Introduction
Cardiorespiratory fitness (i.e., maximum oxygen consumption) is an independent predictor of all-cause mortality in adults, and an important marker of health in children (Imboden et al., 2018; Raghuveer et al., 2020). Cardiopulmonary exercise testing (CPET) is used to measure maximum oxygen consumption (O2max), the gold-standard measure for determining cardiorespiratory fitness, defined as a plateau in O2 despite an increasing workload (Taylor et al., 1955). Measuring O2max in children can be challenging as only a fraction of them reach O2 plateau (COOPER and WEILER-RAVELL, 1984), leading to the common utilization of O2peak, which refers to the highest O2 achieved during CPET. Most of the time, effort criteria such as the peak respiratory exchange ratio [carbon dioxide production (CO2peak)/O2peak], peak heart rate, and the rate of perceived exertion are used to assist in establishing O2peak. However, factors such as obesity, underlying comorbidities, or insufficient personal motivation may impose limitations on children’s capacity to exert maximum effort and achieve the criteria for O2peak. Consequently, this may result in the loss of data.
The oxygen uptake efficiency slope (OUES) is a submaximal metric utilized in CPET to assess the relationship between oxygen consumption (O2, mL/min) and minute ventilation (E, L/min) (Baba et al., 1996). OUES serves as a measure of ventilatory efficiency in relation to oxygen consumption during submaximal exercise. The OUES has found utility as an independent predictor of mortality in adult patients with idiopathic pulmonary hypertension and heart failure (Tang et al., 2017; Lin et al., 2016; Chiang et al., 2024). It is currently unknown whether the OUES can differentiate between healthy children and children with various diseases, but the evidence in adults suggests this.
More recently, the OUES was proposed as a predictor of O2peak in children (Akkerman et al., 2010; Dias et al., 2017; Breithaupt et al., 2012), but results are inconsistent across the literature (Drinkard et al., 2007; Sheridan et al., 2021). Two studies evaluated the comparability of measured O2peak and estimates of O2peak derived from the OUES (Pred-O2peak) in adolescents with obesity (Sheridan et al., 2021), and in 15 years old male adolescents (Drinkard et al., 2007). The authors reported moderate to strong correlation between Pred-O2peak and measured O2peak. However, the values derived from OUES showed large interindividual variation and magnitude bias suggesting that the OUES may not accurately predict O2peak in adolescents. The majority of studies concluding that the OUES is an acceptable alternative to O2peak have relied on correlation or regression statistics to compare both variables. A limitation of this approach is that correlations and regressions do not provide insight into bias or level of agreement between methods.
Studies evaluating the level of agreement between measured O2peak and Pred-O2peak in young children are lacking. To address this limitation, we conducted a secondary analysis examining the validity of OUES in estimating measured O2peak in 7-to-10-year-old children who participated in the Arkansas Active Kids study (NCT03221673). Based on the limited evidence in adolescents, we hypothesized that O2peak values predicted from OUES (Pred-O2peak) do not consistently agree with individually measured O2peak across the range of O2peak values (from lower O2peak to higher O2peak) in our cohort. Therefore, we hypothesized that OUES may not be a reliable predictor of O2peak in young children.
Methods
Subjects
This is a post hoc analysis of data collected from a subset of 94 children enrolled in the Arkansas Active Kids Study (AAK, NCT03221673) who met O2peak criteria as described in the Measurements section. The AAK study is a cross-sectional observational study aimed at identifying modifiable risk factors and phenotypes negatively associated with metabolic health of children. Details of the study protocol and design have been published elsewhere (Bai et al., 2020). Following an overnight fast, participants’ ages 7–10 years attended one study visit at the Arkansas Children’s Nutrition Center, Laboratory for Active Kids and Families. They were advised to avoid strenuous exercise the day before the study visit, but were not required to refrain from all physical activity. All participants were considered in good health. Exclusion criteria were type 1 or type 2 diabetes mellitus; severe persistent asthma (determined by daily use of oral/inhaled corticosteroid to keep asthma symptoms under control and/or frequent use of rescue inhaler) heart disease that required medication; neurological, kidney, liver, hormonal, lung or autoimmune disease; cancer; bleeding disorder; and pre-existing medical conditions or medications as determined by the investigators to affect the outcomes of interest. The Institutional Review Board at the University of Arkansas for Medical Sciences approved the study protocol. All parents and children gave written informed consent and assent, respectively.
