
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Physiol., 27 March 2025
Sec. Gastrointestinal Sciences
Volume 16 - 2025 | https://doi.org/10.3389/fphys.2025.1541020
 Bruno Vincenzi1
Bruno Vincenzi1 Mao Yimin2
Mao Yimin2 Raúl J. Andrade3,4Mauricio Morales Castillo5
Raúl J. Andrade3,4Mauricio Morales Castillo5 Gamar Akhundova-Unadkat5*
Gamar Akhundova-Unadkat5* José M. Mato6
José M. Mato6Drug-induced liver injury (DILI) is a leading cause of drug withdrawal, a particular cause for concern among patients receiving anti-cancer treatment. This review summarizes the available evidence on the efficacy of hepatoprotective drugs in normalizing liver enzyme abnormalities among patients with DILI due to treatment with anti-cancer therapies. Across relevant publications, the effects of several compounds on anti-cancer therapy-induced DILI were assessed. Treatment with hepatoprotective agents which is usually initiated after DILI has been detected and involves cessation of causative anti-cancer therapy, has demonstrated improvements in liver enzyme elevation. However, prophylactic treatment with two agents in particular, ademetionine and bicyclol have shown hepatoprotective effects that enabled patients to continue with their anti-cancer therapy with a reduced subsequently reduced risk of hepatotoxicity. While these publications show some evidence for the benefits of hepatoprotective agents among patients with DILI due to anti-cancer therapy, more research is needed to fully determine the effects of hepatoprotective drugs in resolving DILI signs and symptoms among patients receiving treatment for cancer.
The liver is a prime target for medication-induced damage due to its central role in drug metabolism (Yuan and Kaplowitz, 2013). Drug-induced liver injury (DILI) may be caused by a broad range of pharmaceutical agents including clinical medications and herbal and dietary supplements (Chalasani et al., 2021; Pinazo-Bandera et al., 2023). It is the most common cause of acute liver failure (ALF), and consequently, liver transplant, in both Europe and the US (Bernal and Wendon, 2013; Lee, 2003; Katarey and Verma, 2016). Furthermore, it is a leading cause of drug withdrawal (Ye et al., 2018). In an analysis of 133 drugs withdrawn from the market due to safety reasons between 1990 and 2010, the most common reasons were hepatotoxicity (27.1%) and cardiotoxicity (18.8%) (Craveiro et al., 2020). The true incidence of DILI varies from country to country and across populations and is challenging to estimate with the true incidence likely to be higher than reported (Li et al., 2022a). In population studies, the annual incidence is reported between 2.7 and 19 per 100,000 persons per year (Björnsson, 2024). A recent systematic review and meta-analysis of 14 population-based studies reported the overall incidence of DILI as 4.94 per 100,000 person-years (95% CI: 4.05–5.83), with the highest incidence in Asia (17.82 per 100 00) person-years [95% CI: 6.26–29.38] (Li et al., 2023).
DILI may be intrinsic (or direct) or idiosyncratic. Intrinsic DILI is usually predictable and dose-related with a relatively short time to onset, while idiosyncratic DILI occurs less frequently and is usually unrelated to dose (Brennan et al., 2022). One of the major causes of idiosyncratic DILI is anti-cancer therapy. Anti-cancer therapies known to increase the risk of DILI include chemotherapy, tyrosine kinase inhibitors, and immunotherapies such as immune checkpoint inhibitors that target cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed cell death protein (PD-1) (Vincenzi et al., 2018). DILI caused by anti-cancer therapy is unpredictable, unrelated to dose, and is the leading cause of dose reductions or cycle delays. Furthermore, it can affect outcomes and subsequent treatment choices (Mudd and Guddati, 2021; Vincenzi et al., 2016; Cunningham et al., 2024). The mainstay of treatment for DILI is early recognition and withdrawal of the likely causative agent(s), assessment of liver injury, and close observation for resolution (Ye et al., 2018; Brennan et al., 2022). Chemotherapy agents are hepatotoxic through multiple pathways, thus producing different types of liver injury including elevation of liver enzymes, drug-induced hepatitis, veno-occlusive disease, steatohepatitis, fibrosis and liver failure (Vincenzi et al., 2018; Mudd and Guddati, 2021; Vincenzi et al., 2016). For example, oxaliplatin may cause elevations of liver enzymes but is commonly associated with sinusoidal and vascular injury to the liver which can lead to sinusoidal obstruction syndrome (Vincenzi et al., 2018; Mudd and Guddati, 2021). Immune checkpoint inhibitor-associated hepatoxicity generally manifests as autoimmune hepatitis, although immune-mediated cholangitis can also occur (Vincenzi et al., 2018; Cunningham et al., 2024). In some cases, spontaneous recovery from hepatotoxic effects occurs, without the need for supportive measures (Cunningham et al., 2024; Dara and Ghabril, 2024; Da et al., 2022). Therapeutic options for DILI are very limited. Corticosteroids may be useful in instances where acute autoimmune hepatitis cannot be excluded or to treat hepatotoxicity due to immune checkpoint inhibitors (Brennan et al., 2022; Andrade et al., 2019). Other immunosuppressants such as mycophenolate mofetil have also been used either alongside or as an alternative to corticosteroids (Andrade et al., 2019). Hepatoprotective drugs that have been used for DILI aim to improve liver function, promote liver cell regeneration and/or enhance liver detoxification (Niu et al., 2021). Although there is no unified classification, they can be grouped by mechanism of action into detoxification drugs (e.g., N-acetylcysteine and glutathione), anti-inflammatory drugs (e.g., glycyrrhizic acid), hepatocyte membrane protectors (e.g., polyene phosphatidylcholine), and antioxidants (e.g., bicyclol, silymarin) (Li et al., 2021).
