 Henning Bay Nielsen
Henning Bay Nielsen Stefanos Volianitis
Stefanos Volianitis Niels H. Secher
Niels H. Secher
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 11 April 2022
Sec. Exercise Physiology
Volume 13 - 2022 | https://doi.org/10.3389/fphys.2022.828708
This article is part of the Research Topic Advances in Rowing Physiology View all 17 articles
Rowing performance may be enhanced by attenuated metabolic acidosis following bicarbonate (BIC) supplementation. This study evaluated the dose of BIC needed to eliminate the decrease in plasma pH during maximal ergometer rowing and assessed the consequence for change in plasma volume. Six oarsmen performed “2,000-m” maximal ergometer rowing trials with BIC (1 M; 100–325 ml) and control (CON; the same volume of isotonic saline). During CON, pH decreased from 7.42 ± 0.01 to 7.17 ± 0.04 (mean and SD; p < 0.05), while during BIC, pH was maintained until the sixth minute where it dropped to 7.32 ± 0.08 and was thus higher than during CON (p < 0.05). The buffering effect of BIC on metabolic acidosis was dose dependent and 300–325 mmol required to maintain plasma pH. Compared to CON, BIC increased plasma sodium by 4 mmol/L, bicarbonate was maintained, and lactate increased to 25 ± 7 vs. 18 ± 3 mmol/L (p < 0.05). Plasma volume was estimated to decrease by 24 ± 4% in CON, while with BIC the estimate was by only 7 ± 6% (p < 0.05) and yet BIC had no significant effect on performance [median 6 min 27 s (range 6 min 09 s to 6 min 57 s) vs. 6 min 33 s (6 min 14 s to 6 min 55 s)]. Bicarbonate administration attenuates acidosis during maximal rowing in a dose-dependent manner and the reduction in plasma volume is attenuated with little consequence for performance.
Bicarbonate supplementation is considered an ergogenic agent through enhanced blood buffer capacity whereby fatigue may be attenuated. Although data are inconsistent (Christensen et al., 2014; Krustrup et al., 2015) probably related to different study protocols (Maughan et al., 2018), it seems that bicarbonate administration is associated with enhanced exercise capacity (Nielsen et al., 2002a). Thus, based on a meta-analysis of moderate to high quality, it is concluded that sodium bicarbonate supplementation enhances aerobic power, anaerobic capacity, and thus performance in endurance events lasting ∼45 s to 8 min, muscle endurance, 2,000-m ergometer rowing performance, and high-intensity intermittent running (Grgic et al., 2021).
The enhanced blood buffer capacity following administration of sodium bicarbonate supports arterial O2 saturation (SaO2) by a Bohr effect on the oxygen-haemoglobin dissociation curve (Nielsen et al., 2002b) and could explain the increase in performance. However, neither pulmonary O2 uptake nor muscle oxygenation is affected by expanded blood buffer capacity (Nielsen et al., 2002a). The increase in blood bicarbonate expands the ability to absorb excess intramuscular hydrogen ions whereby lactate transport to blood is facilitated to serve the brain and attenuate central fatigue and thereby enhance performance (van Hall et al., 2009; Volianitis et al., 2011; Siebenmann et al., 2021). An often overlooked effect of sodium bicarbonate is that blood sodium increases. Normally exercise is associated with drop in plasma volume and that is likely attenuated by sodium bicarbonate.
The present report evaluated data from pilot studies carried out to establish the dose of bicarbonate that is required to maintain pH and SaO2 during maximal ergometer rowing (Nielsen et al., 2002b). As the pilot studies used different doses of bicarbonate, we evaluated whether bicarbonate influences pH in a dose-response manner. The volume administered in control and intervention settings was similar which allowed for evaluation of whether the hypertonic sodium bicarbonate solution influences an estimate of changes in plasma volume.