Measurements
Anthropometry and body composition
Body weight (kg) and height (cm) were measured using a digital scale (Seca 877, Seca GbmH and Co. KG, Hamburg, Germany) to the nearest 0.1 kg and 0.1 cm, respectively, and triplicate values were averaged. Body mass index (BMI, kg/m2) was calculated and BMI percentiles were estimated using the Center for Disease Control and Prevention growth charts for ages 2–20 years (Canadian Pediatric Endocrine Group). Body composition was assessed using dual-energy X-ray absorptiometry (DXA, Horizon-A with Advanced Body Composition™, Hologic, Bedford, MA, United States). Fat mass (FM) index [FMI = FM (kg)/height2 (m2)] and fat-free mass (FFM) index [FFMI = FFM (kg)/height2 (m2)] were computed.
Cardiopulmonary exercise testing
O2peak was assessed through an incremental exercise test on a pediatric cycle ergometer (Corival Pediatric, Lode, Groningen, Netherlands). Seat height was modified using a goniometer to a corresponding knee angle of 150°. Incremental workload watts (W) were based on the participants’ height and were as follows: 10 W for children <125 cm tall, 15 W for children ≥125 < 150 cm tall, and 20 W for children ≥150 cm tall. Workloads increased in a stepwise fashion every minute throughout testing. Following a 1-min resting period and 1-min unloaded warmup, workload increased every minute, and participants were asked to keep a pedal frequency of 60–70 rpm. Participants were free to stop the test at any time but were encouraged to perform until voluntary exhaustion. Testing was terminated when the pedal frequency could not be maintained despite strong verbal encouragement. While testing, children were required to wear an indirect calorimetry facemask in order to assess their O2, CO2, and E (Medgraphics Ultima PFX® system, MGC Diagnostics Corporation, St Paul, MN, United States). Prior to the tests, flow and gas calibrations were performed according to the manufacturer’s instructions. Participants also wore a heart rate monitor (Zephyr™ Heart Rate Monitor) or electrocardiogram (Mortara 12-Lead ECG) to measure heart rate during the exercise test. Participants initially underwent heart rate monitoring using Mortara 12-Lead ECG; however, to enhance practicality during the course of the study, we transitioned to the Zephyr™ Heart Rate Monitor.
Criteria for O2peak
O2peak was determined using the highest 20-s average achieved during the final minute prior to exercise test termination. To classify the effort as a O2peak, all three criteria had to be met: a rating of perceived exertion ≥8 on the OMNI scale (Utter et al., 2002), a peak heart rate ≥185 beats/min (or ≥85% of predicted peak heart rate), and a respiratory exchange ratio (RER) ≥ 1.0. Only children who met all three criteria were included in the analysis.
OUES determination
OUES is a slope calculation of O2 versus logarithmically transformed E (in order to create a linear relationship) and is calculated based on this relationship during incremental exercise, where E (L/min) is positioned on the x-axis and O2 (mL/min) on the y-axis. OUES is determined by equation O2 = a log E + b, where ‘a' represents the OUES value (Baba et al., 1996). Higher O2 values with lower E values create a steeper slope indicative of higher cardiorespiratory fitness (CRF) compared to lower slopes. The OUES slope including all respiratory data from the start of the workload up to test termination was assessed (OUES100%). If a plateau in O2 occurred, subsequent data points were excluded. Additionally, to assess OUES at submaximal intensity, an OUES slope was calculated using data only from the start of the workload until a heart rate corresponding to 60% of heart rate reserve (HRR) was reached (OUES60%HRR). For the OUES60%HRR method, HRR was first calculated by subtracting the participant’s resting heart rate from their age-predicted maximum heart rate (208–0.7 x age) (Tanaka et al., 2001). HRR was then multiplied by 0.6, and the participant’s resting heart rate added back to obtain the target heart rate. The slope was then calculated using data from the start of the workload until the target heart rate was reached.
Statistical analysis
Data measures in the interval scale are summarized as mean ± SD whereas data measures in the ordinal or nominal scale are summarized as percentages and counts. Simple linear regression analysis modeled the association of measured O2peak (ml/min, dependent variable) with OUES60%HRR, age (years), sex, race (White and Black), BMI percentile, FMI, and FFMI (independent variables). For statistical analysis, sex and race were dichotomized as 0 or 1, with 0 representing girls and Black individuals, and 1 representing boys or White individuals, respectively. The best-fitted model was created using stepwise multiple linear regression analysis. Regression equations to predict O2peak were derived from simple and multiple linear regression analysis. Regression analyses are presented as parameter estimate (β), standard error (SE), 95% confidence interval (95% CI), R-squared (R2), and variance of inflation factor (VIF) when applicable.