Ademetionine (AdoMet), the main product of methionine metabolism, has been proposed as a therapeutic option for cholestasis owing to DILI. Ademetionine plays a key role in methylation reactions, epigenetic regulation, detoxification reactions, phospholipid synthesis, and glutathione synthesis. It is indicated (via oral, intravenous, or intramuscular routes) for the treatment of adults with intrahepatic cholestasis (IHC) in pre-cirrhotic and cirrhotic stages, as well as IHC in pregnancy, depressive symptoms, and relief of fatigue caused by chronic liver disease; studies have shown anti-proliferative effects in models of breast, colorectal, and liver cancers (Li et al., 2015; Ansorena et al., 2002; Lu et al., 2009; Lu and Mato, 2008). This review focuses on available evidence for the efficacy of hepatoprotective drugs in preventing liver enzyme abnormalities among patients with DILI due to treatment with anti-cancer therapies.
Several studies have assessed the effects of hepatoprotective agents among patients with DILI due to anti-cancer therapies (Table 1). These therapies include ademetionine, bicyclol, glucocorticoids, magnesium isoglycyrrhizinate, monoclonal antibodies and silymarin.
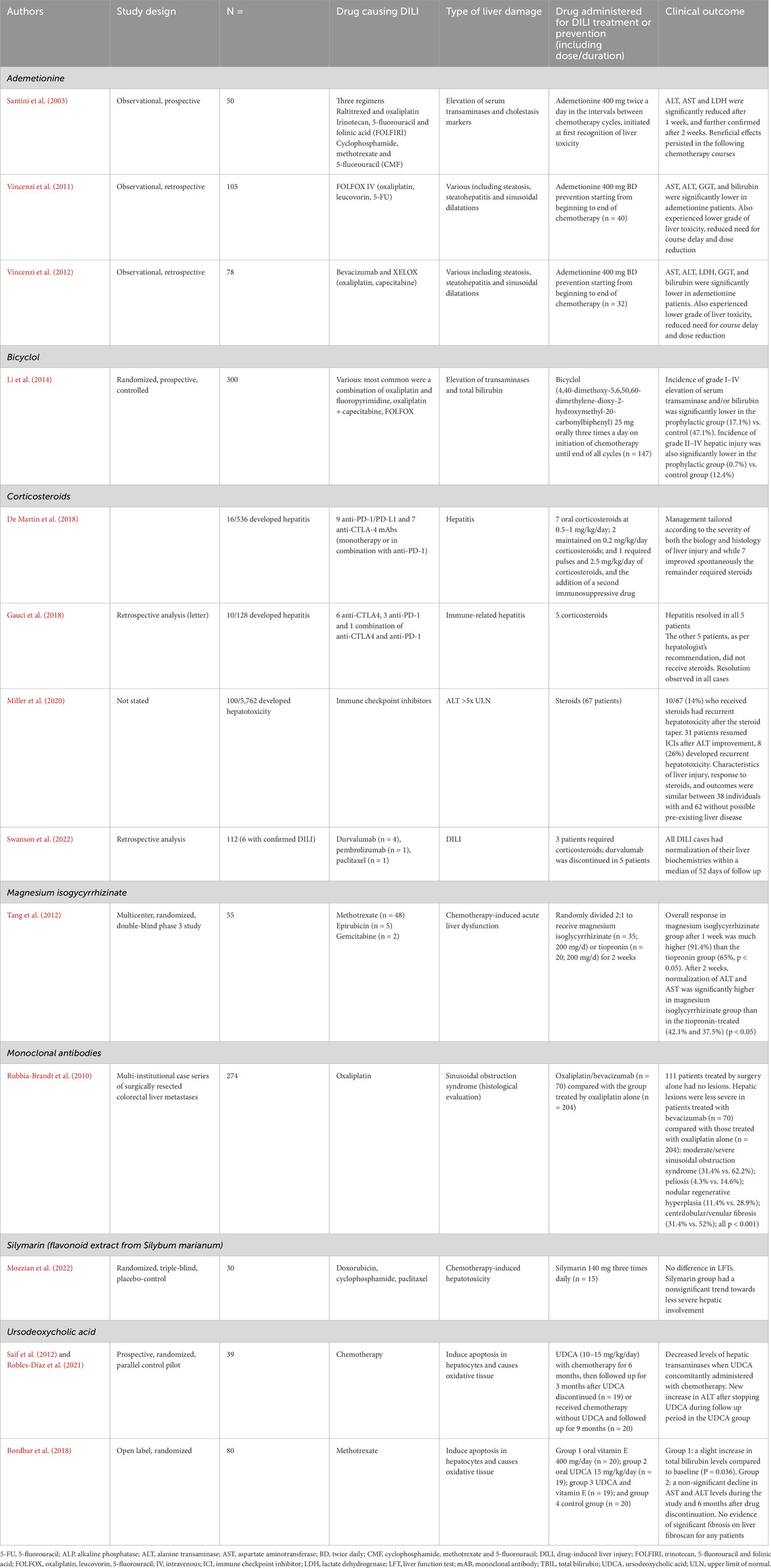
Table 1. Summary of study designs, patient characteristics, DILI cause and type and clinical outcomes for the identified studies.
