 Jaron Ras
Jaron Ras Elpidoforos S. Soteriades
Elpidoforos S. Soteriades Denise L. Smith
Denise L. Smith Andre P. Kengne
Andre P. Kengne Lloyd Leach
Lloyd Leach
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 04 July 2023
Sec. Exercise Physiology
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1210107
This article is part of the Research TopicPhysical Activity Behavior, Obesity, and Stress as Crucial Sources of Health Issues in Stressful OccupationsView all 8 articles
Introduction: Firefighters are often placed in situations that require high levels of physical exertion, leading to significant strain on firefighters’ musculoskeletal system, predisposing them to musculoskeletal discomfort (MSD) and/or musculoskeletal injury (MSI). Physical fitness programs are often recommended and justified, in part, to prevent injuries. The aim of this study was to determine the association between physical fitness and musculoskeletal health (MSH) in firefighters.
Methods: A total of 308 full-time firefighters took part in the study conducted in Cape Town, South Africa. Physical fitness tests encompassed a non-exercise estimation for cardiorespiratory fitness, grip and leg strength for upper and lower body strength, push-ups and sit-ups for muscular endurance, and sit-and-reach for flexibility. The Nordic Musculoskeletal Questionnaire and Cornell Musculoskeletal Discomfort Questionnaire were used to determine MSIs and MSD, respectively. A p-value <0.05 indicated statistical significance.
Results: Every one-unit increase in AbVO2max, push-ups, sit-ups, and sit-and-reach decreased the odds of firefighters reporting MSIs by 5% (p = 0.005), 3% (p = 0.017), 3% (p = 0.006), and 3% (p = 0.034), respectively. Every one repetition increase in push-up capacity increased the odds of firefighters reporting neck, elbow and forearm, wrist and hand, and thigh discomfort by 3% (p = 0.039), 4% (p = 0.031), 5% (p = 0.002), and 5%` (p = 0.007), respectively. Every one repetition increase in sit-up capacity increased the odds of firefighters reporting upper back discomfort and thigh discomfort by 5% (p = 0.045) and 7% (p = 0.013), respectively.
Conclusion: Maintenance of physical fitness is likely beneficial in reducing MSIs, which, however, may increase the feeling of MSD in firefighters. In addition, it may be noticed that there is an ideal level of physical fitness that is conducive to the reduction of MSIs and should be studied further.
Firefighting is globally acknowledged to be a dangerous occupation, routinely placing firefighters in hazardous situations that often require high levels of physical exertion, such as fire suppression, victim rescue, and door breaches (Smith et al., 2013; Smith et al., 2019). These workplace stressors place firefighters at high risk for sustaining serious and, sometimes, career-ending injuries (Poston et al., 2011; Orr et al., 2019). In addition, firefighters are regularly exposed to hazardous chemicals and fumes and high temperatures (Frost et al., 2015a; Smith et al., 2019; Nazari et al., 2020a). Due to the hazards of the profession, firefighters are required to wear heavy and insulated personal protective equipment (PPE) that places additional strain on an already burdened musculoskeletal system (Smith et al., 2013; Smith et al., 2016). As a consequence of the physically exhaustive nature of the profession, which often challenges their abilities to perform their work safely, fire departments have recommended firefighters to engage in regular and structured physical activity to manage these various stressors and workplace hazards (Poplin et al., 2013; Poplin et al., 2016; Nowak et al., 2018).
Frost et al. (2015a) reported that injuries occurring at the fire station (37.9%), during physical training (26.6%), during fire emergencies (14.7%), and non-fire emergencies (12.1%) were the most frequent ones. In addition, injuries and injury-related absenteeism are costly to fire departments and municipalities (Poston et al., 2011). Furthermore, a study reported that only 1%–5% of duty time was spent in fire suppression activities (Kales et al., 2007). However, injuries of higher severity occurred more frequently on the fireground (Poplin et al., 2012). Moreover, higher total number of hours worked by firefighters showed a higher incidence rate of injuries (Poplin et al., 2012). To perform their duties aptly, firefighters are required to maintain all aspects of physical fitness (Williford et al., 1999; Rhea et al., 2004; Michaelides et al., 2008; Chizewski et al., 2021), often through occupational specific exercise interventions (Andrews et al., 2019; Chizewski et al., 2021). Previous studies have indicated that a linear relationship existed between physical fitness and work performance (Williford et al., 1999; Rhea et al., 2004; Chizewski et al., 2021). Injury incidence has been related to increasing age and more years of experience as firefighters (Hong et al., 2012; Frost et al., 2016; Yoon et al., 2016). Studies have shown that firefighters tend to become less active as they age and, along with the attrition of the musculoskeletal system, which is associated with both an increase in age and years of experience, as a product of their work, are significantly predisposed to injuries (Hong et al., 2012; Frost et al., 2015a; Yu et al., 2015). Injuries, particularly moderate-to-severe injuries, result in substantial loss of time from work and, due to medical expenses, become costly to fire departments (Poston et al., 2011; Frost et al., 2016). To reduce the incidence of injuries, it is suggested that firefighters remain physically active in their leisure time or when off-duty (Poplin et al., 2013; Frost et al., 2015a; Nowak et al., 2018), and many fire departments schedule prescribed exercise programs when firefighters are on duty (Vaulerin et al., 2016), though studies have shown that higher overload in workload may predispose firefighters to injury (Vaulerin et al., 2016; Ras and Leach, 2022). This suggests that monitoring the overall weekly workload may be beneficial for firefighters, given the physical nature of their occupation (Poplin et al., 2013; Yu et al., 2015).
Physical fitness has been related to lower the incidence of musculoskeletal injuries (MSIs) in firefighters (Poplin et al., 2013; Poplin et al., 2016). Systematic reviews support the aforementioned finding, where it has been reported that cardiorespiratory fitness, muscle strength, muscular endurance, and flexibility were significantly related to reduction in injuries (de la Motte et al., 2017; Lisman et al., 2017; de la Motte et al., 2019). On the other hand, high weekly duty workloads may be related to insufficient time for recovery among firefighters (Vaulerin et al., 2016; Ras et al., 2022a; Ras and Leach, 2022). Monitoring of overall workload may allow fire departments to adjust the level of total physical activity firefighters are engaged in, either occupational activity or recreational activity, adjusting the workload to allow for more time for rest and recovery, thus reducing the likelihood of overload-related musculoskeletal discomfort (MSD) and/or MSIs (Yu et al., 2015; Bustos et al., 2022; Giuliani-Dewig et al., 2022). It is plausible that higher physical fitness would relate to lower feelings of MSD and pain in firefighters (Azmi and Masuri, 2019; Kodom-Wiredu, 2019; Nazari et al., 2020a). However, it is also possible that higher levels of physical fitness may cause firefighters to exert themselves more vigorously during emergency operations, thereby triggering workload-related feeling of MSD and chronic pain, and this may be exacerbated by repetitive movements (Rintala et al., 2015). Higher physical fitness has been shown to be related to improved occupational performance in firefighters, and it is logical to assume that increased levels of physical activity and physical fitness would also provide an additional benefit of better musculoskeletal health (MSH) (Ras et al., 2022a; Ras et al., 2022b).
It has been reported that firefighters in South Africa have high workloads while on duty, while many firefighters are physically inactive during their leisure time (Ras and Leach, 2022). However, there are firefighters in South Africa who are remarkably physically active both on-duty and off-duty (Ras et al., 2022c; Ras and Leach, 2022), which could place this population at an increased risk of reporting MSD or sustaining MSIs while on duty. It is plausible that firefighters who engage in high levels of duty-related physical activity, but are insufficiently active in their leisure time, (Frost et al., 2015a; Poplin et al., 2016) and those who engage in high levels of both duty-related physical activity and leisure time physical activity could be equally predisposed to MSIs (Vaulerin et al., 2016; Ras and Leach, 2022), possibly due to the mismatch between physical fitness and job tasks, and also due to overload of the musculoskeletal system. There has been insufficient research on the association between physical fitness and MSH in firefighters, particularly in South Africa. The South African Fire and Rescue Services policy on physical fitness is devoid of established guidelines requiring firefighters to remain physically active or maintain a fitness standard, perhaps, in part, due to the lack of research on this population. Therefore, the aim of this study was to determine the association between physical fitness and MSH (MSIs and MSD) in firefighters in the City of Cape Town Fire and Rescue Service (CoCTFRS).
This cross-sectional study recruited 308 firefighters from the CoCTFRS between June and August 2022. Physical testing was used to acquire information on physical fitness (cardiorespiratory fitness, muscular strength and endurance, flexibility, and body composition), and a researcher-generated questionnaire, which included two validated questionnaires, was used to acquire information on MSH (MSIs and MSD). All volunteers for this study provided written informed consent before inclusion. Due to injury or inability to perform the physical fitness tests, the total number of firefighters who completed the physical fitness assessment was reduced to 304 for the grip strength, leg strength, push-up, sit-up, and sit-and-reach tests. The study was approved by the University of the Western Cape Biomedical Research Ethics Committee (BM21/10/9) and authorized by the Chief Fire Officer and the Department of Policy and Strategy. A detailed description of the methods used is available in Ras et al. (2022c).
Data collection took place at a standardized fire station in the metropolitan area of the City of Cape Town during the CoCTFRS’s yearly physical fitness evaluation. Every third firefighter from the 96 platoons (32 fire stations) was selected to participate. Each of the 96 firefighting platoons was made up of eight–twelve firefighters. All full-time firefighters between the ages of 20 and 65 who were on active duty during the time of testing were considered. Firefighters who were on administrative duty or sick leave, firefighters who were removed from active duty due to injury, and those who worked part-time or seasonally were disqualified from participating in the study.