Bland-Altman analysis (Bland and Altman, 1986) was used to evaluate the level of agreement between predicted values O2peak (Pred-O2peak) obtained from regression analysis, and O2peak measured using gold standard techniques. Mean bias between methods was assessed using a two-sample t-test. Magnitude bias was assessed by regressing the difference between the methods on the average of the two methods. The Pearson correlation coefficient was used to measure the correlation of measured O2peak with OUES60%HRR, OUES100%, and Pred-O2peak. Statistical analyses were conducted with SAS® 9.4 (Cary, NC, U.S.A).
Results
Participant characteristics
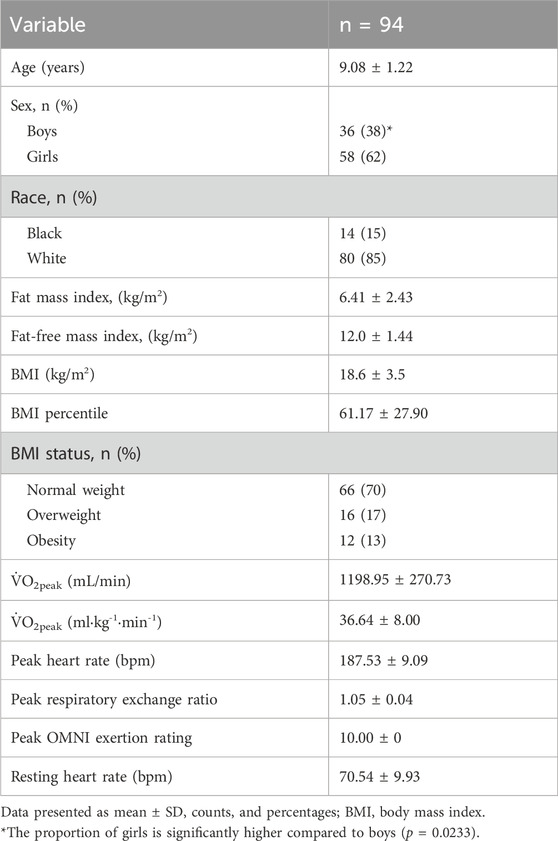
Children (9.1 ± 1.2 years) were predominantly White (85%), with Black children comprising 15% of the cohort. The proportion of girls was higher compared to boys (62% vs. 38%, p = 0.0233). Thirty percent of children had overweight or obesity while 70% of children had normal weight (Table 1).
Bivariate associations between O2peak (mL/min) and variables of interest
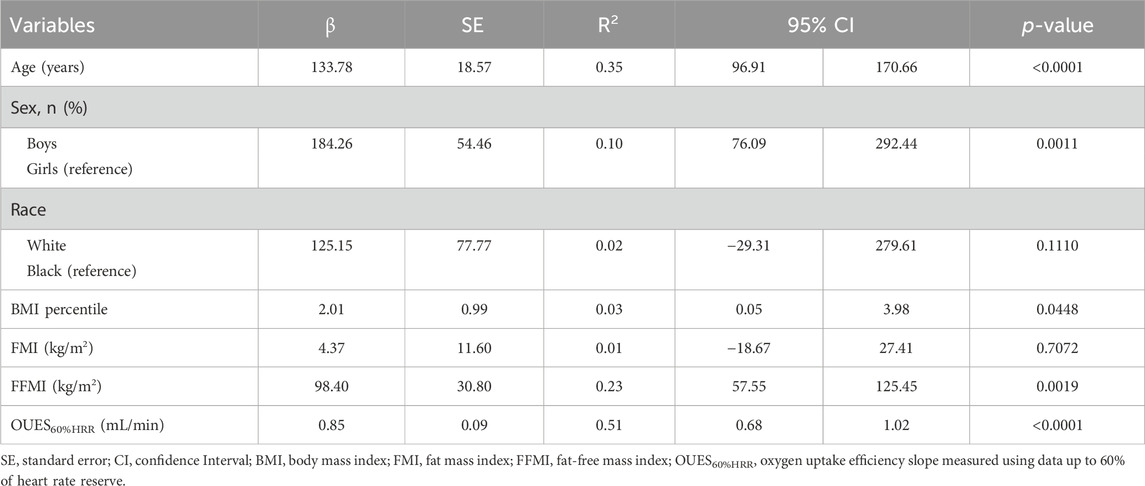
O2peak was independently and positively associated with OUES60%HRR (β = 0.85, p < 0.0001), age (β = 133.8, p < 0.0001), male sex (β = 184.3, p = 0.0011), BMI percentile (β = 2.0, p = 0.0448), and FFMI (98.4, p = 0.0019) (Table 2).