Across 3 studies, 1 prospective study (Santini et al., 2003) and 2 retrospective analyses (Vincenzi et al., 2012; Vincenzi et al., 2011), ademetionine improved or prevented liver enzyme abnormalities among patients with DILI. In the prospective study, AST, ALT and LDH levels were significantly reduced after 1 week of therapy (Table 1) and the effects on these enzymes persisted in subsequent chemotherapy courses allowing patients to receive their scheduled chemotherapy courses with a minimal number of dose reductions or administration delays (Santini et al., 2003). In both retrospective analyses, ademetionine was administered from the beginning to the end of chemotherapy as a preventative measure. Treatment with (compared to without) ademetionine was associated with significantly lower median levels of AST, ALT and γ-GT at the end of adjuvant therapy an also a lower grade of liver toxicity and a reduced need of course delay and dose reduction (Table 1) (Vincenzi et al., 2012; Vincenzi et al., 2011).
Bicyclol, a synthetic drug developed in China, is used to treat inflammatory liver injury. It protects liver cells by stabilizing cell membranes, scavenging free radicals, modulating oxidative stress, inhibiting inflammatory cytokines and promoting autophagic flux (Benić et al., 2022; Zhao et al., 2020). The effect of bicyclol on anti-cancer therapy-induced DILI was assessed in a 2014 study (Zhao et al., 2020). Among 300 patients aged ≥60 years treated for cancer (included colorectal, lung, gastric, lymphoma, pancreas, bile duct and ampulla), incidence of grade I-IV elevation of serum transaminase and/or bilirubin was significantly lower in patients treated with chemotherapy supplemented with daily bicyclol compared with patients treated with chemotherapy alone (Table 1). Chemotherapy included combination regimens with oxaliplatin and fluoropyrimidine, docetaxel, gemcitabine, irinotecan, etoposide and paclitaxel. There were no significant differences between groups regarding cancer types, disease staging, previous chemotherapy and complicating liver metastasis. The incidence of grade II-IV hepatic injury was also significantly lower in the prophylactic group than in the control group (Li et al., 2014). In addition, results of a multicenter, randomized, phase II trial demonstrated the efficacy of bicyclol (low-dose 25 mg times a day, high-dose 50 mg TID vs. polyene phosphatidylcholine control) in the treatment of patients with idiosyncratic acute DILI with significant higher ALT normalization rates at weeks 1, 2, 4, 6 and 8 compared with polyene phosphatidylcholine control. Bicyclol has been included in local guidelines based on this data and a phase 3 trial is ongoing (Tang et al., 2022). It is also useful to note that Abbott sold its non-U.S. developed markets specialty and branded generics business to the company Viatris on 27 February 2015.
Glucocorticoids are often used in the management of DILI owing to their anti-inflammatory, immunosuppressive and antiallergic effects (Li et al., 2022b). Across four retrospective studies among patients treated with corticosteroids for DILI (De Martin et al., 2018; Gauci et al., 2018; Miller et al., 2020; Swanson et al., 2022), most DILI cases resolved following corticosteroid treatment, with a small number requiring maintenance low-dose corticosteroids or additional treatment (Table 1). The first retrospective analysis included 536 patients treated with anti-PD-1/PD-L1 or CTLA-4 immunotherapies, 16 of whom developed grade ≥3 hepatitis and underwent liver investigations. These included viral assays, autoimmune tests and liver biopsy, histological review, and immunostaining of liver specimens (De Martin et al., 2018). Treatment was tailored depending on the severity of liver injury; six patients improved spontaneously, seven received oral corticosteroids at 0.5–1 mg/kg/day, two were maintained on 0.2 mg/kg/day corticosteroids, and one required 2.5 mg/kg/day corticosteroids and the addition of a second immunosuppressive drug. It is important to note that in 37.5% (6/16) patients treated with immune checkpoint inhibitors, the biochemical abnormalities of DILI improved spontaneously, and thus did not require any treatment (De Martin et al., 2018). In the second retrospective analysis, among 10 patients with hepatitis due to anti-CTLA-4 and/or anti-PD-1, hepatitis resolved in 5 patients following corticosteroid treatment and spontaneously in the other 5 patients (Gauci et al., 2018). A total of 100 of 5,762 patients developed DILI after receiving immune checkpoint inhibitor treatment in the third retrospective analysis (Miller et al., 2020). Of the 67 patients who received steroids, only 10 had recurrent hepatotoxicity after steroids taper. Finally, in a retrospective analysis of 6 patients with confirmed DILI (4 following durvalumab treatment, 1 following pembrolizumab treatment and 1 following paclitaxel treatment), 3 patients required corticosteroids, and all DILI cases resolved within a median of 52 days of follow up (Swanson et al., 2022).
