 Lisa Herbig
Lisa Herbig Brady Wagoner
Brady Wagoner Meike Watzlawik
Meike Watzlawik Eric Allen Jensen
Eric Allen Jensen Lars Lorenz
Lars Lorenz Axel Pfleger
Axel Pfleger
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
DATA REPORT article
Front. Polit. Sci. , 08 July 2022
Sec. Political Science Methodologies
Volume 4 - 2022 | https://doi.org/10.3389/fpos.2022.791494
This article is part of the Research Topic Evidence-Based Science Communication in the COVID-19 Era View all 13 articles
The COVID-19 pandemic has introduced a radical rupture into the lives of people around the world. Overnight society slowed to a standstill, strict rules were put in place and people had to adapt to a new set of norms and practices to curb the spread of the virus. In this way, the pandemic has been a naturally occurring experiment on the public's responses to rapid societal changes, bringing earlier niche topics such as trust, compliance, vaccine hesitancy and conspiracy theories to the forefront of both public and scientific discussion. How did people experience, understand and react to these rapid changes? In this article, we describe a dataset of longitudinal semi-structured interviews collected in Germany between December 2020 and September 2021 that sheds light on this question. This dataset was created as part of the Viral Communication project (viralcomm.info), which has investigated public responses to the COVID-19 pandemic in Germany including people's changing perceptions, attitudes, beliefs and behaviors. It complements and deepens the explosion of research that has emerged on how societies organized themselves in the wake of the pandemic.
Research has shown that when COVID-19 restrictions have been communicated persuasively through a collective “we,” most citizens have demonstrated their willingness to make personal sacrifices for the greater good of the community (Moss and Sandbakken, 2021). In constrast, poor, partisan or politicized communication has often led to the opposite, though other factors such as misinformation also play a crucial part (Jetten et al., 2020). Similarly, COVID-19 vaccines have been heralded as a scientific triumph that is key to ending the pandemic, but vaccination has come up against public hesitancy from many and outright resistance from a few. As MacDonald (2015) put it, “vaccination hesitancy is complex and context specific, varying across time, place and vaccines. It is influenced by factors such as complacency, convenience and confidence” (p. 4163). Explaining people's resistance through scientific illiterate or pathological behavior is insufficient to make sense of the complexity and specificities of the issue (Larson, 2020). Instead, a fine-grained analysis of people's COVID-19 vaccination decision-making is needed to fill the gap. With its mixed-methods approach, Viral Communication provides a comprehensive and nuanced approached to the above themes and many more concerning people's evolving responses to the pandemic.
Qualitative longitudinal studies can be done in several ways, including (1) continuous research in the same small society, (2) periodic studies at regular or irregular intervals, and (3) return after a lengthy interval of time has elapsed since the original research was done (Epstein, 2002). The Viral Communication interview study followed the second approach, carrying out three rounds of interviews at regular intervals (3–4 month between interviews). Participants of the longitudinal interview study were purposively sampled from a national representative survey instrument that has been described in a previous publication (Jensen et al., 2021). Interview questions were designed to follow-up on some of the survey questions and to obtain a more in-depth understanding of the relevant topics and discussions (e.g., vaccination, information seeking, trust in political and scientific actors, mask-wearing and conspiracy beliefs). By elaborating on some important themes of the survey, the dataset provides a unique window into health decision making processes, perceived challenges and opportunities as well as the process dynamics of changing attitudes toward mitigation measures during a global health crisis. Researchers can analyse it from a variety of perspectives used in qualitative longitudinal studies (e.g. Davidson, 2009; Shirani and Henwood, 2011; Patrick, 2014; Torregrosa et al., 2015), such as analyzing (1) rich individual cases studies that illustrate the complexity of subjective experience in context, (2) relevant themes within the interview (e.g. vaccination, conspiracy theories, trust) and (3) specific socio-demographic groups (e.g. generational differences in attitudes toward protective measures). Qualitative data (especially longitudinal) is labor intensive and thus still relatively rare. This dataset aims to close this gap by providing researchers with qualitative material that enables a deeper and complex understanding of people's experiences, thinking and behavior through the pandemic.
Three rounds of semi-structured qualitative interviews were conducted between December 2020 and September 2021. Participants were recruited initially through a much larger nationally representative online survey conducted in November/December 2020 (and repeated two more times). The interview data were collected as part of a wider suite of qualitative and quantitative data collection methods employed by the Viral Communication (viralcomm.info) project. The full set of research protocols and procedures for this project were reviewed and approved by the Ethics Committee of Sigmund Freud University. All participants gave their consent to having their full anonymized interviews made available within a public dataset.
