 Pietro Ciliberti1†
Pietro Ciliberti1† Danilo Cardim2,3†Alberto Giardina1†
Danilo Cardim2,3†Alberto Giardina1† Matjaž Groznik4
Matjaž Groznik4 Lorenzo Ball1,5Martina Giovannini5
Lorenzo Ball1,5Martina Giovannini5 Denise Battaglini5Erta Beqiri6Basil Matta7
Denise Battaglini5Erta Beqiri6Basil Matta7 Peter Smielewski6
Peter Smielewski6 Marek Czosnyka6,8Paolo Pelosi1,5
Marek Czosnyka6,8Paolo Pelosi1,5 Chiara Robba1,5*
Chiara Robba1,5*- 1Department of Surgical Sciences and Integrated Diagnostics, University of Genoa, Genoa, Italy
- 2Department of Neurology, University of Texas Southwestern Medical Center, Dallas, TX, United States
- 3Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital, Dallas, TX, United States
- 4Traumatology Department of the University Clinical Center Ljubljana, Ljubljana, Slovenia
- 5Anesthesia and Intensive Care, San Martino Policlinico Hospital, IRCCS for Oncology and Neuroscience, Genoa, Italy
- 6Brain Physics Laboratory, Division of Neurosurgery, Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom
- 7Neurocritical Care Unit, Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom
- 8Institute of Electronic Systems, Warsaw University of Technology, Warsaw, Poland
Introduction: Potential detrimental effects of hyperoxemia on outcomes have been reported in critically ill patients. Little evidence exists on the effects of hyperoxygenation and hyperoxemia on cerebral physiology. The primary aim of this study is to assess the effect of hyperoxygenation and hyperoxemia on cerebral autoregulation in acute brain injured patients. We further evaluated potential links between hyperoxemia, cerebral oxygenation and intracranial pressure (ICP).
Methods: This is a single center, observational, prospective study. Acute brain injured patients [traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), intracranial hemorrhage (ICH)] undergoing multimodal brain monitoring through a software platform (ICM+) were included. Multimodal monitoring consisted of invasive ICP, arterial blood pressure (ABP) and near infrared spectrometry (NIRS). Derived parameters of ICP and ABP monitoring included the pressure reactivity index (PRx) to assess cerebral autoregulation. ICP, PRx, and NIRS-derived parameters (cerebral regional saturation of oxygen, changes in concentration of regional oxy- and deoxy-hemoglobin), were evaluated at baseline and after 10 min of hyperoxygenation with a fraction of inspired oxygen (FiO2) of 100% using repeated measures t-test or paired Wilcoxon signed-rank test. Continuous variables are reported as median (interquartile range).
Results: Twenty-five patients were included. The median age was 64.7 years (45.9–73.2), and 60% were male. Thirteen patients (52%) were admitted for TBI, 7 (28%) for SAH, and 5 (20%) patients for ICH. The median value of systemic oxygenation (partial pressure of oxygen-PaO2) significantly increased after FiO2 test, from 97 (90–101) mm Hg to 197 (189–202) mm Hg, p < 0.0001. After FiO2 test, no changes were observed in PRx values (from 0.21 (0.10–0.43) to 0.22 (0.15–0.36), p = 0.68), nor in ICP values (from 13.42 (9.12–17.34) mm Hg to 13.34 (8.85–17.56) mm Hg, p = 0.90). All NIRS-derived parameters reacted positively to hyperoxygenation as expected. Changes in systemic oxygenation and the arterial component of cerebral oxygenation were significantly correlated (respectively ΔPaO2 and ΔO2Hbi; r = 0.49 (95% CI = 0.17–0.80).
Conclusion: Short-term hyperoxygenation does not seem to critically affect cerebral autoregulation.
Introduction
Acute brain injury is a major cause of mortality and severe disability (Maas et al., 2022). The outcome of these patients is dramatically affected by the quality of treatment in the first hours after the injury and by the prevention of secondary damage in the following hours (Maas et al., 2017; Steyerberg et al., 2019). Secondary brain injury is caused by several mechanisms, including hypotension, hypoxemia, altered cerebral autoregulation and intracranial hypertension (Volpi et al., 2018). More recently, not only the effect of hypoxemia, but also of hyperoxemia has been considered as possible cause of cerebral damage (Robba et al., 2022).
Oxygen is essential for aerobic respiration within mitochondria, but mitochondrial respiration also produces reactive oxygen species (ROS). Excessive administration of oxygen can consequently increase ROS formation, and induce activation of the inflammatory responses, which may cause further cerebral damage (Singer et al., 2021). Acute hyperoxemia can also cause vasoconstriction resulting in reduction of local blood flow, particularly in cerebral and coronary vessels, and possibly alter the vasomotor response of cerebral vessels (Rockswold et al., 2013). Current guidelines (Robba et al., 2020) suggest maintaining an arterial partial pressure of oxygen (PaO2) target of 80–120 mm·Hg in the acute phase of acute brain injury. In patients with traumatic brain injury (TBI), PaO2 values of 150–200 mm·Hg seem to be associated with better functional and cognitive outcome at 6 months, while PaO2 >200 mm·Hg was found to be independently associated with 6-months mortality (Alali et al., 2019). Furthermore, more recently, Rezoagli et al. (Rezoagli et al., 2022) demonstrated that in a large multicenter cohort of TBI patients (n = 1,084) the exposure to higher PaO2 and fraction of inspired oxygen (FiO2) in the first 7 days after ICU admission was independently associated with a higher 6-month mortality, independently of injury severity.
A specific threshold for oxygen neurotoxicity has not yet been identified, as well as the effect of hyperoxemia on cerebral autoregulation (CA) has never been evaluated thoroughly so far. In 2007, Nishimura et al. (2007) evaluated CA using transcranial Doppler in a cohort of healthy volunteers during hyperoxemia, suggesting that dynamic CA may remain unchanged, even with apparent changes in steady-state cerebral blood flow velocities.
At present, the most established method to assess cerebral autoregulation in patients with ICP monitoring in real-time is through the pressure reactivity index (PRx), which is a moving Pearson correlation between slow waves in intracranial pressure (ICP) and arterial blood pressure (ABP). Numerous retrospective studies in different patient populations demonstrated strong correlations between averaged PRx and outcome (Czosnyka et al., 1997; Sorrentino et al., 2012).