Physical fitness was measured in accordance with the American College of Sports Medicine (ACSM) guidelines (Liguori et al., 2021). Cardiorespiratory capacity was calculated using a validated non-exercise calculation (Rexhepi and Brestovci, 2014; Ras et al., 2022c) to estimate oxygen consumption (VO2). The push-up and sit-up tests were used to assess muscular endurance; handgrip and leg strength tests were used to assess upper and lower body muscle strength, respectively; and the sit-and-reach (YMCA sit-and-reach protocol (Liguori et al., 2021)) test was used to assess flexibility. Body mass and lean body mass (LBM) were used as a measure for body composition and assessed using a Tanita© (Tanita©, Tokyo, Japan) BC-1000 Plus bioelectrical impedance (BIA) analyzer. Briefly, for the push-up and sit-up tests, firefighters were required to perform as many push-ups and sit-ups within a minute until volitional fatigue or failure (Liguori et al., 2021). Grip strength was measured using a Takei® 5401-C handgrip dynamometer and leg strength using a Takei® back and leg strength dynamometer, following standardized protocols and with three attempts, with the highest value being recorded (Liguori et al., 2021). The sit-and-reach test required firefighters to reach as forward as far as possible on the ruler of a standardized sit-and-reach box. Cardiorespiratory fitness was estimated using the non-exercise method, using the following formula: oxygen consumption (VO2max) = 3.542 + (−0.014 × Age) + [0.015 × Body Mass (kg)] + (−0.011 × Resting Heart Rate) (Rexhepi and Brestovci, 2014). Relative VO2max (relVO2max) was then calculated from the generated absolute VO2max value. The estimated VO2max formula was reported to be a moderately correlated predictor of VO2max (r = 0.688, p < 0.001;
MSH encompassed MSIs and MSD. For MSIs, the Nordic Musculoskeletal Questionnaire (Crawford, 2007; Chairani, 2020) was used to acquire information on injuries and their location. The Cornell Musculoskeletal Discomfort Questionnaire (Hedge et al., 1999) was used to assess information on the location of discomfort.
Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ) and using the questionnaire converted to weekly metabolic equivalent (MET) minutes (Bohlmann et al., 2001). Using the IPAQ cut-off values for physical activity levels, firefighters were further classified into highly active, which included firefighters who accumulated ≥3000 MET minutes a week of low-, moderate-, and vigorous-intensity MET minutes a week or ≥1,500 of vigorous-intensity MET minutes, only, a week (Bohlmann et al., 2001). Minimally active firefighters were classified as those who accumulated ≥600 MET minutes of low-, moderate-, and vigorous-intensity MET minutes a week. Insufficiently active firefighters were classified as those with <600 MET minutes a week (Bohlmann et al., 2001). In addition, physical activity was classified into total weekly MET minutes, total low-intensity physical activity minutes, total moderate-intensity physical activity minutes, and total vigorous-intensity physical activity minutes.
The data were analyzed using SPSS® software, version 28 (Chicago, Illinois, United States). The Shapiro–Wilk test was used to determine the distribution of the data, and the assumption of normal distribution was retained for the continuous variables of physical fitness and not normally distributed for measures of physical activity. Continuous variables of physical fitness are summarized as means and standard deviations, and continuous variables of physical activity are summarized as medians and 25th to 75th percentiles. Firefighters were classified into the following groups: those with 10-year age intervals, those with MSIs or those uninjured and injury location, and those with or without discomfort and location of discomfort. Group comparisons were based on independent t-tests and analysis of variance (ANOVA) for physical fitness parameters, and the Mann–Whitney U test for physical activity parameters. For the ANOVA analysis, Bonferroni correction was applied. Pearson’s correlation analysis was performed to determine the correlation between physical fitness and age, sex [point-biserial correlation (0 = males and 1 = females)], body mass index (BMI), and weekly MET minutes. Point-biserial correlations were also performed for dichotomous measures of MSH and continuous variables of age, BMI, and weekly MET minutes. In addition, chi-squared test was used to compare MSIs and MSD according to age groups. Univariable and multivariable logistic regressions were performed to determine the association between MSH parameters, which were treated as the outcome/dependent variable, and physical fitness, which designated the exploratory/independent variables. As exploratory variables, physical fitness was used as a continuous measure of physical fitness (abVO2max, relVO2max, grip and leg strength, push-ups, sit-ups, sit-and-reach, and lean body mass). Selection of exploratory variables used as covariates was evidence-based and based on a previous research study that consistently reported an association between MSIs and MSD in firefighters. Collinearity was assessed using the variance inflation factor (VIF) between the exploratory variables used in the adjusted models and deemed acceptable with a VIF of <5. In addition, to ensure autocorrelation was not present between independent variables, a correlation coefficient of <0.8 was used. Due to collinearity between age and years of experience, two separate multivariable models were used. Attributes adjusted for in model 2 included age, sex, BMI, and weekly MET minutes, and in model 3, years of experience was favored over age. A p-value of <0.05 was used to indicate statistical significance.
Table 1 presents the physical fitness measures according to sex and age groups in firefighters. Weight (p < 0.001), BMI (p < 0.001), and weekly MET (p < 0.05) minutes were significantly different between age groups. All physical fitness measures were significantly different between the age groups, particularly abVO2max, relVO2max, sit-ups, push-ups, and sit-and-reach scores (p < 0.001). After Bonferroni correction, abVO2max, relVO2max, grip strength, leg strength sit-ups, push-ups, sit-and-reach, and LBM remained robust to adjustment. According to sex, male firefighters were taller, heavier, and stronger and had a higher abVO2max and LBM. Female firefighters had a higher relVO2max and were more flexible. Age was negatively correlated with abVO2max, relVO2max, leg strength, push-ups, sit-ups, sit-and-reach, and LBM (all p < 0.01). AbVO2max, grip strength, leg strength, and LBM were lower in female firefighters (all p < 0.01). BMI was negatively correlated with abVO2max, relVO2max, push-ups, sit-ups, and sit-and-reach and positively correlated with LBM (all p < 0.01). Weekly MET minutes were positively correlated to abVO2max, leg strength, and sit-and-reach (all p < 0.05). Most MSIs were reported in firefighters aged between 30 and 49 (p = 0.008), which was predominantly upper limb injuries (p = 0.010).
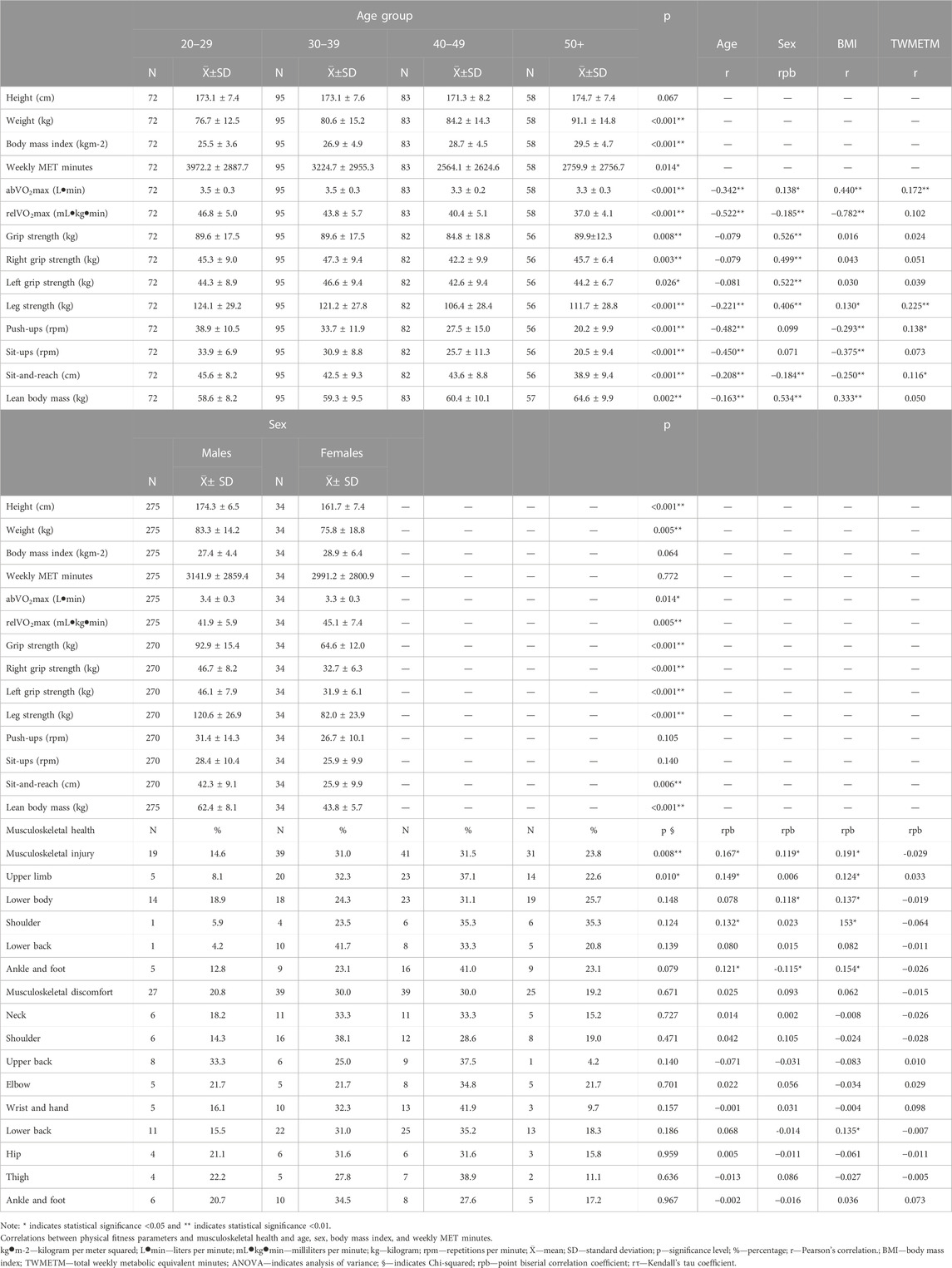
TABLE 1. Physical fitness parameters, musculoskeletal disorders, and musculoskeletal injuries according to age groups in firefighters.