Three rounds of interviews were conducted. The first, second and third rounds of interviews took place in December 2020, April 2021 and September 2021, respectively. Interviews were carried out in the weeks following the online survey so as to be able to triangulate responses between the two data collections methods. All interviews were conducted in German either via telephone or Zoom. Four pilot interviews were initially held to ensure a good flow between questions and that the interviews were around 40 minutes each (balancing the needs of getting sufficient elaboration and not overly taxing participants). The average length per interview was 41 min (Round 1), 42 min (Round 2) and 45 min (Round 3) with the shortest interview being 22 min (Round 1), 27 min (Round 2) and 23 min (Round 3) long and the longest one being 88 min (Round 1), 64 min (Round 2) and 99 min (Round 3).
Within the project's main nationally representative online survey all participants had the option to declare their willingness to participate in three follow-up interviews. In total 278 respondents indicated their willingness to participate in the interview study. A purposive sampling approach was applied to select interview participants aiming for a balanced sample concerning socio-demographic variables as well as attitudes and beliefs. We applied two sets of selection criteria to select the interview participants: The primary set of selection criteria included balancing age group, gender and socio-economic status (SES). Regarding their SES participants were either grouped as having a high (above survey median) or low (below survey median) SES based on their self-indicated yearly income.
In addition, a second level of criteria was applied, focusing on the following attitudes and backgrounds: Level of trust, migration background, vaccination willingness, and attitudes toward protective measures (i.e. mask wearing). This grouping of participants was solely used for the purpose of having a sample representing the wide variety of attitudes and beliefs across different socio-demographic groups in the German population. A full SPSS dataset including all socio-demographic questions and all additional survey items for all interviewees is made available alongside the data for further analysis.
Special attention was paid to the first level criteria, trying to balance out all three variables. If there were multiple possible candidates to contact, the second level criteria were taken into consideration, so as to have a full distribution of attitudes and backgrounds represented in the final sample. A detailed overview of our sampling approach, including selection criteria, can be found in the supplementary material (Table A.1) provided alongside the dataset (https://doi.org/10.5281/zenodo.5556052).
The final sample consisted of 40 participants. An overview of the sample is given in Table 1.
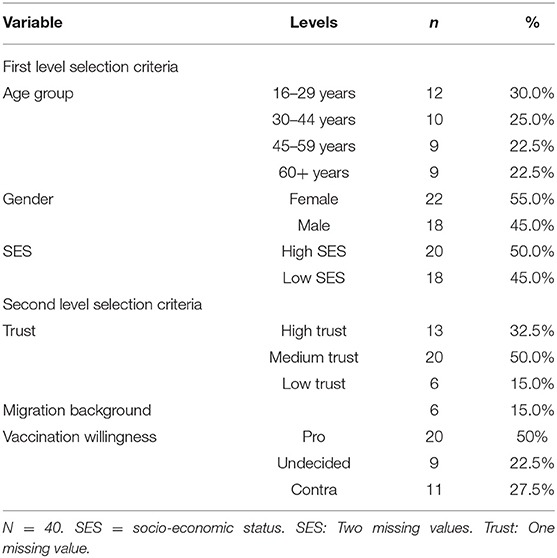
Table 1. Sample characteristics.
In between the first and second round of interviews, two participants dropped out of the study: (1) One woman from the age group 45–59 with a low SES and low trust; and (2) one woman from the age group 16–29 with a high SES and high trust.
Interviewer 1 was a female psychologist with substantial, previous experience in qualitative research. Six interviews in Round 1 were conducted by a second interviewer. Interviewer 2 was a purposely trained male research assistant who, at the time of data collection, was undertaking his undergraduate degree in psychology. Debriefing between the interviewers and an experienced member of the research team took place shortly after each interview.
After explicit consent from participants, all interviews were audio-recorded using the recording function of the computer (telephone interviews) or by using the Zoom recording function. Following the interview, audio files were pre-transcribed using the f4x automatic transcription function. Afterwards, each interview was accurately transcribed and corrected by student assistants using the transcription function of the MAXQDA software. The short greeting at the beginning and goodbye at the end of the interview were not transcribed unless something relevant to the topic was raised there.
