 Jonathan A. Weiss
Jonathan A. Weiss Michelle A. Fardella
Michelle A. Fardella
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 25 May 2018
Sec. Child and Adolescent Psychiatry
Volume 9 - 2018 | https://doi.org/10.3389/fpsyt.2018.00203
This article is part of the Research Topic Comorbidity and Autism Spectrum Disorder View all 33 articles
This study aimed to describe the self-reported experiences of childhood and adult victimization and perpetration in adults with autism spectrum conditions (ASC) compared to a matched sample, and how victimization and perpetration are associated with autism-related difficulties. Forty-five adults with ASC and 42 adults without ASC completed questionnaires regarding violence victimization and perpetration, emotion regulation, and sociocommunicative competence. Participants with ASC reported experiencing, as children, more overall victimization; specifically, more property crime, maltreatment, teasing/emotional bullying, and sexual assault by peers, compared to participants without ASC. Participants with ASC also reported experiencing more teasing/emotional bullying in adulthood and greater sexual contact victimization. No significant differences were found between groups on perpetration. Sociocommunicative ability and emotion regulation deficits did not explain the heightened risk for victimization. Individuals with ASC have an increased vulnerability to violence victimization, which speaks to the need for interventions, and proactive prevention strategies.
Adults with autism spectrum conditions (ASC) may be at considerable risk for interpersonal violence victimization, which refers to violence and abuse that occurs between people, including child maltreatment, intimate partner violence, adolescent dating violence, and bullying (1). Individuals with ASC have a number of impairments in social communication and social interaction across multiple contexts, and exhibit restricted interests and/or repetitive body movements and behaviors (2). The current estimated prevalence of ASC is ~1 in 68, with ~44% having average to above average intellectual abilities (3, 4).
There is a paucity of research examining discrete experiences of interpersonal violence in those with ASC, although what does exist points to an increased risk for child maltreatment, bullying, and sexual victimization (5–7). In children, having an autism diagnosis is associated with an increased chance of physical, emotional, or sexual abuse compared to peers without disabilities (8). More recent research interviewing 182 parents of children with ASC found high rates of reported physical abuse (18.5%), sexual abuse (12.2%), or both kinds (4.4%), though no information on the sources of this abuse was noted (7). Studies have also found high rates of peer victimization in children [65–77%; (6, 9)]. Studies of adults with ASC have largely focused exclusively on sexual victimization. In a college sample, students with ASC were twice as likely to report unwanted sexual contact compared to students without ASC (10). In an online survey, 70% of adults with ASC reported experiencing some form of sexual victimization after age 14 and into adulthood, compared to 45% of those without ASC (5). Authors have suggested that increased risks of bullying, physical, and emotional abuse may also be present in adults with ASC due to heightened social vulnerability (11, 12).
Research has begun to move from an understanding of experiences of interpersonal violence in isolation to understanding the co-occurrence and interconnections between experiences of interpersonal violence, known as polyvictimization, and polyperpetration (13). Too often forms of violence are studied in isolation, and some authors state that focusing on specific forms in isolation may mask the important information that would be gained by studying the complex, varied patterns of traumas (14). Research has yet to examine the broader interpersonal violence experiences of adults with ASC beyond sexual violence victimization, or to look at interpersonal violence perpetration in adults in the community, though what does exist on this latter question suggests no clear association between ASC and violent crime (15–17). Additional research is needed to understand the context of violence across a number of different kinds of acts in adults with ASC.
It is critical to understand the mechanisms that are associated with heightened risk for interpersonal violence (18). Deficits in sociocommunicative competence may be a particular set of risk factors for violence victimization and perpetration in adults with ASC (19, 20). It is well known that individuals with ASC can have challenges with social reasoning, are literal thinkers, and may miss contextual cues (21, 22), and authors have suggested that such sociocommunicative difficulties may be related to an increased risk of sexual abuse (23) and bullying in children with ASC (6). With regard to perpetration, social naivety and misinterpretation of social cues may inadvertently lead to criminal behavior in individuals with ASC, though not specifically to interpersonal violence (24–26). For instance, authors have noted that individuals with ASC inadvertently engage in stalking behaviors when they seek out contact with others for friendship or intimacy [e.g., (27–29)]. No study has tested whether sociocommunicative difficulties explain an increased risk of violence for adults with ASC.
Emotion regulation deficits have also been linked with violence victimization and perpetration in adults in general [e.g., (30)], and may be a particularly salient factor for adults with ASC. In children and adults without ASC, maladaptive emotion regulation is a risk factor for chronic victimization (31, 32). For perpetration, the ability to regulate one's negative emotions may be a factor that helps individuals refrain from initiating violence (33). While difficulties in emotion regulation, emotional expression, and emotion processing have been widely discussed in the ASC literature (34), its link to violence in this population has only been briefly explored, with one study reporting an association among emotion dysregulation and bullying perpetration and victimization in youth (35).
The negative effects of violence are well known in the non-ASC literature (36), and additional efforts to understand the prevalence, characteristics, and causes in adults with ASC are needed. The current study aimed to identify (1) patterns of violence victimization and perpetration in adults with and without ASC across many types, (2) differences in self-reported polyvictimization and polyperpetration, and (3) whether impairments in the areas of sociocommunicative competence and emotion regulation mediate the expected higher rates of violence victimization and perpetration. Self-report was used to gain a reliable estimate of violence victimization and perpetration experiences in adults with ASC living in the community.
Participants with ASC were recruited through study notices distributed by community-based programs and organizations that support those with ASC, online ASC communities, several colleges/universities academic support services, and from study participants to others at their discretion. The comparison group was recruited through postings within the University setting and on community message boards. Advertisements indicated that this was a research project on interpersonal violence in adults that aimed to understand the experiences of interpersonal violence, and that any adult could participate, even if they did not experience violence themselves. Identical recruitment and consent materials were used for both groups. Eligible participants with ASC were required to (a) have a diagnosis of an ASC (e.g., Autism, Asperger Syndrome, Autism Spectrum Disorder, PDD-NOS) according to self-report, which was verified by administering the Autism Diagnostic Observation Schedule-−2nd Edition (37), (b) be 18 years of age or older, and (c) have an estimated IQ above 80 on the Wechsler Abbreviated Scale of Intelligence (38). Participants without ASC had to meet criterion b and c. Equal numbers of men and women with ASC responded to the study advertisements.
