 Sharen Lee1
Sharen Lee1 Jiandong Zhou2
Jiandong Zhou2 Tong Liu3Konstantinos P. Letsas4Sandeep S. Hothi5Vassilios S. Vassiliou6Guoliang Li7Adrian Baranchuk8Raymond W. Sy9,10Dong Chang11
Tong Liu3Konstantinos P. Letsas4Sandeep S. Hothi5Vassilios S. Vassiliou6Guoliang Li7Adrian Baranchuk8Raymond W. Sy9,10Dong Chang11 Qingpeng Zhang2*
Qingpeng Zhang2* Gary Tse3,11*
Gary Tse3,11*- 1Laboratory of Cardiovascular Physiology, Li Ka Shing Institute of Health Sciences, Hong Kong, China
- 2School of Data Science, City University of Hong Kong, Hong Kong, China
- 3Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular Disease, Department of Cardiology, Tianjin Institute of Cardiology, Second Hospital of Tianjin Medical University, Tianjin, China
- 4Second Department of Cardiology, Laboratory of Cardiac Electrophysiology, Evangelismos General Hospital of Athens, Athens, Greece
- 5Heart and Lung Centre, New Cross Hospital, Wolverhampton, United Kingdom
- 6Norwich Medical School, University of East Anglia, Faculty of Medicine, Imperial College London, London, United Kingdom
- 7Arrhythmia Unit, Department of Cardiovascular Medicine, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China
- 8Division of Cardiology, Kingston General Hospital, Queen’s University, Kingston, ON, Canada
- 9Sydney Medical School, University of Sydney, Sydney, NSW, Australia
- 10Department of Cardiology, Royal Prince Alfred Hospital, University of Sydney, Sydney, NSW, Australia
- 11Xiamen Cardiovascular Hospital, Xiamen University, Xiamen, China
Introduction: Patients with Brugada electrocardiographic (ECG) patterns have differing levels of arrhythmic risk. We hypothesized that temporal variations in certain ECG markers may provide additional value for risk stratification. The present study evaluated the relationship between temporal variability of ECG markers and arrhythmic outcomes in patients with a Brugada pattern ECG. Comparisons were made between low-risk asymptomatic subjects versus high-risk symptomatic patients with a history of syncope, ventricular tachycardia (VT) or ventricular fibrillation (VF).
Methods: A total of 81 patients presenting with Brugada patterns were recruited. Serial ECGs and electronic health records from January 2004 to April 2019 were analyzed. Temporal variability of QRS interval, J point-Tpeak interval (JTp), Tpeak-Tend interval (Tp-e), and ST elevation (STe) in precordial leads V1-3, in addition to RR-interval from lead II, was assessed using standard deviation and difference between maximum and minimum values over the serial ECGs.
Results: Patients presenting with type 1 Brugada ECG pattern initially had significantly higher variability in JTp from lead V2 (SD: 33.5 ± 13.8 vs. 25.2 ± 11.5 ms, P = 0.009; max-min: 98.6 ± 46.2 vs. 78.3 ± 47.6 ms, P = 0.047) and ST elevation in lead V1 (0.117 ± 0.122 vs. 0.053 ± 0.030 mV; P = 0.004). Significantly higher variability in Tp-e interval measured from lead V3 was observed in the VT/VF group compared to the syncope and asymptomatic groups (SD: 20.5 ± 8.5 vs. 16.6 ± 7.3 and 14.7 ± 9.8 ms; P = 0.044; max-min: 70.2 ± 28.9 vs. 56.3 ± 29.0 and 43.5 ± 28.5 ms; P = 0.011).
Conclusion: Temporal variability in ECG indices may provide additional value for risk stratification in patients with Brugada pattern.
Introduction
Brugada syndrome (BrS) is an ion channelopathy which results in characteristic electrocardiographic (ECG) changes and predisposes patients with increased risk of ventricular tachycardia (VT), ventricular fibrillation (VF), and sudden cardiac death (SCD). The stratification of SCD risk is influenced by many factors, primarily the ECG pattern and symptoms presented (Gourraud et al., 2017). Syncope, VT and VF are deemed as strong predictors of SCD, while asymptomatic patients are considered to be of relatively low risk (Sieira et al., 2016). ECG markers are being explored for early identification of high-risk patients before they become symptomatic (Asvestas et al., 2018).