Results from stepwise multiple linear regression analysis modeling the association of O2peak (mL/min) with subject characteristics and OUES60%HRR
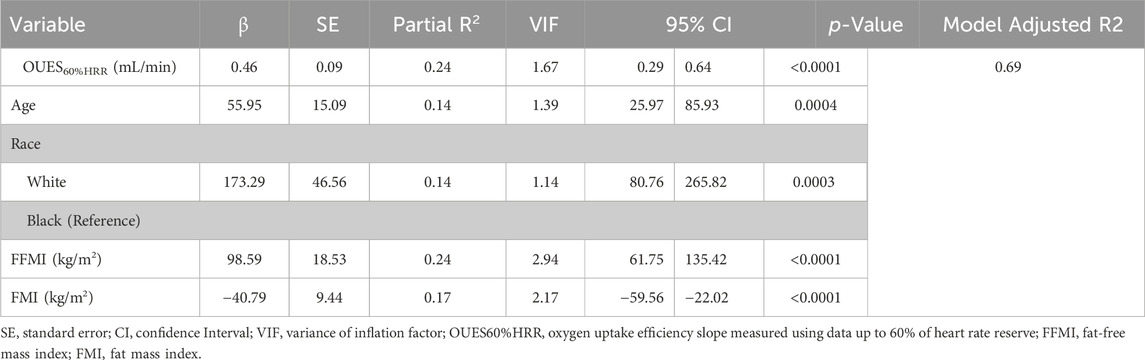
Age, race, sex, FFMI, FMI, height, and OUES60%HRR were all considered in the analysis. OUES60%HRR (β = 0.46, p < 0.0001), age (β = 56.0, p = 0.0004), White race (β = 173.3, p < 0.0003), FFMI (β = 0.98 p < 0.000), and FMI (β = −0.40.8, p < 0.000) were retained in the final model. Sixty-nine percent of the observed variance in O2peak was predicted by this model (Table 3).
Regression equations used to predict O2peak (mL/min) from OUES60%HRR and other variables of interest
Equation 1 derived from the bivariate association between O2peak and OUES60%HRR
Equation 2 derived from multiple linear regression analysis in which OUES and other significant explanatory variables are considered.
Correlation of Pred-O2peak (mL/min) with OUES60%HRR, and OUES100%
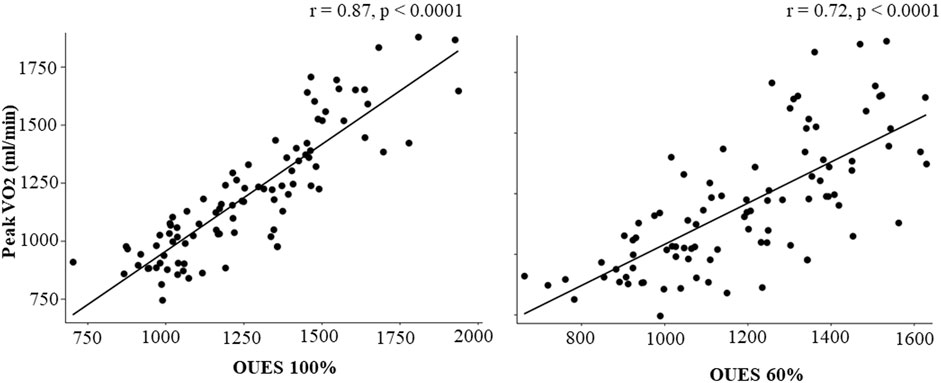
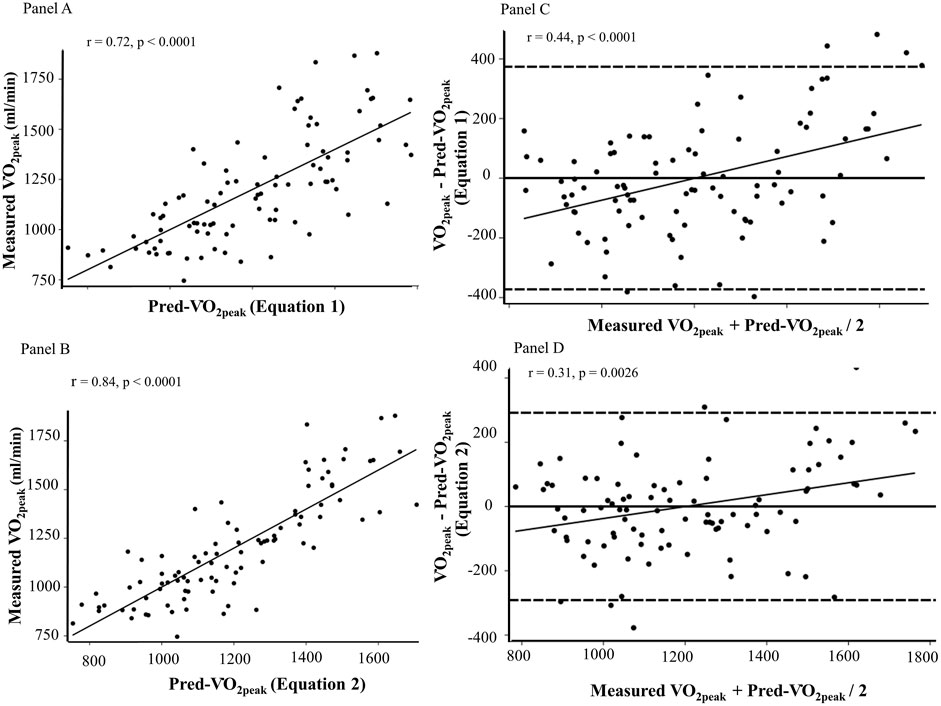
OUES60%HRR (r = 0.72, p < 0.0001) and OUES100% (r = 0.87, p < 0.0001) positively correlated with measured O2peak (Figure 1). Pred-O2peak estimated from Equation 1 (r = 0.72, p < 0.0001) and Equation 2 (r = 0.84, p < 0.0001) positively correlated with measured O2peak (Figure 2, Panel A and B).
Agreement between measured O2peak (mL/min) and Pred-O2peak (mL/min)
The average of Pred-O2peak obtained from Equation 1 (1198.95 ± 270.73 mL/min) and 2 (1198.95 ± 227.92 mL/min) were comparable to the average of measured O2peak (1198.95 ± 270.73, p = 0.9999). The Bland-Altman plots (Figure 2, Panel C and D) show the mean of the difference of measured O2peak - Pred-O2peak at zero (solid black line) thus indicating no mean bias between methods with neither Equation 1 (mean difference ± 2SD: 0.0 ± 372.9, p = NS) nor Equation 2 (mean difference = 0.0 ± 311.3). There was magnitude bias as indicated by the positive association between the difference of measured O2peak–Pred-O2peak (y-axis) and the average of the two methods (x-axis) when Pred-O2peak estimates were computed using Equation 1 [β = 0.38 (confidence level (CL) = 0.22–0.55), p < 0.0001] and 2 [β = 0.79 (CL = 0.07–0.31), p = 0.0028].
Discussion