Table 2 describes the MSH of firefighters according to demographic characteristics and physical activity classification in firefighters. Firefighters who were heavier (p = 0.006), older (p = 0.002), longer in service (p < 0.001), and with a higher BMI (p = 0.004) were more likely to report MSIs. Female firefighters were more likely to be injured (p = 0.038) than firefighters who were moderately active (p = 0.016).
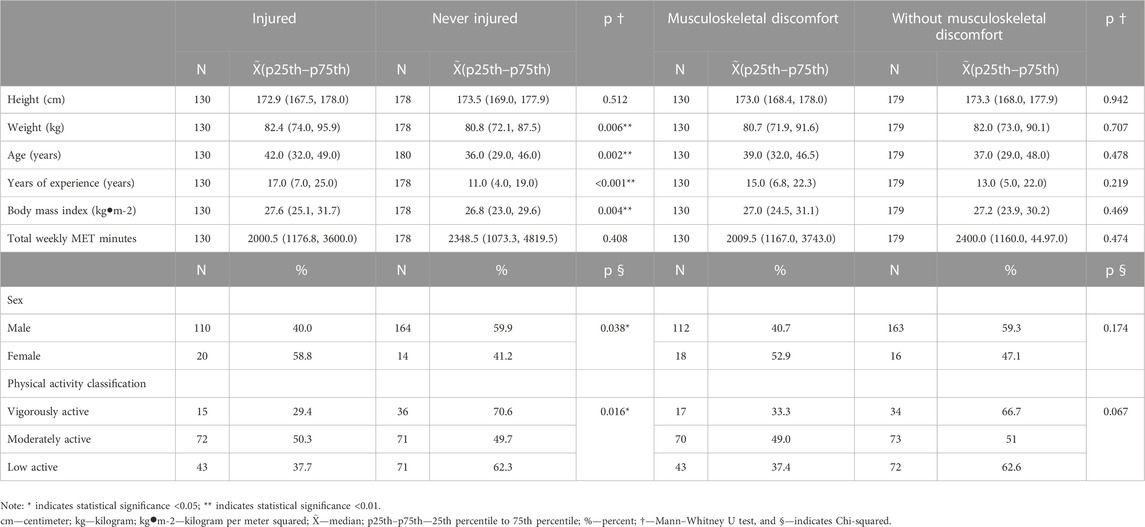
TABLE 2. Musculoskeletal injuries and musculoskeletal discomfort according to demographic characteristics in firefighters.
Table 3 presents the physical activity levels of firefighters according to age, years of experience, BMI, and weekly MET minutes and the physical activity level according to MSIs and MSD. Age (p = 0.049) and weekly MET minutes (p < 0.001) were significantly different between activity levels in firefighters. Firefighters who reported MSIs participated in less vigorous-intensity physical activity than those who never reported an injury (p = 0.004). Firefighters who reported more upper-body injures participated in less low-intensity physical activity (p = 0.044). Firefighters who experienced increased lower back discomfort participated in more low-intensity weekly physical activity (p = 0.002).
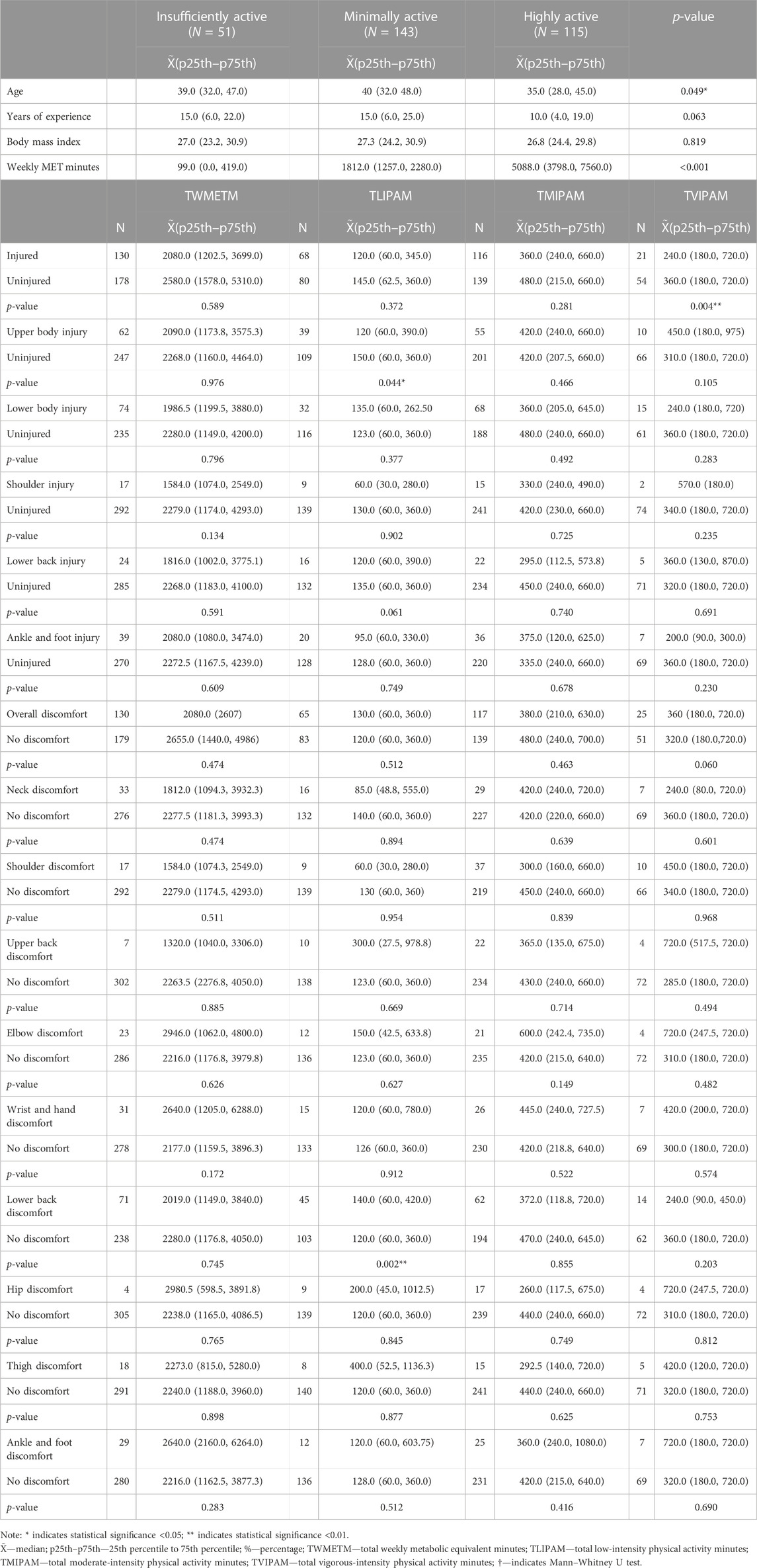
TABLE 3. Physical activity levels of firefighters according to age, years of experience, body mass index, weekly MET minutes, musculoskeletal discomfort, and musculoskeletal injury in firefighters.
Table 4 describes the MSI information according to physical fitness in firefighters. RelVO2max (p = 0.002), push-up (p = 0.008) and sit-up (p = 0.005) capacity, and sit-and-reach (p = 0.015) were significantly different between firefighters who experienced an MSI. Grip strength was significantly different according to the location of injury (p = 0.044). RelVO2max (p = 0.002), push-ups (p = 0.009), and sit-ups (p = 0.011) were significantly lower in firefighters who reported sustaining a shoulder injury. Grip strength (p = 0.021), sit-ups (p = 0.022), and sit-and-reach (p = 0.049) were significantly lower in firefighters who sustained ankle and foot injuries.

TABLE 4. Physical fitness parameters based on musculoskeletal injuries in firefighters.
Table 5 shows MSD and physical fitness parameters at various sites in firefighters. Higher levels of cardiorespiratory fitness, muscular endurance, and strength were related to firefighters reporting MSD. AbVO2max was significantly different between those experiencing MSD and those without MSD (p = 0.038). A higher push-up capacity was related to neck discomfort (p = 0.019), shoulder discomfort (p = 0.047), upper back discomfort (p = 0.036), elbow and forearm discomfort (p = 0.015), wrist and hand discomfort (p < 0.001), hip discomfort (p = 0.043), thigh discomfort (p = 0.003), and ankle and foot discomfort (p = 0.039). Higher sit-up capacity was related to neck discomfort (p = 0.045), elbow and forearm discomfort (p = 0.022), wrist and hand discomfort (p = 0.027), and thigh discomfort (p = 0.006). Higher sit-and-reach score was related to lower neck discomfort (p = 0.029), elbow discomfort (p = 0.044), and thigh discomfort (p = 0.028).