The primary aim of this study is to evaluate the short-term effects of hyperoxemia (obtained through FiO2 = 100%) on cerebral autoregulation assessed via PRx. Secondary outcomes include the assessment of the effect of hyperoxemia on cerebral oxygenation and ICP, and the correlation between changes in cerebral autoregulation and systemic as well as cerebral oxygenation parameters.
Methods
Single center, prospective observational study, conducted from first of January 2021 to first of September 2022, at Policlinico San Martino Hospital, IRCCS for Oncology and Neuroscience, Genova, Italy. The study was approved by the local ethics review board (Comitato Etico Regione Liguria, protocol n. CER Liguria: 23/2020). Approval for the study was obtained according to local regulations. This study was performed according to the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” statement guidelines for observational cohort studies (von Elm et al., 2014) (Additional file 1: ESM Supplementary Table S1). Inclusion criteria were patients above 18 years of age, admitted to the intensive care unit (ICU), following acute brain injury [ABI, defined as TBI, or cerebrovascular disease, such as subarachnoid hemorrhage (SAH) or spontaneous intracranial hemorrhage (ICH)], intubated and mechanically ventilated undergoing multimodal neuromonitoring, assigned to beds equipped with of ICM + software (Smielewski et al., 2005) (according to clinical severity and based on bed availability) and receiving pre-oxygenation with 100% FiO2 for clinical reasons at bedside for optimization of respiratory management. Our unit is a mixed general and neuro-ICU, composed of 28 level 3 beds, of which 12 are equipped with ICM + software. Patients without multimodal monitoring, not mechanically ventilated or not receiving pre-oxygenation with 100% FiO2, or those patients whose next of kins refused to agree about inclusion in the study were excluded.
Data collection
Demographics
Demographical (age, gender, body mass index), clinical data (pre-injury comorbidities such as respiratory, cardiovascular, liver and kidney disease, cancer, diabetes mellitus and hypertension), reason for ICU admission (i.e., TBI, SAH, ICH), neurological status at admission as for Glasgow coma scale (GCS), pupils characteristics (reactivity, iso or anisocoria), type of ICP monitoring (intraparenchymal or external ventricular drain), ICU complications (i.e., acute distress respiratory syndrome, ventilator-associated pneumonia, acute kidney injury, sepsis, vasospasm) and patients’ outcome, such as ICU length of stay, mortality and neurological status (Glasgow Outcome Score) at ICU discharge were collected from electronic medical records.
General ICU management
In the ICU, patients were sedated with Propofol/Midazolam and Fentanest and were mechanically ventilated using an endotracheal tube. Tidal volume was targeted to 6–8 mL per kg of predicted body weight (PBW). Higher values of tidal volume were allowed only if the airway driving pressure was maintained below 15 cm H2O. Respiratory rate was adjusted to aim to normocapnia. The decision to perform an FiO2 trial was based on clinician’s evaluation when optimization of mechanical ventilation was required occurring within 24 h of hospital admission, in order to obtain an estimation of the presence of shunt or low ventilation/perfusion ratio and as part of the evaluation of the respiratory function performed in our ICU (Aboab et al., 2006; Ball et al., 2021). Data on neuromonitoring were obtained at baseline (T0) with FiO2 set as for clinical needs, and after the test (T1) which consisted of applying FiO2 set at 100% (during 10 min for stabilization), as previously described (Cressoni et al., 2017). Arterial blood gases, such as partial pressure of oxygen (PaO2) and of carbon dioxide (PaCO2) before and after FiO2 test were also collected.
Multimodal neuromonitoring and management
Invasive ICP monitoring was inserted for clinical reasons according to our local policies following the latest Brain Trauma Foundation Guidelines (Carney et al., 2017). Patients’ clinical management of intracranial hypertension was performed according to the Seattle algorithm (Chesnut et al., 2020). ICP was monitored continuously with a transducer into the parenchymal space or through an external cerebral fluid shunt. ABP was monitored in the radial or femoral artery zeroed at the level of the right atrium (Baxter Healthcare, CA, United States; Sidcup, United Kingdom). In patients with head elevation, no corrections were made for hydrostatic pressure differences. For the assessment of cerebral oxygenation, we used non-invasive continuous regional cerebral oxygen saturation using the Root® with O3® regional oximetry device (Masimo, CA, United States), with a bilateral sensor applied in the frontotemporal region. Final values of rSO2 and its components at T0 and T1 were calculated as the mean between single instant measurements obtained from the right and left frontotemporal sensors. Different parameters of cerebral oxygenation can be obtained from this monitor: a) rSO2, which represents the regional cerebral oxygen saturation, and is derived as the ratio of the concentration of oxyhemoglobin (O2Hb) and total hemoglobin (cHb = O2Hb + HHb, where HHb is deoxyhemoglobin); b) ΔO2Hbi, which is an index associated with changes of concentration of oxyhemoglobin, thus representing predominantly changes in the arterial component of regional oxygen saturation; c) ΔHHbi, an index reflecting changes in concentration of deoxyhemoglobin, approximately representing changes in the venous component of the oxygen saturation; d) ΔcHbi, an index representing the sum of ΔO2Hbi and ΔHHbi components (Robba et al., 2021a). All continuous physiological data were collected simultaneously and analyzed using ICM+ (Cambridge Enterprise, Cambridge, United Kingdom, https://icmplus.neurosurg.cam.ac.uk) (Smielewski et al., 2005), a clinical research software which can provide real-time analysis of multimodal monitoring modalities at the patient’s bedside. Data collected with ICM+ were sampled at 100 Hz. Artifacts were visually inspected and manually removed from the data time series using artifact removal tools on ICM+. Cerebral autoregulation assessed through PRx was calculated over a 5-min moving window as the Pearson correlation of 30 consecutive 10-s average values of ABP and ICP as previously described (Donnelly et al., 2015). A preserved autoregulation was defined as values of PRx below 0.3 whereas higher values are defined as altered CA (Donnelly et al., 2018; Sorrentino et al., 2012). PRx was calculated from T0 (averaged value of a 10-min period before FiO2 test) and T1 (averaged value of a 10-min period immediately after FiO2 test) periods.