The spatial dispersion of different ECG indices for risk stratification has been well-explored. However, little analysis has been performed on their temporal variability. A recent study has reported significant temporal variability in indices measured from serial ECGs, with greater variability in patients with type 1 pattern (Castro Hevia et al., 2019). In the past, temporal variability in ECG indices has been simply attributed to the recognized dynamicity in Brugada ECG pattern (BrP) (Bayes de Luna et al., 2012). The recent demonstration of the difference in temporal variability between patient subgroups (Gray et al., 2017) inspired our interest to examine the potential use of temporal variability concerning risk stratification. Hence, the present study aims to examine the difference in temporal variability of ECG markers for risk stratification between low-risk asymptomatic patients, and high-risk symptomatic patients with a history of syncope, VT, or VF.
Methods
Patient Selection and Electrocardiographic Measurement
This study received Ethics Approval from The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CREC Ref. No.: 2019.338). Institutional board approval was obtained and waived the need for patient consent in this retrospective study. The present single-center cohort consists of patients who visited the Prince of Wales Hospital, Hong Kong, China from the 1st of January, 2004 to the 1st of April, 2019 with electrocardiogram showing type 1 (cove-shaped) or type 2 (saddle-shaped) Brugada patterns. Patients with zero or one electronically documented ECG were excluded. Discrete ECGs throughout the follow-up duration were analyzed. The following ECG indices for leads V1, V2, and V3 from 12-lead ECG were measured using Philips ECGVue (standard edition): (1) QRS interval; (2) J point-Tpeak interval (J-Tp, interval from J point to the peak of T wave); (3) Tpeak-Tend interval (Tp-e, interval from the peak to the end of T wave returning to baseline); and (4) ST elevation (STe). RR interval was measured from lead II. ECGs were excluded if (1) artefacts were present in leads V1-3; (2) QRS complex and T waves were unidentifiable; and (3) the rhythm was paced.
The patient history was reviewed to identify the presence of syncope, VT and VF. The cohort was divided into three groups based on symptoms documented during follow-up: (1) asymptomatic, (2) syncope, and (3) VT/VF. Patients who presented with both syncope and VT/VF were included in both groups. Patients who presented with type 1 Brugada ECG, and those who did not, were also compared. The average and temporal dispersion of individual ECG indices were calculated. Temporal dispersion was calculated by two methods: (1) maximum – minimum (max-min) value of the index; and (2) standard deviation (SD) of the index over the series of ECG taken.
Statistical Analysis
Statistical analysis was performed using Stata MP 13. Statistical significance is defined as P-value <0.05. Intergroup differences were compared by Kruskal-Wallis’ two-way ANOVA and Fisher’s exact test for continuous and discrete variables, respectively. Pairwise comparison was performed for indices with significant intergroup differences by repeating the Kruskal-Wallis two-way ANOVA. Intra- and inter-observer agreement was assessed by the same investigator 4 weeks apart, and by a second investigator (Supplementary Material). by one-way mixed-effects individual, and two-way random-effects average absolute-agreement intraclass correlation coefficient (ICC), respectively (0 < ICC < 0.4 = poor; 0.4 < ICC < 0.59 = fair; 0.6 < ICC < 0.74 = good; 0.75 < ICC < 1.00 = excellent) (Cicchetti, 1994).
Results
After excluding patients with fewer than two ECG records, the cohort comprised 81 patients (initially type 1 = 35.8%, median follow-up period = 1281 days, interquartile range of follow-up period = 2571 days, 1150 ECGs analyzed, female = 8.6%, age of first BrP = 52.5 ± 1.85, age interquartile range = 24.0 years). All patients were Han Chinese and 79 of the 81 subjects were probands. The remaining two patients were identified from family screening. The age of first BrP and patient sex of the subgroups did not differ significantly (Supplementary Table 1). Both intra- and inter-observer agreement achieved fair to excellent quality (ICC > 0.4; Supplementary Tables 2, 3).
Electrocardiographic indices were compared between patients with an initial type 1 pattern and those who had non-type 1 patterns (Table 1). The initial type 1 group displayed significantly longer lead V3 QRS interval (P = 0.021), shorter lead V3 JTp (P = 0.011), and greater lead V1 ST elevation (P = 0.000) compared to the non-type 1 group. They also showed significantly greater temporal dispersion for both lead V2 JTp (P-value: SD = 0.009, max-min = 0.047) and lead V1 ST elevation (P-value: SD = 0.004, max-min = 0.001).