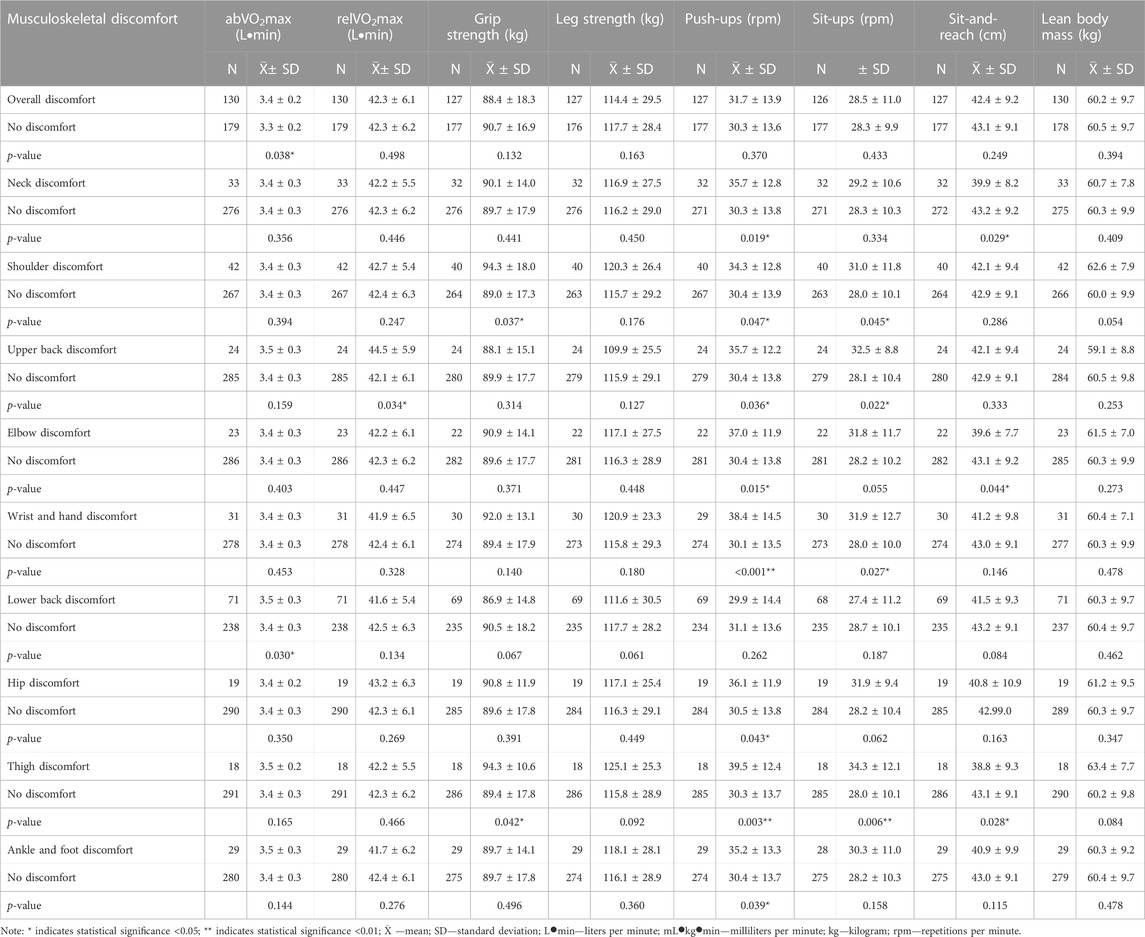
TABLE 5. Physical fitness parameters based on the report of musculoskeletal discomfort at various sites.
Table 6 presents the association between physical fitness and MSIs in firefighters. Univariate analysis indicated that a higher abVO2max (p = 0.005), push-up (p = 0.017) and sit-up capacity (p = 0.006), and sit-and-reach (p = 0.034) were negatively associated with firefighters reporting MSIs. RelVO2max (p = 0.007) and sit-up capacity (p = 0.032) were negatively associated with firefighters reporting upper body MSIs. An increase in grip strength (p = 0.048) and sit-and-reach (p = 0.041) was negatively associated with firefighters reporting lower body MSIs. None of the variables was associated with MSIs after adjustment for covariates. An increase in relVO2max (p = 0.003), push-ups (p = 0.011), and sit-ups (p = 0.013) was negatively associated with firefighters reporting a shoulder injury. Push-ups were significantly and negatively associated with lower back injuries (p = 0.039). An increase in grip strength (p = 0.022), sit-ups (p = 0.024), and sit-and-reach (p = 0.048) was negatively associated with firefighters reporting ankle and foot injuries. After adjustment for covariates, none of the exploratory variables remained significant.
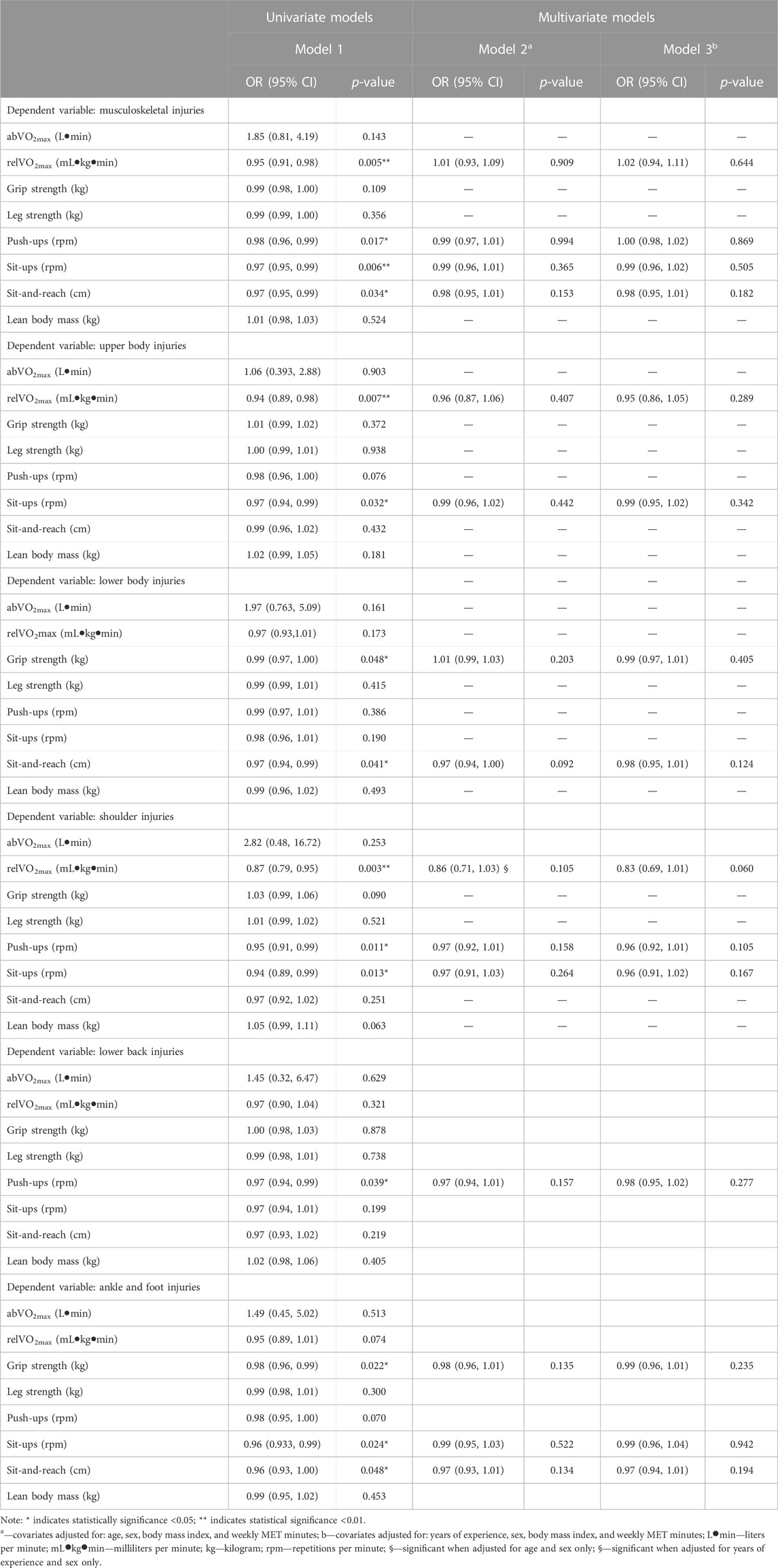
TABLE 6. Association between physical fitness and musculoskeletal injuries in firefighters.
Table 7 presents the association between physical fitness and MSD in firefighters. A higher push-up capacity was positively associated with neck discomfort (p = 0.038), elbow and forearm discomfort (p = 0.031), wrist and hand discomfort (p = 0.002), and thigh discomfort (p = 0.007). A higher sit-up capacity was positively associated with upper back discomfort (p = 0.045) and thigh discomfort (p = 0.013). In model 2, after adjustments for age, sex, BMI, and weekly MET minutes, a one-unit increase in push-up capacity increased the odds of neck discomfort, elbow discomfort, wrist and hand discomfort, and thigh discomfort by 5%, 5%, 6%, and 6%, respectively, and that in sit-up capacity increased the odds of MSD by 9%. In model 3, after adjustments for years of experience, sex, BMI, and weekly MET minutes, a one-unit increase in push-up capacity increased the odds of neck discomfort, elbow discomfort, ankle discomfort, and foot discomfort by 4%, 5%, 6%, and 7%, respectively. A one-unit increase in sit-up capacity increased the odds of reporting thigh discomfort by 8%.
