
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 13 March 2019
Sec. Psychological Therapy and Psychosomatics
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00090
This article is part of the Research Topic Reducing the Mortality Gap in People with Severe Mental Disorders: The Role of Lifestyle Psychosocial Interventions View all 19 articles
 Marco Herbsleb1,2
Marco Herbsleb1,2 Katriona Keller-Varady3
Katriona Keller-Varady3 Thomas Wobrock4
Thomas Wobrock4 Alkomiet Hasan5
Alkomiet Hasan5 Andrea Schmitt5,6
Andrea Schmitt5,6 Peter Falkai5
Peter Falkai5 Holger Horst Werner Gabriel2
Holger Horst Werner Gabriel2 Karl-Jürgen Bär1
Karl-Jürgen Bär1 Berend Malchow1*
Berend Malchow1*People with schizophrenia die on average 15–20 years earlier than age and gender matched controls in the general population. An essential part of this excess mortality in people with schizophrenia is caused by physical illnesses. Among the physical illnesses, cardiovascular disease (CVD) has been identified as the most common natural cause of death in up to 40–45% of the cases. Chronotropic incompetence (CI) is defined as the inability of the heart to increase its beating frequency in proportion to increased physical activity or higher metabolic demand. It is an established independent cardiovascular risk factor for major cardiac events and overall mortality and might explain adaptation intolerance of the cardiovascular system to even minor exercise courses. CI needs objective exercise testing for definitive diagnosis and therefore represents a biological marker indicating the integrity of the cardiovascular system. It was recently described in patients with schizophrenia and might help explain the reduced physical fitness in these patients and the inability of a subgroup of patients to benefit from exercise interventions. In this study, we tried to replicate the occurrence of CI in an independent sample of patients with schizophrenia and evaluated whether CI can be influenced by a continuous endurance training of 12 weeks. Therefore, we re-analyzed the fitness testing data of 43 patients with schizophrenia and 22 aged and gender matched healthy controls. Parameters of aerobic fitness and chronotropic response to exercise were calculated. Patients with schizophrenia were less physically fit than the healthy controls and displayed a significantly higher heart rate at rest. 10 of 43 patients with schizophrenia and no healthy control subject were classified as chronotropically incompetent. Chronotropic response to exercise did not change significantly after 12 weeks of continuous aerobic exercise training. No differences were observed for baseline heart rate and peak heart rate in both subgroups of schizophrenia patients. Aerobic fitness did not improve significantly in the patients with schizophrenia classified as chronotropically incompetent. Our results confirm the occurrence of CI in patients with multi-episode schizophrenia. This should be taken into account when planning an exercise or lifestyle intervention studies in this population. Schizophrenia patients with CI do not seem to benefit as well as schizophrenia patients without CI from aerobic exercise training interventions. Larger, prospective randomized controlled clinical trials with different training interventions are urgently needed to address the topic of schizophrenia patients not responding to exercise and the relationship to the illness itself.
There is a solid body of evidence underpinning the notion that people with schizophrenia die on average 15–20 years earlier than age and gender matched controls in the general population (1–3). This mortality gap between the general population and patients with schizophrenia seems to increase instead of converge over the last decades (4–6). An essential part of this excess mortality in people with schizophrenia is caused by physical illnesses (7–9). In several studies, cardiovascular disease (CVD) has been identified as the most common natural cause of death in up to 40–45% of cases (7, 10). It has been suggested that coronary heart disease is the main contributor to CVD, which is exacerbated by the high-risk profile (obesity, poor diet, lack of exercise, smoking) of most patients with schizophrenia. In addition, patients with schizophrenia take antipsychotic medication on a regular basis, which is known to affect the cardiovascular system additionally (11). Some of the risk factors are potentially reversible by changing the lifestyle and even by considering side effects of some antipsychotics. A non-pharmacological interventional approach to impact cardiovascular risk factors is regular physical exercise (12, 13). As mentioned above, studies have shown that people with severe mental illness like schizophrenia engage in significantly more sedentary behavior and significantly less physical activity compared to healthy controls (14). Additionally to somatic health benefits, aerobic exercise positively impacts core features of the disease itself like cognitive deficits (15–17) and negative symptoms (18). However, although the above-mentioned risk factors seem to be plausible they do not explain the excess mortality of patients with schizophrenia satisfactorily. Moreover, psychiatrists and researchers seem to overlook to some extend the solid body of evidence describing cardiovascular dysregulation in patients with schizophrenia both at rest and during physical activity. It has been shown that young unmedicated patients with schizophrenia show increased heart rates at rest caused by severe autonomic dysfunction (19). An increase in heart rate of 5 beats per minute corresponds to a significant increase in the atherosclerosis progression (20). Life expectancy in animals and humans shows a close relation to the medium heart rate (21). Increased resting heart rate has been shown to be a risk factor for reduced life expectancy in both the general population (22, 23) and in populations with cardiovascular diseases (24, 25). In patients with schizophrenia, the protective vagal component seems to be profoundly impaired leading to reduced heart rate variability or an insensitive baroreflex. While similar findings have been described in patients with depression (26), alcohol withdrawal (27), or anxiety disorders (28) the pronounced degree of changes leads to a unique pattern in patients with schizophrenia. Most of the described alterations in the autonomic nervous system are associated with reduced life expectancy previously shown in various conditions such as diabetes (29), survival after myocardial infarction (30, 31) or in cardiac artery disease (CAD) (32). Thus, more research is needed to better explain cardiovascular dysregulation in schizophrenia because in contrast to patients suffering from severe CAD the cardiac autonomic dysfunction in schizophrenia is not caused by structural or functional alterations of the heart itself but moreover by abnormalities in the brain—heart interaction (33).
More recently, we investigated the putative link between autonomic dysfunction and physical incapacity in these patients. And indeed, Herbsleb et al. (34) were able to present evidence that about half of the tested population of patients with schizophrenia showed a strikingly absent heart rate acceleration during physical exercise. This phenomenon is called chronotropic incompetence of the heart (CI) and was again described in various cardiac conditions (35–38). It is defined as the inability of the heart to increase its beating frequency in proportion to the increase in physical activity or higher metabolic demand and therefore needs an exercise testing of the patients for definitive diagnosis (37). This finding is of paramount importance since CI is a well-described cardiac risk factor of mortality (39–43), it is associated with physical incapacity and might explain to some extend that patients with schizophrenia encounter difficulties to enjoy physical activities. However, this new finding warrants further studies to identify patients at risk and to investigate treatment options.
