
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Physiol. , 30 August 2022
Sec. Redox Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.935269
This article is part of the Research Topic Ozone in Medicine: Biochemical Background, Physiological Modulation and Clinical Applications View all 5 articles
 Bernardino Clavo1,2,3,4,5,6,7,8,9*
Bernardino Clavo1,2,3,4,5,6,7,8,9* Delvys Rodríguez-Abreu10Saray Galván11Mario Federico3
Delvys Rodríguez-Abreu10Saray Galván11Mario Federico3 Gregorio Martínez-Sánchez12Yolanda Ramallo-Fariña4,7,13Carla Antonelli11Gretel Benítez10Dolores Rey-Baltar3Ignacio J Jorge2
Gregorio Martínez-Sánchez12Yolanda Ramallo-Fariña4,7,13Carla Antonelli11Gretel Benítez10Dolores Rey-Baltar3Ignacio J Jorge2 Francisco Rodríguez-Esparragón1,4,6,8*Pedro Serrano-Aguilar7,13,14,15
Francisco Rodríguez-Esparragón1,4,6,8*Pedro Serrano-Aguilar7,13,14,15Background: Pain secondary to chemotherapy-induced peripheral neuropathy (CIPN) can limit the administration of chemotherapy, cancer-treatment outcomes, and the quality of life of patients. Oxidative stress and inflammation are some of the key mechanisms involved in CIPN. Successful treatments for CIPN are limited. This report shows our preliminary experience using ozone treatment as a modulator of oxidative stress in chronic pain secondary to CIPN.
Methods: Ozone treatment, by rectal insufflation, was administered in seven patients suffering from pain secondary to grade II or III CIPN. Pain was assessed by the visual analog scale (VAS).
Results: All patients, except one, showed clinically relevant pain improvement. Median pain score according to the VAS was 7 (range: 5–8) before ozone treatment, 4 (range: 2–6) at the end of ozone treatment (p = 0.004), 5.5 (range: 1.8–6.3) 3 months after the end of ozone treatment (p = 0.008), and 6 (range: 2.6–6.6) 6 months after the end of ozone treatment (p = 0.008). The toxicity grade, according to the Common Terminology Criteria for Adverse Events (CTCAE v.5.0), improved in half of the patients.
Conclusion: This report shows that most patients obtained clinically relevant and long-lasting improvement in chronic pain secondary to CIPN after treatment with ozone. These observed effects merit further research and support our ongoing randomized clinical trial (NCT04299893).
Chemotherapy-induced peripheral neuropathy (CIPN) is one of the most relevant side effects of chemotherapy. Its presentation before the end of chemotherapy (more frequent for oxaliplatin and paclitaxel) can lead to the delay, reduction, or even interruption of the initially planned scheme of chemotherapy, with potential decreases in tumor control. On the other hand, chronic CIPN weeks or months after the end of chemotherapy can lead to persistent impairments in quality of life. CIPN happens in 70–100% of cancer patients after treatment with platinum-based drugs and 19–85% of cancer patients after different neurotoxic chemotherapies (Zajaczkowska et al., 2019). A systematic review and meta-analysis showed a CIPN prevalence of around 2/3 within the first month of the end of chemotherapy with a progressive decrease until 1/3 at 6 months or later (Seretny et al., 2014). Unfortunately, there are no clinically relevant approaches for preventing CIPN and/or treating established CIPN, except for the limited effect described for duloxetine in the treatment of CIPN pain (Smith et al., 2013; Loprinzi et al., 2020; Bae et al., 2021; Zhang, 2021). The development and evaluation of novel strategies to mitigate and manage the chronic side effects of cancer therapy (CIPN included) have been established as urgent areas of research by the American Society of Clinical Oncology (ASCO) (Markham et al., 2020).
The pathomechanism by which chemotherapeutics damage nervous system structures and cause CIPN is multifactorial and involves chronic oxidative stress (OS) and neuroinflammation (Di Cesare Mannelli et al., 2012; Starobova and Vetter, 2017; Shim et al., 2019; Zajaczkowska et al., 2019; Salat, 2020; Bae et al., 2021). Based on those processes, we previously described how ozone can modulate OS and proinflammatory cytokine production as potential mechanisms of action in the prevention and improvement of different chemotherapy-induced toxicities (Clavo et al., 2019) and in CIPN (Clavo et al., 2021a).
The aim of this report was to show our preliminary experience using ozone treatment (O3T) as an adjuvant treatment in the palliative management of patients with chronic pain secondary to CIPN.
