 Ramón González-Matilla
Ramón González-Matilla Vanesa Abuín-Porras
Vanesa Abuín-Porras Isabel Mínguez-Esteban
Isabel Mínguez-Esteban Alberto M. Heredia-Rizo
Alberto M. Heredia-Rizo- 1Departamento de Fisioterapia, Investigación y Deporte. Centro Universitario FISIDEC, Universidad de Córdoba, Córdoba, Spain
- 2Centro de Atención Infantil Temprana, Universidad de Córdoba, Córdoba, Spain
- 3CTS 1110: Understanding Movement and Self in health from Science (UMSS) Research Group, Andalusia, Spain
- 4Department of Physiotherapy, Universidad Europea de Madrid, Faculty of Medicine, Health and Sports, Villaviciosa de Odón, Spain
- 5Instituto de Biomedicina de Sevilla, IBiS (Hospitales Universitarios Virgen del Rocío y Macarena/CSIC/Universidad de Sevilla), Sevilla, Spain
- 6Departamento de Fisioterapia, Universidad de Sevilla, Sevilla, Spain
Introduction: Spasticity and altered muscle tone are key features in children with neurodevelopmental disorders, particularly cerebral palsy (CP). They impact movement, range of motion (ROM), and pain perception, influencing functional abilities and quality of life. Understanding the intrinsic muscle differences in children with CP can help improve clinical assessment and therapeutic interventions. This study aims to evaluate differences in muscle tone, stiffness, ROM, and pain perception between children with CP and typically developing peers using objective biomechanical measures.
Methods: An observational, cross-sectional study was conducted with 40 participants of both sexes (20 children with CP, 20 typically developing peers). Muscle tone and stiffness of the lower limb muscles were measured using the Myoton PRO device. ROM was assessed by goniometry, and pain perception was evaluated using the Visual Analog Scale during a Straight Leg Raise (SLR) test. A generalized linear mixed model was used to detect differences in myotonometry, ROM, and pain perception measurements. In participants with CP, the Pearson product-moment correlation coefficient analysis was used to explore possible associations between clinical features and muscle tone and stiffness.
Results: Children with CP exhibited reduced ROM, with a significant group effect for hip flexion (P < 0.001; η2 = 0.843), knee extension (P < 0.001; η2 = 0.355), and ankle flexion (P < 0.001; η2 = 0.959) and higher pain perception during the SLR test (P < 0.001; η2 = 0.831), compared to controls. Myotonometry revealed significantly increased muscle stiffness of the rectus femoris (P = 0.004; η2 = 0.112) and adductor muscles (P = 0.019; η2 = 0.074) in the CP group, with no differences in muscle tone between the groups. Sex-related differences were found for muscle tone and stiffness, with males showing higher values. Correlation analyses indicated that adductor muscles stiffness was associated with CP severity.
Conclusion: Children with CP demonstrate significant changes in ROM, pain perception, and muscle stiffness, emphasizing the need for targeted therapeutic interventions. These findings support the use of objective biomechanical tools for assessing muscle properties in clinical settings, contributing to better management strategies for spasticity-related impairments.
Introduction
Muscle tone is a complex and dynamic state, resulting from hierarchical and reciprocal anatomical connectivity. It is a multidimensional concept regulated by input and output systems and has critical interplay with power and task performance requirements (Hidler and Rymer, 1999) that involve various body organs and systems, including bones, balance, and other neurological inputs, such as cardiovascular aspects and motivation (Beaudart et al., 2019). Atypical muscle tone is one of the most common clinical features in children with neurodevelopmental disorders, for example, in those with early brain injury or cerebral palsy (CP) (Goo et al., 2018).
Spasticity was first described as a “motor disorder characterized by a velocity-dependent increase in muscle tone, with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex” (Trompetto et al., 2014). This definition emphasizes the fact that spasticity is just one component of the upper motoneuron syndrome. Currently, it has been refined to state that spasticity is not only velocity-dependent but also a length-dependent and acceleration phenomenon (Nourizadeh et al., 2024). Spasticity is often present in pathologies that affect the first motoneuron or directly impact the cerebral cortex (Trompetto et al., 2014). It is estimated that the annual incidence of lower limb spasticity ranges between 30 and 485 per 100,000 for stroke, and between 100 and 235 per 100,000 for traumatic brain injury (Bhimani and Anderson, 2014), with a prevalence of 2.1 per 1,000 for CP (Goo et al., 2018).
Spasticity not only disrupts the balance between muscle excitation and inhibition, but it can also result in secondary impairments, such as contractures (Lackritz et al., 2021), bone deformities (Handsfield et al., 2022), and pain (Penner et al., 2013). These complications may limit physical function and can also contribute to emotional distress, social isolation, and a decreased overall quality of life (Milinis and Young, 2016; Vural et al., 2020). The intrinsic differences that spastic muscles present compared to healthy muscles, such as the level of actin and myosin contraction and the number of sarcomeres affected, support what has been previously described regarding spasticity (Lieber and Fridén, 2019).
Although traditional clinical assessments of muscle tone and spasticity, such as the Modified Ashworth and Tardieu scales, are widely used, they have inherent limitations, including subjective interpretation, limited sensitivity, and low inter-examiner reliability (Yam and Leung, 2006) These drawbacks highlight the need for more precise evaluations. The present study seeks to address these limitations by utilizing objective tools, such as myotonometry, to quantify intrinsic muscle properties objectively.
Despite the expected differences in muscle mechanical and viscoelastic properties between children with neurological disorders and typically developing peers, this aspect has not yet been investigated in detail. This article aims to explore the clinical differences between spastic and normal muscles regarding muscle tone and stiffness, range of motion, and pain perception, and the potential implications these differences may have on movement, psychometric outcomes, and quality of life.