The aim of this study was to evaluate the level of agreement between directly measured O2peak (mL/min) with O2peak estimated from OUES60%HRR in school-age children. Our findings showed no mean bias between methods. However, magnitude bias was present even after considering other significant predictors of O2peak (FMI, FFMI, race, and age) in the regression equation. Specifically, there was an increase in bias (the difference between methods) as the magnitude of the measurements increased (the mean of both methods). The presence of magnitude bias indicates that the accuracy of the prediction varies depending on the level of O2peak, which may limit the interchangeability of OUES-derived O2peak predictions with directly measured O2peak.
Contrary to previous studies that have supported the interchangeability of OUES and O2max or O2peak in school-age children, our results caution against this practice. We observed positive correlations between OUES60%HRR and OUES100% with measured O2peak, as well as with predicted O2peak using two different equations. However, the Bland-Altman plots revealed magnitude bias (Figure 2, Panels C and D), indicating that the agreement between measured O2peak and OUES-predicted O2peak varies across the range of measurements. Consequently, we found large interindividual variations between the OUES-predicted O2peak and the measured O2peak despite identical group averages (1198.95 ± 270.73 mL/min and 1198.95 ± 270.73, respectively). These results underscore the importance of considering not only mean bias and correlation, but also magnitude bias when evaluating the agreement between methods. Submaximal moderate intensity estimate methods, like the OUES60%HRR, may be useful as a rough estimate of CRF in scenarios where maximal testing is impractical or not well-tolerated. However, as our findings demonstrate, while a submaximal OUES end-point provides a strong correlation, the presence of magnitude bias indicates that caution should be used when attempting to apply submaximal estimates interchangeably with directly measured O2peak. Our findings highlight the importance of considering both the convenience of submaximal measures and their limitations in accurately representing CRF.