Seven competitive oarsmen (age 22 ± 2 yrs, height 182 ± 3 cm, weight 78 ± 2 kg; mean with SD) participated in the study after informed consent as approved by the Ethics Committee of Copenhagen (KF 01-280/98; Nielsen et al., 2002a). On the first trial day, the rowers were asked to report their personal record for “2,000-m” ergometer rowing [median 6 min 33 s (range 6 min 03 s to 7 min 02 s)]. No subject had any disease or injury in the 3 weeks prior the trials and was not taking any medication. The subjects were fasting on the day of the experiments which took place in the morning.
Rowing was performed on an ergometer (model C; Concept II, Morrisville, VT). First, the subjects rowed for 12 min at work rates increasing from 150 to 250 W in steps of 50 W every third minute (warm-up; Nielsen et al., 2002b). Then they rowed for 5 min at an individually determined pace including several strokes at maximal intensity. After 5 min of recovery, a 2,000-m all-out time trial simulated an on-water competition. The study aimed to identify the dose of bicarbonate that would abolish acidosis during maximal rowing. Thus, the subjects received doses of sodium bicarbonate (1 M) ranging from 100—325 ml (Table 1) separated by at least 7 days. In the control setting isotonic saline, in similar volume to that provided in the bicarbonate trials, was administered. Sodium bicarbonate comes as 1 mmol/ml; a dose of, e.g., 300 mmol is therefore interchangeable to administration of 300 ml.
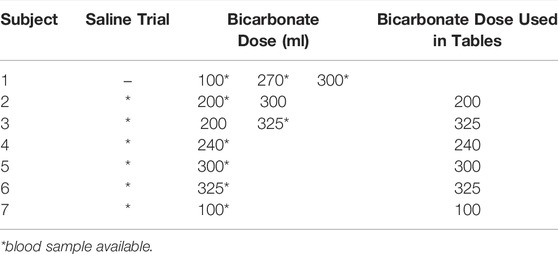
TABLE 1. Bicarbonate dose and availability of blood samples.
A catheter (1.0 mm, 20 gauge) was placed in radial artery of the non-dominant arm and allowed for blood sampling during rowing. Infusion of sodium bicarbonate or saline was administered through a central catheter (1.7 mm, 16 gauge) inserted in an upper arm vein. The intended dose of sodium bicarbonate or saline to be infused was in 60-ml syringes emptied at a constant rate (app. 50–60 ml/min) according to the expected race time as reported by the rower.
Arterial blood samples were obtained anaerobically in heparinized syringes (4042E, SIMS, Radiometer, Copenhagen, Denmark) at rest, during the maximal row, and in the recovery. Samples were turned and kept on ice until analysed for blood-gas variables, haemoglobin (Hgb), haematocrit (Hct), glucose, sodium, calcium, potassium, glucose, and lactate by a ABL 615 apparatus (Radiometer) with co-oximetry for determination of haemoblobin O2 saturation (SaO2). Paired blood sample data were available for six rowers as in one subject (#1) blood sampling failed during the control trial (Table 1). Only data obtained from trials with a maximal dose of bicarbonate used for each individual went into analysis of the data as presented in Tables 2, 3. Several doses of bicarbonate were used which allowed for construction of dose-response-like plot visualising the effect of bicarbonate on pH during ergometer rowing (Figure 1).
