence of negative emotional states (22, 23), especially in the case of emotionally vulnerable problem gamblers (13). Along these lines, GD research has described different groups of gamblers depending on the nature of ER motivations. For instance, McCormick and Taber (24) described two types of gamblers based on arousal levels: over-stimulated or under-stimulated gamblers. This last type is similar to gamblers with alexithymia, described by Bonnaire et al. (25, 26), who are characterized by a need for continuous stimulation, participating in exciting activities such as strategic gambling (e.g., sport bets or poker) (27). In addition, these individuals present greater GD severity than those with a preference for non-strategic gambling (e.g., slot machines or bingo). This passive gambling (non-strategic gambling) is understood as an avoidance strategy when faced with depressive symptoms. As a whole, this suggests that gambling preference/s seem to be clinically significant and provide a way of subtyping individuals with gambling-related problems (27–29).
Other variables, such as gender or age, have a core role in the relationship between ER and GD. Studies carried out in the general population showed significant differences in ER profiles related to age and gender. Positive emotional experiences and the use of strategies to maintain them are more frequent with age (30, 31), whereas more negative and changing emotional states are experienced during adolescence (32–34). In this regard, older people refer to a greater ability in using ER strategies (35, 36). However, ER competence decreases among older people with high levels of emotion activation, for example, in those who have experienced negative life events (35, 36). In relation to gender, a greater tendency toward rumination in women could account for increased anxiety and affective disorders (37, 38). It has also been suggested that women’s higher scores in distraction could lead them to use gambling more frequently as a way to escape or to avoid stressful situations and daily life frustrations (39–41).
Previous research has mainly focused on gambling preferences and GD profiles. However, no study to date has addressed underlying mechanisms (including direct and indirect effects) between ER and other variables, such as gender and age. ER impairments can have a significant impact on the treatment outcome (42, 43). For this reason, identifying the variables associated with ER difficulties is crucial for designing treatments that are more specific and tailored to each patient, with the aim of increasing the response to treatment (43). Therefore, those patients with greater ER difficulties could benefit from specific treatments such as mindfulness (42, 43) or serious games aimed at improving these capabilities (44).
Based on the theoretical framework mentioned above, the aims of the current study were: a) to evaluate differences in ER domains based on gender, age, and gambling preferences; b) to examine the predictive capacity of ER domains on GD severity and to explore the potential moderating role of gender, age, and gambling subtype; and c) to conduct a path analysis model valuing the underlying mechanism between gender, age, gambling preference, ER, and gambling severity. We hypothesized that female gender, strategic gambling, and young age would predict ER deficits, and that these difficulties would be associated with greater gambling severity.
Methods
Participants
The sample consisted of 484 patients (450 men and 34 women) with gambling-related problems, consecutively recruited and receiving outpatient treatment at the Gambling Disorder Unit at the Department of Psychiatry of Bellvitge University Hospital between 2015 and 2017. All patients were over 18 years of age. Exclusion criteria were the presence of an organic medical illness or neurodegenerative condition (such as Parkinson’s disease); a psychotic disorder; and current (or history of) brain injury, a neurological disease, or intellectual disabilities.
Measures
Diagnostic Questionnaire for Pathological Gambling according to DSM criteria (45). This scale includes 19 items to assess DSM diagnostic criteria for GD, based on both the DSM, Fourth Edition, Text Revision (DSM-IV-TR) and DSM-5. The Spanish adaptation of the questionnaire has good psychometric properties (α = 0.81 for general population and α = 0.77 for GD clinical sample; 46). This study analyzed the total number of DSM-5 criteria for GD as a measure of gambling behavior severity.
Difficulties in Emotion Regulation Scale (DERS; 7). This self-report questionnaire contains 36 items that assess difficulties in regulating emotions. It is composed of six first-order scales: 1) non-acceptance of emotional responses, 2) difficulties engaging in goal-directed behavior, 3) impulse-control difficulties, 4) lack of emotional awareness, 5) limited access to effective ER strategies, and 6) lack of emotional clarity. A total scale is also available as a global measure of emotion dysregulation. This study used the Spanish version of the questionnaire, which has demonstrated adequate psychometric features (47).
Sociodemographic and Clinical Variables. Patients completed a semi-structured face-to-face interview regarding GD, psychopathological symptoms, and personality traits (48). The same interview also collected sociodemographic data (e.g., education, occupation, marital status) and additional clinical information, such as gambling preferences (non-strategic versus strategic gambling). Social status was measured using the Hollingshead index, a survey based on educational level and occupational prestige (49).
Table 1 includes the internal consistency (Cronbach’s alpha, α) for the psychometric scales used in the study. Effect sizes for these coefficients, according to Cicchetti (50), were in the fair range (α = 0.714 for DERS lack of emotional awareness scale) to excellent (α = 0.930 for DERS total scale).

Table 1 Sample description (n = 484).
Procedure
The assessment was conducted prospectively upon arrival to the treatment unit and prior to treatment during a face-to-face interview (with a mean duration of 90 min), in which the tests mentioned above were administered.
In this study, the differentiation between strategic versus non-strategic gambling was based on gambling activity, which represented the highest impairment for the participants and was reported as the main reason for seeking treatment.
Statistical Analysis
Statistical analysis was carried out with Stata15 for Windows. Comparisons for mean scores on DERS scales were based on analysis of variance (ANOVA) procedures. Gender comparisons (women versus men) were adjusted for the covariates age and GD severity (DSM-5 total criteria). Group age comparisons (two groups were compared based on the age median in the sample) were adjusted for patients’ gender and GD severity. Comparisons for gambling preference (non-strategic vs. strategic) were adjusted for patients’ gender, age, and GD severity. The effect size for mean differences was estimated through Cohen’s d coefficient (|d| > 0.20 was considered poor effect size, |d| > 0.5 was moderate, and |d| > 0.8 was large; 51). In this study, Finner’s procedure was used to control type I error due to multiple comparisons (this method is included in the family-wise error rate stepwise procedures and offers a more powerful test than Bonferroni correction; 52).