The concept of OUES was first introduced by Baba et al. (Baba et al., 1996) as an index of cardiorespiratory reserve derived from submaximal data during an incremental exercise test. The authors reported this index to be a useful indicator of cardiorespiratory efficiency in children (mean age 11.7 ± 4.4 years) that has a strong correlation to O2max. Thus, they concluded it may be a helpful tool to aid clinicians in monitoring cardiorespiratory status over time. Following its introduction, several studies have evaluated the use of OUES as an indicator of cardiorespiratory fitness in a wide range of populations. There has been a consistently strong correlation seen between OUES and O2max or O2peak (Breithaupt et al., 2012; Drinkard et al., 2007; Sheridan et al., 2021; Pichon et al., 2002; Marinov et al., 2007) in all populations studied (healthy, overweight/obese, cardiovascular and pulmonary disease, etc.). Therefore, the majority of these studies typically report on its potential as a surrogate for O2max or O2peak, especially in those who are unable to give maximum effort. However, Drinkard et al., 2007, Sheridan et al., 2021; Pichon et al., 2002 all noted the wide limits of agreement found by using Bland-Altman analysis, with Pichon observing a ±10.5 mL kg-1·min-1 limit of agreement. A strong limitation of the published evidence in children has been the generalized use of correlation coefficients and linear regression analysis as indicators of agreement between OUES-derived estimates of O2peak and measured O2peak. Correlation is a metric that quantifies the degree of a linear relationship, rather than indicating agreement. For instance, a change in the scale of a measurement does not impact the correlation, but it does affect the agreement. Therefore, inferring that methods can be used interchangeably based solely on a high correlation is not recommended.
Marinov et al. (Marinov et al., 2007) studied 114 children (58 boys and 56 girls) ages 7–18 years to assess the correlation between OUES and O2peak. The authors found no difference in OUES values estimated up to the anaerobic threshold (2600 ± 650 mL/min) and up to peak exercise (2600 ± 650 mL/min). In addition, there was a strong correlation between OUES and O2peak (r = 0.92). In light of this, the authors concluded that OUES is an objective measure of exercise capacity in the pediatric population. However, the study relied on correlation analysis to draw their conclusion, which does not provide a comprehensive assessment of agreement. Similarly, in our study, we observed strong correlations between OUES-derived predicted equations (Equation (1) r = 0.72; Equation (2) r = 0.84) with measured O2peak. However, the absence of magnitude bias assessment in the Marinov et al. study limits the evaluation of OUES accuracy in predicting O2peak. Consequently, our Bland-Altman analysis suggests differing conclusions despite similar methods and correlation strengths.
Only two studies in adolescents (Drinkard et al., 2007; Sheridan et al., 2021) have used alternative statistical approaches to evaluate the comparability between methods. Drinkard et al. (Drinkard et al., 2007) studied n = 150 (n = 107 with obesity and n = 43 with normal weight) adolescents. Initially, 141 adolescents with obesity were screened for eligibility, but 34 of them (24%) did not meet peak criteria and were not included in the analysis. This highlights the importance of exploring alternative methods for predicting O2peak in children with obesity. The authors evaluated the level of agreement in predicting O2peak using OUES at different exercise intensities. Magnitude bias was observed across all intensity levels with large limits of agreement (±478 to ±670 mL/min) despite a moderate to strong correlation range (r = 0.35–0.83). Consequently, the authors concluded that OUES-derived predictions of O2peak offer limited value in predicting CRF in individuals. Similarly, Sheridan et al. (Sheridan et al., 2021) reported magnitude bias with large limits of agreement (±937.5 mL/min) between OUES-predicted and measured O2peak of healthy 15-year-old males, despite a strong correlation (r = 0.77) between the two. Our findings align with these studies in adolescents, as we observed magnitude bias with large limits of agreement (±311.3 mL/min) despite strong correlation strength. Performing Bland-Altman analysis in our study provided a more comprehensive evaluation of OUES-derived predictions of O2peak. While our best-fitted model yielded narrower limits of agreement than Drinkard et al., 2007; Sheridan et al., 2021, there is still significant magnitude bias, and a large variation up to ±311.3 mL/min. This highlights the need for a more accurate OUES-derived equation before interchangeable use with O2peak. Therefore, our study helps fill the existing knowledge gap regarding the application of OUES as a means to predict peak cardiopulmonary capacity in children across developmental stages.