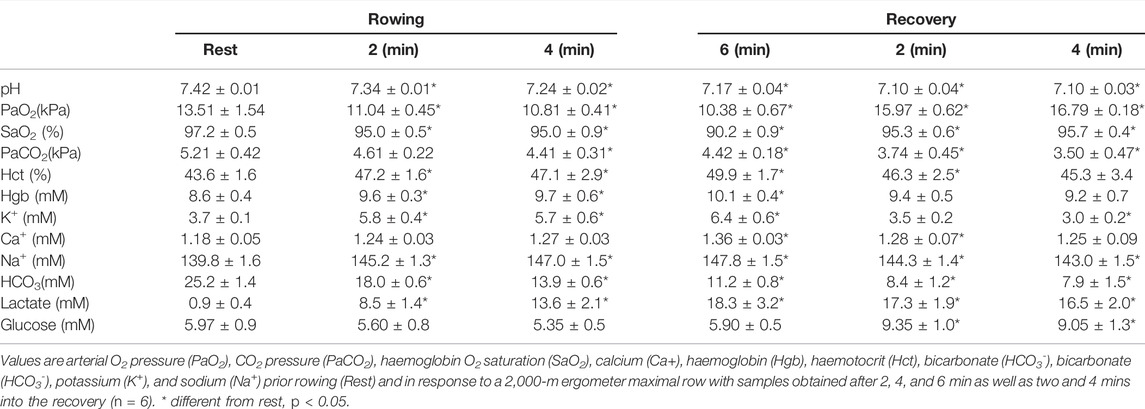
TABLE 2. Blood variables during and after maximal ergometer rowing with infusion of isotonic saline.
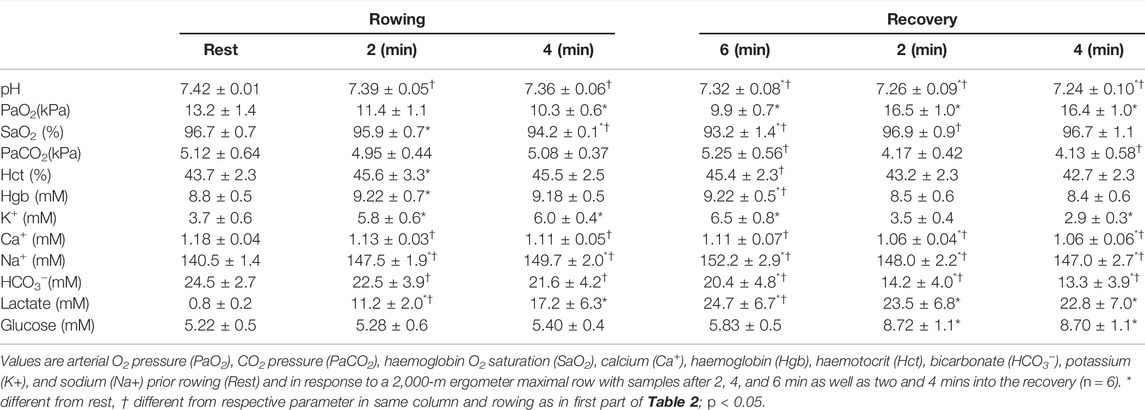
TABLE 3. Blood variables during and after maximal ergometer rowing with infusion of bicarbonate.
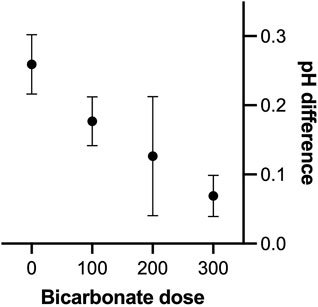
FIGURE 1. pH effect of different doses of bicarbonate administered intravenosly during maximal ergometer rowing in seven oarsmen. X-axis is the dose group of bicarbonate used (100: use of 100 mmol in two subjects, 200 use of 200–240 mmol in four subjects and 300 administration of 300–340 mmol in four subjects) while “0” represent the control saline trial in six subjects. Y-axis is the difference between the pH at rest in samples obtained in the sixth minute of rowing. It is a limitation not all subjects received same amount of bicarbonate.
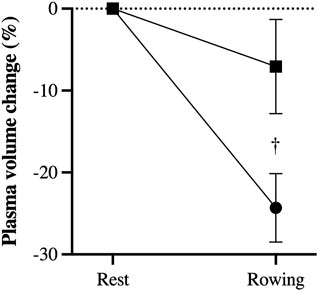
FIGURE 2. Estimated rowing induced decrease in plasma volume (%) in trials with administration of bicarbonate (square) compared to control (circle). †, difference between rowing with bicarbonate and control; p < 0.05.
