 José Afonso1
José Afonso1 Sílvia Rocha-Rodrigues2,3,4
Sílvia Rocha-Rodrigues2,3,4 Filipe M. Clemente2,5
Filipe M. Clemente2,5 Michele Aquino6
Michele Aquino6 Pantelis T. Nikolaidis7
Pantelis T. Nikolaidis7 Hugo Sarmento8
Hugo Sarmento8 Alberto Fílter9,10
Alberto Fílter9,10 Jesús Olivares-Jabalera9,11
Jesús Olivares-Jabalera9,11 Rodrigo Ramirez-Campillo12,13*
Rodrigo Ramirez-Campillo12,13*- 1Centre for Research, Education, Innovation and Intervention in Sport, Faculty of Sport of the University of Porto, Porto, Portugal
- 2Escola Superior de Desporto e Lazer, Instituto Politécnico de Viana do Castelo, Viana do Castelo, Portugal
- 3Research Centre in Sports Sciences, Health Sciences and Human Development, Vila Real, Portugal
- 4Tumor & Microenvironment Interactions Group, Instituto de Investigação e Inovação em Saúde, Porto, Portugal
- 5Instituto de Telecomunicações, Delegação da Covilhã, Covilhã, Portugal
- 6Department of Health and Sport Sciences, Adelphi University, New York, NY, United States
- 7School of Health and Caring Sciences, University of West Attica, Athens, Greece
- 8Research Unit for Sport and Physical Activity, Faculty of Sport Sciences and Physical Education, University of Coimbra, Coimbra, Portugal
- 9FSI Sport Research Lab, Football Science Institute, Granada, Spain
- 10Research Group Physical Activity, Health and Sport CTS-948, University of Pablo de Olavide, Seville, Spain
- 11Sport and Health University Research Institute, Department of Physical and Sports Education, University of Granada, Granada, Spain
- 12Department of Physical Activity Sciences, Universidad de Los Lagos, Santiago, Chile
- 13Centro de Investigación en Fisiología del Ejercicio, Facultad de Ciencias, Universidad Mayor, Santiago, Chile
The incidence and recurrence of hamstrings injuries are very high in sports, posing elevated performance and financial-related costs. Attempts to identify the risk factors involved in predicting vulnerability to hamstrings injury is important for designing exercise-based programs that aim to mitigate the rate and severity of hamstrings injuries and improve rehabilitation strategies. However, research has shown that non-modifiable risk factors may play a greater role than modifiable risk factors. Recognizing non-modifiable risk factors and understanding their implications will afford the prescription of better suited exercise programs, i.e., that are more respectful of the individual characteristics. In a nutshell, non-modifiable risk factors can still be acted upon, even if indirectly. In this context, an underexplored topic is how intra and inter- individual anatomic and physiologic variations in hamstrings (e.g., muscle bellies, fiber types, tendon length, aponeurosis width, attachment sites, sex- and age-related differences) concur to alter hamstrings injuries risk. Some anatomic and physiologic variations may be modifiable through exercise interventions (e.g., cross-sectional area), while others may not (e.g., supernumerary muscle bellies). This apparent dichotomy may hide a greater complexity, i.e., there may be risk factors that are partially modifiable. Therefore, we explored the available information on the anatomic variations of the hamstrings, providing a deeper insight into the individual risk factors for hamstrings injuries and contributing with better knowledge and potential applications toward a more individualized exercise prescription.
Introduction
The hamstrings are a hot topic in Sports Sciences, with a PubMed search using the terms “hamstring∗” and “sport∗” from the year 2020 to the present showing >500 entries. This is because hamstrings injuries are common in the athletic community (Monajati et al., 2016; Sheean et al., 2021). While hamstrings strain injury (HSI) is a commonly used term, it does not encompass all hamstrings injuries; therefore, HSI will only be used if the cited authors specifically refer to that subset of hamstrings injuries. The number of non-contact training-related hamstrings injuries in different sports have increased gradually and systematically [e.g., an annual average 2.3% increase in the total hamstrings injuries rate over the 13-year period (2001–2014)] (Ekstrand et al., 2016; Ertelt and Gronwald, 2017). Anatomic and functional aspects of the hamstrings, including the fact that muscles cross two joints (except the short head of the biceps femoris) and that eccentric action during running or stretching carried out to extreme joint positions, make it prone to vulnerable to strain-related injuries (Edouard et al., 2016).
A systematic review including 13 studies with more than 3,800 athletes and two million sport exposure hours reported an incidence of acute hamstrings injuries ranging from 0.3 to 0.5 per 1,000 exposure hours in women, to 0.3–1.9 per 1,000 exposure hours in men, accounting for 5% to 15% of all soccer-related injuries, with recurrence rates varying from 4 to 68% (Diemer et al., 2021). The prevalence of hamstrings injuries were reported to be more than 60% (unilateral) and more than 30% (bilateral) in baseball players, with ∼30% recurrence rates (Zachazewski et al., 2019), while prevalence rates of 40% were reported for professional soccer players (Ribeiro-Alvares et al., 2020). This is challenging in terms of recovery time and financial costs (Pickering and Kiely, 2018; Shield and Bourne, 2018; Metcalf et al., 2019). In the Australian Football League, data from 10 competitive seasons determined that the financial cost of HSI per club increased by 71% from 2003 to 2012 (Hickey et al., 2014).
A wide body of research explored the implementation of specific exercise-based programs for mitigating hamstrings injury risk (Al Attar et al., 2017; Chebbi et al., 2020). Due to intra- and inter-muscular differences in this group of muscles, exercises designed for the hamstrings may not provide equal stimuli for semitendinosus (ST), semimembranosus (SM), and biceps femoris (BF) (Kellis, 2018). Relevant works suggested that non-modifiable factors (i.e., older age, previous injury) may have a greater impact on risk for hamstrings injuries compared to modifiable ones (Freckleton and Pizzari, 2013; Green et al., 2020). Non-modifiable factors could also extend to aspects of human anatomy which are not possible to modify, such as variations in insertions sites and the presence of supernumerary muscle bellies (Tubbs et al., 2016).
A better knowledge of interindividual variation in hamstrings anatomy and geometry could allow the design of better-individualized interventions, eventually reducing the likelihood of suffering (and aid in the recovery from) an injury (Ertelt and Gronwald, 2017). Interindividual variation in strength levels (specifically eccentric strength), hamstrings muscle fascicle length, muscle-tendon architecture, muscle fiber type and region-specific innervation have been hypothesized as relevant factors for risk of HSI (Timmins, 2017; Huygaerts et al., 2021), and genetic variations have been explored in response to loading and post-exercise recovery (Pickering and Kiely, 2018). However, anatomic and physiologic variations of the hamstrings are more diversified than highlighted here (Tubbs et al., 2016).
Our goal was to explore the available information on the anatomic variations of the hamstrings, provide a deeper insight into the individual risk factors for hamstrings injuries and contribute evidence-based applications for more individualized intervention regimens. Although acute injury prediction, given its multifactorial nature, will probably never be possible (Bahr, 2016), some risk factors can be controlled for. In the first part of this commentary, an overview of hamstrings injuries is provided, including injury mechanisms, both non- and modifiable risk factors, exercise-based strategies to mitigate risk factors, as well as topics of rehabilitation and return to play (RTP). While the literature often dichotomizes risk factors into modifiable and non-modifiable, some non-modifiable risk factors may be partially modifiable, as will be discussed. In the second part, “normal” anatomy of the hamstrings is described, and the inter- and intraindividual variations of hamstrings anatomy and how they might be related to injury risk are explored, considering modifiable and non-modifiable anatomic variations and how to recognize them to prescribe better adjusted exercise. Non-modifiable risk factors can still be acted upon, by designing exercise interventions that are more respectful of those factors.
A systematic review of the literature was not performed, given the scope and goals of this commentary. However, we selected literature published in peer-reviewed journals, most of which indexed in PubMed. The goal was to gather relevant information on a wide variety of topics related to our theme. Where controversy existed, we attempted to provide a balanced discussion, selecting studies with contradictory findings. Where appropriate, renowned textbooks were used (Standring, 2015; Tubbs et al., 2016).
Part 1: An Overview of Hamstrings Injuries
Hamstrings Functions and Injury Mechanisms
The hamstrings are involved in major movements of daily life, such as standing and walking. In the standing position, the line of gravity passes behind the hip, producing an extension moment that needs to be counterbalanced by the hip flexors (Houglum and Bertoti, 2012). On the contrary, the hamstrings need to act toward knee flexion, since the line of gravity falls in front of the knee inducing hyperextension (Smith, 1957). During walking, the hamstrings (and gluteus maximus) act on the hip during the final leg swing phase by generating an eccentric action to decelerate the rate of hip flexion, and concentrically in the following hip extension (Hogervorst and Vereecke, 2015). During the leg swing phase, the hamstrings act eccentrically to decelerate the rate of knee extension (Houglum and Bertoti, 2012).
The hamstrings are important for sport activities involving sprints, jumps, tackles, cutting maneuvers and kicking (Ekstrand et al., 2012). The motion of the kicking leg (e.g., soccer kick) includes a backward and forward motion (Lees and Nolan, 1998). During the backward motion, the hamstrings act using concentric action in hip extension (together with gluteus maximus) and knee flexion and lateral rotation (only the BF) (Fields et al., 2005). During the forward motion, the hamstrings act eccentrically to decelerate hip and knee during respective hip flexion and knee extension motions (Fields et al., 2005). The decelerating action of hamstrings occur at a position (hip flexion and knee extension) where these muscles are passively insufficient (i.e., the muscles reach their maximal length since they are biarticular muscles passing through hip and knee) (Coole and Gieck, 1987). For these reasons, the hamstrings are prone to injury during high-velocity running or sprinting, due to eccentric over-loading at the end of the swing phase (Jönhagen et al., 1994).
A systematic review with 26 studies explored the mechanisms behind the hamstrings injuries (Danielsson et al., 2020); the authors stratified the mechanisms according to the methods used to determine the injury: (i) stretch-related injuries; (ii) kinematic analysis; (iii) electromyography-based kinematic analysis; and (iv) strength-related injuries. In the first group (i.e., stretch-related injuries), all studies reported that hamstrings injuries occurred upon extensive hip flexion with hyperextension of the knee (i.e., the hamstrings were strongly stretched at both joints it crosses, which are the hip and knee). In the review (Danielsson et al., 2020), hamstrings injuries were associated with running-based actions and especially to the late swing phase of the running gait cycle, which may imply a powerful eccentric action. These powerful actions increase as running velocity increases (Higashihara et al., 2010b).
Modifiable Risk Factors
Modifiable risk factors can be modified under certain interventions. In the case of hamstrings risk factors, these include player load, warm-up preparations, lumbo-pelvic hip stability, motor patterns (e.g., “Groucho” position), cardiovascular fitness, fatigue, mobility, low back pain, recovery strategies, strength, asymmetry, nutrition and psychosocial factors (Liu et al., 2012; Mendiguchia et al., 2012; Schuermans et al., 2014; Buckthorpe et al., 2019; Huygaerts et al., 2020). Using proper exercise-based programs, establishing a balance between load and recovery, carefully structuring of the intervention sessions, and providing adequate physical preparation, can readily tackle most of these risk factors, which is valid for nearly all injuries. We do not aim to provide an in-depth discussion of modifiable risk factors, as it would escape the main goals of our work. However, we feel it is relevant to briefly discuss four topics that should be more widely acknowledged (i.e., fatigue) or seen under a more critical perspective (i.e., warm-up, flexibility and functional asymmetry).
Fatigue
Fatigue was associated with decreased eccentric hamstrings strength and an altered neuromuscular coordination, suggesting a higher risk of developing an injury (Jones et al., 2015; Buckthorpe et al., 2019; Huygaerts et al., 2020). In the review of Danielsson et al. (2020), fatigue was associated to HSI, underlining that, aside from strength and flexibility, endurance was a relevant risk factor (Watson et al., 2017; Farley et al., 2020). Eccentric strength endurance of the hamstrings was reported to be significantly lower in male soccer players with previous hamstrings injuries (Schuermans et al., 2014). A study with elite footballers (n = 50) presented contradictory findings when comparing the previously injured limbs (n = 11) with non-injured limbs (n = 89) (Freitas et al., 2021), but the athletes acquired hamstrings injury in the previous 2 years, possibly providing enough time and exercise intervention for the hamstrings to recover their endurance levels. Previous injuries are non-modifiable risk factors, but improvements in endurance and increased tolerance to fatigue can be achieved with exercise training (Delextrat et al., 2018). In this sense, both detraining and hamstrings damage (secondary to a previous injury) may be considered partially modifiable factors.
The Warm-Up
The role of warm-up in reducing injury risk is not clear (Fradkin et al., 2006; McCrary et al., 2015), and adherence to warm-up protocols may interfere with its effectiveness (Owoeye et al., 2020), i.e., the frequency and degree of compliance to the warm-up protocol may largely dictate how effective the protocol is. It is unclear whether different types of warm-ups induce distinct acute effects on modifiable injury risk factors (Niederer et al., 2020). A prospective two-season study registered posterior thigh injuries in 83 Australian rules football players, of which 62 were confirmed to have hamstrings injury through magnetic resonance imaging (MRI) (Verrall et al., 2003). In this study, 15% of hamstrings injuries occurred during the warm-up period and 85% after the warm-up (Verrall et al., 2003). Considering that the main part of an exercise session is longer than the warm-up, these percentages of distribution provide insufficient information. Harking back to the discussion surrounding fatigue (Delextrat et al., 2018; Danielsson et al., 2020), it could be speculated that overly long and/or intense warm-ups may generate excessive fatigue for the remainder of the training session. Warm-up protocols aiming to produce performance potentiation usually generate potentiation and fatigue, and this balance varies from individual to individual (Afonso et al., 2019; Blazevich and Babault, 2019). Regarding hamstrings injury prevention, individually monitoring responses to warm-up is suggested.
The Role of Flexibility
A clear relationship between hamstrings flexibility and injury risk has also not been established (Worrell and Perrin, 1992; Christopher et al., 2019). de la Motte et al. (2019) assessed 27 studies and explicitly stated they considered studies showing association between flexibility and other factors and musculoskeletal injury in military and civilian populations. The authors showed there was moderate yet conflicting evidence associating hamstrings flexibility and musculoskeletal injury risk. It is easy for readers to interpret this association using a causative framework, but caution should be used, as previous hamstrings injuries reduce flexibility until 20–30 days post-injury (Maniar et al., 2016), but reduced flexibility does not necessarily increase injury risk. In this context, the role of stretching in reducing injury risk is controversial (Herbert and Gabriel, 2002; Small et al., 2008; Behm et al., 2015), specifically in the case of hamstrings injuries (Liu et al., 2012; Rogan et al., 2013).
Functional Asymmetry
Some degree of interlimb asymmetries in hamstrings strength is the norm (Boccia et al., 2018; Kulas et al., 2018; Cuthbert et al., 2021) and, if not excessive, are beneficial for performance of tasks involving change of direction and sprinting, without impaired jumping (Coratella et al., 2018). Injured soccer players exhibit a more symmetrical recruitment pattern between ST, SM and BF (corresponding to a less economic hamstrings muscle activation), as opposed to the more asymmetric pattern of subjects without previous injuries (Schuermans et al., 2014). Athletes with previous hamstrings injuries also demonstrated a decrease of ST metabolic activity, compensated by a greater involvement of the BF (Schuermans et al., 2014). The mechanisms underlying the symmetrical muscle activation possibly involve a compensatory increase of BF activation and a maladaptation neuromuscular coordination behavior, resulting in a less efficient hamstrings contraction. This condition, combined with peripheral metabolic changes (e.g., earlier onset of pH changes), leads to muscle fatigue and may explain the reduced endurance capacity, associated to a re-injury of hamstrings (Allen et al., 2008; Schuermans et al., 2016; Suarez-Arrones et al., 2021).