The predictive capacity of ER dimensions (DERS scores, defined as the independent variable) on GD severity (DSM-5 total criteria for GD, defined as the criterion) was assessed with a lineal multiple regression. Independent models were obtained considering DERS first-order scales and DERS total scales, and the modeling was run in three blocks: a) the first block included and set the participants’ gender, age, and gambling preference; b) the second block added DERS scale scores; and c) the third block added and tested the interactions between each DERS scale and gender, age, and gambling subtype. The final model only retained those significant interaction parameters (p ≤ 05), obtained main effects for DERS scales that had no significant interaction parameters and single effects for DERS scales with significant interactions. The predictive capacity of the final model was measured through the adjusted R2 coefficient, and the predictive capacity of each block through the change in the adjusted R2.
Structural equation modeling (SEM) was conducted to test the underlying mechanisms between the patients’ gender, age, gambling preference (non-strategic vs. strategic), ER levels (DERS scale scores), and GD severity (DSM-5 total criteria). Specifically, path analysis was run using the maximum likelihood (ML) estimator, and the overall goodness-of-fit was evaluated through standard statistical measures (53): the root mean square error of approximation (RMSEA), Bentler’s comparative fit index (CFI), the Tucker–Lewis index (TLI), and the standardized root mean square residual (SRMR). RMSEA < 0.10, TLI > 0.9, CFI > 0.9, and SRMR < 0.1 were considered adequate model fit.
Results
Sample Characteristics
Table 1 includes the description of the sociodemographic and clinical variables of the study sample. Most participants were men (93%), born in Spain (92.4%), single (45.7%) or married (or living with a stable partner, 39.7%), with low education levels (56.4% completed primary schools), employed (64.7%), and with middle-low (39.3%) to low (43.0%) social position index. The mean age was 41.3 years (SD = 13.2), the mean age of GD onset was 29.1 years (SD = 11.8), and the mean duration of GD was 5.8 years (SD = 5.9). Regarding gambling variables, the mean number of DSM-5 criteria for GD was 7 (SD = 2), and 56.8% of the patients reported debts related to gambling behaviors. Based on the GD severity classification of DSM-5, n = 31 patients were in the problematic group (6.4% of the participants did not meet clinical criteria for GD diagnosis and reported between one and three symptoms), n = 66 in the low-severity group (13.6%, with four or five symptoms), n = 158 in the moderate-severity group (32.6%, with six or seven symptoms), and n = 229 in the severe group (47.3%, with eight or nine symptoms).
Associations Between Emotion Regulation and Gender, Age, and Gambling Preference
Table 2 contains the results of the ANOVA procedures (adjusted for age and GD severity) in the study [all the models fulfilled goodness-of-fit, with non-significant results (p > .05) in the lack-of-fit tests]. The upper part of this table includes the comparison of mean DERS scores for both genders (ANOVA adjusted for age and GD severity). Significant differences were only found for the non-acceptance of emotions scale: men showed higher mean scores than women (17.6 versus 15.1, p = .031).
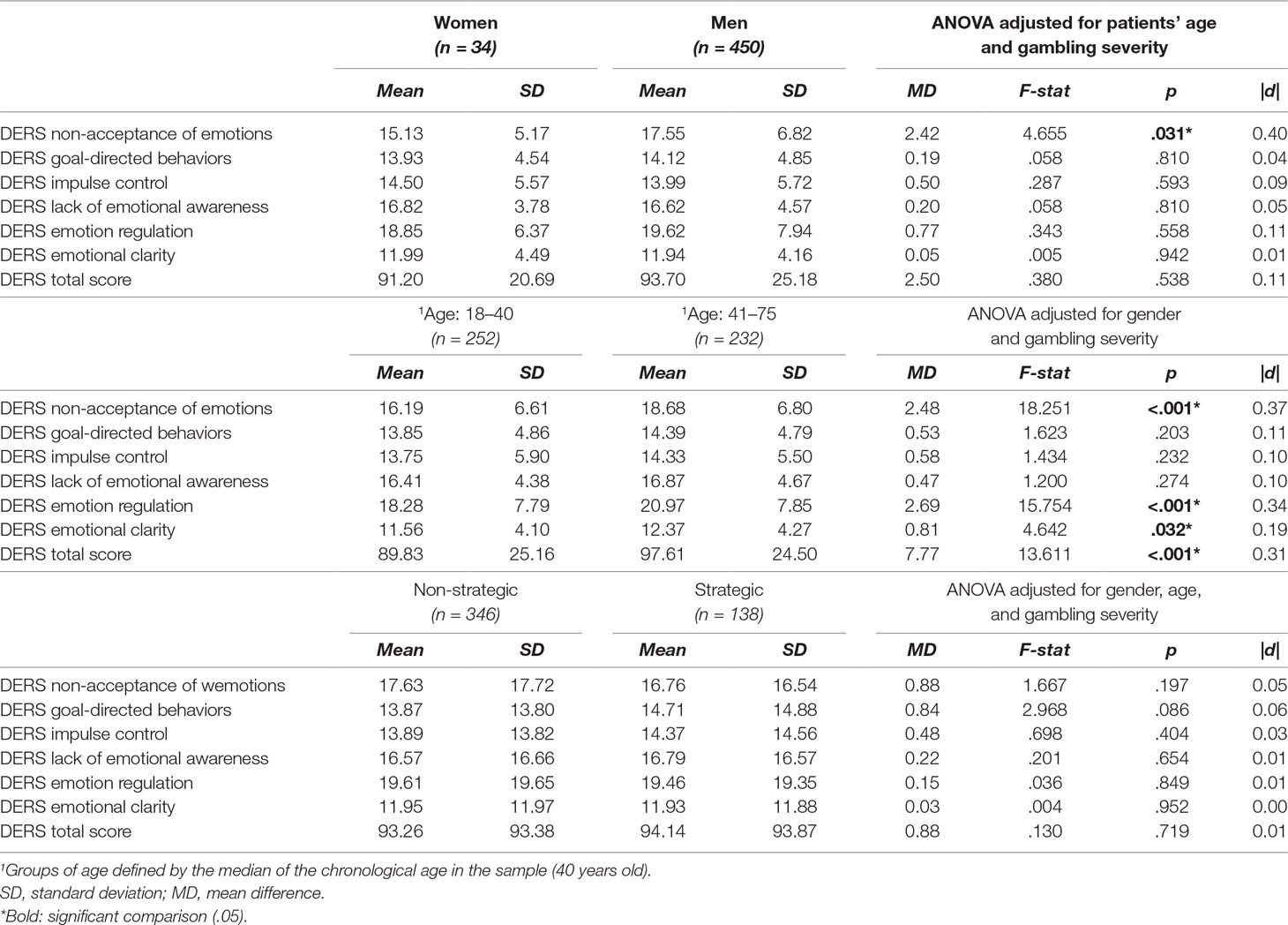
Table 2 Comparison of the DERS scores based on gender, age, and gambling preference.
