
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Physiol., 21 January 2021
Sec. Respiratory Physiology and Pathophysiology
Volume 11 - 2020 | https://doi.org/10.3389/fphys.2020.607913
 Nicolas Vallée1*
Nicolas Vallée1* Sarah Rives1Anne-Virginie Desruelle1Sebastian Marzetti2Valentin Barchasz2Jean-Jacques Risso1Valentin Gies2
Sarah Rives1Anne-Virginie Desruelle1Sebastian Marzetti2Valentin Barchasz2Jean-Jacques Risso1Valentin Gies2Oxygen is a first-line drug in the therapeutic management of patients with SARS-Cov2 (Tobin, 2020). Being limited, oxygen is a resource to save (Maves et al., 2020). In the same time, it should be remembered that medical care can become financially toxic (See and Slonim, 2020) because the cost of healthcare steadily rises (Mycyk, 2020). Is ventilators by lottery (Silva, 2020) the solution? In this way, requiring a low-cost respirator <200€ is attractive (Gies et al., 2020), but its value may be limited in view of the consumption, supply and cost of oxygen. The Swiss newspaper Le Temps reported in its article of July 15, 2020, whose title could be translated as “With Covid-19, the world faces an oxygen shortage,” that the oxygen demand in Italy has increased 10-fold or 14-fold and the costs are likely to soar (Logean, 2020).
We wonder viewing the High oxygen consumption in SARS-COV2 if the development of low-cost oxygen rebreather could be considered? The oxygen rebreather, or closed-circuit rebreather, is a simple apparatus well-known to the world of scuba diving and therefore the main goal is to be able to evolve a long time underwater with a small carry of oxygen (Wingelaar et al., 2017). The device is designed so that the majority of the oxygen delivered to the diver is consumed by the organism: the exhaled oxygen must be able to be re-inhaled through a counterlung, while the exhaled carbon dioxide must be able to be extracted using soda lime canister. When the counterlung is empty, the low pressure triggered by the diver's inspiration is enough to activate a regulator connected to a pressurized oxygen cylinder, which replenishes the bladder instantly. Like respirators, one can imagine that a similar device could be added to it in order to limit the loss of oxygen (Figure 1). Since no gas exhaled by the patient is released into the atmosphere, this type of device can help improve the safety of healthcare workers. The development of such a device is simple but it must obviously consider the health safety rules with the use of filters against the virus, but also the rules in force in the field of diving. For example, it is important to properly calibrate the regulator in order to avoid any additional ventilatory effort, which could lead to alveolar damage (Wilmshurst, 2019): electronic systems can easily overcome the defects of the mechanical systems. It is also crucial to have the ability to change soda lime before it is saturated (Arieli, 2008): lime with colored indicators exists. The reaction of soda lime with CO2 is exothermic (Shaw and Scott, 1998; Silvanius et al., 2019), but the length of the breathing circuits must be sufficient to dissipate the heat. An ice bath around the soda lime canister could also be suitable. It must be taken into account that the exhaled gases are saturated with water, and that water traps for condensation may be necessary. Additionally, if we are looking to obtain a very high FiO2, it is also important to take into account the denitrogenation of the organism (Katz et al., 2017): the nitrogen regularly exhaled can be evacuated by means of regular flushing of the counterlung in the 1st h of treatment. Finally, most of intubated and ventilated COVID patients need levels of positive end-expiratory pressure (PEEP) around 10–15 cm H20 because of their acute respiratory syndrome (Navas-Blanco and Dudaryk, 2020), proportional forces can be applied on the counter lung and the membrane regulator in order to achieve light pressures inside the circuit. These forces can take the appearance of weights, conical springs, or a more complex system synchronized with the respirator. This list is not exhaustive but it retraces the main points that deserve to be raised. This is not insurmountable as divers have been using similar systems for decades.
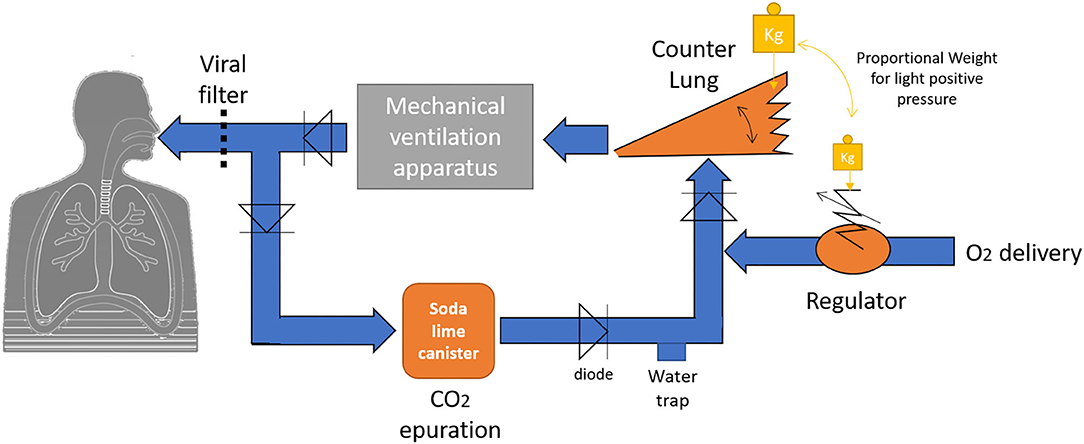
Figure 1. Schematic diagram of a low-cost oxygen rebreather.