Exercise-Based Strategies for Mitigating Injury Risk
Studies assessing the effectiveness of exercise-based programs in mitigating hamstrings injury risk proliferated. The focus has relied on injury prevention, although we prefer terms such as “risk mitigation,” since there is always an inherent injury risk. A systematic review with meta-analysis (SRMA) including 17 studies showed that exercise-based interventions reduced hamstrings injury risk in ∼50% (Vatovec et al., 2020). However, the quality of assessment through the PEDro (Physiotherapy Evidence Database) scale showed major problems in many studies, with nine having a classification ≤4 (i.e., low methodological quality), and none presenting a classification above six points in the PEDro scale (i.e., no study with high quality). Another SRMA assessed 15 articles studying the effects of including the Nordic Hamstrings exercise (NHE) into wider exercise-based programs in hamstrings injury rate (van Dyk et al., 2019), which resulted in ∼50% risk reduction, but the authors showed that half of analyzed articles had high risk of bias in randomization and allocation concealment, and ∼80% had high risk of bias in blinding of outcome assessments, raising concerns regarding the trustworthiness of the findings. In their inclusion criteria (van Dyk et al., 2019), the intervention could be solely focused on the NHE or any wider program including the NHE compared to usual training or alternative programs; it is unclear whether the effects were attributable to the NHE, or to the wider program in which it was included.
Similar results were reported in another SRMA concerning the NHE (Al Attar et al., 2017), although a reasonable risk of bias has been reported elsewhere (Gérard et al., 2020). These two SRMA (Al Attar et al., 2017; Gérard et al., 2020) were alluding to relative risks, reducing the trustworthiness on the potential beneficial effect of the NHE on injury prevention. The feasibility of implementing certain protocols into real-world contexts is questionable since the evidence-based interventions are not always effective, i.e., translating into practical applications may be problematic (McCall et al., 2020). Beyond the intrinsic characteristics of each exercise-based program, its effectiveness depends on the buy-in, i.e., how well participants adhere to, and comply with the program (Buckthorpe et al., 2019). Therefore, the belief of coaches and athletes in the programs will interfere with how well they work. Indeed, the placebo and nocebo effects have been observed in sports science (Hurst et al., 2020; Raglin et al., 2020).
Weekly frequency of exercise-based programs to mitigate injury risk is an important parameter: interventions performed ≥2 times per week were more effective in reducing hamstrings injury risk than interventions performed <2 times per week, even though the differences were not large (Vatovec et al., 2020). Previous research suggested that the compliance to the program (i.e., adhering to and performing the sessions) is an important prognostic factor regarding injury risk (Goode et al., 2015; Chebbi et al., 2020).
While prevention programs are biased toward eccentric strength training of the hamstrings, interventions focused on improving endurance (Danielsson et al., 2020), motor control (Ertelt and Gronwald, 2017), lumbo-pelvic dynamics (Shield and Bourne, 2018), using video and technical feedback to improve biomechanical parameters of movement (Monajati et al., 2016), and isometric strength training (Macdonald et al., 2019) should not be neglected. Sprint training is possibly the most common mechanism to simulate the high load and high velocity eccentric actions of the hamstrings (van den Tillaar et al., 2017). A multifactorial, individualized approach should be included in the specific programs aiming to reduce injury risk (Mendiguchia et al., 2012; Lahti et al., 2020; Suarez-Arrones et al., 2021).
Rehabilitation and Return-to-Play
Rehabilitation and RTP after a hamstrings injury are challenging (Hickey et al., 2017; Taberner et al., 2020). The RTP relies on numerous determinants, such as injury mechanism, level of sport participation, and time to first consultation and pain (Fournier-Farley et al., 2016). It is common for deficits in strength, range of motion (ROM) and muscle morphology alterations to persist after RTP (Sanfilippo et al., 2013; Maniar et al., 2016). Criteria to support safe and appropriate RTP after hamstrings injuries are varied and lack validation (van der Horst et al., 2016). Some exercise-based strategies such as stretching have showed a decreased RTP time, but not reduced the risk of re-injury (Pas et al., 2015), suggesting a misconception in injury management.
The rehabilitation process depends on factors such as the extent and severity of injury, precise anatomic location and the tissue involved (e.g., fascia, muscle and/or tendon). The degree of hamstrings injuries will determine whether surgery is required or not (Ayuob et al., 2020; Sheean et al., 2021), although there is debate regarding the criteria for choosing conservative treatment vs. surgical management (Metcalf et al., 2019; Blakeney, 2020).
Modifiable Versus Non-modifiable Risk Factors
Despite the potential of exercise-based interventions for mitigating hamstrings injury risk, non-modifiable risk factors should be acknowledged, such as age and previous injury (Mendiguchia et al., 2012). A SRMA involving 71,324 athletes from 78 studies analyzed 8,319 HSIs, of which 967 were recurrences (Green et al., 2020). The stronger factors associated with an increased risk of HSI were older age, previous history of HSI, recent HSI, previous calf strain injury, and previous anterior cruciate ligament (ACL) injury, which are non-modifiable factors (Green et al., 2020). In contrast, modifiable risk factors, such as reductions in strength, strength endurance, power, and motor control, were weakly associated to increased risk for his, and flexibility, mobility or ROM were not associated with risk of HSI (Green et al., 2020).
Non-modifiable risk factors for HSI, such as age and previous injury, were consistently associated with an increased risk of injury in a previous SRMA that included 34 articles (Freckleton and Pizzari, 2013). In this SRMA, the only modifiable factor consistently associated with the risk of hamstrings injuries was the quadriceps concentric peak torque. In a prospective study with Australian football league players (n = 125), hamstrings injuries were not associated with NHE strength (Smith et al., 2021). In this study (Smith et al., 2021), player age greater than 25 years and having a previous hamstring, groin or calf injury increased the risk for hamstrings injury. Attention has been devoted to the modifiable risk factors, but non-modifiable factors should be further explored, as well as the mechanisms whereby some non-modifiable factors increase injury risk.
Although it is not possible to erase the existence or previous injuries, or change the age of the player, a better understanding of the hamstrings’ architecture, anatomy and mechanisms may help to deliver a better-individualized exercise-based approach. It was previously established that previous injuries impair ROM (Maniar et al., 2016) and endurance (Farley et al., 2020), both of which can be improved through well-designed exercise intervention protocols. While some architectural features might be modifiable [e.g., cross-sectional area (CSA)], others may not (e.g., variations in insertions), and an understanding of such features may afford a better-individualized exercise prescription. Sex- and age-related risk factors will be explored further in part 2, as they are closely linked to anatomic and physiologic variations. Even when certain factors are non-modifiable, the mechanisms that contribute to the increased injury risk could be individually targeted with better exercise-based interventions, to avoid exacerbating predisposing factors.
Synopsis of the First Part
The hamstrings are highly relevant for major movements of daily life and sports (e.g., standing, walking, sprinting, cutting), and play an especially important role in decelerating knee extension and hip flexion in high-velocity actions, common in athletic scenarios, such as sprinting. Hamstrings are prone to injuries and so it is important to understand the risk factors involved. Exercise-based interventions for mitigating hamstrings injury risk have emphasized the role of eccentrically biased strength training, although lumbo-pelvic dynamics, technical and motor pattern focused work, sprinting, isometric strength training and general strength and endurance training should not be neglected. Weekly frequency and compliance with the interventions constitutes a relevant factor mediating the effectiveness of exercise-based interventions in mitigating injury risk. However, research suggests that non-modifiable risk factors, namely age and previous injuries, may play a more relevant role in hamstrings injury risk than modifiable risk factors. In this context, relevant anatomic variations may alter the risk of hamstrings injury. Acknowledging the relevant anatomic variations may provide relevant information for prescribing exercise interventions, which will be the focus of the second part of this commentary. Box 1 briefly explores hamstrings’ strength evaluation.
BOX 1. Special box – hamstrings’ strength evaluation.
Measuring muscle strength allows evaluating and comparing muscle function and performance to obtain a pattern of intramuscular synergistic recruitment between the BF, ST, and SM muscles (Mjølsnes et al., 2004; Schuermans et al., 2014; Wiesinger et al., 2020). Improvement of hamstrings strength is an important strategy to mitigate injury incidence and recurrence, and one of the RTP criteria (Maniar et al., 2016). Early identification and management of excessive strength asymmetries and muscular imbalances assist in the elaboration of a more effective intervention plan to counteract a potential injury risk scenario (Schuermans et al., 2014; Wiesinger et al., 2020). The stationary isokinetic dynamometry (IKD) is a suitable system for assessment of torque during concentric and eccentric knee flexor action (Aagaard et al., 1998; van Dyk et al., 2018; Wollin et al., 2018), although its use is scarce compared to the Nordic hamstrings device (NHD) (Mjølsnes et al., 2004). The NHD detects strength deficits or side-to-side imbalances (Timmins et al., 2016), exercise-related strength progress (Delahunt et al., 2016), and may aid predicting recovery time after injury (McCall et al., 2016). However, van Dyk et al. (2018) reported a weak within-subject correlation (r = 0.35), demonstrating a systematic bias toward lower strength values with the NHE. Several methodological specificities were not considered when comparing both methods in previous studies, e.g., IKD and NHD tests were performed under different conditions of joint velocity and hip position (Higashihara et al., 2010a; Guex et al., 2016).
To understand these issues, Wiesinger et al. (2020) compared the mechanical output of hamstrings assessed by using both IKD and NHD methods of 25 healthy male athletes in a counterbalanced repeated-measures protocol. Higher total eccentric work, peak torque at greater knee extension angles, greater side-to-side strength difference, and lower eccentric peak torque were observed in IKD compared to NHD, whereas bilateral strength difference was lower in NHD. The electromyographic analysis showed no difference in the activation of BF and ST during IKD and NHD (Wiesinger et al., 2020). These findings suggest that IKD and NHD methods measured distinct hamstrings muscle activation characteristics. Some aspects were difficult to assess, such as intraindividual strength differences, angle of peak torque and side-to-side differences in eccentric knee flexor strength. It should be highlighted that muscles such as the sartorius, gracilis and gastrocnemius also contribute to knee flexion (Standring, 2015).
Surface electromyography (EMG) allow the assessment of muscle activation patterns (Higashihara et al., 2010a). The EMG activity shows that hamstrings muscles have functional differences, as the SM and BF work harder (i.e., greater EMG) during the initial phase of knee flexion, and the ST at deep flexion angles to complement the decrease in EMG of the other two muscles during open kinetic chain exercise (Hirose and Tsuruike, 2018). Miller et al. (2000) found that during isokinetic movements activation, the BF EMG increased with increasing movement velocity, while the ST and SM EMG activation remained constant during six continuous isokinetic knee extension and flexion movements at 60°, 180°, and 300° s–1. In opposition, functional MRI evaluates the intramuscular and intermuscular recruitment patterns with a very high spatial accuracy and detects the magnitude of metabolic activity in muscle tissue although with no real-time information about the amount and timing of the underlying muscle activity (Segal, 2007). Using functional MRI, Schuermans et al. (2014) demonstrated that the more symmetrical and less dissociated the hamstrings muscles work together, the higher the physiological changes would be inside the recruited muscle fibers. Thus, more intramuscular variability can be associated with a reduced metabolic turnover and more economic muscle functioning. MRI-based methods have high costs, risk of injury during assessment, lack of portability and long duration of assessment. Rapid, non-invasive alternative measures of concentric and eccentric hamstrings strength are warranted.
An adapted aneroid sphygmomanometer test (Mondin et al., 2018), a rapid and non-invasive tool, was proposed to assess hamstrings strength. In 14 rugby players, Mondin et al. (2018) found an association between the sphygmomanometer derived pressures at 30 and 90° of knee flexion and isokinetic strength measures, suggesting that this method was reliable to assess hamstrings strength, but not to identify strength asymmetries between dominant and non-dominant legs or knee flexors-to-knee extensors ratios. The limitation of knee flexors-to-knee extensors ratios was explained by the inability of aneroid sphygmomanometer test to measure quadriceps strength at 30° knee flexion with consistency, due to many participants exceeding the readings on the sphygmomanometer scale. This method has a great potential, but requires further studies to be useful as a muscle strength assessment and injury risk screening procedure.
Part 2: Anatomic and Physiologic Variations of the Hamstrings and Potential Implications for Injury Risk
In this second part, we address the main variations or variants of the hamstrings’ anatomy and physiology, which imply that there is a “normal” or “usual” state of affairs. We start by presenting the commonly described anatomic features of the hamstrings, before engaging in an exploration of their variations.
Mainstream Anatomic Description of the Hamstrings
We overview the basic hamstrings anatomy as described in the 41st Edition of Gray’s Anatomy (Standring, 2015). Throughout this section, the information derives from this source, unless otherwise stated. The hamstrings, or ischiocrural muscles, comprise the muscles of the posterior compartment of the thigh, and include the ST, SM and BF (long head – BFlh; short head – BFsh), which attach proximally to the ischial tuberosity (except the BFsh). The ST, SM and BFlh are biarticular muscles, and act in extending the coxofemoral joint (hip), as well as flexing and rotating (medially and laterally) the knee. Distally, the ST and SM attach to the tibia, while both heads of the BF attach to the fibula. The hamstrings present relevant interindividual variation in length. The hamstrings are innervated by the sciatic nerve, emerging at the level of S1 vertebra, although with interindividual variations.
Functionally, the hamstrings play an important role in transferring load between the trunk and the lower limbs, and affect the tension of the thoracolumbar fascia. They affect the normal lumbar lordosis, as their length and strength interferes with the position of the innominate bone. When raising the trunk, the hamstrings act in conjunction with the gluteus maximus. It is highlighted that the hamstrings strongly contract in actions involving the need to extend or control the rate of flexion at the hip, while the gluteus maximus contracts when powerful extension of the hip joint is required. The adductor magnus also performs hip extension, has attachments to the ischial tuberosity, and the ischial portion of the adductor magnus shares innervation from the tibial division of the sciatic nerve. The adductor magnus can be considered to have a proper hamstrings portion (Broski et al., 2016; Jeno and Schindler, 2020). Pathology or diminished functional capacity of the adductor magnus and/or the gluteus maximus may result in a greater demand upon the hamstrings. The coordination of the hamstrings with other muscles of the lumbopelvic region may be relevant in understanding hamstrings injuries (Thelen et al., 2006; Shield and Bourne, 2018). Figure 1 presents an overview of the hamstrings muscles.