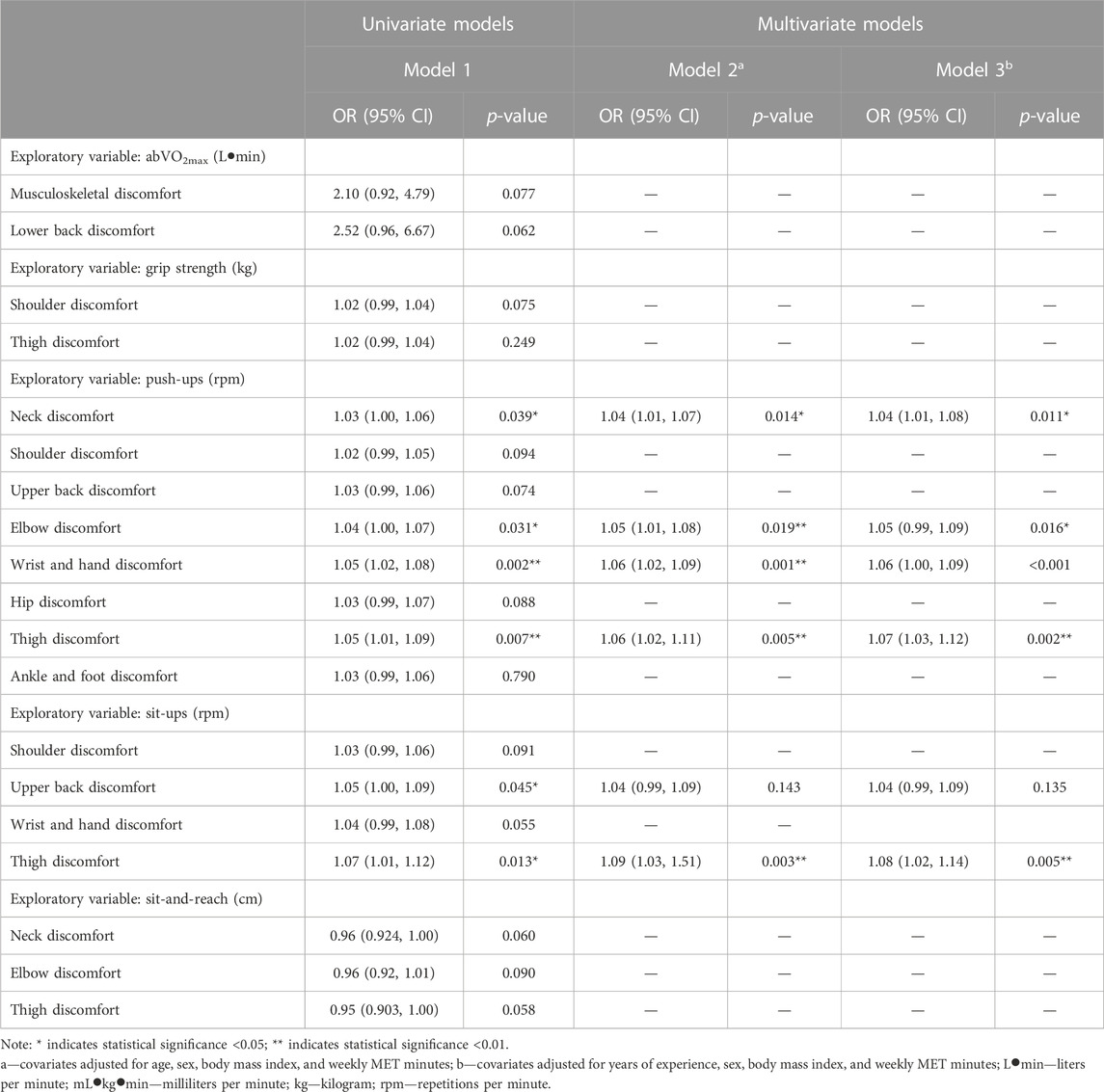
TABLE 7. Association between physical fitness and musculoskeletal discomfort in firefighters.
In this study, we found that firefighters with a higher level of physical fitness reported fewer musculoskeletal injuries. However, higher levels of physical fitness were also associated with increased odds of MSD. Several studies have found that a higher level of physical fitness may reduce the likelihood of MSIs, which is similar to the results of the present study, likely due to the increase in bone mineral density, connective tissue health, muscle mass, and improved balance and coordination (Hong et al., 2012; Poplin et al., 2013; Poplin et al., 2016). The improvements in bone and soft tissue health, as a result of physical activity and increased physical fitness, may increase the volume of physical workload needed to cause a progressive decrease in MSH, which would lead to sudden MSIs on duty. In the current study, fitter firefighters may have reported higher levels of MSD due to overload in workload and insufficient/inadequate recovery or rest following the workload. This hypothesis is supported by the results showing physical activity levels were higher in firefighters who reported MSD, particularly those who were vigorously active. It is also possible that some firefighters experienced MSD due to a high level of physical activity in their leisure time, especially when off-duty, and high levels of occupational activity when on-duty. This persistent overload may predispose firefighters to pain and inflammation, possibly leading to MSD, and possibly, MSIs in firefighters (Vaulerin et al., 2016; Ras and Leach, 2022).
We found that an increase in relVO2max, push-ups, sit-ups, and sit-and-reach decreased the odds of firefighters reporting MSIs. Nowak et al. (2018) reported that firefighters who previously experienced an MSI had a lower push-up and sit-up capacity and lower cardiorespiratory capacity than those without an MSI. In addition, measures of explosive power were also higher in firefighters without injuries than in those who had previous injuries (Nowak et al., 2018). Similarly, Poplin et al. (2013) reported that higher cardiorespiratory capacity was associated with lower incidence of injuries in firefighters. Another study by Poplin et al. (2016) reported that lower levels of physical fitness increased the odds of firefighters sustaining an injury over a 5-year period. Two systematic reviews conducted by de la Motte et al. (2017); Lisman et al. (2017) support the results of the current study, reporting that higher cardiorespiratory fitness and muscular endurance were associated with lower incidences of MSIs. Injury-related absenteeism and the medical expenses associated with it are costly to fire departments, with most of these injuries being related to sprains and strains (Poston et al., 2011; Frost et al., 2016). Physical activity is essential in the strengthening and thickening of connective tissues, an increase in bone mineral density, and improvements in muscle endurance and strength (de la Motte et al., 2017; Lisman et al., 2017), which is likely in firefighters with higher physical fitness levels, reducing the overall reported MSIs seen in the current study. Moreover, studies have suggested that a substantial source of MSIs in firefighters is related to overexertion while engaged in fire suppression and other emergency situations (Frost et al., 2015a; Nowak et al., 2018; Le et al., 2020). Higher levels of physical fitness, particularly muscular strength and endurance, may increase the level of physical exertion needed to induce muscular and cardiorespiratory fatigue that leads to overexertion, thereby providing a protective effect on the musculoskeletal and cardiovascular systems (Henderson et al., 2007; Yu et al., 2015; Nowak et al., 2018; Le et al., 2020). Firefighters who have a higher level of physical fitness perform their duties with more efficiency and rigor. Thus, physical fitness and physicality are integral for firefighters’ occupational performance (Williford et al., 1999; Rhea et al., 2004; Chizewski et al., 2021) and injury prevention (Poplin et al., 2012; Poplin et al., 2013; Vaulerin et al., 2016; Nowak et al., 2018). To ensure the highest occupational efficiency, firefighters should maintain all measures of physical fitness through regular physical activity (Durand et al., 2011; Yu et al., 2015; Nowak et al., 2018). In addition, it is well-documented that cardiorespiratory fitness, muscular strength, and endurance decline as firefighters age, due, in part, to a lack of leisure time physical activity and the natural decline in MSH as a product of the aging process (Baur et al., 2012; Punakallio et al., 2012; Walker et al., 2014; Perroni et al., 2015; Frontera, 2017). This predisposes the firefighters to MSIs, especially, if they lack the necessary levels of physical fitness needed for firefighting. Adequate levels of cardiorespiratory fitness, muscle strength, endurance, and muscular function are important for injury prevention and job performance in firefighters (Smith, 2011; Poplin et al., 2013; Nowak et al., 2018). Furthermore, physical activity has been shown to promote the release of myokines from muscle tissue (Hamrick, 2011; Lee and Jun, 2019). Myokines play an important role in stress response and coordinating both positive and negative musculoskeletal changes to exercise and/or work (Hamrick, 2011; Lee and Jun, 2019). This may, further, support that more physically active and, subsequently, more physically fit firefighters are less likely to sustain MSIs.
The present study showed that higher relVO2max and sit-up capacity were associated with lower odds of firefighters reporting upper limb injuries. In addition, an increase in relVO2max, push-up and sit-up capacity was associated with lower odds of firefighters reporting shoulder injuries and an increase in push-up capacity reduced the odds of firefighting reporting lower back injuries. Previous studies noted that people involved in occupations that require repetitive upper body motions are particularly susceptible to an increase in upper limb injuries (Ranney et al., 1995; Latko et al., 1999). An increase in physical fitness, particularly upper body muscular endurance capacity, may increase the workload needed to lead to overexertion-related shoulder injuries (de la Motte et al., 2017), especially as many firefighting-related duties encompass repetitive upper body movements (Frost et al., 2015a; Nowak et al., 2018). Cady et al. (1979) reported that higher physical fitness, which encompassed a prediction model that included cardiorespiratory endurance, flexibility, muscular strength, and diastolic blood pressure, was associated with lower back injuries in firefighters. Previous studies noted that exercise increases muscular strength and endurance, which could, potentially, reduce the likelihood of lower back injuries in firefighters (Taylor et al., 2014; Mayer et al., 2015; Moon et al., 2015). Similarly, Peate et al. (2007) reported that after an exercise intervention, improvements in abdominal strength and flexibility reduced the incidence of injuries in firefighters. Although not directly related, higher levels of muscular endurance may positively assist firefighters in reducing the incidence of injuries to their upper limbs and trunk, likely due to these areas having an increased stability and higher capacity to tolerate forceful repetitive movements (Cady et al., 1979; Beaton et al., 2002; Peate et al., 2007; de la Motte et al., 2017). The results of the current study indicated that for every 1 kg increase in grip strength and 1 cm increase in sit-and-reach score, there were lower odds of firefighters reporting lower limb injuries by 1% and 3%, respectively. A study reported that a higher sit-and-reach test score was associated with lower incidences of of MSIs (Lisman et al., 2017) and is likely related to a greater range of motion and a lower likelihood of stretching connective tissues to an uncomfortable degree. Similarly, Frost et al. (2015b) reported that push-up, deep squat, and sit-and-reach tasks in the functional movement screening significantly predicted injury status in firefighters. This was supported by Butler et al. (2013) who reported that the sit-and-reach score was a significant predictor of injury status in firefighters.