Therefore, the aim of the current investigation was to examine if the previously revealed impaired heart rate response to physical exercise is a consistent finding, which can be also detected in a further cohort of patients with schizophrenia. Here, we used a different exercise test protocol in order to elucidate the possibility to include data from various studies and to generalize findings. In addition, we evaluated, whether heart rate responses to exercise can be influenced by a moderate-intensity continuous endurance training of 12 weeks in our patients.
We hypothesized that (i) our re-analysis of fitness testing data would reveal CI in a substantial portion of patients with multi-episode schizophrenia, (ii) that CI is again related to reduced physical fitness in this subset of patients, and (iii) that an continuous aerobic exercise training ameliorates or reverses the CI of the heart in the subset of schizophrenia patients affected.
The evaluated cohort consisted of forty-three multi-episode schizophrenia patients and twenty-two healthy controls who successfully completed an interventional, single center continuous aerobic exercise study which took place at the Department of Psychiatry and Psychotherapy at the University Medical Center Göttingen between 2010 and 2013 (44–48). The local ethics committee approved the study protocol, which was in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to inclusion in the study. The trial was registered at www.clinicaltrials.gov (NCT01776112). Briefly, 43 patients with multi-episode schizophrenia and 22 healthy controls were assessed for endurance capacity using an incremental exercise test on a bicycle ergometer before and after the study intervention. The study intervention consisted of standardized continuous endurance training on cycle ergometers three times a week for 30 min over a total intervention period of 12 weeks. A group of 21 patients with schizophrenia played table soccer (also known as foosball is the US) as an additional active control intervention. Healthy controls were matched regarding age and gender to patients in the endurance group (see Table 1). Inclusion criteria were a diagnosis of schizophrenia according to ICD-10, stable psychopathology and antipsychotic medication for 2 weeks prior to the intervention and age between 18 and 60 years. Exclusion criteria were substance abuse (alcohol and illicit drugs (cannabis, amphetamines, cocaine, benzodiazepines, and opioids) assessed with urine drug tests), a worsening of psychopathological symptoms within 2 weeks of the screening period, pregnancy, lactation, or contraindications for endurance training or maximal cardiopulmonary exercise testing (CPET).
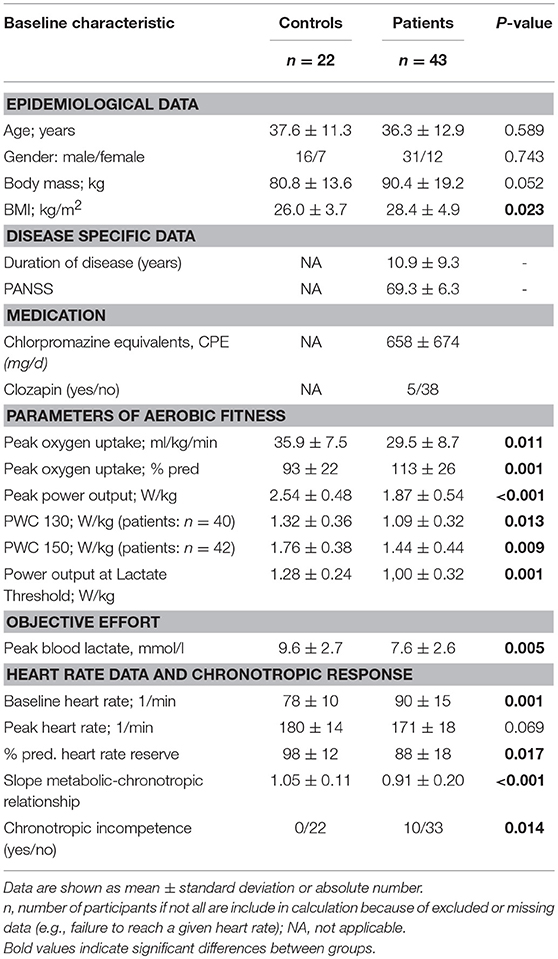
Table 1. Baseline characteristics as well as parameters of aerobic fitness in the control and patient group.
In order to measure aerobic endurance capacity before and after the 12-week intervention, participants performed incremental CPET until subjective exhaustion on an electronically braked bicycle ergometer (Ergoselect 200 K, Ergoline GmbH, Bitz, Germany). After a resting period of 3 min, the incremental bicycle protocol started at a power output of 25, 50, or 75 W on the basis of the anamnestic information for 3 min. The power output was then increased in steps of 25 W every 3 min until the subject reached his or her limit of tolerance. During the CPET, ventilatory indices and gas exchanges and heart rate were measured continuously on a breath-by-breath basis using an automatic mobile wireless ergospirometer (MetaMax 3B, Cortex, Biophysik GmbH, Leipzig, Germany, and T31, Polar Electro Oy, Kempele, Finland). Before each test, the turbine (flow and volume) was calibrated with a syringe (Hans Rudolph Inc., Kansas City). For data analysis, the breath-by-breath gas exchange and ventilatory data were smoothed using a 15-breath moving average, aligned to the time of the central breath. Peak oxygen consumption (VO2peak) was defined as the highest value of 15-breath average occurring during CPET. Capillary whole-blood samples of 0.2 μl were obtained for lactate measurements from the ear lobe when the patient was at rest, and again at the end of the third minute of each 3-min period of the CPET. The blood lactate concentrations were measured by Lactate SCOUT Solo Plus, SensLab GmbH, Leipzig, Germany).
A set of different physiological maximal and submaximal indices was used to describe the aerobic fitness. We calculated the power output at a fixed heart rate of 130 and 150 (known as physical working capacity; PWC 130, PWC 150), as well as the power output at the Lactate Threshold (LT), which are both submaximal indices of aerobic fitness. The time course of lactate was graphically interpolated using an equalizing spline procedure. The LT was defined as the minimum lactate equivalent (the lowest value of the quotient lactate to power output) as describes the first sustained increase in blood lactate concentration above resting level during incremental exercise (49). The evaluation of the LT and the power output achieved at a blood lactate concentrations of 2 mmol/l (for training prescription) were done examiner independent by using a software for performance diagnostic (Ergonizer, Germany, www.ergonizer.de). Moreover, we determined the achieved peak power output (Ppeak) and peak oxygen uptake (VO2peak). More details for the calculation of the PWC, VO2peak, and Ppeak are given in Keller-Varady et al. (45).