Magnesium isoglycyrrhizinate, refined from glycyrrhizic acid which is extracted from the roots of herb Glycyrrhiza glabra, has been shown to have anti-inflammatory, anti-oxidative and hepatoprotective effects (Benić et al., 2022; Li et al., 2022b). It scavenges free radicals, prevents the increase of serum transaminase, reduces hepatocyte degeneration, and reduces necrosis and inflammatory cell infiltration (Benić et al., 2022; Tang et al., 2015). In a multicentre, randomized, double-blind study comparing the effects of magnesium isoglycyrrhizinate with tiopronin among 55 patients with chemotherapy-induced DILI due to methotrexate, epirubicin and gemcitabine (Tang et al., 2012), overall response was significantly higher among patients receiving magnesium isoglycyrrhizinate than patients receiving troponin (Table 1). Furthermore, significantly higher proportions of patients on magnesium isoglycyrrhizinate achieved ALT and AST normalisation after 2 weeks compared with those on tiopronin (Table 1).
The effects of the monoclonal antibody bevacizumab on DILI were assessed among patients with colorectal liver metastases treated with oxaliplatin (Rubbia-Brandt et al., 2010). Hepatic lesions identified through histological evaluation were less severe in patients treated with oxaliplatin/bevacizumab compared with those treated with oxaliplatin alone, with a lower incidence of moderate/severe sinusoidal obstruction syndrome (31.4% versus 62.2%), peliosis (4.3% versus 14.6%), nodular regenerative hyperplasia (11.4% versus 28.9%) and centrilobular/venular fibrosis (31.4% versus 52%). However, the hepatoprotective effects of bevacizumab were not evaluated further.
Silymarin, a flavonoid extracted from the seeds and fruit of Silybum marianum, with antioxidant, antifibrotic and anti-inflammatory properties, has been used as a hepatoprotective agent (Gillessen et al., 2022; Tao et al., 2019). A randomized, triple-blind, placebo-controlled trial in 30 patients with non-metastatic breast cancer assessed the effects of silymarin on DILI induced by treatment with doxorubicin/cyclophosphamide-paclitaxel (AC-T) (Moezian et al., 2022). There was a non-significant trend towards more severe liver involvement in patients receiving placebo compared with those receiving silymarin, based on ultrasonography (p = 0.083). However, no between-group differences in liver involvement were seen based on FibroScan and liver function tests.
Ursodeoxycholic acid (UDCA) has an anti-apoptotic effect on hepatocytes by stabilizing the cell membrane and can protect from damage induced by anti-cancer therapies (Goossens and Bailly, 2019; Bordbar et al., 2018). For example, in a prospective randomized parallel study in 39 children with acute lymphoblastic leukemia (ALL) randomized to receive chemotherapy with or without UDCA for 6 months, all followed up for a further 3 months, UDCA treated patients had a trend towards decreased levels of aminotransferases (Saif et al., 2012; Robles-Díaz et al., 2021). In contrast, in an open-label study in 80 pediatric patients with B-cell ALL on maintenance methotrexate treatment, UDCA and vitamin E (antioxidant) treatment showed minimal hepatoprotective benefit (Bordbar et al., 2018).
This review describes the available evidence evaluating the efficacy of hepatoprotective agents in normalizing liver enzyme abnormalities among patients who developed DILI due to anti-cancer therapies. While the mainstay of DILI treatment is the prompt removal of the causative agent, which often leads to spontaneous recovery, this need to be balanced with a need to avoid further deterioration in liver function and understanding of when to initiate appropriate hepatoprotective treatment (Hosack et al., 2023). Covering a range of hepatoprotective drugs including ademetionine, bicyclol, corticosteroids and silymarin, the publications consistently demonstrated improvements in liver enzyme elevations following treatment. However, the number of studies with ani-cancer drugs associated DILI is limited, and often the number of patients involved are small.
The data presented in this review are in line with a growing body of evidence demonstrating the efficacy of hepatoprotective therapies for DILI treatment. While well-designed randomized controlled studies are still needed in many cases to confirm the efficacy of these agents, several real-world database studies have shown efficacy in patients with DILI including with bicyclol, silybin meglumine (water-soluble form of silymarin), and glycyrrhizin injections (Wang et al., 2019; Yao et al., 2022; Zhang et al., 2022; Wang et al., 2021). These studies are important given that DILI is costly, both with regard to healthcare expenditure and in relation to the human toll (Lisi, 2016). DILI during anti-cancer treatment is a particular cause for concern as treatment dose reduction, delay, or discontinuation has the potential to negatively affect clinical outcomes including overall survival (Azad et al., 2018; Mondaca et al., 2020; Regev et al., 2020). Generally, treatment with hepatoprotective agents in the included studies was combined with cessation of causative anti-cancer therapy. However, in some studies hepatoprotective treatments were given prophylactically, enabling patients to continue with their anti-cancer therapy without liver toxicity. For example, in two studies, ademetionine was given from initiation of chemotherapy, reducing the need for course delay and dose reduction (Vincenzi et al., 2012; Vincenzi et al., 2011). In another study, bicyclol was given three times daily on initiation of chemotherapy, significantly lowering the incidence of grade I-IV serum transaminase elevation (Li et al., 2014).
Although ademetionine protects against apoptosis in normal hepatocytes by inhibiting cytochrome C release, it induces apoptosis in liver cancer cell lines HepG2 and HuH-7 (Ansorena et al., 2002). These findings align with the reported chemo-preventive effects of ademetionine demonstrated in an in vivo model of chemical hepatocarcinogenesis in rats (Lu et al., 2009). Furthermore, the protective effect of ademetionine supplementation was demonstrated in patients with resected colorectal cancer who were treated with the FOLFOX IV adjuvant regimen (Vincenzi et al., 2011). The available evidence therefore strongly suggests that ademetionine does not compromise the antitumor efficacy of chemotherapy and, instead, may enhance treatment outcomes by protecting normal cells, reducing oxidative stress, and restoring epigenetic balance. Further clinical trials are needed to fully establish the optimal use of ademetionine in combination with chemotherapy and to explore its potential in different cancer types and treatment regimens (Fernández-Ramos et al., 2025).