Methods
Study design
A cross-sectional, observational study was conducted, including children diagnosed with CP and age- and sex-matched healthy participants from the same population-based cohort. The study protocol received ethical approval from the Biomedical Research Ethics Committee of the Andalusian Government, Spain (approval code: CI 0214-N-20) and the Ethics Committee for Research with Medicines of the Hospital Clínico San Carlos, Madrid (approval code: 24/544-E). The study adhered to the STROBE guidelines and was prospectively registered in the OSF Registries (https://osf.io/yg7ax). Prior to enrollment, written informed consent was gained from all parents or legal guardians, along with informed assent from the participating minors. Participants and their families received detailed information about the study procedures and the potential risks or adverse effects. All study data was securely stored, ensuring confidentiality and anonymity.
Population and setting
Children and adolescents, aged 6–17 years, diagnosed with CP, were recruited from various public and private specialized Early Intervention Centers in Southern Spain. The inclusion criteria were as follows: a) Gross Motor Function Classification System (GMFCS) level between I to IV, indicating preserved, but potentially severely limited, walking ability, with or without assistive devices (Rosenbaum et al., 2008). At level V, children and adolescents exhibit significant functional limitations, pronounced contractures, and severe positioning challenges, often requiring physical assistance and assistive technology to optimize head alignment, seating, standing, and mobility. All these factors may confound outcome measures, potentially compromising the accuracy and interpretability of the findings; b) increased muscle tone in the lower extremities, defined as a score greater than 0 on the Modified Tardieu Scale (Shu et al., 2021) and a positive response to the Duncan Ely Test (Lee et al., 2015); c) ability to communicate pain (Barney et al., 2018); and d) capacity to follow simple instructions and commands. Exclusion criteria included: a) previous lower limb surgery or interventions limiting joint mobility within the functional range (e.g., ankle joint arthrodesis); b) significant medication adjustments during the study that could influence muscle tone, whether increasing or decreasing it; c) uncontrolled epileptic seizures despite medication; d) having received botulinum toxin injections for the lower extremities within the 3 months before the study; and e) a concurrent new physical therapy treatment that could interfere with the study protocol.
The control group included healthy children and adolescents with normal sensorimotor development, no spasticity, and no previous history of neurological disorders. The same exclusion criteria applied to this group.
Study protocol
Demographic and clinical data, including CP type, affected side, GMFCS level, and use of antispastic medication, were initially collected by the same examiners. Participants were allocated to the study groups depending on their medical diagnosis: CP or normal sensorimotor development. The evaluator remained blinded to the aims of the study and to the clinical condition of participants. All evaluations were conducted during a single session lasting approximately 30–35 min.
Outcome measures
The primary outcome included muscle tone and stiffness of lower limb muscles, assessed using the Myoton PRO (Seo et al., 2023; Trybulski et al., 2024) (Myoton AS, Tallinn, Estonia), which has proven valid and reliable in individuals with neurological disorders, with a good to excellent intra- and inter-rater reliability to assess upper and lower extremity muscles in children with developmental disabilities, including CP (García-Bernal et al., 2021; Kutlutürk Yıkılmaz et al., 2024). With participants in a comfortable and relaxed supine or prone position, measurements were taken at two separate locations (proximal and distal) on the muscle bellies of the hamstrings (biceps femoris), quadriceps (rectus femoris), and adductor muscles (Bell, 2014; Agoriwo et al., 2022). Anatomical landmarks were identified using a wax pencil and the mean of two consecutive measurements, with a 30-s rest interval, was used for analysis.
For the biceps femoris, the proximal point was located midway between the ischial tuberosity and the head of the fibula, with the distal point positioned 6 cm caudally. For the rectus femoris, the proximal point was in the upper third of the muscle, between the anterior superior iliac spine and the upper pole of the patella, whereas the distal spot was located in the medial third of the muscle. For the adductor magnus, the proximal point was positioned in the upper third of the line extending from the internal femoral condyle and the ischiopubic ramus, while the distal point was in the medial third of the muscle (Agyapong-Badu et al., 2013; Drenth et al., 2018; García-Rueda et al., 2023).
Secondary outcomes comprised range of motion (ROM) measurements of the lower limb joints (Herrero et al., 2011; Johansen et al., 2020), and pain perception during the straight leg-raise test (SLR) (Marsico et al., 2016b). For ankle dorsiflexion, participants were seated comfortably at the edge of the table with their back supported and both lower limbs at rest. The goniometer (Enraf Nonius, PRIM group, Spain) was placed with the axis at the external malleolus, with one arm following the fifth metatarsal and the other the diaphysis of the fibula. For knee flexion, participants were in supine. The goniometer axis was at the lateral knee condyle, one arm aligned with the diaphysis of the femur and the other with the diaphysis of the fibula. For hip flexion, participants maintained the same supine position. The goniometer axis was placed at the greater trochanter of the femur, with one arm aligned with the femoral diaphysis, and the other following the midline of the body toward the axilla (Darrah et al., 2014; Bekteshi et al., 2021). The average of two consecutive measurements, with a 30-s rest break, was used for further analysis (Darrah et al., 2014; Johansen et al., 2020; Bekteshi et al., 2021).
Finally, participants were told to rate their self-reported pain intensity, using a Visual Analog Scale (VAS) (Declerck et al., 2016; Shearer et al., 2023), during the SLR test. With participants lying supine, the test was performed bilaterally. The leg was raised straight (knee extended and stretch position) at a speed of approximately 5°/s (Marsico et al., 2016b). Participants were instructed to inform the therapist once they reached the maximum tolerable symptoms. At that point, they were instructed to report their pain intensity. The therapist also registered the child’s description, and location of pain, tension, or tingling sensation. A first trial was conducted to allow familiarization with the produce, followed by two consecutive tests on each lower limb, with a 60-s rest between trials. The average of the two tests was used for further analysis (Kingsnorth et al., 2015; Barney et al., 2018; Shearer et al., 2023).