Between June 2019 and August 2021, 18 patients with different CIPN symptoms were submitted from Clinical Oncology and Radiation Oncology Departments to our multidisciplinary Chronic Pain Unit to evaluate complementary treatment with O3T. Some patients with mild symptoms were not treated with O3T, and some patients were treated with O3T because of numbness, tingling, or paresthesias without pain. Finally, seven patients were treated with O3T because of chronic and painful grade II or III CIPN. They were two males and five females, with a median age of 49 years old (between 36 and 73 years old). Compassionate ozone treatment in our hospital was assessed by the Health Care Ethics Committee, and this study was approved by the Provincial Research Ethics Committee of Las Palmas, Spain (Ref 2019-288-1). Informed written consent was obtained from all patients. See details in Table 1.
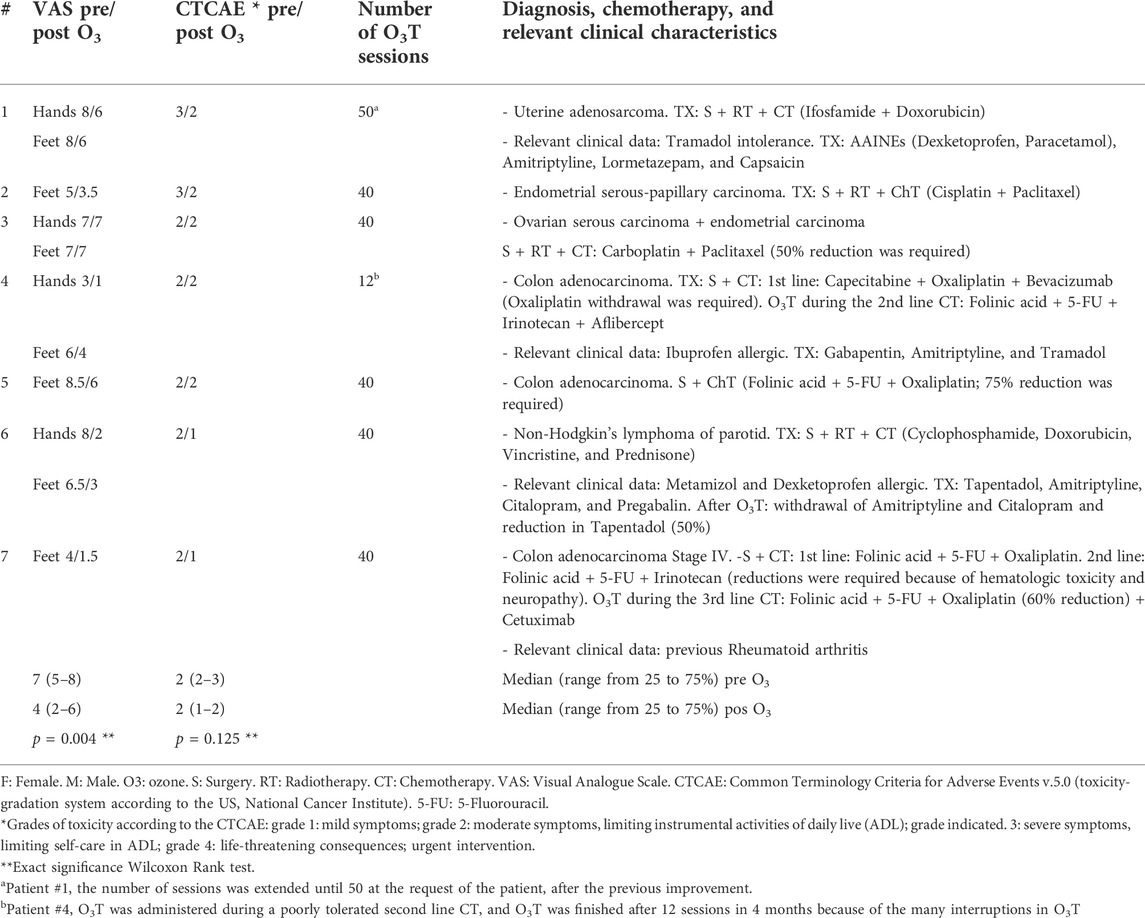
TABLE 1. Clinical characteristics and patient-reported changes in numbness, tingling, pain, and toxicity grade.
Pain, according to the Visual Analog Scale (VAS) ranging from 0 (no pain) to 10 (the worst imaginable pain), was assessed before O3T, at the end of O3T, and at three and 6 months after the end of O3T.