The middle section of Table 2 contains the mean comparisons between the two age groups (classification that was based on the median—percentile 50—age of the sample, 40 years old), adjusted for gender and GD severity. Higher means corresponded to participants in the older age group for DERS non-acceptance of emotions, limited access to effective ER strategies, lack of emotional clarity, and total scales.
The lower part of Table 2 includes the comparison of DERS subscale scores based on gambling preferences (non-strategic versus strategic). No statistically significant differences between both groups were found.
Predictive Model
Table 3 includes the two models valuing the predictive capacity of ER dimensions on GD severity, as well as the potential moderating role of gender, age, and gambling preference. The block assessing the interaction parameters between DERS scores and participants’ gender, age and, gambling preference was not significant (block/step 3 of model 1: F = 1.18, df = 18/440, p = .272; block/step 3 of model 2: F = 1.27, df = 3/460, p = .285), indicating that the contribution of ER to gambling severity is not dependent on/moderated by these features. Considering the regression including DERS first-order scales, gambling severity was higher for younger patients and those with greater levels in ER scales measuring non-acceptance of emotions and impulse control. Regarding the regression modeling for DERS total scale (model 2), gambling severity was also higher for younger participants and those with higher DERS total scores.
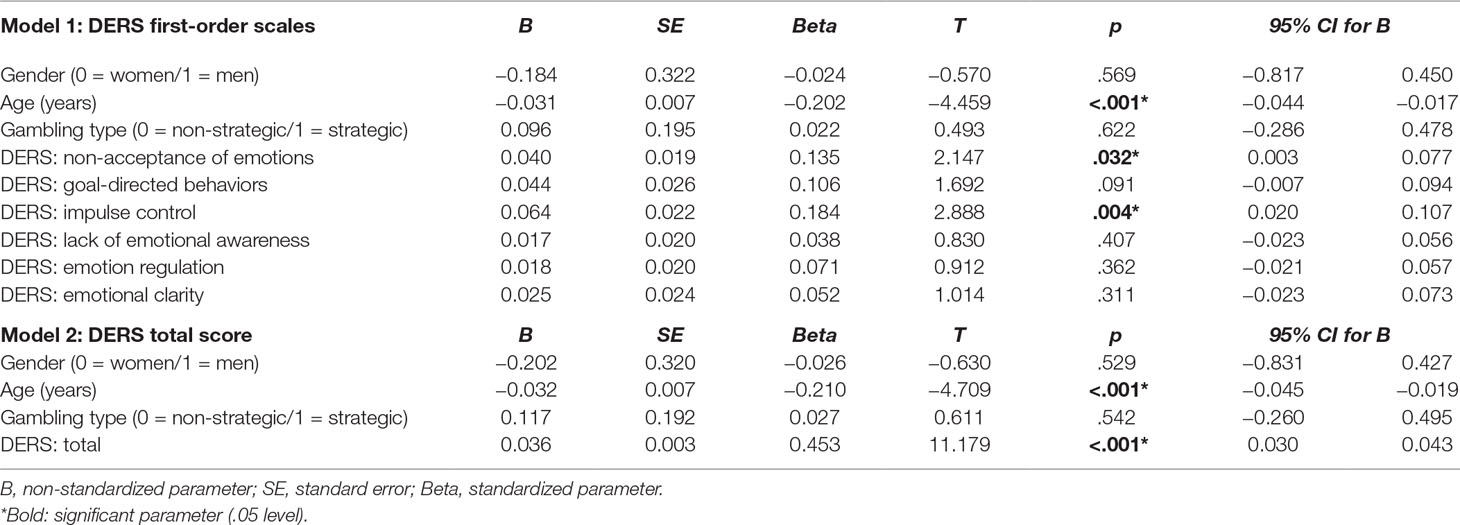
Table 3 Predictive capacity of emotion regulation on gambling severity (DSM-5 total criteria).
Pathways Analysis
Figure 1 includes the path diagram with the standardized coefficients obtained in SEM (Table S1, Supplementary Material, contains complete model results). The independent variables of the model were gender (0 = female, 1 = male) and age (years). The dependent variable was GD severity (DSM-5 total criteria), and the mediational variables were gambling preference (0 = non-strategic; 1 = strategic) and ER levels (a latent variable was defined as a global measure of ER difficulties based on the raw scores on the first-order factors of the DERS). Adequate goodness-of-fit was obtained: RMSEA = 0.054 (95% CI: 0.037 to 0.072), CFI = 0.978, TLI = 0.961, and SRMR = 0.035. The global predictive capacity for the model was around 19%.