Sample size
The sample size was estimated using G*Power software (version 3.1.9.2, University of Kiel, Kiel, Alemania). Based on a similar study in adult neurological patients (García-Bernal et al., 2022), we assumed an α level of 0.05, a statistical power of 80%, and a large effect size (η2 = 0.15) for differences between groups in muscle tone and stiffness using the myotonometer. As a result, a total of 40 participants (20 per group) was required.
Statistical analysis
Statistical processing of the data was performed using SPSS Statistics for Windows software (version 29.0.2.0., IBM Corp, Armonk, NY). Quantitative variables are expressed as mean ± standard deviation (SD), while qualitative variables are presented as frequencies (percentages). Data normality was assessed using the Shapiro-Wilk test. A generalized linear mixed model (GLMM) was applied to detect differences in myotonometry (muscle tone and stiffness) and ROM and pain perception measurements, with sides (left vs. right) and sex (female vs. male) as within-subject factors, and groups (CP vs. control) as the between-subject factor. Bonferroni adjustment for post hoc multiple comparisons was used. In participants with CP, the Pearson product-moment correlation coefficient analysis with Bonferroni’s correction was used to explore possible associations between clinical features (CP type, affected side, medication use, and GMFCS level), and muscle tone and stiffness. Statistical significance was set at p < 0.05.
Results
A total of 40 participants (55% females, 22/40), with a mean age of 8.97 ± 1.74 years, agreed to participate and completed the study. The sample included 20 children with CP and 20 age- and sex-matched controls. No adverse reactions or dropouts occurred during the assessment protocol (Figure 1). Among children with CP, tetraparesis (9/20, 45%), and hemiparesis (8/20, 40%) were the most common presentations, with a predominantly bilateral involvement in more than half of participating minors (11/20, 55%). Participants were classified into GMFCS level I (5/20, 25%), level II (5/20, 25%), or level III (10/20, 50%). Both groups exhibited similar demographic characteristics, except for height (Table 1).
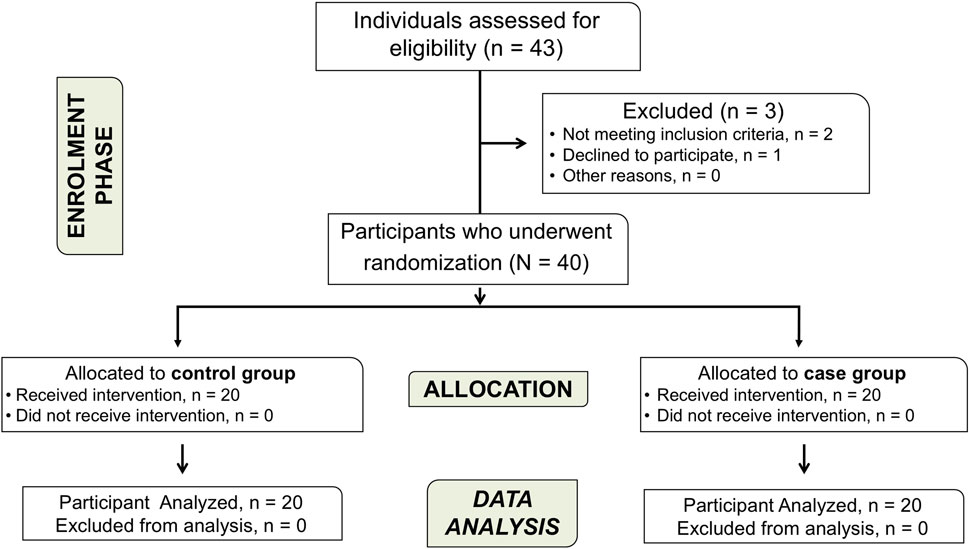
Figure 1. Flowchart diagram of participants.
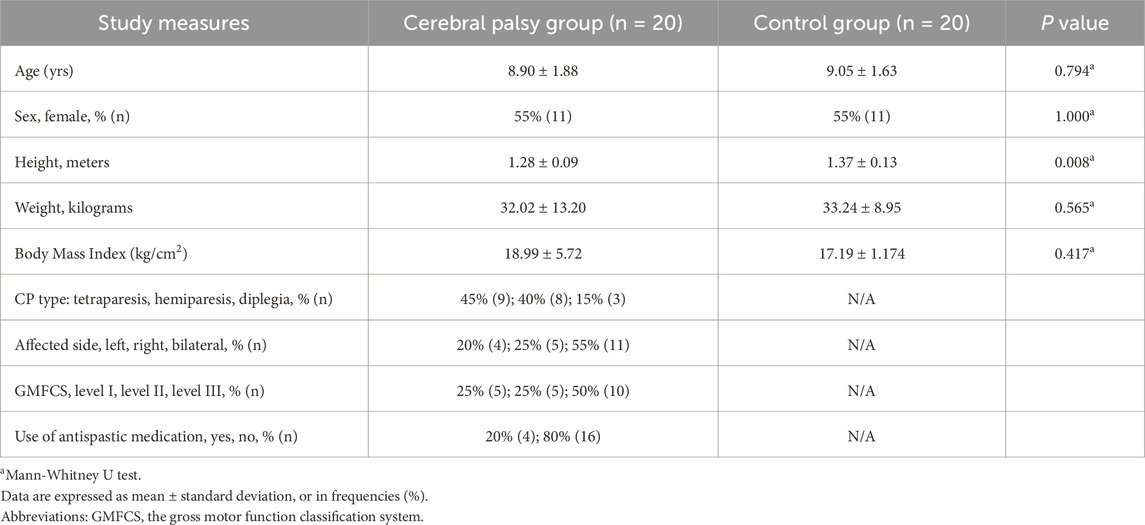
Table 1. Baseline clinical and demographic features of the study sample.