O3T was administered by rectal insufflation on an outpatient basis. Ozone was obtained from clinical-grade oxygen using two medical ozone generators (Ozonosan Alpha-plus®; Dr. Hänsler GmbH, Iffezheim, Germany, and Ozonobaric P, Sedecal, Madrid, Spain). The O3/O2 gas mixture provided by the device was administered via a rectal cannula using standard 60 ml syringes. The initial O3/O2 concentration (in µg/mL: µg of O3 per mL of O2) was 10 μg/ml, and it was increased by 5 μg/ml every two sessions until a final concentration of 30 μg/ml was reached. Typically, for each patient, the gas volume for insufflation started at 180 ml/session and was slowly increased in successive sessions (depending on patient tolerance of bowel bloating) up to a maximum volume of 300 ml/session if tolerated. The initially planned treatment consisted of 40 sessions over 4 months, with three sessions per week during the first 2 months and two sessions per week later, although the final number of O3T sessions could vary according to the clinical evolution.
The SPSS software package (version 15 for Windows) was used for statistical analyses. All data were described as median and range from 25 to 75%. Paired comparisons for quantitative variables were conducted with the exact significance Wilcoxon Rank test. Though more conservative than asymptotic tests, exact tests were used due to the small sample size. p-values of <0.05 were considered statistically significant.
The median duration of O3T was 17 weeks (range from 17 to 17), and the median number of O3T sessions was 40 (range from 40 to 40). One patient commenced with CIPN symptoms 10 months after the end of chemotherapy, and all the other patients commenced with symptoms before the end of chemotherapy. The median time from the initiation of symptoms to the commencement of O3T was 12 months (range from 10 to 48). The median follow-up after the end of O3T was 8 months (range from 6 to 20).
Painful CIPN was independently assessed in 11 different locations, four hands and 7 feet (see Table 1). Six out of the seven patients (86%) reported pain decreases. Initial pain level and pain evolution over time were not necessarily equal in the different locations (hands and feet) for the same patient. In the 11 locations, the median VAS pain score was 7 (range from five to 8) before O3T, 4 (range from two to 6) at the end of O3T (p = 0.004), 5.5 (range from 1.8 to 6.3) 3 months after the end of O3T (p = 0.008), and 6 (range from 2.6 to 6.6) 6 months after the end of O3T (p = 0.008). See Figure 1.
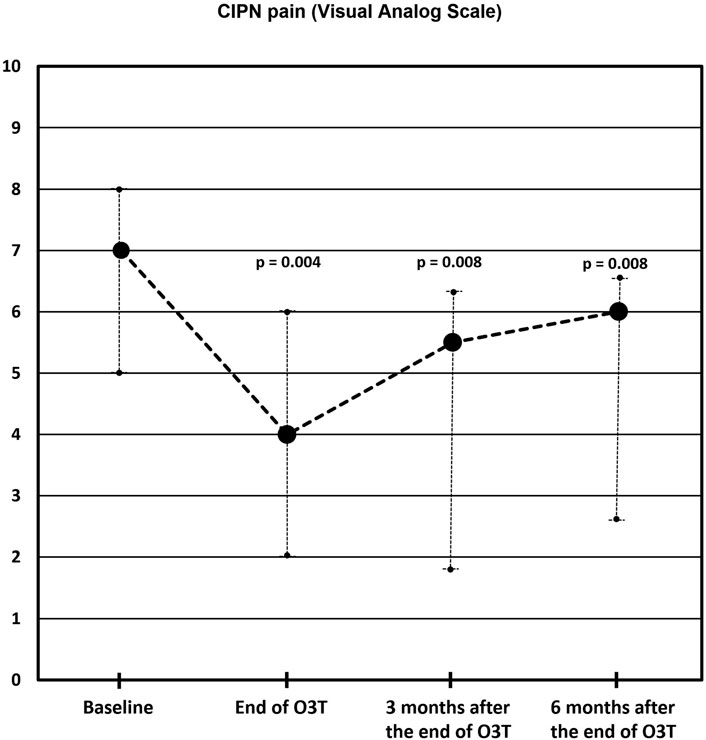
FIGURE 1. Chemotherapy-induced peripheral neuropathy (CIPN) pain according to the Visual Analog Scale (VAS). Compared to the baseline value, the median VAS pain score was significantly lower at the end of O3T (p = 0.004), 3 months (p = 0.008), and 6 months (p = 0.008) after the end of O3T (exact significance Wilcoxon Rank test).
The toxicity grade according to the CTCAE v.5.0 classification decreased in four out of the seven patients (no statically significant).