Statistical analysis
The Shapiro-Wilk test was used to test the normality of the distribution of the variables. Continuous variables are reported as median and interquartile range (IQR = 25th–75th percentiles). Comparisons between different variables at T0 and T1 were made by repeated measures (paired) t-test for normally distributed variables, while non-normally distributed variables were compared by paired Wilcoxon signed-rank test. Graphical representations of these comparisons are presented as boxplots. Dependent variables were expressed as a change from baseline (T0) in absolute terms (Δ change = T1-T0). The correlations coefficients (95% confidence interval (CI)) between systemic and the different neuromonitoring variables were verified using Pearson’s or Spearman’s method, for parametric and non-parametric variables, respectively. All statistical analyses were performed using RStudio software (version 4.1.1). A p-value <0.05 was considered statistically significant.
Results
During the study period, a total of 110 patients with ABI were admitted to our ICU and were considered for inclusion. Fifty-two patients were excluded as they did not undergo multimodal neuromonitoring while 33 patients were not allocated to beds equipped with multimodal monitoring capability where ICM+ software was installed. A final number of 25 patients were included in the analysis. The characteristics of the patients are presented in Table 1. The median age was 64.7 years (45.9–73.2), and 60% were male. Thirteen patients (52%) were admitted for TBI, 7 (28%) for SAH, and 5 (20%) patients for ICH. Hypertension was the most common preinjury comorbidity (6 patients, 24%), and five patients (20%) were smokers. At ICU discharge, five patients had died (20%), and median GOS was 3 (1.8–4.0). According to the Seattle algorithm for patient management (Chesnut et al., 2020), of the 25 patients included none of them was in tier 3, 13 were in tier 1, and 12 were in tier 2.
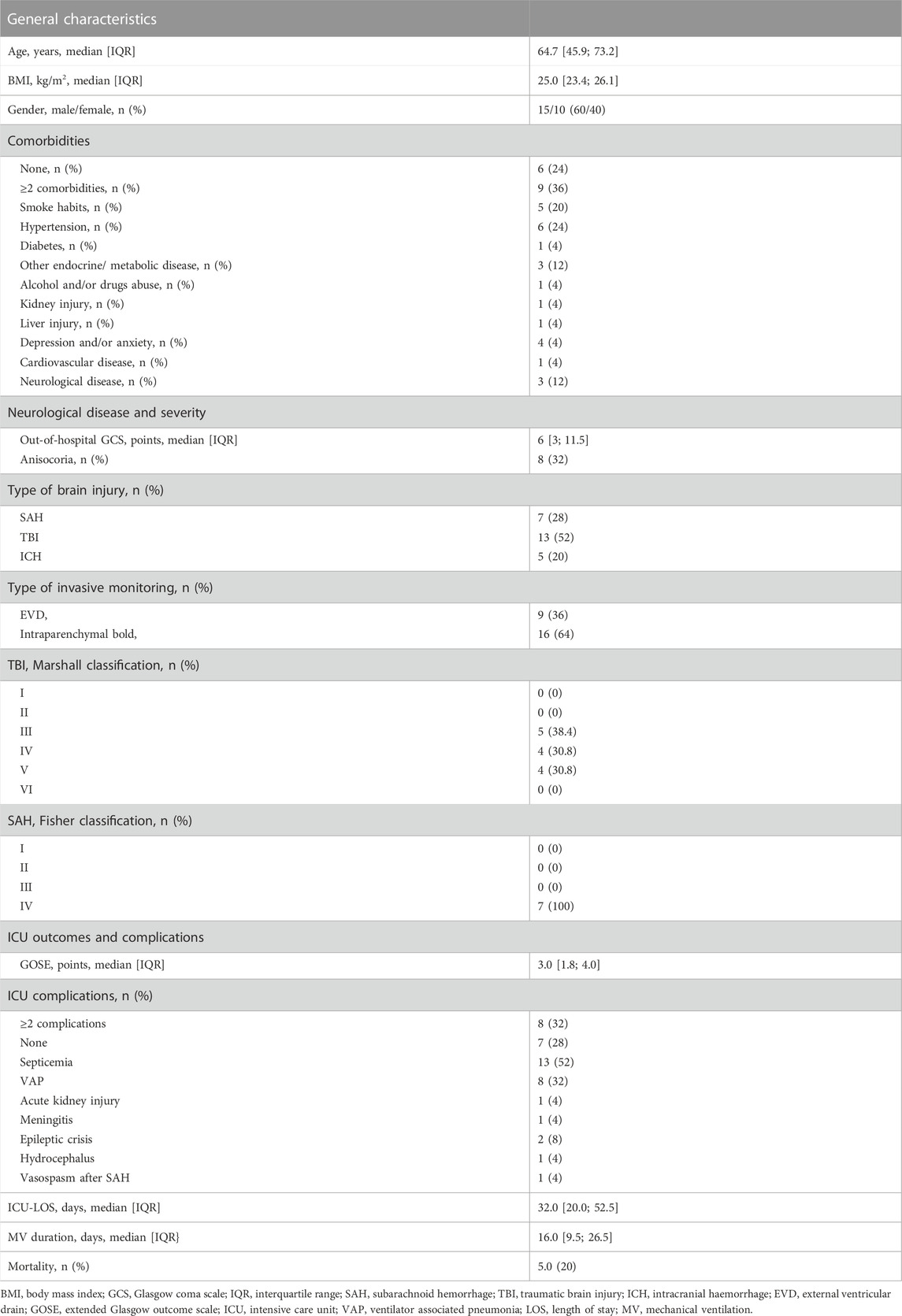
TABLE 1. Demographics, general characteristics, intensive care unit complications.