Muscle tone and stiffness
Table 2 presents the mean muscle stiffness (N/m) and tone (Hz) scores for the biceps femoris, rectus femoris, and adductor magnus (left and right sides) in both groups.
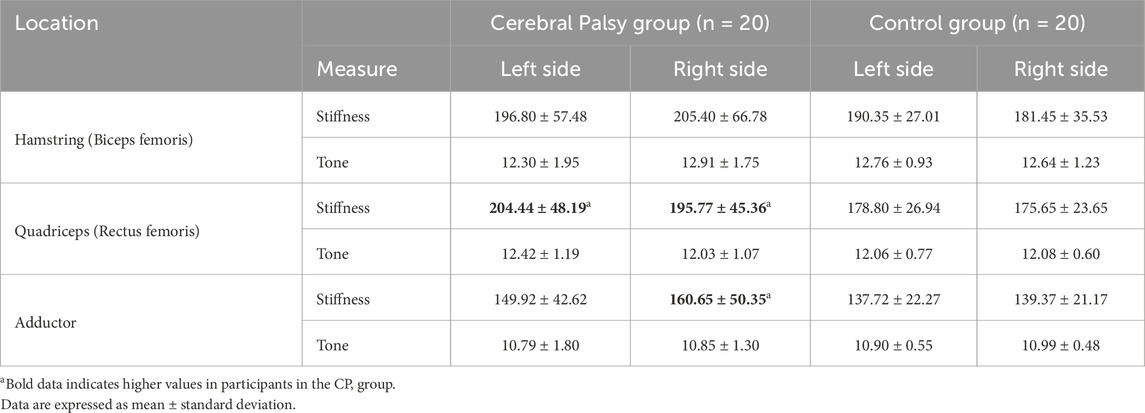
Table 2. Myotonometry measurements for muscle stiffness (N/m), and tone (Hz) in children with Cerebral Palsy (CP) and controls.
For muscle tone, the GLMM detected significantly higher values in males than females at the rectus femoris (F = 15.561; P < 0.001; η2 = 0.178) and adductor muscles (F = 8.579; P = 0.005; η2 = 0.106), with a significant group*sex interaction at both locations: rectus femoris: F = 5.599; P = 0.021; η2 = 0.072; adductor: F = 10.300; P = 0.002; η2 = 0.125. For muscle stiffness, significantly higher values were observed in the CP group at the rectus femoris (F = 9.042; P = 0.004; η2 = 0.112) and adductor muscles (F = 5.741; P = 0.019; η2 = 0.074). A significant sex effect was also found at the rectus femoris (F = 6.472; P = 0.013; η2 = 0.082), along with a group*sex interaction for the adductor muscle (F = 6.680; P = 0.012; η2 = 0.085).
Lower limb range of motion and pain perception
Bilateral ROM measurements for hip flexion, knee extension, and ankle flexion in both groups are shown in Table 3. The GLMM demonstrated a significant group effect for hip flexion (F = 387.387; P < 0.001; η2 = 0.843), knee extension (F = 39.646; P < 0.001; η2 = 0.355), and ankle flexion (F = 1,684.244; P < 0.001; η2 = 0.959), with no sides or sex effect. Regarding pain perception (ROM during the SLR test), a significant group effect (F = 353.035; P < 0.001; η2 = 0.831), and group*sex interaction (F = 5.042; P = 0.028; η2 = 0.065) were observed.
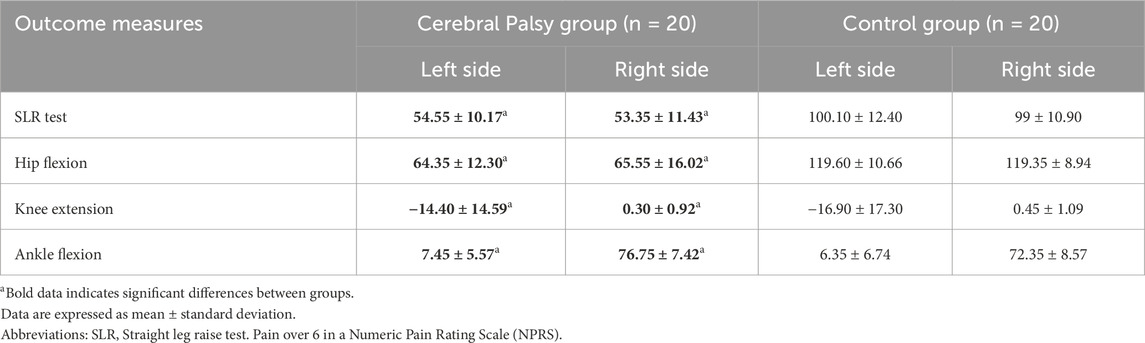
Table 3. Range of motion for hip flexion, knee extension, and ankle flexion in children with Cerebral Palsy and controls.
Correlation analysis
Among participants with CP, significant correlations were identified between: a) the affected side and adductor muscle tone (r = 0.484, P = 0.030) and stiffness (r = 0.469, P = 0.037); b) and CP type and adductor muscle stiffness (r = 0.461, P = 0.041) (Table 4).