This preliminary report showed that adjuvant treatment with rectal O3T led to improvement in most patients with chronic pain secondary to CIPN, a frequent side effect of difficult management.
The pathogenesis and perpetuation of CIPN are multifactorial and may vary depending on the used drugs. Multiple involved mechanisms have been described as microtubule disruption, the alteration of calcium homeostasis and ion channel functions, DNA and/or mitochondrial damage, apoptosis, myelin sheath damage, and the induction of reactive oxygen species (ROS) by chemotherapy drugs with the further OS. At the same time, OS is linked to several of these factors, as well as to the induction of pro-inflammatory mediators that lead to immunological and inflammatory alterations (Di Cesare Mannelli et al., 2012; Starobova and Vetter, 2017; Shim et al., 2019; Zajaczkowska et al., 2019; Salat, 2020; Bae et al., 2021). ROS can also activate the apoptotic pathway in neuronal cells through mitochondrial pathway stimulation, including caspase activation (Zajaczkowska et al., 2019).
Recently, we described the potential role of O3T in the modulation of OS and inflammation in CIPN in detail (Clavo et al., 2019; Clavo et al., 2021a). Briefly, low/moderate ozone concentrations administered by rectal insufflation interact with unsaturated fatty acids from cell membranes in the intestinal mucosa. This produces a short and limited OS, with the generation of second messengers (e.g., aldehyde such as 4-hydroxynonenal (4-HNE) and H2O2), and the further and non-specific enhancement of adaptive antioxidant mechanisms, along with the transient upregulation of nuclear factor erythroid 2-related factor 2 (Nrf2). These effects are induced in a hormetic dose–response relationship. Therefore, the ozone effect is an “indirect effect” that does not follow a linear relationship. Significantly low ozone concentrations can have no effect, and significantly high concentrations can lead to undesired effects (Re et al., 2014; Galie et al., 2019; Tricarico and Travagli, 2021; Viebahn-Haensler and Leon Fernandez, 2021). In the same way, moderate physical exercise (not significantly low or high intensity) also induces temporal and soft increases in OS that lead to enhancements of antioxidant defense mechanisms and the regulation of OS (Kruk et al., 2019), with potential benefits for the prevention (Kleckner et al., 2018) and treatment (Kneis et al., 2019; Dhawan et al., 2020) of CIPN in randomized clinical trials. Both O3T and physical exercise share this hormetic dose-response based on the redox-activation of the nuclear factor erythroid 2-related factor 2 (Nrf2) (Re et al., 2014; Galie et al., 2019; Calabrese and Kozumbo, 2021; Viebahn-Haensler and Leon Fernandez, 2021). In addition, it has been demonstrated in animal models that O3T reduces the expressions of caspase-1-3-9 (Guclu et al., 2016) or normalizes mRNA caspase-1, caspase-12, and caspase-8 gene levels (Fuccio et al., 2009). Moreover, O3T inhibits autophagy of nerve root cells by decreasing cleaved caspase-3 expression, suppresses light chain 3B (LC3B) and Beclin one expression, decreases phosphodiesterase 2A and NF-kB p65 expression, and reduces nerve apoptosis by blocking the NF-kB signaling pathway (Wu et al., 2018).
Several other potential treatments based on the exogenous administration of antioxidants (e.g., acetylcysteine, amifostine, glutathione, vitamin E, and calmangafodipir) have been evaluated for the prevention or treatment of CIPN, although without conclusive results to date (Loprinzi et al., 2020). Overall, a potential explanation for the inconclusive results could be that those studies have been based on the increase of “only one” antioxidant or the use of a drug enhancing “only one step” in the overall and complex antioxidant defense mechanisms of the body. In contrast, as stated above, an appropriate ozone concentration can produce a limited (in magnitude and duration) and non-specific OS that is able to activate Nrf2 and induce an “overall” enhancement of the antioxidant defense mechanisms and the modulation of inflammatory cytokines all over the body. Once they are enhanced, some tissues could use them to palliate some pro-oxidative status (at the systemic or local level) as those associated with the side effects of radiotherapy (Clavo et al., 2005; Clavo et al., 2011; Clavo et al., 2013a), chemotherapy (Clavo et al., 2019), or CIPN. Additionally, we have described the beneficial effect of ozone treatment in different pain syndromes as refractory headaches (Clavo et al., 2013b), and refractory pelvic pain after cancer treatment (Clavo et al., 2021b), and a recent review has updated the evidence on ozone treatment in pain medicine, especially relevant in knee osteoarthritis and low-back pain (Hidalgo-Tallon et al., 2022).
