 Min Zhao
Min Zhao Shuyu Yang3,4†
Shuyu Yang3,4† Xiaojie Su
Xiaojie Su Tzu-Chieh Hung
Tzu-Chieh Hung
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 11 July 2022
Sec. Metabolic Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.938149
Background & Aims: Hepatitis B virus (HBV) infection is a significant cause of liver function damage. However, previous studies on HBV mainly aimed at ordinary people, and there is a lack of consensus on the relationship between HBV infection and gestational diabetes mellitus (GDM) and whether HBV-infected pregnant women should undergo antiviral treatment. In addition, systematic studies on the impact of HBV infection on GDM have rarely been studied directly. Therefore, the overall goal of this study was to pursue the association between HBV infection, liver function, and GDM using Xiamen area gestational big data.
Methods: Using the Xiamen Primary Health Information System-maternal and child health information system, the data on participants (138,867 in total) expected confinement between 2008 and 2018 were included. Using univariate and multivariate logistic regressions, we constructed models to determine the role of HBV infection and liver function status in GDM. In addition, an analysis of variance tests was performed to study whether the relationship between HBsAg and GDM differed in the normal liver function and the abnormal liver function subgroups.
Results: HBsAg's positive status showed a substantial correlation with GDM onset in univariate and multivariate logistic regressions (p < 0.001). Subgroup analysis among HBsAg, liver function, and GDM suggests that both HBsAg and liver function affect the onset of GDM and have the highest prevalence of both abnormalities. Furthermore, ANOVA was used to investigate the association of HBsAg positive (p < 0.001), abnormal liver function (p < 0.001), and their interaction (p = 0.302) on the onset of GDM. This result showed that HBsAg is an independent factor of GDM pathogenesis, regardless of liver function status.
Conclusion: HBsAg and liver function are independent factors in GDM. Therefore, regarding these results, while clinicians consider the traditional risk factors of GDM, it is necessary to consider the HBV infection status. Conducting a dietary intervention for HBsAg-positive pregnant women at the early stage of pregnancy is conducive to reducing the adverse effects.
Gestational diabetes mellitus (GDM) was defined as any degree of glucose intolerance that was first recognized during pregnancy, regardless of hyperglycemia (Zhang et al., 2010). The incidence of GDM has shown an upward trend recently, approaching the incidence of type 2 diabetes and obesity. According to reports, the incidence of gestational diabetes is about 16–18% (Musilova et al., 2012) and about 7.7% in China (Atlas, 2015).
The pathogenesis of GDM is not entirely understood. From an evolutionary point of view, placental hormone secretion antagonizes insulin action in the medium and later term of pregnancy, which leads to physiological increase in insulin resistance. This mechanism is designed to limit maternal glucose utilization and thereby shunt an adequate amount of supply to the growing fetus (Hay, 2006). When maternal insulin secretion cannot compensate for pregnancy-induced insulin resistance, it leads to maternal hyperglycemia, which causes severe complications of GDM and obesity (Kampmann et al., 2019). GDM carries risks for the mother, fetus, and neonate. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study demonstrated that the risk of adverse maternal, fetal, and neonatal outcomes continuously increased as a function of maternal glycemia at 24–28 weeks of gestation, even within ranges previously considered normal for pregnancy (Metzger et al., 2008). Therefore, early diagnosis of gestational diabetes and lifestyle interventions for high-risk pregnant women can reduce the risk of gestational diabetes and reduce adverse outcomes. However, the current clinical diagnosis of gestational diabetes is mainly based on oral glucose tolerance tests at 24–28 weeks of pregnancy, which brings difficulties to early diagnosis and highlights the importance of screening and close follow-up in the high-risk group such as older or obese pregnant women.
Hepatitis B virus (HBV) infection is one of the most prevalent infectious diseases, affecting about two billion people worldwide, among which about 5% of pregnant women have chronic HBV infection (Li et al., 2011). HBV infection is a routine screening program for pregnant women, with a view to early detection of pregnant women with abnormal liver function caused by HBV replication or pregnant women with high virus load prone to mother-to-child transmission. HBV infection is associated with multiple pregnancy complications, such as spontaneous preterm birth and habitual abortion (Atalay et al., 2016). In addition, previous studies have also reported that HBV could continuously destroy islet cells, causing insulin secretion deficiency to induce GDM (Shetty et al., 2000; Kim et al., 2012; Rawat and Boucharf, 2015; Barthel et al., 2016). A study has shown that the incidence of diabetes in patients with chronic liver disease is significantly higher than that in the healthy population (Rouabhia et al., 2010). However, the association between HBV infection and GDM remains inconclusive, especially in HBV-infected pregnant women with a normal liver function who were often overlooked in clinical practice.
HBV infection is a significant cause of liver function damage. The liver is the principal organ to secrete bile and store glycogen and vital in maintaining blood sugar stability. Changes in maternal hormone levels and the immune status during pregnancy can affect HBV the infection status, affect liver function, aggravate glucose metabolism disorders, and affect the course of pregnancy. However, previous studies on HBV are primarily aimed at ordinary people, and there is a lack of consensus on the relationship between HBV infection and GDM and whether HBV-infected pregnant women should undergo antiviral treatment. Although the vertical transmission of HBV from the mother to the child has been effectively controlled with the widespread use of the hepatitis B vaccine, systematic studies on the impact of HBV infection on GDM have rarely been studied directly. Therefore, the overall goal of this study was to pursue the association between HBV infection, liver function, and GDM using Xiamen area gestational big data.
This retrospective cohort study was conducted under the ethical guidelines of the Declaration of Helsinki and was approved by the review board of the First Affiliated Hospital of Xiamen University. The participants whose expected date of confinement was between 2008 and 2018 were collected in this study using the area population-based clinical data from the Xiamen Primary Health Information System-maternal and child health information system. This system is a governmental data warehouse, established and managed by the Xiamen Municipal Health Committee. It consisted of the public life-cycle medical information collected from 28 primary medical institutions in Xiamen, including birth, adolescence, childbearing, menopause, and old age. The inclusion criteria accepted in the present study were as follows: 1) aged below 40 years old; 2) BMI under 28; and 3) no history of a previous diabetes diagnosis. The exclusion criteria were as follows: the person was unconscious or had critically ill, learning difficulties, or severe mental illness, and the fetus had an abnormal ultrasound result.
The GDM diagnostic criteria used in this study were the International Association of Diabetes and Pregnancy Study Group (IADPSG) standard. Pre-gestational diabetes mellitus (PGDM) patients are excluded before the 75 g OGTT. The fasting plasma glucose level, 1-h, and 2-h blood glucose levels after the oral glucose admission were measured. The typical blood glucose values should be less than 5.1 mmol/L, 10.0 mmol/L, and 8.5 mmol/L (92, 180, and 153 mg/dl). A diagnosis of GDM occurs when any blood glucose level meets or exceeds the criteria.
The HBsAg status inclusion criteria for this study were as follows: maternal HBV infection (prenatal screening HBsAg positive). The normal interval of the liver function indicators is defined as follows: ALT [5, 40] U/L, AST [0, 40] U/L, ALB [35, 50] g/L, TBil [3.4, 20.5] μmol/L, and DBil [0, 6.84] umol/L.
The following clinical variables of patients were included and analyzed: alcohol, cardiopathy, pneumopathy, hypertension, smoking, epilepsy, hyperthyroidism, nephropathy, hematopathy, family diabetes history, folic acid consumption, menarche age, hemoglobin (HBG), white blood count (WBC), platelet count (PLT), serum creatinine (SCr), blood urea nitrogen (BUN), body mass index (BMI), age, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (ALB), total bilirubin (TBil), direct bilirubin (DBil), international normalized ratio (INR), and hepatitis B surface antigen (HBsAg). In addition, according to the liver function test, the patients were further classified into liver function normal and abnormal cohorts to investigate the association between the HBV status, liver function status, and diagnosis of GDM. The definition of the abnormal liver function status accepted in the present study was defined as the patients who harbored any abnormal liver function indicators, such as liver enzymes, bilirubin, albumin, and INR.
An extract-transform-load process was performed through SQL server 2008 R2 database software (Microsoft), and the patients’ data containing missing indistinct values were excluded. As a result, 0.25% of extreme data at both ends were truncated; thus, 99.5% of the remaining data were investigated (Figure 1).
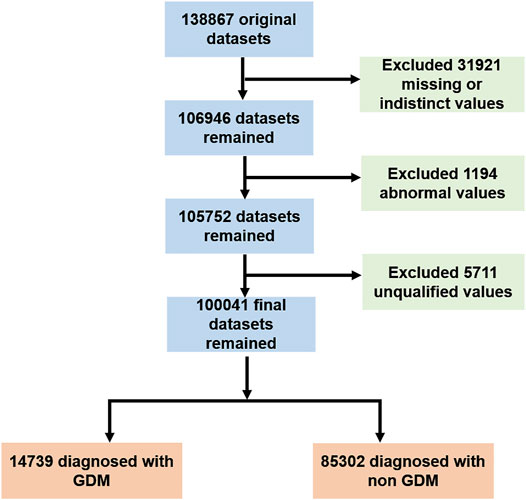
FIGURE 1. Selection of the study population.
Continuous data were expressed as the mean and standard deviation (SD) and were analyzed using t-tests. Categorical data were presented as count and percentage and were compared using Pearson’s chi-squared tests. Univariate and multivariate logistic regressions were applied to determine the role of HBV infection and liver function status in GDM. In order to further study whether the relationship between HBsAg and GDM was different in the normal liver function and the abnormal liver function subgroups, analysis of variance (ANOVA) tests were performed.
All statistical tests were two-sided, made at a 5% significance level, and performed using R version 4.1.1 (R Project, Vienna, Austria).
A total of 100,041 pregnant women who met the inclusion and exclusion criteria were included in the present study (as shown in Figure 1). The baseline characteristics of the total cohort and the comparison of clinical variables between HBsAg positive and negative cohorts are shown in Table 1. The result showed that the positive HBsAg cohort was significantly associated with a high proportion of GDM (p < 0.001), while the other variables were not statistically significant between these two cohorts.
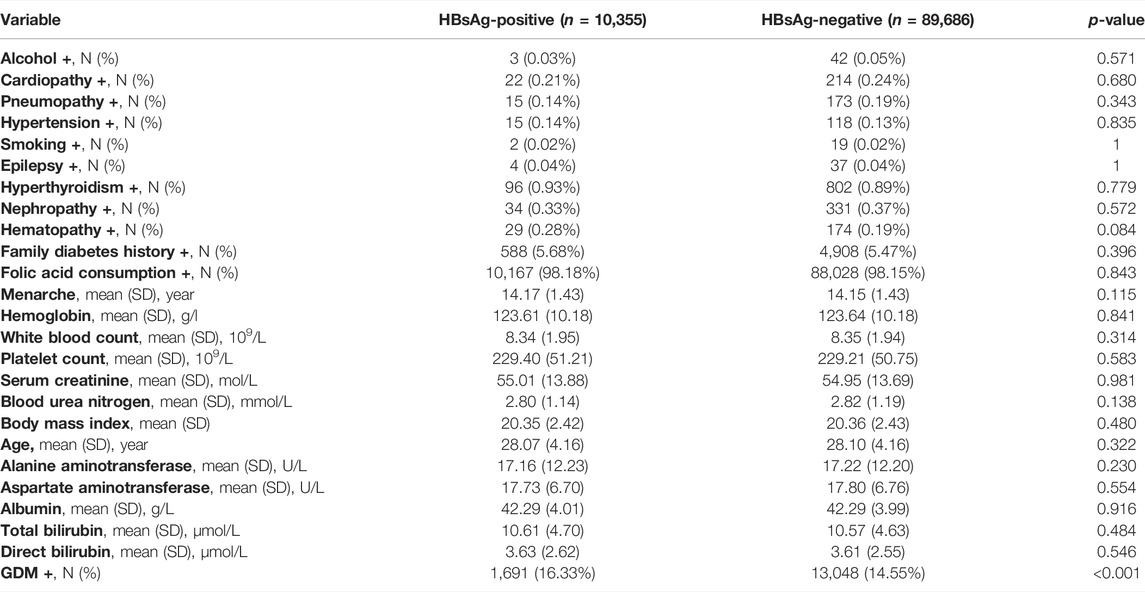
TABLE 1. Baseline characteristics in HBsAg-negative and -positive groups.
As shown in Table 2, univariate logistic regression analysis identified that 15 variables were associated with GDM diagnosis (both p < 0.05), among which the HBsAg positive status was positively associated with GDM (odds ratio [OR] with 95% confidence interval [CI] = 1.147 [1.086–1.212]; p < 0.001). The further multivariate logistic analysis identified that the HBsAg status remained as the independent risk factor for GDM after the correction of other confound variables (odds ratio [OR] with 95% confidence interval [CI] = 1.174 [1.167–1.180]; p < 0.001). In addition to the significant correlation between the HBsAg status and GDM onset, the result of the present study was that several liver function indicators, such as high levels of AST, ALT, and TBIL, showed a substantial correlation with GDM onset in both uni- and multivariate analyses as well.
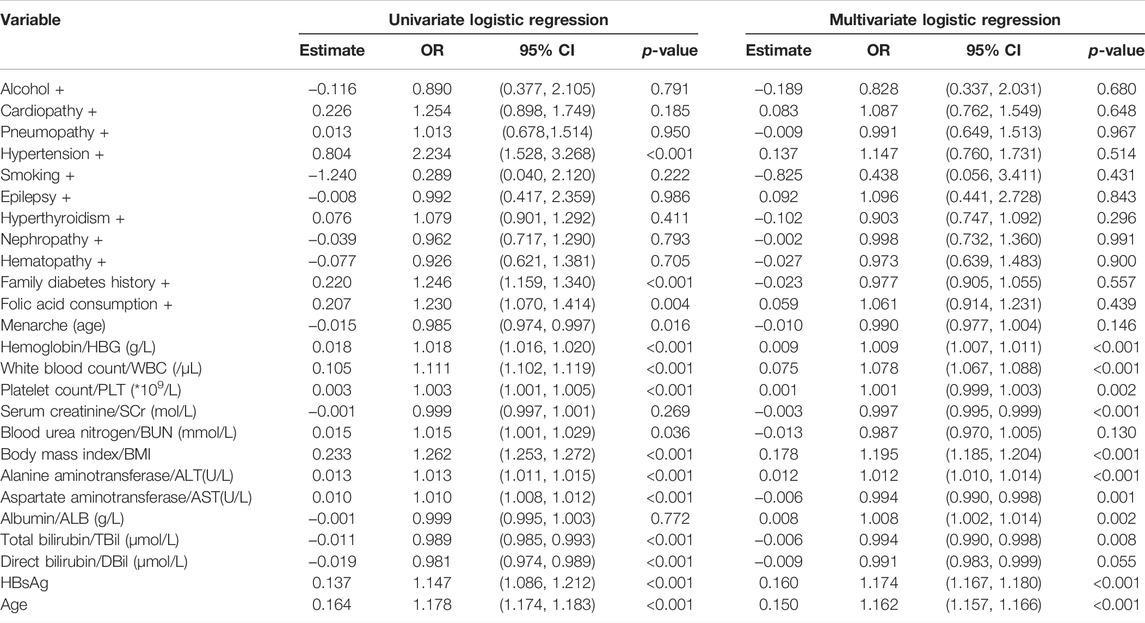
TABLE 2. Univariate and multivariate logistic regressions in GDM populations.
We further analyzed the data into two groups to investigate the relationship between the prevalence of GDM and HBV infection in the normal liver function and abnormal liver function groups.
The results showed a positive correlation between HBsAg and GDM, regardless of liver function. In the group with abnormal liver function, the prevalence of GDM in HBsAg-positive pregnant women was 18.38%; for HBsAg-negative pregnant women, it was 15.78%. In the group with normal liver function, the prevalence of GDM in HBsAg-positive pregnant women was 15.90%, and for HBsAg negative pregnant women, it was 14.30% (Table 3).

TABLE 3. GDM prevalence in different groups.
Interestingly, the prevalence of GDM showed a step-by-step increase with the liver function status and HBsAg status. The prevalence ranged from 14.30 to 18.38% (Figure 2). This result suggests that both HBsAg and the liver function affect the onset of GDM and have the highest prevalence of both abnormalities.
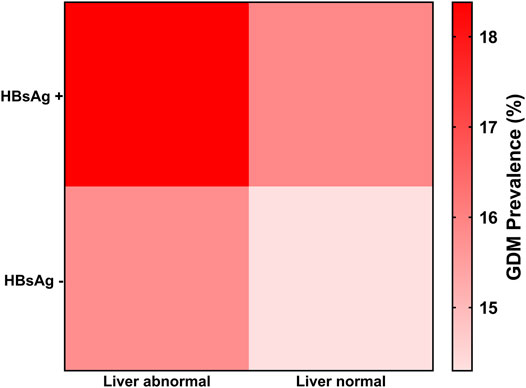
FIGURE 2. GDM prevalence in live function normal and abnormal groups.
Furthermore, ANOVA was used to investigate the association of HBsAg-positive status (p < 0.001), abnormal liver function (p < 0.001), and their interaction with the onset of GDM. The results showed that both factors were statistically significantly associated with GDM onset. However, the combined interaction (p = 0.302) was not statistically significant with GDM onset (Table 4). It shows that abnormal liver function and HBsAg-positive status are independent factors of GDM.

TABLE 4. Variance analysis of HBsAg, liver function, and their interaction on the onset of GDM.
Our previous study (Zhao et al., 2021) identified eight independent pre-/early-pregnancy predictors, namely, pre-pregnancy BMI, pre-pregnancy intake of folic acid, white cell count, platelet count, alanine transaminase, albumin, direct bilirubin, and creatinine, which were significantly associated with the later GDM risk. Moreover, we established a nomogram model with these predictors, which had an over-roll of 85% accuracy in early detection of GDM progress based on the pregnant women’s clinical data from the Xiamen Primary Health Information System-maternal and child health information system.
Our results showed a statistically significant association of liver function indicators with GDM disease in the present study. ALT and AST are the primary indicators of the evaluation of liver function. The results showed that ALT and AST in the GDM group were significantly higher than in the non-GDM group. HBV virus infection carries liver injury as the primary clinical symptom. In glycogenolysis, glucose polymers are stored in the liver glycogen. In glycolysis, glycogen can be decomposed into glucose and converted into energy. The synthesis and degradation of liver glycogen are controlled by insulin. Under normal conditions, the body can synthesize and degrade liver glycogen. HBV virus infection can cause hepatocyte necrosis and inflammatory cell infiltration. This phenomenon is pronounced under high viral load HBV infection (active virus period)–induced liver damage; liver glycogen synthesis damage can cause elevated blood sugar levels. Some scholars believe that autoimmune pancreatitis caused by high load HBV virus infection leads to autoantibodies against insulin cells and is the critical factor of GDM (Spardling et al., 2013; Sarkar and NorahTerrault, 2014). Bilirubin acts as a biochemical antioxidant to inhibit radical oxygen formation and lipid oxidation, and it also inhibits inflammatory and immune responses (Mark, 2013). HBV may be interfering with glucose homeostasis through insulin sensitivity. This effect may have bypassed the protective mechanism of the antioxidants. Barthel’s result shows that HBV induces activation of nuclear factor erythroid 2 related factors 2 (Nrf2), which causes intracellular retention of the Insulin receptor (INSR), reducing cell surface functional INSR, further induces the weakening of insulin binding, and causes insulin signaling inhibition (Barthel et al., 2016). Kim’s research demonstrated that the six trans-membrane protein of prostate 2 (STAMP2) protein physically interacts with and decreases the hepatitis B virus X protein (HBx) stability, thereby counteracting HBx-induced hepatic lipid accumulation and insulin resistance (Kim et al., 2012). In addition, recent studies have found that HBX interferes with the host cell PI3K/Akt insulin signaling pathway, leading to impaired insulin signaling transduction and a decline in liver cell glycogen synthesis, and elevated blood glucose concentration (Rawat and Boucharf, 2015).
Our results showed that HBsAg was an independent factor in GDM. HBV-induced liver injury is usually accompanied by different degrees of pancreas injury. Some basic tissue embryology research (Shetty et al., 2000) shows that the liver and pancreas have the exact embryonic origin and similar tissue structures. HBV virus also has a solid affinity for pancreatic tissue. HBV virus particles can be found in pancreatic biopsy in some patients with cirrhosis. Studies have shown that (Sirilert et al., 2014) patients with severe HBV infection and cirrhosis can have increased insulin resistance, and some patients can have abnormal glucose metabolism. Pregnant women with HBV virus infection can lead to islet beta-cell injury, and the decrease of insulin secretion directly induces gestational diabetes mellitus.
Our results further suggest that HBsAg is an independent factor of GDM pathogenesis, regardless of the liver function status. Liver function and HBV interaction did not have a statistical significance with GDM.
Our result demonstrates that pregnant women infected by HBV, regardless of their liver function status, are more vulnerable to GDM. Therefore, we recommend that clinicians and policymakers consider health management strategies for HBV-infected pregnant women at the early stage of their pregnancy. MNT has been widely used in clinical practice (Erkamp et al., 2020; Liu et al., 2020). MNT determines the medical and nutritional treatment program through high-risk screening of pregnant women and changes unhealthy lifestyles through nutrition education during pregnancy, individualized blood sugar levels, and weight management. The content of the MNT protocol includes diet and physical exercise, and it is a clinical non-pharmacological therapeutic intervention for pregnant women with GDM. Badon’s study has suggested the management of an unhealthy lifestyle in early pregnancy, including diet, physical exercise, smoking cessation, and stress management. This study believes that earlier health management of blood sugar, blood fats, and body weight during pregnancy can reduce the risk of pregnancy-associated syndromes such as GDM (Badon et al., 2018). In addition, MNT programs, including dietary and exercise intervention protocols, are beneficial in reducing the risk of complications of GDM from the glucose control disorder during pregnancy (Cosson et al., 2017).
A significant limitation is that the hepatitis B vaccine–inoculated groups were not excluded in this study, requiring further investigation. In terms of current practice, the present study is a local, regional study using IADPSG criteria to define GDM, which, although recommended by the World Health Organization (WHO, 2013), is not universally adopted (NICE, 2015). Glycohemoglobin is a critical reference parameter for diagnosing gestational diabetes mellitus (Powe, 2017); this study’s lack of glycohemoglobin data is also a deficiency.
In conclusion, this study demonstrates an association between HBsAg and an increased risk of gestational diabetes mellitus, regardless of the liver function status, which may have implications for the clinical diagnosis and treatment of GDM: intensive follow-up for GDM should be required for HBV-infected patients with or without liver function damage. Regarding these results, while clinicians consider the traditional risk factors of GDM, it is necessary to consider the HBV infection status. Conducting an MNT or undergoing antiviral treatment for HBsAg-positive pregnant women at the early stage of pregnancy is conducive to reducing the adverse effects.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
MZ and SY: protocol/project development. MZ and YL: data collection or management. XS and T-CH: data analysis. WZ: manuscript writing/editing.
This study is granted by the Natural Science Foundation of Fujian Province, China (Grant No. 2019J01571).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank all the doctors, nurses, technicians, and patients involved at our center for their dedication to the study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2022.938149/full#supplementary-material
Atalay E., Cenk G., Cuneyt Eftal T., Ozeren M. (2016). The Effect of Associated Structural Malformations in the Prediction of Chromosomal Abnormality Risk of Fetuses with Echogenic Bowel. J. Maternal-Fetal Med., 41–45.
Badon S. E., Miller R. S., Qiu C. (2018). Maternal Healthy Lifestyle during Early Pregnancy and Offspring Birthweight: Differences by Off-Spring Sex. J. Matern. Fetal Neonatal Med. 31 (9), 1111–1117. doi:10.1080/14767058.2017.1309383
Barthel S. R., Medvedev R., Heinrich T., Büchner S. M., Kettern N., Hildt E. (2016). Hepatitis B Virus Inhibits Insulin Receptor Signaling and Impairs Liver Regeneration via Intracellular Retention of the Insulin Receptor. Cell. Mol. Life Sci. 73 (21), 4121–4140. doi:10.1007/s00018-016-2259-1
Cosson E., Baz B., Gary F. (20172017). Poor Reliability and Poor Adherence to Self-Monitoring of Blood Glucose Are Common in Women with Gestational Diabetes Mellitus and May Be Associated with Poor Pregnancy Outcomes. Diabetes Care 40 (9), 1181–1186. doi:10.2337/dc17-0369
Erkamp J. S., Geurtsen M. L., Liesbeth D. (20202020). Associations of Maternal Early-Pregnancy Glucose Concentrations with Placental Hemo-Dynamics, Blood Pressure, and Gestational Hypertensive Disorders. Am. J. Hypertens. 33 (7), 660–669. doi:10.1093/ajh/hpaa070
Hay W. (20062006). Placental-fetal Glucose Exchange and Fetal Glucose Metabolism. Trans. Am. Clin. Climatol. Assoc. 117, 321–340.
Kampmann U., Knorr S., Fuglsang J. (2019). Determinants of Maternal Insulin Resistance during Pregnancy: An Updated over Review. J. Diabetes Res. 20192019, 5320156. doi:10.1155/2019/5320156
Kim H. Y., Cho H. K., Yoo S. K., Cheong J. H. (2012). Hepatic Stamp2 Decreases Hepatitis B Virus X Protein-Associated Metabolic Deregulation. Exp. Mol. Med. 44, 622–632. doi:10.3858/emm.2012.44.10.071
Li K., Wang Y., Li H., Yang H. (2011). A Study of 579 Pregnant Women with Premature Rupture of Membranes at Term. Int. J. Gynaecol. obstetrics official organ Int. Fed. Gynaecol. Obstetrics 112 (1), 45–47. doi:10.1016/j.ijgo.2010.07.026
Liu B., Cai J., Xu Y. (20202020). Early Diagnosed Gestational Diabetes Melli- Tus Is Associated with Adverse Pregnancy Outcomes: a Prospective Cohort Study. J. Clin. Endocrinol. Metab. 105 (12), dgaa633. doi:10.1210/clinem/dgaa633
McCarty M. F. (2013). Serum Bilirubin May Serve as a Marker for Increased Heme Oxygenase Activity and Inducibility in Tissues – A Rationale for the Versatile Health Protection Associated with Elevated Plasma Bilirubin. Med. Hypotheses (4). doi:10.1016/j.mehy.2013.07.013
Metzger B. E., Lowe L. P., Dyer A. R. (20082008). HAPO Study Cooperative Research Group. Hyperglycemia and Adverse Pregnancy Outcomes. N. Engl. J. Med. 358, 1991–2002. doi:10.1056/NEJMoa0707943
Musilova I., Kacerovsky M., Hornychova H., Kostal M., Jacobsson B. O. (2012). Pulsation of the Fetal Splenic Vein-Aa Potential Ultrasound Marker of Histological Chorioamnionitis and Funisitis in Women with Preterm Prelabor Rupture of Membranes. Acta Obstetricia Gynecol. Scand. 91 (9), 1119–1123. doi:10.1111/j.1600-0412.2012.01450.x
NICE guidelines (2015). Diabetes in Pregnancy: Management of Diabetes and its Complications from Preconception to the Postnatal Period, 2015.
Powe C. E. (20172017). Early Pregnancy Biochemical Predictors of Gestational Diabetes Mellitus. Curr. Diab Rep. 17, 12. doi:10.1007/s11892-017-0834-y
Rawat S., Bouchard Michael J. (2015). The Hepatitis B Virus (HBV) HBx Protein Activates AKT to Simultaneously Regulate HBV Replication and Hepatocyte Survival. J. virology (2). doi:10.1128/JVI.02440-14
Rouabhia S., Malek R., Bounecer H., Dekaken A., Amor F. B., Sadelaoud M. (2010). Prevalence of Type 2 Diabetes in Algerian Patients with Hepatitis C Virus Infection. World J. Gastroenterology 16 (27), 3427–3431. doi:10.3748/wjg.v16.i27.3427
Sarkar M. M. D., NorahTerrault A. M. D. (2014). Ending Vertical Transmission of Hepatitis B: The Third Trimester Intervention. Hepatology 2. doi:10.1002/hep.27145
Shetty A., Wilson S., Kuo P., Laurin J. L., Allen E. M. (2000). Liver Transplantation Improves Cirrhosis-Associated Impaired Oral Glucose Tolerance. Transplantation 69 (11), 2451–2454. doi:10.1097/00007890-200006150-00043
Sirilert S., Traisrisilp K., Sirivatanapa P., Tongsong T. (2014). Pregnancy Outcomes Among Chronic Carriers of Hepatitis B Virus. Int. J. Gynecol. Obstetrics 126 (2), 106–110. doi:10.1016/j.ijgo.2014.02.019
Spradling P. R., Simons B., Narayanan M., Xing J., Mcmahon B. J. (2013). Incidence of Diabetes Mellitus in a Population-Based Cohort of Persons with Chronic Hepatitis B Virus Infection. J. Viral Hepat. 20 (7), 510–513. doi:10.1111/jvh.12071
WHO (2013). “Guidelines Approved by the Guidelines Review Committee,” in Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy (Geneva: World Health Organization), 2013.
Zhang X., Gregg E. W., Williamson D. F. (20102010). A1C Level and Future Risk of Diabetes: a Systematic Review. Diabetes Care 33, 1665–1673. doi:10.2337/dc09-1939
Keywords: GDM, HBV, liver, retrospective, big data
Citation: Zhao M, Yang S, Su X, Hung T-C, Liu Y and Zheng W (2022) Hepatitis B Virus Infection and Increased Risk of Gestational Diabetes Regardless of Liver Function Status: A Xiamen Area Population-Based Study. Front. Physiol. 13:938149. doi: 10.3389/fphys.2022.938149
Received: 07 May 2022; Accepted: 06 June 2022;
Published: 11 July 2022.
Edited by:
Chun Yang, Nanjing Medical University, ChinaReviewed by:
Zhenyu Lin, Fuzhou University, ChinaCopyright © 2022 Zhao, Yang, Su, Hung, Liu and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Zhao, eG16bWR5eXlAeG11LmVkdS5jbg==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.