Changes in plasma volume were estimated by modified Strauss formula (Strauss et al., 1951) as also reported by Fudim and Miller (2018) in which values for Hgb and Hct variables are incorporated. Thus, changes in plasma volume was taken as {l00 X [(Hgb B/Hgb D) X (1-Hct D)/(l- Hct B)]−100}, where B is before rowing and D during rowing.
Data are presented as mean and standard deviation (SD). For the evaluation of data in Table 2 and 3 one-way analysis of variance (ANOVA) was applied across the measure points for each parameter to be evaluated in each type of intervention. If significant interactions were found, a two-way t-test for paired data was used to locate differences. Evaluation of performance and plasma volume was by t-test only and a p–value < 0.05 was considered statistically significant.
The time for rowing was similar in trials with sodium bicarbonate and infusion of saline [median 6 min 27 s (range 6 min 09 s to 6 min 57 s) vs. 6 min 33 s (6 min 14 s to 6 min 55 s), respectively; p > 0.05] as four rowers improved their race time while two subjects (dose only 100 and 240 ml bicarbonate) demonstrated slower race time by 1 and 3 s. The perceived exertion (Borg scale) was similar in the two trials [median of 19 (range 16–19) vs. 19 (17–19), respectively; p > 0.05].
During control maximal rowing, arterial lactate increased to the last minute of exercise (Table 2) with higher values with bicarbonate (Table 3). The level of lactate remained high in the recovery and for the sodium bicarbonate trial, lactate tended to remain higher than in response to saline (p = 0.052 and p = 0.061). Thus, blood lactate increased more (by 6.6 ± 4.1 mM) in the sodium bicarbonate compared with the control trial. The maximal lactate level was 30.8 mM.
Blood bicarbonate was markedly reduced during maximal rowing with saline to a minimum of 10.2 mM and it was further reduced in the recovery (Table 2). With the infusion of sodium bicarbonate (Table 3), blood bicarbonate remained stable until the sixth min of exercise. Both during rowing and in the recovery, blood bicarbonate remained higher than in the control trial.
In response to rowing with saline, pH decreased to reach the lowest level in the sixth minute (minimum pH 7.13) and it was further reduced in the recovery (minimum pH 7.06, Table 2). With infusion of sodium bicarbonate, pH remained almost stable until the sixth minute and remained higher than in the control trial in the recovery (Table 3). Infusion of bicarbonate abolished the rowing-induced acidosis in a dose-dependent manner (Figure 1). Thus to limit the rowing-induced reduction in pH, the effective dose of bicarbonate was 300–325 mM.
In the control trial PaO2 decreased during maximal exercise (lowest value 9.82 kPa) and also SaO2 decreased to reach a minimum of 88.7% in the last minute but was re-established in the recovery (Table 2) and sodium bicarbonate trial improved SaO2. The saline trial reduced PaCO2 while rowing with sodium bicarbonate did not affcet PaCO2 and it remained higher than in the control trial. The Hct and Hgb increased in response to maximal rowing but with bicarbonate these variables were lower than in the control trial.
Plasma glucose was unchanged during rowing but increased in recovery without an effect of bicarbonate supplementation (Tables 2). Also potassium increased during rowing with no significant effect of sodium bicarbonate, while modest hypokalimea manifested in the recovery. During rowing with saline plasma calcium increased, while during rowing with bicarbonate it remained close to the resting level and below that observed during control exercise. Following rowing with bicarbonate, modest reduction in Ca++ was noted. In response to maximal rowing plasma sodium increased in both trials but to a larger extent in the trial with bicarbonate administration (by ≈ 4 mmol/L).
During rowing with saline the estimated plasma volume was reduced by 24 ± 4%, while with bicarbonate administration that reduction was by only 7 ± 6% (p < 0.05).
This study addresses two important issues 1) the effect of bicarbonate on acidosis and associated blood buffering capacity and 2) potential influence of bicarbonate on plasma volume. The data were collected retrospectively from a study that was conducted in a prospective manner. Here the effect of administration of bicarbonate i.v. (rather than orally as in most studies) is addressed.