The clinical manifestations of DILI are heterogeneous and its severity varies from mild liver function elevations to the development of severe liver injury/disease (Hassan and Fontana, 2019). This was highlighted in the current review, which described publications demonstrating a range of liver enzyme elevations necessitating a number of different treatment approaches. The varying clinical approaches taken in these clinical cases highlight the unmet clinical and regulatory challenges and areas for future research that remain in relation to DILI management (Brennan et al., 2022; McGill and Jaeschke, 2019). First, DILI is difficult to predict, diagnose, and treat because its presentation is similar to many hepatobiliary disorders (Ye et al., 2018). As such, there is a need for specific non-invasive diagnostic tests, approved biomarkers and evidence-based diagnostic scales to reduce the reliance on exclusion of other causes of liver disease. The lack of diagnostic tools is compounded by limited mechanistic understanding of toxicity (Grove et al., 2023). Further information in this area would support development and approval of optimal DILI management paradigms. Importantly, this review also highlights a lack of properly designed clinical trials evaluating the efficacy of new treatments as well as older drugs (Andrade et al., 2019; Garcia-Cortes et al., 2020). Further research in this area is required, particularly in the context of anti-cancer therapy-induced DILI, in order to determine the best treatment approaches that will allow patients to continue with their cancer treatment and maximize clinical outcomes.
This review summarizes the available evidence for the benefits of hepatoprotective agents among patients with DILI due to anti-cancer therapy, with some agents such as ademetionine allowing patients to remain on therapy with a reduced need for dose reductions or delays. However, the review also emphasizes the need for more clinical evidence on the efficacy of hepatoprotective agents in the treatment of DILI caused by anti-cancer therapies, and their potential role as prophylactic therapy. Given the substantial clinical relevance of DILI during anti-cancer treatment, i.e., reduction, delay or discontinuation of anti-cancer therapy and the potential impact on clinical outcomes, these data will provide clinicians with important evidence to support treatment decisions for clinically vulnerable patients.
BV: Conceptualization, Writing–original draft, Writing–review and editing. MY: Conceptualization, Writing–original draft, Writing–review and editing. RA: Conceptualization, Writing–original draft, Writing–review and editing. MM: Conceptualization, Writing–original draft, Writing–review and editing. GA-U: Conceptualization, Writing–original draft, Writing–review and editing. JM: Conceptualization, Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Abbott Operations Switzerland. Editorial assistance was provided by Metamols Ltd., funded by Abbott Operations Switzerland.
BV reports consulting fees from Eisai, Lilly, Bayer, Deciphera, PharmaMar, Blueprint, Pfizer, GSK, Accord, Abbott and research support from PharmaMar, Novartis, and Lilly; MY reports no conflicts of interest; RA reports consulting fees from Abbott, Bayer, Boehringer Ingelhein, ENYO, InnoCare Janssen, Johnson & Johnson, Novo-Nordisk, Obseva, Roche, Sanofi, Silence Therapeutics and Vivet; MM and GA-U are employees of Abbott Products Operations AG, Allschwil, Switzerland and own shares in Abbott; JMM has no conflict of interest to declare.
The authors declare that this study received funding from Abbott Operations Switzerland. The funder had the following involvement in the study: study design, decision to publish, and preparation of the manuscript.
The reviewer RL declared a shared affiliation with the authors YM to the handling editor at the time of review.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Andrade R. J., Chalasani N., Bjornsson E. S., Suzuki A., Kullak-Ublick G. A., Watkins P. B., et al. (2019). Drug-induced liver injury. Nat. Rev. Dis. Prim. 5 (1), 58. doi:10.1038/s41572-019-0105-0
Ansorena E., Garcia-Trevijano E. R., Martinez-Chantar M. L., Huang Z. Z., Chen L., Mato J. M., et al. (2002). S-adenosylmethionine and methylthioadenosine are antiapoptotic in cultured rat hepatocytes but proapoptotic in human hepatoma cells. Hepatology 35 (2), 274–280. doi:10.1053/jhep.2002.30419