The interviews were transcribed using an intelligent verbatim transcription approach with only minor adjustments to the transcripts: Pauses were removed and some minor corrections were made (filler words were removed). Within the transcripts questions asked by the Interviewer are indicated by “I1:” or “I2:” respectively. Responses by the Interviewees are introduced by the corresponding interview number (e.g., “02: I don't think that…” for interview number 02). All names that are not part of the public life (e.g., Angela Merkel is kept in) as well as all parts that indicate a location or occupation that could lead to identifying one of the participants have been anonymized. Relevant sections and words have been replaced by inserting “XXXXX.” Notes about how something was verbalized (e.g., laughing, incomprehensible, ironic) have been bolded and inserted in parentheses. Words pronounced with strong emphasis were underlined.
The interviews were developed to further elaborate on some of the responses in the survey instrument. The topics and questions slightly varied from one interview round to the next, to adjust for new developments and make the interviews less repetitive. All interviews followed a semi-structured interview guide with a fixed set of open-ended questions for each participant. If interesting aspects and topics were mentioned by the interviewee, the interviewer followed up on those aspects with additional questions and asked for clarification and examples where needed.
At the start of each interview, participants were asked to give a short summary of what had happened in Germany with regards to the pandemic in the past 6 months, or since the last interview. This question was asked to help participants “arrive” in the interview situation, but also to identify which “key events” or “critical moments” (biographical or historical) are remembered and perceived as significant, and the consequences they have on individual attitudes and beliefs (Holland, 2011). After that, participants were asked for challenges and coping mechanisms during that time period. This “warm-up” phase was followed by different thematic sections that aimed to further probe participants' answers to the survey, asking for more details and information on the specific topics. A short overview of the thematic sections in each round of interviews can be found below, while the detailed interview guides are provided alongside the dataset (https://doi.org/10.5281/zenodo.5556052).
Data collection for the Phase I interview study took place from the 1st of December 2020 to the 28th of December 2020.
The interviews took place shortly after the second round of severe restrictions (called ‘lockdown light') was introduced in Germany in the beginning of November 2020. Despite those measures, numbers were rising and a second ‘hard lockdown' was introduced on December 16th, including strict contact restrictions, school closures and the closure of “non-essential” business. Shortly before the Christmas holidays, due to the new delta variant, travel from the UK and South Africa was restricted. Concerning the vaccines, the first dose of the Pfizer/BioNTech vaccine was already administered in the UK on the 8th of December but was not available to the general public yet. On December 21, the European Commission authorized the BioNTech/Pfizer vaccine. The first vaccine in Germany was administered on the 26th of December. Only one of our interviews was carried out after that date (Interview Nr. 41).
Topics covered in the interview include: Information/misinformation, trust/distrust in different political/scientific actors and institutions, compliance, vaccination, the cause of the outbreak and conspiracy beliefs. An exemplary question for each respective section can be found below.
• Information/Misinformation: “What sources of information are most important to you when looking for information about the coronavirus? What makes this source relevant to you?”
• Trust/Distrust in different political/scientific actors: “In your survey, you mentioned that you have [high/low trust] in [political/scientific actor; e.g., the WHO, Angela Merkel]. Can you tell me more about why you feel that way?”
• Compliance: “What are the most important measures you use to protect yourself from the coronavirus? In your survey response, you mentioned that you're [frequency of mask wearing] wearing a protective mask where it is mandatory. Could you describe how you feel wearing a face mask?”
• Vaccination: “In your survey response, you mentioned that you'd [vaccination willingness] get a voluntary coronavirus vaccination. Could you explain why you're feeling that way?”
• Cause of the outbreak of the COVID-19 pandemic: “What do you see as the cause of the outbreak?”
• Conspiracy beliefs: “In the survey response you indicated that you [agree/strongly agree] with the statement that [Conspiracy belief]. Can you explain your reasons for agreeing with this statement?”
Data collection for the Phase II interview study took place from the 6th of April 2021 to the 28th of April 2021.
In April 2021, case numbers remained persistently high. Vaccination was still not available to everyone and the distribution followed a prioritization based on age, health status and occupation. In the previous month, the AstraZeneca vaccine was suspended on March 15 after reports of rare, but serious, blood clots. A few days later, on March 19, vaccination with AstraZeneca in Germany continued until the 30th of March 2021, when it is decided to only vaccinate people over the age of 60 with the AstraZeneca vaccine. On April 6th, the AstraZeneca vaccine was made available to the whole population, regardless of the prioritization group. In the beginning of April, 11.6 % of the population received at least one dose of vaccination. By the end of April, this number rose to more than 25%.