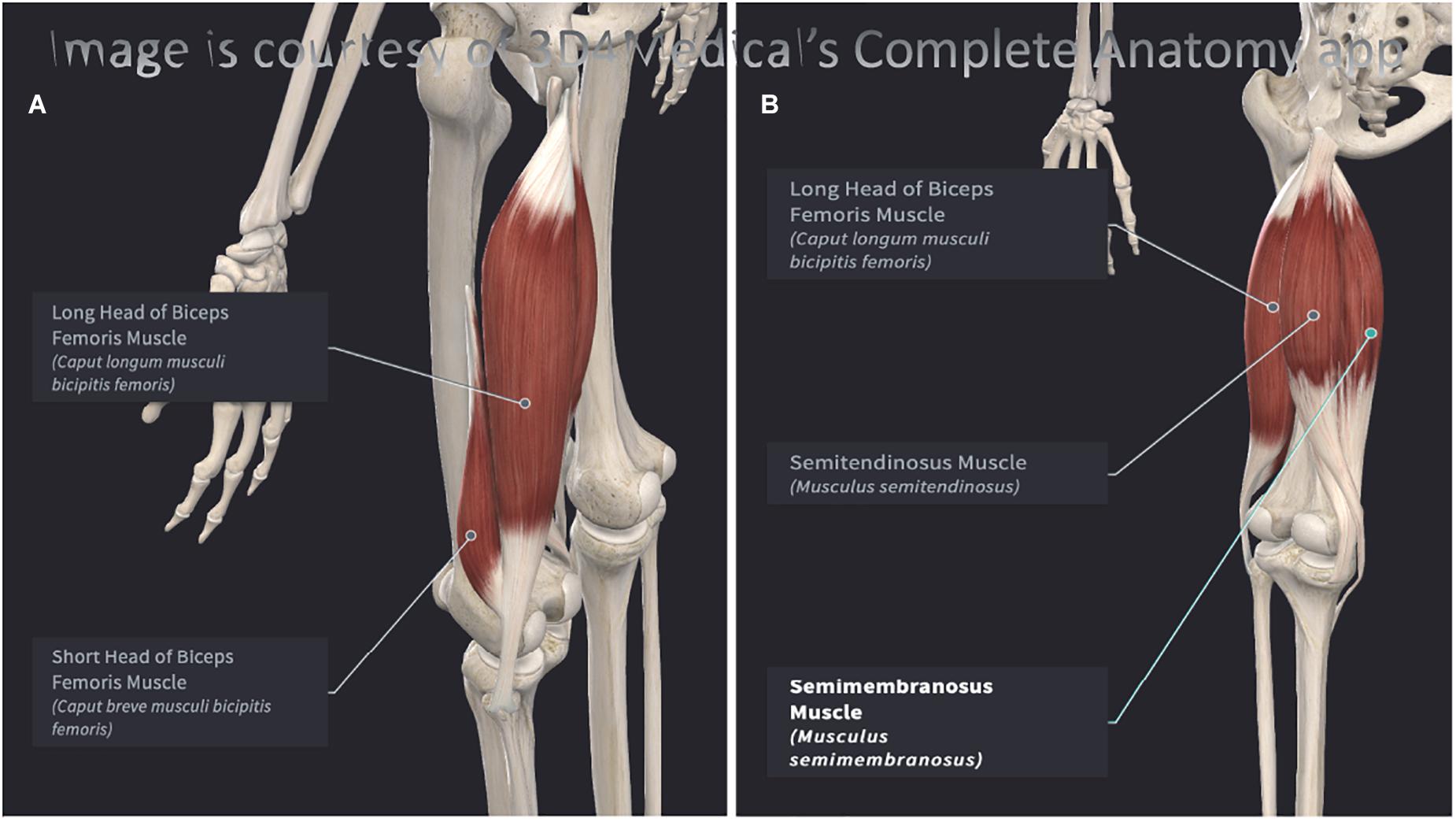
Figure 1. (A) Posterolateral view of the left hamstrings. (B) Posteromedial view of the left hamstrings. Both images were elaborated with Complete Anatomy 2021, version 7.0.0. (desktop version for Mac OS) and reproduced here with permission (3D4Medical, Elsevier).
Semitendinosus
The ST has a posteromedial position in the thigh and has a long tendon. Proximally, its tendon is shared with the BFlh, but then these muscles diverge. In the first ±7.5 cm of their path, they share an aponeurosis. The belly of the ST usually spans only until the mid-thigh, after which its long tendon runs until its attachment in the upper part of the medial surface of the tibia, behind the attachment of the sartorius muscle and distal to the attachment of gracilis muscle. The terminal portion the ST tendon is united with the tendon of gracilis (further reinforcing the functional connections between the hamstrings and the adductor group), provides an expansion to the deep fascia of the leg and to the medial head of the gastrocnemius, and anatomically (and perhaps functionally) links the ST with the medial gastrocnemius. It is open to speculation whether pathology or dysfunction of the medial gastrocnemius interfere with the action of the ST. Usually, the midpoint of the ST receives a muscular slip from the BFlh, denoting a role in lateral force transfer.
Innervation to the ST is provided by the sciatic nerve (L5, S1, S2), through its tibial division. This pattern is shared with the SM, which lies deep to the ST, and by the BFlh, but not by the BFsh. Beyond the actions common to all hamstrings, the ST (as well as the SM) can medially rotate the knee when this joint is semi-flexed. With the hip extended, ST (and SM) can act to produce medial rotation of the thigh.
Semimembranosus
The SM also lies posteromedially in the thigh, deep to the ST. Proximally, it exhibits a long and flat tendon attached to the ischial tuberosity, and it receives fibrous expansions that flank the adductor magnus. Distally, the SM has a ramified pattern, sharing fibers with both ST and BFlh. Circa the mid-thigh, the SM gives off muscle fibers that converge to a second aponeurosis that attaches distally over the terminal tendon. The SM distal tendon divides into five components: anterior, direct, capsular, inferior and the oblique popliteal ligament (Beltran et al., 2003). The SM has a close anatomic relationship with the medial gastrocnemius, usually separated by a bursa.
Gray’s Anatomy describes that the SM can vary considerably in size and may be absent (which could potentially overload the ST) or double (which could potentially underload the ST). Proximally, the SM can arise from the sacrotuberous ligament instead of the ischial tuberosity. It can have muscular slips to the femur or to the adductor magnus. Although myotendinous and avulsion injuries are common in the SM, complete tears are seldom reported in the literature (Beltran et al., 2003).
Biceps Femoris
Unlike the ST and SM, the BF occupies a posterolateral position in the thigh. Proximally, the BFlh attaches to the ischial tuberosity, through a common tendon with the ST, but it can also insert into the sacrotuberous ligament. The BFlh has a fusiform belly, and its fibers terminate in an aponeurosis that also receives fibers from the BFsh. Pennation angle of the BFlh fibers is non-uniform, being greater in the proximal-middle sections, in comparison to the distal and extreme proximal sections (Huygaerts et al., 2021). The BFsh has its proximal attachment in the lateral lip of the linea aspera and this attachment may extend upward to almost the level of gluteus maximus. Distally, these muscles share a common tendon inserting into the head of the fibula and send expansions to the fibular collateral ligament and to the lateral condyle of the tibia. A variation noted in Gray’s Anatomy description is the absence of the BFsh.
While the BFlh shares innervation with the ST and SM, arising from the tibial division of the sciatic nerve (L5, S1, S2), the BFsh is innervated by nerves emerging from the same levels, but traveling in the common fibular division of the sciatic nerve. This differential innervation of the two heads of the BF may result in asynchrony and impaired coordination (Beltran et al., 2012; Huygaerts et al., 2021), potentially placing the BF at greater risk of injury (Burkett, 1975; Entwisle et al., 2017). Theoretical models have proposed that BF may be at increased injury risk in comparison with ST and SM (Dolman et al., 2014), owing to an additional BF compensation induced by a poor ST endurance, placing the BF at higher injury risk (Schuermans et al., 2014). In a retrospective study with 275 men soccer players who had sustained hamstrings injuries, the BFlh was the most commonly affected (56.5%), followed by the ST (24.4%), SM (13.7%), and BFsh (5.6%) (Crema et al., 2016). In Australian rules football players, injury of the BF represented 78% of all hamstrings injuries (Verrall et al., 2003). Beyond the actions common to all hamstrings, the BF can laterally rotate the knee when this joint is semi-flexed. With the hip extended, BF can act to produce lateral rotation of the thigh.
Anatomic and Physiologic Variations of the Hamstrings
The hamstrings integrate the posterior compartment of the thigh, considered to be the most variable compartment (Tubbs et al., 2016). We explore known anatomic variations to unfold their implications for injury risk. It is unlikely that any single risk factor allows establishing a strong relationship with injury risk, but recognizing their existence may provide a more thorough understanding of individualized injury risk. Technological developments may translate that enhanced knowledge into practical applications. Table 1 summarizes the articles exploring anatomic variations of the hamstrings.
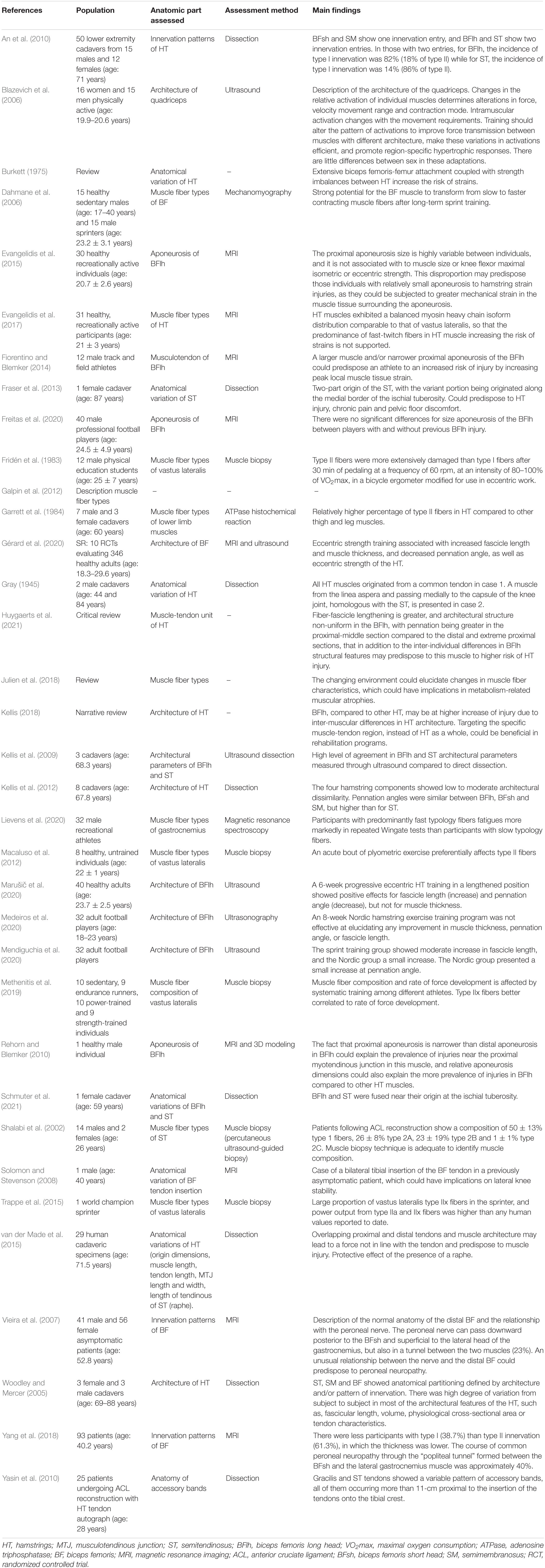
Table 1. Summary of studies cited in Section “Anatomic and Physiologic Variations of the Hamstrings.”
Muscle Bellies
Cadaveric analysis showed that the extension of BFsh attachments to the femur vary substantially between individuals, leading to the hypothesis that individuals with more extensive attachments may apply more force, potentially increasing the risk of a strain injury (Burkett, 1975). The opposite interpretation is also possible, as attachments that are more extensive would allow the BFsh muscle belly to be more firmly attached to the femur, and therefore may be at less risk of a strain injury. The two heads of the BF have different proximal attachments and innervation, possibly representing muscles that were independent, but fused during the human evolutionary process (Tubbs et al., 2016). In some individuals the BFlh and BFsh remain separate, and occasionally the BFsh is absent (Tubbs et al., 2016). From 29 cadaveric specimens with a median age of 71.5 (range from 45 to 98), BFlh and BFsh extended approximately 42.0 and 29.8 cm, respectively (van der Made et al., 2015).
The ST can be partly fused with the SM (Tubbs et al., 2016) or the BFlh (Schmuter et al., 2021), and may present accessory slips to the coccyx, sacrotuberous ligament or to the ischial tuberosity (Fraser et al., 2013). Supernumerary ST bellies have been observed (Gray, 1945). Although ST and BFlh usually share a common proximal tendon attachment and aponeurosis, complete separation of these two muscles has been reported (Tubbs et al., 2016). Of note, the tendon of the ST may receive muscle slips from the quadratus femoris (Tubbs et al., 2016).
The SM can be doubled, absent, or split, and up to four bellies have been described inserting into the adductor magnus, planum popliteum and tibia (Tubbs et al., 2016). The ST, SM and BFlh may originate from a common tendon, which can be continuous with the intermuscular septum and, occasionally, envelop the piriformis muscle (Tubbs et al., 2016), providing another example of the connections between the hamstrings and other muscles of the lumbo-pelvic region.
Muscle Fiber Type
The muscle fibers vary in their morphology and histochemical properties (Galpin et al., 2012). Classifications of fiber muscle types have evolved through the years and certain classifications are still debated (Talbot and Maves, 2016). Here, we use the original classification reported by the authors being cited. There are important functional differences between different muscle fiber types, such as distinct metabolic properties (Mishra et al., 2015). There may be a bidirectional relationship, whereby metabolic environment also influences the characteristics of the muscle fibers (Julien et al., 2018). Type II muscle fibers are more easily fatigued than type I fibers (Lievens et al., 2020), and more susceptible to plyometric- (Macaluso et al., 2012) as well as eccentric-induced muscle damage (Fridén et al., 1983). Despite this information, eccentric actions have been emphasized by many programs for reducing injury risk of the hamstrings (van der Horst et al., 2015; Almeida et al., 2018; Elerian et al., 2019). Perhaps athletes with greater percentage of type II fibers should follow a more careful monitoring of the eccentric work they perform.
A previous cadaveric study with seven men and three women (37 to 76 years upon death) showed that type II fibers composed 48.5 to 59.5% of the proximal BFlh, 51.0 to 58% of the distal BFlh, 45.5 to 69.0% of the BFsh, 51.0 to 57.5% of the proximal ST, 50.0 to 69.5% of the distal ST, 47.5 to 54.5% of the proximal SM, and 44.0 to 55.5% of the distal ST (Garrett et al., 1984). In a study with 15 sedentary men aged 17 to 40 years old (Dahmane et al., 2006), the BF had a mixed fiber composition of ∼50% type 1 and ∼50% type 2 (25.2 ± 1.3% type 2a, 20.7 ± 1.4% type 2x and 5.7 ± 0.7% type 2c), meaning that BF has a considerable amount of fast-twitch fibers. Biopsies of the BFlh performed in 31 healthy, young men, showed a balanced distribution of myosin heavy chains (MHC), with 47.1 ± 9.1% MHC-I, 35.5 ± 8.5% MHC-IIA, and 17.4 ± 9.1% MHC-IIX (Evangelidis et al., 2017). For the ST, a composition of 50 ± 13% type 1 fibers, 26 ± 8% type 2A, 23 ± 19% type 2B and 1 ± 1% type 2C was found on biopsies from 16 patients 7–11 months after ACL surgery (Shalabi et al., 2002). In this reported ST composition (Shalabi et al., 2002), the standard-deviations of the reported ST muscle composition were relevant, especially in type 2B fibers, denoting interindividual variation.
It has been suggested that high-level sprinters are sharply different than the average person, with a percentage of up to ∼70% of type 2 fibers in the lower limb muscles, but this was derived from analysis of the vastus lateralis (Trappe et al., 2015), and should not be generalized to other lower limb muscles. Differences in fiber type composition of the lower limbs have been observed between endurance runners, power-trained individuals, and strength-trained individuals (Methenitis et al., 2019), but again these findings were extrapolated from observations of the vastus lateralis. In vivo knowledge of hamstrings muscle composition in humans remains largely unknown (Evangelidis et al., 2017).
As Lievens et al. (2020) pointed out, athletes with distinct muscle typology should train differently, and the individualization of training on the basis of this information is important to optimize performance and lowering the risk of potential injury. Unfortunately, knowledge of muscle fiber composition of the human hamstrings is scarce for building a broad picture. Furthermore, feasibility may require the development of more readily available, non-invasive, non-expensive technologies.
Pennation Angles
A study analyzed the pennation angles of BFlh and ST muscles from six legs derived from three male cadavers (Kellis et al., 2009). The BFlh and ST exhibited very similar pennation angles through cadaveric dissection (13.52 ± 2.35° versus 13.39 ± 3.31°) and ultrasound (13.88 ± 2.76° versus 13.34 ± 2.61°). The small standard deviation was suggestive of non-relevant intra- and interindividual variations. A posterior study of the same group dissected eight cadavers (age: 67.8 ± 4.3 years) (Kellis et al., 2012) and demonstrated that pennation angles of the BFlh, BFsh and SM were similar (13.46 ± 2.88°, 13.17 ± 2.60°, and 15.95 ± 2.39°, respectively), but substantially different from the pennation angle of the ST (9.14 ± 3.54°), which differs from the results found in their previous work (Kellis et al., 2009). The authors used a combination of mean fiber length, sarcomere length, physiological CSA, and pennation angle to calculate a similarity index (δ) between pairs of muscles, with lower values denoting greater similarity. While the BFlh and BFsh had a δ = 0.54, and BFlh and SM had a δ = 0.35, denoting a moderate similarity, there was low similarity between SM and ST (δ = 0.98) and between BFlh and ST (δ = 1.17). These findings underline that although the hamstrings are usually treated as a muscle group, there are relevant inter-muscular architectural differences between its individual muscles (Kellis et al., 2012).
A SRMA showed a limited to moderate confidence in evidence that eccentric training performed for a minimum of 4 weeks decreased the BFlh pennation angle (Gérard et al., 2020), which was also shown in a recent study (Marušič et al., 2020). However, another study with 32 soccer players (age, 18–23 years) performing an 8-week NHE program once a week versus twice a week showed no between-group differences in BFlh pennation angles (Medeiros et al., 2020). A prospective controlled study with soccer players analyzed the NHE and sprint interventions, showing that only the NHE induced small increases in the BFlh pennation angle (Mendiguchia et al., 2020), contradicting the decreases seen in previous studies (Gérard et al., 2020; Marušič et al., 2020). Results are conflicting, largely limited to the BFlh and involve a narrow set of exercise modalities. Further research is warranted to understand how different exercise modalities affect pennation angles.
Tendons
There is variation in the accessory bands of the hamstrings tendons (Yasin et al., 2010), as well as in tendon length. One study showed that the muscle belly of the SM originated at varying distances from the ischial tuberosity in different subjects, ranging from 8.6 to 14.5 cm (Woodley and Mercer, 2005). Interindividual variations in tendon-to-fiber length ratios may play a role in injury risk, as in the case of tendons of similar structure, tendon length critically influences compliance (Huygaerts et al., 2021). If two athletes have different ratios for the ST, it is possible that one will be at increased risk of injury than the other. It was hypothesized that bigger tendon-to-fiber length ratios provide a greater buffer to the muscle belly, potentially affording increased protection from injury, but this requires confirmation (Kellis, 2018; Huygaerts et al., 2021).
Aponeurosis
The aponeurosis may affect different muscle regions distinctly, demanding greater elongation of fibers in certain regions and less so in others (Blazevich et al., 2006; Huygaerts et al., 2021). A modeling study suggested that smaller ratios of aponeurosis to muscle width generated larger maximum peak local strain, postulating those larger muscles and/or narrower aponeurosis increased risk of injury (Fiorentino and Blemker, 2014). Interindividual variation in anatomic structure may put individuals with distinct aponeurosis to muscle width ratio at different levels of injury risk. However, an MRI study conducted in 30 healthy young men performing maximum voluntary actions of knee flexion showed interindividual variability in the area of the BFlh proximal aponeurosis, ranging from 7.5 to 33.5 cm (Evangelidis et al., 2015), and this area was not correlated with BFlh maximal anatomic CSA. The aponeurosis-to-muscle area ratio exhibited six-fold variability, with an interindividual ratio variation of 83%, and aponeurosis size was not related to isometric or eccentric knee flexion strength (Evangelidis et al., 2015). The authors stated that “individuals with a relatively small aponeurosis may be at increased risk of HSI” (Evangelidis et al., 2015, p. 1383), but this was not demonstrated.
A study using MRI to compare 80 thighs from 40 professional soccer players with (n = 9) or without previous (n = 71) BFlh injury in the preceding 3 years, suggested that proximal aponeurosis size of the BFlh was not an independent risk factor for HSI (Freitas et al., 2020). Notwithstanding, another computational modeling study suggested that varying the width, length and thickness of the BFlh aponeurosis had an impact on the location and magnitude of peak stretches within the muscle (Rehorn and Blemker, 2010). The authors found that location and magnitude of peak stretch could be explained by the difference in widths between the proximal and distal aponeurosis of the BFlh (Rehorn and Blemker, 2010). Aponeurosis characteristics may not represent an independent risk factor, but their interaction with factors such as tendon length, muscle belly anatomic CSA, among others, may provide further cues to better understand its relationship with hamstrings injury.
Innervation Patterns
Interindividual differences in innervation patterns of the hamstrings should be acknowledged, and their relationship with injury explored (Huygaerts et al., 2021). In some persons, the BFsh has two distinct regions, each innervated by a separate nerve (Woodley and Mercer, 2005). In the same study, two of the six subjects had a common trunk for nerve supply to SM and an inferior compartment for ST (Woodley and Mercer, 2005). The nerve to SM had branches to the adductor magnus muscle, highlighting the functional connections between the adductor magnus and the hamstrings. Woodley and Mercer (2005) showed that the primary branch of the nerve to SM, that supplied its distal region, had varied entry points (i.e., the location where the nerve branch pierces the muscle belly), from 22.5 cm distal to the ischial tuberosity in one, and 34.5 cm in another. Similar variations were found for both ST and BF (Woodley and Mercer, 2005). In a dissection of 50 cadaveric lower limbs, motor entry points and intramuscular nerve endings of the hamstrings were examined (An et al., 2010). In ST and BFlh, two distinct branching nerve patterns were found, classified into type I (only one primary motor branch emerging from the sciatic nerve) and type II (two primary motor branches) (An et al., 2010). In the BFlh, 82% of lower limbs presented a type I innervation, while in ST 86% had a type II innervation (An et al., 2010). Whether (and to what extent) subjects with different pattern type present alterations of motor coordination or how they affect functional performance is currently unknown.
In one study, two observers retrospectively reviewed one hundred 1.5-T knee MRI studies in 97 asymptomatic subjects (41 men and 56 women) for assessing anatomy of the distal BF (Vieira et al., 2007). The posterior extent of the BFsh was ≤1 cm in 50% of subjects, between 1–2 cm in 34%, between 2–3 cm in 15%, and ≥3 cm in one subject. The distal extent of the muscle belly of BFsh from the joint space varied from −2 cm in 5% of subjects to +2 cm in 2%, with 51% presenting 0 cm, and ∼42% showed +1 or −1 cm. The length and path of the BFsh showed interindividual variation in asymptomatic subjects. In this distal MRI assessment (Vieira et al., 2007), the muscle belly of the BFlh was identified in 40% of the subjects, and not visible in 60% of the subjects, suggesting that interindividual differences exist for muscle belly-to-distal tendon length ratios for the BFlh. In 77% of subjects the common peroneal nerve was situated superficial to the lateral head of the gastrocnemius and posterior to the BFsh; in the other 23% of subjects, a narrow tunnel between the lateral head of the gastrocnemius and the BFsh enveloped this nerve, but this tunneling effect did not result in neuropathy (Vieira et al., 2007).
A similar study retrospectively analyzed 1.5-T knee MRI scans of 93 Korean subjects, divided into types according to the course of the common peroneal nerve: type I (no tunnel) and type II (tunnel) (Yang et al., 2018): ∼40% of subjects were classified as type II, which is superior to the percentage observed in the aforementioned study (Vieira et al., 2007). This suggests that the prevalence of certain anatomic features may vary geographically (possibly related to genetic, environmental, and historical factors). In this study (Yang et al., 2018), type II subjects had significantly greater BFsh thickness. The functional relevance of these anatomic variations is not straightforward.
Attachment Sites
Despite traditional textbook description of the BF distal tendon as attaching to the fibular head (Standring, 2015), at least one case is described where the distal tendon of the BF inserted on the lateral aspect of the tibia, posterior to the iliotibial band and above the level of the fibular head (Solomon and Stevenson, 2008). In this case, the BF did have attachments to the fibular head, but these were muscular in nature. Whether this feature interferes with the mechanics of knee lateral rotation, implicates in the proximal actions (i.e., at hip joint level), or changes the coordination with other hip lateral rotators muscles (e.g., gluteus maximus, piriformis), remains speculative.
Sex and Age-Related Differences in Hamstrings’ Anatomy and Physiology
This section addressed sex and age-related differences in hamstrings’ features, and Table 2 summarizes the articles consulted in this section.
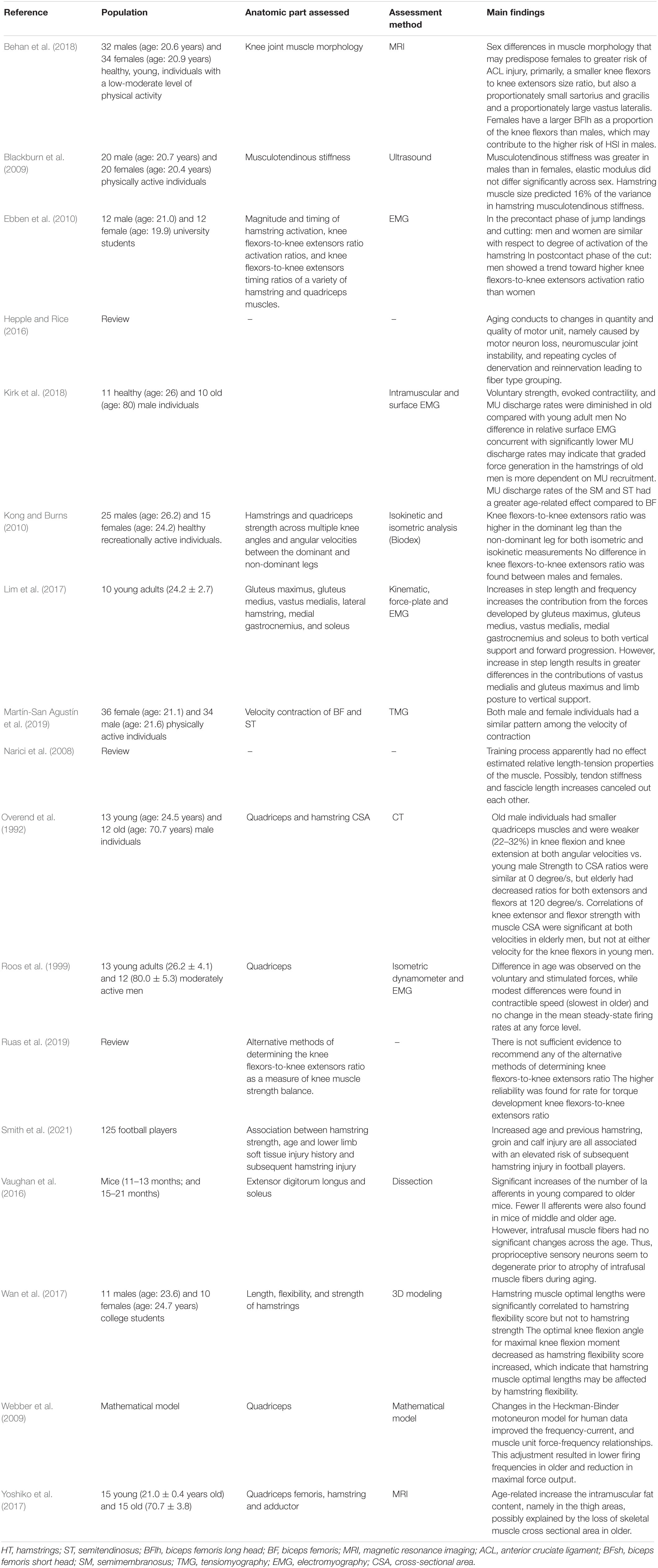
Table 2. Summary of studies cited in Section “Sex- and Age-Related Differences in Hamstrings’ Anatomy and Physiology.”
Sex-Related Differences in Hamstrings’ Anatomy and Physiology
A study with recreational athletes (11 men and 10 women) assessed the relationship between hamstrings optimal length and hamstrings flexibility and isokinetic strength (Wan et al., 2017). While hamstrings muscle optimal length correlated with hamstrings flexibility, these factors did not demonstrate a relationship with hamstrings strength. For the same flexibility score, women had shorter hamstrings optimal muscle length than men. Thus, at any given ROM during a movement, hamstrings muscle maximal strain may differ between sexes. Another study used tensiomyography to assess normalized response velocity in BF, ST, rectus femoris, vastus medialis and vastus lateralis muscles of recreationally active young adult women (n = 36) and men (n = 34) (Martín-San Agustín et al., 2019). Comparisons between women and men were adjusted by height and mass. Sex-related differences were observed in velocity of action, with women having >15% differences between BF-to-quadriceps ratio, as well as ratios in the hamstrings, in comparison to men. These ratios should probably be termed knee flexors-to-knee extensors ratios, as more muscles than merely the hamstrings and the quadriceps are involved in the regulation of knee flexion and extension (Standring, 2015).
Sex-based differences in magnitude and timing of hamstrings and quadriceps activation during drop jump, sprint, and cutting (45°) tasks were assessed in 24 young adults (12 men, 12 women) (Ebben et al., 2010). In the post-contact phase of the cutting movement, men showed greater activation of all the hamstrings in comparison to women, while women produced longer bursts of the rectus femoris and vastus medialis activation. Hamstrings’ stiffness was shown to be greater in men than in women, but without differences in stress, strain, and elastic modulus (Blackburn et al., 2009). Blackburn et al. (2009) speculated that the smaller hamstrings stiffness observed in women could compromise their ability to resist changes in length associated with joint perturbation. However, the authors recognized that the sex-related differences in hamstrings stiffness could be partly attributed to anatomic CSA (Blackburn et al., 2009). It has been suggested that age or training level are more relevant than sex to explain differences in knee flexors-to-knee extensor ratios (Kong and Burns, 2010). It is also possible that the specific method used to determine knee flexors-to-knee extensors ratios (e.g., ratios calculated by angle-specific torque, rate of torque development) provide different results [for more information, see Ruas et al. (2019)].
Other evidence suggests that sex-related anatomic differences play a prominent role in explaining the differences in knee flexors-to-knee extensors ratios between men and women. A study with 1.5T MRI of healthy, but untrained young men (n = 32) and women (n = 34), showed sex-related differences in the maximal anatomic CSA of knee flexors and extensors (Behan et al., 2018). Women had a smaller ratio of knee flexors to knee extensor anatomic CSA. Although the hamstrings are not the only knee flexors, they play a prominent role in this action. In comparison with men, women showed a greater proportion of vastus lateralis, BFlh and SM in relation to their respective muscle groups. Conversely, women showed a lesser proportion in sartorius, gracilis and BFsh.