Effect of FiO2 test on cerebral and systemic factors
The median value of PaO2 significantly increased after FiO2 test, from 97 (90–101) mm·Hg to 197 (189–202) mm·Hg, p < 0.0001 (Table 2). Similarly, SpO2 increased after FiO2 test, from 96 (95–97) % to 100 (100–100) %, p < 0.0001 (paired Wilcoxon test), but PaCO2 did not significantly change (42 (39–44) mm·Hg at T0 and 42 (38–45) mm·Hg at T1, p = 1) (ESM, Supplementary Figure S1). After FiO2 test, no statistically significant changes were observed in PRx values (from 0.21 (0.10–0.43) to 0.22 (0.15–0.36), p = 0.68), as well as on ICP (from 13.42 (9.12–17.34) mm·Hg to 13.34 (8.85–17.56) mmHg, p = 0.99), and CPP values (from 69.20 (60.47–74.72) mm Hg to 71.08 (62.56–75.34) mm Hg, p = 0.76) (Table 2; Figure 1). On an individual basis, nine patients had PRx >0.3 at T0 and T1, consisting of the same individuals at both timepoints. All NIRS parameters increased significantly after FiO2 test (Δ absolute changes). rSO2 increased by 3.12 (2.18–4.00) %, p < 0.0001; ΔO2Hbi by 3.10 (1.60–5.16) μM.cm, p < 0.0001; and ΔHHbi by 1.11 (0.49–2.10) μM.cm, p < 0.0001 (paired Wilcoxon test), respectively (Figure 2).
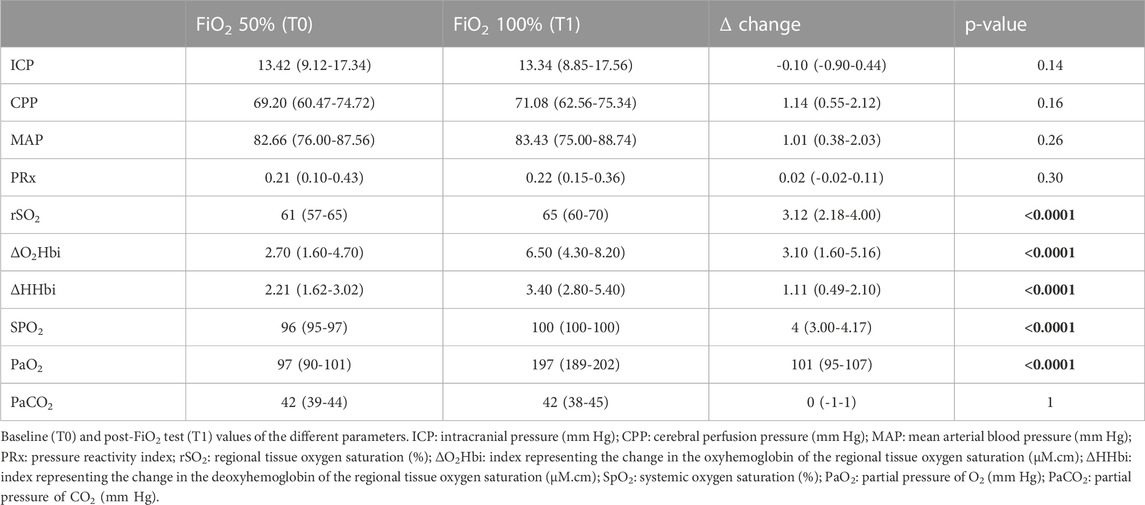
TABLE 2. Systemic and neuromonitoring data before and after the FiO2 test. Data are presented as median and interquartile range.
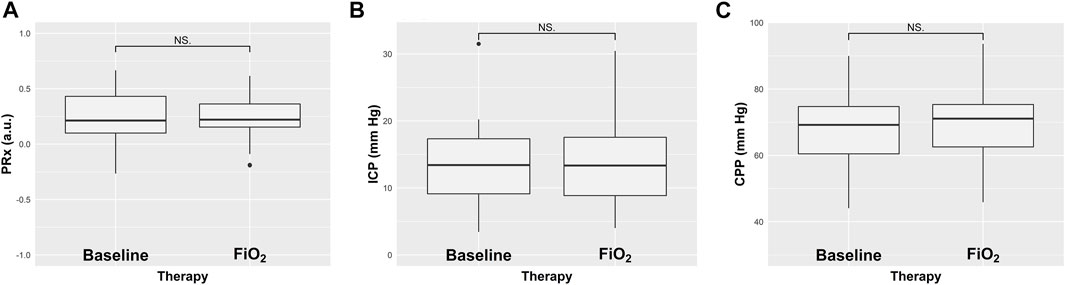
FIGURE 1. Boxplots representing the effect of increased fraction of inspired oxygen (FiO2) on cerebral autoregulation measured with pressure reactivity test (PRx) (A), intracranial pressure (ICP) (B), and cerebral perfusion pressure (CPP) (C) from baseline. Values are presented as median and interquartile range.
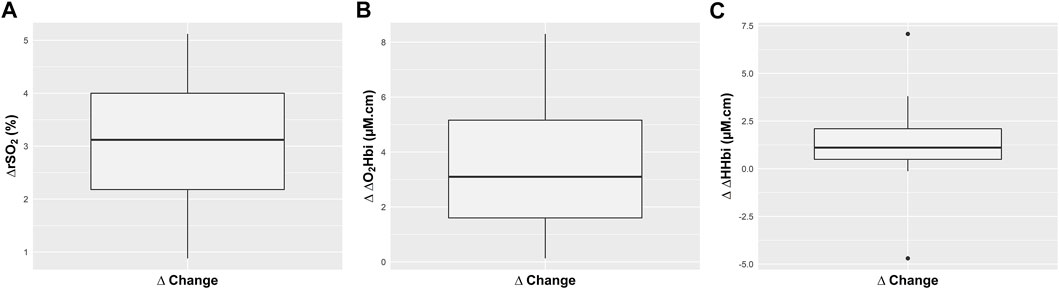
FIGURE 2. Boxplots representing the effect of fraction of increased inspired oxygen (FiO2) on absolute changes (∆) in regional cerebral oxygen saturation (rSO2) (A), and in the arterial (ΔO2Hbi) (B) and venous (ΔHHbi) (C) component of cerebral oxygenation. Values are presented as median and interquartile range.
Correlation between changes in systemic and neuromonitoring parameters
Absolute changes in systemic oxygenation and concentration of oxygenated hemoglobin were significantly correlated [ΔPaO2 and Δ ΔO2Hbi, r = 0.49 (95% CI = 0.17–0.80), p = 0.01 (Spearman’s rank correlation coefficient)] (Figure 3). No other significant correlation was found between the changes of PRx, ICP and other multimodal monitoring parameters with systemic parameters (Table 3).