The influence of maximal ergometer rowing on blood buffer capacity is pronounced (Nielsen et al., 1999). Evaluation of the dose-response effect of bicarbonate on pH reveals that about 300 mmol is required to eliminate acidosis during rowing, while administration of 100 mmol produces only a marginal effect. Thus, with production of lactate lowering blood pH towards, e.g., 7.1, administration of limited volume of sodium bicarbonate pH becomes only partially reversed. Importantly, intracellular pH is also affected by administration of bicarbonate (Nielsen et al., 2002b) and in perspective these observations provide an albeit indirect estimate of the anaerobic contribution to the work performed (Volianitis et al., 2020). With regards to the ergogenic effect of bicarbonate administration it is acknowledged that the intervention depends on the extend of acidosis provoked during the rowing trial (i.e., if the deviation from resting pH is marginal, enhancement of the blood buffering capacity will have minimal ergogenic effect). An important limitation is that it requires the subjects to be equally motivated in all trials as here supported by rate of perceived exertion of about 19. As indicated the data were obtained to evaluate the dose of bicarbonate needed to eliminate the decrease in pH associated with maximal rowing. The dose-response curve represented by Figure 1 was constructed only with a minimal number of observations needed to conduct the main study. The ideal dose-response curve would include data from a set-up where all subjects received different doses at separate occasions but such endeavour should be undertaken in future studies. Yet, the current data provide for a perspective on anaerobic metabolism during maximal exercise.
The other important observation relates to plasma volume changes during rowing. Exercise induces a rapid fluid-shift with a drop in plasma volume during even short-term maximal exercise (Kaltreider and Mieneely, 1940; Sullivan et al., 1993). Haemoconcentration is important for maintained arterial oxygen content and may compensate for (Schierbauer et al., 2021) or likely limit an increase in cardiac output (González-Alonso et al., 2006). By use of indirect measures to estimate changes in plasma volume, administration of sodium bicarbonate was associated with attenuated decrease in plasma volume. Likely, an increase in plasma sodium counteracts transport of fluid from the intravascular compartment. Therefore, studies evaluating the effect of sodium bicarbonate on performance should account also for plasma volume changes. Such consideration may be of relevance especially for prolonged exercise and exercise in the heat.
Blood variables evaluate the influence of rowing on blood oxygenation. As reported by Nielsen et al. (2002a), maximal ergometer rowing is associated with significant hypoxaemia as also observed for running (Rowell et al., 1964; Dempsey et al., 1984; Dempsey and Wagner, 1999). The O2 dissociation curve is right shifted by a decrease in pH and even a modest drop in PaO2 becomes of consequence for SaO2 that may reach 85–87% when large muscle mass is engaged (Rasmussen et al., 1991) including ergometer rowing (Hanel et al., 1994). Thus, when exercise-indued hypoxaemia is reversed by breathing an O2 enriched atmosphere, exercise capacity increases (Nielsen et al., 1998; Nielsen et al., 1999). This study evaluated the amount of bicarbonate needed to maintain SaO2 despite the drop in PaO2 during maximal ergometer rowing.
Interpretation of data is limited by the small number of subjects included of potential consequence for statistical significance for difference in performance and, unfortunately, blood sampling failed for one subject. Thus, an increase in performance would not be expected for those subject who received smallest dose of bicarbonate. Also, plasma volume change was based on indirect measures. The use of Hgb and Hct to estimate changes in plasma volume was proposed by Strauss et al. (1951) and Dill and Costill (1974) found the approach feasible for estimation of changes during exercise. Yet, Fudim and Miller (2018) report that in heart failure patients plasma volume calculated by formulae using Hgb/Hct correlate only moderately to a direct evaluation. Furthermore, it is likely that use of isotonic saline in the control setting has supported plasma volume. Yet, a strength of the study is that subjects acted as their own control.