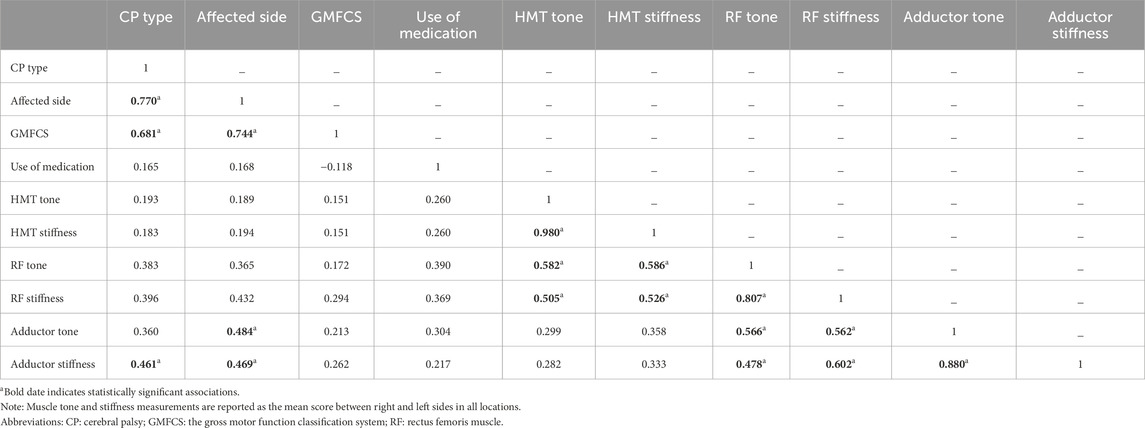
Table 4. Correlation coefficient matrix between clinical features of participants with CP and muscle tone and stiffness at hamstring, rectus femoris, and adductor muscles.
Discussion
The purpose of this study was to analyze the differences in children with neurological disorders associated with spasticity (CP) versus children with typical development in terms of intrinsic muscle properties, such as muscle stiffness and tone, ROM, and pain perception.
When considering myotonometry assessments, we only observed significant differences between groups for muscle stiffness of the rectus femoris and adductor magnus, but not for the biceps femoris. These results support those of Upachit et al., which suggests changes in myofascial and viscoelastic muscle properties, with a significant increase in muscle stiffness at rest, as well as mild muscle metabolism and atrophy, in individuals with pathologies associated with central degeneration (Upachit et al., 2025). In line with our results, Sagerer et al. reported increased stiffness and a short relaxation time in patients with neuromuscular disorders, highlighting the importance of intrinsic muscle tone and variability in tone distribution (Sagerer et al., 2024). Studies conducted in patients with stroke and Parkinson’s disease have also observed significant differences in stiffness when compared to healthy individuals (Brandín-de la Cruz et al., 2022; García-Bernal et al., 2022; 2023). In contrast to our results, Lukas et al. did not find significant differences in five disease groups regarding myotonometry assessments when comparing healthy individuals and patients with neuromuscular diseases. Measurements with the myotonometry device were unable to distinguish between the five different groups of disorders displaying increased stiffness or decreased muscle tone due to muscle atrophy (Lukas et al., 2023). For muscle tone (tension), as measured by myotonometry, there were no significant differences between the study groups. This may be due to the fact that both spasticity and hypertonia have a strong direct relationship with altered muscle tone, and sometimes this can create some confusion when identifying them (Hidler and Rymer, 1999). Interestingly, our findings suggest that sex seems to influence myotonometry values, with higher muscle tone and stiffness in males than in females, regardless of the study group, but only for the rectus femoris and adductor muscles. In line with this, Więch et al. (2020), investigated the effect of muscle tone on the body composition of children with CP, and reported a direct association between increased caloric needs and the increase of muscle tone, with differences between males and females in their study. As for correlations, significant associations were only found between adductor muscles tone or stiffness and some clinical parameters, such as CP type and the affected side. However, these results have to be taken cautiously, due to the small sample size and the observational design, which does not allow to imply causality. A rigorous assessment of potential sex differences should be addressed in future research involving a sufficiently large study sample.
As regards lower limb ROM, our findings showed significant differences between children with spasticity and normally developing peers. Reduced ROM and spasticity are frequent accompanying symptoms in CP that affect gait, posture, and daily function (Nordmark et al., 2009; Marsico et al., 2016a). Spasticity can also limit active joint ROM, and gross and fine motor function, with a potential influence to increase pain (Lindén et al., 2019). In the study by Nordmark et al. (2009), a decrease in the average ROM was found in children from 2 to 14 years in most assessed joints and muscles, especially for hip abduction and external rotation, knee extension, and ankle dorsiflexion. Cloodt et al. (2024) also concluded that the hamstrings muscles length decreased from childhood to adulthood in individuals with CP, regardless of the GMFCS level, and that knee extension was mainly reduced during the follow-up period for those with a GMFCS level between II to V. This supports previous results in children with CP, aged 4–17 years, who were able to walk at least 10 m on a flat, straight path (with or without assistive devices), and had significantly reduced passive ROM compared to children of the same age with typical development (McDowell et al., 2012).
Finally, regarding pain perception during the SLR test, the present results demonstrate significant differences between the study groups. The clinical measurement of hamstring muscles length is often used in decision-making regarding the evaluation and treatment of children with CP (Cloodt et al., 2021). In this regard, Marsico et al. (2016b) showed how children with spasticity report a higher degree of limitation in the SLR and suggested that pain perception prevented children to achieve a larger ROM while performing the test. Several authors have found that increased pain is more frequently localized in the lower limbs (between 32% and 82% of cases) and to a lesser extent in the upper limbs (4%–19% of cases) (Doralp and Bartlett, 2010; Mckinnon et al., 2019), which severely limits physical function (Certanec Gonzalez and Icarte Barrientos, 2017). In fact, one in four children and youth with CP experience moderate to severe pain that restricts daily life activities, with hip subluxation/dislocation and dystonia being the most common causes of this limitation. Additionally, nearly 4% of children/youth with CP complain of severe pain that prevents most movement-related activities, which has a profound social and emotional burden, especially during the early ages (Penner et al., 2013).