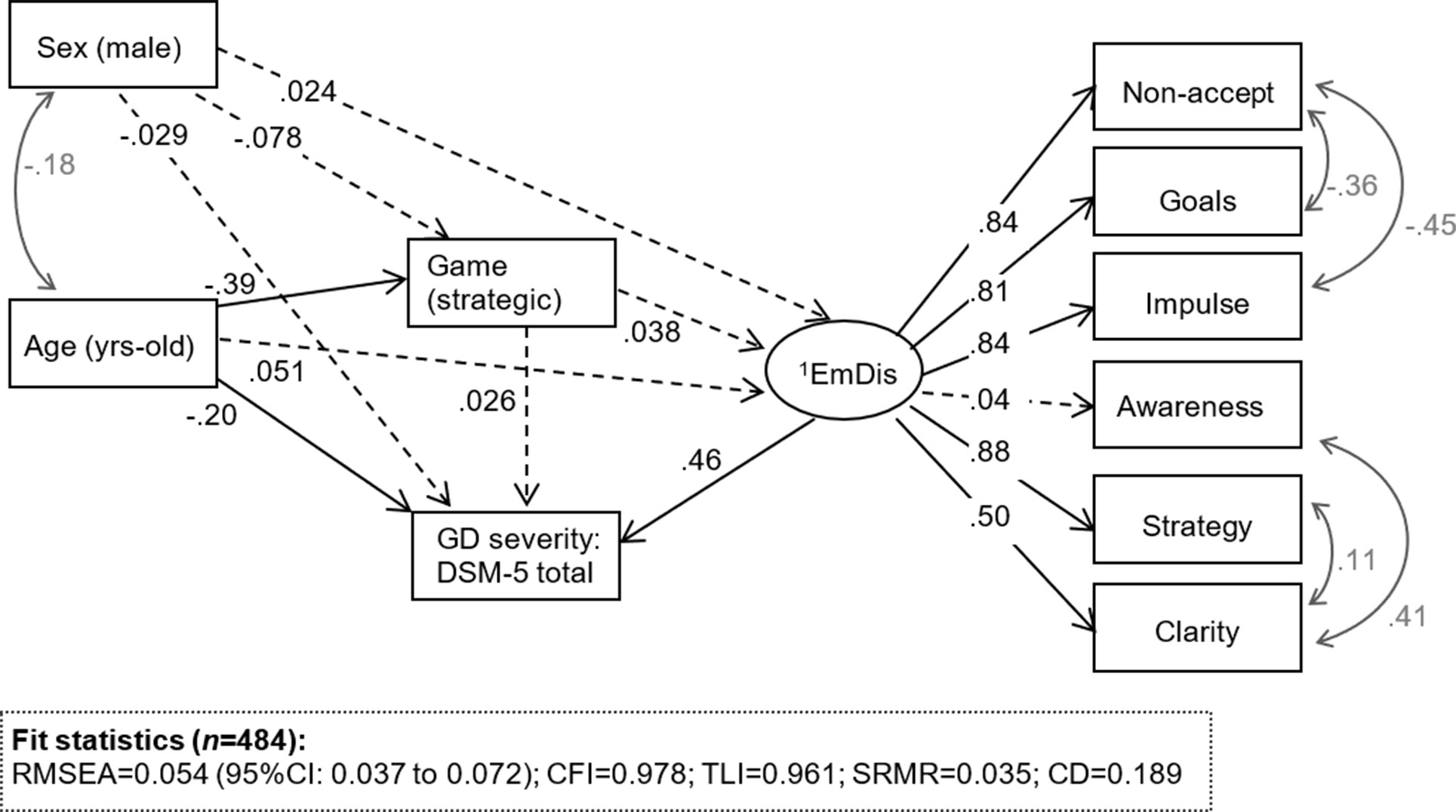
Figure 1 Sem model for the whole sample, standardized coefficients. Note. 1EmDis: emotional dysregulation (latent variable defined with the DERS first order scales). Continous line: significant coefficient (.05 level). Dash-line: non-significant coefficient. Grey: covariance parameter
Regarding the latent variable, all DERS subscales obtained significant and high loadings (higher than 0.30), except for the awareness dimension. DERS scores obtained a direct effect on GD severity (the higher the scores, the higher the GD severity), and age also registered a direct effect on this criterion (the younger the patients, the higher the number of GD DSM-5 criteria). No direct effect of gender and gambling preference on gambling severity was found. DERS scores and gambling preference were not mediational variables between gender or age and gambling severity.
Discussion
The present study analyzed the role of ER, as measured on the DERS, on GD severity and the potential differences in gender, age, and gambling preference. The main results of our study demonstrate higher levels of the non-acceptance of emotions among men, worse ER scores in older patients, and no significant differences in ED regarding gambling preferences (comparing non-strategic versus strategic activities). Path analysis showed direct effects of age and ER scores on GD severity and that ED and gambling preference did not mediate the relationship between gender or age and GD severity.
Contrary to hypothesized, the comparison of ER profiles by gender showed more difficulties in ER for men compared to women (specifically, men had poorer performance in the non-acceptance of emotions domain). A possible explanation of this finding could be due to the fact that men tend to adopt less adaptive strategies, namely, emotional suppression rather than cognitive reappraisal (54). On the contrary, women show greater predisposition to report their emotional states and to use more adaptive ER strategies than men (55–58). This greater emotional awareness has been observed in women even from an early age (59–61). Similarly, some studies suggest non-aware and automatic ER in men on leisure activities (62–64), showing a tendency to suppress emotional experience (35). This increased difficulty in accepting emotions could drive men to get involved in distracting activities as an experiential avoidance strategy and also lead to other forms of psychopathology (such as alcohol abuse) (39).
Also, contrary to our hypothesis regarding age, in this sample, older patients showed higher scores in three first-order scales of DERS (limited access to effective ER strategies, lack of emotional clarity, and non-acceptance of emotions) as well as in DERS total scores. Based on the available data, we would expect worse performance in ER for younger patients (32–34). One possible explanation accounting for our results could come from GD itself: patients’ involvement in persistent, uncontrollable, and unwanted gambling behavior generates significant emotional discomfort (distress), which could increase maladaptive ER strategies even at older ages. This hypothesis requires further empirical research, however. In line with this, some pioneering studies suggest that some strategies, such as emotional suppression, may be a useful form of ER for managing stressors in older age, which entails a possible decoupling of the psychological distress with age (65). However, these results must be evaluated with caution, since they have not assessed the specific contribution of ER domains in clinical samples of GD patients.