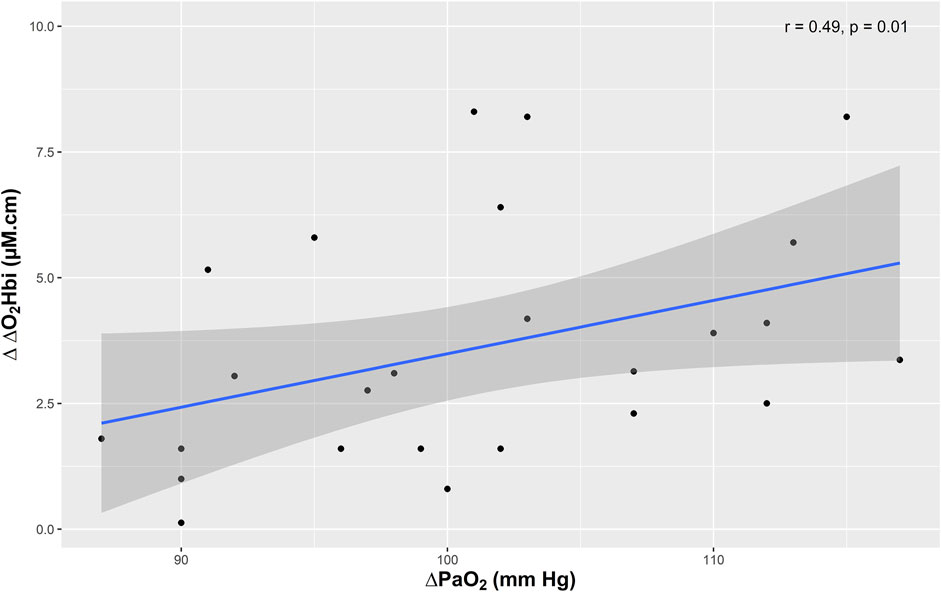
FIGURE 3. Scatter plots showing the correlation (r) between changes in the arterial component of cerebral oxygenation (ΔO2Hbi) and partial pressure of oxygen (PaO2).
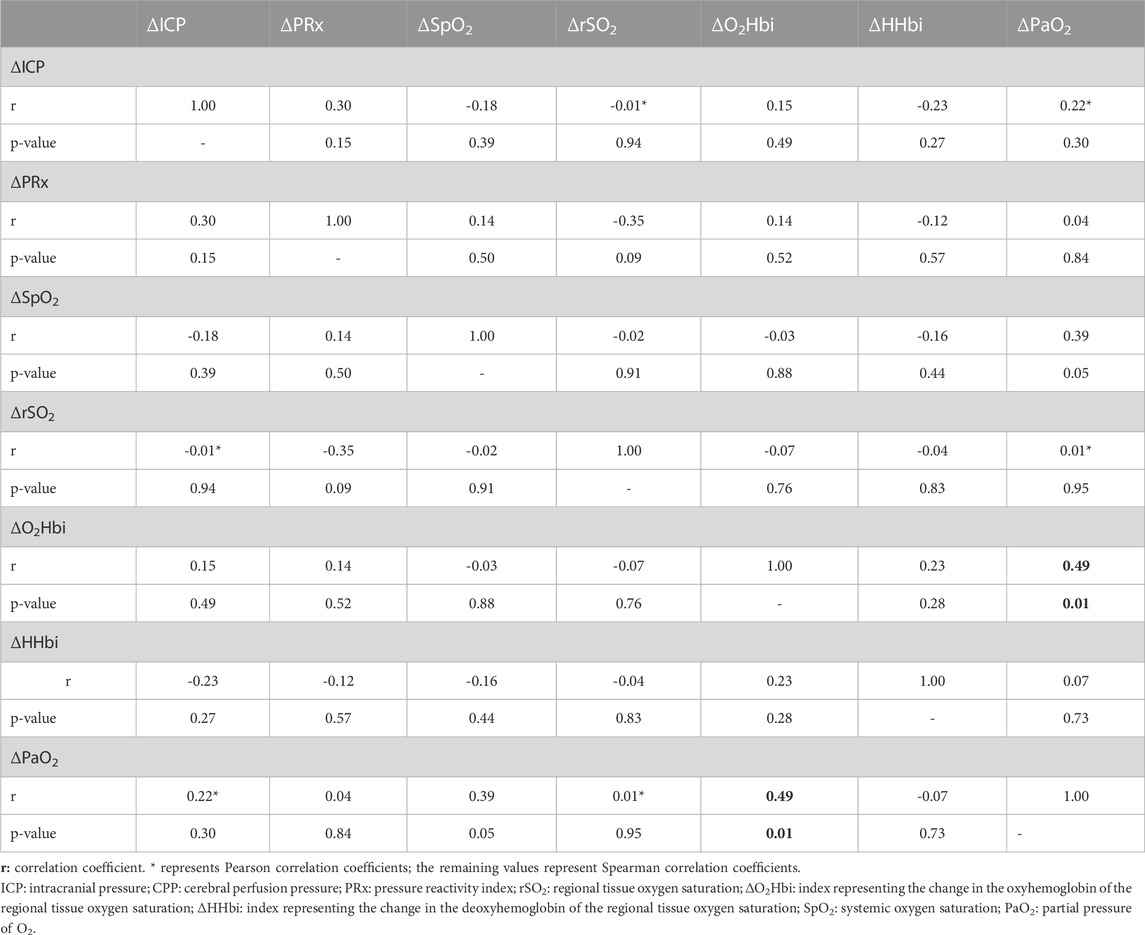
TABLE 3. Correlation between changes(Δ) in systemic and neuromonitoring parameters.
Discussion
In patients with ABI and mechanically ventilated, we found that the increase in systemic PaO2 at FiO2 100% oxygen for 10 min does not affect cerebral autoregulation. The use of specific indices derived from NIRS allowed for hypothesizing on the arterial and venous components of cerebral oxygenation and thus the pathophysiological interplay between systemic and cerebral oxygenations and CA.