From a clinical perspective, our findings highlight the importance of targeted, muscle-specific interventions for children with CP, particularly focusing on reducing stiffness in the rectus femoris and adductor muscles. Objective biomechanical measures, such as myotonometry, may facilitate early identification of stiffness, guiding individualized treatments. Addressing reduced ROM and increased pain can significantly improve functional outcomes, mobility, and quality of life.
Study limitations
As for the limitations of this study, we must mention that, despite the sample size estimation, the number of participants was not large enough to extrapolate the results. Also, participants with GMFCS level V were excluded, so it would be interesting to conduct the same study on a larger sample, including children and adolescents with GMFCS level V, in order to improve the generalizability of the findings. We did not collect data for the medication that children in the typically developing group may have been taking, which could potentially influence some of the current results. Despite the efforts to blind outcome assessors, due to the clinical characteristics of participants, an effective blinding was not feasible. Further studies should be developed to analyze and observe more accurately the intrinsic differences between spastic muscles and typical development muscles in children and adolescents.
Conclusion
Our findings suggest differences in muscle stiffness, ROM, and pain perception during the SLR test, between children with CP and their typically developing peers, particularly highlighting greater stiffness in specific lower limb muscles. These findings emphasize the importance of objective biomechanical assessment to guide targeted interventions aimed at reducing muscle stiffness and improving functional outcomes. Future research should explore longitudinal changes in muscle properties and investigate the effectiveness of specific therapeutic modalities informed by biomechanical measurements, thus further optimizing clinical management strategies for children with CP.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Biomedical Research Ethics Committee of the Andalusian Government, Spain (approval code: CI 0214-N-20) and the Ethics Committee for Research with Medicines of the Hospital Clínico San Carlos, Madrid (approval code: 24/544-E). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
RG-M: Conceptualization, Data curation, Writing – original draft, Writing – review and editing. VA-P: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review and editing. IM-E: Data curation, Writing – original draft, Writing – review and editing. AH-R: Conceptualization, Formal Analysis, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was partially funded by the Ilustre Colegio Profesional de Fisioterapeutas de Andalucía (ID number: AI-06/2022).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Agoriwo M. W., Muckelt P. E., Yeboah C. O., Sankah B. E. A., Agyapong-Badu S., Akpalu A., et al. (2022). Feasibility and reliability of measuring muscle stiffness in Parkinson’s Disease using MyotonPRO device in a clinical setting in Ghana. Ghana Med. J. 56, 78–85. doi:10.4314/gmj.v56i2.4
Agyapong-Badu S., Aird L., Bailey L., Mooney K., Mullix J., Warner M., et al. (2013). Interrater reliability of muscle tone, stiffness and elasticity measurements of rectus femoris and biceps brachii in healthy young and older males. Work. Pap. Heal. Sci. 1, 1–6.
Barney C. C., Stibb S. M., Merbler A. M., Summers R. L. S., Deshpande S., Krach L. E., et al. (2018). Psychometric properties of the brief pain inventory modified for proxy report of pain interference in children with cerebral palsy with and without cognitive impairment. PAIN Rep. 3, e666. doi:10.1097/PR9.0000000000000666
Beaudart C., Rolland Y., Cruz-Jentoft A. J., Bauer J. M., Sieber C., Cooper C., et al. (2019). Assessment of muscle function and physical performance in daily clinical practice: a position paper endorsed by the European society for clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO). Calcif. Tissue Int. 105, 1–14. doi:10.1007/s00223-019-00545-w
Bekteshi S., Vanmechelen I., Konings M., Ortibus E., Feys H., Monbaliu E. (2021). Clinical presentation of spasticity and passive range of motion deviations in dyskinetic cerebral palsy in relation to dystonia, choreoathetosis, and functional classification systems. Dev. Neurorehabil. 24, 205–213. doi:10.1080/17518423.2020.1858457
Bell S. (2014). The reliability and validity of the myotonometer as a measure of hamstring muscle stiffness. Medicine, 5631961.
Bhimani R., Anderson L. (2014). Clinical understanding of spasticity: implications for practice. Rehabil. Res. Pract. 2014, 279175–279210. doi:10.1155/2014/279175
Brandín-de la Cruz N., Calvo S., Rodríguez-Blanco C., Herrero P., Bravo-Esteban E. (2022). Effects of dry needling on gait and muscle tone in Parkinson’s disease: a randomized clinical trial. Acupunct. Med. 40, 3–12. doi:10.1177/09645284211039232
Certanec Gonzalez Z., Icarte Barrientos C. (2017). Dolor crónico en niños y jóvenes con parálisis cerebral. Rehabil. Integr. 12, 75–84.