There are no clinically relevant treatments for painful CIPN (Smith et al., 2013; Loprinzi et al., 2020; Bae et al., 2021; Zhang, 2021). The only agent that has appropriate evidence for the treatment of CIPN pain is duloxetine (60 mg once daily), based on a randomized clinical trial with 231 patients recruited by 10 centers (Smith et al., 2013; Loprinzi et al., 2020). The authors of this study reported a decreased pain of any amount of 59% in the duloxetine group and 38% in the placebo group. However, although the difference was statistically significant (p = 0.003), the magnitude of the improvement was modest, with a mean difference in average pain score of 0.73 (CI: 0.26, 1.20) between the duloxetine (1.06 score improvement) and placebo (0.34 score improvement) groups on a scale from 0 to 10 (Brief Pain Inventory-Short Form). These results show that further strategies for the management of chronic pain secondary to CIPN are required (Smith et al., 2013). This way, research on new approaches for the management of chronic side effects of cancer therapy (painful CIPN included) has been established as urgent area of research by the American Society of Clinical Oncology (Markham et al., 2020).
We highlight three aspects of the observed pain decreases in our study. First, most patients with painful CIPN reported long-term improvement after O3T (86%), even if two of them were treated with O3T during the second or the third line of chemotherapy (patients #4 and #7, respectively). This is more than twice the reported percentage (38%) of patients with improvement in the placebo groups of other studies on pain due to CIPN (Smith et al., 2013). Second, the magnitude of the observed effect (three points at the end of O3T) compared well with the effect described for duloxetine. Third, although the O3T effect decreased over time, it remained clinically relevant 6 months after the end of O3T, which was associated with decreased requirements for pain killer drugs and increased daily living activities. This protracted effect also compared well with the effect described for duloxetine study, which did not address long-term duloxetine treatment beyond 5 weeks, and half of its effect was lost 1 week after the treatment was finished. The longlasting effect of ozone in painful CIPN agrees with the effect of ozone described 9 months after the end of O3T in patients with chronic pelvic pain secondary to radiotherapy (Clavo et al., 2021b), and the effect described years after the end of O3T in patients with refractory hemorrhagic radiation-induced proctitis (Clavo et al., 2013a; Clavo et al., 2015) or refractory headache (Clavo et al., 2013b).
In our study, O3T by rectal insufflations was used instead of the systemic treatment through venous approach because the former has lower risks in cancer patients. Cancer patients with chronic and unresolved problems usually are frail patients. They already have the risk of several complications that could be erroneously attributed to O3T by a venous approach, but harder to be attributed to a rectal approach. On the other hand, after chemotherapy, the conventional venous access is difficult for most of these patients, and in that condition, it is not easy to think in a repetitive punction, several times per week, for several months, for blood extraction and reinfusion. Moreover, many cancer patients are using subcutaneous venous access, placed by the oncologist for chemotherapy administration, and these systems sometimes must be removed because of infection or thrombosis that we would not like to be attributed to ozone treatment.
The main side effect of O3T was found to be meteorism and bowel bloating secondary to gas insufflation, which usually disappeared after gas release by the patient and matches the results of previous reports (Clavo et al., 2013a; Viebahn-Hansler et al., 2016). The gas volume for rectal insufflation started at 180 ml/session and was slowly increased in successive sessions according to patient tolerance until 300 ml (if possible) or a well-tolerated volume. The planned maximum volume of 300 ml/session (total amount of 9,000 µg of O3 by session) was administered in all patients except three (patients #3, #4, and #6). Patient #3 was treated with 300 ml most days, although volume was between 240 and 300 ml during the full treatment depending on the feeling of abdominal distension. In patient #4, O3T was administered during the second-line chemotherapy, which produced diarrhea and chemotherapy interruptions, and only 120 ml of gas was insufflated in the ozone sessions. Patient #6 presented self-limited episodes of abdominal pain with/without diarrhea after two O3T sessions with a gas insufflation of 300 ml; then, O3T was continued with 240 ml of gas insufflation without further problems. No other side effects were associated with O3T in the patient study group.
This is a preliminary report with two relevant limitations. First, our study was a non-RCT with small sample size; however, they were patients refractory to conventional treatment after a median time of 12 months before the commencement of O3T. Second, the sample comprised patients with different tumor locations and different chemotherapy treatments, although most patients were treated because of colorectal cancer or gynecological tumors using platinum-based drugs.