In the present study, with the introduction of age, sex, years of experience, BMI, and physical activity levels in the multivariate models, the significant associations were removed from all significant outcomes for MSIs. This suggests that although higher levels of physical fitness are necessary to protect firefighters from sustaining injuries, there are additional components that form part of a larger system of factors that also contribute to MSI prevention, which is supported by previous research (Nabeel et al., 2007; Vaulerin et al., 2016; Nowak et al., 2018; Ras and Leach, 2022). Firefighters remaining physically active to meet a minimum level of health-related physical fitness may be a prerequisite in reducing MSIs, but beyond this level may lead to chronic pain and injury (Poplin et al., 2016; Vaulerin et al., 2016; Lentz et al., 2019; Ras and Leach, 2022). This was seen in the present data, where firefighters who were more vigorously active reported less MSIs. However, similarly, firefighters who experienced MSD tended toward being more physically active, particularly vigorously active, as well. Although there were instances where this tended toward significance, statistical significance was not seen, perhaps due to the relatively small numbers of firefighters experiencing MSD. Previous studies have reported that older firefighters, with more years of experience, and who were heavier and more physically inactive, were particularly susceptible to sustaining MSIs while on duty (Poston et al., 2011; Jahnke et al., 2013; Phelps et al., 2018; Nazari et al., 2020b; Hollerbach et al., 2020). Moreover, studies found women were especially susceptible to MSIs, due to multiple factors, such as poor fitting equipment, lower muscle mass, particularly in the upper limbs, and lower bone mineral density (Sinden et al., 2013; McQuerry et al., 2019; Song et al., 2019). After adjusting for age, sex, and BMI in the multivariate analysis, we noted that our results no longer achieved significance. This was also noted in correlations where age, sex, and BMI were positively correlated to MSIs in firefighters. In addition, it is likely that due to working as a firefighter for longer periods, regardless of their fitness levels, these firefighters were more likely to sustain an injury during their career (Poston et al., 2011; Hong et al., 2012; Frost et al., 2015a).
We found that push-up capacity was significantly associated with increased odds of firefighters reporting discomfort in the neck, elbow and forearm, wrist and hand, and thigh regions. In addition, an increase in sit-up capacity was associated with an increase in the odds of firefighters reporting upper back and thigh discomfort. Rintala et al. (2015) reported that fitter pilots flew their aircrafts at speeds that induce higher acceleration speeds and physical workloads and, due to this higher workload, reported more symptoms of musculoskeletal pain, but fewer musculoskeletal disabilities. This may also relate to the firefighting profession, where fitter firefighters may perform their duties with greater rigor, power, and force (Williford et al., 1999; Chizewski et al., 2021), which may overload the firefighter’s musculoskeletal system. These fitter firefighters might be engaged in more vigorous-intensity work at fire or emergency scenarios, compared to their less fit counterparts, which leads to MSD. In addition, if firefighters participate in regular vigorous-intensity leisure-time physical activity, this may exacerbate an already strained musculoskeletal system, or overload the musculoskeletal system, leading to burnout, that increases the risk of MSIs (Vaulerin et al., 2016; Ras and Leach, 2022). This might cause additional MSD in firefighters, but have a positive effect on reducing MSIs, as seen in the current results. However, managing the overall workload may be key to maintaining MSH and reducing injury incidence in firefighters. Previous research has noted that monitoring overall workload is important for firefighters (Poplin et al., 2013; Vaulerin et al., 2016; de la Motte et al., 2017; Ras and Leach, 2022). This could provide a possible explanation to why fitter firefighters were more likely to report MSD, especially if the MSD caused by high workloads could, eventually, lead to overuse injury (Vaulerin et al., 2016). Lusa et al. (2015) reported that firefighters who reported sleep disturbances had chronic low back pain symptoms (Halson, 2008). Abbasi et al. (2018) reported that firefighters who were heavily physically active had poorer sleep quality and were more likely to report MSDs. Due to sleep being integral to recovery, this may provide an explanation as to why fitter firefighters experienced more MSD in the current results. In contrast to the current results, Nabeel et al. (2007) reported that higher levels of physical fitness were associated with a significant decrease in the incidence of chronic pain in police officers. Similarly, Beaton et al. (2002) reported that neck, back, and shoulder pain was significantly lower in firefighters who participated in more frequent aerobic exercise. It may be that MSD is an indication of excessive workload or insufficient recovery, which has been supported in other populations, such as nurses, paramedics, surgeons, and welders (Menzel et al., 2004; Tam and Yeung, 2006; Szeto et al., 2009; Shahriyari et al., 2020). However, this area is understudied in firefighters, and the findings are not particularly intuitive. Investigating MSD may provide valuable insight into MSH of firefighters and how this may eventually lead, or predispose, firefighters to injury. It is recommended that more research be conducted in this area to better understand the causal mechanisms between physical fitness and MSD, and the implications of MSD for the likelihood of sustaining an injury.
This was the first study examining the relationship between physical fitness and MSH in CoCTFRS firefighters, a demographic that has received little attention with respect to scientific research. The study used validated instruments and trained researchers who objectively assessed the markers of physical fitness, except cardiorespiratory fitness (Ras et al., 2022c). Validated questionnaires were used to assess MSH. This work contributes unique information to a field of study that has not yet received adequate attention, particularly in a South African setting. The present study, however, has some limitations. The study’s cross-sectional design prevents the inference of causal associations. The study estimated relative and absolute cardiorespiratory fitness using a non-exercise calculation. The under-representation of female firefighters limits the generalizability of results to female firefighters. Although the study had a relatively large sample size, the low number of firefighters with MSD and MSIs limits the power of the statistical analysis.
The findings of the present study emphasize the need for firefighters maintaining high levels of physical fitness to lessen the risk of MSIs, particularly cardiorespiratory fitness, muscular endurance, and flexibility. In addition, our finding of a positive association between physical fitness and MSD indicates that care must be taken to implement well-structured fitness programs that take into account the need for adequate rest and recovery. This research highlights the importance of maintaining and/or improving physical fitness on MSH in firefighters, in the CoCTFRS, thus emphasizing the need for policy change. It is recommended that occupational health and safety professionals, as well as policymakers, ensure that firefighters participate in regular physical activity that is monitored for total weekly workload to reduce the likelihood of overexertion and ensure adequate recovery, and maintain an ideal level of health-related physical fitness to aid their occupational wellbeing. Furthermore, the development of workload guidelines is needed to further support the physical fitness requirements of firefighting and reduce the likelihood of MSIs and discomfort in firefighters. In future research, longitudinal studies are warranted to evaluate a potential causal relationship between physical fitness and improvements or decrements on the incidence of MSIs and, especially, MSD as this area is understudied with respect to firefighters. Although female firefighters represent a relatively small proportion of firefighters in the CoCTFRS, a larger and more representative sample of female firefighters should be included in future studies to allow for the generalizability of results to the female firefighter population.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the University of the Western Cape (UWC) Biomedical Research Ethics Committee (BMREC). The patients/participants provided their written informed consent to participate in this study.
JR, DS, ES, AK, and LL contributed to conception and design of the study. JR organized the database, performed the statistical analysis, collected the data, and wrote the first draft of the manuscript. JR, DS, ES, AK, and LL proofread and edited the drafts of the manuscript. All authors contributed to the article and approved the submitted version.
This research was funded by the National Research Foundation (NRF) (grant number 141282) and The Ryoichi Sasakawa Young Leaders Fellowship Fund (SLYFF). Neither funding bodies was involved in the study design, data collection, or interpretation of the data.
The authors thank all firefighters who consented to voluntarily participate in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbasi, M., Rajabi, M., Yazdi, Z., and Shafikhani, A. A. (2018). Factors affecting sleep quality in firefighters. Sleep Hypn. 20 (4), 283–289. doi:10.5350/sleep.hypn.2018.20.0163
Andrews, K. L., Gallagher, S., and Herring, M. P. (2019). The effects of exercise interventions on health and fitness of firefighters: A meta-analysis. Scand. J. Med. Sci. Sports 29 (6), 780–790. doi:10.1111/sms.13411
Azmi, N. L. A. M., and Masuri, M. G. (2019). Work-related musculoskeletal disorder (WMSDs) and functional status of firefighters in Klang Valley. Healthscope: The Official Research Book of Faculty of Health Sciences, UiTM, 2. Retrieved from http://healthscopefsk.com/index.php/research/article/view/74
Baur, D. M., Christophi, C. A., Cook, E. F., and Kales, S. N. (2012). Age-related decline in cardiorespiratory fitness among career firefighters: Modification by physical activity and adiposity. J. Obes. 2012, 710903. doi:10.1155/2012/710903
Beaton, R., Murphy, S., Salazar, M., and Johnson, L. C. (2002). Neck, back, and shoulder pain complaints in urban firefighters: The benefits of aerobic exercise. J. Musculoskelet. Pain 10 (3), 57–67. doi:10.1300/J094v10n03_04
Bohlmann, I. M., Mackinnon, S., Kruger, H., Leach, L., van Heerden, J., Cook, I., et al. (2001). Is the international physical activity questionnaire (IPAQ) valid and reliable in the South African population? Med. Sci. Sports Exerc 33, S119. doi:10.1097/00005768-200105001-00672
Bustos, D., Guedes, J. C., Santos Baptista, J., Vaz, M., Torres Costa, J., and Fernandes, R. J. (2022). “Physiological monitoring systems for firefighters (A short review),” in Occupational and environmental safety and health III [internet]. Editors P. M. Arezes, J. S. Baptista, P. Carneiro, J. Castelo Branco, N. Costa, and J. Duarte (Cham: Springer International Publishing), 293–305. doi:10.1007/978-3-030-89617-1_27
Butler, R. J., Contreras, M., Burton, L. C., Plisky, P. J., Goode, A., County, O., et al. (2013). Modifiable risk factors predict injuries in firefighters during training academies. Work 00, 11–17. doi:10.3233/WOR-121545
Cady, L. D., Bischoff, D. P., O’Connell, E. R., Thomas, P. C., and Allan, J. H. (1979). Strength and fitness and subsequent back injuries in firefighters. J. Occup. Med. 21 (4), 269–272. Avaliable At: http://www.jstor.org/stable/45005468.