Effects of Aging in Hamstrings’ Structure and Function
There is limited evidence regarding the effect of aging in hamstrings’ anatomy, although ages >25 years have been associated with increased risk of hamstrings injury (Smith et al., 2021). Kirk et al. (2018) found that voluntary strength, evoked contractility, and motor unit (MU) discharge rates were diminished in a group of 10 elderly (mean age: 80 ± 5 years) compared to a group of 11 young men (26 ± 4 years). These findings could be due to the infiltration of non-contractile tissue in aged hamstrings (Overend et al., 1992; Yoshiko et al., 2017), altered MU facilitation, age-related remodeling (Webber et al., 2009; Hepple and Rice, 2016), muscle fiber membrane dysfunction, decreased sarcoplasmic reticulum function, altered calcium ion kinetics, and changes in connective tissue elements (Narici et al., 2008; Hepple and Rice, 2016). Hamstrings have a significantly lower MU discharge rates in the elderly, as opposite to findings in the vastus medialis portion of the quadriceps (Roos et al., 1999). In vitro and animal studies suggest that the loss of proprioceptive sensory neurons and innervation differences occur at different rates between flexors and extensors during the aging process (Vaughan et al., 2016).
Additionally, ST and SM could be more affected by aging than BF, providing evidence that musculature and neuromuscular system could be differently impacted by aging (Kirk et al., 2018). As a longer step length may require higher contributions from the hip and knee extensor musculature (Lim et al., 2017), hamstrings modifications with aging, and the decreased muscle strength, may explain why elderly people choose shorter length steps and walk more slowly (Lim et al., 2017). These findings warrant further investigation.
The Consequences of Previous Knee Surgeries
Knee surgeries often harvest hamstrings tendons, potentially increasing the risk for future hamstrings injuries. When harvesting hamstrings tendons for surgical purpose, such as patellar tendon (Friedman et al., 2020) or ACL reconstruction (Keyhani et al., 2020), iatrogenic nerve injuries can occur (Colombet and Graveleau, 2016; Ruffilli et al., 2017). For example, the common fibular nerve emerges posterior to the BF distal tendon, to which it adheres (Standring, 2015); collecting part of the BF tendon for knee surgeries presents considerable risks. Consequently, the ST has been a common choice (comparable to gracilis in terms of effects) for transfer in surgical treatments (Yasin et al., 2010; Colombet and Graveleau, 2016), including those for the ACL (Horteur et al., 2020; Keyhani et al., 2020), medial collateral ligament (Cao et al., 2016) and patellar tendon (Jain et al., 2014; Friedman et al., 2020).
In a study of female soccer players (n = 90) that had undergone ACL reconstruction, with data available for a minimum of a 2-year follow-up, the outcomes for hamstrings autograft and bone-patellar tendon-bone autografts were very similar (Britt et al., 2020). Notwithstanding, a meta-analysis of 5,561 patients undergoing ACL reconstruction found that hamstrings autografts were less likely than bone-patellar tendon-bone autografts to incur in a contralateral ACL rupture (Zhou et al., 2020). The safety of surgical procedures and its effects on the specific injury addressed should not be disregarded (Jain et al., 2014). Nonetheless, these autografts may increase the fragility of the hamstrings and put them at increased risk of sport-related injuries. One study assessed recreationally active participants (five men and nine women) that had returned to sport after unilateral ACL reconstruction using ST tendon autografts (Messer et al., 2020). The athletes had undergone surgery between 12 to 78 months prior to the study and MRI was used to compare the surgical limb to the other limb. The surgically treated limbs’ STs had significantly smaller anatomic CSA and muscle volume than non-surgical limbs, and the surgically treated limbs also exhibited a lower exercise-induced transverse relaxation time. Surgically treated limbs also exhibited higher volumes of the SM and BFsh, perhaps to compensate for the lower volumes of the ST (Messer et al., 2020).
Using ST autografts for ACL reconstruction has long-term consequences for the hamstrings of the surgically treated limb, such as ST and gracilis hypotrophy (Sherman et al., 2021). Although alternatives such as peroneus longus autografts are being explored for ACL reconstruction (Rhatomy et al., 2019), it is possible that could bring some problems for the ankle and foot, since peroneus longus (a.k.a., fibularis longus) acts in eversion and plantar flexion of the foot and also provides support to the longitudinal and transverse arches of the foot (Standring, 2015). Trade-offs are unavoidable, and their consequences should be acknowledged and addressed by rehabilitation programs, requiring multifactorial approaches including different modalities of strength training, variation in the exercises, balance knee- and hip-dominant exercises, and careful managing of loading (Buckthorpe et al., 2020).
Albeit inadvertently, surgical procedures that extract tissue from the ST may compromise the endurance of this muscle (Vairo, 2014; Lee and Lee, 2020). Consequently, the BF will produce greater force and for a longer period to compensate for this reduced capacity of the ST (Schuermans et al., 2014). This could lead to the BF fatiguing earlier and/or being exposed to loads that exceed its capacity. Paradoxically, this may expose the “healthier” muscle (i.e., BF) to increased injury risk, and may explain why the majority of acute HSI occur in the BFlh (Freitas et al., 2021; Huygaerts et al., 2021). Still, a study with healthy subjects performing an indoor running task showed that the largest peak strain was achieved by the BF, while the highest peak force and the most power and work were generated by the SM (Schache et al., 2012), so this issue is open to debate.
Synopsis of the Second Part
The hamstrings complex comprises the posterior compartment of the thigh, consisting of the ST, SM, and BF (BFlh and BFsh) muscles. They are biarticular muscles that act as hip extensors and knee flexors and rotators and play a critical role in several daily and sports activities. Regarding the main hamstrings anatomic and physiological variations discussed in the previous sections, it was shown that a high degree of variability exists in many of the architecture variables addressed. Lower tendons and aponeurosis to muscle ratios, higher number of type II fibers, variations in attachment sites and innervation patterns, and knee surgeries in which portions of the ST are extracted, could place the hamstrings complex musculature, especially the BF muscle, at increased risk of injury. Additionally, neuromuscular variations in women and the aging process affect the hamstrings musculature, further increasing the risk of hamstrings injury in women and elderly people.
The high level of anatomic variability from subject to subject and the variability of the study designs used in the literature, makes it difficult to draw general recommendations, and advises against adopting one-size-fits-all exercise programs. Since most sports-related injuries have a clear multifactorial nature (Monajati et al., 2016; Green et al., 2020; Lahti et al., 2020), studies may fail to find a clear relationship between the injury and any given risk factor. This does not imply that a particular risk factor is irrelevant in the probability of suffering a hamstrings injury. Although the study of resting muscle architecture of the hamstrings may provide relevant insights, it is unclear whether this provides valid information for dynamic architecture and gearing during dynamic movements (Huygaerts et al., 2021).
Concluding Remarks
Hamstrings injuries present a challenge in sports science and practice, and many exercise-based programs have been proposed to mitigate injury risk, focusing on modifiable injury risk factors. But scientifically reported data shows that non-modifiable risk factors potentially play a more relevant role than modifiable risk factors. This suggests that greater efforts should be implemented to understand and identify the non-modifiable risk factors, such as relevant anatomic variations (e.g., tendons, aponeurosis, fiber types). The possession of this enhanced knowledge may help designing better-individualized exercise interventions, considering the non-modifiable particularities of the athlete. If a certain anatomic variation puts the athlete at greater risk of injury (e.g., nerve entrapments or tunneling), training programs can design better-individualized stimuli instead of delivering one-size-fits-all solutions. The recognition and assessment of non-modifiable risk factors allows coaches to act upon them, i.e., to prescribe exercise programs that are well-suited for those identified variations. As an example: if athletes with a greater percentage of type II fibers incur in greater damage induced by eccentric exercise, coaches can reduce the weekly volume, intensity and/or frequency of eccentrically biased exercises. Figure 2 synthesizes the concepts and domains approached in our work.
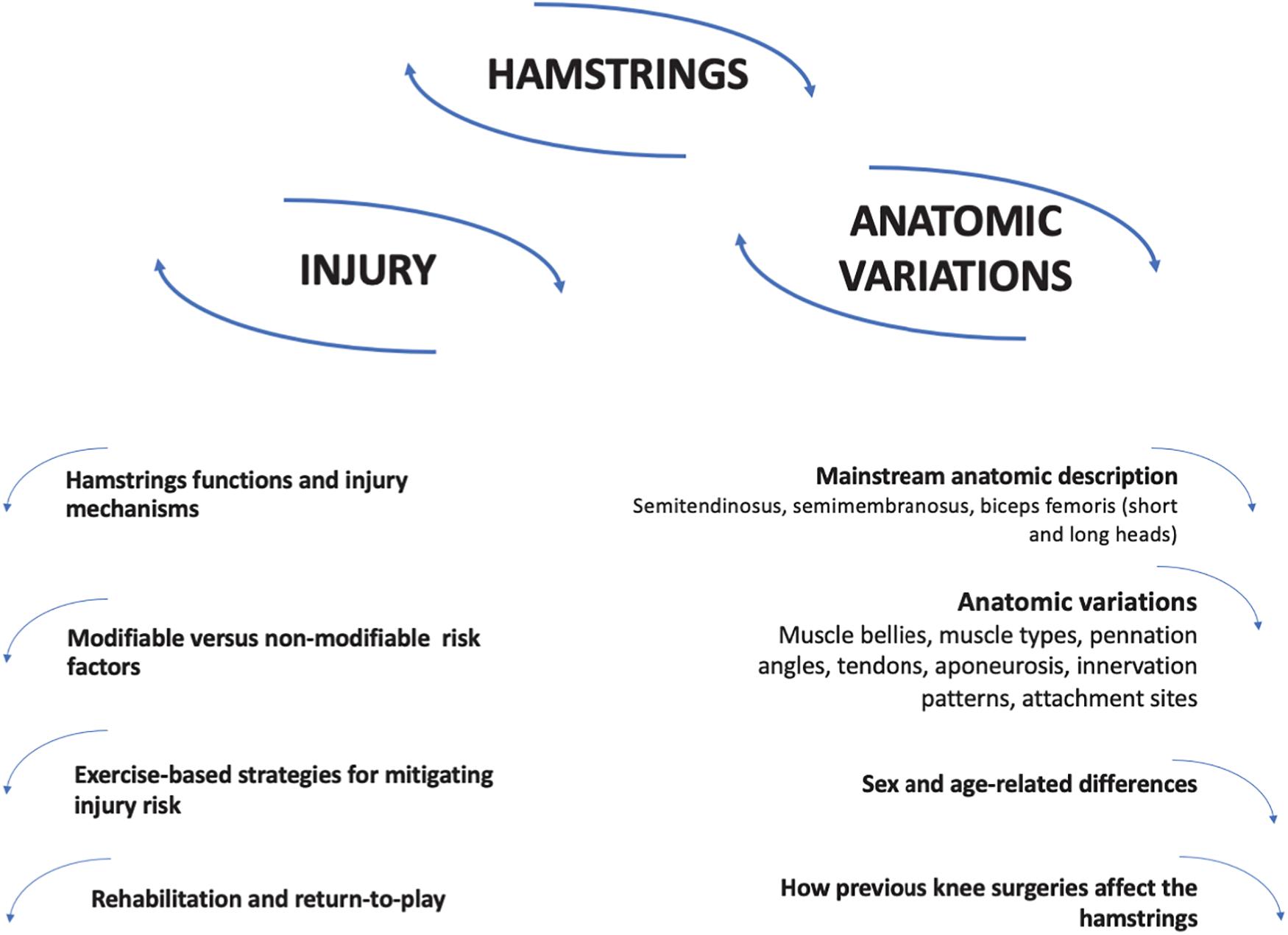
Figure 2. Overview of concepts and hamstrings anatomic and physiologic variations.
The literature has identified the need for prospective studies evaluating the influence or architectural variables in hamstrings injury, as well as the importance of targeting architectural changes in injury reduction programs, highlighting that ultrasound is potentially the most reliable technique to detect such changes (Behan et al., 2019). In the case of non-modifiable anatomic variations (e.g., number of muscular insertions into bone), it would be important to explore differential responses to exercise protocols, providing coaches with the tools for better individualizing training prescription. Of course, it is quite complicated to carry out the “gold-standard” study designs required to detect risk factors and validate screening tools (Bahr, 2016), as large-scale prospective, long-term, randomized studies assessing multiple outcomes at multiple time points are very difficult to implement. Still, this should not discourage researchers from progressively better and more complete attempts to address this complex, yet fascinating topic. We therefore encourage researchers to develop more large-scale prospective studies, including some of the mentioned architecture variables, with reliable yet non-invasive techniques such as ultrasound, to widen the body of knowledge regarding this subject matter.
As limitations of this work, we did not perform a systematic review of the literature, given the scope and goals. It is possible that relevant information has eluded our searches, although we tried our best to provide and thorough and balanced account. Where controversies existed, we attempted to explore its complexities and provide contradictory accounts.
Practical Implications
Improved knowledge of interindividual variations in hamstrings anatomy and physiology will help coaches designing better individualized exercise programs. As an example, athletes with greater percentage of type II muscle fibers in the hamstrings should probably be allowed greater recovery times between sessions of eccentrically biased exercise. Muscle bellies with more extensive attachments to the femur may provide some degree of injury protection when producing forces of great magnitude, but this requires further exploration. Pennation angles, tendon-to-fiber length ratios, attachment sites and features of the aponeurosis, as well as the interaction between these factors, have unclear relationships with injury risk, with further research required before practical implications are promoted. The extensive anatomic and neurologic connections between the hamstrings and the gluteal and adductor muscles suggests that training programs should include exercises that demand the interaction of these three muscle groups, instead of relying solely on more hamstring-dominant exercises (e.g., the NHE).
While coaches tend to focus on modifiable risk factors, such as strength and endurance, non-modifiable risk factors may be acted upon, by designing exercise interventions that better comply with the identified characteristics. For example, in the case of athletes with previous knee injuries using ST autografts (non-modifiable factor), coaches should recognize that hamstrings endurance may be compromised, designing exercise interventions that gradually improve their endurance, but also recognizing that those athletes may benefit from shorter training sessions and/or shorter durations of play in matches. Improvements in the quality, availability and costs of imaging techniques will expand the assessment of interindividual anatomic variations, better individualizing exercise prescription.
Author Contributions
JA, SR-R, and FMC contributed to conception and design of the review. MA, PN, HS, AF, JO-J, and RR-C wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank 3D4Medical (Elsevier) for allowing us to use images elaborated with Complete Anatomy 2021, version 7.0.0. (Desktop version for Mac OS) (Figure 1).