No significant differences between gambling preference (comparing non-strategic and strategic gambling) and ER profile in our sample were found. A possible explanation for our results could be the psychometric measures used. Perhaps the inclusion of other measures of ER and related constructs would yield different results. In line with this, studies have related gambling preference with alexithymia. For instance, Bonnaire et al. (26) demonstrated problems of alexithymia in individuals with a preference for strategic gambling (e.g., sport bets or poker) and depressive symptoms in those with a preference for non-strategic gambling (e.g., slot machines or bingo). Similarly, other authors (28, 29, 65) found a subtype of addicted gamblers who experience high levels of excitement and narcissistic traits. These individuals would be involved in strategic gambling, which induces elevated arousal though a high excitatory potential, suggesting possible alexithymia.
In the present study, gambling severity was higher for younger patients. So, GD severity was higher in patients with higher levels across several ER domains (e.g., non-acceptance of emotions and impulse control), as well as ER global measure. Greater GD severity in younger individuals could be explained by a preference of strategic gambling in this population. In addition, this subtype of gambling causes a higher level of gambling-related biases, such as illusion of control (66, 67), increasing the severity of the disorder. In line with this, previous studies showed that strategic gambling is associated with increased severity and with young gamblers, while non-strategic gamblers tend to be older and less severe (26, 68–71). Likewise, an early onset of GD is generally related to a severe presentation, as well as dysfunctional personality traits and greater psychopathology (46, 72). Other studies have shown less severity with advancing age, although medical problems and depression increase (68, 69). In accordance with other studies (25, 26, 73), in which ER-related constructs, such as alexithymia, were positively correlated with gambling severity, our results also indicated higher levels of ER deficits when gambling severity was higher. The severity of the disorder was higher in the younger group, but older patients showed greater levels of ER. Some studies have identified associations between psychopathology and older age (72), suggesting that gambling could be a dysfunctional strategy to cope with or to regulate negative emotions in these cases (74, 75).
Our study has several limitations that need to be considered when interpreting the results. Firstly, the sample of this work includes mainly men with medium-low to low social position levels and primary school education. Secondly, the number of women featured in the study is very small compared to men, which could decrease statistical power (that is, increase in the likelihood of a type II error and therefore the ability to detect the real effect of gender on the relationship between ER and gambling). It must be argued, however, that this study included all the patients consecutively arriving at the treatment unit, where the proportion of GD in men is higher. The number of women was enough to allow for statistical analyses. Thirdly, the size of the non-strategic gambler group was greater than the strategic gambling group, and this could have interfered in our results. Further studies with larger sample sizes are needed to increase statistical power and external generalization validity.
In spite of these limitations, the results of this study highlight the importance of taking into account gender, age, and gambling type during treatment. The severity presented by the younger patients and those with a high level of ER could hinder cognitive–behavioral therapy. Although this treatment is effective for GD, in these cases, other approaches could be considered (42, 76, 77). This subgroup could benefit from mindfulness-based interventions (MBI), such as mindfulness-based relapse prevention (MBRP; 78, 79). These types of treatment programs target the experiences of craving and negative affect. In addition, MBI is directly aimed at treating the experiential avoidance observed in these patients, improving their metacognitive capacities (80–83).
Conclusions
This study provides greater understanding about the role of ER in GD. On one hand, our results suggest greater severity of GD among individuals with high ER deficits and in younger individuals. On the other hand, ER deficits are higher in men and older individuals. No differences in ER strategies based on gambling preference (strategic vs. non-strategic) were found. Future research should focus on exploring ER and other related constructs such as alexithymia, as well as on developing treatments that target difficulties in these aspects. Therefore, this study has been carried out through a statistical variable–centered approach, focused on the etiological objective of explaining the relationships and the underlying mechanisms between ER and gambling severity. Future research based on alternative and complementary statistical procedures such as person-centered approaches (e.g., mixture models or cluster analysis) should focus on identifying the dynamics of emergent therapeutic needs based on the categorizing of individuals into common subgroups based on substantive variables (such as ER domains) and on understanding the pattern of relationships of these empirical latent clusters with predictors, correlates, and therapy outcomes.
Data Availability
All datasets generated for this study are included in the manuscript and the supplementary files.
Ethics Statement
This study was carried out in accordance with the latest version of the Declaration of Helsinki. The Ethics Committee of the University Hospital of Bellvitge approved the study and written informed consent was obtained and signed from all final participants.
Author Contributions
MS, SJ-M, IS, RG, and JMM were in charge of research project elaboration. MS, SJ-M, IS, and RG were in charge of organization. MS, SJ-M, IS, and RG were in charge of design. MS, MG, RG, NM-B, GM-B, AP-G, TM-M, CV-A, TS, NA, MG-P, and SJ-M were in charge of execution. Writing of the first draft was done by MS. Review and critique were done by MS, SJ-M, IS, JT, SG-S, and FF-A.
Funding
This manuscript and research were supported by grants from the Instituto de Salud Carlos III (ISCIII) and cofounded by the FEDER funds/European Regional Development Fund (ERDF), a way to build Europe. CIBERobn and CIBERsam are initiatives of ISCIII. This work was also supported by the Ministerio de Economía y Competitividad (PSI2015-68701-R) and by the Delegación del Gobierno para el Plan Nacional sobre Drogas(2017I067).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00625/full#supplementary-material
References
1. Williams AD, Grisham JR, Erskine A, Cassedy E. Deficits in emotion regulation associated with pathological gambling. Br J Clin Psychol (2012) 51:223–38. doi: 10.1111/j.2044-8260.2011.02022.x
2. Kober H. Emotion regulation in substance use disorders. In: Gross JJ, editor. Handbook of emotion regulation., 2nd ed. The Guilford Press (2014). p. 428–46.