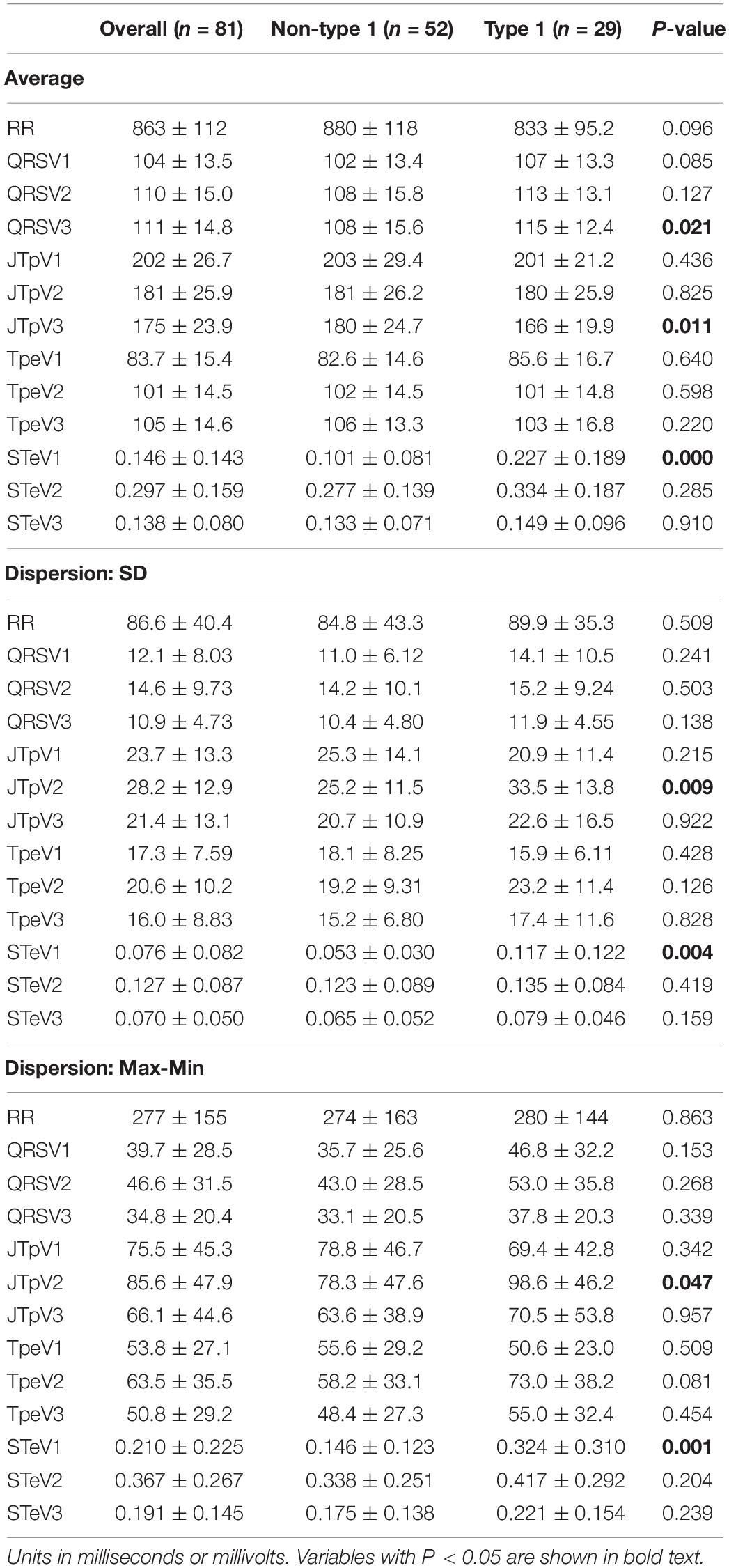
Table 1. ECG biomarkers for initial type 1 vs. non-type 1 patterns.
Subsequent analyses were conducted by comparing ECG indices between asymptomatic patients (n = 39), patients with syncope (n = 38), and patients with VT/VF (n = 13) group. Within the syncope and VT/VF subgroups, five and two patients in the respective groups were initially asymptomatic, and developed syncope or VT/VF over the course of follow-up. A significant increase in variability was found in Tp-e measured form lead V3 under both standard deviation (P = 0.044) and maximum – minimum (P = 0.011) calculations, as shown in Table 2. Under further pairwise comparison, VT/VF group had significantly greater temporal dispersion in comparison to the asymptomatic group with both standard deviation (P = 0.021) and maximum – minimum (P = 0.007) methods, and to the syncope group under maximum- minimum (P = 0.046) calculation. Furthermore, the average extent of STe in lead V3 is significantly higher in VT/VF group in comparison to both the syncope (P = 0.039) and the asymptomatic group (P = 0.010) under pairwise comparison.