To our knowledge, this is the first physiological study assessing the effect of hyperoxemia on CA using continuous monitoring of cerebrovascular pressure reactivity. Previous studies have questioned the effect of hyperoxemia on cerebral dynamics, but without focusing on the importance of cerebral autoregulation. This is clinically relevant, as recent evidence suggests that hyperoxemia can be detrimental to ABI patients and has been associated with poor neurological outcome and independently associated with higher in-hospital fatality (Rincon et al., 2014; Hirunpattarasilp et al., 2022). Cerebral autoregulation is a compensatory mechanism of the brain that allows maintenance of constant cerebral blood flow (CBF) regardless of changes in perfusion pressure (Claassen et al., 2021). The blood pressure range within which cerebral autoregulation is preserved is wide in healthy individuals. In patients with acute brain injuries, this range narrows and the risk of secondary damage increases (Donnelly et al., 2015). Impaired CA has been shown to be associated with worse outcome, highlighting the importance of its assessment (Rincon et al., 2014; Hirunpattarasilp et al., 2022).
PRx is an index of cerebrovascular reactivity which assesses the response of ICP to spontaneous vasogenic changes in ABP (Czosnyka et al., 1997). A positive PRx means a positive gradient of the regression line between the slow oscillations of ABP and ICP, which are associated with passive behavior of non-reactive cerebral arterioles. In this case, an increase in ABP would cause the arterioles to passively dilate, thus the cerebral blood volume would increase, leading to an increase in ICP. Instead, a negative value of PRx reflects reactive cerebral arterioles which actively counteract a change in CPP to maintain CBF stable (Sorrentino et al., 2012). PRx is described as a surrogate index of global cerebral autoregulation. Although other tools are currently available for CA assessment, PRx is considered the most reliable method in neurocritical care patients requiring ICP monitoring. It is the only index validated against the gold standard static methods of direct cerebral perfusion assessment (Steiner et al., 2003; Brady et al., 2007; Depreitere et al., 2021).
Hypoperfusion and hypoxemia are common mechanisms of secondary damage after ABI (Volpi et al., 2018); however, very little is known about the effect of hyperoxemia (Raj et al., 2013; Robba et al., 2021b). Breathing 100% oxygen in normal subject results in vasoconstriction of cerebral blood vessels, which decreases CBF and increases brain tissue oxygenation pressure. However, in TBI, the vascular and tissue responses to hyperoxemia may work differently and may potentially lead to an alteration of the vasomotor response and therefore of autoregulation (Johnston et al., 2003). As discussed by Rezoagli et al. (2022) in their study with TBI patients, increasing PaO2 does not necessarily increase the delivery of oxygen in the injured brain parenchyma. This is related to the fact that oxygen flux is complexly governed by a combination of diffusion and consumption rather than simply tissue difusion (Ercole, 2022). These considerations indicate that the use of hyperoxia, even in the presence of low PbtO2 may be harmful rather than beneficial, given hyperoxia was independently associated with a higher 6-month mortality rate (Ercole, 2022; Rezoagli et al., 2022). At present, findings regarding which hyperoxemia target should be used in ABI patients are inconclusive, and current guidelines only suggest targeting PaO2 values to a range of 80–120 mm·Hg8.
We found no significant change in PRx values after the FiO2 test, which suggests that cerebral autoregulation was, at least, not critically affected by the challenge. This analysis considered the nine patients that had unchanged impaired CA status (PRx >0.3) at both T0 and T1. Moreover, increased systemic PaO2 promoted significant changes in all NIRS parameters, ΔO2Hbi, ΔHHbi and rSO2, suggesting a probable increase in both hemoglobin O2 saturation and cerebral blood flow, thus decreasing O2 extraction fraction. On the other hand, the observed change in PaO2 in our cohort after hyperoxia (ΔPaO2) was only directly correlated with the absolute changes in the arterial component of cerebral oxygenation (as indicated by Δ ΔO2Hbi). This suggests a potential modulation of the arterial component of cerebral oxygenation by increased systemic oxygenation.
A recently published study investigating the effects of hyperoxia on cerebral blood flow velocity and regional oxygen saturation in patients with focal severe TBI found that an increase in rSO2 from normal levels is observed after hyperoxemia only when CA is impaired (Sahoo et al., 2017). This finding suggests that arterial hyperoxia does not lead to an increase in cerebral oxygenation when autoregulation is intact. This previous study (Sahoo et al., 2017) had a considerably higher absolute change in rSO2 after hyperoxia in individuals presenting impaired CA compared to our findings presented here, approximately 11% vs. 3%, respectively. In our case, the substantially smaller change might represent a larger individual variability within patients rather than a true increase in rSO2 caused by impaired CA, or due to the possibility that CA was only partially preserved before and after hyperoxia in our cohort.
PRx, as a means to assess CA globally, reflects largely the myogenic component (pressure reactivity), and to a lesser extent the metabolic component (i.e., cerebrovascular response to O2 and CO2 changes) of cerebral blood flow regulation. Cerebrovascular reactivity to oxygen, for instance, is hampered when cerebral autoregulation is impaired, so that rSO2 increases passively with increasing PaO2. The physiological cerebrovascular response to significant hyperoxia is vasoconstriction (which promotes decrease in cerebral blood volume), while when oxygen reactivity is impaired hyperoxia does not change the vascular resistance (Sahoo et al., 2017). In our cohort, we observed an increase in cerebral blood volume, as indicated by the sum of positive changes in ΔO2Hbi and ΔHHbi (i.e., ΔcHbi). Despite a major increase in PaO2 (from 97 to 197 mm·Hg) after FiO2 test, we did not observe a considerable change in rSO2, nor was this correlated to changes in PaO2. This likely suggests that in our patient cohort CA was at least partially impaired, especially the metabolic component of CA which cannot be fully explained by PRx. Another important remark to consider in the interpretation of our findings is that CA was measured in the non-injured brain tissue, and while total brain PaO2 may be elevated, this increase may not be present in the injured tissue (Ercole, 2022). In this sense, the measure of CA is not a de facto measure of generalized brain health, particularly in regional settings of ABI, where ICP is measured outside of the injured site.
Several limitations of the present study should be addressed. First, the single center design and the small sample cohort limit the generalization of our results. Secondly, due to the lack of a control group, the impact of hyperoxemia on mortality and neurological outcome was not assessed. Thirdly, the FiO2 test was of short duration as for our clinical practice; a more prolonged test could help to better elucidate the long-term impact of hyperoxemia on brain oxygenation in patients with ABI. Further prospective confirmatory studies are necessary to identify a higher hyperoxia threshold which can potentially affect cerebral dynamics and outcome (Grensemann et al., 2022) and to properly define the optimal target of oxygen delivery in acute neurocritical care patient settings and its effects on cerebral dynamics and clinical outcomes. Furthermore, known limitations of NIRS, such as the potential influence of extracranial contamination (particularly in HHb and O2Hb signals), the nature of HHb and HbO2 dependent on the unknown scattering coefficient likely differing on an individual basis, and the unknown contribution of venous and arterial components to the measured signals, particularly the O2Hb, are potential confounders in our study.