3. Estévez A, Herrero FD, Sarabia GI, Jauregui BP. Mediating role of emotional regulation between impulsive behavior in gambling, internet and videogame abuse, and dysfunctional symptomatology in young adults and adolescents. Adicciones (2014) 26(4):282–90. doi: 10.20882/adicciones.26
4. Estévez A, Jáuregui P, Sánchez-Marcos I, López-González H, Griffiths M. Attachment and emotion regulation in substance addictions and behavioral addictions. J Behav Addict (2017) 6(4):534–44. doi: 10.1556/2006.6.2017.086
5. Elmas HG, Cesur G, Oral ET. Alexithymia and pathological gambling: the mediating role of difficulties in emotion regulation. Turk J Psychiatry (2017) 28(1):17–24. doi: 10.5080/u13779
6. Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol (1998) 2(3):271–99. doi: 10.1037/1089-2680.2.3.271
7. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess (2004) 26(1):41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
8. Rogier G, Velotti P. Conceptualizing gambling disorder with the process model of emotion regulation. J Behav Addict (2018) 7(2):239–51. doi: 10.1556/2006.7.2018.5
9. Noël X, Saeremans M, Komreich C, Bechara A, Jaafari N, Fantini-Hauwel C. On the processes underlying the relationship between alexithymia and gambling severity. J Gambl Stud (2018) 34(4):1049–66. doi: 10.1007/s10899-017-9715-1
10. Parker JD, Wood LM, Bond BJ, Shaughnessy P. Alexithymia in young adulthood: a risk factor for pathological gambling. Psychother Psychosom (2005) 74:51–5. doi: 10.1159/000082027
11. Toneatto T, Lecce J, Bagby M. Alexithymia and pathological gambling. J Addict Disord (2009) 28:193–8. doi: 10.1080/10550880903014775
12. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. (2013). Washington, DC: American Psychiatric Association
13. Blaszczynski A, Nower L. A pathways model of problem and pathological gambling. Addiction (2002) 97:487–99. doi: 10.1046/j.1360-0443.2002.00015.x
14. Moon M, Lister JJ, Milosevic A, Ledgerwood DM. Subtyping non–treatment-seeking problem gamblers using the pathways model. J Gambl Stud (2017) 33(3):841–53. doi: 10.1007/s10899-016-9658-y
15. Granero R, Fernández-Aranda F, Mestre-Bach G, Steward T, García-Caro B, Prever F, et al. Clustering of treatment-seeking women with gambling disorder. J Behav Addict (2018) 7(3):770–80. doi: 10.1556/2006.7.2018.93
16. Sheppes G, Suri G, Gross JJ. Emotion regulation and psychopathology. Ann Rev Clin Psychol (2015) 11:379–405. doi: 10.1146/annurev-clinpsy-032814-112739
17. Lumley MA, Roby KJ. Alexithymia and pathological gambling. Psychother Psychosom (1995) 63:2001–206. doi: 10.1159/000288960
18. Grant JE, Kim SW. Gender differences in pathological gamblers seeking medication treatment. Compr Psychiatry (2002) 43(1):56–62. doi: 10.1053/comp.2002.29857
19. Álvarez-Moya EM, Jiménez-Murcia S, Granero R, Vallejo J, Krug I, Bulik CM, et al. Comparison of personality risk factors in bulimia nervosa and pathological gambling. Compr Psychiatry (2007) 48(5):452–7. doi: 10.1016/j.comppsych.2007.03.008
20. Orlowski S, Bischof A, Besser B, Bischof G, Rumpf HJ. Deficits in emotion regulation strategies among problematic and pathological gamblers in a sample of vocational school students. J Behav Addict (2019) 8(1):94–102. doi: 10.1556/2006.7.2018.136
21. Di Trani M, Renzi A, Vari C, Zavattini GC, Solano L. Gambling disorder and affect regulation: the role of alexithymia and attachment style. J Gambl Stud (2017) 33:649–59. doi: 10.1007/s10899-016-9637-3
22. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev (2010) 30(2):217–37. doi: 10.1016/j.cpr.2009.11.004
23. Kassel JD, Veilleux JC, Heinz AJ, Braun AR, Conrad M. Emotions and addictive processes. Chapter 22. In: Miller P, editor. Principles of Addiction, 1st edn, vol. I, San Diego; London; Walthan: Elsevier (2013) p. 213–22.
24. McCormick RA, Taber JI. Attributional style in pathological gamblers in treatment. J Abnormal Psychol (1988) 97(3):368–70. doi: 10.1037/0021-843X.97.3.368
25. Bonnaire C, Bungener C, Varescon I. Subtypes of French pathological gamblers: comparison of sensation seeking, alexithymia and depression scores. J Gambl Stud (2009) 28:455–71. doi: 10.1007/s10899-009-9142-z
26. Bonnaire C, Barrault S, Aïte A, Cassotti M, Moutier S, Varescon I. Relationship between pathological gambling, alexithymia and gambling type. Am J Addict (2017) 26:152–60. doi: 10.1111/ajad.12506
27. Odlaug BL, Marsh PJ, Kim SW, Grant JE. Strategic vs. nonstrategic gambling: characteristics of pathological gamblers based on gambling preference. Ann Clin Psychiatry (2011) 23:105–12.
28. Lesieur HR. Cluster analysis of types of inpatient pathological gamblers. Dissertation Abstracts International (2001) 62:2065.
29. Ledgerwood DM, Petry NM. Subtyping pathological gamblers based on impulsivity, depression, and anxiety. Psychol Addict Behav (2010) 24(4):680–8. doi: 10.1037/a0019906
30. Larson R, Moneta G, Richards MH, Wilson S. Continuity, stability, and change in daily emotional experience across adolescence. Child Dev (2002) 73:1151–65. doi: 10.1111/1467-8624.00464
31. Riediger M, Wrzus C, Wagner G. Happiness is pleasant, or is it? Representations of affect valence are associated with contra-hedonic motivation and mixed affect in daily life. Emotion (2014) (5):950–61. doi: 10.1037/a0037711
32. Zimmer-Gembeck MJ, Skinner EA. Review: the development of coping across childhood and adolescence: an integrative review and critique of research. Int J Behav Dev (2011) 35:1–17. doi: 10.1177/0165025410384923
33. Phillips LH, Henry JD, Hosie JA, Milne AB. Effective regulation of the experience and expression of negative affect in old age. J Gerontol B: Psychol Sci Soc Sci (2008) 63:138–45. doi: 10.1093/geronb/63.3.P138
34. Kessler E, Staudinger UM. Affective experience in adulthood and old age: the role of affective arousal and perceived affect regulation. Psychol Aging (2009) 24:349–62. doi: 10.1037/a0015352
35. Mroczek DK, Almeida DM. The effect of daily stress, personality and age on daily negative affect. J Pers (2004) 72:355–78. doi: 10.1111/j.0022-3506.2004.00265.x
36. Fischer AH, Manstead ASR. The relation between gender and emotions in different cultures. In: Fischer AH, editor. Gender and emotion: social psychological perspectives. Cambridge Univ. Press (2000). p. 71–94.
