 Kyle G. P. J. M. Boyle1
Kyle G. P. J. M. Boyle1 Andrea A. Beglinger1Heinrich Häusler1Anna Stahel1
Andrea A. Beglinger1Heinrich Häusler1Anna Stahel1 Esther I. Schwarz2,3
Esther I. Schwarz2,3 Christina M. Spengler1,4*
Christina M. Spengler1,4*- 1Exercise Physiology Lab, Institute of Human Movement Sciences and Sport, ETH Zurich, Zurich, Switzerland
- 2Faculty of Medicine, University of Zurich, Zurich, Switzerland
- 3Department of Pulmonology, University Hospital Zurich, University of Zurich, Zurich, Switzerland
- 4Zurich Center for Integrative Human Physiology (ZIHP), University of Zurich, Zurich, Switzerland
Background: Mechanical ventilation can lead to lung injury and diaphragmatic dysfunction. Rapid bilateral anterolateral magnetic phrenic nerve stimulation (rBAMPS) may attenuate both of the aforementioned issues by inducing diaphragm activation. However, in order for rBAMPS to become part of standard of care, the reliability of inspiratory responses to rBAMPS needs to be established.
Methods: Eighteen healthy participants (9F) underwent five blocks of 1-s rBAMPS at 25 Hz starting at 20% of maximal stimulator output with 10% increments. Three blocks were completed on the same day to test within-day reliability, and two additional blocks were each completed on subsequent days to test between-day reliability. Mean transdiaphragmatic pressure (Pdi,mean), tidal volume (VT), discomfort, pain, and paresthesia were recorded for each rBAMPS. Relative and absolute reliability of both Pdi,mean and VT were quantified by calculating intraclass correlation coefficients (ICC) and standard error of measurements (SEM), respectively. An ordinal regression was used to determine changes of sensory ratings within and between days.
Results: At all stimulator outputs, within-day Pdi,mean displayed “good” reliability (ICC range 0.78–0.89). Between days, Pdi,mean reliability was also “good” (ICC range 0.79–0.87) at stimulator outputs of 20%–50% of maximum, but “moderate” (ICC range 0.56–0.72) at stimulator outputs of 60%–100%. SEM for Pdi,mean within day ranged from 0.9 to 3.4 across tested stimulator outputs and increased on average by 1.4 ± 0.9 between days. The VT reliability was “good” to “excellent” within (ICC range 0.82–0.94) and between (ICC range 0.81–0.96) days at all stimulator outputs. SEM for VT within day ranged from 0.08 to 0.36 and from 0.11 to 0.30 between days and tended to be larger at stimulator outputs greater than 50% of maximum. Subsequent blocks within day were associated with decreased discomfort and pain (P ≤ 0.043), while subsequent days were associated with decreased discomfort and paresthesia (P < 0.001).
Discussion: rBAMPS appears to induce reliable diaphragmatic contractions, while select sensory responses become blunted over repeated stimulations. However, as reliability is slightly lower between days compared to within day, stimulation parameters may need to be adjusted to achieve similar responses on different days.
1 Introduction
Despite the necessity to treat respiratory failure, mechanical ventilation, particularity positive pressure ventilation, is not without its drawbacks. Although not an exclusive list, two possible glaring consequences of mechanical ventilation include the following: 1) ventilator-induced lung injury (VILI) caused by positive pressure that generates stress and strain on the lungs (Slutsky and Ranieri, 2014) and 2) ventilator-induced diaphragmatic dysfunction (VIDD) caused by the inactivity of the respiratory muscles (Vassilakopoulos and Petrof, 2004). Diaphragmatic atrophy is associated with a reduced ability for volitional inspiration and thus is associated with the patient’s prolonged reliance on mechanical ventilation (Dres et al., 2017). Given that diaphragmatic atrophy (a hallmark symptom of VIDD) occurs in as little as 18 h (Levine et al., 2008), the implementation of an early, safe, and reliable intervention is paramount for a positive patient prognosis.
Inducing diaphragm contractions via neurostimulation during mechanical ventilation may attenuate both aforementioned drawbacks by reducing the diaphragm’s inactivity, while simultaneously reducing the pressure required by mechanical ventilation by generating negative intrathoracic pressure swings that are more representative of physiological breathing. In fact, neurostimulation during mechanical ventilation has been shown to protect against diaphragm atrophy and dysfunction in animal models (Masmoudi et al., 2013; Yang et al., 2013; Reynolds et al., 2017). In humans, development of new as well as advancements in older technologies have produced a variety of methods to perform diaphragm neurostimulation, as described elsewhere (Etienne et al., 2023). One such promising method, due to its non-invasive nature, is magnetic phrenic nerve stimulation. Although phrenic nerve stimulation cannot replace mechanical ventilation, its addition to mechanical ventilation may provide protection against VILI and VIDD.
Previous research has explored the use of rapid cervical magnetic stimulation (rCMS) (Adler et al., 2011), rapid bilateral anterolateral magnetic phrenic nerve stimulation (rBAMPS) (Sander et al., 2010; Boyle et al., 2022), and rapid anterior magnetic stimulation (raMS) (Boyle et al., 2022) with respect to diaphragm pacing in healthy humans. For instance, recent work by our group showed that raMS could not produce sufficient diaphragm contractions due to the likely co-activation of the brachial plexus, which resulted in excessive chest and shoulder movement, which ultimately shifted the magnetic coil out of position (Boyle et al., 2022). Adler et al. (2011), however, showed that rCMS was capable of producing sufficient diaphragmatic contractions, but with a lack of ventilatory response attributed to upper airway collapse (UAC). On the contrary, rBAMPS has been shown to mitigate (but not alleviate) the occurrence of UAC and produce diaphragm contractions capable of inducing ventilation (Sander et al., 2010; Boyle et al., 2022). Therefore, rBAMPS may serve as the optimal technique to perform non-invasive diaphragm stimulation in an ICU setting.
In order for non-invasive rapid magnetic stimulation to become part of standard of care within the ICU, the reliability of responses needs to be assessed. Although the reliability of various characteristics of diaphragmatic twitch responses has been explored in depth (Bellemare and Bigland-Ritchie, 1984; Mills et al., 1995; Criner et al., 1999; Luo et al., 2002; Welch et al., 2017; Ramsook et al., 2021), the reliability of responses to rapid trains of magnetic stimulation is less clear. Therefore, the present study sought to determine the within- and between-day test–retest reliability of inspiratory responses to rBAMPS in healthy humans (the ReStim study). In addition, the present study explored whether there is a change to various side-effects in response to rBAMPS within, as well as between days.
2 Materials and methods
2.1 Ethical approval
This study was approved by the Cantonal Ethics Committee of Zurich (Project ID 2020-03033), conformed with the guidelines of the Declaration of Helsinki, and was registered on clinicaltrials.gov (NCT05302752).
2.2 Experimental design
The study took place over three visits to the Exercise Physiology Lab at ETH in Zurich, Switzerland, which can be visualized in Figure 1. Briefly, on the first visit, the participants’ lung function and respiratory muscle strength were evaluated before undergoing three blocks (blocks 1–3) of 1-s rBAMPS at 25 Hz to test within-day test–retest reliability. Each block consisted of at least three trains of rBAMPS at each stimulator output starting at 20% of maximal stimulator output, with increases in 10% increments until 100% was reached, or participant cessation. To test between-day test–retest reliability, participants underwent a single matching block of rBAMPS on day 2 and day 3, which was subsequently compared to block 1 on day 1. During all five stimulation blocks, cardiorespiratory measurements and side-effects were measured throughout, and each visit began with 6 min of resting breathing to quantify baseline measurements. All study visits occurred at the same time of day (within 2 h) at least 24 h apart. Participants were instructed to abstain from caffeine consumption and physical activity on the day of each study visit, as well as intense exercise 48 h before.
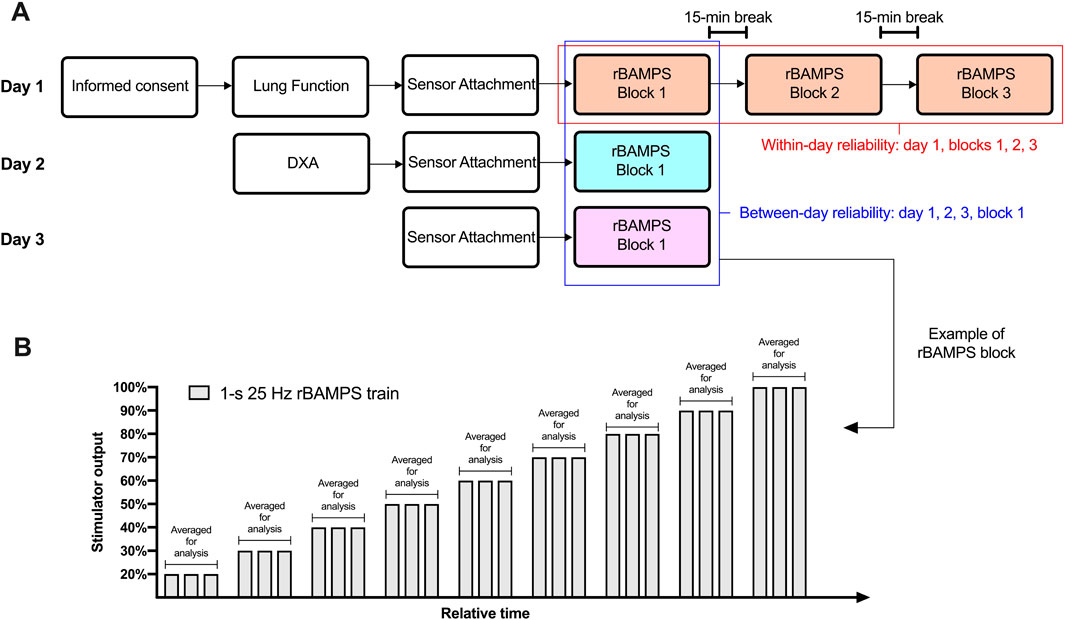
Figure 1. Study protocol. (A) Overview of the three study days including all completed tasks and what rapid bilateral anterolateral magnetic phrenic nerve stimulation (rBAMPS) blocks were compared to each other. (B) Example of an rBAMPS block that was conducted on all study days. DXA, dual-energy X-ray absorptiometry.
2.3 Participants
Eighteen healthy individuals participated in the study (9M:9F). Two participants (2F) did not complete visits on day 2 and day 3. Therefore, data for between-day reliability are presented for 16 participants only (9M:7F). Participant characteristics can be found in Table 1.
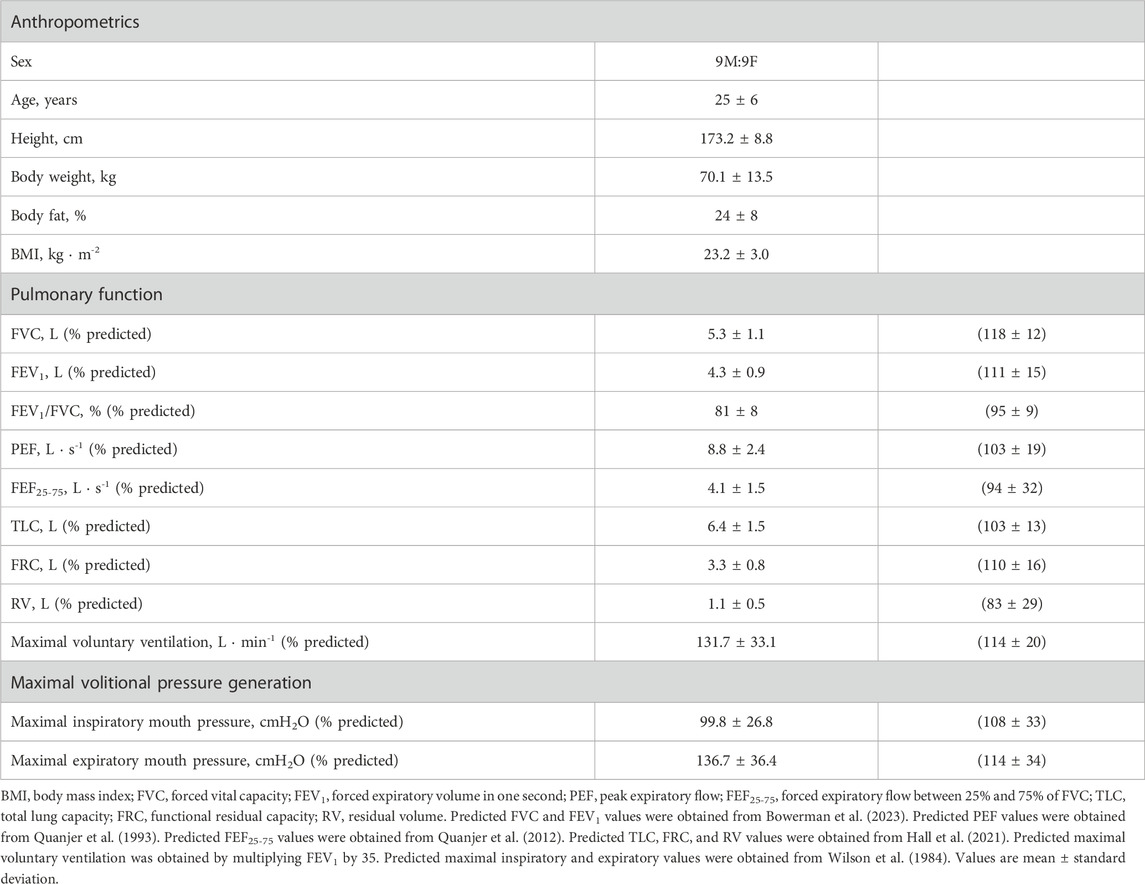
Table 1. Participant characteristics.
2.4 Lung function and respiratory muscle strength
Standard spirometry and body plethysmography were conducted with a commercially available testing system and body box (Quark PFT and Q-Box, COSMED, Rome, Italy) according to current guidelines (Miller et al., 2005; Wanger et al., 2005), with the participants seated in an upright position. Maximal inspiratory and expiratory pressures (MIP and MEP, respectively) were evaluated according to current guidelines (American Thoracic Society/European Respiratory, 2002; Laveneziana et al., 2019) from residual volume and total lung capacity, respectively, using a respiratory pressure meter (RP Check, MD Diagnostics Ltd., Kent, United Kingdom). Participant values were converted to percentage of predicted for all of MIP and MEP (Wilson et al., 1984), lung volumes (Hall et al., 2021), and spirometry values (Quanjer et al., 1993; Quanjer et al., 2012; Bowerman et al., 2023) using the newly established race-neutral equations for spirometry when possible (Bowerman et al., 2023).
2.5 Respiratory responses to rBAMPS
Transdiaphragmatic pressure (Pdi) was assessed using two balloon-tipped catheters (Adult Esophageal Balloon Catheters 47-9005, Cooper Surgical, Trumbull, CT, United States) connected to calibrated differential pressure transducers (DP45, Validyne Engineering, Northbridge, CA, United States). First, the participant’s nasal cavity and throat were numbed with local anesthetic (Xylocaine Spray 10%, Aspen Pharma Schweiz GmbH, Baar, Switzerland) prior to insertion of both balloons one at a time through the same nare into the stomach. Participants were then instructed to perform a Valsalva maneuver to remove the air from the balloons, which were subsequently filled with 1 and 2 mL of air. The balloon with 2 mL of air remained in the stomach to record the gastric pressure (Pga), while the balloon with 1 mL of air was placed in the lower third of the esophagus to record the esophageal pressure (Pes). Specifically, the balloon was withdrawn in 1-cm increments while the participants performed sniff maneuvers until the first instance of a negative deflection occurred. The balloon was then withdrawn 10 cm to ensure its complete removal from the stomach. Participants were then moved into the semi-recumbent position, and the positioning of the esophageal balloon was confirmed with the occlusion test (Baydur et al., 1982), while the gastric balloon was confirmed to be in the stomach by pressing on the abdomen and assessing for a positive pressure deflection. Adjustments in the final positioning of each balloon were made as needed. Both balloons were adhered with a tape to ensure the same position throughout testing, and each balloon was placed in the same position on subsequent days. Pdi was calculated as Pga - Pes. Participants were also instrumented with a pneumotachometer to continuously record the flow (Series 3813, Hans Rudolph, Shawnee, KS, United States). Two respiratory belt transducers (TN1132/ST, ADInstruments, Dunedin, New Zealand) that generate a linear voltage (0–100 mV) proportional to changes in length were used to assess changes in thoracic (ΔTC) and abdominal circumference (ΔAC). The thoracic belt was placed over the nipple line in men and directly below the breasts in women. The abdominal belt was placed over the navel in all participants.
2.6 Side-effects to rBAMPS
Participants were asked to rate their sensation of discomfort, pain, and paresthesia in response to each train of rBAMPS using a visual scale. The scale ranged from 0 to 10 points, and 0 was anchored as “none,” while 10 was anchored as “maximal” (the maximum the participant could imagine). Changes in the galvanic skin response (ΔGSR) were assessed following each rBAMPS train using a commercially available system (FE116 GSP Amp, ADInstruments, Dunedin, New Zealand). The electrodes used (MLT118F GSR Electrodes, ADInstruments, Dunedin, New Zealand) were placed on the participant’s index and ring fingers on their middle phalanx.
2.7 Protocol of rBAMPS blocks
All magnetic stimulations were conducted with a dual-head 46-mm butterfly shaped coil (Cool Twin B-46, MagVenture, Farum, Denmark [max dB/dt = 22 kT/s, 317μs]) connected to a single commercially available magnetic stimulator (MagPro ×100, MagVenture, Farum, Denmark) and an active cooling unit (cooler coil unit + high performance option, MagVenture, Farum, Denmark). All rBAMPS occurred at the end of a passive expiration, and participants were instructed to keep their glottis open, if possible. Stimulation took place with participants lying in a hospital bed in a semi-recumbent position such that their torso was raised to 30°. Participants’ heads were placed in a vacuum cushion (Vacuform® 2.0 vacuum pillow 30 × 40 cm, Synmedic AG, Zurich, Switzerland), with their necks slightly extended. The pillow formed to their head such that head and neck position could be replicated on following visits. Additionally, the positions of the participant’s clavicular notch, anterior superior iliac spine, and patella were recorded in reference to a measuring tape fastened to the side of the hospital bed so that the body position could be replicated.
The coil heads were positioned bilaterally on both anterolateral sides of the neck as described previously (Boyle et al., 2022). Briefly, the initial position for each coil head was the location that yielded the highest Pdi twitch (Pdi,tw) in response to a single stimulation at 100% of stimulator output. Following this, a series of rBAMPS trains were conducted at 25 Hz and 20%–50% of maximal stimulator output to evaluate co-activation that resulted in excessive movement of the participant’s head, shoulders, and arms. If the responses resulted in excessive movement, as indicated by both the experimenters and participant (such that the participant could not tolerate higher stimulator outputs), the location that resulted in the next highest Pdi,tw was tested in a similar matter. Once the optimal stimulation location was determined, the coils were secured with custom-made lever arms. The location of the coil heads was marked with a skin marker on the participant’s neck, photographed, and measured in reference to their clavicular notch and angle of their lower mandible in order to replicate the position between successive stimuli and days.
Each rBAMPS block consisted of at least three rBAMPS trains at each stimulator output starting at 20% of the maximal intensity of the stimulator with increases in 10% increments. All rBAMPS were 1 s in duration at a stimulation frequency of 25 Hz and occurred at least 30 s apart. Three rBAMPS blocks (blocks 1, 2, and 3) were conducted on visit 1 to test within-day reliability, with 15 min between each. A single identical block of rBAMPS was conducted on both day 2 and day 3 to test the between-day reliability. All rBAMPS trains and Pdi,tw assessments were conducted at functional residual capacity, which was assessed by comparing end-expiratory Pes prior to the stimulation with that of baseline resting breathing values.
2.8 Data acquisition and analysis
Physiological measurements were converted from analog to digital with two 16-channel data acquisition systems (PowerLab 16/35, ADInstruments, Dunedin, New Zealand) and collected using LabChart software (Version 8, ADInstruments, Dunedin, New Zealand) with a sampling frequency of 2,000 Hz. The integral of the inspiratory flow was taken to calculate the tidal volume (VT), which was then body temperature pressure saturated corrected. Data were analyzed using a custom-written LabChart macro that calculated the mean or peak changes in variables within specific analysis windows. The analysis window in rBAMPS that resulted in a VT response spanned from the onset of stimulation until the absence of inspiratory flow. During rBAMPS that resulted in no activity or UAC, the analysis window was 1 s following the onset of stimulation. ΔGSR was taken within a 10-s analysis window from the onset of stimulation regardless of the response type. Relative mean and peak changes in Pdi (Pdi,mean and Pdi,peak); relative peak ΔTC, ΔAC, and ΔGSR; and absolute VT responses were used for statistical analysis. Finally, the responses to individual rBAMPS trains at matching stimulator outputs within a block were averaged together to compare to subsequent blocks (Figure 1B). Within each participant, only stimulator outputs in which the participant tolerated all three rBAMPS trains across all within-day or between-day blocks were used for analysis.
2.9 Statistics
Test–retest reliability of rBAMPS was assessed by calculating intraclass correlation coefficients (ICC) for Pdi,mean, Pdi,peak, VT, ΔTC, and ΔAC within (blocks 1, 2, and 3 on day 1) and between days (block 1 of days 1, 2, and 3) at each stimulator output using a two-way mixed-effects model testing for absolute agreement. ICC values were interpreted as poor (ICC <0.5), moderate (ICC = 0.50–0.75), good (ICC = 0.75–0.90), and excellent (ICC >0.90) reliability according to Koo and Li (2016). Standard error of measurements (SEM) at each stimulator output was calculated in original units as standard deviation •
3 Results
3.1 Reliability at matched stimulator outputs
Pdi,mean in response to rBAMPS at all tested stimulator outputs along with associated ICC (95% confidence intervals), SEM, and MDC values, within day and between day is presented in Figure 2. The within-day grand means for Pdi,mean were 11.4 ± 4.8, 9.1 ± 3.8, and 8.4 ± 3.4 cmH2O during blocks 1, 2, and 3, respectively. There was a significant effect of stimulator output (P < 0.0001) and block on within-day Pdi,mean (P < 0.001). Post hoc testing revealed that Pdi,mean within day was significantly higher on block 1 when compared to block 2 from 40% to 100% of maximal stimulator output (all P < 0.038), and when compared to block 3, from 40% to 80% of maximal stimulator output (all P < 0.023). No significant differences were detected between within-day blocks 2 and 3 at any tested stimulator output. Within-day Pdi,mean displayed “good” reliability (ICC range 0.78–0.89) at all tested stimulator outputs. Between-day, Pdi,mean grand means were 11.5 ± 4.9 cmH2O on day 1, 9.1 ± 4.9 cmH2O on day 2, and 8.8 ± 4.5 cmH2O on day 3. A significant effect of stimulator output (P < 0.0001) and day (P = 0.020) was detected on between-day Pdi,mean. However, post hoc tests revealed only a significant difference between days 1 and 3 at 40% of stimulator output (P = 0.03), but no difference on any other day and stimulator output combination (all P > 0.083). Between-day Pdi,mean displayed “good” reliability from 20% to 50% of maximal stimulator output (ICC range 0.79–0.87), but “moderate” reliability at stimulator outputs from 60% to 100% (ICC range 0.56–0.72). SEM ranged from 0.9 to 3.4 within day and increased on average by 1.4 ± 0.9 between days. The MDC ranged from 2.5 to 9.4 within day and 3.3 to 15.2 between days. The within-participant within-block CV was 82% at 20% of maximal stimulator output, 42% at 30% of maximal stimulator output, and ranged from 7% to 17% at 40% to 100% of maximal stimulator output. The reliability of Pdi,peak was similar to that of Pdi,mean and can be found in the supplemental material of this paper.
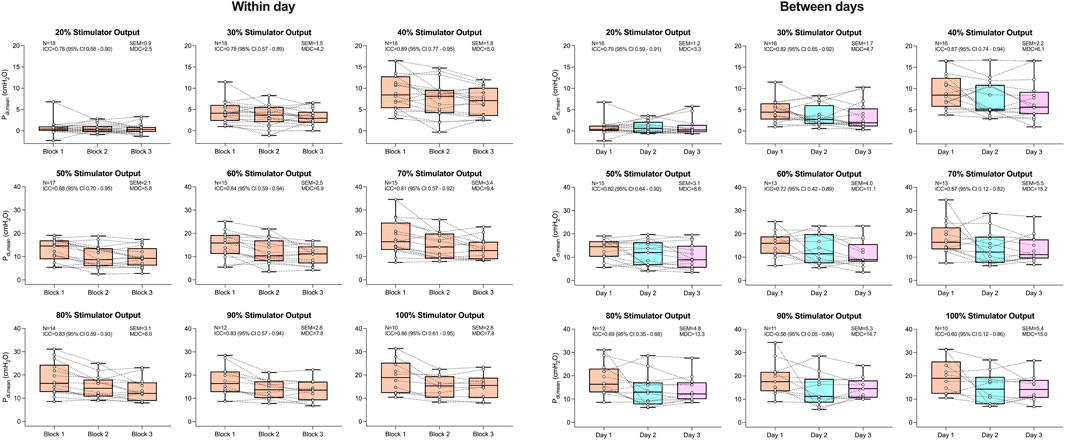
Figure 2. Mean transdiaphragmatic pressure generation (Pdi,mean) in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. Single-participant data points are represented by white circles connected by dotted lines. Upper and lower bands of the underlying box plots represent the interquartile ranges, while the black line represents the median. Box plot whiskers represent min and max values. Number of participants, intraclass correlation coefficients with 95% confidence intervals, standard error of measurement, and minimal detectable change are presented in text at each stimulator output.
Figure 3 displays VT in response to rBAMPS reliability both within and between days. Within-day VT grand mean responses were 0.88 ± 0.62 (block 1), 0.87 ± 0.51 (block 2), and 0.85 ± 0.49 L (block 3), while between-day grand means were 0.90 ± 0.63 (day 1), 0.83 ± 0.59 (day 2), and 0.86 ± 0.55 L (day 3). A significant effect of stimulator output on VT was detected both within and between days (both P < 0.0001). No significant effects of within- (P = 0.680) or between-day (P = 0.438) rBAMPS blocks were detected on VT. ICCs for VT were good to excellent at all stimulator outputs, both within (range 0.82–0.94) and between days (range 0.81–0.96). Within-day VT SEM values ranged 0.08–0.25 from 20% to 50% of maximal stimulator output and 0.28–0.36 at stimulator outputs from 60% to 100%. VT SEM values between days from 20% to 50% of maximal stimulator output were 0.11–0.22, and were 0.25–0.30 from 60% to 100% of maximal stimulator output. The MDC values were 0.22–1.0 within day and 0.30–0.83 between days. Within-block CVs were 55%, 51% and 31% at 20%, 30%, and 40% of maximal stimulator output, respectively, and were 10%–19% from 50% to 100% of maximal stimulator output.
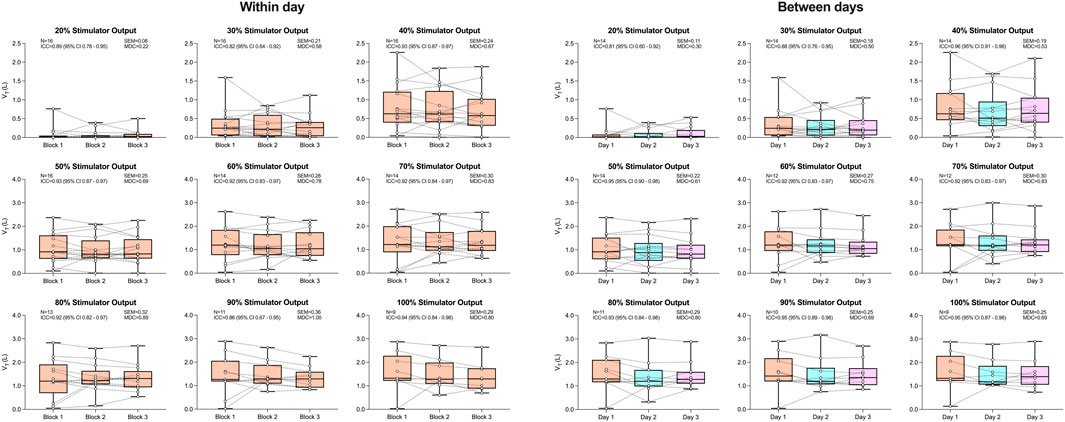
Figure 3. Tidal volume in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. Single-participant data points are represented by white circles connected by dotted lines. Upper and lower bands of the underlying box plots represent the interquartile ranges, while the black line represents the median. Box plot whiskers represent min and max values. Number of participants, intraclass correlation coefficients with 95% confidence intervals, standard error of measurement, and minimal detectable change are presented in text at each stimulator output.
The reliability of both ΔAC and ΔTC can be found in Figures 4, 5, respectively. No significant effects of block on both ΔAC and ΔTC were detected within or between days (all P > 0.052). Both respiratory belts displayed good-to-excellent within-day reliability (ΔAC ICC range 0.75–0.94; ΔTC ICC range 0.77–0.98) at all stimulator outputs excluding 30% (both ICCs = 0.74). Between days, ΔAC and ΔTC showed moderate reliability at 20% (both ICCs = 0.70) and 30% (ICC = 0.73 and 0.74, respectively) of maximal stimulator output. At all other stimulator outputs, between-day reliability was good to excellent for ΔAC (ICC range 0.77–0.90) and excellent for ΔTC (ICC range 0.91–0.96).
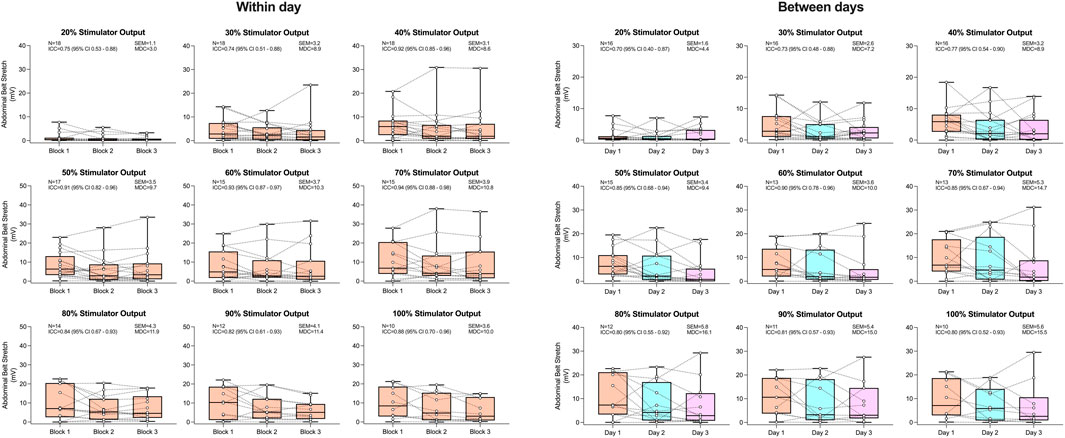
Figure 4. Abdominal belt stretch in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. Single-participant data points are represented by white circles connected by dotted lines. Upper and lower bands of the underlying box plots represent the interquartile ranges, while the black line represents the median. Box plot whiskers represent min and max values. Number of participants, intraclass correlation coefficients with 95% confidence intervals, standard error of measurement, and minimal detectable change are presented in text at each stimulator output.

Figure 5. Thoracic belt stretch in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. Single-participant data points are represented by white circles connected by dotted lines. Upper and lower bands of the underlying box plots represent the interquartile ranges, while the black line represents the median. Box plot whiskers represent min and max values. Number of participants, intraclass correlation coefficients with 95% confidence intervals, standard error of measurement, and minimal detectable change are presented in text at each stimulator output.
3.2 Side-effects to rBAMPS
All side-effects in response to rBAMPS including discomfort, pain, paresthesia, and ΔGSR are found in Figure 6. The within-day grand means for discomfort were 3.4 ± 1.5 (block 1), 3.0 ± 1.4 (block 2), and 2.6 ± 1.4 (block 3) points. Each subsequent rBAMPS block within day was associated with reduced discomfort (estimate = −0.35, Z = −3.18, P = 0.001), as well as less instances of participants selecting greater than 3 points (estimate = −0.33, Z = 2.12, P = 0.034, odds ratio [95% confidence interval] = 0.716 [0.526–0.975]). Grand mean discomfort values across days corresponded to 3.5 ± 1.6 on day 1, 2.3 ± 1.4 on day 2, and 1.8 ± 1.1 on day 3. Each subsequent day was also associated with reduced discomfort (estimate = −0.81, Z = −6.55, P < 0.001) and a reduced likelihood of participants selecting greater than 3 points (estimate = −0.79, Z = −4.67, P < 0.001, odds ratio = 0.453 [0.32–0.631]). Each subsequent rBAMPS block within day was associated with reduced pain (estimate = −0.29, Z = −2.02, P = 0.043), while subsequent days were associated with reduced paresthesia (estimate = −0.59, Z = −4.33, P = <0.001), as well as a reduced likelihood of rating paresthesia greater than three points (estimate = −0.66, Z = −3.19, P < 0.001, odds ratio = 0.518 [0.346–0.776]). Increasing discomfort, pain, and paresthesia (as well as increased instances of selecting greater than 3 points) were all significantly associated with increasing stimulator output both within and between days (all P ≤ 0.001).
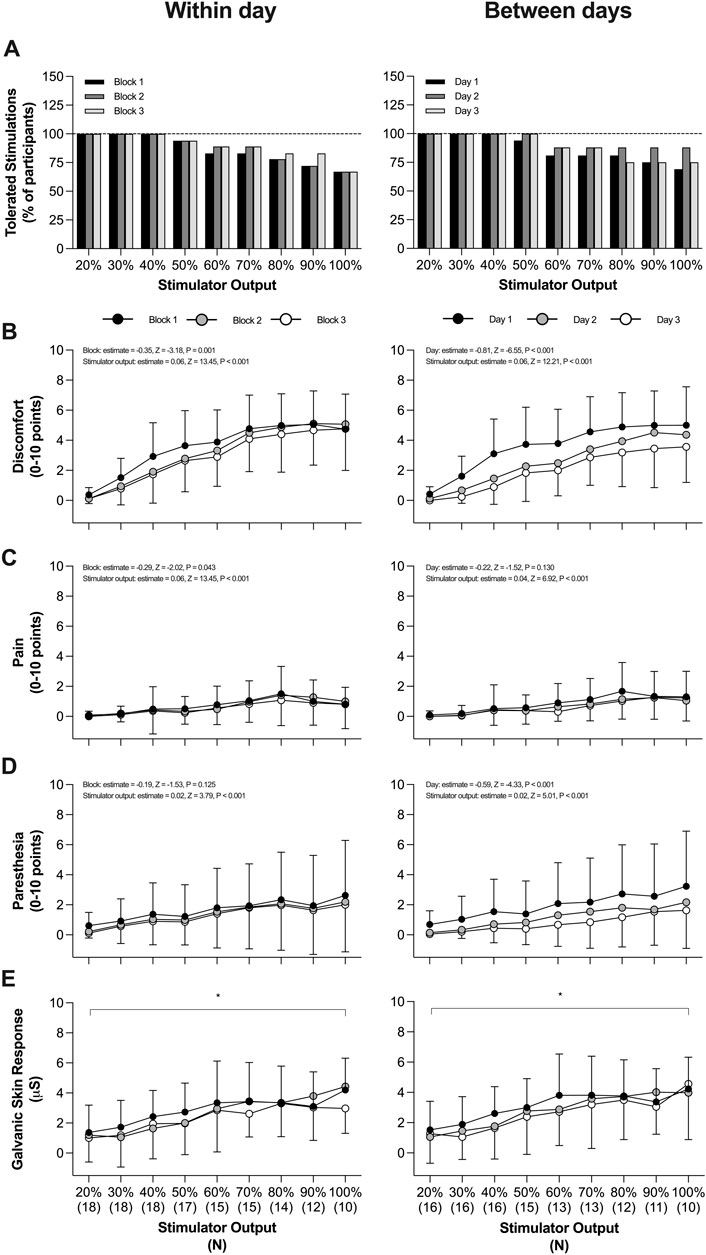
Figure 6. Side-effects in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. (A) Tolerability with increasing stimulator output (defined as participant undergoing three trains). (B) Discomfort within and between days. (C) Pain within and between days. (D) Paresthesia within and between days.(B–D) include plotted group data as mean and standard deviation with model coefficients from an ordinal regression presented in text. (E) Change in galvanic skin response within and between days. Plotted data represent group mean and standard deviation. Symbols on the panel correspond to the results of a mixed-effects model analysis such that *, main effect of stimulator output. All panels P < 0.05.
No significant effect of block was detected on ΔGSR within- (P = 0.513) or between-days (P = 0.441). A significant effect of stimulator output was detected on ΔGSR both within- (P < 0.0001) and between-days (P = 0.002). The odds of experiencing at least one UAC within a day did not change with subsequent blocks (estimate = −0.14, Z = −1.06, P = 0.287, odds ratio = 0.867 [0.668–1.13]). However, the odds of experiencing at least one UAC decreased with subsequent days (estimate = −0.32, Z = −2.17, P = 0.030, odds ratio = 0.725 [0.542–0.969]). Within participants that experienced at least one UAC and were tested on all 3 days (13 of 16 participants), the mean percentage of UAC occurrences (expressed as percentage of total number of rBAMPS trains conducted on the participant) was on average 33% ± 33% on day 1, 22% ± 28% on day 2, and 22% ± 30% on day 3.
4 Discussion
The primary aim of the present study was to determine the reliability of rBAMPS-elicited inspiratory responses within and between days. In addition, we sought to determine if participants report reduced perception of discomfort, pain, and paresthesia during repeated sessions of rBAMPS. Our findings suggest that both Pdi and VT in response to rBAMPS are reliable at various stimulator outputs across sessions within and between days. It should be noted, however, that both relative and absolute indexes of reliability indicate a reduced reliability of rBAMPS between days compared to within days, especially at stimulator outputs exceeding 50% of maximum. Finally, our findings suggest that the application of rBAMPS became less painful and uncomfortable following repeated sessions within a day and became less uncomfortable and produced lesser sensations of paresthesia following repeated sessions across days.
4.1 Reliability
In order for rapid phrenic nerve stimulation to become part of the standard of care in the ICU, stimulations must produce effective diaphragmatic contractions, and these contractions need to be reliable over time. To our knowledge, no study has systematically assessed the reliability of Pdi in response to rapid magnetic stimulation within and between days, while the reliability of Pdi,tw elicited from a single stimulus has been explored at length (Criner et al., 1999; Luo et al., 2002; Ramsook et al., 2021). Ramsook et al. (2021) showed good relative within-day reliability of Pdi,tw during cervical magnetic stimulation with an ICC value of 0.89, which is in line with our findings obtained through a variety of tested stimulator outputs (ICC range 0.78–0.89). The authors also showed good between-day reliability of Pdi,tw with an ICC of 0.87, which is similar to the between-day reliability of Pdi,mean responses in the present study between 20% and 50% of maximal stimulator output, but greater than responses at outputs from 60% to 100%. It is possible that the decreased reliability between days in the present study is in part due to the increased difficulty in placing the magnetic coils on subsequent days in the exact same position during bilateral anterolateral magnetic phrenic nerve stimulation compared to cervical magnetic stimulation. For instance, during bilateral anterolateral magnetic phrenic nerve stimulation, two coils need to get placed in the exact same position, while during cervical magnetic stimulation, a singular circular coil needs re-placement. With respect to bilateral stimulation, Criner et al. (1999) reported a within-day CV of 5.3% during bilateral electric phrenic nerve stimulation, while (Luo et al., 2002) reported a CV of 11% between days using bilateral anterolateral magnetic phrenic nerve stimulation. The present study reports greater variation during rBAMPS and is likely due in part to the additional movement that occurs during rapid stimulation compared to single twitches.
The present study tested the reliability of respiratory belts in response to rBAMPS due to their potential ability to be a non-invasive index of diaphragmatic contraction. Both ΔTC and ΔAC displayed good-to-excellent reliability at the majority of tested stimulator outputs both within and between days. Both respiratory belts displayed greater reliability compared to Pdi, but this may actually reflect that they are less responsive and sensitive in comparison to the balloon catheters. Indeed, previous work by our group showed a very poor correlation between ΔTC and Pdi,mean (r = 0.11) and a moderate correlation between ΔAC and Pdi,mean (r = 0.52) (Boyle et al., 2022), indicating neither belt has a strong relationship with the gold-standard measurement of Pdi. Conducting the same analysis in the present study reveals a moderate correlation between Pdi,mean with both ΔTC (r = 0.50, P < 0.001) and ΔAC (r = 0.52, P < 0.001). The increased correlation we report here compared to the aforementioned study is likely due to the greater sample size. Regardless, both belts still only show a moderate level of correlation with Pdi and their usefulness in quantifying diaphragmatic contractions still needs to be further explored.