Azad A., Chang P., Devuni D., Bichoupan K., Kesar V., Branch A. D., et al. (2018). Real world experience of drug induced liver injury in patients undergoing chemotherapy. J. Clin. Gastroenterol. Hepatol. 2 (3), 18. doi:10.21767/2575-7733.1000047
Benić M. S., Nežić L., Vujić-Aleksić V., Mititelu-Tartau L. (2022). Novel therapies for the treatment of drug-induced liver injury: a systematic review. Front. Pharmacol. 12, 785790. doi:10.3389/fphar.2021.785790
Bernal W., Wendon J. (2013). Acute liver failure. N. Engl. J. Med. 369 (26), 2525–2534. doi:10.1056/NEJMra1208937
Björnsson E. S. (2024). The epidemiology of newly recognized causes of drug-induced liver injury: an update. Pharm. (Basel) 17 (4), 520. doi:10.3390/ph17040520
Bordbar M., Shakibazad N., Fattahi M., Haghpanah S., Honar N. (2018). Effect of ursodeoxycholic acid and vitamin E in the prevention of liver injury from methotrexate in pediatric leukemia. Turk J. Gastroenterol. 29 (2), 203–209. doi:10.5152/tjg.2018.17521
Brennan P. N., Cartlidge P., Manship T., Dillon J. F. (2022). Guideline review: easl clinical practice guidelines: drug-induced liver injury (DILI). Frontline Gastroenterol. 13 (4), 332–336. doi:10.1136/flgastro-2021-101886
Chalasani N. P., Maddur H., Russo M. W., Wong R. J., Reddy K. R.Practice Parameters Committee of the American College of Gastroenterology (2021). ACG clinical guideline: diagnosis and management of idiosyncratic drug-induced liver injury. Am. J. Gastroenterol. 116 (5), 878–898. doi:10.14309/ajg.0000000000001259
Craveiro N. S., Lopes B. S., Tomás L., Almeida S. F. (2020). Drug withdrawal due to safety: a review of the data supporting withdrawal decision. Curr. Drug Saf. 15 (1), 4–12. doi:10.2174/1574886314666191004092520
Cunningham M., Gupta R., Butler M. (2024). Checkpoint inhibitor hepatotoxicity: pathogenesis and management. Hepatology 79 (1), 198–212. doi:10.1097/HEP.0000000000000045
Da C. T., Wu G. Y., Vaziri H. (2022). Immunotherapy-induced hepatotoxicity: a review. J. Clin. Transl. Hepatol. 10 (6), 1194–1204. doi:10.14218/JCTH.2022.00105
Dara L., Ghabril M. (2024). A state-of-the-art update on hepatotoxicity: introduction to the special series on drug-induced liver injury. Clin. Liver Dis. Hob. 23 (1), e0212. doi:10.1097/CLD.0000000000000212
De Martin E., Michot J. M., Papouin B., Champiat S., Mateus C., Lambotte O., et al. (2018). Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 68 (6), 1181–1190. doi:10.1016/j.jhep.2018.01.033
Fernández-Ramos D., Lopitz-Otsoa F., Lu S. C., Mato J. M. (2025). S-adenosylmethionine: a multifaceted regulator in cancer pathogenesis and therapy. Cancers (Basel) 17 (3), 535. doi:10.3390/cancers17030535
Garcia-Cortes M., Robles-Diaz M., Stephens C., Ortega-Alonso A., Lucena M. I., Andrade R. J. (2020). Drug induced liver injury: an update. Arch. Toxicol. 94 (10), 3381–3407. doi:10.1007/s00204-020-02885-1
Gauci M. L., Baroudjian B., Zeboulon C., Pages C., Pote N., Roux O., et al. (2018). Immune-related hepatitis with immunotherapy: are corticosteroids always needed? J. Hepatol. 69 (2), 548–550. doi:10.1016/j.jhep.2018.03.034
Gillessen A., Angelico F., Chen J., Lu L., Lucena M. I., Fu Q., et al. (2022). Silymarin for treating toxic liver disease: international consensus recommendations. Gastro Hep Adv. 1 (5), 882–893. doi:10.1016/j.gastha.2022.05.006
Goossens J. F., Bailly C. (2019). Ursodeoxycholic acid and cancer: from chemoprevention to chemotherapy. Pharmacol. Ther. 203, 107396. doi:10.1016/j.pharmthera.2019.107396
Grove J. I., Stephens C., Lucena M. I., Andrade R. J., Weber S., Gerbes A., et al. (2023). Study design for development of novel safety biomarkers of drug-induced liver injury by the translational safety biomarker pipeline (transbioline) consortium: a study protocol for a nested case-control study. Diagn Progn. Res. 7 (1), 18. doi:10.1186/s41512-023-00155-z
Hassan A., Fontana R. J. (2019). The diagnosis and management of idiosyncratic drug-induced liver injury. Liver Int. 39 (1), 31–41. doi:10.1111/liv.13931
Hosack T., Damry D., Biswas S. (2023). Drug-induced liver injury: a comprehensive review. Ther. Adv. Gastroenterol. 16, 17562848231163410. doi:10.1177/17562848231163410
Katarey D., Verma S. (2016). Drug-induced liver injury. Clin. Med. (Lond) 16 (Suppl. 6), s104–s109. doi:10.7861/clinmedicine.16-6-s104
Lee W. M. (2003). Acute liver failure in the United States. Semin. Liver Dis. 23 (3), 217–226. doi:10.1055/s-2003-42641
Li M., Luo Q., Tao Y., Sun X., Liu C. (2021). Pharmacotherapies for drug-induced liver injury: a current literature review. Front. Pharmacol. 12, 806249. doi:10.3389/fphar.2021.806249