Limitations
Participants in this study were predominantly White; therefore, extrapolation of these results to other races must be done with caution. While our criteria for classifying O2peak are in line with current pediatric recommendations, it should be acknowledged that this variable could be prone to underestimation in this population if using less conservative criteria.
One could argue a limitation of our study is the use of the same group of subjects for both deriving the OUES method and subsequently testing it against measured O2peak. This methodological choice likely led to the zero mean bias observed in the Bland-Altman analysis, as the prediction equations were optimized based on the same dataset. This bias could give the impression that the OUES method is more accurate than it might be if applied to an independent cohort. It is important to recognize that using an independent group of subjects for validation is a more robust approach, as it reduces the risk of overfitting and provides a clearer picture of the method’s generalizability. In future studies, we recommend that the OUES method be validated in a separate cohort to ensure that the bias is not artificially minimized, and to better assess the true predictive performance of the method. Despite this limitation, the Bland-Altman analysis in our study still provides valuable information about the variability between the estimated and measured O2peak values. However, readers should interpret the zero mean bias with caution, understanding that it may not fully reflect the method’s accuracy in a broader population.
Experimental considerations
The study is strengthened by the use of direct measurements of body composition and the inclusion of multiple variables in the regression analysis, which enhances the comprehensiveness of the study into factors influencing the use of OUES as a predictor of O2peak. While our study emphasizes caution in interpreting the OUES as an accurate predictor for O2peak in children, the OUES still offers important insights into cardiorespiratory efficiency during submaximal exercise, especially in those who are unable or unwilling to give maximum effort. Clinicians and researchers should consider the context of its use, and the goal of their assessments when deciding to use the OUES. Future research should focus on developing novel models that better reflect the relationship between O2 and E by incorporating additional variables or further adjustments that account for individual differences. Accurate estimates of O2peak in children with varying ranges of cardiorespiratory fitness and BMI are needed. OUES estimates of O2peak and gold standard measurements of O2peak do not agree equally throughout the range of measurements. Therefore, caution is advised when using OUES to predict O2peak in children.
In conclusion, our comprehensive OUES-derived equation, incorporating age, race, sex, FFMI, and FMI, demonstrated a strong correlation with measured O2peak. However, the presence of magnitude bias and large interindividual variation indicates that the OUES is not an accurate predictor of CRF in children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the University of Arkansas for Medical Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
TE: Writing–review and editing, Writing–original draft, Data curation. EB: Writing–review and editing, Writing–original draft, Investigation, Conceptualization. JW: Writing–review and editing, Writing–original draft, Investigation, Conceptualization. ED: Writing–review and editing, Writing–original draft, Investigation, Conceptualization.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was funded by USDA-ARS Projects 3092-51000-056-04A and 6026-51000-012-06S. ED, EB, and JW are partially supported by NIH-NIGMS award 5P20GM109096.
Acknowledgments
The authors thank the children and their families for their participation in this study, and Isania Bazan, MSc, for support with data analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Akkerman M., VAN Brussel M., Bongers B. C., Hulzebos E. H., Helders P. J., Takken T. (2010). Oxygen uptake efficiency slope in healthy children. Pediatr. Exerc Sci. 22, 431–441. doi:10.1123/pes.22.3.431
PubMed Abstract | CrossRef Full Text | Google Scholar
Baba R., Nagashima M., Goto M., Nagano Y., Yokota M., Tauchi N., et al. (1996). Oxygen uptake efficiency slope: a new index of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. J. Am. Coll. Cardiol. 28, 1567–1572. doi:10.1016/s0735-1097(96)00412-3
PubMed Abstract | CrossRef Full Text | Google Scholar
Bai S., Goudie A., Borsheim E., Weber J. L. (2020). The Arkansas Active Kids Study: identifying contributing factors to metabolic health and obesity status in prepubertal school-age children. Nutr. Health 27, 273–281. doi:10.1177/0260106020975571
PubMed Abstract | CrossRef Full Text | Google Scholar
Bland J. M., Altman D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307–310.