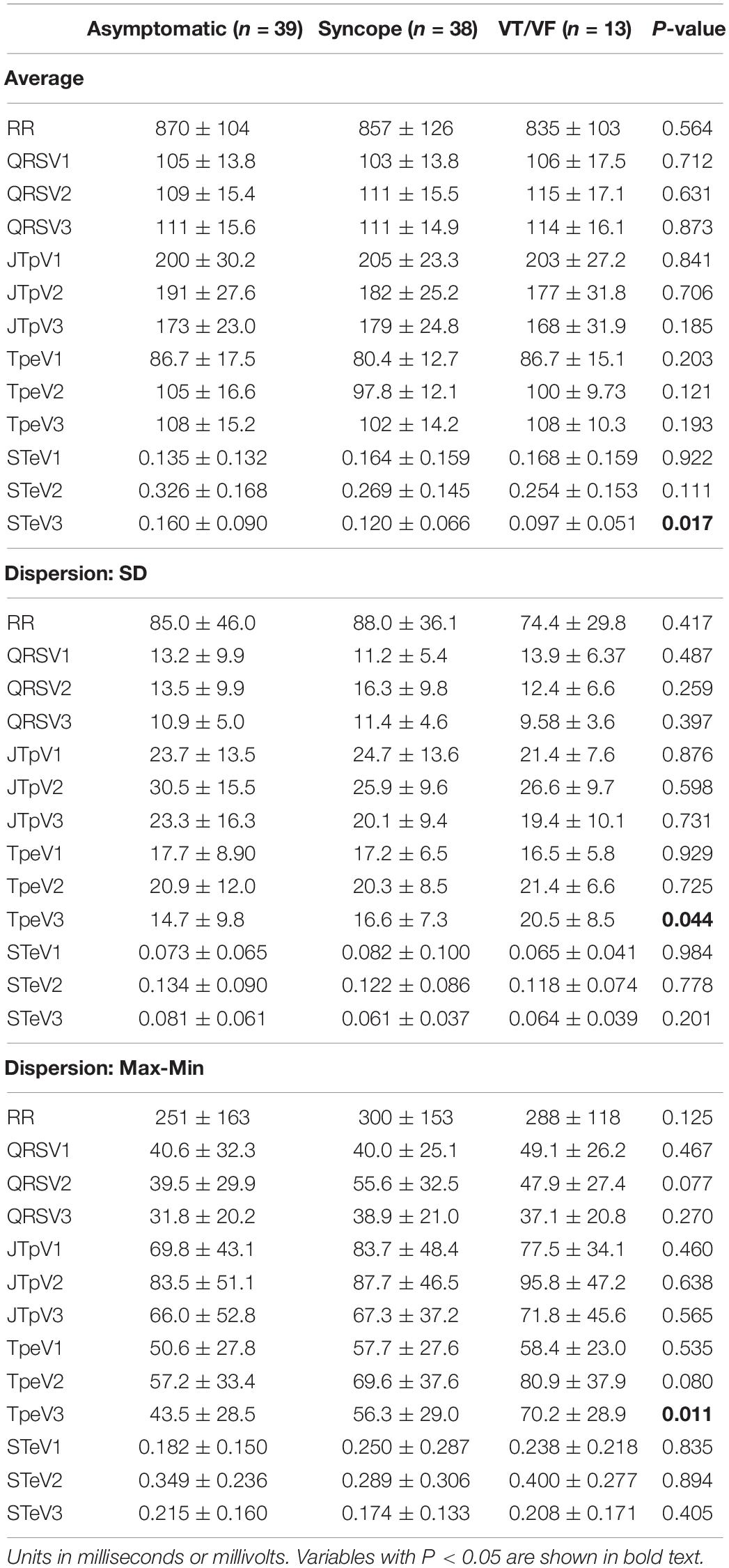
Table 2. ECG biomarkers categorized based on symptoms.