Although this was a preliminary study, the magnitude and length of the observed effects and the limited therapeutical approaches for CIPN support further research with larger sample sizes, such as our ongoing randomized clinical trial (NCT04299893), to confirm our results.
This preliminary report shows that most patients could obtain clinically relevant and long-term improvement in chronic pain secondary to CIPN after ozone treatment. The observed effects of ozone as an adjuvant treatment in the management of painful CIPN merit further research and support our ongoing randomized clinical trial.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Compassionate ozone treatment in our hospital was assessed by the Health Care Ethics Committee, and this study was approved by the Provincial Research Ethics Committee of Las Palmas, Spain (Ref 2019-288-1). The patients/participants provided their written informed consent to participate in this study.
Conceptualization: BC, DR-A, SG, MF, GM-S, FR-E, and PS-A; formal analysis: BC, YR-F, and PS-A; methodology: BC, YR-F, FR-E, and PS-A; initial management and oncology follow-up: DR-A, SG, MF, CA, GB, and DR-B.; treatment with ozone therapy: BC, and IJ; writing—original draft: BC, GM-S, YR-F, FR-E, and PS-A; writing—review, editing and approval of the final version: BC, DR-A, SG, MF, GM-S, YR-F, CA, GB, DR-B, IJ, FR-E, and PS-A.; funding acquisition: Grant PI 19/00458 by BC and DR-A. Grant BF1-19-13 by BC, and Grant PI 016/2019 by BC. All authors have read and agreed to the published version of the manuscript.
This study was partially supported by a grant (PI 19/00458) from the Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation, Madrid, Spain and European Regional Development Fund—ERDF), a grant (016/2019) from the Fundación DISA (Las Palmas, Spain), and a grant (BF1-19-13) from the Fundación Española del Dolor (Spanish Pain Foundation, Madrid, Spain).
One ozone therapy device used in this study (Ozonosan Alpha-plus®) at the Dr. Negrín University Hospital was provided by Renate Viebahn (Hänsler GmbH, Iffezheim, Germany). The use of the other ozone therapy device in this study (Ozonobaric-P, SEDECAL, Madrid, Spain) was supported by a grant (COV20/00702) from the Instituto de Salud Carlos III (Spanish Ministry of Science and Innovation, Madrid, Spain). The utilization of the EQ-5D-5L™ questionnaire by our group was approved (ID 45255) by © EuroQol Research Foundation. EQ-5D™ is a trademark of the EuroQol Research Foundation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Bae E. H., Greenwald M. K., Schwartz A. G. (2021). Chemotherapy-induced peripheral neuropathy: Mechanisms and therapeutic avenues. Neurotherapeutics 18 (4), 2384–2396. doi:10.1007/s13311-021-01142-2
Calabrese E. J., Kozumbo W. J. (2021). The hormetic dose-response mechanism: Nrf2 activation. Pharmacol. Res. 167, 105526. doi:10.1016/j.phrs.2021.105526
Clavo B., Ceballos D., Gutierrez D., Rovira G., Suarez G., Lopez L., et al. (2013a). Long-term control of refractory hemorrhagic radiation proctitis with ozone therapy. J. Pain Symptom Manage. 46 (1), 106–112. doi:10.1016/j.jpainsymman.2012.06.017
Clavo B., Gutierrez D., Martin D., Suarez G., Hernandez M. A., Robaina F. (2005). Intravesical ozone therapy for progressive radiation-induced hematuria. J. Altern. Complement. Med. 11 (3), 539–541. doi:10.1089/acm.2005.11.539
Clavo B., Martinez-Sanchez G., Rodriguez-Esparragon F., Rodriguez-Abreu D., Galvan S., Aguiar-Bujanda D., et al. (2021a). Modulation by ozone therapy of oxidative stress in chemotherapy-induced peripheral neuropathy: The background for a randomized clinical trial. Int. J. Mol. Sci. 22 (6), 2802. doi:10.3390/ijms22062802
Clavo B., Navarro M., Federico M., Borrelli E., Jorge I. J., Ribeiro I., et al. (2021b). Long-term results with adjuvant ozone therapy in the management of chronic pelvic pain secondary to cancer treatment. Pain Med. 22 (9), 2138–2141. doi:10.1093/pm/pnaa459