37. Tamres LK, Janicki D, Helgeson VS. Sex differences in coping behavior: a meta-analytic review and an examination of relative coping. Pers Soc Psychol Rev (2002) 6:2–30. doi: 10.1207/S15327957PSPR0601_1
38. Granero R, Penelo E, Martínez-Giménez R, Álvarez-Moya E, Gómez-Peña M, Aymamí MN, et al. Sex differences among treatment-seeking adult pathologic gamblers. Compr Psychiatry (2009) 50:173–80. doi: 10.1016/j.comppsych.2008.07.005
39. Jakubczyk A, Trucco EM, Kopera M, Kobylinski P, Suszek H, Fudalej S, et al. The association between impulsivity, emotion regulation, and symptoms of alcohol use disorder. J Subs Abuse Treat (2018) 91:49–56. doi: 10.1016/j.jsat.2018.05.004
40. Tavares H, Zilberman ML, Beites FJ, Gentil V. Gender differences in gambling progression. J Gambl Stud (2001) 17(2):151–9. doi: 10.1023/A:1016620513381
41. Hing N, Russell A, Tolchard B, Nower L. Risk factors for gambling problems: an analysis by gender. J Gambl Stud (2016) 32(2):511–34. doi: 10.1007/s10899-015-9548-8
42. McIntosh CC, Crino RD, O’Neill K. Treating problem gambling samples with cognitive behavioural therapy and mindfulness-based interventions. Clin Trial J Gambl Stud (2016) 32(4):1305–25. doi: 10.1007/s10899-016-9602-1
43. Sancho M, De Gracia M, Rodríguez RC, Mallorquí-Bagué N, Sánchez-González J, Trujols J, et al. Mindfulness-based interventions for the treatment of substance and behavioral addictions: a systematic review. Front Psychiatry (2018) 9:95. doi: 10.3389/fpsyt.2018.00095
44. Tárrega S, Castro-Carreras L, Fernández-Aranda F, Granero R, Giner-Bartolomé C, Aymamí N, et al. A serious videogame as an additional therapy tool for training emotional regulation and impulsivity control in severe gambling disorder. Front Psychol (2015) 6:1721. doi: 10.3389/fpsyg.2015.01721
45. Stinchfield R. Reliability, validity, and classification accuracy of a measure of DSM-IV diagnostic criteria for pathological gambling. Am J Psychiatry (2003) 160(1):180–2. doi: 10.1176/appi.ajp.160.1.180
46. Jiménez-Murcia S, Stinchfield R, Alvarez-Moya E, Jaurrieta N, Bueno B, Granero R, et al. Reliability, validity, and classification accuracy of a Spanish translation of a measure of DSM-IV diagnostic criteria for pathological gambling. J Gambl Stud (2009) 25:93–104. doi: 10.1007/s10899-008-9104
47. Hervás G, Jódar R. Adaptación al castellano de la Escala de Dificultades en la Regulación Emocional. Clin y Salud (2008) 9:139–56.
48. Jiménez-Murcia S, Alvarez-Moya EM, Stinchfield R, Fernández-Aranda F, Granero R, Aymamí MN, et al. Age of onset in pathological gambling: clinical, therapeutic and personality correlates. J Gambl Stud (2010) 26(2):235–48. doi: 10.1007/s10899-009-9175-3
50. Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess (1994) 6(4):284–90. doi: 10.1037/1040-3590.6.4.284
51. Kelley K, Preacher KJ. On effect size. Psychol Methods (2012) 17(2):137–52. doi: 10.1037/a0028086
52. Finner H. On a monotonicity problem in step-down multiple test procedures. J Am Stat Assoc (1993) 88:920–3. doi: 10.2307/2290782
53. Barrett P. Structural equation modelling: adjudging model fit. personality and individual differences. (2007) 42: (5):815–24. doi: 10.1016/j.paid.2006.09.018
54. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol (2003) 85(2):348–62. doi: 10.1037/0022-3514.85.2.348
55. Barrett L, Bliss-Moreau E. She’s emotional. He’s having a bad day: attributional explanations for emotion stereotypes. Emotion (2009) 9:648–58. doi: 10.1037/a0016821
56. Nolen-Hoeksema S. Emotion regulation and psychopathology: the role of gender. Ann Rev Clin Psychol (2012) 8:161–87. doi: 10.1146/annurev-clinpsy-032511-143109
57. Hyde JS, Mezulis AH, Abramson LY. The ABCs of depression: integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychol Rev (2008) 115:291–313. doi: 10.1037/0033-295X.115.2.291
58. Nolen-Hoeksema S, Aldao A. Gender and age differences in emotion regulation strategies and their relationship to depressive symptoms. Pers Individ Differs (2011) 51:704–8. doi: 10.1016/j.paid.2011.06.012
59. Ciarrochi J, Hynes K, Crittenden N. Can men do better if they try harder: sex and motivational effects on emotional awareness. Cogn Emot (2005) 19:133–41. doi: 10.1080/02699930441000102
60. Zahn-Waxler C, Shirtcliff EA, Marceau K. Disorders of childhood and adolescence: gender and psychopathology. Ann Rev Clin Psychol (2008) 4:275–303. doi: 10.1146/annurev.clinpsy.3.022806.091358
61. Joseph DL, Newman DA. Emotional intelligence: an integrative meta-analysis and cascading model. J Appl Psychol (2010) 95:54–78. doi: 10.1037/a0017286
62. Zarbatany L, McDougall P, Hymel S. Gender-differentiated experience in the peer culture: links to intimacy in preadolescence. Soc Dev (2000) 9:62–79. doi: 10.1111/1467-9507.00111
63. Rose AJ. Co-rumination in the friendships of girls and boys. Child Dev (2002) 73:1830–43. doi: 10.1111/1467-8624.00509