Li M., Luo Q., Tao Y., Sun X., Liu C. (2022b). Pharmacotherapies for drug-induced liver injury: a current literature review. Front. Pharmacol. 12, 806249. doi:10.3389/fphar.2021.806249
Li M., Wang Y., Lv T. T., Liu J. M., Kong Y. Y., Jia J. D., et al. (2023). Mapping the incidence of drug-induced liver injury: a systematic review and meta-analysis. J. Dig. Dis. 24 (5), 332–339. doi:10.1111/1751-2980.13205
Li T. W., Peng H., Yang H., Kurniawidjaja S., Panthaki P., Zheng Y., et al. (2015). S-adenosylmethionine and methylthioadenosine inhibit beta-catenin signaling by multiple mechanisms in liver and colon cancer. Mol. Pharmacol. 87 (1), 77–86. doi:10.1124/mol.114.095679
Li X., Tang J., Mao Y. (2022a). Incidence and risk factors of drug-induced liver injury. Liver Int. 42 (9), 1999–2014. doi:10.1111/liv.15262
Li X., Zhou J., Chen S., Guan M., Wang Y., Zhao L., et al. (2014). Role of bicyclol in preventing chemotherapeutic agent-induced liver injury in patients over 60 Years of age with cancer. J. Int. Med. Res. 42 (4), 906–914. doi:10.1177/0300060514527058
Lu S. C., Mato J. M. (2008). S-adenosylmethionine in cell growth, apoptosis and liver cancer. J. Gastroenterol. Hepatol. 23 (Suppl. 1), S73–S77. doi:10.1111/j.1440-1746.2007.05289.x
Lu S. C., Ramani K., Ou X., Lin M., Yu V., Ko K., et al. (2009). S-adenosylmethionine in the chemoprevention and treatment of hepatocellular carcinoma in a rat model. Hepatology 50 (2), 462–471. doi:10.1002/hep.22990
McGill M. R., Jaeschke H. (2019). Biomarkers of drug-induced liver injury. Adv. Pharmacol. 85, 221–239. doi:10.1016/bs.apha.2019.02.001
Miller E. D., Abu-Sbeih H., Styskel B., Nogueras Gonzalez G. M., Blechacz B., Naing A., et al. (2020). Clinical characteristics and adverse impact of hepatotoxicity due to immune checkpoint inhibitors. Am. J. Gastroenterol. 115 (2), 251–261. doi:10.14309/ajg.0000000000000398
Moezian G. S. A., Javadinia S. A., Sales S. S., Fanipakdel A., Elyasi S., Karimi G. (2022). Oral silymarin formulation efficacy in management of Ac-T protocol induced hepatotoxicity in breast cancer patients: a randomized, triple blind, placebo-controlled clinical trial. J. Oncol. Pharm. Pract. 28 (4), 827–835. doi:10.1177/10781552211006182
Mondaca S. P., Liu D., Flynn J. R., Badson S., Hamaway S., Gounder M. M., et al. (2020). Clinical implications of drug-induced liver injury in early-phase oncology clinical trials. Cancer 126 (22), 4967–4974. doi:10.1002/cncr.33153
Mudd T. W., Guddati A. K. (2021). Management of hepatotoxicity of chemotherapy and targeted agents. Am. J. Cancer Res. 11 (7), 3461–3474.
Niu H., Sanabria-Cabrera J., Alvarez-Alvarez I., Robles-Diaz M., Stankeviciute S., Aithal G. P., et al. (2021). Prevention and management of idiosyncratic drug-induced liver injury: systematic review and meta-analysis of randomised clinical trials. Pharmacol. Res. 164, 105404. doi:10.1016/j.phrs.2020.105404
Pinazo-Bandera J. M., Toro-Ortiz J. P., Andrade R. J., Garcia-Cortes M. (2023). Drug-induced cholestasis: causative agents and challenges in diagnosis and management. Explor Dig. Dis. 2, 202–222. doi:10.37349/edd.2023.00027
Regev A., Avigan M. I., Kiazand A., Vierling J. M., Lewis J. H., Omokaro S. O., et al. (2020). Best practices for detection, assessment and management of suspected immune-mediated liver injury caused by immune checkpoint inhibitors during drug development. J. Autoimmun. 114, 102514. doi:10.1016/j.jaut.2020.102514
Robles-Díaz M., Nezic L., Vujic-Aleksic V., Björnsson E. S. (2021). Role of ursodeoxycholic acid in treating and preventing idiosyncratic drug-induced liver injury. A systematic review. Front. Pharmacol. 12, 744488. doi:10.3389/fphar.2021.744488
Rubbia-Brandt L., Lauwers G. Y., Wang H., Majno P. E., Tanabe K., Zhu A. X., et al. (2010). Sinusoidal obstruction syndrome and nodular regenerative hyperplasia are frequent oxaliplatin-associated liver lesions and partially prevented by bevacizumab in patients with hepatic colorectal metastasis. Histopathology 56 (4), 430–439. doi:10.1111/j.1365-2559.2010.03511.x
Saif M. M., Farid S. F., Khaleel S. A., Sabry N. A., El-Sayed M. H. (2012). Hepatoprotective efficacy of ursodeoxycholic acid in pediatrics acute lymphoblastic leukemia. Pediatr. Hematol. Oncol. 29 (7), 627–632. doi:10.3109/08880018.2012.713083
Santini D., Vincenzi B., Massacesi C., Picardi A., Gentilucci U. V., Esposito V., et al. (2003). S-adenosylmethionine (adomet) supplementation for treatment of chemotherapy-induced liver injury. Anticancer Res. 23 (6D), 5173–5179.