Clavo B., Rodriguez-Esparragon F., Rodriguez-Abreu D., Martinez-Sanchez G., Llontop P., Aguiar-Bujanda D., et al. (2019). Modulation of oxidative stress by ozone therapy in the prevention and treatment of chemotherapy-induced toxicity: Review and prospects. Antioxidants (Basel) 8 (12), E588. doi:10.3390/antiox8120588
Clavo B., Santana-Rodriguez N., Gutierrez D., Lopez J. C., Suarez G., Lopez L., et al. (2013b). Long-term improvement in refractory headache following ozone therapy. J. Altern. Complement. Med. 19 (5), 453–458. doi:10.1089/acm.2012.0273
Clavo B., Santana-Rodriguez N., Llontop P., Gutierrez D., Ceballos D., Mendez C., et al. (2015). Ozone therapy in the management of persistent radiation-induced rectal bleeding in prostate cancer patients. Evid. Based. Complement. Altern. Med. 2015, 480369. doi:10.1155/2015/480369
Clavo B., Suarez G., Aguilar Y., Gutierrez D., Ponce P., Cubero A., et al. (2011). Brain ischemia and hypometabolism treated by ozone therapy. Forsch. Komplementmed. 18 (5), 283–287. doi:10.1159/000333795
Dhawan S., Andrews R., Kumar L., Wadhwa S., Shukla G. (2020). A randomized controlled trial to assess the effectiveness of muscle strengthening and balancing exercises on chemotherapy-induced peripheral neuropathic pain and quality of life among cancer patients. Cancer Nurs. 43 (4), 269–280. doi:10.1097/NCC.0000000000000693
Di Cesare Mannelli L., Zanardelli M., Failli P., Ghelardini C. (2012). Oxaliplatin-induced neuropathy: Oxidative stress as pathological mechanism. Protective effect of silibinin. J. Pain 13 (3), 276–284. doi:10.1016/j.jpain.2011.11.009
Fuccio C., Luongo C., Capodanno P., Giordano C., Scafuro M. A., Siniscalco D., et al. (2009). A single subcutaneous injection of ozone prevents allodynia and decreases the over-expression of pro-inflammatory caspases in the orbito-frontal cortex of neuropathic mice. Eur. J. Pharmacol. 603 (1-3), 42–49. doi:10.1016/j.ejphar.2008.11.060
Galie M., Covi V., Tabaracci G., Malatesta M. (2019). The role of Nrf2 in the antioxidant cellular response to medical ozone exposure. Int. J. Mol. Sci. 20 (16), E4009. doi:10.3390/ijms20164009
Guclu A., Erken H. A., Erken G., Dodurga Y., Yay A., Ozcoban O., et al. (2016). The effects of ozone therapy on caspase pathways, TNF-α, and HIF-1α in diabetic nephropathy. Int. Urol. Nephrol. 48 (3), 441–450. doi:10.1007/s11255-015-1169-8
Hidalgo-Tallon F. J., Torres-Morera L. M., Baeza-Noci J., Carrillo-Izquierdo M. D., Pinto-Bonilla R. (2022). Updated review on ozone therapy in pain medicine. Front. Physiol. 13, 840623. doi:10.3389/fphys.2022.840623
Kleckner I. R., Kamen C., Gewandter J. S., Mohile N. A., Heckler C. E., Culakova E., et al. (2018). Effects of exercise during chemotherapy on chemotherapy-induced peripheral neuropathy: A multicenter, randomized controlled trial. Support. Care Cancer 26 (4), 1019–1028. doi:10.1007/s00520-017-4013-0
Kneis S., Wehrle A., Muller J., Maurer C., Ihorst G., Gollhofer A., et al. (2019). It's never too late - balance and endurance training improves functional performance, quality of life, and alleviates neuropathic symptoms in cancer survivors suffering from chemotherapy-induced peripheral neuropathy: Results of a randomized controlled trial. BMC Cancer 19 (1), 414. doi:10.1186/s12885-019-5522-7
Kruk J., Aboul-Enein H. Y., Kladna A., Bowser J. E. (2019). Oxidative stress in biological systems and its relation with pathophysiological functions: The effect of physical activity on cellular redox homeostasis. Free Radic. Res. 53 (5), 497–521. doi:10.1080/10715762.2019.1612059
Loprinzi C. L., Lacchetti C., Bleeker J., Cavaletti G., Chauhan C., Hertz D. L., et al. (2020). Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J. Clin. Oncol. 38 (28), 3325–3348. doi:10.1200/JCO.20.01399