The interventions in the patients with schizophrenia consisted of a 12-week training procedure. Participants participated in three training sessions per week lasting exactly 30 min each. The sessions consisted of moderate-intensity endurance training on cycle ergometers. The exercise intensity was set to the individual power output achieved at a blood lactate concentrations of 2 mmol/l, determined during the preceding CPET. Power output was than increased gradually, corresponding to improvements in endurance performance, by a mean of 8 ± 1 % after 11 ± 6 training sessions, controlled by lactate concentration monitoring.
To assess chronotropic response, the metabolic-chronotropic relationship (MCR; also known as the chronotropic index) was calculated according to (50) using the ratio of heart rate reserve (predicted HRpeak (220—age)—HR at rest) to metabolic reserve (VO2peak—VO2 at rest) during the CPET. The MCR adjusts for age, physical fitness and functional capacity and is unaffected by the exercise protocol as well as effort-independent (37). The increase in percentage heart rate reserve in relation to the increase in percentage metabolic reserve (also known as oxygen uptake reserve) was obtained by linear regression analysis using the least squares method of the mean values acquired for VO2 and HR data in the last 30 s of each incremental step of the CPET. In healthy adults, the percentage of heart rate reserve achieved during exercise equals the percentage of metabolic reserve achieved, so that the median MCR slope is near around 1.0 with a 95% confidence interval between 0.8 and 1.3 (50).
For statistical analysis, SPSS for Mac (version 25.0.0.1) was used. All parameters were tested for normal distribution with the Kolmogorov–Smirnov test or with Shapiro-Wilk-Test by subgroup analysis. Epidemiological data and objective effort during exercise testing of patients and controls as well as subgroups of patients (CI vs. non CI patients) were compared by either using parametric or non-parametric two-sample tests as well as Chi-squared tests for comparison of nominal data. To investigate basic differences of aerobic fitness and heart rate parameters between all patients and controls, we performed two separate multivariate analyses of variance (MANOVAs). We conducted a first MANOVA for aerobic fitness parameters with the inter-subject factor GROUP (patients vs. controls) including VO2peak, Ppeak, PWC 130, PWC 150, as well as LT (all normalized to body mass) followed-up by univariate analysis of variances (ANOVAs). The second MANOVA for all participants was performed by applying the factor GROUP (patients vs. controls) and included the following heart rate parameters: baseline heart rate, peak heart rate, and percentage of the predicted heart rate reserve (% pred. heart rate reserve). ANOVAs were then calculated for single parameters. To investigate the main hypothesis of our study, the metabolic–chronotropic relationship slope (MCR slope) of patients and controls was analyzed. Controls and patients with a MCR slope below the cut-off value of 0.8 were referred as chronotropic incompetent whereas subjects with a MCR slope above a value of 0.8 were classified as chronotropic competent (50). Group differences of the MCR slope between patients and controls were verified with a parametric two-sample t-test. We repeated a MANOVA with respect to physical fitness for the factor SUBGROUP (CI vs. nonCI patients) followed-up by univariate ANOVAs. Due to the influence of chronotropic incompetence on the heart rate derived fitness indices PWC 130 and PWC 150, we abstained form including these parameters in the analysis. The effects of the continuous aerobic endurance training on aerobic fitness indices (including VO2peak, Ppeak, PWC 130, PWC 150, and LT) in subgroups of patients (CI vs. nonCI) were examined using the dependent sample t-test or the Wilcoxon matched pairs signed rank test as the nonparametric alternative. We applied the same procedure to investigate the effects of training MCR-slope in CI and non-CI patients. The significance level was set 0.05 (two-sided) and fitted using Bonferroni adjustment procedure to account for inflation of alpha level by multiple testing.
The MANOVA for aerobic fitness indices (VO2peak, Ppeak, PWC 130, PWC 150, LT) revealed a significant difference [F(5, 56) = 5.66; P < 0.001] between all schizophrenia patients and healthy controls. The follow-up univariate ANOVAs indicated significant differences for VO2peak (F = 6.93; P < 0.05), Ppeak (F = 21.84; P < 0.001), PWC 130 (F = 6.57; P < 0.05), PWC 150 (F = 7.35; P < 0.01 and LT (F = 11.38; P < 0.01; see Table 1).
The second MANOVA for heart rate parameters revealed a significant effect for the factor GROUP [F(3, 61) = 6.45; P < 0.01]. As depicted in Table 1, the ANOVAs showed significant differences between all patients and controls for baseline heart rate (F = 11.60, p < 0.01) and percentage of predicted heart rate reserve (F = 6.02, P < 0.05), whereas only a trend was found for peak heart rate (F = 3.42, P < 0.069).
Based on cut-off values by Burbaker and Kitzman, (37) and Wilkoff and Miller, (50), 10 of 43 patients with schizophrenia had an impaired heart rate response to exercise and were classified as chronotropically incompetent, whereas no healthy control subject was below the cut-off value. Furthermore, a significant difference was observed between the mean MCR slopes of patients and controls (P < 0.001, see Table 1 and Figure 1). The MANOVA that compared aerobic fitness indices (VO2peak, Ppeak, and LT) between subgroups of patients (CI vs. nonCI patients) revealed no significant difference between groups [F(3, 39) = 1.76; P = 0.170] (see Table 2 and Figure 2).
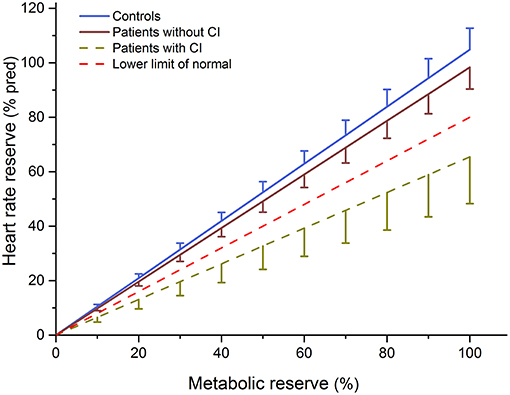
Figure 1. Mean ± 90% confidence limit of the metabolic–chronotropic relationship of patients with (CI) and without (non-CI) chronotropic incompetence as well as control subjects. The dotted line represents the lower limit of normal (slope < 0.8).
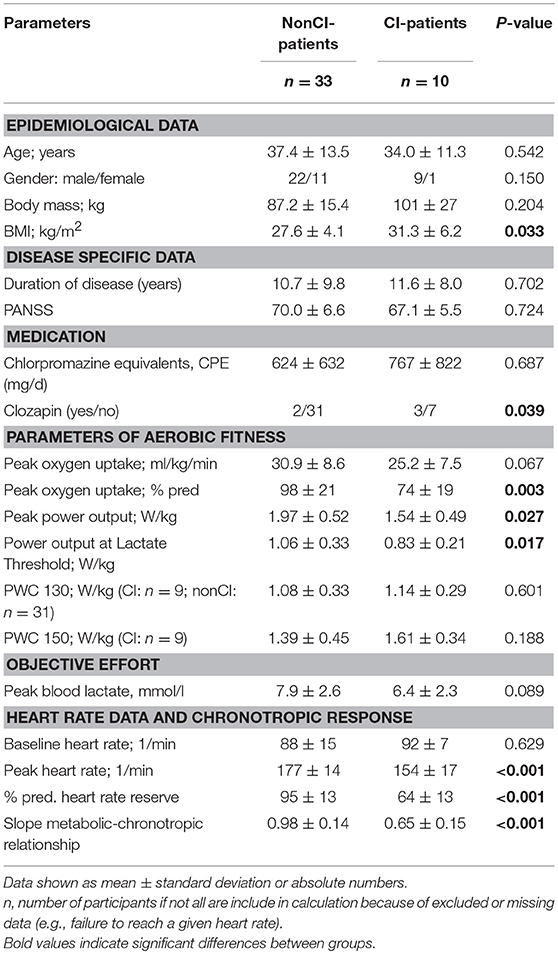
Table 2. Baseline characteristics as well as parameters of aerobic fitness in patients with schizophrenia with (SZ-CI) and without chronotropic incompetence (SZ-nonCI).
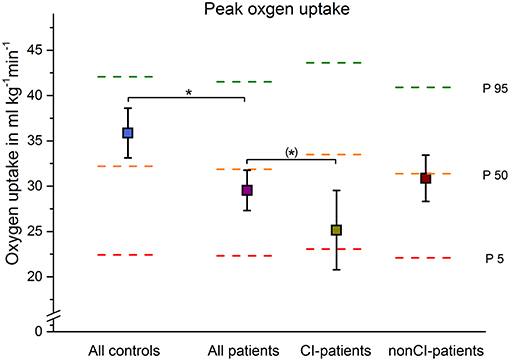
Figure 2. Mean ± 90% confidence limit of peak oxygen uptake of all patients, and patients with (CI) and without (non-CI) chronotropic incompetence are depicted in comparison to controls. The dotted horizontal lines represent contemporary age, gender, and body size specific reference percentiles (51). Significant or a trend differences are indicated by *p < 0.05 or (*) p < 0.1, respectively.
The MCR-slope as an index of chronotropic response to exercise did not change significantly in both, the CI and the non-CI subgroup after 12 weeks of continuous aerobic exercise training compared to baseline (see Table 3). Furthermore, no differences were observed for baseline heart rate and peak heart rate in both groups.
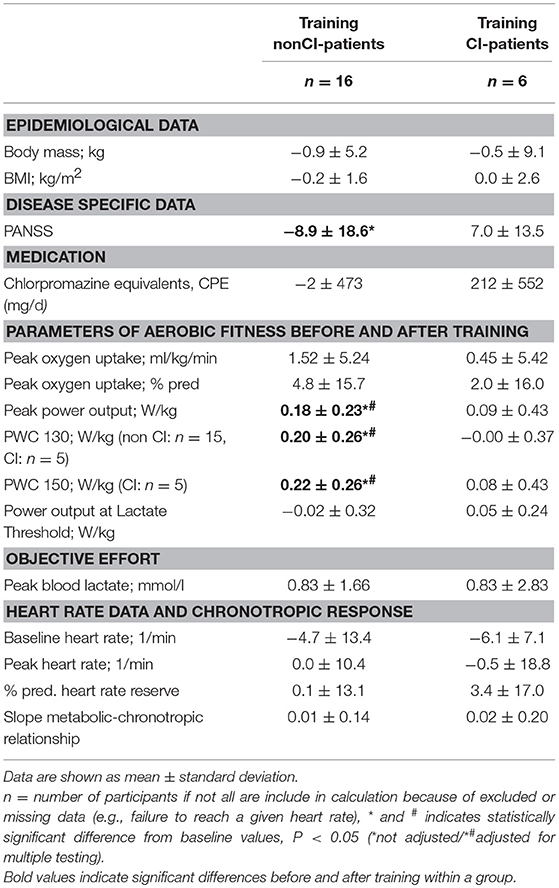
Table 3. Differences to baseline in disease specific data, indices of aerobic fitness, and heart rate data after a 12-week moderate-intensity aerobic training in patients without (SZ-nonCI) and with (SZ-CI) chronotropic incompetence.
Of the 22 schizophrenia patients who underwent the 12-week continuous aerobic exercise training intervention, 6 were classified as chronotropic incompetent based on the MCR-Slope as described above. The epidemiological data, aerobic fitness and heart rate parameters are highlighted in Table 3. Aerobic fitness improved significantly (as indicated by Ppeak, PWC 130, PWC 150) in the non-CI group, but contrary to our initial hypothesis it did not change significantly in the CI-group (see Table 3). However, no significant responses to training in both groups were observed for VO2peak and LT.
Our study shows in agreement with previous reports that healthy controls show better fitness levels than patients with schizophrenia, despite being age and gender matched and engaging in no sports 2 years before entering the study (45). In addition, this study confirmed in 10 out of 43 patients the pattern of chronotropic incompetence in patients with schizophrenia and thus corroborates the first description in the disease although studied in a different fitness test design. Most intriguingly, we did not observe a significant impact of a twelve-week moderate continuous exercise training on CI values in patients.