PubMed Abstract | Google Scholar
Breithaupt P. G., Colley R. C., Adamo K. B. (2012). Using the oxygen uptake efficiency slope as an indicator of cardiorespiratory fitness in the obese pediatric population. Pediatr. Exerc Sci. 24, 357–368. doi:10.1123/pes.24.3.357
PubMed Abstract | CrossRef Full Text | Google Scholar
Chiang W. J., Lee J. T., Hung S. Y., Hsu P. C., Chou C. L. (2024). Prognostic value of body surface area-adjusted oxygen uptake efficiency slope in heart failure patients. Acta Cardiol. Sin. 40, 322–330. doi:10.6515/ACS.202405_40(3).20240105A
PubMed Abstract | CrossRef Full Text | Google Scholar
Dias K. A., Masterson C. E., Wallen M. P., Tjonna A. E., Hosseini M. S., Davies P. S. W., et al. (2017). Assessment of the 5-minute oxygen uptake efficiency slope in children with obesity. Pediatr. Exerc Sci. 29, 350–360. doi:10.1123/pes.2016-0248
PubMed Abstract | CrossRef Full Text | Google Scholar
Drinkard B., Roberts M. D., Ranzenhofer L. M., Han J. C., Yanoff L. B., Merke D. P., et al. (2007). Oxygen-uptake efficiency slope as a determinant of fitness in overweight adolescents. Med. Sci. Sports Exerc 39, 1811–1816. doi:10.1249/mss.0b013e31812e52b3
PubMed Abstract | CrossRef Full Text | Google Scholar
Imboden M. T., Harber M. P., Whaley M. H., Finch W. H., Bishop D. L., Kaminsky L. A. (2018). Cardiorespiratory fitness and mortality in healthy men and women. J. Am. Coll. Cardiol. 72, 2283–2292. doi:10.1016/j.jacc.2018.08.2166
PubMed Abstract | CrossRef Full Text | Google Scholar
Lin Y. S., Huang H. Y., Lin W. H., Wei J., Chen J. C., Kuo L. Y., et al. (2016). Oxygen uptake efficiency slope predicts major cardiac events in patients with end-stage heart failure. Transpl. Proc. 48, 956–958. doi:10.1016/j.transproceed.2015.10.076
CrossRef Full Text | Google Scholar
Raghuveer G., Hartz J., Lubans D. R., Takken T., Wiltz J. L., Mietus-Snyder M., et al. (2020). Cardiorespiratory fitness in youth: an important marker of health: a scientific statement from the American heart association. A Sci. Statement Am. Heart Assoc. Circulation 142 (7), e101–e118. doi:10.1161/CIR.0000000000000866
PubMed Abstract | CrossRef Full Text | Google Scholar
Sheridan S., Mccarren A., Gray C., Murphy R. P., Harrison M., Wong S. H. S., et al. (2021). Maximal oxygen consumption and oxygen uptake efficiency in adolescent males. J. Exerc Sci. Fit. 19, 75–80. doi:10.1016/j.jesf.2020.11.001
PubMed Abstract | CrossRef Full Text | Google Scholar
Tang Y., Luo Q., Liu Z., Ma X., Zhao Z., Huang Z., et al. (2017). Oxygen uptake efficiency slope predicts poor outcome in patients with idiopathic pulmonary arterial hypertension. J. Am. Heart Assoc. 6, e005037. doi:10.1161/JAHA.116.005037
PubMed Abstract | CrossRef Full Text | Google Scholar
Taylor H. L., Buskirk E., Henschel A. (1955). Maximal oxygen intake as an objective measure of cardio-respiratory performance. J. Appl. Physiol. 8, 73–80. doi:10.1152/jappl.1955.8.1.73
PubMed Abstract | CrossRef Full Text | Google Scholar
Utter A. C., Robertson R. J., Nieman D. C., Kang J. (2002). Children's OMNI Scale of Perceived Exertion: walking/running evaluation. Med. Sci. Sports Exerc 34, 139–144. doi:10.1097/00005768-200201000-00021
PubMed Abstract | CrossRef Full Text | Google Scholar
 Timothy Edwards
Timothy Edwards Elisabet Børsheim
Elisabet Børsheim Judith L. Weber2,3
Judith L. Weber2,3 Eva C. Diaz
Eva C. Diaz