Markham M. J., Wachter K., Agarwal N., Bertagnolli M. M., Chang S. M., Dale W., et al. (2020). Clinical cancer advances 2020: Annual report on progress against cancer from the American society of clinical oncology. J. Clin. Oncol. 38 (10), 1081. doi:10.1200/JCO.19.03141
Re L., Martinez-Sanchez G., Bordicchia M., Malcangi G., Pocognoli A., Morales-Segura M. A., et al. (2014). Is ozone pre-conditioning effect linked to nrf2/EpRE activation pathway in vivo? A preliminary result. Eur. J. Pharmacol. 742, 158–162. doi:10.1016/j.ejphar.2014.08.029
Salat K. (2020). Chemotherapy-induced peripheral neuropathy: Part 1-current state of knowledge and perspectives for pharmacotherapy. Pharmacol. Rep. 72 (3), 486–507. doi:10.1007/s43440-020-00109-y
Seretny M., Currie G. L., Sena E. S., Ramnarine S., Grant R., MacLeod M. R., et al. (2014). Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 155 (12), 2461–2470. doi:10.1016/j.pain.2014.09.020
Shim H. S., Bae C., Wang J., Lee K. H., Hankerd K. M., Kim H. K., et al. (2019). Peripheral and central oxidative stress in chemotherapy-induced neuropathic pain. Mol. Pain 15, 1744806919840098. doi:10.1177/1744806919840098
Smith E. M., Pang H., Cirrincione C., Fleishman S., Paskett E. D., Ahles T., et al. (2013). Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: A randomized clinical trial. JAMA 309 (13), 1359–1367. doi:10.1001/jama.2013.2813
Starobova H., Vetter I. (2017). Pathophysiology of chemotherapy-induced peripheral neuropathy. Front. Mol. Neurosci. 10, 174. doi:10.3389/fnmol.2017.00174
Tricarico G., Travagli V. (2021). The relationship between ozone and human blood in the course of a well-controlled, mild, and transitory oxidative eustress. Antioxidants (Basel) 10 (12), 1946. doi:10.3390/antiox10121946
Viebahn-Haensler R., Leon Fernandez O. S. (2021). Ozone in medicine. The low-dose ozone concept and its basic biochemical mechanisms of action in chronic inflammatory diseases. Int. J. Mol. Sci. 22 (15), 7890. doi:10.3390/ijms22157890
Viebahn-Hansler R., Leon Fernandez O. S., Fahmy Z. (2016). Ozone in medicine: Clinical evaluation and evidence classification of the systemic ozone applications, major autohemotherapy and rectal insufflation, according to the requirements for evidence-based medicine. Ozone Sci. Eng. 38, 322–345. doi:10.1080/01919512.2016.1191992
Wu M. Y., Xing C. Y., Wang J. N., Li Y., Lin X. W., Fu Z. J. (2018). Therapeutic dosage of ozone inhibits autophagy and apoptosis of nerve roots in a chemically induced radiculoneuritis rat model. Eur. Rev. Med. Pharmacol. Sci. 22 (6), 1787–1797. doi:10.26355/eurrev_201803_14598
Zajaczkowska R., Kocot-Kepska M., Leppert W., Wrzosek A., Mika J., Wordliczek J. (2019). Mechanisms of chemotherapy-induced peripheral neuropathy. Int. J. Mol. Sci. 20 (6), E1451. doi:10.3390/ijms20061451
Keywords: antioxidants, cancer survivorship, cancer therapy-induced side effects, chemotherapy-induced peripheral neuropathy, neuropathic pain, oxidative stress, ozone therapy, pain
Citation: Clavo B, Rodríguez-Abreu D, Galván S, Federico M, Martínez-Sánchez G, Ramallo-Fariña Y, Antonelli C, Benítez G, Rey-Baltar D, Jorge IJ, Rodríguez-Esparragón F and Serrano-Aguilar P (2022) Long-term improvement by ozone treatment in chronic pain secondary to chemotherapy-induced peripheral neuropathy: A preliminary report. Front. Physiol. 13:935269. doi: 10.3389/fphys.2022.935269
Received: 03 May 2022; Accepted: 09 August 2022;
Published: 30 August 2022.
Edited by:
Ali Mobasheri, University of Oulu, FinlandReviewed by:
Manuela Malatesta, University of Verona, ItalyCopyright © 2022 Clavo, Rodríguez-Abreu, Galván, Federico, Martínez-Sánchez, Ramallo-Fariña, Antonelli, Benítez, Rey-Baltar, Jorge, Rodríguez-Esparragón and Serrano-Aguilar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bernardino Clavo, YmVybmFyZGlub2NsYXZvQGdtYWlsLmNvbQ==; Francisco Rodríguez-Esparragón, YWZyb2Rlc3BAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.