Conclusion
In mechanically ventilated neurocritical care patients with ABI, short-term hyperoxemia does not seem to critically affect cerebral autoregulation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Policlinico San Martino Ethical Committee, Genova, Italy. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CR, PP, and MC supervised the work. PC, DC, AG, MG, LB, and DB collected the data and performed initial statistical analysis. All the authors participated in study conception, procedure, data interpretation and analysis. CR, DC, PC, and AG wrote the first draft. All the authors worked on the first draft and approved the final version for submission.
Acknowledgments
The authors would like to thank the Italian Ministero della Salute for the support.
Conflict of interest
BM is Consultant for Masimo; CR received fees for lectures from Masimo and Healthcare; PS and MC are creators of the ICM + software and receive a portion of its licensing fees.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2023.1113386/full#supplementary-material
References
Aboab J., Louis B., Jonson B., Brochard L. (2006). Relation between PaO2/FIO2 ratio and FIO2: A mathematical description. Intensive Care Med. 32 (10), 1494–1497. doi:10.1007/s00134-006-0337-9
Alali A. S., Temkin N., Vavilala M. S., Lele A. V., Barber J., Dikmen S., et al. (2019). Matching early arterial oxygenation to long-term outcome in severe traumatic brain injury: Target values. J. Neurosurg. 132 (2), 537–544. doi:10.3171/2018.10.Jns18964
Ball L., Robba C., Maiello L., Herrmann J., Gerard S. E., Xin Y., et al. (2021). Computed tomography assessment of PEEP-induced alveolar recruitment in patients with severe COVID-19 pneumonia. Crit. Care 25 (1), 81. doi:10.1186/s13054-021-03477-w
Brady K. M., Lee J. K., Kibler K. K., Smielewski P., Czosnyka M., Easley R. B., et al. (2007). Continuous time-domain analysis of cerebrovascular autoregulation using near-infrared spectroscopy. Stroke 38 (10), 2818–2825. doi:10.1161/strokeaha.107.485706
Carney N., Totten A. M., O'Reilly C., Ullman J. S., Hawryluk G. W., Bell M. J. (2017). Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 80 (1), 6–15. doi:10.1227/neu.0000000000001432
Chesnut R., Aguilera S., Buki A., Bulger E., Citerio G., Cooper D. J., et al. (2020). A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: The Seattle international severe traumatic brain injury consensus conference (SIBICC). Intensive Care Med. 46 (5), 919–929. doi:10.1007/s00134-019-05900-x
Claassen J., Thijssen D. H. J., Panerai R. B., Faraci F. M. (2021). Regulation of cerebral blood flow in humans: Physiology and clinical implications of autoregulation. Physiol. Rev. 101 (4), 1487–1559. doi:10.1152/physrev.00022.2020
Cressoni M., Chiumello D., Algieri I., Brioni M., Chiurazzi C., Colombo A., et al. (2017). Opening pressures and atelectrauma in acute respiratory distress syndrome. Intensive Care Med. 43 (5), 603–611. doi:10.1007/s00134-017-4754-8
Czosnyka M., Smielewski P., Kirkpatrick P., Laing R. J., Menon D., Pickard J. D. (1997). Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery. 41 (1), 11–17. discussion 17-9. doi:10.1097/00006123-199707000-00005
Depreitere B., Citerio G., Smith M., Adelson P. D., Aries M. J., Bleck T. P., et al. (2021). Cerebrovascular autoregulation monitoring in the management of adult severe traumatic brain injury: A delphi consensus of clinicians. Neurocrit Care 34 (3), 731–738. doi:10.1007/s12028-020-01185-x
Donnelly J., Aries M. J., Czosnyka M. (2015). Further understanding of cerebral autoregulation at the bedside: Possible implications for future therapy. Expert Rev. Neurother. 15 (2), 169–185. doi:10.1586/14737175.2015.996552
Donnelly J., Czosnyka M., Adams H., Robba C., Steiner L. A., CarDim D., et al. (2018). Pressure reactivity-based optimal cerebral perfusion pressure in a traumatic brain injury cohort. Acta Neurochir. Suppl. 126, 209–212. doi:10.1007/978-3-319-65798-1_43
Ercole A. (2022). Hyperoxia and traumatic brain injury: Time to stop cooking the books? Intensive Care Med. 49, 123–124. doi:10.1007/s00134-022-06938-0
Grensemann J., Mader M. M., Westphal M., Kluge S., Czorlich P. (2022). Hyperoxia is dose-dependently associated with an increase of unfavorable outcomes in ventilated patients with aneurysmal subarachnoid hemorrhage: A retrospective cohort study. Neurocrit Care 37 (2), 523–530. doi:10.1007/s12028-022-01534-y
Hirunpattarasilp C., Shiina H., Na-Ek N., Attwell D. (2022). The effect of hyperoxemia on neurological outcomes of adult patients: A systematic review and meta-analysis. Neurocrit Care. 36 (3), 1027–1043. doi:10.1007/s12028-021-01423-w
Johnston A. J., Steiner L. A., Gupta A. K., Menon D. K. (2003). Cerebral oxygen vasoreactivity and cerebral tissue oxygen reactivity. Br. J. Anaesth. 90 (6), 774–786. doi:10.1093/bja/aeg104
Maas A. I. R., Menon D. K., Adelson P. D., Andelic N., Bell M. J., Belli A., et al. (2017). Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16 (12), 987–1048. doi:10.1016/s1474-4422(17)30371-x
Maas A. I. R., Menon D. K., Manley G. T., Abrams M., Akerlund C., Andelic N., et al. (2022). Traumatic brain injury: Progress and challenges in prevention, clinical care, and research. Lancet Neurol. 21 (11), 1004–1060. doi:10.1016/s1474-4422(22)00309-x
Nishimura N., Iwasaki K., Ogawa Y., Shibata S. (2007). Oxygen administration, cerebral blood flow velocity, and dynamic cerebral autoregulation. Aviat. Space Environ. Med. 78 (12), 1121–1127. doi:10.3357/asem.2177.2007