References
Aagaard, P., Simonsen, E. B., Magnusson, S. P., Larsson, B., and Dyhre-Poulsen, P. (1998). A new concept for isokinetic hamstring: quadriceps muscle strength ratio. Am. J. Sports Med. 26, 231–237. doi: 10.1177/03635465980260021201
Afonso, J., Buzzachera, C. F., and Fernandes, R. J. (2019). Commentary: do thirty-second post-activation potentiation exercises improve the 50-m freestyle sprint performance in adolescent swimmers? Front. Physiol. 10:215. doi: 10.3389/fphys.2019.00215
Al Attar, W. S. A., Soomro, N., Sinclair, P. J., Pappas, E., and Sanders, R. H. (2017). Effect of injury prevention programs that include the nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sports Med. 47, 907–916. doi: 10.1007/s40279-016-0638-2
Allen, D. G., Lamb, G. D., and Westerblad, H. (2008). Skeletal muscle fatigue: cellular mechanisms. Physiol. Rev. 88, 287–332. doi: 10.1152/physrev.00015.2007
Almeida, M. O., Maher, C. G., and Saragiotto, B. T. (2018). Prevention programmes including Nordic exercises to prevent hamstring injuries in football players (PEDro synthesis). Br. J. Sports Med. 52, 877–878. doi: 10.1136/bjsports-2017-098862
An, X. C., Lee, J. H., Im, S., Lee, M. S., Hwang, K., Kim, H. W., et al. (2010). Anatomic localization of motor entry points and intramuscular nerve endings in the hamstring muscles. Surg. Radiol. Anat. 32, 529–537. doi: 10.1007/s00276-009-0609-5
Ayuob, A., Kayani, B., and Haddad, F. S. (2020). Acute surgical repair of complete, nonavulsion proximal semimembranosus injuries in professional athletes. Am. J. Sports Med. 48, 2170–2177. doi: 10.1177/0363546520934467
Bahr, R. (2016). Why screening tests to predict injury do not work—and probably never will…: a critical review. Br. J. Sports Med. 50:776. doi: 10.1136/bjsports-2016-096256
Behan, F. P., Maden-Wilkinson, T. M., Pain, M. T. G., and Folland, J. P. (2018). Sex differences in muscle morphology of the knee flexors and knee extensors. PLoS One 13:e0190903. doi: 10.1371/journal.pone.0190903
Behan, F. P., Timmins, R., and Opar, D. A. (2019). The architecture of a hamstring strain injury. Aspetar Sports Med. J. 8, 40–43.
Behm, D., Blazevich, A. J., Kay, A., and McHugh, M. (2015). Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl. Physiol. Nutr. Metab. 41, 1–11.
Beltran, J., Matityahu, A., Hwang, K., Jbara, M., Maimon, R., Padron, M., et al. (2003). The distal semimembranosus complex: normal MR anatomy, variants, biomechanics and pathology. Skelet. Radiol. 32, 435–445. doi: 10.1007/s00256-003-0641-1
Beltran, L., Ghazikhanian, V., Padron, M., and Beltran, J. (2012). The proximal hamstring muscle–tendon–bone unit: a review of the normal anatomy, biomechanics, and pathophysiology. Eur. J. Radiol. 81, 3772–3779. doi: 10.1016/j.ejrad.2011.03.099
Blackburn, J. T., Bell, D. R., Norcross, M. F., Hudson, J. D., and Kimsey, M. H. (2009). Sex comparison of hamstring structural and material properties. Clin. Biomech. 24, 65–70. doi: 10.1016/j.clinbiomech.2008.10.001
Blakeney, W. G. (2020). Editorial commentary: proximal hamstring tendon injuries: is the research hamstrung by the use of poor outcome measures? Arthroscopy 36, 1308–1310. doi: 10.1016/j.arthro.2020.01.015
Blazevich, A. J., and Babault, N. (2019). Post-activation potentiation versus post-activation performance enhancement in humans: historical perspective, underlying mechanisms, and current issues. Front. Physiol. 10:1359. doi: 10.3389/fphys.2019.01359
Blazevich, A. J., Gill, N. D., and Zhou, S. (2006). Intra- and intermuscular variation in human quadriceps femoris architecture assessed in vivo. J. Anat. 209, 289–310. doi: 10.1111/j.1469-7580.2006.00619.x
Boccia, G., Brustio, P. R., Buttacchio, G., Calabrese, M., Bruzzone, M., Casale, R., et al. (2018). Interlimb asymmetries identified using the rate of torque development in ballistic contraction targeting submaximal torques. Front. Physiol. 9:1701–1701. doi: 10.3389/fphys.2018.01701
Britt, E., Ouillette, R., Edmonds, E., Chambers, H., Johnson, K., Bastrom, T., et al. (2020). The challenges of treating female soccer players with ACL injuries: hamstring versus bone-patellar tendon-bone autograft. Orthop. J. Sports Med. 8:2325967120964884. doi: 10.1177/2325967120964884
Broski, S. M., Murthy, N. S., Krych, A. J., Obey, M. R., and Collins, M. S. (2016). The adductor magnus “mini-hamstring”: MRI appearance and potential pitfalls. Skelet. Radiol. 45, 213–219. doi: 10.1007/s00256-015-2291-5
Buckthorpe, M., Danelon, F., La Rosa, G., Nanni, G., Stride, M., and Della Villa, F. (2020). Recommendations for hamstring function recovery after ACL reconstruction. Sports Med. 51, 607–624. doi: 10.1007/s40279-020-01400-x
Buckthorpe, M., Wright, S., Bruce-Low, S., Nanni, G., Sturdy, T., Gross, A. S., et al. (2019). Recommendations for hamstring injury prevention in elite football: translating research into practice. Br. J. Sports Med. 53:449. doi: 10.1136/bjsports-2018-099616
Burkett, L. N. (1975). Investigation into hamstring strains: the case of the hybrid muscle. J. Sports Med. 3, 228–231. doi: 10.1177/036354657500300504
Cao, J. G., Wang, L., Zhao, H. W., and Liu, J. (2016). Semitendinosus and gracilis transfer for treatment of medial collateral ligament injury of total knee arthroplasty. Eur. Rev. Med. Pharmacol. Sci. 20, 3738–3742.
Chebbi, S., Chamari, K., Van Dyk, N., Gabbett, T., and Tabben, M. (2020). Hamstring injury prevention for elite soccer players: a real-world prevention program showing the effect of players’ compliance on the outcome. J. Strength Cond. Res. [Epub ahead of print]. doi: 10.1519/JSC.0000000000003505
Christopher, S. M., McCullough, J., Snodgrass, S. J., and Cook, C. (2019). Do alterations in muscle strength, flexibility, range of motion, and alignment predict lower extremity injury in runners: a systematic review. Arch. Physiother. 9:2. doi: 10.1186/s40945-019-0054-7
Colombet, P., and Graveleau, N. (2016). Minimally invasive anterior semitendinosus harvest: a technique to decrease saphenous nerve injury. Arthrosc. Tech. 5, e139–e142. doi: 10.1016/j.eats.2015.10.011
Coole, W. G., and Gieck, J. H. (1987). An analysis of hamstring strains and their rehabilitation. J. Orthop. Sports Phys. Ther. 9, 77–85. doi: 10.2519/jospt.1987.9.2.77
Coratella, G., Beato, M., and Schena, F. (2018). Correlation between quadriceps and hamstrings inter-limb strength asymmetry with change of direction and sprint in U21 elite soccer-players. Hum. Movement Sci. 59, 81–87. doi: 10.1016/j.humov.2018.03.016
Crema, M. D., Guermazi, A., Tol, J. L., Niu, J., Hamilton, B., and Roemer, F. W. (2016). Acute hamstring injury in football players: association between anatomical location and extent of injury—a large single-center MRI report. J. Sci. Med. Sport 19, 317–322. doi: 10.1016/j.jsams.2015.04.005
Cuthbert, M., Comfort, P., Ripley, N., McMahon, J. J., Evans, M., and Bishop, C. (2021). Unilateral vs. bilateral hamstring strength assessments: comparing reliability and inter-limb asymmetries in female soccer players. J. Sports Sci. [Epub ahead of print]. doi: 10.1080/02640414.2021.1880180
Dahmane, R., Djordjevic, S., and Smerdu, V. (2006). Adaptive potential of human biceps femoris muscle demonstrated by histochemical, immunohistochemical and mechanomyographical methods. Med. Biol. Eng. Comput. 44, 999–1006. doi: 10.1007/s11517-006-0114-5
Danielsson, A., Horvath, A., Senorski, C., Alentorn-Geli, E., Garrett, W. E., Cugat, R., et al. (2020). The mechanism of hamstring injuries - a systematic review. BMC Musculoskelet. Disord. 21:641. doi: 10.1186/s12891-020-03658-8
de la Motte, S. J., Lisman, P., Gribbin, T. C., Murphy, K., and Deuster, P. A. (2019). Systematic review of the association between physical fitness and musculoskeletal injury risk: part 3-flexibility, power, speed, balance, and agility. J. Strength Cond. Res. 33, 1723–1735. doi: 10.1519/jsc.0000000000002382
Delahunt, E., McGroarty, M., De Vito, G., and Ditroilo, M. (2016). Nordic hamstring exercise training alters knee joint kinematics and hamstring activation patterns in young men. Eur. J. Appl. Physiol. 116, 663–672. doi: 10.1007/s00421-015-3325-3
Delextrat, A., Piquet, J., Matthews, M. J., and Cohen, D. D. (2018). Strength-endurance training reduces the hamstrings strength decline following simulated football competition in female players. Front. Physiol. 9:1059. doi: 10.3389/fphys.2018.01059
Diemer, W. M., Winters, M., Tol, J. L., Pas, H., and Moen, M. H. (2021). Incidence of acute hamstring injuries in soccer: a systematic review of 13 studies involving more than 3800 athletes with 2 million sport exposure hours. J. Orthop. Sports Phys. Ther. 51, 27–36. doi: 10.2519/jospt.2021.9305
Dolman, B., Verrall, G., and Reid, I. (2014). Physical principles demonstrate that the biceps femoris muscle relative to the other hamstring muscles exerts the most force: implications for hamstring muscle strain injuries. Muscles Ligaments Tendons J. 4, 371–377.
Ebben, W. P., Fauth, M. L., Petushek, E. J., Garceau, L. R., Hsu, B. E., Lutsch, B. N., et al. (2010). Gender-based analysis of hamstring and quadriceps muscle activation during jump landings and cutting. J. Strength Cond. Res. 24, 408–415. doi: 10.1519/JSC.0b013e3181c509f4
Edouard, P., Branco, P., and Alonso, J.-M. (2016). Muscle injury is the principal injury type and hamstring muscle injury is the first injury diagnosis during top-level international athletics championships between 2007 and 2015. Br. J. Sports Med. 50:619. doi: 10.1136/bjsports-2015-095559
Ekstrand, J., Healy, J. C., Waldén, M., Lee, J. C., English, B., and Hägglund, M. (2012). Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br. J. Sports Med. 46:112. doi: 10.1136/bjsports-2011-090155
Ekstrand, J., Waldén, M., and Hägglund, M. (2016). Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA elite club injury study. Br. J. Sports Med. 50, 731–737. doi: 10.1136/bjsports-2015-095359
Elerian, A. E., El-Sayyad, M. M., and Dorgham, H. A. A. (2019). Effect of pre-training and post-training nordic exercise on hamstring injury prevention, recurrence, and severity in soccer players. Ann. Rehabil. Med. 43, 465–473. doi: 10.5535/arm.2019.43.4.465
Entwisle, T., Ling, Y., Splatt, A., Brukner, P., and Connell, D. (2017). Distal musculotendinous T junction injuries of the biceps femoris: an MRI case review. Orthopaed. J. Sports Med. 5:2325967117714998. doi: 10.1177/2325967117714998
Ertelt, T., and Gronwald, T. (2017). M. biceps femoris - a wolf in sheep’s clothing: the downside of a lower limb injury prevention training. Med. Hypothes. 109, 119–125. doi: 10.1016/j.mehy.2017.10.002
Evangelidis, P. E., Massey, G. J., Ferguson, R. A., Wheeler, P. C., Pain, M. T. G., and Folland, J. P. (2017). The functional significance of hamstrings composition: is it really a “fast” muscle group? Scand. J. Med. Sci. Sports 27, 1181–1189. doi: 10.1111/sms.12786
Evangelidis, P. E., Massey, G. J., Pain, M. T., and Folland, J. P. (2015). Biceps femoris aponeurosis size: a potential risk factor for strain injury? Med. Sci. Sports Exerc. 47, 1383–1389. doi: 10.1249/mss.0000000000000550
Farley, J. B., Barrett, L. M., Keogh, J. W. L., Woods, C. T., and Milne, N. (2020). The relationship between physical fitness attributes and sports injury in female, team ball sport players: a systematic review. Sports Med. Open 6:45. doi: 10.1186/s40798-020-00264-9
Fields, K. B., Bloom, O. J., Priebe, D., and Foreman, B. (2005). Basic biomechanics of the lower extremity. Prim. Care 32, 245–251. doi: 10.1016/j.pop.2004.11.006
Fiorentino, N. M., and Blemker, S. S. (2014). Musculotendon variability influences tissue strains experienced by the biceps femoris long head muscle during high-speed running. J. Biomech. 47, 3325–3333. doi: 10.1016/j.jbiomech.2014.08.010
Fournier-Farley, C., Lamontagne, M., Gendron, P., and Gagnon, D. H. (2016). Determinants of return to play after the nonoperative management of hamstring injuries in athletes: a systematic review. Am. J. Sports Med. 44, 2166–2172. doi: 10.1177/0363546515617472
Fradkin, A. J., Gabbe, B. J., and Cameron, P. A. (2006). Does warming up prevent injury in sport? The evidence from randomised controlled trials? J. Sci. Med. Sport 9, 214–220. doi: 10.1016/j.jsams.2006.03.026
Fraser, P., Wood, A. R., and Rosales, A. (2013). Anatomical variation of the semitendinosus muscle origin. Int. J. Anat. Variat. 6, 225–227.