Despite increasing vaccination efforts, the number of new infections stayed high and the German government announced another short, but very strict, nationwide lockdown over the easter holidays (“Osterruhe”) from April 1st to April 5th. After massive criticism and great confusion about the practical implementation, Angela Merkel had to publicly apologize and reverse the decision.
There were slight changes to the questions of each theme and an additional theme was added at the end:
• Information/Misinformation: “What specific information about the coronavirus are you looking for? Are you satisfied with the information you find?”
• Trust/Distrust in different political/scientific actors: “In the second survey, you mentioned that you have [high/low trust] in [political/scientific actor; e.g., the WHO, Angela Merkel], while in the first survey you indicated that you have [high/low trust]. Can you tell me more about why your level of trust in [political/scientific actor] has [increased/decreased]?”
• Compliance: “Are there situations where you break your ‘mask-wearing routine'?”
• Vaccination: “[Do/did] you have any concerns about being vaccinated?”
• Cause of the outbreak: “How did this pandemic come about?”
• Conspiracy beliefs: “In the first survey response, you indicated that you [level of agreement] with the statement that [Conspiracy belief], while in the second survey you indicated that you [level of agreement]. Can you explain why your opinion has changed?”
• NEW: Outlook and Lessons Learned: “How would you determine the end of the pandemic?”, “Are there any lessons learned from the pandemic for the future?”
Data collection for the Phase III interview study took place from the 2nd of September 2021 to the 23rd of September 2021.
By September, 84% of the German population had received at least one dose of vaccination. The case numbers were relatively low, and the public discussion has shifted to one focusing on the ‘re-opening' of society and mandatory vaccination. On September 26, federal elections were held in Germany, leading to a change of government after 16 years of Angela Merkel's chancellorship.
Again, slight changes were made to questions within the existing themes:
• Information/Misinformation: “What specific information about the coronavirus are you looking for? Are you satisfied with the information you find?”
• Trust/Distrust in different political/scientific actors: “Does the COVID pandemic have a decisive influence on your voting behavior in this year's federal election? How far?”
• Compliance: “Has your mask-wearing behavior changed for you since we last spoke? In what way? Why?”
• Vaccination: “Has anything changed for you since you had the full vaccine coverage? Are there situations in which you feel unprotected against the virus?”
• Conspiracy beliefs: “In the second survey response, you indicated that you [level of agreement] with the statement that [Conspiracy belief], while in the third survey you indicated that you [level of agreement]. Can you explain why your opinion has changed?”
• Outlook and Lessons Learned: “What lessons do you personally draw from this time?”
All interview transcripts (in German) are accessible on the open science publication platform Zenodo: https://doi.org/10.5281/zenodo.5556052. In addition, the interview guides for phase I, II and III are provided in English and German. An SPSS file including relevant demographic and contextual information (incl. selection criteria) about all interview participants of the Viral Communication project is provided as an anonymised version. All data can be linked through the ID number (ranging between “01” and “41”) that identifies each participant. This ID number stays the same throughout all three interviews (e.g. “05_1” for participant “05”s first interview, “05_2” for participant “05”s second interview and “05_3” for participant “05”s third interview).
This dataset will be especially of interest to researchers that want to study topics such as people's changing narratives of the pandemic in Germany, trust in authorities and institutions, the dynamics of compliance and non-compliance with measures (esp., face-masks), vaccination decision-making and belief in conspiracy theories, to name a few key topics. Researchers applying natural language processing techniques (e.g., automated sentiment analysis, topic modeling, framing) might be especially interested in this unique dataset. Furthermore, the dataset is relevant to political scientist for answer questions related to varying levels of trust in political actors and institutions. For example, it can be helpful in answering questions about why trust increased/decreased over time. The same applies to researchers in communication science trying to explain why certain information sources are favored over others and how trust in those sources changed over the course of the pandemic.