Raj R., Bendel S., Reinikainen M., Kivisaari R., Siironen J., Lang M., et al. (2013). Hyperoxemia and long-term outcome after traumatic brain injury. Crit. Care 17 (4), R177. doi:10.1186/cc12856
Rezoagli E., Petrosino M., Rebora P., Menon D. K., Mondello S., Cooper D. J., et al. (2022). High arterial oxygen levels and supplemental oxygen administration in traumatic brain injury: Insights from CENTER-TBI and OzENTER-TBI. Intensive Care Med. 48 (12), 1709–1725. doi:10.1007/s00134-022-06884-x
Rincon F., Kang J., Vibbert M., Urtecho J., Athar M. K., Jallo J. (2014). Significance of arterial hyperoxia and relationship with case fatality in traumatic brain injury: A multicentre cohort study. J. Neurol. Neurosurg. Psychiatry. 85 (7), 799–805. doi:10.1136/jnnp-2013-305505
Robba C., Ball L., Battaglini D., Cardim D., Moncalvo E., Brunetti I., et al. (2021). Early effects of ventilatory rescue therapies on systemic and cerebral oxygenation in mechanically ventilated COVID-19 patients with acute respiratory distress syndrome: A prospective observational study. Crit. Care. 25 (1), 111. doi:10.1186/s13054-021-03537-1
Robba C., Ball L., Battaglini D., Iannuzzi F., Brunetti I., Fiaschi P., et al. (2022). Effects of positive end-expiratory pressure on lung ultrasound patterns and their correlation with intracranial pressure in mechanically ventilated brain injured patients. Crit. Care 26 (1), 31. doi:10.1186/s13054-022-03903-7
Robba C., Citerio G., Taccone F. S., Galimberti S., Rebora P., Vargiolu A., et al. (2021). Multicentre observational study on practice of ventilation in brain injured patients: The VENTIBRAIN study protocol. BMJ Open 11 (8), e047100. doi:10.1136/bmjopen-2020-047100
Robba C., Poole D., McNett M., Asehnoune K., Bosel J., Bruder N., et al. (2020). Mechanical ventilation in patients with acute brain injury: Recommendations of the European society of intensive care medicine consensus. Intensive Care Med. 46 (12), 2397–2410. doi:10.1007/s00134-020-06283-0
Rockswold S. B., Rockswold G. L., Zaun D. A., Liu J. (2013). A prospective, randomized Phase II clinical trial to evaluate the effect of combined hyperbaric and normobaric hyperoxia on cerebral metabolism, intracranial pressure, oxygen toxicity, and clinical outcome in severe traumatic brain injury. J. Neurosurg. 118 (6), 1317–1328. doi:10.3171/2013.2.Jns121468
Sahoo S., Sheshadri V., Sriganesh K., Madhsudana Reddy K. R., Radhakrishnan M., Umamaheswara Rao G. S. (2017). Effect of hyperoxia on cerebral blood flow velocity and regional oxygen saturation in patients operated on for severe traumatic brain injury-the influence of cerebral blood flow autoregulation. World Neurosurg. 98, 211–216. doi:10.1016/j.wneu.2016.10.116
Singer M., Young P. J., Laffey J. G., Asfar P., Taccone F. S., Skrifvars M. B., et al. (2021). Dangers of hyperoxia. Crit. Care 25 (1), 440. doi:10.1186/s13054-021-03815-y
Smielewski P., Czosnyka M., Steiner L., Belestri M., Piechnik S., Pickard J. D. (2005). ICM+: Software for on-line analysis of bedside monitoring data after severe head trauma. Acta Neurochir. Suppl. 95, 43–49. doi:10.1007/3-211-32318-x_10
Sorrentino E., Diedler J., Kasprowicz M., Budohoski K. P., HaubriCh C., Smielewski P., et al. (2012). Critical thresholds for cerebrovascular reactivity after traumatic brain injury. Neurocrit Care. 16 (2), 258–266. doi:10.1007/s12028-011-9630-8
Steiner L. A., Coles J. P., Johnston A. J., Chatfield D. A., Smielewski P., Fryer T. D., et al. (2003). Assessment of cerebrovascular autoregulation in head-injured patients: A validation study. Stroke. 34 (10), 2404–2409. doi:10.1161/01.Str.0000089014.59668.04
Steyerberg E. W., Wiegers E., Sewalt C., Buki A., Citerio G., De Keyser V., et al. (2019). Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: A European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 18 (10), 923–934. doi:10.1016/s1474-4422(19)30232-7
Volpi P. C., Robba C., Rota M., Vargiolu A., Citerio G. (2018). Trajectories of early secondary insults correlate to outcomes of traumatic brain injury: Results from a large, single centre, observational study. BMC Emerg. Med. 18 (1), 52. doi:10.1186/s12873-018-0197-y
von Elm E., Altman D. G., Egger M., Pocock S. J., Gøtzsche P. C., Vandenbroucke J. P., et al. (2014). The strengthening the reporting of observational studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 12 (12), 1495–1499. doi:10.1016/j.ijsu.2014.07.013
Keywords: hyperoxygenation, cerebral autoregulation, brain injury, intracranial pressure, cerebral oxygenation
Citation: Ciliberti P, Cardim D, Giardina A, Groznik M, Ball L, Giovannini M, Battaglini D, Beqiri E, Matta B, Smielewski P, Czosnyka M, Pelosi P and Robba C (2023) Effects of short-term hyperoxemia on cerebral autoregulation and tissue oxygenation in acute brain injured patients. Front. Physiol. 14:1113386. doi: 10.3389/fphys.2023.1113386
Received: 01 December 2022; Accepted: 25 January 2023;
Published: 08 February 2023.
Edited by:
Raimond L. Winslow, Northeastern University, United StatesReviewed by:
Brian Leonard Appavu, Phoenix Children’s Hospital, United StatesAnthony Richard Bain, University of Windsor, Canada
Copyright © 2023 Ciliberti, Cardim, Giardina, Groznik, Ball, Giovannini, Battaglini, Beqiri, Matta, Smielewski, Czosnyka, Pelosi and Robba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Robba, a2lhcm9iYmFAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship