 Ning Que
Ning Que
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 25 January 2023
Sec. Exercise Physiology
Volume 14 - 2023 | https://doi.org/10.3389/fphys.2023.1058637
This article is part of the Research Topic Biomechanical Performance and Relevant Mechanism of Physical Medicine and Rehabilitation for Neuromusculoskeletal Disorders View all 32 articles
Objective: Kinesio taping (KT) and vibration treatment (VT) can alleviate delayed-onset muscle soreness (DOMS) to some extent. However, the literature reports on the difference between the two treatments, and whether a joint intervention (JI) works better than single treatments remains unknown. This study compares the effects of KT, VT and JI on DOMS in college students.
Methods: A total of 88 college students were randomly divided into the KT (KTG, n = 21), VT (VTG, n = 22), JI (JIG, n = 23) and control (CG, n = 22) groups. All subjects underwent DOMS moulding. The baseline; immediate and 24, 48 and 72 h visual analogue scale (VAS) scores and knee extensor maximum isometric voluntary contraction (MIVC) were determined.
Results: The intergroup comparison showed the following results. 1) The VAS scores of the four groups peaked at 24 h and gradually decreased. The immediate, 24 h and 48 h VAS scores followed the order: JIG > KTG and VTG > CG. The 72 h VAS score followed the order: KTG < VTG < JIG < CG. 2) The knee extension MIVC in the four groups was lowest at 24 h and then gradually increased. JIG had larger immediate MIVC than CG. KTG, VTG and JIG had larger 24 h MIVC than CG. JIG had larger 48 h MIVC than KTG and CG.
Conclusion: KT and VT can reduce muscle pain and strength loss caused by DOMS to varying degrees. VT is better than KT in improving pain. The combined intervention worked better than single interventions.
Delayed-onset muscle soreness (DOMS) occurs from 8 h to 24 h after unaccustomed or intense centrifugal exercise and can peak and gradually relieve within 48–72 h, requiring approximately 1 week to restore (Afonso et al., 2021; Fleckenstein et al., 2021; Sonkodi et al., 2021; Torre et al., 2021). DOMS comes with a series of muscle structural, histological and biochemical changes, thus affecting physical fitness and exercise training effects. The increased risk of exercise injury (Akinci et al., 2020; Pupo et al., 2021) and reduced adverse effects caused by DOMS deserve concern.
In 1973, Dr. Kenso Kase invented the kinesio taping (KT) technology (Tran et al., 2021; Turgut et al., 2021). Previous studies confirmed the positive effect of KT on DOMS. KT intervention before DOMS moulding reduces bicep soreness in young men and accelerates the maximum isometric voluntary contraction (MIVC) recovery in muscles (Lee et al., 2015). KT intervention lowers the cold and thermal pain thresholds and the visual analogue scale (VAS) score for young male biceps brachii (DOMS) for 24 h (Bae et al., 2014). KT intervention also reduces centrifugal pain in the rectus femoris and hamstring (DOMS) for 24 and 168 h and improves the performance of hamstrings (Haksever et al., 2016). Furthermore, a meta-analysis suggested that appropriate vibration treatment (VT) can relieve DOMS symptoms (Lu et al., 2019). VT significantly reduces the VAS score and MIVC in ordinary young women (elbow DOMS, 50 Hz, 5 min) (Imtiyaz et al., 2014). The joint activity of ordinary male college students is increased (elbow DOMS, 20 Hz, 30 min), and the immediate VAS score (Lau and Nosaka, 2011) is reduced. MIVC for ordinary young males/females is increased (radial wrist extensor DOMS, 20 Hz, 2 min) (Koh et al., 2013). The VAS score of ordinary male college students is reduced (DOMS, 20 Hz–45 Hz, 10 min) (Wheeler and Jacobson, 2013). The above two methods can alleviate DOMS to some extent. KT can lift the skin of the ligation site, increase the tissue space and accelerate the blood and lymphatic circulation and inflammatory response (Tran et al., 2021). VT increases muscle discharge, local muscle temperature and blood flow to the skin; accelerates blood and lymphatic circulation and alleviates inflammatory response and pain (Lau and Nosaka, 2011; Koh et al., 2013; Wheeler and Jacobson, 2013; Imtiyaz et al., 2014; Lu et al., 2019). However, the literature only reports on the difference between the two treatments, and whether a joint intervention works better than single treatments remains unknown. Compared with single treatment (KT or VT), joint intervention may be a better way to delay DOMS.
This study explores the effect of KT with VT on DOMS symptoms in college students and provides the basis for the combined KT and VT intervention to reduce exercise-induced DOMS. The study hypothesises that the combination of KT and VT is more effective in relieving DOMS symptoms than a single treatments.
This study was approved by our school’s ethics committee (2021.011). Special male college badminton students were recruited during the holidays. The inclusion criteria were as follows: students (1) between 18 and 20 years old, (2) weighing 60 kg–70 kg, (3) exercising irregularly for the last 2 weeks and (4) who complied with the Declaration of Helsinki and provided informed consent. The exclusion criteria were as follows: students with (1) motor injury to the lower limbs, (2) heart pacemaker installation, (3) cardiovascular disease and (4) epilepsy or other central nervous system diseases.
This study based the sample size on previous research results regarding the previous study on Kinesio Taping and Vibration Treatment in College Students’Delayed-Onset Muscle Soreness (Imtiyaz et al., 2014; Haksever et al., 2016), a 4 (groups) × 5 (measurement times) experimental design and a 10% sample wastage rate. G-power program was applied to calculate the effect size and total sample size. With an effect size of 0.3, α level of 0. 05 and power of 0.8, a sample size of at least 84 samples was needed. Ninety-two subjects were recruited. Four cases did not continue because of personal reasons. A total of 88 subjects completed the whole experiment (Figure 1). The random-number distribution method was used to divide subjects into four groups, i.e., KT (KTG), VT (VTG), joint intervention (JIG) and control (CG) groups. No significant difference in age, height and body weight was observed amongst groups (p > 0.05, Table 1). For VTG, VT was given after DOMS moulding. For KTG, Y-shaped binding was conducted for 15 min before DOMS moulding (Kirmizigil et al., 2019). After moulding, when VTG performed vibration intervention, KTG sat and rested. JIG, KTG and VTG interventions were simultaneous. For CG, no intervention happened except DOMS moulding.
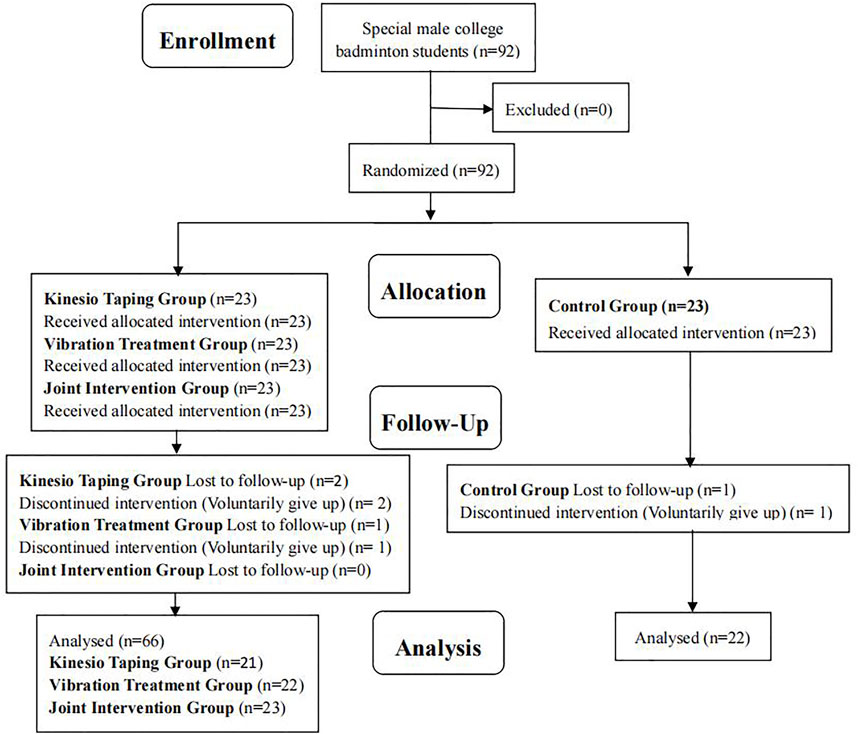
FIGURE 1. Participant selection flow diagram.

TABLE 1. Participants’ basic information.
In accordance with the previous method of DOMS knee moulding in the sports population (Pumpa et al., 2011; Song and Yang, 2022), all subjects underwent a maximum oxygen intake test 1 week before the moulding process (German Cortex cardiopulmonary function tester model: Metalyzer 3B). Moulding happened after a week, and subjects ran downhill on the treadmill (American ICON, model: 59916/350i; −10° grade, five groups of 8 min, with 2 min flat walking between groups). Each subject’s exercise intensity was matched on the basis of the maximum oxygen intake, ensuring that all subjects maintained similar intensity while completing the downhill run. All participants were monitored to maintain their intensity at 80% of their maximum heart rate (Model No. M430; Polar, Finland) during downhill running. The treadmill speed was appropriately adjusted if the heart rate was excessively low or high. All participants were followed up within 72 h of DOMS moulding to ensure no other training or treatment (Figure 2).
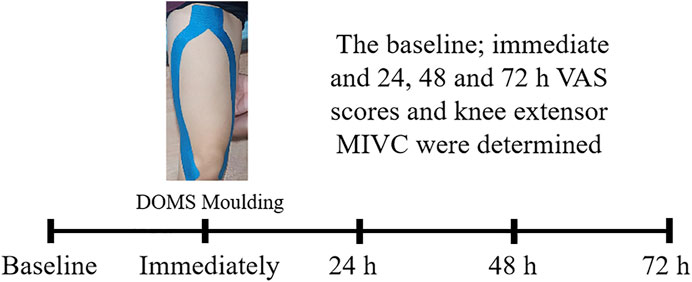
FIGURE 2. Intervention process.
The “Y” ligation of the bilateral knees of KTG and JIG was conducted by a professional physical therapist 15 min before DOMS moulding (Kirmizigil et al., 2019) (KT was provided by the LP Support company, specification: 5 cm × 5 m, color: blue), stretched to 125% of the original length (Boobphachart et al., 2017). (Figure 2). To prevent KT shedding throughout DOMS moulding and within 72 h, we checked immediately and at 24, 48 and 72 h with the same ligation.
Under the guidance of the experimenter, the American Power-Plate® pro5™ (71-PR5-3100, Frequencies 25–50 Hz) was used for 10 min on VTG and JIG (squatting and launching on the vibrational platform), referring to the vibration frequency interval and amplitude where VT had a positive effect on DOMS (Lau and Nosaka, 2011; Koh et al., 2013; Wheeler and Jacobson, 2013; Imtiyaz et al., 2014; Lu et al., 2019). This study’s vibration frequency and amplitude were 45 Hz and 3 mm (G-Factor 7 45 Hz/High Amplitude), respectively. Four groups of subjects underwent VAS score and knee extension maximum isometric muscle strength tests at DOMS baseline or before moulding and after moulding, 24, 48 and 72 h.
The VAS score was used to evaluate the pain of the DOMS (quadriceps femoris) to allow the subject to draw a vertical line on a 10 cm line (0 cm, painless; 10 cm, most painful; 0–10 and left and right knee averaging) (Cheng and Jiang, 2020; Arieh et al., 2022).
The MIVC test was performed on left and right knee joints. The subject took a seated position, and the trunk and hip joints were fixed using a wide band. During the test, the subject underwent MIVC at knee flexion 30°, and the subject makes full effort (using the maximum force as far as possible) to extend the knee joint. The test time is 15 s, at this time, the maximum peak torque recorded by the isokinetic instrument is MIVC. The left and right knees of each subject were tested. The analysis index was peak torque (Cheng and Jiang, 2020; Cheng et al., 2021), and the left and right knee data of all subjects were averaged.
SPSS 19.0 software, mean ± standard deviation for four groups. A two-way analysis of variance with mixed design was used to test whether groups, the main effect of time, and group (4) and time (5) interacted. If group and time interacted, the one-way ANOVA with repeated measures would vary at different time points. If time had the main effect, different time points were compared. If groups had a main effect, differences between groups were compared. The Bonferroni for posthoc comparisons was adjusted to ensure that the overall type I rate per ANOVA was not greater than 0.05. The significance level was 0.05.
The results of five time points for the four subjects are shown in Table 2; Table 3. First, the two-way ANOVA VAS score and knee extension MIVC group × time interacted (p < 0.01), showing differences at different time points within the one-way ANOVA group. The comparison of baseline data between groups showed that VAS scores (F(3, 84) = 0.292, p = 0.746) and MIVC (F(3, 84) = 0.354, p = 0.692) were not significantly different (p > 0.05, Table 1).

TABLE 2. VAS scores test for knee extension at different times.

TABLE 3. MIVC Test for Knee Extension at different times. (Nm).
VAS score: Table 2 shows that the VAS score of the four groups peaked and gradually decreased at 24 h after DOMS moulding. The comparison between groups showed the following results. KTG and VTG had lower immediate, 24 h and 48 h VAS scores than CG (p < 0.05). JIG had lower immediate, 24 h and 48 h VAS scores than CG (p < 0.01). KTG and VTG had higher immediate, 24 h and 48 h VAS scores than JIG (p < 0.05). VTG and JIG had lower 72 h VAS score than CG (p < 0.01). KTG had higher 72 h VAS score than VTG (p < 0.01). KTG (p < 0.01) and VTG (p < 0.05) had higher 72 h VAS score than JIG.
MIVC: Table 3 shows that the MIVC of the four groups was lowest at 24 h after DOMS moulding. The comparison between groups showed the following results. JIG had larger immediate MIVC than CG (p < 0.05). KTG, VTG and JIG had larger 24 h MIVC than CG (p < 0.05). JIG had larger 48 h MIVC than KTG and CG (p < 0.05).
This study seeks to explore pain and MIVC changes caused by KT and VT on special college badminton students’ DOMS and provides the basis for reducing exercise-induced DOMS. We have tested the hypothesis that the combination of KT and VT is more effective in alleviating DOMS symptoms than single treatment.
This study found that KT significantly reduces immediate, 24 h and 48 h VAS scores. This finding confirms the results of previous similar studies on KT, which show that biceps brachii and DOMS moulding reduce immediate, 24 h, 48 h (Bae et al., 2014) and 72 h (Lee et al., 2015) VAS scores. KT is equally effective when subjects are female, and the DOMS site is the thigh, thus reducing the VAS score for the rectus femoris and hamstrings at 48 and 168 h in young women (Haksever et al., 2016).
Why does KT reduce muscle pain caused by DOMS? The vessel diameter of the DOMS site decreases, thus impairing blood flow reaction and causing hyperalgesia (Ko and Clarkson, 2020). Tissue swelling at the DOMS damage site affects blood and lymph circulation (Fang and Nasir, 2021). KT can lift the skin of the ligation site, increase the tissue space and accelerate the blood and lymphatic circulation and the inflammatory response. This lifting can help relieve pressure on nociceptors directly under the skin and remove the accumulated metabolites (Tran et al., 2021), thus reducing pain and feeling. Alternatively, KT provides sustained tactile and proprioceptive inputs to the ligation site, thereby inhibiting the input of nociception (Saki et al., 2022).
This study found that KT significantly enhances the MIVC of the knee extensor for 24 h. The meta-analysis (including four randomised controlled trials) confirmed our conclusion that KT significantly increases the knee extensor muscle (DOMS) MIVC (Tran et al., 2021). KT increases skin input then enhances the function of neuromuscles, promotes muscle activity at the ligation site, improves muscle structure and contributes to a slight increase in muscle force (Tran et al., 2021). Furthermore, the subject reduces the muscle strength test caused by pain (does not exert more force).
This study found that VT significantly reduces immediate, 24 h, 48 h and 72 h VAS scores. Previous studies showed that VT reduces muscle pain in the knee joint immediately after DOMS. VT significantly reduces the immediate, 24 h and 48 h VAS scores (20 Hz–45 Hz, 10 min) of ordinary college male students (Wheeler and Jacobson, 2013) and significantly reduces the VAS scores (30 Hz, 10 min) of men at 96 and 120 h (Broadbent et al., 2010). In the present study, VT at 45 Hz for 10 min is adopted for DOMS sites. The vibration frequency and time of the intervention vary, and the VAS score is significantly reduced at different measurement times. These findings are similar to those of previous studies (Broadbent et al., 2010; Wheeler and Jacobson, 2013), showing that VT can relieve muscle pain after DOMS moulding.
Several current views explained the pain reduction caused by VT. VT stimulates myospindle and motor neurons, causing strong muscle contraction to produce a perceptual response and relieve pain. VT activates large-muscle diameter fibres, inhibits small-diameter fibres and reduces pain. VT also accelerates the stimulation of inhibitory interneurons in the middle nerve endings of the spinal nerve and reduces the transmission of perceptual information from the spinal cord to the brain (feedback of proprioceptors for nociception inhibition) to reduce pain. VT increases muscle discharge, local muscle temperature and blood flow to the skin; accelerates blood and lymphatic circulation and alleviates the inflammatory response and pain (Lau and Nosaka, 2011; Koh et al., 2013; Wheeler and Jacobson, 2013; Imtiyaz et al., 2014; Lu et al., 2019).
VTG has significantly higher MIVC than CG (24 h). In previous studies, VT (50 Hz, 5 min) on the elbow in ordinary young women shows that the MIVC increases at 72 h (Koh et al., 2013). VT (50 Hz, 30 min) on common male/female femoral quadriceps reveals a significant increase in MIVC for 24 h (Bakhtiary et al., 2007). The above study partly supports the present study’s conclusions. The analysis may be related to the activation of increased motor units (DOMS sites) in increased muscle tension. Muscle spindle stimulation by vibration may increase the afferent activities of muscle spindles, which may increase background tension in the vibrated muscles (Bakhtiary et al., 2007; Broadbent et al., 2010; Koh et al., 2013). Furthermore, given the reduced muscle pain, the subject is believed to have reduced muscle strength caused by pain (afraid to force) during the isometric muscle force test.
This study has compared KTG, VTG and JIG. The VAS score of JIG at 72 h decreases significantly compared with that of the control group. The MIVC of the extensor knee muscles is significantly increased at 24 and 48 h. The VAS scores of JIG immediate ∼72 h are considerably smaller than those of KTG and VTG, indicating that the combined intervention can better relieve the muscle pain caused by DOMS than single treatments. The MIVC of JIG is significantly higher than that of KTG (48 h), indicating that the combined intervention significantly affects muscle force at 48 h than single treatments. No literature report has been made on combining conditions on muscle pain and strength at the DOMS site. The effects are also speculated to increase after the joint intervention of KT and VT, and we can provide evidence for similar future studies. This study has found that the VAS score (72 h) of VTG is less than that of KTG, indicating that VT relieves muscle pain caused by DOMS better than KT over time. Our results suggest that, in clinical practice, reasonable KT and VT intervention may delay the symptoms of DOMS when the exercise population performs high-intensity exercise.
This study has some limitations. First is the small sample size, which only comprise special college badminton students. Second, no blood indicator is collected. Lastly, a placebo treatment is not designed. Further expansion of the sample is needed to explore how KT and VT improve DOMS symptoms.
KT and VT can significantly reduce muscle pain and strength loss caused by DOMS. VT works better than KT in improving pain. The combination treatment is better than single interventions.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
This study was approved by the ethics committee of Chengdu Sport University (2021.011). Before the assessment, every participant received the same detailed information about the testing procedure. Every participant signed the informed consent. The patients/participants provided their written informed consent to participate in this study.
Author contributions NQ: designing this study and writing initial draft and revision. NQ: making figure and table. NQ: rechecking the manuscript and putting forward suggestions for amendment. NQ: revising language and content, supervision, project administration, and funding acquisition. NQ contributed to the article and approved the submitted version.
Thanks to the subjects who participated in the experiment. Thanks to the experimenters who participated in the experiment.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Afonso J., Clemente F. M., Nakamura F. Y., Morouco P., Sarmento H., Inman R. A., et al. (2021). The effectiveness of post-exercise stretching in short-term and delayed recovery of strength, range of motion and delayed onset muscle soreness: A systematic review and meta-analysis of randomized controlled trials. Front. Physiol. 12, 677581. doi:10.3389/fphys.2021.677581
Akinci B., Zenginler Yazgan Y., Altinoluk T. (2020). The effectiveness of three different recovery methods on blood lactate, acute muscle performance, and delayed-onset muscle soreness: A randomized comparative study. J. Sports Med. Phys. Fit. 60 (3), 345–354. doi:10.23736/S0022-4707.19.10142-9
Arieh H., Abdoli B., Farsi A., Haghparast A. (2022). Assessment of motor skill accuracy and coordination variability after application of local and remote experimental pain. Res. Sports. Med. 30 (3), 325–341. doi:10.1080/15438627.2021.1888104
Bae S. H., Lee Y. S., Kim G. D., Kim K. Y. (2014). The effects of kinesio-taping applied to delayed onset muscle soreness on changes in pain. Bio-science bio-technology 6 (3), 133–142. doi:10.14257/ijbsbt.2014.6.3.16
Bakhtiary A. H., Safavi-Farokhi Z., Aminian-Far A. (2007). Influence of vibration on delayed onset of muscle soreness following eccentric exercise. Br. J. Sports Med. 41 (3), 145–148. doi:10.1136/bjsm.2006.031278
Boobphachart D., Manimmanakorn N., Manimmanakorn A., Thuwakum W., Hamlin M. J. (2017). Effects of elastic taping, non-elastic taping and static stretching on recovery after intensive eccentric exercise. Res. Sports Med. 25 (2), 181–190. doi:10.1080/15438627.2017.1282360
Broadbent S., Rousseau J. J., Thorp R. M., Choate S. L., Jackson F. S., Rowlands D. S. (2010). Vibration therapy reduces plasma IL6 and muscle soreness after downhill running. Br. J. Sports Med. 44 (12), 888–894. doi:10.1136/bjsm.2008.052100
Cheng L., Jiang Y. (2020). Effect of extracorporeal shock wave therapy on pain and forearm rotating muscle strength in patients with tennis elbow. Med. Sport. 73 (4), 661–672. doi:10.23736/S0025-7826.20.03685-6
Cheng L., Xu H., He B. X., Zhou J. (2021). Changes in isokinetic muscle strength of the knee in elite female adolescent volleyball players after 4 years of systematic training. Med. Sport. 74 (3), 384–395. doi:10.23736/S0025-7826.21.03885-0
Fang W., Nasir Y. (2021). The effect of curcumin supplementation on recovery following exercise-induced muscle damage and delayed-onset muscle soreness: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 35 (4), 1768–1781. doi:10.1002/ptr.6912
Fleckenstein J., Neuberger E. W., Bormuth P., Comes F., Schneider A., Banzer W., et al. (2021). Investigation of the sympathetic regulation in delayed onset muscle soreness: Results of an RCT. Front. Physiol. 12, 697335. doi:10.3389/fphys.2021.697335
Haksever B., Kinikli G. L., Tunay V. B., Karahan S., Donmez G. (2016). Effect of kinesiotaping intervention on knee muscle strength and delayed onset muscle soreness pain following eccentric fatigue training. Fiz. Rehabil. 27 (1), 12–18. doi:10.21653/tfrd.269447
Imtiyaz S., Veqar Z., Shareef M. Y. (2014). To compare the effect of vibration therapy and massage in prevention of delayed onset muscle soreness (DOMS). J. Clin. Diagn. Res. 8 (1), 133–136. doi:10.7860/JCDR/2014/7294.3971
Kirmizigil B., Chauchat J. R., Yalciner O., Iyigun G., Angin E., Baltaci G. (2019). The effectiveness of kinesio taping in recovering from delayed onset muscle soreness: A crossover study. J. Sport. Rehabil. 29 (4), 385–393. doi:10.1123/jsr.2018-0389
Ko G. W. Y., Clarkson C. (2020). The effectiveness of acupuncture for pain reduction in delayed-onset muscle soreness: A systematic review. Acupunct. Med. 38 (2), 63–74. doi:10.1177/0964528419887978
Koh H. W., Cho S. H., Kim C. Y., Cho B. J., Kim J. W., Bo K. H. (2013). Effects of vibratory stimulations on maximal voluntary isometric contraction from delayed onset muscle soreness. J. Phys. Ther. Sci. 25 (9), 1093–1095. doi:10.1589/jpts.25.1093
Lau W. Y., Nosaka K. (2011). Effect of vibration treatment on symptoms associated with eccentric exercise-induced muscle damage. Am. J. Phys. Med. Rehabil. 90 (8), 648–657. doi:10.1097/PHM.0b013e3182063ac8
Lee Y. S., Bae S. H., Hwang J. A., Kim K. Y. (2015). The effects of kinesio taping on architecture, strength and pain of muscles in delayed onset muscle soreness of biceps brachii. J. Phys. Ther. Sci. 27 (2), 457–459. doi:10.1589/jpts.27.457
Lu X., Wang Y., Lu J., You Y., Zhang L., Zhu D., et al. (2019). Does vibration benefit delayed-onset muscle soreness?: A meta-analysis and systematic review. J. Int. Med. Res. 47 (1), 3–18. doi:10.1177/0300060518814999
Pumpa K. L., Fallon K. E., Bensoussan A., Papalia S. (2011). The effects of Lyprinol(®) on delayed onset muscle soreness and muscle damage in well trained athletes: A double-blind randomised controlled trial. Complement. Ther. Med. 19 (6), 311–318. doi:10.1016/j.ctim.2011.08.004
Pupo J. D., Kons R. L., Gheller R. G., Costa F. E., Vecchia L. D., Detanico D. (2021). Neuromuscular impairment after high-intensity running and vertical jump exercise protocols. Isokinet. Exerc Sci. 29 (4), 361–367. doi:10.3233/IES-210129
Saki F., Romiani H., Ziya M., Gheidi N. (2022). The effects of gluteus medius and tibialis anterior kinesio taping on postural control, knee kinematics, and knee proprioception in female athletes with dynamic knee valgus. Phys. Ther. Sport. 53, 84–90. doi:10.1016/j.ptsp.2021.11.010
Song W., Yang Y. (2022). Effect of Kinesio taping on delayed-onset muscle soreness in elite athletes. J. Sports Med. Phys. Fit. 62 (5), 667–672. doi:10.23736/S0022-4707.21.12280-7
Sonkodi B., Kopa Z., Nyirády P. (2021). Post orgasmic illness syndrome (POIS) and delayed onset muscle soreness (DOMS): Do they have anything in common? Cells 10 (8), 1867. doi:10.3390/cells10081867
Torre M. F., Martinez-Ferran M., Vallecillo N., Jiménez S. L., Romero-Morales C., Pareja-Galeano H. (2021). Supplementation with vitamins C and E and exercise-induced delayed-onset muscle soreness: A systematic review. Antioxidants (Basel) 10 (2), 279. doi:10.3390/antiox10020279
Tran L., Makram A. M., Makram O. M., Elfaituri M. K., Morsy S., Ghozy S., et al. (2021). Efficacy of kinesio taping compared to other treatment modalities in musculoskeletal disorders: A systematic review and meta-analysis. Res. Sports Med. 2021, 1–24. doi:10.1080/15438627.2021.1989432
Turgut E., Can E. N., Demir C., Maenhout A. (2021). Evidence for taping in overhead athlete shoulders: A systematic review. Res. Sports Med. 21, 1–30. doi:10.1080/15438627.2021.1988950
Keywords: delayed-onset muscle soreness, kinesio taping, vibration treatment, pain, muscular strength
Citation: Que N (2023) Effect of kinesio taping in combination with vibration treatment on college students’ delayed-onset muscle soreness. Front. Physiol. 14:1058637. doi: 10.3389/fphys.2023.1058637
Received: 30 September 2022; Accepted: 17 January 2023;
Published: 25 January 2023.
Edited by:
Qipeng Song, Shandong Sport University, ChinaCopyright © 2023 Que. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ning Que, bmluZ3F1ZWNkc2NAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.