 Mengyun Feng
Mengyun Feng Jian Li
Jian Li Jinzhen Zhao2
Jinzhen Zhao2 Qi Han
Qi Han
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Physiol. , 02 July 2024
Sec. Exercise Physiology
Volume 15 - 2024 | https://doi.org/10.3389/fphys.2024.1392483
Background: Physical activities play an important role in alleviating the aging problem and improving the physical fitness of middle-aged and elderly people. Blood flow restriction (BFR) training, also known as pressure training, has been widely used to improve athletes’ performance and rehabilitation, which is a relatively novel exercise method for improving the physical fitness of middle-aged and elderly people. The purpose of this study is to conduct a systematic review and meta-analysis of domestic and foreign randomized controlled trial studies on BFR training for middle-aged and elderly women, further explore the impact of BFR training on health status.
Methods: Meta-analysis was performed according to PRISMA standards, and charts were drawn using Review Manager 5.4 and Stata 17 software. In this study, the keywords such as “pressure training”, “blood restriction training”, “elderly women”, “KAATSU”, “blood flow restriction training” were used on CNKI, China Science and Technology Journal Database, PubMed, Embase, Web of Science, Cochrane Library, EBSCO, Scopus, and randomized controlled trials were searched in all languages. The search was performed from the establishment of database to 2 January 2024. The results of the combined effect were represented by standard mean differences.
Results: Among the 681 literature retrieved, six eligible English articles were included in this meta-analysis. The overall effect test of the combined effect was performed on 10 groups of data, and the results were SMD = −0.18 (95%CI: −0.91 to 0.56; p > 0.05), the maximum dynamic force of 1RM SMD = 0.97 (95%CI: 0.35 to 1.58; p < 0.05), leg compression force SMD = −0.10 (95%CI: −0.78 to 0.57; p > 0.05), heart rate SMD = 0.33 (95%CI: −2.50 to 3.17; p > 0.05), systolic blood pressure (SBP) SMD = −1.44 (95%CI: −2.17 to −0.70; p < 0.05), diastolic blood pressure (DBP) SMD = −0.69 (95%CI: 2.54 to 1.15; p > 0.05).
Conclusion: BFR training had a significant effect on the increase of the maximum dynamic force of 1RM and decrease of blood pressure in middle-aged and elderly women, but there was no significant difference found in heart rate and leg compression force.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42024491642.
In 2022, the World Health Organization pointed out that at present, all countries are facing the important problem of population aging, and by the end of 2022, China’s population aged 60 and above will reach 280.04 million, accounting for 19.8% of the total population (Linlin, 2023). With the development of economy, the aging problem of society is becoming more and more serious, and the occurrence probability of chronic diseases among middle-aged and elderly women in China is also greatly increased (Wang et al., 2019). Aging will lead to a large loss of muscle and bone components in the body, musculoskeletal dysfunction and cardiovascular disease are the most common chronic diseases. Physical exercise can improve the physical function of middle-aged and elderly people (Dipietro et al., 2019; Amato et al., 2022), appropriate exercise can improve muscle strength, respiratory system function (Agostini et al., 2023), reduce the incidence of chronic diseases and improve the physical fitness for middle-aged and elderly people (Guoqiang, 2006). Middle-aged and elderly women have high limitations in the choice of sports mode due to their own functional status, especially middle-aged and elderly women with osteoporosis and hypertension. In traditional high-intensity training, the loading intensity that promotes strength growth is close to 60%–80% of 1RM (Hunter et al., 2004), which is easy to cause injury and a suddenly increase in blood pressure (Carroll et al., 1992; Kallinen and Markku, 1995). For middle-aged and elderly women, it is impractical to increase strength by increasing training load, resistance or training volume, and there are many experiments proved that the effect of high-intensity exercise can be achieved through BFR combined with low-intensity exercise (Thiebaud et al., 2013; Vechin et al., 2015; Mânica et al., 2020). Therefore, it is very important to explore the suitable exercise mode for middle-aged and elderly women.
In the 1960s, Japanese sports doctor Sato (2005) first proposed the application of blood flow restriction (BFR) to sports training, the initial BFR training is the use of bicycle inner tubes tied to the limb parts of training, with the extensively increased application of BFR training, the equipment is becoming more and more advanced and efficient. BFR training, also known as pressure training, refers to the use of specific tools to compress the proximal end of the limb and block blood flow within a certain range, during which time, low-intensity BFR training can stimulate muscle growth. Now, it is widely used to increase muscle mass and strength, improve aerobic capacity, prevent disused muscular atrophy, and accelerate the recovery process after injury and surgery (Wei Jia et al., 2019).
BFR exercise may be an effective exercise method for improving the health status of middle-aged and elderly women, but there are few studies on the effectiveness of BFR training for middle-aged and elderly women, and whether it can promote their health is still controversial. Some studies suggest that BFR training may cause abnormal cardiovascular reactions (Iida et al., 2011; Ozaki et al., 2011; Santler and Goerge, 2017; Cristina-Oliveira et al., 2020), and the safety of BFR training needs to be studied (Spranger et al., 2015). Although it has some shortcomings/weakness, most experts still take BFR training and find that it can quickly and effectively enhance the physique of the elderly (Clarkson et al., 2017; Barili et al., 2018; Letieri et al., 2019; Kargaran et al., 2021; Maciel et al., 2021; Xiong and Liu, 2023). In this study, meta-analysis was used to integrate the results of BFR training for middle-aged and elderly women, and on the basis of collecting various indicators affecting muscle shape, blood pressure and strength, quantitative analysis was conducted to verify its effectiveness and reliability of the combined results from current research.
This review is registered at PROSPERO (Registry Information) and was written in accordance with the standards for systematic reviews and meta-analyses published by PRISMA (Registration number: CRD42024491642).
The inclusion criteria used in this analysis were: 1) The study type was randomized controlled trial (RCT); 2) BFR intervention was performed in the experimental group; 3) The subjects were middle-aged and elderly women over 55 years old, and there was no significant difference in their baseline characteristics; 4) Muscle strength, muscle mass and heart rate were included in the results, and data were expressed as mean ± standard deviation (SD); 5) Include sufficient data to calculate the effect size; 6) The intervention intensity and duration of BFR are not restricted.
The literature will be excluded if: 1) Repetitive literature; 2) There is a copyright problem or the full text cannot be obtained; 3) The data in the paper are fuzzy, the outcome indicators and data are incomplete; 4) Research design errors; 5) Use of other drugs or change the subjects' medication habits.
To identify eligible studies, literature searches were conducted in Chinese and English databases including CNKI, China Science and Technology Journal Database, PubMed, Embase, Web of science, Cochrane Library, EBSCO and Scopus from inception to 2 January 2024 (search deadline). It is not limited by regions, publication types or languages.
The search terms used were pressure training, blood restriction training, blood obstruction training, elderly women; KAATSU, KAATSU training, blood flow restriction training, BFR therapy, BFRT, occlusion training, blood flow restriction with exercise, resistance training associated with blood flow restriction, resistance training associated with BFR, elderly women. Each synonym is retrieved using the “or” connection. The search type is: “KAATSU or KAATSU training or blood flow restriction training or BFR therapy or BFRT or occlusion training or blood flow restriction with exercise or resistance training associated with blood flow restriction or resistance training associated with BFR” and elderly women.
In the first screening, the titles, abstracts and keywords of the relevant literature retrieved were browsed and evaluated according to the inclusion criteria, and the literature that do not meet the criteria are excluded. Screening with Zotero software was applied to remove duplicate entries. The second screening determining the final literature based on the full text and the systematic exclusion of studies that did not meet the inclusion criteria. Data extraction was carried out independently by two researchers, and any differences were resolved by a third researcher or by consensus. From the eligible literature, we extracted the following relevant information: 1) The name of the first author; 2) The year of publication; 3) The comparison result datasets between the experimental group and all control groups without BFR training; 4) Training scheme, frequency and time of experimental group and control group; 5) BFR group cuff pressure; 6) Outcomes: muscle strength, blood pressure, heart rate. All the relevant datasets were extracted and calculated in a spreadsheet Table 1.
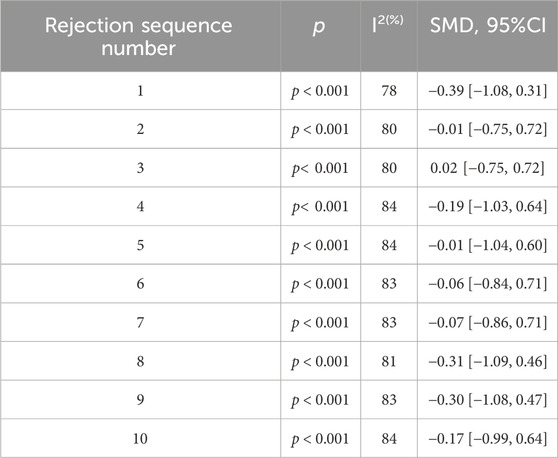
Table 1. Sensitivity analysis of included references.
The risk of bias was assessed in accordance with the Cochrane Manual for Systematic Review of Interventions, and each study was individually evaluated using seven criteria to assess the risk of bias. Evaluation was conducted independently by two investigators from random sequence generation, assignment method concealment, implementation bias, measurement bias, follow-up bias, selective reporting of findings, and other sources of bias. For each trial, we assessed and graded the risk as low, possibly low, unclear, possibly high, or high bias risk. If the risk of bias is low or likely to be low in all areas, the overall risk of bias is classified as low; if the risk of bias is not clear for the above risks of bias, it is graded as not clear risk; high if the risk of bias is high or likely to be high when it has at least one risk of bias. Disputes are handled by a third researcher or through discussion and negotiation before a decision is made.
Meta-data analysis was conducted independently by two authors. Basic information of subjects was extracted in the form of mean value, standard deviation (SD) and sample size. Baseline values and post-treatment values were used for meta-analysis. The software Review Manager 5.4 and Stata 17 were used to process the data and generate forest as well as funnel plots. In this paper, continuous result variables are used, and plots are represented by standard mean differences (SMD). Heterogeneity exists when P ≤ 0.1 or I2 ≥ 50% for the overall effect analysis. When there was no heterogeneity, the fixed effect model was used. When heterogeneity was present, random effects model was applied. Subgroup analysis or regression analysis and sensitivity analysis were used to explore the sources of heterogeneity, forest plots were used to assess different impacts between intervention and control, and funnel plots were used to analyze publication bias. p < 0.05 was considered statistically significant.
A total of 681 articles were retrieved in the database, and the literature were imported into Zotero, a literature management software. After removing duplicate records and multiple screening, 21 articles were found to meet the inclusion criteria. Due to the reasons of data acquisition, six eligible English articles were finally included in the study. Figure 1 shows the literature screening process.
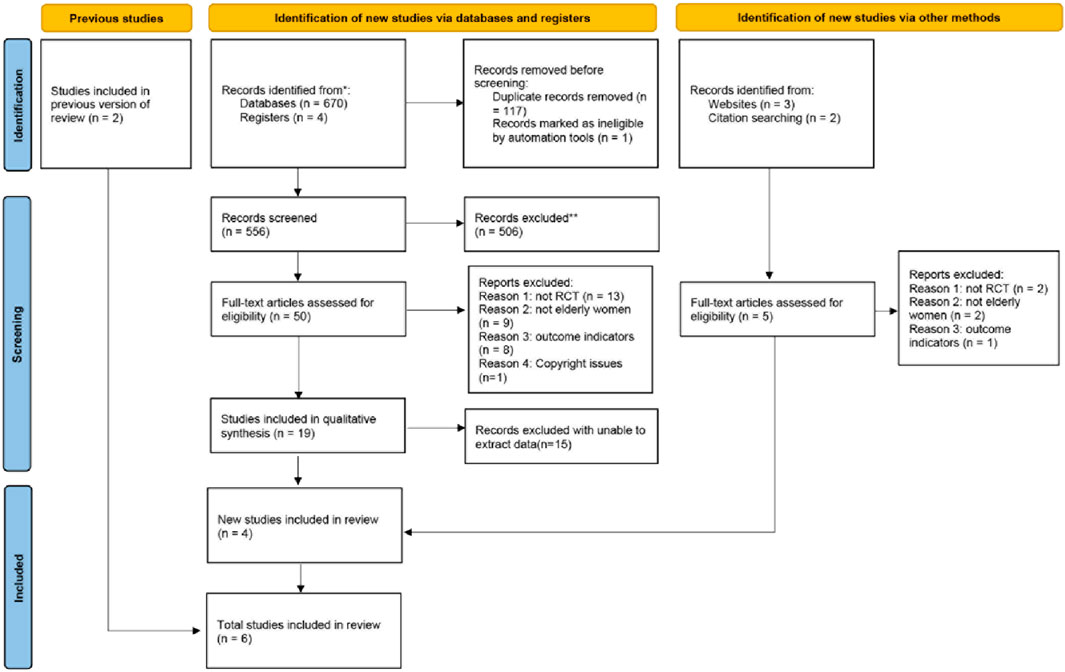
Figure 1. Literature screening process.
The six eligible trials included a total of 129 elderly women over 55 years of age, 48 in the experimental group and 81 in the control group.
Table 2 shows the features of all included studies. The experimental group took BFR training, while, the control group did not perform any type of BFR intervention. Muscle strength, heart rate and blood pressure are taken as outcome indicators to analyze whether they can promote the health of elderly women.
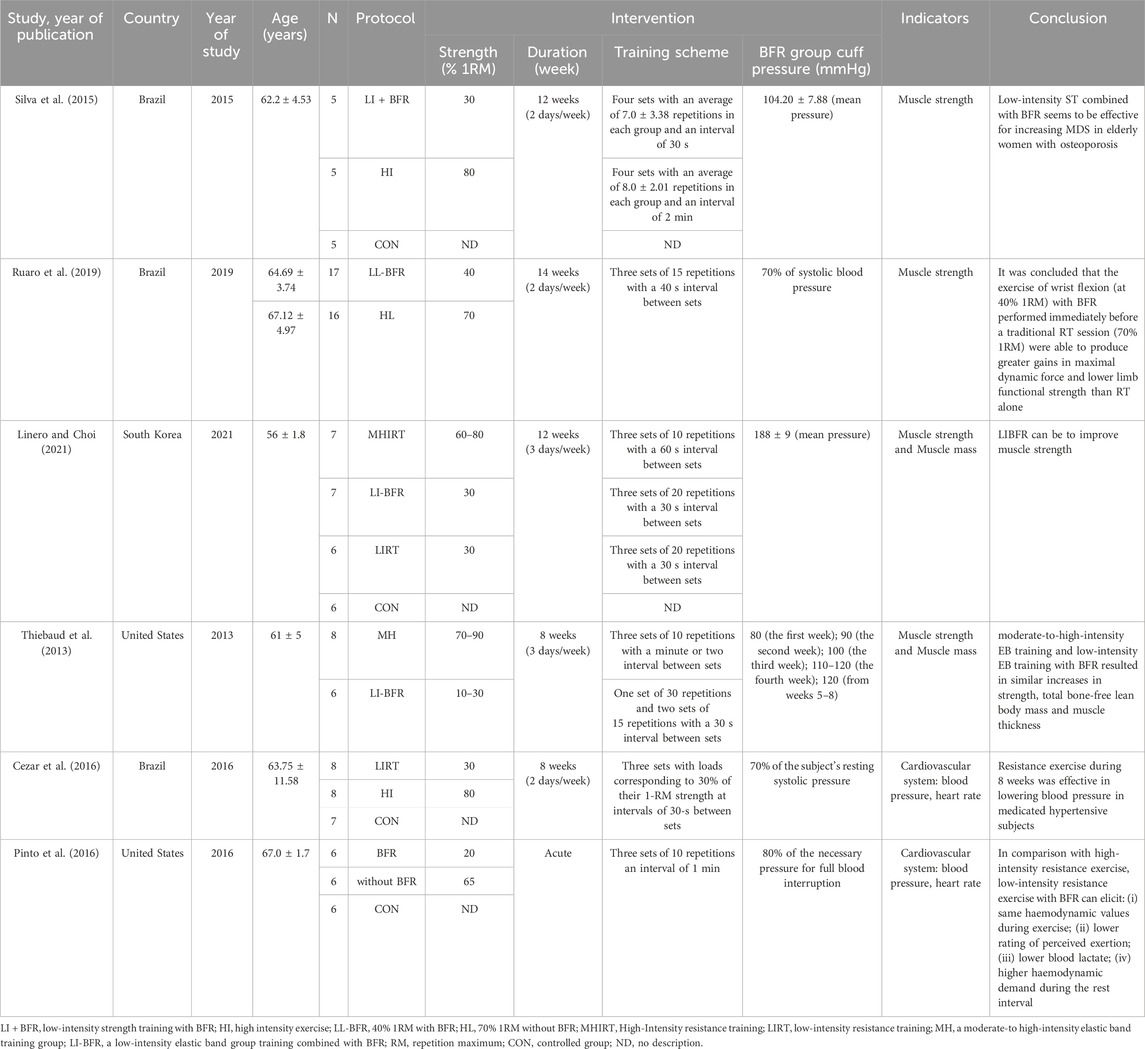
Table 2. Features of all included studies.
Figure 2 is the risk of bias assessment diagram. Figure 3 is the general summary risk of bias diagram: randomization of sequencing has 50% studies at low risk, 50% at unknown risk and 0% at high risk. The allocation selection method is observed with 50% studies at low risk, 50% at unclear risk and 0% at high risk. The blinding of participants had 17% studies at low risk, 66% at unknown risk, and 17% at high risk. The blinding of experiment operators was evaluated with 33% studies at low risk, 67% at unknown risk, and 0% at high risk. The incomplete reporting of the outcome data was 67% studies at low risk, 33% at unknown risk, and 0% at high risk. Selective reporting of results is at low risk, where no unclear risk and high risk was reported. The other sources of bias are unclear.
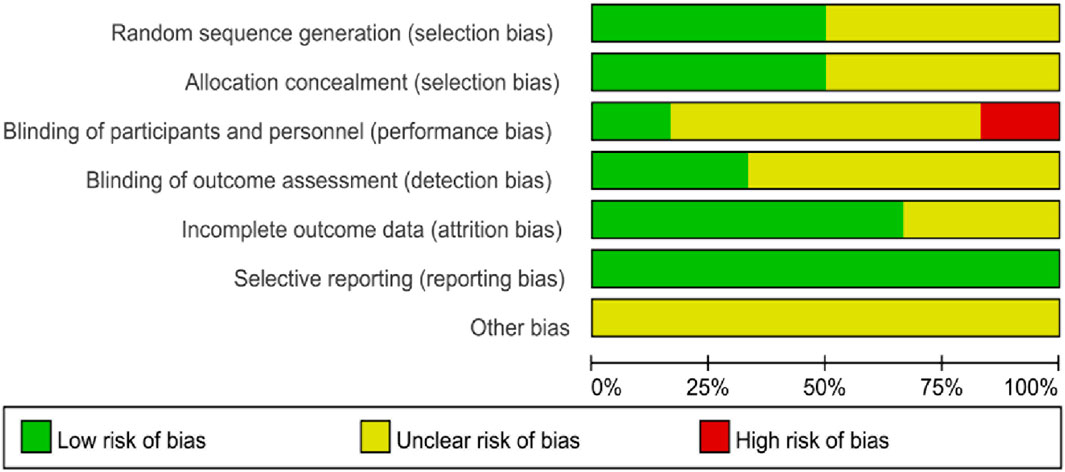
Figure 2. Risk assessment diagram of bias in included studies.
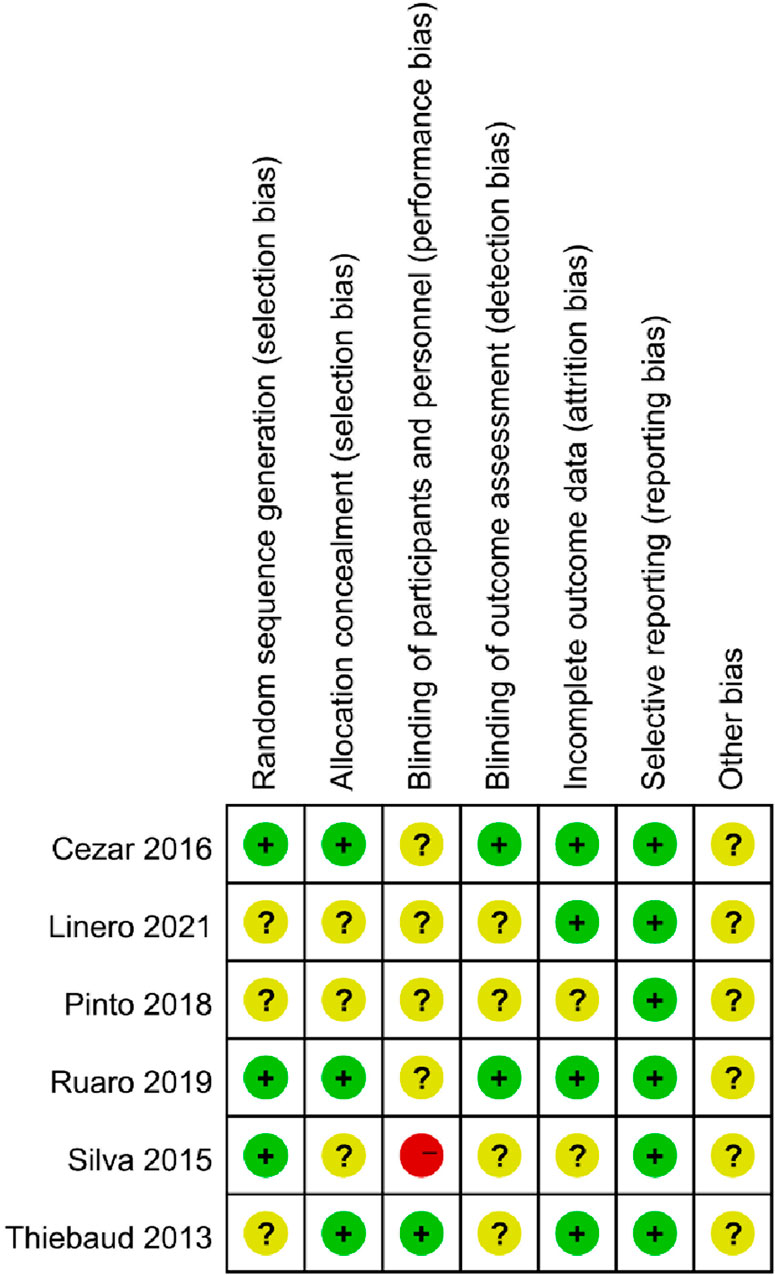
Figure 3. Risk profile of bias in included studies.
The overall effect test was conducted on six articles and 10 groups of data included in this study. The forest plot in Figure 4 showed that the heterogeneity among the included studies was high (I2 = 82%, p < 0.05) regarding all the included health indicators, so the random effects model was adopted. The combined effect size was SMD = −0.18 (95%CI: −0.91 to 0.56; p > 0.05), and the standard mean difference between the two groups was not significantly different.
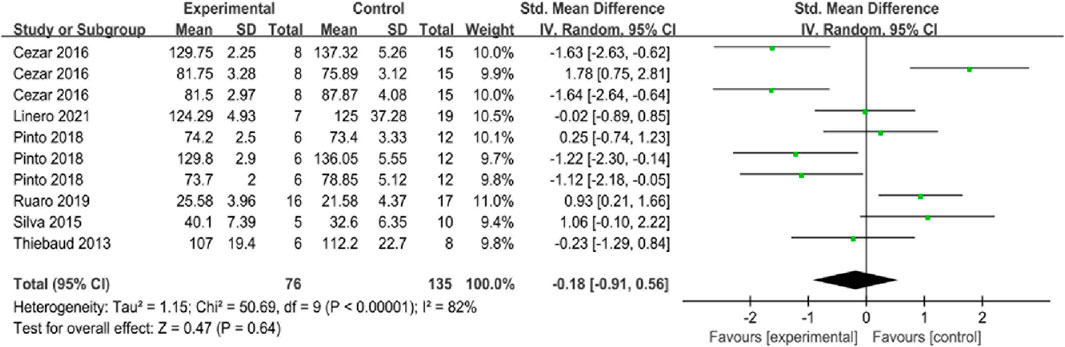
Figure 4. Forest plot for comprehensive analysis of included documents.
Two studies reported the maximum dynamic force of 1RM, with a total of 48 subjects. As shown in Figure 5, I2 = 0% (p > 0.05), indicating that there was no heterogeneity between the two studies, so the fixed-effect model was selected for the 1RM analysis. The results showed that BFR could significantly enhance the maximum dynamic force of 1RM in middle-aged and elderly women, and the intervention effect was better than that of the control group, with SMD = 0.97 (95%CI: 0.35 to 1.58; p < 0.05), indicating that the experimental group was better than the control group in enhancing the maximum dynamic force of 1RM.

Figure 5. Forest plot of the maximum dynamic force of 1RM in the included literature.
The leg compression force was reported in two studies with a total of 40 subjects. As shown in Figure 6, I2 = 0% (p > 0.05), indicating that there was no heterogeneity between the two studies, so the fixed-effect model was selected for leg compression force analysis. Results of meta-analysis showed that SMD = −0.10 (95%CI: −0.78 to 0.57; p > 0.05), which indicates that the mean difference between the two groups was not significantly different.

Figure 6. Forest plot of leg compression force in the included literature.
Two studies examined the effects of flow-restricted training on heart rate, involving a total of 41 subjects. As shown in Figure 7, heavy heterogeneity between the two studies was found, where I2 = 93% (p < 0.1), therefore the random effects model was selected for analysis. The results of meta-analysis showed that SMD = 0.33 (95%CI: −2.50 to 3.17; p > 0.05), indicating that there was no significant different impact on heart rate between the two groups.

Figure 7. Heart rate forest plot of included references.
When assigning medium-high intensity resistance training without BFR as the control group, it was observed that p ≤ 0.1, I2 = 74% (Appendix 1). Meanwhile, when assigning the group without any training as the control group, it was found that p ≤ 0.1, I2 = 96% (Appendix 2). The heterogeneity can be induced by the differences in the subjects selection, different study design, and the measurement methods and time.
Two studies examined the effect of BFR training on blood pressure, involving a total of 41 subjects. As shown in Figure 8, I2 = 68% (p = 0.02), with significant heterogeneity among the four studies being observed, therefore, the random effects model is applied. Results of meta-analysis showed a significant overall effect size SMD = −1.05 (95%CI: −1.95 to −0.16; p < 0.05), which indicates that BFR training can significantly reduce blood pressure of middle-aged and elderly women, and its effect is better than that of control group.
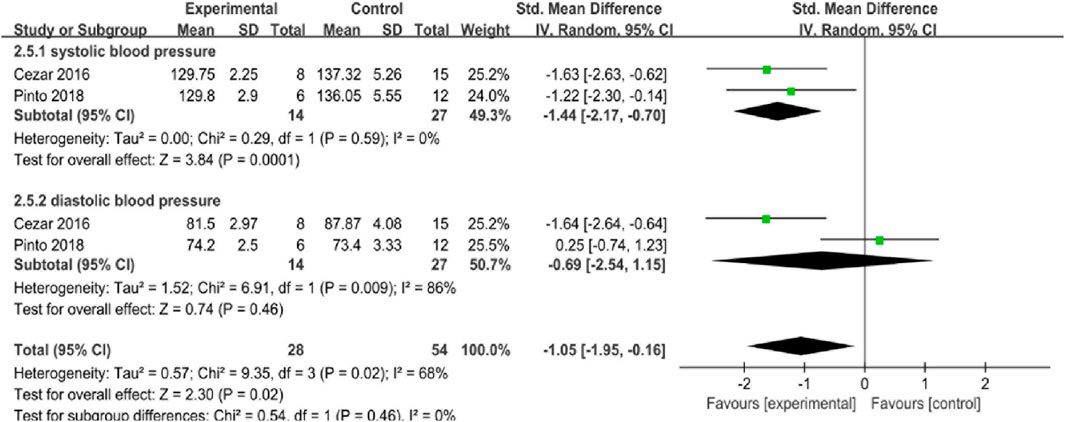
Figure 8. Forest plot of blood pressure in included literature.
The heterogeneity of systolic blood pressure (SBP) was I2 = 0% (p = 0.59), where SMD = −1.44 (95%CI: −2.17 to −0.70; p < 0.05), indicating that BFR training can significantly reduce SBP of middle-aged and elderly women, and the experimental group is better than the control group in reducing SBP. Diastolic blood pressure (DBP), I2 = 86% (p = 0.009), SMD = −0.69 (95%CI: −2.54 to 1.15; p > 0.05), indicating that the experimental group and the control group might have similar effects on DBP, therefore, the significant overall effect of BFR on blood pressure majorly relies on its impact on the changes of SBP.