We conclude that the effect of bicarbonate on arterial pH and thus oxygen saturation is dose-dependent and that a potential effect of bicarbonate on performance should take into account the effect on plasma sodium and attenuated reduction in plasma volume during maximal exercise.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethical committee of Cogenhagen. The patients/participants provided their written informed consent to participate in this study.
HN, SV, NS contributed to execution of study, data collection and construction of manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Morten Strømstad MSc and Per Bredmose MD are acknowledged for excellent assistance.
Christensen P. M., Petersen M. H., Friis S. N., Bangsbo J. (2014). Caffeine, but Not Bicarbonate, Improves 6 Min Maximal Performance in Elite Rowers. Appl. Physiol. Nutr. Metab. 39, 1058–1063. doi:10.1139/apnm-2013-0577
Dempsey J. A., Hanson P. G., Henderson K. S. (1984). Exercise-induced Arterial Hypoxaemia in Healthy Human Subjects at Sea Level. J. Physiol. 355, 161–175. doi:10.1113/jphysiol.1984.sp015412
Dempsey J. A., Wagner P. D. (1999). Exercise-induced Arterial Hypoxemia. J. Appl. Physiol. 87, 1997–2006. doi:10.1152/jappl.1999.87.6.1997
Dill D. B., Costill D. L. (1974). Calculation of Percentage Changes in Volumes of Blood, Plasma, and Red Cells in Dehydration. J. Appl. Physiol. 37, 247–248. doi:10.1152/jappl.1974.37.2.247
Fudim M., Miller W. L. (2018). Calculated Estimates of Plasma Volume in Patients With Chronic Heart Failure-Comparison With Measured Volumes. J. Card. Fail. 24, 553–560. doi:10.1016/j.cardfail.2018.07.462
González-Alonso J., Mortensen S. P., Dawson E. A., Secher N. H., Damsgaard R. (2006). Erythrocytes and the Regulation of Human Skeletal Muscle Blood Flow and Oxygen Delivery: Role of Erythrocyte Count and Oxygenation State of Haemoglobin. J. Physiol. 572, 295–305. doi:10.1113/jphysiol.2005.101121
Grgic J., Grgic I., Del Coso J., Schoenfeld B. J., Pedisic Z. (2021). Effects of Sodium Bicarbonate Supplementation on Exercise Performance: an Umbrella Review. J. Int. Soc. Sports Nutr. 18, 71. doi:10.1186/s12970-021-00469-7
Hanel B., Clifford P. S., Secher N. H. (1994). Restricted Postexercise Pulmonary Diffusion Capacity Does Not Impair Maximal Transport for O2. J. Appl. Physiol. 77, 2408–2412. doi:10.1152/jappl.1994.77.5.2408
Kaltreider N. L., Meneely G. R. (1940). The Effect of Exercise on the Volume of the Blood. J. Clin. Invest. 19, 627–634. doi:10.1172/jci101165
Krustrup P., Ermidis G., Mohr M. (2015). Sodium Bicarbonate Intake Improves High-Intensity Intermittent Exercise Performance in Trained Young Men. J. Int. Soc. Sports Nutr. 12, 25. doi:10.1186/s12970-015-0087-6
Maughan R. J., Burke L. M., Dvorak J., Larson-Meyer D. E., Peeling P., Phillips S. M., et al. (2018). IOC Consensus Statement: Dietary Supplements and the High-Performance Athlete. Br. J. Sports Med. 52, 439–455. doi:10.1136/bjsports-2018-099027
Nielsen H. B., Boushel R., Madsen P., Secher N. H. (1999). Cerebral Desaturation during Exercise Reversed by O2 Supplementation. Am. J. Physiology-Heart Circulatory Physiol. 277, H1045–H1052. doi:10.1152/ajpheart.1999.277.3.h1045