The sample included 45 adults with ASC between 18-53 years of age (M = 30.00, SD = 1.48) and 42 adults without ASC, matched on mean chronological age, between 19 and 54 years (M = 32.12, SD = 8.62). Groups did not significantly differ with respect to the percentage of men (42.5% ASC; 50% non-ASC) or on self-identified minority status (15.6% ASC; 31% non-ASC). Participants were also similar in IQ estimates (non-ASC M = 113.33, SD = 16.10, Range 87–146; ASC M = 110.22, SD = 13.19, Range 81–134; t (85) = −0.98, p = 0.36), and in the percentage who obtained at least a college degree (85% ASC; 95% non-ASC). All participants lived in the Greater Toronto Area. Participants in the ASC group reported a diagnosis of ASC and met the clinical cut-off on the ADOS-2 Module 4 (37). Participants without ASC reported that they did not identify with being on the autism spectrum and had never received a diagnosis of an ASC (e.g., autism, Asperger's Syndrome, etc…).
The ADOS-2 (37) is a semi-structured observational measure that examines social and communicative behaviors, and was used to verify ASC status for the ASC group. The ADOS has been found to have good test-retest reliability and excellent internal consistency (37).
The four-subset WASI (38) was administered to obtain a general estimate of intellectual functioning (Full Scale IQ). This measure has been shown to have adequate to high test-retest reliability (r = 0.72–0.95) depending on the subtest, and high internal consistency across groups and subtests (Cronbach's alpha = 0.87–0.98). The WASI has been used in adults with ASC as a brief measure of IQ (39).
The JVQ-AR was used as a measure of childhood victimization, adult victimization, and adult perpetration. The original child victimization version is a 34-item self-report questionnaire that collects information on several forms of childhood victimization (40). The questionnaire assesses the frequency of 34 discrete forms of childhood victimization, scored as a dichotomy (1 = experienced; 0 = not experienced). For childhood victimization, participants are asked about any experiences from birth up until the 18th birthday (0 through 17 years 12 months). The 34 questions fall within six categories: property crime, physical assault, child maltreatment, peer/sibling victimization, sexual victimization, and witnessed/indirect victimization. For adult victimization, a modified version of JVQ-AR was used where participants reported on any of 29 victimization experiences across the same 6 categories, which occurred from their 18th birthday onward. Items that pertained to childhood experiences were removed. Scores are provided for each individual item and each aggregate category. Polyvictimization was computed by summing the endorsed victimization items, with scores ranging from 0 to 34 for childhood victimization, and 0 to 29 for adult victimization [as recommended by (41)], with higher scores indicating a greater number of discrete victimization experiences.
For adult perpetration, a modified version of the JVQ-AR was used where participants were asked about perpetration experiences that occurred from age 18 on. Items pertaining to witnessing violence (e.g., witnessing domestic violence) and child maltreatment (e.g., being bullied by peers) were removed, since the focus of this questionnaire was adulthood and perpetration experiences (i.e., acts committed by the individual during adulthood). Polyperpetration was computed by summing the endorsed perpetration items, with scores ranging from 0 to 19, with higher scores indicating a greater number of discrete acts of violence.
The DERS (42) is a 36-item self-report measure of emotion regulation ability. Subscales assess six dimensions of difficulties: Nonacceptance, Goals, Impulse, Awareness, Strategies, and Clarity. Participants rate how often statements apply to them on a Likert scale with answer categories: 1 = almost never to 5 = almost always. An overall score was used for the current study. Higher scores indicate greater difficulty with emotion regulation. The DERS has been shown to have good internal consistency, test-retest reliability, and construct validity (42–44), and was recently used in a sample of young adults with ASC (45). Internal consistency for the DERS across the whole sample and individual groups demonstrated good to excellent reliability (whole sample α = 0.95, ASC group α = 0.89, no ASC group α = 0.94).
Sociocommunicative competence was measured utilizing the self-report version of the MSCS (46). The MSCS is designed to assess social competence among adolescents and adults with ASC. Psychometric evidence provided preliminary support for the reliability and validity of the scale [Cronbach's alpha reliabilities for domain, subscale, and total scores were all above 0.84; (46)]. The MSCS measures seven domains of social competence: social motivation, social inferencing, demonstrating empathic concern, social knowledge, verbal conversation skills, nonverbal sending skills, and emotion regulation. Participants rated how statements applied to them, where 1 = not true or almost never true, to 5 = very true or almost always true. An overall score was used for the current study, without including emotion regulation (given the use of the DERS). Overall Cronbach's alpha within both groups demonstrated excellent internal consistency (no ASC group α = 0.95, ASC group α = 0.93).
All participants met in person with a trained graduate student. Informed consent was obtained, IQ was assessed, and for those with ASC, the ADOS-2 was completed. Participants were then provided with a laptop computer to complete questionnaires on the online Qualtrics data system (www.qualtrics.com). The University ethics board approved this research. Participants with and without ASC received a gift card to an online retailer for their participation. The informed consent articulated the limits of confidentiality and that participants may have experienced feelings of discomfort generated by the content of the questions asked. A list of support resources were provided to all participants, and they were informed that if they experienced any emotional distress and wanted to speak with a counselor, the researcher would facilitate. One participant with ASC requested this information.
Chi-square analyses and odds ratios were used to examine whether there were differences in the self-report of victimization and perpetration between groups. Due to non-normal data, the Mann Whitney test was calculated to compare groups on self-reported breadth of victimization and perpetration, on sociocommunicative competence, and emotion regulation abilities. Preliminary analyses revealed no differences when comparing men to women in either of the two groups (e.g., men with ASC vs. women with ASC, or men without ASC to women without ASC) on overall polyvictimization or polyperpetration, and on aggregate scores, within either the ASC group or non-ASC group (all p's >.10).
To establish whether self-reported polyvictimization and polyperpetration experiences would be mediated by deficits in sociocommunicative competence and emotion regulation, a test of multiple mediation was run using SPSS INDIRECT macro script for testing multiple mediator models with bootstrapping (47). Given the large age range and concerns that men and women could differ in terms of their experiences of victimization or perpetration, all mediation analyses entered age and sex as control variables (the same analyses were run without these controls and no differences emerged in the pattern of results).
As shown in Table 1, during their childhood, participants with ASC were 6.7 times more likely to report experiencing a form of property crime, largely the result of being more likely to have been robbed than peers without ASC. Those with ASC were 4 times more likely to report experiencing a form of child maltreatment, including physical abuse, and psychological or emotional abuse from adults, 27.1 times more likely to endorse teasing from peers, 3.7 times more likely to endorse bullying from peers, and 7.3 times more likely to endorse sexual assault by a peer, compared to adults without ASC. Participants without ASC were 4.4 times more likely to endorse having sexual relations with someone over 18 than participants with ASC. Participants with ASC reported significantly higher polyvictimization than those without ASC (U = 1204, p = 0.03; ASC M = 12.62, SD = 5.45; no ASC M = 10.05, SD = 7.12).
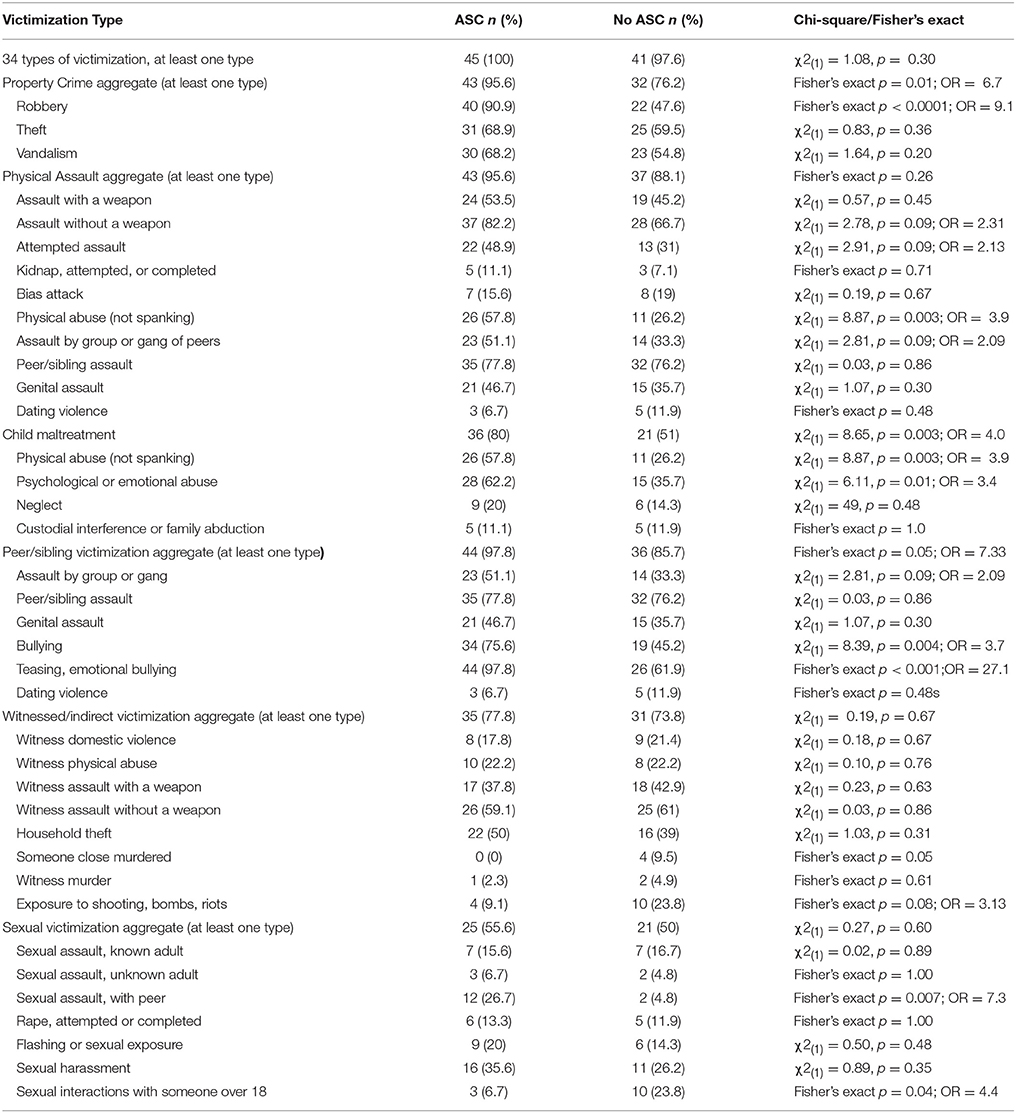
Table 1. Frequency Table for the 34 types of childhood victimization on the JVQ-AR as reported by adults with and without ASC.
As shown in Table 2, participants with ASC were 2.7 times more likely to endorse that they had experienced teasing during adulthood. There was a trend toward those with ASC being more likely to report sexual assault from a known adult, attempted or complete rape, and dating violence. Sexual victimization was further examined in order to separate contact victimization versus noncontact victimization. Sexual assault (by a known adult or unknown adult), and rape (attempted or completed) were summed (resulting in a score of 0–3). Individuals with ASC had significantly higher scores on this composite score than those without ASC (U = 1148.5, p = 0.03; ASC group M = 0.67, SD = 0.93; no ASC group M = 0.29, SD = 0.71) Participants without ASC were 4.4 times more likely to endorse assault with a weapon during adulthood. Participants with ASC did not report greater polyvictimization in adulthood than those without ASC (U = 894, p = 0.66; ASC group M = 6.16, SD = 5.52; no ASC M = 5.95, SD = 4.22).
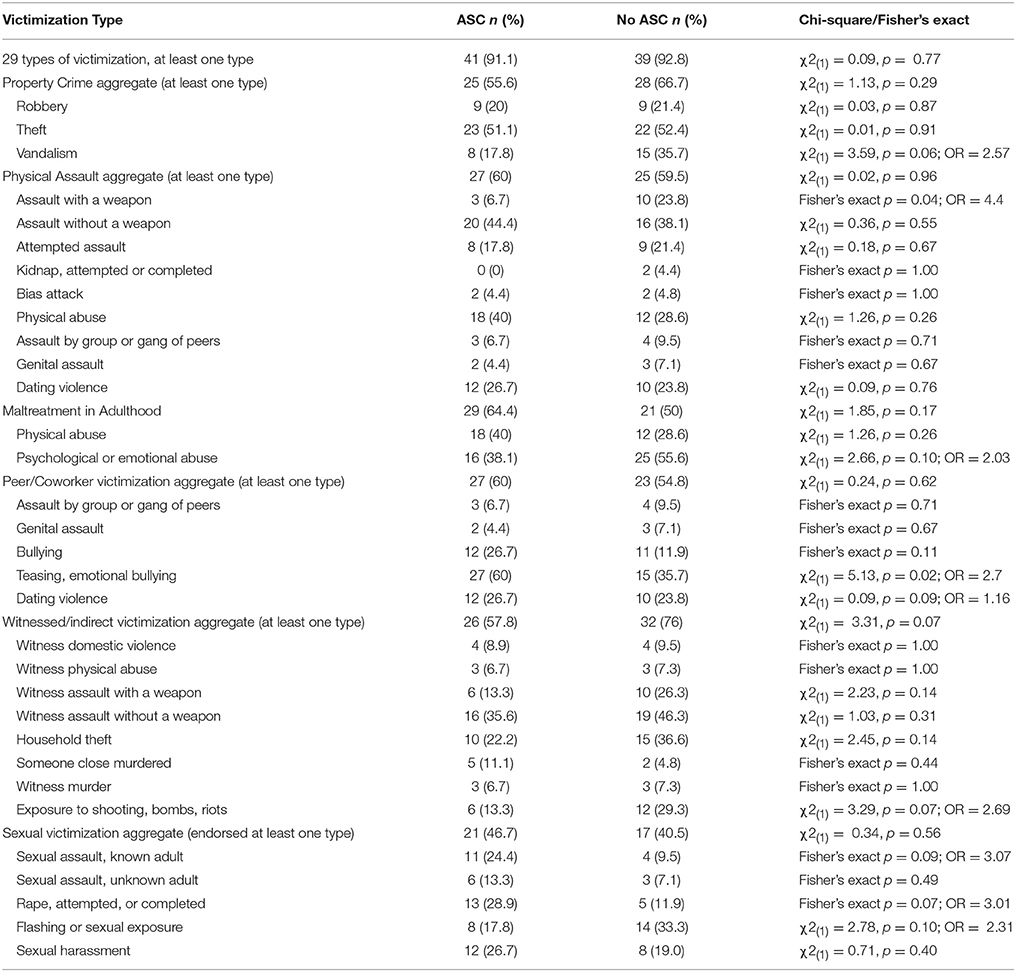
Table 2. Frequency table for the 29 types of adulthood victimization on the modified JVQ-AR as reported by adults with and without ASC.
Table 3 presents the frequencies of endorsing each type and category of perpetration, and the comparisons across groups. No significant differences were found between groups on any form of perpetration, with very low rates reported. Groups did not differ on their polyperpetration score (U = 1006, p = 0.59, ASC group mean = 2.40, SD = 3.02; no ASC group M = 1.90, SD = 2.09).
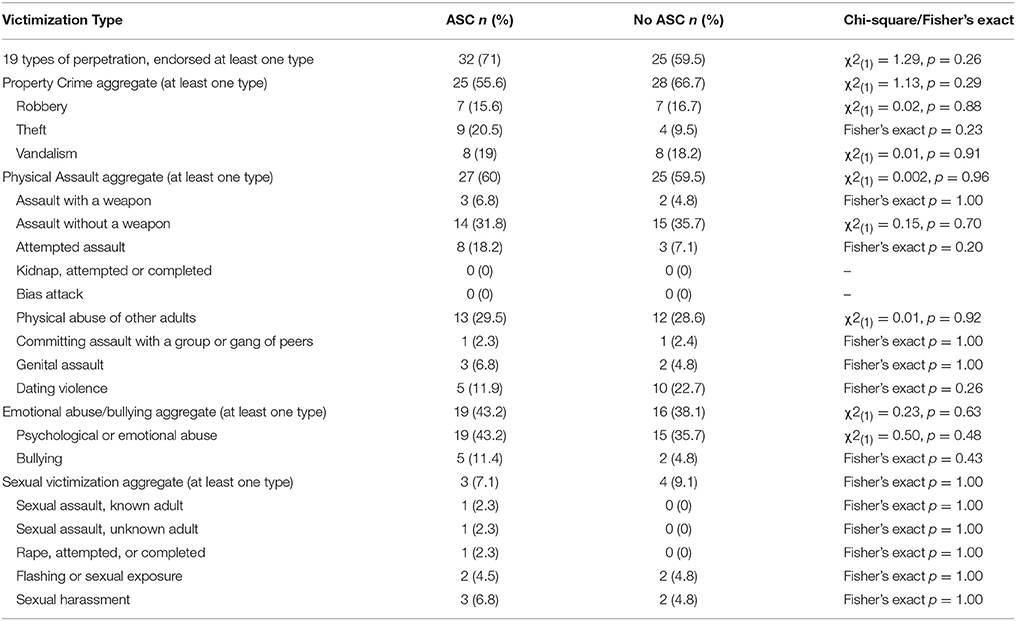
Table 3. Frequency table for the 19 types of adulthood perpetration on the modified JVQ-AR as reported by adults with and without ASC.
As expected, the ASC group reported less developed sociocommunicative competence (ASC M = 3.32, SD = 0.40; no ASC M = 4.05, SD = 0.40; U = 200.00, p < 0.001) and poorer emotion regulation abilities (ASC M = 2.72, SD = 0.57; no ASC M = 1.88, SD = 0.51; U = 200.00, p < 0.001) compared to the comparison group. Neither sociocommunicative competence or emotion regulation were significantly correlated with childhood polyvictimization or adult polyvictimization in the ASC group or the non ASC group (all p's > 0.05). Multiple mediation analyses were used in order to further examine whether emotion regulation and sociocommunicative competence were related to the group differences found in childhood polyvictimization experiences. Table 4 shows the unstandardized coefficients of each pathway, the confidence intervals, and the bootstrapping results based on 1,000 resamples. The total direct effect (path c) of ASC status approached significance before entering the mediator variables, z = 1.95, p = 0.05. The relationship between ASC diagnosis and polyvictimization in childhood was not mediated by sociocommunicative status or emotion regulation. The direction of estimates in the mediator pathways (path a) indicated that having ASC was associated with lower sociocommunicative competence (t = −8.30, p < 0.001), and poorer emotion regulation (t = 7.27, p < 0.001). The total indirect effects did not suggest the presence of mediation, as emotion regulation and sociocommunicative competence were not related to polyvictimization (path b). Mediation analyses were not computed for adult polyvictimization or polyperpetration, as no significant differences were found between groups.
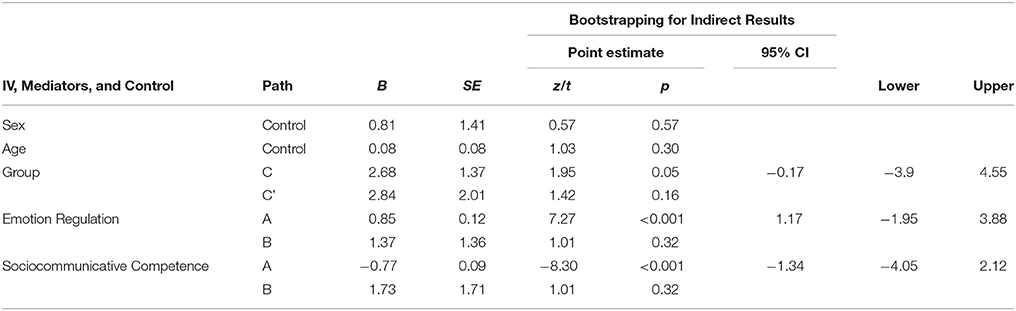
Table 4. Multiple mediation analysis results for the mediating effect of sociocommunicative competence and emotion regulation on the relationship between group and childhood polyvictimization after controlling for sex and age.
This is the first study to explore self-reported experiences of many forms of victimization and perpetration in adults with ASC compared to those without. ~90% of participants with and without ASC reported experiencing at least one form of victimization in childhood, and approximately the same number reported victimization in adulthood. Using the same measure of childhood victimization, other research has found that 97% of college age women (48) and 80% of young adult men and women who had been identified as “at risk for high school drop out” endorse experiencing at least one form of victimization in childhood (36). It appears that using a broad measure of violence experiences, in a broader range of adult ages, results in similar high rates.
Adults with ASC reported a greater breadth of victimization during childhood compared to adults without ASC, matched on sex, IQ, and age. Adults with ASC were more likely to report that as a child, they experienced physical abuse, psychological/emotional abuse from an adult, peer/sibling victimization, various forms of bullying from peers, robbery, and sexual assault by a peer than respondents without ASC. The current research also shows that they are at risk for violence victimization more broadly in childhood. Although the short and long-term impact of victimization, or trauma more broadly, on individuals with ASC is relatively unknown, peer victimization in youth with ASC has been related to internalizing and externalizing symptoms (6, 49), and maltreatment among youth with ASC has been related to externalizing behavior, suicide attempts, conduct and academic problems (7). It is important that childhood victimization in various contexts (home, school, and community) be addressed in order to keep this vulnerable group of youth safe. There is emerging evidence for strength-based school programming to reduce experiences of victimization in general (50), and these programs could be examined for their utility in decreasing victimization for those with ASC.
No differences were found between groups on polyvictimization in adulthood, though differences did emerge in specific kinds. Individuals with ASC were more likely to report experiencing teasing/emotional bullying from other adults, which speaks to a continued risk for interpersonal difficulties with peers across the lifespan. Adults with ASC, whether in the role as an employee or with peers in the community, may benefit from specific training on what constitutes bullying and harassment and how to effectively manage those situations (51). Adults with ASC were also more likely to endorse experiencing some form of sexual victimization that involved contact, including sexual assault and rape, in line with previous research (5). There has been some research advocating for interventions targeting the risk of sexual victimization of individuals with developmental disabilities (52), focusing often on addressing self-protection and assertiveness [e.g., (53)], and education on sexual abuse for support workers (54). In considering how to best reduce the risk of interpersonal violence victimization for adults with ASC, proactive and accessible programming that promotes inclusion and healthy relationships within relevant contexts (including the home, school, workplace, and community levels) are needed.
Groups had similar rates across all forms of perpetration, categories of perpetration, and on polyperpetration, largely due to the equally low endorsements. Low rates were found for both severe and more minor occurrences of violence perpetration. These results map onto the existing reviews finding low rates of perpetration in individuals with ASC and no clear association with violent crime (15, 16). While other studies have examined inpatients, file reviews of incarcerated individuals, or parent/caregiver report, the current study is the first to compare two matched community samples. Researchers and clinicians have cautioned that the sensational and unusual nature of some criminal incidents with individuals with ASC may garner media attention, and perpetuate the notion that individuals with ASC are more violent that individuals without ASC, which is not the case (55). It may be the case that perpetrators with ASC present differently than perpetrators without ASC, with authors describing the links between the symptomology of ASC and offending behaviors (56). These differences will not emerge in examining rates per se, but in the nuances of how perpetration is expressed and the contexts that underlie these behaviors.
Contrary to expectations, sociocommunicative ability and emotion regulation deficits in adults with ASC did not explain a heightened risk for victimization. In fact, neither polyvictimization in childhood or adulthood was correlated with either variable, in either group. In the typical population, many additional factors have been associated with discrete types of victimization (e.g., bullying) and with overall risk, including age, gender, childhood experiences of victimization (emotional/physical/sexual abuse), and mental and physical health problems [e.g., (57–62)], which could be examined in future research. As well, models of victimization largely underscore the important of context, and the dynamics among individual and contextual factors (13). Researchers have begun to study the interplay, and differential impact, of individual and contextual factors, and some have found that contextual factors, such as dangerous neighborhoods, play an important role in adult repeat victimization (63). This study did not consider contextual risk factors for interpersonal violence (e.g., SES, education, family relationships etc.), which may provide a more comprehensive understanding of polyvictimization experiences.
The present study is based on retrospective reporting, which limits any discussion of causality and directionality. Longitudinal design could be used to further examine the pathways that lead to violence victimization and perpetration. Participation was not anonymous, questions were answered in the presence of a researcher, and we did not measure social desirability, making it difficult to know whether participants in either group were under reporting their experiences. We also did not attempt to substantiate reports with other informants, as we sought to understand and value self-reported experiences. Future research could examine both self- and informant-report to examine how responses may be correlated. It is possible that this sample represents a more well-adjusted and functional group of individuals with ASC, and it is unclear whether these results generalize to those who have greater difficulties, as the link between level of functioning and the violence experiences of those with ASC is not well understood. We also did not employ the ADOS-2 to ensure that the comparison group did not have significant symptoms of ASC, though none reported identifying as on the spectrum or being diagnosed with ASC.
This study has both statistical and psychometric limitations. This study was aimed to describe different kinds of victimization and perpetration, and was the first study to apply the JVQ-AR with an adult focus and with respondents with ASC. Alternative measures of violence that are psychometrically validated could provide different results, and are an important endeavor given the current pattern of reported polyvictimization. Additionally, our study had a small sample size and relatively low power for low frequency occurring kinds of victimization or perpetration. There multiple exploratory comparisons do increase the risk of Type I error, and we did not correct for this as a result of the exploratory nature of these comparisons and the relatively small, but important, clinical sample. This remains an important first step to inform future investigations. Finally, this sample of participants had proportionally more women than expected in ASC research, and it is likely that this does not reflect the gender distribution in the population. While the two groups were matched on gender, education level, ethnicity status, age, and IQ, we did not collect or match on other demographics which may differ between groups or be associated with victimization (e.g., employment status, poverty).
Participants with ASC are at considerable risk for experiencing polyvictimization in childhood and for bullying and sexual contact victimization in adulthood. This increased vulnerability to victimization, especially in childhood, highlights the need for intervention and proactive prevention strategies to decrease vulnerability and impact. These findings have serious implications for how we discuss violence victimization, and suggest that understanding interpersonal violence more broadly is critical to ensuring that we identify and target factors that may place people with ASC at risk for many kinds of negative experience.
This study was carried out in accordance with the recommendations of the Canadian Tri-Council Policy Statement Ethical Conduct for Research Involving Human Participants, and the York University Senate Policy, Research Involving Human Participants. The protocol was approved by the York University Human Participants Review (Ethics) Sub-Committee of the Office of Research Ethics. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
MF and JW conceptualized the study, analyzed the data, and contributed to manuscript preparation; MF conducted the recruitment and data collection. All authors agree to be accountable for the content of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank all the participants. JW was funded by the Chair in ASD Treatment and Care Research, funded by the Canadian Institutes of Health Research in partnership with Kids Brain Health Foundation, Sinneave Family Foundation, CASDA, Autism Speaks Canada and Health Canada, while MF was funded by the Canadian Institutes of Health Research Frederick Banding and Charles Best Canada Graduate Scholarship.
1. Hamby S, Grych JH. The Web of Violence Exploring Connections Among Different Forms of Interpersonal Violence and Abuse. Dordrecht; New York, NY: Springer (2013).
2. American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Arlington, VA: American Psychiatric Publishing.
3. Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders: autism and developmental disabilities monitoring network, 14 sites, United States, 2008. MMWR Surveill Summ. (2012) 61:1–19.
4. Centers for Disease Control and Prevention. Prevalence and characteristics of autism spectrum disorder among children aged 8 Years — autism and developmental disabilities monitoring network, 11 sites, United States, 2012. Surveill Summ. (2016) 65:1–23.
5. Brown-Lavoie SM, Viecili MA, Weiss JA. Sexual knowledge and victimization in adults with autism spectrum disorders. J Autism Dev Disord. (2014) 44:2185–96. doi: 10.1007/s10803-014-2093-y
6. Cappadocia MC, Weiss JA, Pepler D. Bullying experiences among children and youth with autism spectrum disorders. J Autism Dev Disord. (2012) 42:266–77. doi: 10.1007/s10803-011-1241-x
7. Mandell DS, Walrath CM, Manteuffel B, Sgro G, Pinto-Martin JA. The prevalence and correlates of abuse among children with autism served in comprehensive community-based mental health settings. Child Abuse Neglect (2005) 29:1359–72. doi: 10.1016/j.chiabu.2005.06.006
8. Sullivan PM, Knutson JF. Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Neglect (2000) 24:1257–73. doi: 10.1016/S0145-2134(00)00190-3
9. Carter S. Bullying of students with Asperger syndrome. Issues Compr Pediatr Nurs. (2009) 32:145–4. doi: 10.1080/01460860903062782
10. Brown KR, Peña EV, Rankin S. Unwanted sexual contact: students with autism and other disabilities at greater risk. J Coll Stud Dev. (2017) 58:771–6. doi: 10.1353/csd.2017.0059
11. Fisher MH, Moskowitz AL, Hodapp RM. Differences in social vulnerability among individuals with autism spectrum disorder, Williams syndrome, and Down syndrome. Res Autism Spectr. Disord. (2013). 7:931–7. doi: 10.1016/j.rasd.2013.04.009
12. Jawaid A, Riby DM, Owens J, White SW, Tarar T, Schulz PE. ‘Too withdrawn' or ‘too friendly’: considering social vulnerability in two neurodevelopmental disorders. J Intellect Disabil Res. (2012) 56:335–50. doi: 10.1111/j.1365-2788.2011.01452.x
13. Finkelhor D, Ormrod R, Turner H, Holt M. Pathways to poly-victimization. Child Maltreat. (2009) 14:316–29. doi: 10.1177/1077559509347012
14. Kazdin AE. Conceptualizing the challenge of reducing interpersonal violence. Psychol Viol. (2011). 1:166–87. doi: 10.1037/a0022990
15. Bjørkly S. Risk and dynamics of violence in Asperger's syndrome a systematic review of the literature. Aggress Violent Behav. (2009) 14:306–12. doi: 10.1016/j.avb.2009.04.003
16. Ghaziuddin M, Tsai L, Ghaziuddin N. Brief report: violence in asperger syndrome, a critique. J Autism Dev Disord. (1991) 21:349–54. doi: 10.1007/BF02207331
17. King C, Murphy GH. A systematic review of people with autism spectrum disorder and the criminal justice system. J Autism Dev Disord. (2014) 44:2717–33. doi: 10.1007/s10803-014-2046-5
18. Sevlever M, Roth ME, Gillis JM. Sexual abuse and offending in Autism Spectrum Disorders. Sex Disabil. (2013) 31:189–200. doi: 10.1007/s11195-013-9286-8
19. Barnhill GP. Outcomes in adults with Asperger syndrome. Focus Autism Other Dev Disabl. (2007) 22:116–26. doi: 10.1177/10883576070220020301
20. Howlin P. Outcome in adult life for more able individuals with autism or Asperger syndrome. Autism (2000) 4:63–83. doi: 10.1177/1362361300004001005
21. Happe FGE. An advanced test of theory of mind: understanding of story characters' thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. J Autism Dev Disord. (1994) 24:129–54. doi: 10.1007/BF02172093
22. Jolliffe T, Baron-Cohen S. A test of central coherence theory: linguistic processing in high-functioning adults with autism or Asperger syndrome: is local coherence impaired? Cognition (1999) 71:149–85. doi: 10.1016/S0010-0277(99)00022-0
23. Howlin P, Clements J. Is it possible to assess the impact of abuse on children with pervasive developmental disorders? J Autism Dev Disord. (1995) 25:337–54. doi: 10.1007/BF02179372
24. Haskins BG, Silva JA. Asperger's disorder and criminal behavior: Forensic-Psychiatric considerations. J Am Acad Psychiatry Law (2006) 34:374–84.
25. Murrie DC, Warren JI, Kristiansson M, Dietz PE. Asperger's syndrome in forensic settings. Int J Forensic Ment Health (2002) 1:59–70. doi: 10.1080/14999013.2002.10471161
26. Palermo MT. Pervasive developmental disorders, psychiatric comorbidities, and the law. Int J Offender Ther Comp Criminol. (2004) 48:40–8. doi: 10.1177/0306624X03257713
27. Church C, Alisanski S, Amanullah S. The social, behavioral and academic experiences of children with Asperger syndrome. Focus Autism Other Dev Disabl. (2000) 15:12–20. doi: 10.1177/108835760001500102
28. Stokes M, Newton N, Kaur A. Autistic spectrum disorders and stalking. Autism (2004) 8:337–9. doi: 10.1177/1362361304045220
29. Stokes M, Newton N, Kaur A. Stalking, and social and romantic functioning among adolescents and adults with autism spectrum disorder. J Autism Dev Disord. (2007) 37:1969–86. doi: 10.1007/s10803-006-0344-2
30. Gratz KL, Paulson A, Jakupcak M, Tull MT. Exploring the relationship between childhood maltreatment and intimate partner abuse: Gender differences in the mediating role of emotion dysregulation. Violence Vict. (2009) 24:68–82. doi: 10.1891/0886-6708.24.1.68
31. Mahady-Wilton M, Craig WM, Pepler DJ. Emotional regulation and display in classroom bullying: characteristic expressions of affect, coping styles and relevant contextual factors. Soc Dev. (2000) 9:226–45. doi: 10.1111/1467-9507.00121
32. Walsh K, DiLillo D, Messman-Moore T. Lifetime sexual victimization and poor risk perception: does emotion dysregulation account for the links?. J Interpers Violence (2012) 27:3054–71. doi: 10.1177/0886260512441081
33. McNulty JK, Hellmuth JC. Emotion regulation and intimate partner violence in newlyweds. J Family Psychol. (2008) 22:794–7. doi: 10.1037/a0013516
34. Mazefsky CA, Herrington J, Siegel M, Scarpa A, Maddox BB, Scahill L, et al. The role of emotion regulation in autism spectrum disorder. J Am Acad Child Adolesc Psychiatry (2013) 52:679–88. doi: 10.1016/j.jaac.2013.05.006
35. Rieffe C, Camodeca M, Pouw LBC, Lange AMC, Stockmann L. Don't anger me! Bullying, victimization, and emotion dysregulation in young adolescents with ASD. Eur J Dev Psychol. (2012) 9:351–70. doi: 10.1080/17405629.2012.680302
36. Hooven C, Nurius PS, Logan-Greene P, Thompson EA. Childhood violence exposure: Cumulative and specific effects on adult mental health. J Fam Violence (2012) 27:511–22. doi: 10.1007/s10896-012-9438-0
37. Lord C, Rutter M, DiLavore PC, Risi S, Gotham K, Bishop S. (2012). Autism Diagnostic Observation Schedule: ADOS-2. Torrance: Western Psychological Services.
38. Wechsler D. Wechsler Abbreviated Scale of Intelligence. San Antonio, TX: Psychological Corporation (1999).
39. Kandalaft MR, Didehbani N, Krawczyk DC, Allen TT, Chapman SB. Virtual reality social cognition training for young adults with high-functioning autism. J Autism Dev Disord. (2012) 43:34–44. doi: 10.1007/s10803-012-1544-6
40. Hamby SL, Finkelhor D, Ormrod RK, Turner HA. (2004). The Juvenile Victimization Questionnaire (JVQ): Administration and Scoring Manual. Durham, NH: Crimes Against Children Research Center.
41. Finkelhor D, Ormrod R, Turner H, Hamby SL. The victimization of children and youth: a comprehensive, national survey. Child Maltreat. (2005) 10:5–25. doi: 10.1177/1077559504271287
42. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
43. Gratz KL, Gunderson JG. Preliminary data on an acceptance-based emotion regulation group intervention for deliberate self-harm among women with borderline personality disorder. Behav Ther. (2006) 37:25–35. doi: 10.1016/j.beth.2005.03.002
44. Tull MT, Barrett HM, McMillan ES, Roemer L. A preliminary investigation of the relationship between emotion regulation difficulties and posttraumatic stress symptoms. Behav Ther. (2007) 38:303–13. doi: 10.1016/j.beth.2006.10.001
45. Swain D, Scarpa A, White S, Laugeson E. Emotion dysregulation and anxiety in adults with ASD: does social motivation play a role? J Autism Dev Disord. (2015) 45:3971–7. doi: 10.1007/s10803-015-2567-6
46. Yager J, Iarocci G. The development of the Multidimensional Social Competence Scale: a standardized measure of social competence in autism spectrum disorders. Autism Res. (2013) 6:631–41. doi: 10.1002/aur.1331
47. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. (2004) 36:717–31. doi: 10.3758/BF03206553
48. Richmond JM, Elliott AN, Pierce TW, Aspelmeier JE, Alexander AA. Polyvictimization, childhood victimization, and psychological distress in college women. Child Maltreat. (2009) 14:1270147. doi: 10.1177/1077559508326357
49. Storch EA, Larson MJ, Ehrenreich-May J, Arnold EB, Jones AM, Renno P, et al. Peer victimization in youth with autism spectrum disorders and co-occurring anxiety: relations with psychopathology and loneliness. J Dev Phys Disabil. (2012) 24:575–90. doi: 10.1007/s10882-012-9290-4
50. Rawana JS, Norwood SJ, Whitley J. A mixed-method evaluation of a strength-based bullying prevention program. Can J Sch Psychol. (2011) 26:283–300. doi: 10.1177/0829573511423741
51. McGrath L, Jones R, Hastings RP. Outcomes of anti-bullying intervention for adults with intellectual disabilities. Res Dev Disabil. (2010) 31:376–80. doi: 10.1016/j.ridd.2009.10.006
52. McEachern AG. Sexual abuse of individuals with disabilities: prevention strategies for clinical practice. J Child Sex Abus. (2012) 21:386–98. doi: 10.1080/10538712.2012.675425
53. Bruder C, Kroese BS. The efficacy of interventions designed to prevent and protect people with intellectual disabilities from sexual abuse: a review of the literature. J Adult Protect. (2005) 7:13–27. doi: 10.1108/14668203200500009
54. Bowman RA, Scotti JR, Morris TL. Sexual abuse prevention: a training program for developmental disabilities service providers. J Child Sex Abus. (2010) 19:119–127. doi: 10.1080/10538711003614718
55. Ghaziuddin M. Violent behavior in autism spectrum disorder: Is it a fact, or fiction? Curr Psychiatr. (2013) 12:23.
56. Mogavero MC. Autism, sexual offending, and the criminal justice system. J Intell Disab Off Behav. (2016) 7:116–126. doi: 10.1108/JIDOB-02-2016-0004
57. Brown J, Cohen P, Johnson JG, Salzinger S. A longitudinal analysis of risk factors for child maltreatment: findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse Negl. (1998) 22:1065–78. doi: 10.1016/S0145-2134(98)00087-8
58. Darves-Bornoz JM, Lemperiere T, Degiovanni A, Gaillard P. Sexual victimization in women with schizophrenia and bipolar disorder. Soc Psychiatry Psychiatr Epidemiol. (1995) 30:78–84. doi: 10.1007/BF00794947
59. Moffitt TE, Robins RW, Caspi A. A couples analysis of partner abuse with implications for abuse prevention policy. Criminol Public Policy (2001) 1:5–36. doi: 10.1111/j.1745-9133.2001.tb00075.x
60. Schumacher JA, Feldbau-Kohn S, Smith Slep AM, Heyman RE. Risk factors for male-to-female partner physical abuse. Aggress Violent Behav. (2001) 6:281–352. doi: 10.1016/S1359-1789(00)00027-6
61. Vicary JR, Klingaman LR, Harkness W. L. Risk factors associated with date rape and sexual assault of adolescent girls. J Adolesc. (1995) 18:289–306. doi: 10.1006/jado.1995.1020
62. Widom CS, White HR. Problem behaviours in abused and neglected children grown up: prevalence and co-occurrence of substance abuse, crime and violence. Crim Behav Mental Health (1997) 7:287–310. doi: 10.1002/cbm.191
Keywords: autism, emotion regulation, social skills, victimization, perpetration, bullying, adults, maltreatment
Citation: Weiss JA and Fardella MA (2018) Victimization and Perpetration Experiences of Adults With Autism. Front. Psychiatry 9:203. doi: 10.3389/fpsyt.2018.00203
Received: 24 February 2018; Accepted: 02 May 2018;
Published: 25 May 2018.
Edited by:
Manuel Fernando Casanova, School of Medicine Greenville, University of South Carolina, United StatesReviewed by:
Marisa Fisher, Michigan State University, United StatesCopyright © 2018 Weiss and Fardella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan A. Weiss, am9ud2Vpc3NAeW9ya3UuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.