Cloodt E., Krasny J., Jozwiak M., Rodby-Bousquet E. (2021). Interrater reliability for unilateral and bilateral tests to measure the popliteal angle in children and youth with cerebral palsy. BMC Musculoskelet. Disord. 22, 275. doi:10.1186/s12891-021-04135-6
Cloodt E., Lindgren A., Rodby-Bousquet E. (2024). Knee and ankle range of motion and spasticity from childhood into adulthood: a longitudinal cohort study of 3,223 individuals with cerebral palsy. Acta Orthop. 95, 200–205. doi:10.2340/17453674.2024.40606
Darrah J., Wiart L., Gorter J. W., Law M. (2014). Stability of serial range-of-motion measurements of the lower extremities in children with cerebral palsy: can we do better? Phys. Ther. 94, 987–995. doi:10.2522/ptj.20130378
Declerck M., Verheul M., Daly D., Sanders R. (2016). Benefits and enjoyment of a swimming intervention for youth with cerebral palsy: an RCT study. Pediatr. Phys. Ther. 28, 162–169. doi:10.1097/PEP.0000000000000235
Doralp S., Bartlett D. J. (2010). The prevalence, distribution, and effect of pain among adolescents with cerebral palsy. Pediatr. Phys. Ther. 22, 26–33. doi:10.1097/PEP.0b013e3181ccbabb
Drenth H., Zuidema S. U., Krijnen W. P., Bautmans I., Van Der Schans C., Hobbelen H. (2018). Psychometric properties of the MyotonPRO in dementia patients with paranoia. Gerontology 64, 401–412. doi:10.1159/000485462
García-Bernal M. I., González-García P., Casuso-Holgado M. J., Cortés-Vega M. D., Heredia-Rizo A. M. (2022). Measuring mechanical properties of spastic muscles after stroke. Does muscle position during assessment really matter? Arch. Phys. Med. Rehabil. 103, 2368–2374. doi:10.1016/j.apmr.2022.05.012
García-Bernal M. I., González-García P., Madeleine P., Casuso-Holgado M. J., Heredia-Rizo A. M. (2023). Characterization of the structural and mechanical changes of the biceps brachii and gastrocnemius muscles in the subacute and chronic stage after stroke. Int. J. Environ. Res. Public Health 20, 1405. doi:10.3390/ijerph20021405
García-Bernal M. I., Heredia-Rizo A. M., González-García P., Casuso-Holgado M. J. (2021). Validity and reliability of myotonometry for assessing muscle viscoelastic properties in patients with stroke: a systematic review and meta-analysis. Sci. Rep. 11 (1), 5062. doi:10.1038/s41598-021-84656-1
García-Rueda L., Cabanas-Valdés R., Salgueiro C., Rodríguez-Sanz J., Pérez-Bellmunt A., López-de-Celis C. (2023). Immediate effects of TECAR therapy on gastrocnemius and quadriceps muscles with spastic hypertonia in chronic stroke survivors: a randomized controlled trial. Biomedicines 11, 2973. doi:10.3390/biomedicines11112973
Goo M., Tucker K., Johnston L. M. (2018). Muscle tone assessments for children aged 0 to 12 years: a systematic review. Dev. Med. Child. Neurol. 60, 660–671. doi:10.1111/dmcn.13668
Handsfield G. G., Williams S., Khuu S., Lichtwark G., Stott N. S. (2022). Muscle architecture, growth, and biological Remodelling in cerebral palsy: a narrative review. BMC Musculoskelet. Disord. 23, 233–317. doi:10.1186/s12891-022-05110-5
Herrero P., Carrera P., García E., Gámez-Trullén E. M., Oliván-Blázquez B. (2011). Reliability of goniometric measurements in children with cerebral palsy: a comparative analysis of universal goniometer and electronic inclinometer. A pilot study. BMC Musculoskelet. Disord. 12, 155. doi:10.1186/1471-2474-12-155
Hidler J. M., Rymer W. Z. (1999). A simulation study of reflex instability in spasticity: origins of clonus. IEEE Trans. Rehabil. Eng. 7, 327–340. doi:10.1109/86.788469
Johansen M., Haslund-Thomsen H., Kristensen J., Thorgaard Skou S. (2020). Photo-based range-of-motion measurement: reliability and concurrent validity in children with cerebral palsy. Pediatr. Phys. Ther. 32, 151–160. doi:10.1097/PEP.0000000000000689
Kingsnorth S., Orava T., Provvidenza C., Adler E., Ami N., Gresley-Jones T., et al. (2015). Chronic pain assessment tools for cerebral palsy: a systematic review. Pediatrics 136, e947–e960. doi:10.1542/peds.2015-0273
Kutlutürk Yıkılmaz S., Çevik Saldıran T., Öztürk Ö., Öktem S. (2024). Intersession intra-rater and inter-rater reliability of myotonometer for upper and lower extremity muscles in children with spinal muscular atrophy. Diagnostics 14, 2300. doi:10.3390/diagnostics14202300
Lackritz H., Parmet Y., Frenkel-Toledo S., Baniña M. C., Soroker N., Solomon J. M., et al. (2021). Effect of post-stroke spasticity on voluntary movement of the upper limb. J. Neuroeng. Rehabil. 18, 81–14. doi:10.1186/s12984-021-00876-6
Lee S. Y., Sung K. H., Chung C. Y., Lee K. M., Kwon S. S., Kim T. G., et al. (2015). Reliability and validity of the Duncan-Ely test for assessing rectus femoris spasticity in patients with cerebral palsy. Dev. Med. Child. Neurol. 57, 963–968. doi:10.1111/dmcn.12761
Lieber R. L., Fridén J. (2019). Muscle contracture and passive mechanics in cerebral palsy. J. Appl. Physiol. 126, 1492–1501. doi:10.1152/japplphysiol.00278.2018
Lindén O., Hägglund G., Rodby-Bousquet E., Wagner P. (2019). The development of spasticity with age in 4,162 children with cerebral palsy: a register-based prospective cohort study. Acta Orthop. 90, 286–291. doi:10.1080/17453674.2019.1590769
Lukas K., Gutschmidt K., Schoser B., Wenninger S. (2023). Evaluation of myotonometry for myotonia, muscle stiffness and elasticity in neuromuscular disorders. J. Neurol. 270, 5398–5407. doi:10.1007/s00415-023-11867-z