In the present study, we identified impaired chronotropic responses with a step-wise incremental exercise test in contrast to the ramp-wise protocol used in the previous study by Herbsleb et al. (34). However, in this independent sample only 23% of the multi-episode patients with schizophrenia showed CI. This is lower than in our previous study where the proportion of SZ-CI consisted of 43% (34). The difference to higher share of CI cases in our previous study may relate to the composition of groups rather than other causes given the small sample size. It seems not plausible that the cause of the higher occurrence of CI in the study of Herbsleb et al. (34) is mainly explained by the different exercise test protocols that were used. Although the ramp-wise protocol results in lower mean HR as well as VO2 values at the common power output than step-wise tests [(52), the impact of the test protocol on the MCR slope (which is the relationship of HR and VO2 values) is considered to be negligible. A variety of exercise testing protocols and modes of testing have been used to evaluates the MCR relationship (37) since the originally description by Wilkoff and Miller (50), that used a step-wise incremental treadmill exercise test. However, in order to adequately assess the chronotropic response to metabolic stress of exercise the following points should be considered in future study designs: (i) participants should be encouraged to exercise until the subject reaches his or her limit of tolerance, (ii) exhaustion levels should be objectively evaluated by either measuring blood lactate values or the respiratory exchange ratio (ratio of carbon dioxide output to oxygen uptake), (iii) a sophisticated gas-exchange analysis is needed or specific test protocols (e.g., Bruce treadmill protocol, Chronotropic Assessment Exercise Protocol) should be applied and iv) a step-wise incremental exercise test with stage durations ≥3 min is recommended to obtain a near steady-state heart rate and to satisfy the equations conditions.
Since CI is known to be a cardiac risk factor larger trials might even elucidate possible clinical key factors associated with CI. To date, we were unable to find a substantial difference between CI and non-CI patients with respect to psychopathology, body mass index, duration of disease or the prescribed medication (see Table 1). However, it should be noted that patients taking clozapine were not included in the first analysis and the putative influence of clozapine on cardiovascular regulation should be investigated separately in future studies.
Various pathophysiological mechanisms have been proposed leading to chronotropic incompetence in cardiac conditions. For instance, Bristow and colleagues found a 50% or greater reduction in β-adrenergic receptor density in the left ventricular myocardium of failing hearts explanted during transplant surgery (53). These and other findings suggest that in heart failure patients, a decrease in β-receptor density leads to a diminished sensitivity of the β-adrenergic pathway and a decrease in β-agonist–stimulated muscle contractility. We would like to speculate that the long lasting augmented sympathetic drive might lead to a reduction of β-receptor density in patients with schizophrenia. In addition, we cannot exclude that the chronic stress of a multi-episode disease such as schizophrenia might be associated with reduced excretion of catecholamines during an exercise bout. Although we have not observed a difference between both patient groups with respect to medication (34), we cannot completely exclude that anti-dopaminergic activity of some antipsychotics might influence the acute stress response. Since the definite pathophysiology of schizophrenia remains unclear, concepts of neuroinflammation and specifically autoimmune encephalitis or autoimmune psychosis have again gained more ground recently (54–57). However, the definite contribution is still discussed controversially, especially in those cases with no neurological symptoms (58). For the diagnosis of Autoimmune-Encephalitis clinical, imaging and CSF criteria have been proposed (59). Autoimmune antibodies are known to cause autonomic dysfunction in a lot of diseases like Sjögren syndrome or Guillain–Barré syndrome but also in conditions called pure autonomic failure (60). To the best of our knowledge the patients with multi-episode schizophrenia included in this study showed no yellow or red signs pointing to autoimmune etiology (61). Nevertheless, autoimmune antibodies were not studied specifically in the cerebrospinal fluid prior to inclusion in the study and hence cannot be ruled out to cause or promote autonomic dysfunction, here described as CI, in a subgroup of the patients. Nevertheless, CI could be a relatively easy to obtain objective biological marker to study the conjunction with inflammation pathways. Thus, this should be elucidated in further studies in this field and shift the focus on pathophysiological mechanisms to understand regulatory problems in patients with schizophrenia. This might help to decrease some obstacles impeding patients to engage in physical activities on a regular basis and to benefit from it (62). If CI is of importance in a substantial subset of patients with schizophrenia then one needs to think about other routines to accustom patients with schizophrenia to regular physical activity.
It is therefore intriguing that 12 weeks of continuous aerobic exercise training had no impact on CI measures in this study and that patients with multi-episode schizophrenia and CI did not benefit from the regular aerobic exercise in terms of fitness parameters or heart rate at rest. More studies are urgently needed to learn how to modulate the cardiac risk factor CI in patients with schizophrenia. One needs to consider different exercise protocols, longer durations of exercise and adjustments as well as an optimal assessment of CI in the first place. In addition, we need to learn the influence of antipsychotic medication on CI. Especially promising might be the application of high intensity training, which seems to be feasible in patients with schizophrenia (63–66). Herbsleb et al. (67) showed in an case report that a 6-week high intensity training improved autonomic function substantially while no such effect was observed after 6 weeks of continuous training in a patient with schizophrenia. Most intriguingly, the previously observed pattern of autonomic dysfunction returned after 6 weeks of detraining. This study underlines the importance of the choice of the training method as well the introduction of long-lasting training concepts in psychiatry.
Some limitations need to be taken into account. This is an exploratory secondary analysis of the fitness testing results of previously published data (44–46). Though the initial study protocol (44) was not primarily designed to reveal CI it contained thorough fitness testing [executed by a trained sports scientist (KKV)] to objectively assess cardiovascular fitness levels in the included patients with schizophrenia before and after the exercise intervention. However, the obtained data allowed us to calculate the metabolic-chronotropic relationship and hence CI post-hoc. As outlined above, the presence of CI can detected regardless the protocol (continuous or step-wise increase of the workload) during formal exercise testing and a variety of exercise testing protocols can be used (37, 52). This is of high interest when re-analyzing fitness testing data of existing exercise studies to shed more light on the phenomenon of exercise intolerance in patients with schizophrenia and to determine to which extend CI might be a contributing factor. The sample size is relatively small, especially those of SZ-CI that underwent 12 weeks of continuous aerobic exercise training.
Our results confirm the occurrence of CI in patients with multi-episode schizophrenia. Thorough fitness testing is necessary to reveal CI, but it does not seem to make a difference if the workload during the test is raised continuously or stepwise every 3 min. This should be taken into account when planning an exercise or lifestyle intervention study in patients with schizophrenia. Further studies are also needed to confirm CI in a prospective sample of patients with schizophrenia and to examine the underlying pathology of CI in patients with schizophrenia, i.e., by performing additional structural and functional examinations of the heart, as CI might rely to a specific cardiovascular pathophysiology in patients with schizophrenia. Furthermore, schizophrenia patients with CI do not seem to benefit as well as schizophrenia patients without CI from moderate continuous aerobic exercise training interventions, which may explain mixed results in this population in the literature. Larger, prospective randomized controlled clinical trials with different training interventions are urgently needed to address the topic of schizophrenia patients not responding to exercise and the relationship to the illness itself.