4.2 Factors influencing reliability
There are a number of factors that likely influence the reliability of rBAMPS. For example, whether or not participants had the presence of UAC between days dramatically influenced the reliability of our reported data. Within the participants of the present study, two had consistent UAC during day 1 (resulting in the absence of VT and large Pdi) and less instances of UAC during days 2 and 3 (resulting in the presence of a VT and reduced Pdi during some rBAMPS). Alternatively, one participant had many instances of UAC on days 2 and 3, but not day 1. By removing these select participants from analysis, all variables show increased test–retest reliability at all stimulator outputs, and the significant effect of day on Pdi,mean is eliminated. For example, the lowest reported ICCs are Pdi,mean between days at 70% (ICC = 0.57) and 90% (ICC = 0.56) of maximal stimulator output, which both increase to 0.89 and 0.84, respectively, when the participants with inconsistent UAC are removed from the sample. Finally, it should be noted that two additional participants had UAC during nearly every rBAMPS on all visits, and these participants do not alter the reliability results. As such, it is paramount to relieve UAC during rBAMPS to optimize the reliability of the technique in participants with inconsistent UAC responses. In a clinical context, the occurrence of UAC is likely irrelevant in intubated patients, while it still might be a concern when using rBAMPS during non-invasive mechanical ventilation.
Another factor that likely influences rBAMPS reliability is the placement and replacement of the magnetic coils. Within days, coils were only repositioned in a small subset of participants (N = 6) due to a bathroom break. When performing a sub analysis in those participants, ICCs did not change between the two blocks in which coils needed to be repositioned, compared to the two blocks where the coils remained stationary during the break. This may be due to the fact that coils could be easily repositioned within days as the coil position was marked with ink. Between days it is feasible to suggest that despite efforts of the authors to reposition the coils in the exact same position, it was not always the case, and in part reflects the decrease in Pdi,mean reliability between days compared to within days. As such, finding the optimal coil position to stimulate the phrenic nerves each day is recommended in order to achieve similar responses.
4.3 Side-effects
The present study reports a reduction in discomfort and pain across rBAMPS blocks within day, as well as a reduction in discomfort and paresthesia between days. Previous research has reported habituation effects over repeated bouts of exposure to hot and cold stimuli (LeBlanc and Potvin, 1966; Bingel et al., 2007; Rennefeld et al., 2010) due to protective responses of the central nervous system. Despite this, we cautiously interpret our results and suggest that more consistent exposure to rBAMPS would need to be further explored to determine if a true habituation effect occurs. If a habituation to rBAMPS does exist, it would potentially allow patients to be stimulated at higher levels of stimulator outputs for a given level of pain or discomfort, or potentially increase their highest tolerated stimulator output over time. This would ultimately lead to increased stimulus to the diaphragm, potentially increasing protective effects.
4.4 Limitations
There are various limitations to consider in the present study. First, the participants undergoing stimulation were conscious healthy individuals. Whether responses are equally reliable in sedated patients needs to be established. In addition, how patients’ progress clinically may further influence the reliability of rBAMPS could not be accounted for in the present study. For example, a decrease in lung compliance or an increase in subcutaneous edema may both affect responses to rBAMPS. Second, the participants in the present study were not undergoing mechanical ventilation, and the interaction between rBAMPS and mechanical ventilation needs to be further explored in the context of reliability. Third, the present study performed 1-s rBAMPS at 25 Hz; thus, the generalizability of these results is not yet known. Finally, the present study only compared a total of nine rBAMPS trains at each level of stimulator output within and between days, which does not represent the likely application of rBAMPS in a clinical setting.
4.5 Conclusions
The present study reports rBAMPS as a tool to produce reliable diaphragmatic contractions. Despite this, to ensure patient safety, systems that automatically adjust stimulator output to avoid overinflation of the lung still need to be established. In addition, given the reliability of diaphragmatic contraction decreases between days compared to within days, stimulation parameters may need to be adjusted in order to achieve the same desired responses between days. Finally, rBAMPS appears to be a relatively painless experience that becomes more comfortable after repeated bouts.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Cantonal Ethics Committee of Zurich (Project ID 2020-03033). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KB: conceptualization, data curation, investigation, methodology, project administration, supervision, visualization, and writing–original draft. AB: investigation and writing–review and editing. HH: investigation and writing–review and editing. AS: investigation and writing–review and editing. ES: supervision and writing–review and editing. CS: conceptualization, funding acquisition, project administration, resources, supervision, validation, and writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Swiss National Science Foundation (grant no. 32003B_212561) and funds of ETH Zurich.
Acknowledgments
The authors would like to thank all study participants for their valuable time and patience. In addition, the authors highly appreciate the support of Patrick Schön with data acquisition.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2025.1481766/full#supplementary-material
SUPPLEMENTAL FIGURE S1 | Peak transdiaphragmatic pressure generation (Pdi,peak) in response to rapid bilateral anterolateral magnetic phrenic nerve stimulation. Single-participant data points are represented by white circles connected by dotted lines. Upper and lower bands of the underlying box plots represent the interquartile ranges, while the black line represents the median. Box plot whiskers represent min and max values. Number of participants, intraclass correlation coefficients with 95% confidence intervals, standard error of measurement, and minimal detectable change are presented in text at each stimulator output.