Marsico P., Tal-Akabi A., van Hedel H. J. A. (2016a). The relevance of nerve mobility on function and activity in children with Cerebral Palsy. BMC Neurol. 16, 194–199. doi:10.1186/s12883-016-0715-z
Marsico P., Tal-Akabi A., Van Hedel H. J. A. (2016b). Reliability and practicability of the straight leg raise test in children with cerebral palsy. Dev. Med. Child. Neurol. 58, 173–179. doi:10.1111/dmcn.12797
McDowell B. C., Salazar-Torres J. J., Kerr C., Cosgrove A. P. (2012). Passive range of motion in a population-based sample of children with spastic cerebral palsy who walk. Phys. Occup. Ther. Pediatr. 32, 139–150. doi:10.3109/01942638.2011.644032
Mckinnon C. T., Meehan E. M., Harvey A. R., Antolovich G. C., Morgan P. E. (2019). Prevalence and characteristics of pain in children and young adults with cerebral palsy: a systematic review. Dev. Med. Child. Neurol. 61, 305–314. doi:10.1111/dmcn.14111
Milinis K., Young C. A.Trajectories of Outcome in Neurological Conditions TONiC study (2016). Systematic review of the influence of spasticity on quality of life in adults with chronic neurological conditions. Disabil. Rehabil. 38, 1431–1441. doi:10.3109/09638288.2015.1106592
Nordmark E., Hägglund G., Lauge-Pedersen H., Wagner P., Westbom L. (2009). Development of lower limb range of motion from early childhood to adolescence in cerebral palsy: a population-based study. BMC Med. 7, 65–11. doi:10.1186/1741-7015-7-65
Nourizadeh M., Shadgan B., Abbasidezfouli S., Juricic M., Mulpuri K. (2024). Methods of muscle spasticity assessment in children with cerebral palsy: a scoping review. J. Orthop. Surg. Res. 19, 401–415. doi:10.1186/s13018-024-04894-7
Penner M., Xie W. Y., Binepal N., Switzer L., Fehlings D. (2013). Characteristics of pain in children and youth with cerebral palsy. Pediatrics 132, e407–e413. doi:10.1542/peds.2013-0224
Rosenbaum P. L., Palisano R. J., Bartlett D. J., Galuppi B. E., Russell D. J. (2008). Development of the gross motor function classification system for cerebral palsy. Dev. Med. Child. Neurol. 50, 249–253. doi:10.1111/j.1469-8749.2008.02045.x
Sagerer E., Wirner-Piotrowski C., Mijic M., Arndt M., Garcia-Angarita N., Schoser B., et al. (2024). Nociceptive pain in patients with neuromuscular disorders: a cross-sectional clinical study. J. Neuromuscul. Dis. 11, 1111–1122. doi:10.3233/JND-240068
Seo H., Kim J., Yu C., Lim H. (2023). Intra-rater and inter-rater reliability analysis of muscle-tone evaluation using a myotonometer for children with developmental disabilities. Healthcare 11, 782. doi:10.3390/healthcare11060782
Shearer H. M., Verville L., Côté P., Hogg-Johnson S., Fehlings D. L. (2023). Clinical course of pain intensity in individuals with cerebral palsy: a prognostic systematic review. Dev. Med. Child. Neurol. 65, 24–37. doi:10.1111/dmcn.15358
Shu X., McConaghy C., Knight A. (2021). Validity and reliability of the Modified Tardieu Scale as a spasticity outcome measure of the upper limbs in adults with neurological conditions: a systematic review and narrative analysis. BMJ Open 11, 0507111–e50810. doi:10.1136/bmjopen-2021-050711
Trompetto C., Marinelli L., Mori L., Pelosin E., Currà A., Molfetta L., et al. (2014). Pathophysiology of spasticity: implications for neurorehabilitation. Biomed. Res. Int. 2014, 354906. doi:10.1155/2014/354906
Trybulski R., Kużdżał A., Wilk M., Więckowski J., Fostiak K., Muracki J. (2024). Reliability of MyotonPro in measuring the biomechanical properties of the quadriceps femoris muscle in people with different levels and types of motor preparation. Front. Sport. Act. Living 6, 1453730–1453813. doi:10.3389/fspor.2024.1453730
Upachit T., Piyaselakul S., Srivanitchapoom P., Tretriluxana J. (2025). Investigation of passive tone and viscoelasticity in neck muscles in pre-symptomatic neck flexion abnormality in Parkinson’s disease: observational study. J. Bodyw. Mov. Ther. 42, 397–401. doi:10.1016/j.jbmt.2025.01.012
Vural M., Yalcinkaya E. Y., Celik E. C., Gunduz B., Bozan A., Erhan B. (2020). Assessment of quality of life in relation to spasticity severity and socio-demographic and clinical factors among patients with spinal cord injury. J. Spinal Cord. Med. 43, 193–200. doi:10.1080/10790268.2018.1543093
Więch P., Ćwirlej-Sozańska A., Wiśniowska-Szurlej A., Kilian J., Lenart-Domka E., Bejer A., et al. (2020). The relationship between body composition and muscle tone in children with cerebral palsy: a case-control study. Nutrients 12, 1–12. doi:10.3390/nu12030864
Keywords: cerebral palsy, muscle stiffness, spasticity, pain perception, myotonometry
Citation: González-Matilla R, Abuín-Porras V, Mínguez-Esteban I and Heredia-Rizo AM (2025) Biomechanical and clinical differences in muscle tone, stiffness, range of motion, and pain perception in children with cerebral palsy: a cross-sectional study. Front. Physiol. 16:1588084. doi: 10.3389/fphys.2025.1588084
Received: 05 March 2025; Accepted: 27 March 2025;
Published: 15 April 2025.
Edited by:
Bruno Bastide, Lille University of Science and Technology, FranceReviewed by:
Madhurima Saha, University of Florida, United StatesExal Garcia-Carrillo, Universidad Bernardo O’Higgins, Chile
Copyright © 2025 González-Matilla, Abuín-Porras, Mínguez-Esteban and Heredia-Rizo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vanesa Abuín-Porras, dmFuZXNhLmFidWluQHVuaXZlcnNpZGFkZXVyb3BlYS5lcw==