MH analyzed the data and wrote the first draft of the study. KK-V designed and performed the study and critically analyzed the data. TW, AH, and AS designed the study, gave critical comments, and revised the first draft of the study. PF and BM designed and performed the study, critically analyzed the data, gave critical comments, and revised the first draft of the study. HHWG gave critical comments and critically analyzed the data. K-JB designed the study, gave critical comments, critically analyzed the data, and revised the first draft of the study.
We would like to express our sincere thanks to the family of Mrs. Ricarda Maucher for their generous financial support. KK-V was supported by the Dorothea Schlözer Program at the University of Göttingen. This work was partially supported by the Deutsche Forschungsgemeinschaft (1950/5-1 to PF). This research was funded by the grants Klinische Forschergruppe (KFO) 241 and PsyCourse (FA241/16-1) from the Deutsche Forschungsgemeinschaft (DFG) to PF. Further funding was received from the German Federal Ministry of Education and Research (BMBF) through the research network on psychiatric diseases ESPRIT (grant number 01EE1407E) to PF, AH, and AS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Tiihonen J, Lonnqvist J, Wahlbeck K, Klaukka T, Niskanen L, Tanskanen A, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet. (2009) 374:620–7. doi: 10.1016/S0140-6736(09)60742-X
2. Bushe CJ, Taylor M, Haukka J. Mortality in schizophrenia: a measurable clinical endpoint. J Psychopharmacol. (2010) 24:17–25. doi: 10.1177/1359786810382468
3. Chang CK, Hayes RD, Perera G, Broadbent MT, Fernandes AC, Lee WE, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE. (2011) 6:e19590. doi: 10.1371/journal.pone.0019590
4. Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch. General Psychiatry. (2007) 64:1123–31. doi: 10.1001/archpsyc.64.10.1123
5. Lawrence D, Hancock KJ, Kisely S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: retrospective analysis of population based registers. BMJ. (2013) 346:f2539. doi: 10.1136/bmj.f2539
6. Saha S, Whiteford H, McGrath J. Modelling the incidence and mortality of psychotic disorders: data from the second Australian national survey of psychosis. Aust N Z J Psychiatry. (2014) 48:352–9. doi: 10.1177/0004867413513341
7. Ringen PA, Engh JA, Birkenaes AB, Dieset I, Andreassen OA. Increased mortality in schizophrenia due to cardiovascular disease - a non-systematic review of epidemiology, possible causes, and interventions. Front Psychiatry. (2014) 5:137. doi: 10.3389/fpsyt.2014.00137
8. Olfson M, Gerhard T, Huang C, Crystal S, Stroup TS. Premature mortality among adults with schizophrenia in the United States. JAMA Psychiatry. (2015) 72:1172–81. doi: 10.1001/jamapsychiatry.2015.1737
9. Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. (2017) 16:163–80. doi: 10.1002/wps.20420
10. Hennekens CH, Hennekens AR, Hollar D, Casey DE. Schizophrenia and increased risks of cardiovascular disease. Am Heart J. (2005) 150:1115–21. doi: 10.1016/j.ahj.2005.02.007
11. Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med. (2009) 360:225–35. doi: 10.1056/NEJMoa0806994
12. Lavie CJ, Thomas RJ, Squires RW, Allison TG, Milani RV. Exercise training and cardiac rehabilitation in primary and secondary prevention of coronary heart disease. Mayo Clin Proc. (2009) 84:373–83. doi: 10.1016/S0025-6196(11)60548-X
13. Pagels P, Raustorp A, Archer T, Lidman U, Alricsson M. Influence of moderate, daily physical activity on body composition and blood lipid profile in Swedish adults. J Phys Act Health. (2012) 9:867–74. doi: 10.1123/jpah.9.6.867
14. Vancampfort D, Firth J, Schuch FB, Rosenbaum S, Mugisha J, Hallgren M, et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: a global systematic review and meta-analysis. World Psychiatry. (2017) 16:308–15. doi: 10.1002/wps.20458
15. Firth J, Cotter J, Elliott R, French P, Yung AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. 45:1343–61. doi: 10.1017/S0033291714003110
16. Falkai P, Malchow B, Schmitt A. Aerobic exercise and its effects on cognition in schizophrenia. Curr Opin Psychiatry. (2017) 30:171–5. doi: 10.1097/YCO.0000000000000326
17. Firth J, Stubbs B, Rosenbaum S, Vancampfort D, Malchow B, Schuch F, et al. Aerobic exercise improves cognitive functioning in people with schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2017) 43:546–56. doi: 10.1093/schbul/sbw115
18. Dauwan M, Begemann MJ, Heringa SM, Sommer IE. Exercise improves clinical symptoms, quality of life, global functioning, and depression in schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2016) 42:588–99. doi: 10.1093/schbul/sbv164
19. Bär KJ. Cardiac autonomic dysfunction in patients with schizophrenia and their healthy relatives - A small review. Front Neurol. (2015) 6:139. doi: 10.3389/fneur.2015.00139
20. Caetano J, Delgado Alves J. Heart rate and cardiovascular protection. Eur J Intern Med. (2015) 26:217–22. doi: 10.1016/j.ejim.2015.02.009
21. Boudoulas KD, Borer JS, Boudoulas H. Heart Rate, Life Expectancy and the Cardiovascular System: therapeutic considerations. Cardiology. (2015) 132:199–212. doi: 10.1159/000435947
22. Greenland P, Daviglus ML, Dyer AR, Liu K, Huang CF, Goldberger JJ, et al. Resting heart rate is a risk factor for cardiovascular and noncardiovascular mortality: the Chicago Heart Association Detection Project in Industry. Am J Epidemiol. (1999) 149:853–62. doi: 10.1093/oxfordjournals.aje.a009901
23. Jensen MT, Suadicani P, Hein HO, Gyntelberg F. Elevated resting heart rate, physical fitness and all-cause mortality: a 16-year follow-up in the Copenhagen Male Study. Heart. (2013) 99:882–7. doi: 10.1136/heartjnl-2012-303375
24. Diaz A, Bourassa MG, Guertin MC, Tardif JC. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur Heart J. (2005) 26:967–74. doi: 10.1093/eurheartj/ehi190
25. Jensen MT, Kaiser C, Sandsten KE, Alber H, Wanitschek M, Iversen A, et al. Heart rate at discharge and long-term prognosis following percutaneous coronary intervention in stable and acute coronary syndromes–results from the BASKET PROVE trial. Int J Cardiol. (2013) 168:3802–6. doi: 10.1016/j.ijcard.2013.06.034