References
Adler D., Gottfried S. B., Bautin N., Mirkovic T., Schmidt M., Raux M., et al. (2011). Repetitive magnetic stimulation of the phrenic nerves for diaphragm conditioning: a normative study of feasibility and optimal settings. Appl. Physiology Nutr. Metabolism-Physiologie Appliquee Nutr. Metabolisme 36 (6), 1001–1008. doi:10.1139/H11-095
American Thoracic Society/European Respiratory S. (2002). ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 166 (4), 518–624. doi:10.1164/rccm.166.4.518
Baydur A., Behrakis P. K., Zin W. A., Jaeger M., Milic-Emili J. (1982). A simple method for assessing the validity of the esophageal balloon technique. Am. Rev. Respir. Dis. 126 (5), 788–791. doi:10.1164/arrd.1982.126.5.788
Bellemare F., Bigland-Ritchie B. (1984). Assessment of human diaphragm strength and activation using phrenic nerve stimulation. Respir. Physiol. 58 (3), 263–277. doi:10.1016/0034-5687(84)90003-3
Bingel U., Schoell E., Herken W., Buchel C., May A. (2007). Habituation to painful stimulation involves the antinociceptive system. Pain 131 (1-2), 21–30. doi:10.1016/j.pain.2006.12.005
Bowerman C., Bhakta N. R., Brazzale D., Cooper B. R., Cooper J., Gochicoa-Rangel L., et al. (2023). A race-neutral approach to the interpretation of lung function measurements. Am. J. Respir. Crit. Care Med. 207 (6), 768–774. doi:10.1164/rccm.202205-0963OC
Boyle K. G. P. J. M., Eichenberger P. A., Schon P., Spengler C. M. (2022). Inspiratory response and side-effects to rapid bilateral magnetic phrenic nerve stimulation using differently shaped coils: implications for stimulation-assisted mechanical ventilation. Respir. Res. 23 (1), 357. doi:10.1186/s12931-022-02251-y
Criner G. J., Travaline J. M., Holt G. A., Bosse C. G., Kelsen S. G. (1999). Variability of electrophrenic diaphragm twitch stimulation over time in normal subjects. Respir. Physiol. 118 (1), 39–47. doi:10.1016/s0034-5687(99)00057-2
Dres M., Dube B. P., Mayaux J., Delemazure J., Reuter D., Brochard L., et al. (2017). Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am. J. Respir. Crit. Care Med. 195 (1), 57–66. doi:10.1164/rccm.201602-0367OC
Etienne H., Morris I. S., Hermans G., Heunks L., Goligher E. C., Jaber S., et al. (2023). Diaphragm neurostimulation assisted ventilation in critically ill patients. Am. J. Respir. Crit. Care Med. 207 (10), 1275–1282. doi:10.1164/rccm.202212-2252CP
Hall G. L., Filipow N., Ruppel G., Okitika T., Thompson B., Kirkby J., et al. (2021). Official ERS technical standard: global Lung Function Initiative reference values for static lung volumes in individuals of European ancestry. Eur. Respir. J. 57 (3), 2000289. doi:10.1183/13993003.00289-2020
Koo T. K., Li M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15 (2), 155–163. doi:10.1016/j.jcm.2016.02.012
Laveneziana P., Albuquerque A., Aliverti A., Babb T., Barreiro E., Dres M., et al. (2019). ERS statement on respiratory muscle testing at rest and during exercise. Eur. Respir. J. 53 (6), 1801214. doi:10.1183/13993003.01214-2018
LeBlanc J., Potvin P. (1966). Studies on habituation to cold pain. Can. J. Physiol. Pharmacol. 44 (2), 287–293. doi:10.1139/y66-033
Levine S., Nguyen T., Taylor N., Friscia M. E., Budak M. T., Rothenberg P., et al. (2008). Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 358 (13), 1327–1335. doi:10.1056/NEJMoa070447
Luo Y. M., Hart N., Mustfa N., Man W. D., Rafferty G. F., Polkey M. I., et al. (2002). Reproducibility of twitch and sniff transdiaphragmatic pressures. Respir. Physiol. Neurobiol. 132 (3), 301–306. doi:10.1016/s1569-9048(02)00115-5
Masmoudi H., Coirault C., Demoule A., Mayaux J., Beuvin M., Romero N., et al. (2013). Can phrenic stimulation protect the diaphragm from mechanical ventilation-induced damage? Eur. Respir. J. 42 (1), 280–283. doi:10.1183/09031936.00045613
Miller M. R., Hankinson J., Brusasco V., Burgos F., Casaburi R., Coates A., et al. (2005). Standardisation of spirometry. Eur. Respir. J. 26 (2), 319–338. doi:10.1183/09031936.05.00034805
Mills G. H., Kyroussis D., Hamnegard C. H., Wragg S., Moxham J., Green M. (1995). Unilateral magnetic stimulation of the phrenic nerve. Thorax 50 (11), 1162–1172. doi:10.1136/thx.50.11.1162
Quanjer P. H., Stanojevic S., Cole T. J., Baur X., Hall G. L., Culver B. H., et al. (2012). Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur. Respir. J. 40 (6), 1324–1343. doi:10.1183/09031936.00080312
Quanjer P. H., Tammeling G. J., Cotes J. E., Pedersen O. F., Peslin R., Yernault J. C. (1993). Lung volumes and forced ventilatory flows. Eur. Respir. J. 6 (Suppl. 16), 5–40. doi:10.1183/09041950.005s1693
Ramsook A. H., Molgat-Seon Y., Boyle K. G., Mitchell R. A., Puyat J. H., Koehle M. S., et al. (2021). Reliability of diaphragm voluntary activation measurements in healthy adults. Appl. Physiol. Nutr. Metab. 46 (3), 247–256. doi:10.1139/apnm-2020-0221
Rennefeld C., Wiech K., Schoell E. D., Lorenz J., Bingel U. (2010). Habituation to pain: further support for a central component. Pain 148 (3), 503–508. doi:10.1016/j.pain.2009.12.014
Reynolds S. C., Meyyappan R., Thakkar V., Tran B. D., Nolette M. A., Sadarangani G., et al. (2017). Mitigation of ventilator-induced diaphragm atrophy by transvenous phrenic nerve stimulation. Am. J. Respir. Crit. Care Med. 195 (3), 339–348. doi:10.1164/rccm.201502-0363OC
Sander B. H., Dieck T., Homrighausen F., Tschan C. A., Steffens J., Raymondos K. (2010). Electromagnetic ventilation: first evaluation of a new method for artificial ventilation in humans. Muscle and Nerve 42 (3), 305–310. doi:10.1002/mus.21698
Slutsky A. S., Ranieri V. M. (2014). Ventilator-induced lung injury. N. Engl. J. Med. 370 (10), 980. doi:10.1056/NEJMc1400293
Vassilakopoulos T., Petrof B. J. (2004). Ventilator-induced diaphragmatic dysfunction. Am. J. Respir. Crit. Care Med. 169 (3), 336–341. doi:10.1164/rccm.200304-489CP
Wanger J., Clausen J. L., Coates A., Pedersen O. F., Brusasco V., Burgos F., et al. (2005). Standardisation of the measurement of lung volumes. Eur. Respir. J. 26 (3), 511–522. doi:10.1183/09031936.05.00035005
Welch J. F., Mildren R. L., Zaback M., Archiza B., Allen G. P., Sheel A. W. (2017). Reliability of the diaphragmatic compound muscle action potential evoked by cervical magnetic stimulation and recorded via chest wall surface EMG. Respir. Physiol. Neurobiol. 243, 101–106. doi:10.1016/j.resp.2017.05.011
Wilson S. H., Cooke N. T., Edwards R. H., Spiro S. G. (1984). Predicted normal values for maximal respiratory pressures in caucasian adults and children. Thorax 39 (7), 535–538. doi:10.1136/thx.39.7.535
Keywords: rapid magnetic stimulation, phrenic nerve stimulation, reliability, diaphragm contraction, tidal volume, transdiaphragmatic pressure, non-invasive ventilation, diaphragm atrophy
Citation: Boyle KGPJM, Beglinger AA, Häusler H, Stahel A, Schwarz EI and Spengler CM (2025) Within- and between-day test–retest reliability of responses to rapid bilateral anterolateral magnetic phrenic nerve stimulation in healthy humans (ReStim). Front. Physiol. 16:1481766. doi: 10.3389/fphys.2025.1481766
Received: 16 August 2024; Accepted: 02 January 2025;
Published: 11 February 2025.
Edited by:
Hans Haverkamp, Washington State University Health Sciences Spokane, United StatesReviewed by:
Troy J. Cross, The University of Sydney, AustraliaAhmet Baydur, University of Southern California, Australia
Copyright © 2025 Boyle, Beglinger, Häusler, Stahel, Schwarz and Spengler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina M. Spengler, Y2hyaXN0aW5hLnNwZW5nbGVyQGhlc3QuZXRoei5jaA==