64. Rose AJ. Structure, content, and socioemotional correlates of girls’ and boys’ friendships. Merrill-Palmer Q (2007) 53:489–506. doi: 10.1353/mpq.2007.0019
65. Brummer L, Stopa L, Bucks R. The influence of age on emotion regulation strategies and psychological distress. Behav Cognit Psychother (2013) 42:1–14. doi: 10.1017/S1352465813000453
66. Rogier G, Velotti P. Narcissistic implications in gambling disorder: the mediating role of emotion dysregulation. J Gambl Stud (2018) 34:1241–60. doi: 10.1007/s10899-018-9759-x
67. Myrseth H, Brunborg G, Eidem M. Differences in cognitive distortions between pathological and non-pathological gamblers with preferences for chance or skill games. J Gambl Stud (2010) 26(4):561–9. doi: 10.1007/s10899-010-9180-6
68. Lourains FK, Dowling NA, Enticott PG, Bradshaw JL, Trueblood JS, Stout JC. Strategic and non-strategic problem gamblers differ on decision-making under risk and ambiguity. Addiction (2014) 109:1128–37. doi: 10.1111/add.12494
69. Moragas L, Granero R, Stinchfield R, Fernández-Aranda F, Fröberg F, Aymamí N, et al. Comparative analysis of distinct phenotypes in gambling disorder based on gambling preferences. BMC Psychiatry (2015) 15:1–11. doi: 10.1186/s12888-015-0459-0
70. Gourdriaan AE, Slutske WS, Krull JL, Sher KJ. Longitudinal patterns of gambling activities and associated risk factors in college students. Addiction (2009) 104:1219–32. doi: 10.1111/j.1360-0443.2009.02573.x
71. Stevens M, Young M. Who plays what? Participation profiles in chance versus skill-based gambling. J Gambl Stud (2010) 26:89–103. doi: 10.1007/s10899-009-9143-y
72. Granero R, Penelo E, Stinchfield R, Fernández-Aranda F, Savvidou LG, Fröberg F, et al. Is pathological gambling moderated by age? J Gambling Stud (2014) 30:475–92. doi: 10.1007/s10899-013-9369-6
73. Bonnaire C, Bungener C, Varescon I. Alexithymia in pathological gambling: a risk factor for all gamblers? J Gambl Stud (2013) 29:83–96. doi: 10.1007/s10899-012-9297-x
74. Atkinson J, Sharp C, Schmitz J, Yaroslavsky I. Behavioral activation and inhibition, negative affect, and gambling severity in a sample of young adult college students. J Gambl Stud (2012) 28(3):437–49. doi: 10.1007/s10899-011-9273-x
75. Sauvaget A, Jiménez-Murcia S, Fernández-Aranda F, Fagundo AB, Moragas L, Wolz I, et al. Unexpected online gambling disorder in late-life: a case report. Front Psychol (2015) 6:655. doi: 10.3389/fpsyg.2015.00655
76. Toneatto T, Vettese L, Nguyen L. The role of mindfulness in the cognitive–behavioural treatment of problem gambling. J Gambl Issues (2017) 19:91–100. doi: 10.4309/jgi.2007.19.12
77. de Lisle SM, Dowling NA, Allen JS. Mindfulness and problem gambling: a review of the literature. J Gambl Stud (2012) 28:719–39. doi: 10.1007/s10899-011-9284-7
78. Bowen S, Chawla N, Collins SE, Witkiewitz K, Hsu S, Grow J, et al. Mindfulness-based relapse prevention for substance use disorders: a pilot efficacy trial. Subst Abuse (2009) 30(4):295–305. doi: 10.1080/08897070903250084
79. Bowen S, Chawla N, Marlatt GA. Mindfulness-based relapse prevention for addictive behaviors: a clinician’s guide. New York: Guilford Press (2010).
80. Riley B. Experiential avoidance mediates the association between thought suppression and mindfulness with problem gambling. J Gamb Stud (2014) 30:163–71. doi: 10.1007/s10899-012-9342-9
81. Jáuregui P, Urbiola I, Estévez A. Metacognition in pathological gambling and its relationship with anxious and depressive symptomatology. J Gambl Stud (2016) 32:675–88. doi: 10.1007/s10899-015-9552-z
82. Pietrzak RH, Morasco BJ, Blanco C, Grant BF, Petry NM. Gambling level and psychiatric and medical disorders in older adults: results from the national epidemiologic survey on alcohol and related conditions. Am J Geriatric Psychiatry (2007) 15(4):301–13. doi: 10.1097/01.JGP.0000239353.40880.cc
Keywords: behavioral addiction, emotion regulation, gambling disorder, risk, severity, age, gender
Citation: Sancho M, de Gracia M, Granero R, González-Simarro S, Sánchez I, Fernández-Aranda F, Trujols J, Mallorquí-Bagué N, Mestre-Bach G, del Pino-Gutiérrez A, Mena-Moreno T, Vintró-Alcaraz C, Steward T, Aymamí N, Gómez-Peña M, Menchón JM and Jiménez-Murcia S (2019) Differences in Emotion Regulation Considering Gender, Age, and Gambling Preferences in a Sample of Gambling Disorder Patients. Front. Psychiatry 10:625. doi: 10.3389/fpsyt.2019.00625
Received: 17 April 2019; Accepted: 05 August 2019;
Published: 11 September 2019.
Edited by:
Qinghua He, Southwest University, ChinaReviewed by:
Damien Brevers, Free University of Brussels, BelgiumPatrizia Velotti, University of Genoa, Italy
Copyright © 2019 Sancho, de Gracia, Granero, González-Simarro, Sánchez, Fernández-Aranda, Trujols, Mallorquí-Bagué, Mestre-Bach, del Pino-Gutiérrez, Mena-Moreno, Vintró-Alcaraz, Steward, Aymamí, Gómez-Peña, Menchón and Jiménez-Murcia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Sancho, bXNhbmNob25hQHNhbnRwYXUuY2F0; Susana Jiménez-Murcia, c2ppbWVuZXpAYmVsbHZpdGdlaG9zcGl0YWwuY2F0