26. Koschke M, Boettger MK, Schulz S, Berger S, Terhaar J, Voss A, et al. Autonomy of autonomic dysfunction in major depression. Psychosom Med. (2009) 71:852–60. doi: 10.1097/PSY.0b013e3181b8bb7a
27. Jochum T, Hoyme J, Schulz S, Weissenfels M, Voss A, Bär KJ. Diverse autonomic regulation of pupillary function and the cardiovascular system during alcohol withdrawal. Drug Alcohol Depend. (2016) 159:142–51. doi: 10.1016/j.drugalcdep.2015.12.030
28. Yeragani VK, Chokka P, Tancer M, Sivaraju A, Bär KJ. Increased beat-to-beat 'R' amplitude variability in patients with panic disorder. Int J Cardiol. (2010) 143:431–2. doi: 10.1016/j.ijcard.2008.12.003
29. Vinik AI, Casellini C, Parson HK, Colberg SR, Nevoret ML. Cardiac autonomic neuropathy in diabetes: a predictor of cardiometabolic events. Front Neurosci. (2018) 12:591. doi: 10.3389/fnins.2018.00591
30. Savonen KP, Lakka TA, Laukkanen JA, Rauramaa TH, Salonen JT, Rauramaa R. Usefulness of chronotropic incompetence in response to exercise as a predictor of myocardial infarction in middle-aged men without cardiovascular disease. Am J Cardiol. (2008) 101:992–8. doi: 10.1016/j.amjcard.2007.11.045
31. Waks JW, Buxton AE. Risk stratification for sudden cardiac death after myocardial infarction. Annu Rev Med. (2018) 69:147–64. doi: 10.1146/annurev-med-041316-090046
32. Fioranelli M, Bottaccioli AG, Bottaccioli F, Bianchi M, Rovesti M, Roccia MG. Stress and Inflammation in Coronary Artery Disease: a review psychoneuroendocrineimmunology-based. Front Immunol. (2018) 9:2031. doi: 10.3389/fimmu.2018.02031
33. Bär KJ, Boettger MK, Berger S, Baier V, Sauer H, Yeragani VK, et al. Decreased baroreflex sensitivity in acute schizophrenia. J Appl Physiol. (2007) 102:1051–6. doi: 10.1152/japplphysiol.00811.2006
34. Herbsleb M, Schumann A, Malchow B, Puta C, Schulze PC, Gabriel HW, et al. Chronotropic incompetence of the heart is associated with exercise intolerance in patients with schizophrenia. Schizophr Res. (2018). 197:162–9. doi: 10.1016/j.schres.2018.02.020
35. Clark AL, Coats AJ. Chronotropic incompetence in chronic heart failure. Int J Cardiol. (1995) 49:225–31. doi: 10.1016/0167-5273(95)02316-O
36. Roche F, Pichot V, Da Costa A, Isaaz K, Costes F, Dall'Acqua T, et al. Chronotropic incompetence response to exercise in congestive heart failure, relationship with the cardiac autonomic status. Clin Physiol. (2001) 21:335–42. doi: 10.1046/j.1365-2281.2001.00328.x
37. Brubaker PH, Kitzman DW. Chronotropic incompetence: causes, consequences, and management. Circulation. (2011) 123:1010–20. doi: 10.1161/CIRCULATIONAHA.110.940577
38. Magri D, Agostoni P, Sinagra G, Re F, Correale M, Limongelli G, et al. Clinical and prognostic impact of chronotropic incompetence in patients with hypertrophic cardiomyopathy. Int J Cardiol. (2018) 271:125–31. doi: 10.1016/j.ijcard.2018.04.019
39. Ellestad MH. Chronotropic incompetence. The implications of heart rate response to exercise (compensatory parasympathetic hyperactivity?) Circulation. (1996) 93:1485–7. doi: 10.1161/01.CIR.93.8.1485
40. Lauer MS, Okin PM, Larson MG, Evans JC, Levy D. Impaired heart rate response to graded exercise. Prognostic implications of chronotropic incompetence in the Framingham Heart Study. Circulation. (1996) 93:1520–6. doi: 10.1161/01.CIR.93.8.1520
41. Lauer MS, Francis GS, Okin PM, Pashkow FJ, Snader CE, Marwick TH. Impaired chronotropic response to exercise stress testing as a predictor of mortality. JAMA. (1999) 281:524–9. doi: 10.1001/jama.281.6.524
42. Elhendy A, Mahoney DW, Khandheria BK, Burger K, Pellikka PA. Prognostic significance of impairment of heart rate response to exercise: impact of left ventricular function and Myocardial ischemia. J Am Coll Cardiol. (2003) 42:823–30. doi: 10.1016/S0735-1097(03)00832-5
43. Azarbal B, Hayes SW, Lewin HC, Hachamovitch R, Cohen I, Berman DS. The incremental prognostic value of percentage of heart rate reserve achieved over myocardial perfusion single-photon emission computed tomography in the prediction of cardiac death and all-cause mortality: superiority over 85% of maximal age-predicted heart rate. J Am Coll Cardiol. (2004) 44:423–30. doi: 10.1016/j.jacc.2004.02.060
44. Malchow B, Keller K, Hasan A, Dorfler S, Schneider-Axmann T, Hillmer-Vogel U, et al. Effects of endurance training combined with cognitive remediation on everyday functioning, symptoms, and cognition in multiepisode schizophrenia patients. Schizophr Bull. (2015) 41:847–58. doi: 10.1093/schbul/sbv020
45. Keller-Varady K, Hasan A, Schneider-Axmann T, Hillmer-Vogel U, Adomssent B, Wobrock T, et al. Endurance training in patients with schizophrenia and healthy controls: differences and similarities. Eur Arch Psychiatry Clin Neurosci. (2016) 266:461–73. doi: 10.1007/s00406-015-0651-8
46. Malchow B, Keeser D, Keller K, Hasan A, Rauchmann BS, Kimura H, et al. Effects of endurance training on brain structures in chronic schizophrenia patients and healthy controls. Schizophr Res. (2016) 173:182–91. doi: 10.1016/j.schres.2015.01.005
47. Papiol S, Popovic D, Keeser D, Hasan A, Schneider-Axmann T, Degenhardt F, et al. Polygenic risk has an impact on the structural plasticity of hippocampal subfields during aerobic exercise combined with cognitive remediation in multi-episode schizophrenia. Transl Psychiatry. (2017) 7:e1159. doi: 10.1038/tp.2017.131
48. Roeh MB, Levold K, Labusga M, Keller-Varady K, Schneider-Axmann T, Hasan A, et al. Effects of three months of aerobic endurance training on motor cortical excitability in schizophrenia patients and healthy subjects. Neuropsychobiology. (2018) 12:1–8. doi: 10.1159/000489714
49. Dickhuth HH, Huoneker M, Münzel T, Drexler H, Berg A, Keul J. Individual anerobic threshold for evaluation of competitive athletes and patients with left ventricular dysfunction. In: Bachl N, Graham TE, Löllgen H, editors. Advances in Ergometry, (Berlin Heidelberg: Springer) (1991) p. 173–9.