Chairani, A. (2020). “Validity and reliability test of the nordic musculoskeletal questionnaire with formal and informal sector workers,” in Childhood stunting, wasting, and obesity, as the critical global health issues: Forging cross-sectoral solutions (Solo, Indonesia: Universitas Sebelas Maret), 100. Available from: http://theicph.com/id_ID/2021/03/11/validity-and-reliability-test-of-the-nordic-musculoskeletal-questionnaire-with-formal-and-informal-sector-workers/u45_aulia-chairani_fp_medicine/.
Chizewski, A., Box, A., Kesler, R., and Petruzzello, S. J. (2021). Fitness fights fires: Exploring the relationship between physical fitness and firefighter ability. Int. J. Environ. Res. Public Health 18 (22), 11733. doi:10.3390/ijerph182211733
Crawford, J. O. (2007). The nordic musculoskeletal questionnaire. Occup. Med. (Chic Ill) 57 (4), 300–301. doi:10.1093/occmed/kqm036
de la Motte, S. J., Gribbin, T. C., Lisman, P., Murphy, K., and Deuster, P. A. (2017). Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 2—muscular endurance and muscular strength. J. Strength & Cond. Res. 31 (11), 3218–3234. doi:10.1519/JSC.0000000000002174
de la Motte, S. J., Lisman, P., Gribbin, T. C., Murphy, K., and Deuster, P. A. (2019). Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 3—flexibility, power, speed, balance, and agility. J. Strength & Cond. Res. 33 (6), 1723–1735. doi:10.1519/JSC.0000000000002382
Durand, G., Tsismenakis, A. J., Jahnke, S. A., Baur, D. M., Christophi, C. A., and Kales, S. N. (2011). Firefighters’ physical activity: Relation to fitness and cardiovascular disease risk. Med. Sci. Sports Exerc 43 (9), 1752–1759. doi:10.1249/MSS.0b013e318215cf25
Frontera, W. R. (2017). Physiologic changes of the musculoskeletal system with aging: A brief review. Phys. Med. Rehabil. Clin. N. Am. [Internet] 28 (4), 705–711. doi:10.1016/j.pmr.2017.06.004
Frost, D. M., Beach, T. A. C., Crosby, I., and McGill, S. M. (2015a). Firefighter injuries are not just a fireground problem. Work 52 (4), 835–842. doi:10.3233/wor-152111
Frost, D. M., Beach, T. A. C., Crosby, I., and McGill, S. M. (2016). The cost and distribution of firefighter injuries in a large Canadian Fire Department. Work 55 (3), 497–504. doi:10.3233/WOR-162420
Frost, D. M., Beach, T. A. C., McGill, S. M., and Callaghan, J. P. (2015b). The predictive value of general movement tasks in assessing occupational task performance. Work 52 (1), 11–18. doi:10.3233/WOR-141902
Giuliani-Dewig, H. K., Gerstner, G. R., Mota, J. A., and Ryan, E. D. (2022). Examining the usability of workload monitoring in firefighter recruits. J. Occup. Environ. Med. 64 (10), 865–868. doi:10.1097/JOM.0000000000002592
Halson, S. L. (2008). Nutrition, sleep and recovery. Eur. J. Sport Sci. 8 (2), 119–126. doi:10.1080/17461390801954794
Hamrick, M. W. (2011). A role for myokines in muscle-bone interactions. Exerc Sport Sci. Rev. 39 (1), 43–47. doi:10.1097/JES.0b013e318201f601
Hedge, A., Morimoto, S., and Mccrobie, D. (1999). Effects of keyboard tray geometry on upper body posture and comfort. Ergon. [Internet] 42 (10), 1333–1349. doi:10.1080/001401399184983
Henderson, N. D., Berry, M. W., and Matic, T. (2007). Field measures of strength and fitness predict firefighter performance on physically demanding tasks. Pers. Psychol. 60, 431–473. doi:10.1111/j.1744-6570.2007.00079.x
Hollerbach, B. S., Kaipust, C. M., Poston, W. S. C., Haddock, C. K., Heinrich, K. M., and Jahnke, S. A. (2020). Injury correlates among a national sample of women in the US fire service. J. Occup. Environ. Med. 62 (8), 634–640. doi:10.1097/JOM.0000000000001918
Hong, O., Phelps, S., Feld, J., and Vogel, S. (2012). Occupational injuries, duty status, and factors associated with injuries among firefighters. Workplace Health Saf. 60 (12), 517–523. doi:10.1177/216507991206001203
Jahnke, S. A., Poston, W. S. C., Haddock, C. K., and Jitnarin, N. (2013). Injury among a population based sample of career firefighters in the central USA. Inj. Prev. 19, 393–398. doi:10.1136/injuryprev-2012-040662
Kales, S. N., Soteriades, E. S., Christophi, C. A., and Christiani, D. C. (2007). Emergency duties and deaths from heart disease among firefighters in the United States. N. Engl. J. Med. [Internet] 356 (12), 1207–1215. doi:10.1056/NEJMoa060357
Kodom-Wiredu, J. K. (2019). The relationship between firefighters’ work demand and work-related musculoskeletal disorders: The moderating role of task characteristics. Saf. Health Work 10 (1), 61–66. doi:10.1016/j.shaw.2018.05.004
Latko, W. A., Armstrong, T. J., Franzblau, A., Ulin, S. S., Werner, R. A., and Albers, J. W. (1999). Cross-sectional study of the relationship between repetitive work and the prevalence of upper limb musculoskeletal disorders. Am. J. Ind. Med. [Internet 36 (2), 248–259. doi:10.1002/(sici)1097-0274(199908)36:2<248::aid-ajim4>3.0.co;2-q
Le, A. B., Smith, T. D., McNulty, L. A., Dyal, M. A., and Dejoy, D. M. (2020). Firefighter overexertion: A continuing problem found in an analysis of non-fatal injury among career firefighters. Int. J. Environ. Res. Public Health 17 (21), 1–11. doi:10.3390/ijerph17217906
Lee, J. H., and Jun, H. S. (2019). Role of myokines in regulating skeletal muscle mass and function. Front. Physiol. 10, 42. doi:10.3389/fphys.2019.00042
Lentz, L., Randall, J. R., Gross, D. P., Senthilselvan, A., and Voaklander, D. (2019). The relationship between physical fitness and occupational injury in emergency responders: A systematic review. Am. J. Industrial Med. 62, 3–13. doi:10.1002/ajim.22929
Liguori, G., Medicineof, A. C., and Fountaine, C. J. (2021). ACSM’s Guidelines for Exercise Testing and Prescription; American College of Sports Medicine Series, American College of Sports medicine series (Philadelphia: Wolters Kluwer). Available from: https://books.google.co.za/books?id=6P-azQEACAAJ.
Lisman, P. J., de la Motte, S. J., Gribbin, T. C., Jaffin, D. P., Murphy, K., and Deuster, P. A. (2017). A systematic review of the association between physical fitness and musculoskeletal injury risk: Part 1—cardiorespiratory endurance. J. Strength & Cond. Res. 31 (6), 1744–1757. doi:10.1519/JSC.0000000000001855
Lusa, S., Miranda, H., Luukkonen, R., and Punakallio, A. (2015). Sleep disturbances predict long-term changes in low back pain among Finnish firefighters: 13-year follow-up study. Int. Arch. Occup. Environ. Health 88 (3), 369–379. doi:10.1007/s00420-014-0968-z
Mayer, J. M., Quillen, W. S., Verna, J. L., Chen, R., Lunseth, P., and Dagenais, S. (2015). Impact of a supervised worksite exercise program on back and core muscular endurance in firefighters. Am. J. Health Promot. 29 (3), 165–172. doi:10.4278/ajhp.130228-QUAN-89
McQuerry, M., Kwon, C., and Johnson, H. (2019). A critical review of female firefighter protective clothing and equipment workplace challenges. Res. J. Text. Appar. 23, 94–110. doi:10.1108/rjta-01-2019-0002
Menzel, N. N., Brooks, S. M., Bernard, T. E., and Nelson, A. (2004). The physical workload of nursing personnel: Association with musculoskeletal discomfort. Int. J. Nurs. Stud. 41 (8), 859–867. doi:10.1016/j.ijnurstu.2004.03.012
Michaelides, M. A., Parpa, K. M., Thompson, J., and Brown, B. (2008). Predicting performance on a firefighter's ability test from fitness parameters. Res. Q. Exerc Sport 79 (4), 468–475. doi:10.1080/02701367.2008.10599513
Moon, T. Y., Kim, J. H., Gwon, H. J., Hwan, B. S., Kim, G. Y., Smith, N., et al. (2015). Effects of exercise therapy on muscular strength in firefighters with back pain. J. Phys. Ther. Sci. 27 (3), 581–583. doi:10.1589/jpts.27.581
Nabeel, I., Baker, B. A., McGrail, M. P., and Flottemesch, T. J. (2007). Correlation between physical activity, fitness, and musculoskeletal injuries in police officers. Minn Med. 90 (9), 40–43.