Freckleton, G., and Pizzari, T. (2013). Risk factors for hamstring muscle strain injury in sport: a systematic review and meta-analysis. Br. J. Sports Med. 47:351. doi: 10.1136/bjsports-2011-090664
Freitas, S. R., Abrantes, F., Santos, F., Mascarenhas, V., Oliveira, R., Firmino, T., et al. (2020). Is biceps femoris aponeurosis size an independent risk factor for strain injury? Int. J. Sports Med. 41, 552–557. doi: 10.1055/a-1028-7322
Freitas, S. R., Mendes, B., Firmino, T., Correia, J. P., Witvrouw, E. E. M. C., Raúl Oliveira, E., et al. (2021). Semitendinosus and biceps femoris long head active stiffness response until failure in professional footballers with vs. without previous hamstring injury. Eur. J. Sport Sci. [Epub ahead of print]. doi: 10.1080/17461391.2021.1910347
Fridén, J., Sjöström, M., and Ekblom, B. (1983). Myofibrillar damage following intense eccentric exercise in man. Int. J. Sports Med. 4, 170–176. doi: 10.1055/s-2008-1026030
Friedman, J. M., You, J. S., Hodax, J. D., Aung, M. S., Feeley, B. T., Zhang, A. L., et al. (2020). Patellar tendon reconstruction with hamstring autograft for the treatment of chronic irreparable patellar tendon injuries. Knee 27, 1841–1847. doi: 10.1016/j.knee.2020.09.002
Galpin, A. J., Raue, U., Jemiolo, B., Trappe, T. A., Harber, M. P., Minchev, K., et al. (2012). Human skeletal muscle fiber type specific protein content. Anal. Biochem. 425, 175–182. doi: 10.1016/j.ab.2012.03.018
Garrett, W. E. Jr., Califf, J. C., and Bassett, F. H. III (1984). Histochemical correlates of hamstring injuries. Am. J. Sports Med. 12, 98–103. doi: 10.1177/036354658401200202
Gérard, R., Gojon, L., Decleve, P., and Van Cant, J. (2020). The effects of eccentric training on biceps femoris architecture and strength: a systematic review with meta-analysis. J. Athl. Train. 55, 501–514. doi: 10.4085/1062-6050-194-19
Goode, A. P., Reiman, M. P., Harris, L., DeLisa, L., Kauffman, A., Beltramo, D., et al. (2015). Eccentric training for prevention of hamstring injuries may depend on intervention compliance: a systematic review and meta-analysis. Br. J. Sports Med. 49, 349–356. doi: 10.1136/bjsports-2014-093466
Gray, D. J. (1945). Some anomalous hamstring muscles. Anat. Rec. 91, 33–38. doi: 10.1002/ar.1090910105
Green, B., Bourne, M. N., van Dyk, N., and Pizzari, T. (2020). Recalibrating the risk of hamstring strain injury (HSI): a 2020 systematic review and meta-analysis of risk factors for index and recurrent hamstring strain injury in sport. Br. J. Sports Med. 54, 1081–1088. doi: 10.1136/bjsports-2019-100983
Guex, K., Degache, F., Morisod, C., Sailly, M., and Millet, G. P. (2016). Hamstring architectural and functional adaptations following long vs. short muscle length eccentric training. Front. Physiol. 7:340. doi: 10.3389/fphys.2016.00340
Hepple, R. T., and Rice, C. L. (2016). Innervation and neuromuscular control in ageing skeletal muscle. J. Physiol. 594, 1965–1978. doi: 10.1113/JP270561
Herbert, R. D., and Gabriel, M. (2002). Effects of stretching before and after exercising on muscle soreness and risk of injury: systematic review. Bmj 325:468. doi: 10.1136/bmj.325.7362.468
Hickey, J., Shield, A. J., Williams, M. D., and Opar, D. A. (2014). The financial cost of hamstring strain injuries in the Australian Football League. Br. J. Sports Med. 48, 729–730. doi: 10.1136/bjsports-2013-092884
Hickey, J., Timmins, R. G., Maniar, N., Williams, M. D., and Opar, D. A. (2017). Criteria for progressing rehabilitation and determining return-to-play clearance following hamstring strain injury: a systematic review. Sports Med. 47, 1375–1387. doi: 10.1007/s40279-016-0667-x
Higashihara, A., Ono, T., Kubota, J., and Fukubayashi, T. (2010a). Differences in the electromyographic activity of the hamstring muscles during maximal eccentric knee flexion. Eur. J. Appl. Physiol. 108, 355–362. doi: 10.1007/s00421-009-1242-z
Higashihara, A., Ono, T., Kubota, J., Okuwaki, T., and Fukubayashi, T. (2010b). Functional differences in the activity of the hamstring muscles with increasing running speed. J. Sports Sci. 28, 1085–1092. doi: 10.1080/02640414.2010.494308
Hirose, N., and Tsuruike, M. (2018). Differences in the electromyographic activity of the hamstring, gluteus maximus, and erector spinae muscles in a variety of kinetic changes. J. Strength Cond. Res. 32, 3357–3363. doi: 10.1519/jsc.0000000000002747
Hogervorst, T., and Vereecke, E. E. (2015). Evolution of the human hip. Part 2: muscling the double extension. J. Hip. Preserv. Surg. 2, 3–14. doi: 10.1093/jhps/hnu014
Horteur, C., Cavalié, G., Gaulin, B., Cohen Bacry, M., Morin, V., Cavaignac, E., et al. (2020). Saphenous nerve injury after anterior cruciate ligament reconstruction: reduced numbness area after ligamentoplasty using quadriceps tendon compared with hamstring tendon. Knee 27, 1151–1157. doi: 10.1016/j.knee.2020.05.020
Houglum, P. A., and Bertoti, D. B. (2012). Brunnstrom’s Clinical Kinesiology, 6th Edn. Philadelphia, PA: F.A. Davis Company.
Hurst, P., Schipof-Godart, L., Szabo, A., Raglin, J., Hettinga, F., Roelands, B., et al. (2020). The Placebo and Nocebo effect on sports performance: a systematic review. Eur. J. Sport Sci. 20, 279–292. doi: 10.1080/17461391.2019.1655098
Huygaerts, S., Cos, F., Cohen, D. D., Calleja-González, J., Guitart, M., Blazevich, A. J., et al. (2020). Mechanisms of hamstring strain injury: interactions between fatigue, muscle activation and function. Sports 8:65. doi: 10.3390/sports8050065
Huygaerts, S., Cos, F., Cohen, D. D., Calleja-González, J., Pruna, R., Alcaraz, P. E., et al. (2021). Does muscle-tendon unit structure predispose to hamstring strain injury during running? A critical review. Sports Med. 51, 215–224. doi: 10.1007/s40279-020-01385-7
Jain, J. K., Vidyasagar, J. V., and Chabra, R. (2014). Percutaneous reconstruction of patellar tendon using semitendinosus tendon in chronic patellar tendon injury–case series and outcome. Knee 21, 726–730. doi: 10.1016/j.knee.2014.02.002
Jeno, S. H., and Schindler, G. S. (2020). Anatomy, Bony Pelvis and Lower Limb, Thigh Adductor Magnus Muscles. Treasure Island, FL: StatPearls Publishing.
Jones, R. I., Ryan, B., and Todd, A. I. (2015). Muscle fatigue induced by a soccer match-play simulation in amateur Black South African players. J. Sports Sci. 33, 1305–1311. doi: 10.1080/02640414.2015.1022572
Jönhagen, S., Németh, G., and Eriksson, E. (1994). Hamstring injuries in sprinters. The role of concentric and eccentric hamstring muscle strength and flexibility. Am. J. Sports Med. 22, 262–266. doi: 10.1177/036354659402200218
Julien, I. B., Sephton, C. F., and Dutchak, P. A. (2018). Metabolic networks influencing skeletal muscle fiber composition. Front. Cell Dev. Biol. 6:125–125. doi: 10.3389/fcell.2018.00125
Kellis, E. (2018). Intra- and inter-muscular variations in hamstring architecture and mechanics and their implications for injury: a narrative review. Sports Med. 48, 2271–2283. doi: 10.1007/s40279-018-0975-4
Kellis, E., Galanis, N., Kapetanos, G., and Natsis, K. (2012). Architectural differences between the hamstring muscles. J. Electromyogr. Kinesiol. 22, 520–526. doi: 10.1016/j.jelekin.2012.03.012
Kellis, E., Galanis, N., Natsis, K., and Kapetanos, G. (2009). Validity of architectural properties of the hamstring muscles: correlation of ultrasound findings with cadaveric dissection. J. Biomech. 42, 2549–2554. doi: 10.1016/j.jbiomech.2009.07.011
Keyhani, S., Kazemi, S. M., Sajjadi, M. M., and Elmi, A. (2020). A comparison between oblique and vertical incisions on the hamstring tendon harvesting in anterior cruciate ligament reconstruction and infrapatellar branch injury of the saphenous nerve. Rev. Bras. Ortop. 55, 374–379. doi: 10.1055/s-0039-1692695
Kirk, E. A., Gilmore, K. J., and Rice, C. L. (2018). Neuromuscular changes of the aged human hamstrings. J. Neurophysiol. 120, 480–488. doi: 10.1152/jn.00794.2017
Kong, P. W., and Burns, S. F. (2010). Bilateral difference in hamstrings to quadriceps ratio in healthy males and females. Phys. Ther. Sport 11, 12–17. doi: 10.1016/j.ptsp.2009.09.004
Kulas, A. S., Schmitz, R. J., Shultz, S. J., Waxman, J. P., Wang, H.-M., Kraft, R. A., et al. (2018). Bilateral quadriceps and hamstrings muscle volume asymmetries in healthy individuals. J. Orthopaed. Res. 36, 963–970. doi: 10.1002/jor.23664
Lahti, J., Mendiguchia, J., Ahtiainen, J., Anula, L., Kononen, T., Kujala, M., et al. (2020). Multifactorial individualised programme for hamstring muscle injury risk reduction in professional football: protocol for a prospective cohort study. BMJ Open Sport Exerc. Med. 6:e000758. doi: 10.1136/bmjsem-2020-000758
Lee, O. S., and Lee, Y. S. (2020). Changes in hamstring strength after anterior cruciate ligament reconstruction with hamstring autograft and posterior cruciate ligament reconstruction with tibialis allograft. Knee Surg. Relat. Res. 32:27. doi: 10.1186/s43019-020-00047-2
Lees, A., and Nolan, L. (1998). The biomechanics of soccer: a review. J. Sports Sci. 16, 211–234. doi: 10.1080/026404198366740
Lievens, E., Klass, M., Bex, T., and Derave, W. (2020). Muscle fiber typology substantially influences time to recover from high-intensity exercise. J. Appl. Physiol. 128, 648–659. doi: 10.1152/japplphysiol.00636.2019
Lim, Y. P., Lin, Y.-C., and Pandy, M. G. (2017). Effects of step length and step frequency on lower-limb muscle function in human gait. J. Biomech. 57, 1–7. doi: 10.1016/j.jbiomech.2017.03.004
Liu, H., Garrett, W. E., Moorman, C. T., and Yu, B. (2012). Injury rate, mechanism, and risk factors of hamstring strain injuries in sports: a review of the literature. J. Sport Health Sci. 1, 92–101. doi: 10.1016/j.jshs.2012.07.003
Macaluso, F., Isaacs, A. W., and Myburgh, K. H. (2012). Preferential Type II muscle fiber damage from plyometric exercise. J. Athl. Train. 47, 414–420. doi: 10.4085/1062-6050-47.4.13
Macdonald, B., McAleer, S., Kelly, S., Chakraverty, R., Johnston, M., and Pollock, N. (2019). Hamstring rehabilitation in elite track and field athletes: applying the British athletics muscle injury classification in clinical practice. Br. J. Sports Med. 53:1464. doi: 10.1136/bjsports-2017-098971
Maniar, N., Shield, A. J., Williams, M. D., Timmins, R. G., and Opar, D. A. (2016). Hamstring strength and flexibility after hamstring strain injury: a systematic review and meta-analysis. Br. J. Sports Med. 50, 909–920. doi: 10.1136/bjsports-2015-095311
Martín-San Agustín, R., Medina-Mirapeix, F., Alakhdar, Y., and Benítez-Martínez, J. C. (2019). Sex differences in the velocity of muscle contraction of the hamstring and quadriceps among recreationally active young adults. J. Strength Cond. Res. 33, 1252–1257. doi: 10.1519/jsc.0000000000003122
Marušič, J., Vatovec, R., Marković, G., and Šarabon, N. (2020). Effects of eccentric training at long-muscle length on architectural and functional characteristics of the hamstrings. Scand. J. Med. Sci. Sports 30, 2130–2142. doi: 10.1111/sms.13770
McCall, A., Dupont, G., and Ekstrand, J. (2016). Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA elite club injury study teams: a survey of teams’ head medical officers. Br. J. Sports Med. 50, 725–730. doi: 10.1136/bjsports-2015-095259
McCall, A., Pruna, R., Van der Horst, N., Dupont, G., Buchheit, M., Coutts, A. J., et al. (2020). Exercise-based strategies to prevent muscle injury in male elite footballers: an expert-led delphi survey of 21 practitioners belonging to 18 teams from the big-5 european leagues. Sports Med. 50, 1667–1681. doi: 10.1007/s40279-020-01315-7
McCrary, J. M., Ackermann, B. J., and Halaki, M. (2015). A systematic review of the effects of upper body warm-up on performance and injury. Br. J. Sports Med. 49, 935–942. doi: 10.1136/bjsports-2014-094228
Medeiros, T. M., Ribeiro-Alvares, J. B., Fritsch, C. G., Oliveira, G. S., Severo-Silveira, L., Pappas, E., et al. (2020). Effect of weekly training frequency with the nordic hamstring exercise on muscle-strain risk factors in football players: a randomized trial. Int. J. Sports Physiol. Perform. [Epub ahead of print]. doi: 10.1123/ijspp.2018-0780
Mendiguchia, J., Alentorn-Geli, E., and Brughelli, M. (2012). Hamstring strain injuries: are we heading in the right direction? Br. J. Sports Med. 46:81. doi: 10.1136/bjsm.2010.081695
Mendiguchia, J., Conceição, F., Edouard, P., Fonseca, M., Pereira, R., Lopes, H., et al. (2020). Sprint versus isolated eccentric training: comparative effects on hamstring architecture and performance in soccer players. PLoS One 15:e0228283. doi: 10.1371/journal.pone.0228283
Messer, D. J., Shield, A. J., Williams, M. D., Timmins, R. G., and Bourne, M. N. (2020). Hamstring muscle activation and morphology are significantly altered 1-6 years after anterior cruciate ligament reconstruction with semitendinosus graft. Knee Surg. Sports Traumatol. Arthrosc. 28, 733–741. doi: 10.1007/s00167-019-05374-w
Metcalf, K. B., Knapik, D. M., and Voos, J. E. (2019). Damage to or injury of the distal semitendinosus tendon during sporting activities: a systematic review. HSS J. 15, 185–189. doi: 10.1007/s11420-018-9639-z
Methenitis, S., Spengos, K., Zaras, N., Stasinaki, A. N., Papadimas, G., Karampatsos, G., et al. (2019). Fiber type composition and rate of force development in endurance- and resistance-trained individuals. J. Strength Cond. Res. 33, 2388–2397. doi: 10.1519/jsc.0000000000002150
Miller, J. P., Croce, R. V., and Hutchins, R. (2000). Reciprocal coactivation patterns of the medial and lateral quadriceps and hamstrings during slow, medium and high speed isokinetic movements. J. Electromyogr. Kinesiol. 10, 233–239. doi: 10.1016/S1050-6411(00)00012-2
Mishra, P., Varuzhanyan, G., Pham, A. H., and Chan, D. C. (2015). Mitochondrial dynamics is a distinguishing feature of skeletal muscle fiber types and regulates organellar compartmentalization. Cell Metab. 22, 1033–1044. doi: 10.1016/j.cmet.2015.09.027
Mjølsnes, R., Arnason, A., Østhagen, T., Raastad, T., and Bahr, R. (2004). A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 14, 311–317. doi: 10.1046/j.1600-0838.2003.367.x
Monajati, A., Larumbe-Zabala, E., Goss-Sampson, M., and Naclerio, F. (2016). The effectiveness of injury prevention programs to modify risk factors for non-contact anterior cruciate ligament and hamstring injuries in uninjured team sports athletes: a systematic review. PLoS One 11:e0155272. doi: 10.1371/journal.pone.0155272
Mondin, D., Owen, J. A., Negro, M., and D’Antona, G. (2018). Validity and reliability of a non-invasive test to assess quadriceps and hamstrings strength in athletes. Front. Physiol. 9:1702. doi: 10.3389/fphys.2018.01702
Narici, M. V., Maffulli, N., and Maganaris, C. N. (2008). Ageing of human muscles and tendons. Disabil. Rehabil. 30, 1548–1554. doi: 10.1080/09638280701831058
Niederer, D., Willberg, C., Kruse, A., Exler, N., Giesche, F., Vogt, L., et al. (2020). Acute effects of preventive warm-up exercises on modifiable risk factors for anterior cruciate ligament injuries: a three-arm randomized-controlled crossover trial. J. Sports Med. Phys. Fitness 60, 92–101. doi: 10.23736/s0022-4707.19.09949-3
Overend, T. J., Cunningham, D. A., Kramer, J. F., Lefcoe, M. S., and Paterson, D. H. (1992). Knee extensor and knee flexor strength:cross-sectional area ratios in young and elderly men. J. Gerontol. 47, M204–M210. doi: 10.1093/geronj/47.6.M204
Owoeye, O. B. A., Emery, C. A., Befus, K., Palacios-Derflingher, L., and Pasanen, K. (2020). How much, how often, how well? Adherence to a neuromuscular training warm-up injury prevention program in youth basketball. J. Sports Sci. 38, 2329–2337. doi: 10.1080/02640414.2020.1782578
Pas, H. I., Reurink, G., Tol, J. L., Weir, A., Winters, M., and Moen, M. H. (2015). Efficacy of rehabilitation (lengthening) exercises, platelet-rich plasma injections, and other conservative interventions in acute hamstring injuries: an updated systematic review and meta-analysis. Br. J. Sports Med. 49, 1197–1205. doi: 10.1136/bjsports-2015-094879
Pickering, C., and Kiely, J. (2018). Hamstring injury prevention: a role for genetic information? Med. Hypothes. 119, 58–62. doi: 10.1016/j.mehy.2018.07.011
Raglin, J., Szabo, A., Lindheimer, J. B., and Beedie, C. (2020). Understanding placebo and nocebo effects in the context of sport: a psychological perspective. Eur. J. Sport Sci. 20, 293–301. doi: 10.1080/17461391.2020.1727021
Rehorn, M. R., and Blemker, S. S. (2010). The effects of aponeurosis geometry on strain injury susceptibility explored with a 3D muscle model. J. Biomech. 43, 2574–2581. doi: 10.1016/j.jbiomech.2010.05.011
Rhatomy, S., Asikin, A. I. Z., Wardani, A. E., Rukmoyo, T., Lumban-Gaol, I., and Budhiparama, N. C. (2019). Peroneus longus autograft can be recommended as a superior graft to hamstring tendon in single-bundle ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 27, 3552–3559. doi: 10.1007/s00167-019-05455-w
Ribeiro-Alvares, J. B., Dornelles, M. P., Fritsch, C. G., de Lima, E. S. F. X., Medeiros, T. M., Severo-Silveira, L., et al. (2020). Prevalence of hamstring strain injury risk factors in professional and under-20 male football (Soccer) players. J. Sport Rehabil. 29, 339–345. doi: 10.1123/jsr.2018-0084
Rogan, S., Wüst, D., Schwitter, T., and Schmidtbleicher, D. (2013). Static stretching of the hamstring muscle for injury prevention in football codes: a systematic review. Asian J. Sports Med. 4, 1–9.