In the Review Manager 5.4 software, after removing the included data one by one in the meta-analysis of the merging effect of 10 groups of data, it was found that the heterogeneity of the results after the elimination did not change significantly, which failed to change the heterogeneity of the merging effect analysis. Since only two literature are included in Figure 7 for analysis, it is not possible to conduct heterogeneity analysis if one of them is excluded.
The data were incorporated into Stata17 and Egger test was adopted to test the publication bias, which showed no significant publication bias with p > 0.05. Figure 9 shows the funnel plot of reporting bias risk.
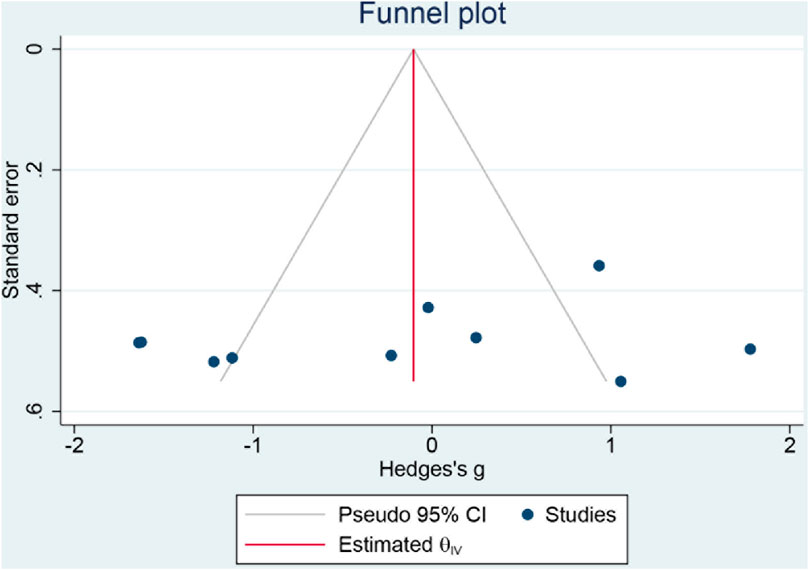
Figure 9. Funnel plot of risk of reporting biases.
BFR training refers to the use of specific tools to add pressure the outside of the limb to achieve the purpose of obstructing blood flow within a certain range, combining with low-intensity exercise (Kraemer and Ratamess, 2004), inducing muscle reactive hyperemia (Pan Yanrong et al., 2021), promote the increase of protein synthesis and growth hormone secretion (Ronghai, 2019), which improves skeletal muscle adaptability, and then increases muscle thickness and cross-sectional area (Ferraz et al., 2018), and ultimately improves muscle strength (Madarame et al., 2011). Flow-restricted training can inhibit the expression of FOXO3A protein, thereby reducing the expression of Atrogin-1 and MuRF-1, and alleviate muscle atrophy (Sandri et al., 2004; Mammucari et al., 2007; Manini et al., 2011). When limiting blood flow, the training limb is suffering from ischemic stress, the peripheral artery metabolic pressure increases, and accompanied by higher active potential, resulting in a phenomenon similar to fatigue, and then, recruit type II fast-twitch muscle fiber, alternating the muscle fiber percentage, and stimulate muscle hypertrophy (Yasuda et al., 2005).
However, while improving muscle strength, BFR training will lead to relative ischemia and hypoxia of limbs (Yasuda et al., 2010), increase the release of K+ and Na+ to the extra cellular matrix (Franz et al., 2020), accumulation of metabolites such as lactic acid (Teixeira et al., 2018), acidosis, excessive metabolic pressure, and prone to thrombosis, abnormal cardiovascular reactions, muscle fatigue and injury. Due to the decline of body function, middle-aged and elderly people are at risk of various cardiovascular diseases (Yu Wei and Liu, 2022). For instance, physically inactive and attenuated muscle metabolism might be the risk factors for the developing and progression of cardiovascular or metabolic disorders.
Although BFR training has some potential risks, there are still a large number of experts taking this training method for clinical practice and research. After collecting the adverse events reported in the study, only two adverse events were reported (Ozawa et al., 2015; Harper et al., 2019), and fewer adverse events were reported than resistance training in the same study, and the intervention appears to be safe compared to high-intensity training. After a 6-month resistance training program, older women gain only one-fifth of the muscle strength of older men, and can gain more benefits from training by increasing the volume and intensity of exercise training, but for middle-aged and older women, high-intensity and high-load exercise is difficult to adapt (Hunter et al., 2004). Thiebaud et al. found that moderate to high intensity elastic band (EB) training and low intensity EB training were similar to BFR in improving strength, lean muscle mass and muscle thickness (Thiebaud et al., 2013). Vechin et al. found that both training regimens can effectively increase the quadriceps muscle strength and 1RM of the leg press, which is a feasible alternative exercise for people who cannot use high intensity exercise (Vechin et al., 2015). Mânica et al. found that BFR combined with low-intensity aerobic exercise had similar anti-inflammatory effects in older women with hypertension, and that BFR combined with low-intensity exercise promoted better immune responses and adaptation than low-intensity regimens (Mânica et al., 2020). These studies further confirm that BFR training is an important alternative to high-intensity resistance training and an effective training method for promoting bone health and muscle strength. BFR training is feasible for middle-aged and elderly women, but there are few studies on the optimal duration, intensity and flow-restriction tools of BRF training, and it is necessary to design appropriate training programs according to each person’s physical condition in the specific implementation process.
According to Figure 8, it appears that the overall effect size of quantitatively combined synthesis of SBP and DBP was improved with SMD = −1.05 (95%CI: −1.95 to −0.16; p < 0.05). Though blood flow restriction did not improve DBP compared to the control group by itself, where SMD = −0.69 (95%CI: −2.54 to 1.15; p > 0.05), and it showed that the SBP was downregulated after blood flow restriction training with SMD = −1.44 (95%CI: −2.17 to −0.70; p < 0.05). American Heart Association (AHA) and global healthcare practitioners recognize elevated SBP and DBP are among the risk factors of developing cardiac artery diseases (CAD) and cardiovascular diseases (CVD) (Price et al., 2019; Naidu et al., 2022; Kittleson et al., 2023). In this study, it can be observed that blood flow restriction training intervention has beneficial effect on the regulation of blood pressure, especially through down-regulating SBP, probably through enhancing eNOS synthesis and promoting the secretion of nitric oxide (NO) to the blood vessels smooth muscle endothelial cells (Li et al., 2020; Bao et al., 2022; Cai and Chen, 2022; Wu et al., 2022). Therefore, it is recommended for the elderly to practice blood flow restriction training under appropriate workload, which can be helpful in maintaining their regular blood pressure and have potential benefits in decreasing CAD and CVD risk factors.
This study investigated whether BFR training can effectively promote the physical health of middle-aged and elderly women. A total of six randomized controlled trial studies with middle-aged and elderly women were summarized, and 129 elderly women aged over 55 were included. The results of meta-analysis showed that flow-restricted training had significant effects on the improvement of muscle strength and reduction of SBP in middle-aged and elderly women, while there was no significant difference in heart rate and DBP. According to the included literature, the included subjects of their experiment were osteoporosis patients, hypertension patients and healthy elderly women, and the ethnics of population were diverse.
The muscle strength of middle-aged and elderly people will decrease with age (Genping, 2019), and the decline of muscle mass can lead to the osteoporosis and fall risk of elderly and middle-aged people (Ma et al., 2020). The muscle strength increases after BFR training (Yasuda et al., 2016; Early et al., 2020). After menopause, changes in hormone levels in the body will lead to decreased muscle strength, osteoporosis and high blood pressure (Li, 2022). Therefore, this study further systematically analyzed middle-aged and elderly women to clarify the health promotion effect of BFR, and through BFR training, middle-aged and elderly women can carry out physical exercise in a safe and efficient way. The results of this study are similar to those of previous studies in strengthening muscle strength (Slysz et al., 2016; Hughes et al., 2017; Liu Haoyan et al., 2023). Compared with previous studies on heart rate and blood pressure, there were some differences (Fei, 2016; Zhang et al., 2022). Wang Fang (Fei, 2016) reported a significant decrease in systolic blood pressure, but no significant difference in diastolic blood pressure compared with control group. However, Zhang et al. (2022) reported that BFR training can cause a sharp increase in heart rate and blood pressure in the elderly.
In the study (Patterson et al., 2019), the relevant suggestions about the safety of BFR training are put forward for BFR frequency, load, restriction time, cuff pressure, etc., but in the specific BFR training process, it is still necessary to be adjusted according to the different conditions of the subjects. Through literature review, it was found that there were great differences in the settings of these in the existing studies, and there were too few literature within the recommended range and in line with other inclusion criteria of this study. Therefore, the inclusion criteria of this study did not put forward restrictions on the cuff pressure value and time of the experimental BFR group. Therefore, BFR training should be treated with caution to improve the safety and effectiveness of BFR training as a form of exercise. In the future, the design and control factors of BFR training for different populations still need to be further explored, and the added pressure and training load that affect the actual BFR should be fully considered, and a safe and reasonable training scheme should be designed according to individuals’ needs.
This study is the first meta-analysis to explore the effect of BFR training on health promotion in middle-aged and elderly women. All randomized controlled trials were included, and the sources of heterogeneity were carefully analyzed.
The number of included literature was small, with only six RCTs, and some literature were of average quality. This study searched multiple databases in all language types, but the number of relevant studies obtained was small, and some articles were excluded because it was difficult to extract the required data, and too few literature were included in each outcome indicator. In the future, we can further increase the number randomized double-blind controlled trial studies on BFR training in middle-aged and elderly women. The heterogeneity of both heart rate and DBP was high, and the source of heterogeneity was explored. Differences in the health status of subjects, baseline measurement, experimental design and the different exercise type and compression zone might be the source of heterogeneity in this paper. The time and region of included studies might have different impact on the research results.
BFR training has a significant effect on improving and reducing blood pressure in middle-aged and elderly women. Middle-aged and elderly women can be recommended with BFR exercise to improve their health status. There is no significant different effect been observed in regard of improving heart rate and leg pressure strength, and further research is needed in the future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
MF: Writing–original draft, Data curation, Formal Analysis, Investigation, Methodology, Conceptualization. JL: Writing–review and editing, Conceptualization, Project administration, Supervision, Validation, Writing–original draft. JZ: Data curation, Writing–original draft. XP: Data curation, Writing–original draft. MW: Data curation, Writing–original draft. QH: Supervision, Validation, Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by Science Foundation of Ministry of Education of China 22YJC890011.
We would like to thank all the participants who have been involved in the manuscript and authors from included studies.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2024.1392483/full#Supplementary-Material
BFR, blood flow restriction; RCT, randomized controlled trials; M, Mean; SD, Standard Deviation; SMD, standard mean differences; RM, repetition maximum; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Agostini D., Gervasi M., Ferrini F., Bartolacci A., Stranieri A., Piccoli G., et al. (2023). An integrated approach to skeletal muscle health in aging. Nutrients 15 (8), 1802. doi:10.3390/nu15081802
Amato A., Baldassano S., Vasto S., Schirò G., Davì C., Drid P., et al. (2022). Effects of a resistance training protocol on physical performance, body composition, bone metabolism, and systemic homeostasis in patients diagnosed with Parkinson’s disease: a pilot study. Int. J. Environ. Res. Public Health. 19 (20), 13022. doi:10.3390/ijerph192013022
Bao C., He Q., Wang H., Sun Y., Xu Y., Pan Y., et al. (2022). Artemisinin and its derivate alleviate pulmonary hypertension and vasoconstriction in rodent models. Oxid. Med. Cell. Longev. 2022, 2782429. doi:10.1155/2022/2782429
Barili A., Corralo V. D. S., Cardoso A. M., Mânica A., Bonadiman B., Bagatini M. D., et al. (2018). Acute responses of hemodynamic and oxidative stress parameters to aerobic exercise with blood flow restriction in hypertensive elderly women. Mol. Biol. Rep. 45 (5), 1099–1109. doi:10.1007/s11033-018-4261-1
Cai D., Chen S. Y. (2022). Nanoparticle endothelial delivery of PGC-1α attenuates hypoxia-induced pulmonary hypertension by attenuating EndoMT-caused vascular wall remodeling. Redox Biol. 58, 102524. doi:10.1016/j.redox.2022.102524
Carroll J. F., Pollock M. L., Graves J. E., Leggett S. H., Spitler D. L., Lowenthal D. T. (1992). Incidence of injury during moderate- and high-intensity walking training in the elderly. J. Gerontol. 47 (3), M61–M66. doi:10.1093/geronj/47.3.m61
Cezar M., De Sá C., Corralo V., Copatti S., Santos G., Da Silva-Grigoletto M. (2016). Effects of exercise training on blood pressure in medicated hypertensive patients with blood flow restriction. Mot. Rev. Educ. Fis. 22, 9–17. doi:10.1590/s1980-6574201600020002
Clarkson M., Conway L., Warmington S. (2017). Blood flow restriction walking and physical function in older adults: a randomized control trial. J. Sci. Med. Sport 20, 1041–1046. doi:10.1016/j.jsams.2017.04.012
Cristina-Oliveira M., Meireles K., Spranger M. D., O’Leary D. S., Roschel H., Peçanha T. (2020). Clinical safety of blood flow-restricted training? A comprehensive review of altered muscle metaboreflex in cardiovascular disease during ischemic exercise. Am. J. Physiol. Heart Circ. Physiol. 318 (1), H90–H109. doi:10.1152/ajpheart.00468.2019
Dipietro L., Campbell W. W., Buchner D. M., Erickson K. I., Powell K. E., Bloodgood B., et al. (2019). Physical activity, injurious falls, and physical function in aging: an umbrella review. Med. Sci. Sports Exerc. 51 (6), 1303–1313. doi:10.1249/MSS.0000000000001942
Early K. S., Rockhill M., Bryan A., Tyo B., Buuck D., McGinty J. (2020). Effect of blood flow restriction training on muscular performance, pain and vascular function. Int. J. Sports Phys. Ther. 15 (6), 892–900. doi:10.26603/ijspt20200892
Fei W. (2016). A meta-analysis and empirical study on the effects of pressure resistance training on cardiovascular system. Master's thesis, China Institute of Sport Science. doi:10.27984/d.cnki.ggjty.2016.000002
Ferraz R. B., Gualano B., Rodrigues R., Kurimori C. O., Fuller R., Lima F. R., et al. (2018). Benefits of resistance training with blood flow restriction in knee osteoarthritis. Med. Sci. Sports Exerc 50 (5), 897–905. doi:10.1249/MSS.0000000000001530
Franz A., Berndt F., Raabe J., Harmsen J. F., Zilkens C., Behringer M. (2020). Invasive assessment of hemodynamic, metabolic and Ionic consequences during blood flow restriction training. Front. Physiol. 11, 617668. doi:10.3389/fphys.2020.617668
Genping L. (2019). Correlation between bone mineral density and physical exercise in the elderly. Chin. J. Gerontology 39 (12), 2938–2940. doi:10.3969/j.issn.1005-9202.2019.12.037
Guoqiang X. (2006). Effect of physical sports on the body function of old people. Chin. J. Tissue Eng. Res. (08), 129–131. doi:10.3321/j.issn:1673-8225.2006.08.055
Harper S. A., Roberts L. M., Layne A. S., Jaeger B. C., Gardner A. K., Sibille K. T., et al. (2019). Blood-flow restriction resistance exercise for older adults with knee osteoarthritis: a pilot randomized clinical trial. J. Clin. Med. 8 (2), 265. doi:10.3390/jcm8020265
Hughes L., Paton B., Rosenblatt B., Gissane C., Patterson S. D. (2017). Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Br. J. Sports Med. 51 (13), 1003–1011. doi:10.1136/bjsports-2016-097071
Hunter G. R., McCarthy J. P., Bamman M. M. (2004). Effects of resistance training on older adults. Sports Med. 34 (5), 329–348. doi:10.2165/00007256-200434050-00005
Iida H., Nakajima T., Kurano M., Yasuda T., Sakamaki M., Sato Y., et al. (2011). Effects of walking with blood flow restriction on limb venous compliance in elderly subjects. Clin. Physiol. Funct. Imaging 31 (6), 472–476. doi:10.1111/j.1475-097X.2011.01044.x
Kallinen M., Markku A. (1995). Aging, physical activity and sports injuries. An overview of common sports injuries in the elderly. Sports Med. 20 (1), 41–52. doi:10.2165/00007256-199520010-00004
Kargaran A., Abedinpour A., Saadatmehr Z., Yaali R., Amani-Shalamzari S., Gahreman D. (2021). Effects of dual-task training with blood flow restriction on cognitive functions, muscle quality, and circulatory biomarkers in elderly women. Physiol. Behav. 239, 113500. doi:10.1016/j.physbeh.2021.113500
Kittleson M. M., Panjrath G. S., Amancherla K., Davis L. L., Deswal A., Dixon D. L., et al. (2023). 2023 ACC expert consensus decision pathway on management of heart failure with preserved ejection fraction: a report of the American college of cardiology solution set oversight committee. J. Am. Coll. Cardiol. 81 (18), 1835–1878. doi:10.1016/j.jacc.2023.03.393
Kraemer W. J., Ratamess N. A. (2004). Fundamentals of resistance training: progression and exercise prescription. Med. Sci. Sports Exerc 36 (4), 674–688. doi:10.1249/01.mss.0000121945.36635.61
Letieri R. V., Furtado G. E., Barros P. M. N., Farias M. J. A. D., Antunez B. F., Gomes B. B., et al. (2019). Effect of 16-week blood flow restriction exercise on functional fitness in sarcopenic women: a randomized controlled trial. Int. J. Morphol. 37, 59–64. doi:10.4067/s0717-95022019000100059
Li J. Z. P. (2022). Research progress on the effect of resistance training on cardiovascular health of middle-aged and elderly women. Contemp. Sports Technol. 12 (01), 20–26. doi:10.16655/j.cnki.2095-2813.2109-1579-3410
Li Y., Talotta-Altenburg L. M., Silimperi K. A., Ciabattoni G. O., Lowe-Krentz L. J. (2020). Endothelial nitric oxide synthase activation is required for heparin receptor effects on vascular smooth muscle cells. Am. J. Physiol. Cell. Physiol. 318 (3), C463–C475. doi:10.1152/ajpcell.00284.2018
Linero C., Choi S.-J. (2021). Effect of blood flow restriction during low-intensity resistance training on bone markers and physical functions in postmenopausal women. J. Exerc. Sci. Fit. 19 (1), 57–65. doi:10.1016/j.jesf.2020.09.001
Linlin J. (2023). There are more than 280 million senior citizens aged 60 or above. Chinese newspapers for the elderly. doi:10.28108/n.cnki.nclnb.2023.000452
Liu Haoyan W. X., Xing Y., Wu Y. (2023). Effects of KAATSU training on lower limb muscle strength in middle-aged and elderly people: a meta-analysis. China Sport Sci. Technol. 59 (07), 71–80. doi:10.16470/j.csst.2021051
Ma W., Liu Y., Qi G., Ying Y. (2020). Analysis of multi-cause falls in the elderly with balance dysfunction. Chin. J. Rehabilitation 35 (10), 547–551. doi:10.3870/zgkf.2020.10.010
Maciel A. W. S., Pinto L. M., Campos R. C. A., Ferreira A. C., Dias-Filho C. A. A., Dias C. J. M., et al. (2021). Acute effects of resistance exercise with blood flow restriction in elderly women: a pilot study. J. Aging Phys. Act. 29 (3), 361–371. doi:10.1123/japa.2020-0137
Madarame H., Ochi E., Tomioka Y., Nakazato K., Ishii N. (2011). Blood flow-restricted training does not improve jump performance in untrained young men. Acta Physiol. Hung 98 (4), 465–471. doi:10.1556/APhysiol.98.2011.4.10
Mammucari C., Milan G., Romanello V., Masiero E., Rudolf R., Del Piccolo P., et al. (2007). FoxO3 controls autophagy in skeletal muscle in vivo. Cell. Metab. 6 (6), 458–471. doi:10.1016/j.cmet.2007.11.001
Mânica A., De Sá C. A., Barili A., Corralo V. S., Bonadiman B. S., Oliveira G. G., et al. (2020). Exercise with blood flow restriction as a new tool for health improvement in hypertensive elderly women: the role of purinergic enzymes. J. Sports Med. Phys. Fit. 60 (11), 1477–1485. doi:10.23736/S0022-4707.20.10956-3
Manini T. M., Vincent K. R., Leeuwenburgh C. L., Lees H. A., Kavazis A. N., Borst S. E., et al. (2011). Myogenic and proteolytic mRNA expression following blood flow restricted exercise. Acta Physiol. (Oxf) 201 (2), 255–263. doi:10.1111/j.1748-1716.2010.02172.x
Naidu S. S., Baran D. A., Jentzer J. C., Hollenberg S. M., van Diepen S., Basir M. B., et al. (2022). SCAI SHOCK stage classification expert consensus update: a review and incorporation of validation studies: this statement was endorsed by the American college of cardiology (ACC), American college of emergency physicians (ACEP), American heart association (AHA), European society of cardiology (ESC) association for acute cardiovascular care (ACVC), international society for heart and lung transplantation (ISHLT), society of critical care medicine (SCCM), and society of thoracic surgeons (STS) in December 2021. J. Am. Coll. Cardiol. 79 (9), 933–946. doi:10.1016/j.jacc.2022.01.018
Ozaki H., Miyachi M., Nakajima T., Abe T. (2011). Effects of 10 weeks walk training with leg blood flow reduction on carotid arterial compliance and muscle size in the elderly adults. Angiology 62 (1), 81–86. doi:10.1177/0003319710375942
Ozawa Y., Koto T., Shinoda H., Tsubota K. (2015). Vision loss by central retinal vein occlusion after KAATSU training: a case report. Med. Baltim. 94 (36), e1515. doi:10.1097/MD.0000000000001515
Pan Yanrong F. Y., Wang M., Yuan J., Liang M., Li S. (2021). On the adaptive mechanism,dose-effect relationship and safety of KAATSU training. J. Xichang Univ. 35 (02), 98–105+19. doi:10.16104/j.issn.1673-1891.2021.02.018
Patterson S. D., Hughes L., Warmington S., Burr J., Scott B. R., Owens J., et al. (2019). Blood flow restriction exercise: considerations of methodology, application, and safety. Front. Physiol. 10, 533. doi:10.3389/fphys.2019.00533
Pinto R. R., Karabulut M., Poton R., Polito M. D. (2018). Acute resistance exercise with blood flow restriction in elderly hypertensive women: haemodynamic, rating of perceived exertion and blood lactate. Clin. Physiol. Funct. Imaging 38 (1), 17–24. doi:10.1111/cpf.12376
Price O. J., Tsakirides C., Gray M., Stavropoulos-Kalinoglou A. (2019). ACSM preparticipation health screening guidelines: a UK university cohort perspective. Med. Sci. Sports Exerc 51 (5), 1047–1054. doi:10.1249/MSS.0000000000001868
Ronghai S. (2019). Study on the practical application and physiological mechanism of pressure training to promote muscle fitness. Chin. J. Rehabilitation Med. 34 (07), 856–861. doi:10.3969/j.issn.1001-1242.2019.07.022
Ruaro M., Santana J., Gusmão N., De França E., Nascimento-Carvalho B., Farinazo K., et al. (2019). Effects of strength training with and without blood flow restriction on quality of life in elderly women. doi:10.7752/jpes.2019.01078
Sandri M., Sandri C., Gilbert A., Skurk C., Calabria E., Picard A., et al. (2004). Foxo transcription factors induce the atrophy-related ubiquitin ligase atrogin-1 and cause skeletal muscle atrophy. Cell. 117 (3), 399–412. doi:10.1016/s0092-8674(04)00400-3
Santler B., Goerge T. (2017). Chronic venous insufficiency - a review of pathophysiology, diagnosis, and treatment. J. Dtsch. Dermatol Ges. 15 (5), 538–556. doi:10.1111/ddg.13242
Sato Y. (2005). The history and future of KAATSU Training. Int. J. KAATSU Train. Res. 1 (1), 1–5. doi:10.3806/ijktr.1.1
Silva J., Neto G., Freitas E., Pereira Neto E., Batista G., Torres M., et al. (2015). Chronic effect of strength training with blood flow restriction on muscular strength among women with osteoporosis. J. Exerc. Physiologyonline. 18, 33–41.
Slysz J., Stultz J., Burr J. F. (2016). The efficacy of blood flow restricted exercise: a systematic review & meta-analysis. J. Sci. Med. Sport 19 (8), 669–675. doi:10.1016/j.jsams.2015.09.005
Spranger M. D., Krishnan A. C., Levy P. D., O’Leary D. S., Smith S. A. (2015). Blood flow restriction training and the exercise pressor reflex: a call for concern. Am. J. Physiol. Heart Circ. Physiol. 309 (9), H1440–H1452. doi:10.1152/ajpheart.00208.2015
Teixeira E. L., Barroso R., Silva-Batista C., Laurentino G. C., Loenneke J. P., Roschel H., et al. (2018). Blood flow restriction increases metabolic stress but decreases muscle activation during high-load resistance exercise. Muscle Nerve 57 (1), 107–111. doi:10.1002/mus.25616
Thiebaud R. S., Loenneke J. P., Fahs C. A., Rossow L. M., Kim D., Abe T., et al. (2013). The effects of elastic band resistance training combined with blood flow restriction on strength, total bone-free lean body mass and muscle thickness in postmenopausal women. Clin. Physiol. Funct. Imaging 33 (5), 344–352. doi:10.1111/cpf.12033
Vechin F. C., Libardi C. A., Conceição M. S., Damas F. R., Lixandrão M. E., Berton R. P., et al. (2015). Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J. Strength Cond. Res. 29 (4), 1071–1076. doi:10.1519/JSC.0000000000000703
Wang L. M., Chen Z. H., Zhang M., Zhao Z. P., Huang Z. J., Zhang X., et al. (2019). Study of the prevalence and disease burden of chronic disease in the elderly in China. Zhonghua Liu Xing Bing Xue Za Zhi 40 (3), 277–283. doi:10.3760/cma.j.issn.0254-6450.2019.03.005
Wei Jia L. B., Yang W., Wang X., Feng L., Li Y. (2019). The effects and mechanisms of blood flow restriction training. China Sport Sci. 39 (04), 71–80. doi:10.16469/j.css.201904008
Wu J., Fang S., Lu K. T., Kumar G., Reho J. J., Brozoski D. T., et al. (2022). Endothelial cullin3 mutation impairs nitric oxide-mediated vasodilation and promotes salt-induced hypertension. Funct. (Oxf) 3 (3), zqac017. doi:10.1093/function/zqac017
Xiong W., Liu X. (2023). Effects of whole-body vibration training combined with KAATSU training on lower limb joint muscle strength in older women. Front. Physiol. 14, 1231088. doi:10.3389/fphys.2023.1231088
Yasuda T., Abe T., Brechue W. F., Iida H., Takano H., Meguro K., et al. (2010). Venous blood gas and metabolite response to low-intensity muscle contractions with external limb compression. Metabolism 59 (10), 1510–1519. doi:10.1016/j.metabol.2010.01.016
Yasuda T., Abe T., Sato Y., Midorikawa T., Kearns C. F., Inoue K., et al. (2005). Muscle fiber cross-sectional area is increased after two weeks of twice daily KAATSU-resistance training. Int. J. KAATSU Train. Res. 1 (2), 65–70. doi:10.3806/ijktr.1.65
Yasuda T., Fukumura K., Tomaru T., Nakajima T. (2016). Thigh muscle size and vascular function after blood flow-restricted elastic band training in older women. Oncotarget 7 (23), 33595–33607. doi:10.18632/oncotarget.9564
Yu Wei S. G., Liu Y. (2022). Benefit and physiological mechanism of low-intensity resistance training withblood flow restriction intervention on muscle fitness. Chin. J. Tissue Eng. Res. 26 (17), 2768–2774. doi:10.12307/2022.549
Zhang T., Tian G., Wang X. (2022). Effects of low-load blood flow restriction training on hemodynamic responses and vascular function in older adults: a meta-analysis. Int. J. Environ. Res. Public Health 19 (11), 6750. doi:10.3390/ijerph19116750


Keywords: blood flow restriction, KAATSU, elderly women, BFR, health
Citation: Feng M, Li J, Zhao J, Pan X, Wang M and Han Q (2024) Effect of blood flow restriction training on health promotion in middle-aged and elderly women: a systematic review and meta-analysis. Front. Physiol. 15:1392483. doi: 10.3389/fphys.2024.1392483
Received: 27 February 2024; Accepted: 06 June 2024;
Published: 02 July 2024.
Edited by:
Mallikarjuna Korivi, Zhejiang Normal University, ChinaReviewed by:
Alessandra Amato, University of Catania, ItalyCopyright © 2024 Feng, Li, Zhao, Pan, Wang and Han. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jian Li, bGlqaWFuMjUwNkBic3UuZWR1LmNu; Qi Han, aGFucWkwNDE4QDE2My5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.