Nazari, G., Macdermid, J. C., Sinden, K., and D’Amico, R. (2020b). Prevalence of musculoskeletal symptoms among Canadian firefighters. Work 67 (1), 185–191. doi:10.3233/WOR-203264
Nazari, G., Osifeso, T. A., and MacDermid, J. C. (2020a). Distribution of number, location of pain and comorbidities, and determinants of work limitations among firefighters. Rehabil. Res. Pract. 2020, 1942513. doi:10.1155/2020/1942513
Nowak, A. M., Molik, B., Wójcik, A., Rutkowska, I., Nowacka-Dobosz, S., Kowalczyk, M., et al. (2018). Physical activity and injuries relating to physical fitness of professional firefighters. Adv. Rehabilitation 32 (2), 13–22. doi:10.5114/areh.2018.77933
Orr, R., Simas, V., Canetti, E., and Schram, B. (2019). A profile of injuries sustained by firefighters: A critical review. Int. J. Environ. Res. Public Health 16 (20), 3931. doi:10.3390/ijerph16203931
Peate, W. F., Bates, G., Lunda, K., Francis, S., and Bellamy, K. (2007). Core strength: A new model for injury prediction and prevention. J. Occup. Med. Toxicol. 2 (1), 3. doi:10.1186/1745-6673-2-3
Perroni, F., Guidetti, L., Cignitti, L., and Baldari, C. (2015). Age-related changes in upper body strength and lower limb power of professional Italian firefighters. Sport Sci. Health 11 (3), 279–285. doi:10.1007/s11332-015-0236-y
Phelps, S. M., Drew-Nord, D. C., Neitzel, R. L., Wallhagen, M. I., Bates, M. N., and Hong, O. S. (2018). Characteristics and predictors of occupational injury among career firefighters. Workplace Health Saf. 66 (6), 291–301. doi:10.1177/2165079917740595
Poplin, G. S., Harris, R. B., Pollack, K. M., Peate, W. F., and Burgess, J. L. (2012). Beyond the fireground: Injuries in the fire service. Inj. Prev. 18 (4), 228–233. doi:10.1136/injuryprev-2011-040149
Poplin, G. S., Roe, D. J., Burgess, J. L., Peate, W. F., and Harris, R. B. (2016). Fire fit: Assessing comprehensive fitness and injury risk in the fire service. Int. Arch. Occup. Environ. Health 89 (2), 251–259. doi:10.1007/s00420-015-1068-4
Poplin, G. S., Roe, D. J., Peate, W., Harris, R. B., and Burgess, J. L. (2013). Original contribution the association of aerobic fitness with injuries in the fire service. Am. J. Epidemiol. 10, 149. doi:10.1093/aje/kwt213
Poston, W. S. C., Jitnarin, N., Haddock, C. K., Jahnke, S. A., and Tuley, B. C. (2011). Obesity and injury-related absenteeism in a population-based firefighter cohort. Obesity 19 (10), 2076–2081. doi:10.1038/oby.2011.147
Punakallio, A., Lindholm, H., Luukkonen, R., and Lusa, S. (2012). Lifestyle factors predicting changes in aerobic capacity of aging firefighters at 3-and 13-year follow-ups. J. Occup. Environ. Med. 54 (9), 1133–1141. doi:10.1097/JOM.0b013e3182554b11
Ranney, D., Wells, R., and Moore, A. (1995). Upper limb musculoskeletal disorders in highly repetitive industries: Precise anatomical physical findings. Ergon. [Internet] 38 (7), 1408–1423. doi:10.1080/00140139508925198
Ras, J., Kengne, A. P., Smith, D., Soteriades, E. S., and Leach, L. (2022b). Effects of cardiovascular health, musculoskeletal health and physical fitness on occupational performance of firefighters: Protocol for a systematic review and meta-analysis. BMJ Open 12 (7), 061435. doi:10.1136/bmjopen-2022-061435
Ras, J., and Leach, L. (2022). Relationship between physical activity, coronary artery disease risk factors and musculoskeletal injuries in the city of Cape Town fire and rescue service. Inq. J. Health Care Organ. Provis. Financing 59, 84485. doi:10.1177/00469580221084485
Ras, J., Smith, D. L., Kengne, A. P., Soteriades, E. E., and Leach, L. (2022a). Cardiovascular disease risk factors, musculoskeletal health, physical fitness, and occupational performance in firefighters: A narrative review. J. Environ. Public Health 2022, 7346408. doi:10.1155/2022/7346408
Ras, J., Smith, D. L., Soteriades, E. S., Kengne, A. P., and Leach, L. (2022c). A pilot study on the relationship between cardiovascular health, musculoskeletal health, physical fitness and occupational performance in firefighters. Eur. J. Investig. Health Psychol. Educ. [Internet] 12 (11), 1703–1718. doi:10.3390/ejihpe12110120
Rexhepi, A. M., and Brestovci, B. (2014). Prediction of VO2max based on age, body mass, and resting heart rate. Hum. Mov. [Internet] 15 (1), 56–59. doi:10.2478/humo-2014-0003
Rhea, M. R., Alvar, B. A., and Gray, R. (2004). Physical fitness and job performance of firefighters. J. Strength Cond. Res. [Internet] 18 (2), 348–352. doi:10.1519/R-12812.1
Rintala, H., Häkkinen, A., Siitonen, S., and Kyröläinen, H. (2015). Relationships between physical fitness, demands of flight duty, and musculoskeletal symptoms among military pilots. Mil. Med. 180 (12), 1233–1238. doi:10.7205/MILMED-D-14-00467
Shahriyari, M., Afshari, D., and Latifi, S. M. (2020). Physical workload and musculoskeletal disorders in back, shoulders and neck among welders. Int. J. Occup. Saf. Ergonomics 26 (4), 639–645. doi:10.1080/10803548.2018.1442401
Sinden, K., MacDermid, J., Buckman, S., Davis, B., Matthews, T., and Viola, C. (2013). A qualitative study on the experiences of female firefighters. Work 45, 97–105. doi:10.3233/WOR-121549
Smith, D. L., Barr, D. A., and Kales, S. N. (2013). Extreme sacrifice: Sudden cardiac death in the US fire service. Extrem Physiol. Med. 2 (1), 6–9. doi:10.1186/2046-7648-2-6
Smith, D. L., DeBlois, J. P., Kales, S. N., and Horn, G. P. (2016). Cardiovascular strain of firefighting and the risk of sudden cardiac events. Exerc Sport Sci. Rev. 44 (3), 90–97. doi:10.1249/JES.0000000000000081
Smith, D. L. (2011). Firefighter fitness: Improving performance and preventing injuries and fatalities. Curr. Sports Med. Rep. 10 (3), 167–172. doi:10.1249/JSR.0b013e31821a9fec
Smith, D. L., Haller, J. M., Korre, M., Sampani, K., Porto, L. G. G., Fehling, P. C., et al. (2019). The relation of emergency duties to cardiac death among US firefighters. Am. J. Cardiol. 123 (5), 736–741. doi:10.1016/j.amjcard.2018.11.049
Song, J. Y., Kim, M. G., and Ahn, Y. S. (2019). Injury-related hospital admission of female firefighters in South Korea. Int. J. Occup. Saf. Ergonomics 25 (4), 575–582. doi:10.1080/10803548.2017.1411666
Sun, Q., Chen, S., Wang, Y., Zhang, J., Lavie, C., and Sui, X. (2022). Cross-validation of non-exercise estimated cardiorespiratory fitness: The NHANES study. J. Surg. Res. Pract. 2022, 1–19. doi:10.46889/jcmr.2022.31009
Szeto, G. P. Y., Ho, P., Ting, A. C. W., Poon, J. T. C., Cheng, S. W. K., and Tsang, R. C. C. (2009). Work-related musculoskeletal symptoms in surgeons. J. Occup. Rehabil. 19 (2), 175–184. doi:10.1007/s10926-009-9176-1
Tam, G. Y. T., and Yeung, S. S. (2006). Perceived effort and low back pain in non-emergency ambulance workers: Implications for rehabilitation. J. Occup. Rehabil. 16 (2), 231–240. doi:10.1007/s10926-006-9019-2
Taylor, P., Beach, T. A. C., Frost, D. M., Mcgill, S. M., and Callaghan, J. P. (2014). Physical fitness improvements and occupational low-back loading – An exercise intervention study with firefighters. Ergonomics 57, 744–763. doi:10.1080/00140139.2014.897374
Vaulerin, J., d’Arripe-Longueville, F., Emile, M., and Colson, S. S. (2016). Physical exercise and burnout facets predict injuries in a population-based sample of French career firefighters. Appl. Ergon. 54, 131–135. doi:10.1016/j.apergo.2015.12.007
Walker, A., Driller, M., Argus, C., Cooke, J., and Rattray, B. (2014). The ageing Australian firefighter: An argument for age-based recruitment and fitness standards for urban fire services. Ergonomics 57, 612–621. doi:10.1080/00140139.2014.887790
Williford, H. N., Duey, W. J., Olson, M. S., Howard, R., and Wang, N. (1999). Relationship between fire fighting suppression tasks and physical fitness. Ergonomics 42 (9), 1179–1186. doi:10.1080/001401399185063
Yoon, J. H., Kim, Y. K., Kim, K. S., and Ahn, Y. S. (2016). Characteristics of workplace injuries among nineteen thousand Korean firefighters. J. Korean Med. Sci. 31 (10), 1546–1552. doi:10.3346/jkms.2016.31.10.1546
Yu, C. C. W., Au, C. T., Lee, F. Y. F., So, R. C. H., Wong, J. P. S., Mak, G. Y. K., et al. (2015). Association between leisure time physical activity, cardiopulmonary fitness, cardiovascular risk factors, and cardiovascular workload at work in firefighters. Saf. Health Work 6 (3), 192–199. doi:10.1016/j.shaw.2015.02.004
Keywords: firefighting, discomfort, injury, workload, physical activity, strength, endurance, cardiorespiratory
Citation: Ras J, Soteriades ES, Smith DL, Kengne AP and Leach L (2023) Association between physical fitness and musculoskeletal health in firefighters. Front. Physiol. 14:1210107. doi: 10.3389/fphys.2023.1210107
Received: 25 April 2023; Accepted: 19 June 2023;
Published: 04 July 2023.
Edited by:
Filip Kukic, Abu Dhabi Police, United Arab EmiratesReviewed by:
Marcos Michaelides, University of Central Lancashire, CyprusCopyright © 2023 Ras, Soteriades, Smith, Kengne and Leach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaron Ras, MzQwNTYxOEBteXV3Yy5hYy56YQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.