NV wrote and the other authors proofread and validated the concepts and the manuscript. All authors contributed to the article and approved the submitted version.
This work should be attributed to the Institut de Recherches Biomédicales des Armées laboratories. It was supported by Grant No. SAN-1-0516 from the Direction Générale de l'Armement of the French army, Paris, France.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Arieli, R. (2008). The effect of over-or underfilling the soda lime canister on CO2 absorption in two closed-circuit oxygen rebreathers. Undersea Hyperbar. Med. 35, 213–218.
Gies, V., Barchasz, V., and Glotin, H. (2020). Low Cost Artificial Ventilator Embedding Unsupervised Learning for Hardware Failure Detection. La Garde: Smiot.
Katz, I., Murdock, J., Palgen, M., and Farjot, G. (2017). A physiologically based model for denitrogenation kinetics. Med. Gas Res. 7, 256–259. doi: 10.4103/2045-9912.222449
Logean, S. (2020). Avec le Covid-19, le Monde Fait Face à Une Pénurie D'oxygène. Lausanne: Le temps.
Maves, R. C., Downar, J., Dichter, J. R., Hick, J. L., Devereaux, A., Geiling, J. A., et al. (2020). Triage of scarce critical care resources in COVID-19: an implementation guide for regional allocation an expert panel report of the Task force for mass critical care and the American college of chest physicians. Chest. 158, 212–225. doi: 10.1016/j.chest.2020.03.063
Mycyk, M. B. (2020). Extracorporeal membrane oxygenation shows promise for treatment of poisoning some of the time: the challenge to do better by aiming higher. Criti. Care Med. 48, 1235–1237. doi: 10.1097/CCM.0000000000004431
Navas-Blanco, J. R., and Dudaryk, R. (2020). Management of respiratory distress syndrome due to COVID-19 infection. BMC Anesthesiol. 20, 1–6. doi: 10.1186/s12871-020-01095-7
See, H., and Slonim, A. D. (2020). Financial Toxicity after hospitalization; considerations in coronavirus disease 2019 recovery. Criti. Care Med. 48, 1233–1234. doi: 10.1097/CCM.0000000000004436
Shaw, M., and Scott, D. (1998). Performance characteristics of a to and fro disposable soda lime canister. Anaesthesia 53, 454–460.
Silva, D. S. (2020). Ventilators by lottery: the least unjust form of allocation in the COVID-19 Pandemic. Chest 158, 890–891. doi: 10.1016/j.chest.2020.04.049
Silvanius, M., Mitchell, S. J., Pollock, N. W., Frånberg, O., Gennser, M., Lindén, J., et al. (2019). The performance of ‘temperature stick'carbon dioxide absorbent monitors in diving rebreathers. Diving Hyperb. Med. 49, 48–56. doi: 10.28920/dhm49.1.48-56
Tobin, M. J. (2020). “Basing respiratory management of COVID-19 on physiological principles,” in American Journal of Respiratory and Critical Care Medicine, 201:1319–1320. doi: 10.1164/RCCM.202004-1076ED
Wilmshurst, P. T. (2019). Immersion pulmonary oedema: a cardiological perspective. Diving Hyperb. Med. 49, 30–40. doi: 10.28920/dhm49.1.30-40
Keywords: rebreather, ventilation, crisis, dioxygen, ICU
Citation: Vallée N, Rives S, Desruelle A-V, Marzetti S, Barchasz V, Risso J-J and Gies V (2021) High Oxygen Consumption in SARS-COV2: Could the Development of Low-Cost Oxygen Rebreather Be Considered? Front. Physiol. 11:607913. doi: 10.3389/fphys.2020.607913
Received: 22 September 2020; Accepted: 21 December 2020;
Published: 21 January 2021.
Edited by:
Giuseppe Andrea Miserocchi, University of Milano-Bicocca, ItalyReviewed by:
Carmen Silvia Valente Barbas, University of São Paulo, BrazilCopyright © 2021 Vallée, Rives, Desruelle, Marzetti, Barchasz, Risso and Gies. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolas Vallée, bmljb2xhcy52YWxsZWU1QGhvdG1haWwuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.