50. Wilkoff BL, Miller RE. Exercise testing for chronotropic assessment. Cardiol Clin. (1992) 10:705–17. doi: 10.1016/S0733-8651(18)30211-X
51. Koch B, Schaper C, Ittermann T, Spielhagen T, Dorr M, Volzke H, et al. Reference values for cardiopulmonary exercise testing in healthy volunteers: the SHIP study. Eur Respir J. (2009) 33:389–97. doi: 10.1183/09031936.00074208
52. Zuniga JM, Housh TJ, Camic CL, Bergstrom HC, Traylor DA, Schmidt RJ, et al. Metabolic parameters for ramp versus step incremental cycle ergometer tests. Appl Physiol Nutr Metab. (2012) 37:1110–7. doi: 10.1139/h2012-098
53. Bristow MR, Hershberger RE, Port JD, Gilbert EM, Sandoval A, Rasmussen R, et al. Beta-adrenergic pathways in nonfailing and failing human ventricular myocardium. Circulation. (1990) 82:I12–25.
54. Bogerts B, Winopal D, Schwarz S, Schlaaff K, Dobrowolny H, Mawrin C, et al. Evidence of neuroinflammation in subgroups of schizophrenia and mood disorder patients: a semiquantitative postmortem study of CD3 and CD20 immunoreactive lymphocytes in several brain regions. Neurol. Psychiatry Brain Res. (2017) 23:2–9. doi: 10.1016/j.npbr.2016.11.001
55. Cai HQ, Catts VS, Webster MJ, Galletly C, Liu D, O'Donnell M, et al. Increased macrophages and changed brain endothelial cell gene expression in the frontal cortex of people with schizophrenia displaying inflammation. Mol Psychiatry. (2018). doi: 10.1038/s41380-018-0235-x. [Epub ahead of print].
56. Najjar S, Steiner J, Najjar A, Bechter K. A clinical approach to new-onset psychosis associated with immune dysregulation: the concept of autoimmune psychosis. J Neuroinflammation. (2018) 15:40. doi: 10.1186/s12974-018-1067-y
57. Steiner J, Prüss H, Kohler S, Frodl T, Hasan A, Falkai P. Autoimmune encephalitis with psychosis: warning signs, step-by-step diagnostics and treatment. World J Biol Psychiatry. 4:1–14. doi: 10.1080/15622975.2018.1555376
58. Oviedo-Salcedo T, de Witte L, Kumpfel T, Kahn RS, Falkai P, Eichhorn P, et al. Absence of cerebrospinal fluid antineuronal antibodies in schizophrenia spectrum disorders. Br J Psychiatry. (2018) 212:318–20. doi: 10.1192/bjp.2018.24
59. Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. (2016) 15:391–404. doi: 10.1016/S1474-4422(15)00401-9
60. McKeon A, Benarroch EE. Autoimmune autonomic disorders. Handb Clin Neurol. (2016) 133:405–16. doi: 10.1016/B978-0-444-63432-0.00022-0
61. Herken J, Prüss H. Red Flags: Clinical signs for identifying autoimmune encephalitis in psychiatric patients. Front Psychiatry. (2017) 8:25. doi: 10.3389/fpsyt.2017.00025
62. Firth J, Rosenbaum S, Stubbs B, Gorczynski P, Yung AR, Vancampfort D. Motivating factors and barriers towards exercise in severe mental illness: a systematic review and meta-analysis. Psychol Med. (2016) 46:2869–81. doi: 10.1017/S0033291716001732
63. Heggelund J, Nilsberg GE, Hoff J, Morken G, Helgerud J. Effects of high aerobic intensity training in patients with schizophrenia: a controlled trial. Nord J Psychiatry. (2011) 65:269–75. doi: 10.3109/08039488.2011.560278
64. Heggelund J, Kleppe KD, Morken G, Vedul-Kjelsas E. High aerobic intensity training and psychological States in patients with depression or schizophrenia. Front Psychiatry. (2014) 5:148. doi: 10.3389/fpsyt.2014.00148
65. Engh JA, Andersen E, Holmen TL, Martinsen EW, Mordal J, Morken G, et al. Effects of high-intensity aerobic exercise on psychotic symptoms and neurocognition in outpatients with schizophrenia: study protocol for a randomized controlled trial. Trials. (2015) 16:557. doi: 10.1186/s13063-015-1094-2
66. Wu MH, Lee CP, Hsu SC, Chang CM, Chen CY. Effectiveness of high-intensity interval training on the mental and physical health of people with chronic schizophrenia. Neuropsychiatr Dis Treat. (2015) 11:1255–63. doi: 10.2147/NDT.S81482
Keywords: schizophrenia, exercise, chronotropic incompetence, cardiac autonomic dysfunction, heart rate response
Citation: Herbsleb M, Keller-Varady K, Wobrock T, Hasan A, Schmitt A, Falkai P, Gabriel HHW, Bär K-J and Malchow B (2019) The Influence of Continuous Exercising on Chronotropic Incompetence in Multi-Episode Schizophrenia. Front. Psychiatry 10:90. doi: 10.3389/fpsyt.2019.00090
Received: 24 October 2018; Accepted: 07 February 2019;
Published: 13 March 2019.
Edited by:
Andrea Fiorillo, University of Campania L. Vanvitelli, ItalyCopyright © 2019 Herbsleb, Keller-Varady, Wobrock, Hasan, Schmitt, Falkai, Gabriel, Bär and Malchow. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Berend Malchow, YmVyZW5kLm1hbGNob3dAbWVkLnVuaS1qZW5hLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.