Roos, M. R., Rice, C. L., Connelly, D. M., and Vandervoort, A. A. (1999). Quadriceps muscle strength, contractile properties, and motor unit firing rates in young and old men. Muscle Nerve 22, 1094–1103. doi: 10.1002/(SICI)1097-4598(199908)22:8<1094::AID-MUS14<3.0.CO;2-G
Ruas, C. V., Pinto, R. S., Haff, G. G., Lima, C. D., Pinto, M. D., and Brown, L. E. (2019). Alternative methods of determining hamstrings-to-quadriceps ratios: a comprehensive review. Sports Med. Open 5:11. doi: 10.1186/s40798-019-0185-0
Ruffilli, A., De Fine, M., Traina, F., Pilla, F., Fenga, D., and Faldini, C. (2017). Saphenous nerve injury during hamstring tendons harvest: does the incision matter? A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 25, 3140–3145. doi: 10.1007/s00167-016-4217-8
Sanfilippo, J. L., Silder, A., Sherry, M. A., Tuite, M. J., and Heiderscheit, B. C. (2013). Hamstring strength and morphology progression after return to sport from injury. Med. Sci. Sports Exerc. 45, 448–454. doi: 10.1249/MSS.0b013e3182776eff
Schache, A. G., Dorn, T. W., Blanch, P. D., Brown, N. A., and Pandy, M. G. (2012). Mechanics of the human hamstring muscles during sprinting. Med. Sci. Sports Exerc. 44, 647–658. doi: 10.1249/MSS.0b013e318236a3d2
Schmuter, G., Hajtovic, S., Guce, R. G., and Matthews, K. (2021). Rare fusion of the semitendinosus and the long head of the biceps femoris muscles in a human cadaver. Cureus 13:e12474. doi: 10.7759/cureus.12474
Schuermans, J., Van Tiggelen, D., Danneels, L., and Witvrouw, E. (2014). Biceps femoris and semitendinosus–teammates or competitors? New insights into hamstring injury mechanisms in male football players: a muscle functional MRI study. Br. J. Sports Med. 48, 1599–1606. doi: 10.1136/bjsports-2014-094017
Schuermans, J., Van Tiggelen, D., Danneels, L., and Witvrouw, E. (2016). Susceptibility to hamstring injuries in soccer: a prospective study using muscle functional magnetic resonance imaging. Am. J. Sports Med. 44, 1276–1285. doi: 10.1177/0363546515626538
Segal, R. L. (2007). Use of imaging to assess normal and adaptive muscle function. Phys. Ther. 87, 704–718. doi: 10.2522/ptj.20060169
Shalabi, A., Eriksson, K., Jansson, E., and Wredmark, T. (2002). Ultrasound-guided percutaneous biopsies of the semitendinosus muscle following ACL reconstruction–a methodological description. Int. J. Sports Med. 23, 202–206. doi: 10.1055/s-2002-23179
Sheean, A. J., Arner, J. W., and Bradley, J. P. (2021). Proximal hamstring tendon injuries: diagnosis and management. Arthroscopy 37, 435–437. doi: 10.1016/j.arthro.2020.12.201
Sherman, D. A., Rush, J. L., Glaviano, N. R., and Norte, G. E. (2021). Hamstrings muscle morphology after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Sports Med. [Epub ahead of print]. doi: 10.1007/s40279-021-01431-y
Shield, A. J., and Bourne, M. N. (2018). Hamstring injury prevention practices in elite sport: evidence for eccentric strength vs. lumbo-pelvic training. Sports Med. 48, 513–524. doi: 10.1007/s40279-017-0819-7
Small, K., Mc Naughton, L., and Matthews, M. (2008). A systematic review into the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury. Res. Sports Med. 16, 213–231. doi: 10.1080/15438620802310784
Smith, J. W. (1957). The forces operating at the human ankle joint during standing. J. Anat. 91, 545–564.
Smith, N. A., Franettovich Smith, M. M., Bourne, M. N., Barrett, R. S., and Hides, J. A. (2021). A prospective study of risk factors for hamstring injury in Australian football league players. J. Sports Sci. 39, 1395–1401. doi: 10.1080/02640414.2021.1875613
Solomon, L. B., and Stevenson, A. W. (2008). Tibial insertion of the biceps femoris tendon: anatomical and radiological description of an anatomical variant. Clin. Anat. 21, 802–804. doi: 10.1002/ca.20722
Standring, S. (2015). Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41st Edn. Amsterdam: Elsevier.
Suarez-Arrones, L., Nakamura, F. Y., Maldonado, R. A., Torreno, N., Di Salvo, V., and Mendez-Villanueva, A. (2021). Applying a holistic hamstring injury prevention approach in elite football: 12 seasons, single club study. Scand. J. Med. Sci. Sports 31, 861–874. doi: 10.1111/sms.13913
Taberner, M., Haddad, F. S., Dunn, A., Newall, A., Parker, L., Betancur, E., et al. (2020). Managing the return to sport of the elite footballer following semimembranosus reconstruction. BMJ Open Sport Exerc. Med. 6:e000898. doi: 10.1136/bmjsem-2020-000898
Talbot, J., and Maves, L. (2016). Skeletal muscle fiber type: using insights from muscle developmental biology to dissect targets for susceptibility and resistance to muscle disease. Wiley Interdiscipl. Rev. Dev. Biol. 5, 518–534. doi: 10.1002/wdev.230
Thelen, D. G., Chumanov, E. S., Sherry, M. A., and Heiderscheit, B. C. (2006). Neuromusculoskeletal models provide insights into the mechanisms and rehabilitation of hamstring strains. Exerc. Sport Sci. Rev. 34, 135–141. doi: 10.1249/00003677-200607000-00008
Timmins, R. G. (2017). Biceps femoris architecture: the association with injury and response to training. Br. J. Sports Med. 51, 547–548. doi: 10.1136/bjsports-2016-097044
Timmins, R. G., Bourne, M. N., Shield, A. J., Williams, M. D., Lorenzen, C., and Opar, D. A. (2016). Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br. J. Sports Med. 50, 1524–1535. doi: 10.1136/bjsports-2015-095362
Trappe, S., Luden, N., Minchev, K., Raue, U., Jemiolo, B., and Trappe, T. A. (2015). Skeletal muscle signature of a champion sprint runner. J. Appl. Physiol. 118, 1460–1466. doi: 10.1152/japplphysiol.00037.2015
Tubbs, R. S., Shoja, M. M., and Loukas, M. (2016). Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation. Hoboken, NJ: Wiley Blackwell.
Vairo, G. L. (2014). Knee flexor strength and endurance profiles after ipsilateral hamstring tendons anterior cruciate ligament reconstruction. Arch. Phys. Med. Rehabil. 95, 552–561. doi: 10.1016/j.apmr.2013.10.001
van den Tillaar, R., Solheim, J. A. B., and Bencke, J. (2017). Comparison of hamstring muscle activation during high-speed running and various hamstring strengthening exercises. Int. J. Sports Phys. Ther. 12, 718–727.
van der Horst, N., Smits, D. W., Petersen, J., Goedhart, E. A., and Backx, F. J. (2015). The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am. J. Sports Med. 43, 1316–1323. doi: 10.1177/0363546515574057
van der Horst, N., van de Hoef, S., Reurink, G., Huisstede, B., and Backx, F. (2016). Return to play after hamstring injuries: a qualitative systematic review of definitions and criteria. Sports Med. 46, 899–912. doi: 10.1007/s40279-015-0468-7
van der Made, A. D., Wieldraaijer, T., Kerkhoffs, G. M., Kleipool, R. P., Engebretsen, L., van Dijk, C. N., et al. (2015). The hamstring muscle complex. Knee Surg. Sports Traumatol. Arthrosc. 23, 2115–2122. doi: 10.1007/s00167-013-2744-0
van Dyk, N., Behan, F. P., and Whiteley, R. (2019). Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 53, 1362–1370. doi: 10.1136/bjsports-2018-100045
van Dyk, N., Witvrouw, E., and Bahr, R. (2018). Interseason variability in isokinetic strength and poor correlation with Nordic hamstring eccentric strength in football players. Scand. J. Med. Sci. Sports 28, 1878–1887. doi: 10.1111/sms.13201
Vatovec, R., and Kozinc, Ž, and Šarabon, N. (2020). Exercise interventions to prevent hamstring injuries in athletes: a systematic review and meta-analysis. Eur. J. Sport Sci. 20, 992–1004. doi: 10.1080/17461391.2019.1689300
Vaughan, S. K., Stanley, O. L., and Valdez, G. (2016). Impact of aging on proprioceptive sensory neurons and intrafusal muscle fibers in mice. J. Gerontol. Ser. A 72, 771–779. doi: 10.1093/gerona/glw175
Verrall, G. M., Slavotinek, J. P., Barnes, P. G., and Fon, G. T. (2003). Diagnostic and prognostic value of clinical findings in 83 athletes with posterior thigh injury: comparison of clinical findings with magnetic resonance imaging documentation of hamstring muscle strain. Am. J. Sports Med. 31, 969–973. doi: 10.1177/03635465030310063701
Vieira, R. L., Rosenberg, Z. S., and Kiprovski, K. (2007). MRI of the distal biceps femoris muscle: normal anatomy, variants, and association with common peroneal entrapment neuropathy. AJR Am. J. Roentgenol. 189, 549–555. doi: 10.2214/ajr.07.2308
Wan, X., Qu, F., Garrett, W. E., Liu, H., and Yu, B. (2017). Relationships among hamstring muscle optimal length and hamstring flexibility and strength. J. Sport Health Sci. 6, 275–282. doi: 10.1016/j.jshs.2016.04.009
Watson, A., Brindle, J., Brickson, S., Allee, T., and Sanfilippo, J. (2017). Preseason aerobic capacity is an independent predictor of in-season injury in collegiate soccer players. Clin. J. Sport Med. 27, 302–307.
Webber, S. C., Porter, M. M., and Gardiner, P. F. (2009). Modeling age-related neuromuscular changes in humans. Appl. Physiol. Nutr. Metab. 34, 732–744. doi: 10.1139/h09-052 %m 19767810
Wiesinger, H.-P., Gressenbauer, C., Kösters, A., Scharinger, M., and Müller, E. (2020). Device and method matter: a critical evaluation of eccentric hamstring muscle strength assessments. Scand. J. Med. Sci. Sports 30, 217–226. doi: 10.1111/sms.13569
Wollin, M., Thorborg, K., and Pizzari, T. (2018). Monitoring the effect of football match congestion on hamstring strength and lower limb flexibility: potential for secondary injury prevention? Phys. Ther. Sport 29, 14–18. doi: 10.1016/j.ptsp.2017.09.001
Woodley, S. J., and Mercer, S. R. (2005). Hamstring muscles: architecture and innervation. Cells Tissues Organs 179, 125–141. doi: 10.1159/000085004
Worrell, T. W., and Perrin, D. H. (1992). Hamstring muscle injury: the influence of strength, flexibility, warm-up, and fatigue. J. Orthop. Sports Phys. Ther. 16, 12–18. doi: 10.2519/jospt.1992.16.1.12
Yang, J., Cho, Y., Cho, J., Choi, H., Jeon, J., and Kang, S. (2018). Anatomical variants of “Short Head of Biceps Femoris Muscle” associated with common peroneal neuropathy in korean populations : an MRI based study. J. Korean Neurosurg. Soc. 61, 509–515. doi: 10.3340/jkns.2018.0018
Yasin, M. N., Charalambous, C. P., Mills, S. P., and Phaltankar, P. M. (2010). Accessory bands of the hamstring tendons: a clinical anatomical study. Clin. Anat. 23, 862–865. doi: 10.1002/ca.21020
Yoshiko, A., Hioki, M., Kanehira, N., Shimaoka, K., Koike, T., Sakakibara, H., et al. (2017). Three-dimensional comparison of intramuscular fat content between young and old adults. BMC Med. Imaging 17:12. doi: 10.1186/s12880-017-0185-9
Zachazewski, J., Silvers, H., Li, B., Pohlig, R., Ahmad, C., and Mandelbaum, B. (2019). Prevalence of hamstring injuries in summer league baseball players. Int. J. Sports Phys. Ther. 14, 885–897.
Zhou, P., Liu, J. C., Deng, X. T., and Li, Z. (2020). Hamstring autograft versus patellar tendon autograft for anterior cruciate ligament reconstruction, which graft has a higher contralateral anterior cruciate ligament injury rate?: A meta-analysis of 5561 patients following the PRISMA guidelines. Medicine 99:e21540. doi: 10.1097/md.0000000000021540
Keywords: hamstrings injuries, interindividual variation, kinesiology, muscle architecture, exercise prescription, hamstrings anatomy
Citation: Afonso J, Rocha-Rodrigues S, Clemente FM, Aquino M, Nikolaidis PT, Sarmento H, Fílter A, Olivares-Jabalera J and Ramirez-Campillo R (2021) The Hamstrings: Anatomic and Physiologic Variations and Their Potential Relationships With Injury Risk. Front. Physiol. 12:694604. doi: 10.3389/fphys.2021.694604
Received: 13 April 2021; Accepted: 16 June 2021;
Published: 07 July 2021.
Edited by:
Ricardo Ferraz, University of Beira Interior, PortugalReviewed by:
Barbara St. Pierre Schneider, University of Nevada, Las Vegas, United StatesPedro Alexandre Duarte-Mendes, Instituto Politécnico de Castelo Branco, Portugal
Ayako Higashihara, Keio University, Japan
Copyright © 2021 Afonso, Rocha-Rodrigues, Clemente, Aquino, Nikolaidis, Sarmento, Fílter, Olivares-Jabalera and Ramirez-Campillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo Ramirez-Campillo, ci5yYW1pcmV6QHVsYWdvcy5jbA==