In general, the longitudinal character of the data for each participant is of particular value in that it provides a rare opportunity to track people's thoughts and feelings through time. For example, one can see how initial COVID-19 vaccine resistance is progressively overcome by most participants, while a minority of participants become progressively more extreme in their attitudes against it. We also asked people to recall the last 6 months of the pandemic in Germany and to imagine the next period of time in the future; thus, researchers can compare future expectations and subsequent narrations of the past. Another feature worth noting is the dialogical character of some questions: participants were asked how they would respond to others who have an opposing belief with regards to some issue (e.g., face-masks). Finally, the combination with the SPSS dataset containing survey responses of all 40 participants that is provided alongside the interview data offers various options for triangulation. In short, the dataset provides researchers with an extremely rich material to better understand how people have experienced and made sense of the pandemic situation through time.
The anonymized datasets generated for this study can be found on the open science publication platform Zenodo https://doi.org/10.5281/zenodo.5556052.
The studies involving human participants were reviewed and approved by Ethics Committee of Sigmund Freud University. The patients/participants provided their written informed consent to participate in this study.
LH and BW wrote the report. MW, BW, and LH were responsible for the interview study within the viral communication project. The interview guides were designed by MW, BW, EJ, and LH. EJ commented on the draft of the article. AP and LL helped with the interview process and analysis. All authors contributed to the article and approved the submitted version.
This research was funded by the German Federal Ministry of Education and Research (BMBF) [Grant Number: 01KI20500]. Aalborg University paid for the open access publication fees. This content is solely the responsibility of the authors and does not necessarily represent the official views of the BMBF or Aalborg University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the participants who agreed to be interviewed for this study and shared their experiences and ideas. We would also like to thank our student assistants for providing transcription services.
Davidson, R. (2009). More than ‘Just Coping': The Antecedents and Dynamics of Resilience in a Qualitative Longitudinal Study. Soc. Policy Soc. 8, 115–125. doi: 10.1017/S1474746408004636
Epstein, T. S. (2002). Mysore villages revisited. Chronicling Cultures: Long-Term Field Research in Anthropology, Walnut Creek, CA: AltaMira.
Holland, J. (2011). “Timescapes: living a qualitative longitudinal study,” in Forum Qualitative Sozialforschung/Forum: Qualitative Social Research. 12. doi: 10.17169/fqs-12.3.1729
Jensen, E. A., Pfleger, A., Lorenz, L., Jensen, A. M., Wagoner, B., Watzlawik, M., et al. (2021). Exploring viral communication: a repeated measures dataset. Front. Psychol. 13, 817648–817648.
Jetten, J., Reicher, S. D., Haslam, S. A., and Cruwys, T. (2020). Together Apart: The psychology of Covid-19. Sage.
Larson, H. (2020). Stuck: How Vaccine Rumors Start - and Why They Don't Go Away. Oxford University Press.
MacDonald, N. E., and the SAGE working group on vaccine hesitancy (2015). Vaccine hesitancy: Definition, scope and determinants. Vaccine 33, 4161. doi: 10.1016/j.vaccine.2015.04.036
Moss, S. M., and Sandbakken, E. M. (2021). “Everybody needs to do their part, so we can get this under control.” reactions to the norwegian government meta?narratives on COVID?19 measures. Polit. Psychol. 42, 881–898.
Patrick, R. (2014). Working on welfare: findings from a qualitative longitudinal study into the lived experiences of welfare reform in the UK. J. Soc. Policy 43, 705–25. doi: 10.1017/S0047279414000294
Shirani, F., and Henwood, K. (2011). Continuity and change in a qualitative longitudinal study of fatherhood: relevance without responsibility. Int, J. Soc. Res. Methodol. 14, 17–29. doi: 10.1080/13645571003690876
Keywords: COVID-19, mask-wearing, vaccination, conspiracy beliefs, trust, information behavior, longitudinal interview study
Citation: Herbig L, Wagoner B, Watzlawik M, Jensen EA, Lorenz L and Pfleger A (2022) Trajectories of Experience Through the Pandemic: A Qualitative Longitudinal Dataset. Front. Polit. Sci. 4:791494. doi: 10.3389/fpos.2022.791494
Received: 22 December 2021; Accepted: 16 June 2022;
Published: 08 July 2022.
Edited by:
Gordon Sammut, University of Malta, MaltaReviewed by:
Madeline O'Brien, Icahn School of Medicine at Mount Sinai, United StatesCopyright © 2022 Herbig, Wagoner, Watzlawik, Jensen, Lorenz and Pfleger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisa Herbig, bC5qLmhlcmJpZ0B1dmEubmw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.