Swanson L. A., Kassab I., Tsung I., Schneider B. J., Fontana R. J. (2022). Liver injury during durvalumab-based immunotherapy is associated with poorer patient survival: a retrospective analysis. Front. Oncol. 12, 984940. doi:10.3389/fonc.2022.984940
Tang G. H., Yang H. Y., Zhang J. C., Ren J. J., Sang X. T., Lu X., et al. (2015). Magnesium isoglycyrrhizinate inhibits inflammatory response through STAT3 pathway to protect remnant liver function. World J. Gastroenterol. 21 (43), 12370–12380. doi:10.3748/wjg.v21.i43.12370
Tang J., Gu J., Chu N., Chen Y., Wang Y., Xue D., et al. (2022). Efficacy and safety of bicyclol for treating patients with idiosyncratic acute drug-induced liver injury: a multicenter, randomized, phase II trial. Liver Int. 42 (8), 1803–1813. doi:10.1111/liv.15290
Tang L., Feng L., Zan S., Yuanjue S., Yang Y. (2012). Magnesium isoglycyrrhizinate used in the treatment of chemotherapeutic drugs-induced acute liver dysfunction: a phase III clinical trial. Tumor 32, 738–743. doi:10.3781/j.issn.1000-7431.2012.09.012
Tao L., Qu X., Zhang Y., Song Y., Zhang S. X. (2019). Prophylactic therapy of silymarin (milk thistle) on antituberculosis drug-induced liver injury: a meta-analysis of randomized controlled trials. Can. J. Gastroenterol. Hepatol. 2019, 3192351. doi:10.1155/2019/3192351
Vincenzi B., Armento G., Spalato Ceruso M., Catania G., Leakos M., Santini D., et al. (2016). Drug-induced hepatotoxicity in cancer patients - implication for treatment. Expert Opin. Drug Saf. 15 (9), 1219–1238. doi:10.1080/14740338.2016.1194824
Vincenzi B., Daniele S., Frezza A. M., Berti P., Vespasiani U., Picardi A., et al. (2012). The role of S-adenosylmethionine in preventing oxaliplatin-induced liver toxicity: a retrospective analysis in metastatic colorectal cancer patients treated with bevacizumab plus oxaliplatin-based regimen. Support Care Cancer 20 (1), 135–139. doi:10.1007/s00520-010-1078-4
Vincenzi B., Russo A., Terenzio A., Galvano A., Santini D., Vorini F., et al. (2018). The use of same in chemotherapy-induced liver injury. Crit. Rev. Oncol. Hematol. 130, 70–77. doi:10.1016/j.critrevonc.2018.06.019
Vincenzi B., Santini D., Frezza A. M., Berti P., Vespasiani U., Picardi A., et al. (2011). The role of S-adenosyl methionine in preventing folfox-induced liver toxicity: a retrospective analysis in patients affected by resected colorectal cancer treated with adjuvant folfox regimen. Expert Opin. Drug Saf. 10 (3), 345–349. doi:10.1517/14740338.2011.562888
Wang Y., Lai R., Zong P., Xu Q., Shang J., Zhang X., et al. (2021). Bicyclol for the treatment of drug-induced liver injury: a propensity score matching analysis using a nationwide inpatient database. J. Int. Med. Res. 49 (4), 3000605211005945. doi:10.1177/03000605211005945
Wang Y., Wang Z., Gao M., Zhong H., Chen C., Yao Y., et al. (2019). Efficacy and safety of magnesium isoglycyrrhizinate injection in patients with acute drug-induced liver injury: a phase II trial. Liver Int. 39 (11), 2102–2111. doi:10.1111/liv.14204
Yao L., Zhang J., Jin J., Li H., Li L., Han X., et al. (2022). An analysis of the efficacy and safety of compound glycyrrhizin injections in the treatment of drug-induced liver injury using a nationwide database. Int. J. Clin. Pharm. 44 (3), 731–740. doi:10.1007/s11096-022-01402-x
Ye H., Nelson L. J., Gomez Del Moral M., Martinez-Naves E., Cubero F. J. (2018). Dissecting the molecular pathophysiology of drug-induced liver injury. World J. Gastroenterol. 24 (13), 1373–1385. doi:10.3748/wjg.v24.i13.1373
Yuan L., Kaplowitz N. (2013). Mechanisms of drug-induced liver injury. Clin. Liver Dis. 17 (4), 507–518. vii. doi:10.1016/j.cld.2013.07.002
Zhang B., Jiang G., Wang L., Li X., Zhao C., Tan Q., et al. (2022). An analysis of silybin meglumine tablets in the treatment of drug-induced liver injury as assessed for causality with the updated Roussel Uclaf Causality Assessment method using a nationwide database. Br. J. Clin. Pharmacol. 89 (4), 1329–1337. doi:10.1111/bcp.15575
Keywords: anti-cancer therapy, drug-induced liver injury, hepatoprotective drugs, liver enzyme abnormalities, narrative review
Citation: Vincenzi B, Yimin M, Andrade RJ, Morales Castillo M, Akhundova-Unadkat G and Mato JM (2025) Management of drug-induced liver injury associated with anti-cancer therapy. Front. Physiol. 16:1541020. doi: 10.3389/fphys.2025.1541020
Received: 06 December 2024; Accepted: 05 March 2025;
Published: 27 March 2025.
Edited by:
Giuliano Ramadori, University of Göttingen, GermanyReviewed by:
Andreas Benesic, Krankenhaus GmbH Weilheim - Schongau, GermanyCopyright © 2025 Vincenzi, Yimin, Andrade, Morales Castillo, Akhundova-Unadkat and Mato. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gamar Akhundova-Unadkat, Z2FtYXIuYWtodW5kb3ZhdW5hZGthdEBhYmJvdHQuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.