Nielsen H. B., Bredmose P. P., Strømstad M., Volianitis S., Quistorff B., Secher N. H. (2002a). Bicarbonate Attenuates Arterial Desaturation during Maximal Exercise in Humans. J. Appl. Physiol. 93, 724–731. doi:10.1152/japplphysiol.00398.2000
Nielsen H. B., Hein L., Svendsen L. B., Secher N. H., Quistorff B. (2002b). Bicarbonate Attenuates Intracellular Acidosis. Acta Anaesthesiol. Scand. 46, 579–584. doi:10.1034/j.1399-6576.2002.460516.x
Nielsen H. B., Madsen P., Svendsen L. B., Roach R. C., Secher N. H. (1998). The Influence of P a O2 , pH and S a O2 on Maximal Oxygen Uptake. Acta Physiol. Scand. 164, 89–97. doi:10.1046/j.1365-201x.1998.00405.x
Nielsen H. B. (1999). pH after Competitive Rowing: the Lower Physiological Range? Acta Physiol. Scand. 165, 113–114. doi:10.1046/j.1365-201x.1999.00485.x
Rasmussen J., Hanel B., Diamant B., Secher N. H. (1991). Muscle Mass Effect on Arterial Desaturation after Maximal Exercise. Med. Sci. Sports Exerc. 23, 1349–1352. doi:10.1249/00005768-199112000-00005
Rowell L. B., Taylor H. L., Wang Y., Carlson W. S. (1964). Saturation of Arterial Blood with Oxygen during Maximal Exercise. J. Appl. Physiol. 19, 284–286. doi:10.1152/jappl.1964.19.2.284
Schierbauer J., Hoffmeister T., Treff G., Wachsmuth N. B., Schmidt W. F. J. (2021). Effect of Exercise-Induced Reductions in Blood Volume on Cardiac Output and Oxygen Transport Capacity. Front. Physiol. 12 (12), 679232. doi:10.3389/fphys.2021.679232
Siebenmann C., Sørensen H., Bonne T. C., Zaar M., Aachmann-Andersen N. J., Nordsborg N. B., et al. (2021). Cerebral Lactate Uptake during Exercise Is Driven by the Increased Arterial Lactate Concentration. J. Appl. Physiol. 131, 1824–1830. doi:10.1152/japplphysiol.00505.2021
Strauss M. B., Davis R. K., Rosenbaum J. D., Rossmeisl E. C. (1951). "Water Diuresis" Produced during Recumbency by the Intravenous Infusion of Isotonic Saline Solution 1. J. Clin. Invest. 30, 862–868. doi:10.1172/jci102501
Sullivan W., Alejandro‐De Leon D., Heather L. M., Jordan R., Gutin B. (1993). Plasma Volume Changes in Trained and Untrained Men during Submaximal and Maximal Work. Sports Med. Train. Rehabil. 4, 281–290. doi:10.1080/15438629309511992
van Hall G., Stømstad M., Rasmussen P., Jans Ø., Zaar M., Gam C., et al. (2009). Blood Lactate Is an Important Energy Source for the Human Brain. J. Cereb. Blood Flow Metab. 29, 1121–1129. doi:10.1038/jcbfm.2009.35
Volianitis S., Rasmussen P., Seifert T., Nielsen H. B., Secher N. H. (2011). Plasma pH Does Not Influence the Cerebral Metabolic Ratio during Maximal Whole Body Exercise. J. Physiol. 589, 423–429. doi:10.1113/jphysiol.2010.195636
Keywords: plasma volume, bicarbonate supplementation, rowing, hypoxaemia, desaturation, acidosis, bohr effect
Citation: Nielsen HB, Volianitis S and Secher NH (2022) Dose of Bicarbonate to Maintain Plasma pH During Maximal Ergometer Rowing and Consequence for Plasma Volume. Front. Physiol. 13:828708. doi: 10.3389/fphys.2022.828708
Received: 03 December 2021; Accepted: 08 March 2022;
Published: 11 April 2022.
Edited by:
Stuart Goodall, Northumbria University, United KingdomReviewed by:
Daniel Peart, Northumbria University, United KingdomCopyright © 2022 Nielsen, Volianitis and Secher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henning Bay Nielsen, aGVubmluZ2JheUBob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.