Discussion
The present study demonstrates that increased temporal variability in Tp-e is found in patients with Brugada pattern of higher SCD risk. Tp-e has been used to quantify the transmural dispersion of ventricular repolarization and used in BrS risk-stratification (Xia et al., 2005; Tse et al., 2018a). Increased transmural dispersion prolongs ventricular repolarization, which can lead to re-entry in phase 2 and subsequently ventricular tachyarrhythmia (Yan and Antzelevitch, 1999). Although the dynamicity of the Brugada pattern is well known, the significance of temporal variability in the risk stratification of BrS patients has not been fully explored (Viskin et al., 2018). The significant temporal variability in Tp-e amongst the high-risk arrhythmic group suggests the presence of a temporal variation in the transmural repolarization dispersion, and increased ventricular repolarization instability may explain the marked increase SCD risk in the symptomatic group. The fluctuations in the extent of transmural dispersion are further supported by the insignificant difference in Tp-e, and the dynamic manifestation of Brugada ECG pattern (Antzelevitch et al., 2005). Differing with the study by Castro Hevia et al. (2019), significant temporal variability was not noted in QRS duration in the present study, which might be attributed to the difference in calculation methodology. The significant intergroup differences in the average value of ECG indices is due to the diverse electrocardiographic pattern.
Although the diagnosis of Brugada syndrome focuses on the characteristic ECG pattern in leads V1 and V2, the present study demonstrates that lead V3 can also be useful in risk stratification. Information from lead V3 is often considered to be redundant in the clinical diagnosis of Brugada syndrome since it is less sensitive than leads V1-2 for Brugada ECG changes (Govindan et al., 2010). However, the present findings suggest that lead V3 might be able to provide insights into risk stratification through its sensitivity for ECG variability, and for which further research is needed to explore its clinical value in variability detection. It has been reported that Tp-e is longest in V3 when measured in children, possibly due to a higher number of M cells distributed in the interventricular septum (Bieganowska et al., 2013). The difference in temporal variability across the leads highlights the heterogeneity in ventricular repolarization of Brugada patients. Further research on the spatiotemporal dispersion of ECG indices is needed to elucidate the dynamicity in Brugada pattern.
The insignificant difference between the asymptomatic and syncope groups could be explained by the exact etiology of syncope. It has been reported that whilst patients presenting with unexplained syncope and a positive electrophysiological study are at high risk for arrhythmia, those with neurally mediated syncope share a similar prognosis to asymptomatic patients (Giustetto et al., 2017). Furthermore, there is growing evidence for similar genetic mutations to be present in both epilepsy and BrS. Syncope of such potential non-cardiogenic origins is unlikely to be affected by temporal variability of cardiac conduction and repolarisation, which might explain the insignificant results (Parisi et al., 2013; Tiron et al., 2015).
To reduce bias in ECG analysis, automatic measurements by the ECG machine can be applied. However, a comparison should be made against manual measurements to confirm accuracy in the detection of different ECG features, for example, the J point in Brugada ECGs. Future studies should further evaluate the use of automatic measurements in all ECG parameters analyzed in the present study and assess the clinical applications of the ECG parameters, particularly Tp-e. Whilst clinical studies have demonstrated that prolonged Tp-e reflects the presence of a resolved, temporary, arrhythmogenic substrate in patients with acute myocardial infarction, and predicts mortality for these patients, further research is required to explore its applicability in outcome prediction for spontaneous arrhythmia due to a channelopathy (Haarmark et al., 2009; Elitok et al., 2015).
Strengths and Limitations
There are several notable strengths of the present study. Firstly, a comprehensive analysis of different ECG features has been performed, with 3–50 ECGs measured per patient, and a total of more than 1000 ECGs analyzed. This extended previous studies using only single ECG measurements at baseline (Tse et al., 2018b; Lee et al., 2020). Moreover, there is good inter and intra-observer variability, as reflected by the intra-class coefficient. Several limitations should also be noted for the present study. First, the cohort is small and from a single center, hence findings should be externally validated and tested in a separate larger cohort in the future. Gender differences were not explored in the present study due to the limited number of female patients (n = 7). Since the majority of the patients were distributed in the middle ages (median age of first Brugada BrP onset = 53.0 years, interquartile range = 20.0 years), in addition to the relatively small cohort, the age differences were not examined. Unfortunately, only two patients undergone genetic testing in the present cohort, hence their genetic status cannot be commented upon. Moreover, the retrospective nature of the present study is susceptible to the bias inherent to such analyses. Besides, the sensitivity of the caliper used in measurement is limited by its one-decimal-place display, which results in a larger error in measuring small values, such as STe. The intervals between serial ECGs taken is variable between patients, and within a single patient, with more ECGs taken when the patients are less stable. Therefore, the ECG indices measured may tend to reflect a state of instability Errors may also be introduced in view of different operators undertaking the ECGs on different days. Furthermore, the relatively short follow-up duration limits the predictive value of the ECG parameters found toward patient life expectancy.
Conclusion
The present study demonstrates the presence of increased temporal variability in Tp-e amongst high-risk BrS patients, which illustrates a potential role for the analysis of serial changes in the surface ECG in the prognostic workup of BrS. Further research into the spatiotemporal dispersion of Brugada ECG patterns is need to gain insights into the dynamicity of Brugada electrophysiological changes.
Data Availability Statement
The anonymized dataset and relevant materials have been made publicly available at Zenodo and can be accessed here: https://zenodo.org/record/3351892; https://zenodo.org/record/3266172; and https://zenodo.org/record/3266179.
Ethics Statement
The studies involving human participants were reviewed and approved by The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (The Joint CUHK-NTEC CREC). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
SL and GT contributed to the study conception, data acquisition, database building, statistical analysis, manuscript drafting, and manuscript revision. All authors contributed to the data interpretation, statistical analysis, and manuscript revision.
Funding
This study was supported by the Research Grants Council of Hong Kong (T32-102/14-N to QZ), the Research Foundation of Major Science and Technology Projects of Tianjin Municipal Science and Technology Bureau (18ZXRHSY00180 to TL), and the National Natural Science Foundation of China (NSFC: 71972164 and 71972164 to TL).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2020.00953/full#supplementary-material
References
Antzelevitch, C., Brugada, P., Brugada, J., and Brugada, R. (2005). Brugada syndrome: from cell to bedside. Curr. Probl. Cardiol. 30, 9–54.
Asvestas, D., Tse, G., Baranchuk, A., Bazoukis, G., Liu, T., Saplaouras, A., et al. (2018). High risk electrocardiographic markers in Brugada syndrome. Int. J. Cardiol. Heart Vasc. 18, 58–64.
Bayes de Luna, A., Brugada, J., Baranchuk, A., Borggrefe, M., Breithardt, G., Goldwasser, D., et al. (2012). Current electrocardiographic criteria for diagnosis of brugada pattern: a consensus report. J. Electrocardiol. 45, 433–442.
Bieganowska, K., Sawicka-Parobczyk, M., Bieganowski, M., and Piskorski, J. (2013). Tpeak -tend interval in 12-lead electrocardiogram of healthy children and adolescents tpeak -tend interval in childhood. Ann. Noninvas. Electrocardiol. 18, 344–351.
Castro Hevia, J., Dorantes Sanchez, M., Martinez Lopez, F., Castaneda Chirino, O., Falcon Rodriguez, R., Puga Bravo, M., et al. (2019). Multiple serial ECGs aid with the diagnosis and prognosis of Brugada syndrome. Int. J. Cardiol. 277, 130–135.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 6, 284–290.
Elitok, A., Ikitimur, B., Onur, I., Oz, F., Emet, S., Karaayvaz, E. B., et al. (2015). The relationship between T-wave peak-to end interval and ST segment recovery on intracoronary ECG during primary PCI. Eur. Rev. Med. Pharmacol. Sci. 19, 1086–1091.
Giustetto, C., Cerrato, N., Ruffino, E., Gribaudo, E., Scrocco, C., Barbonaglia, L., et al. (2017). Etiological diagnosis, prognostic significance and role of electrophysiological study in patients with Brugada ECG and syncope. Int. J. Cardiol. 241, 188–193.
Gourraud, J. B., Barc, J., Thollet, A., Le Marec, H., and Probst, V. (2017). Brugada syndrome: Diagnosis, risk stratification and management. Arch. Cardiovasc. Dis. 110, 188–195.
Govindan, M., Batchvarov, V. N., Raju, H., Shanmugam, N., Bizrah, M., Bastiaenen, R., et al. (2010). Utility of high and standard right precordial leads during ajmaline testing for the diagnosis of Brugada syndrome. Heart 96, 1904–1908.
Gray, B., Kirby, A., Kabunga, P., Freedman, S. B., Yeates, L., Kanthan, A., et al. (2017). Twelve-lead ambulatory electrocardiographic monitoring in Brugada syndrome: potential diagnostic and prognostic implications. Heart Rhythm 14, 866–874.
Haarmark, C., Hansen, P. R., Vedel-Larsen, E., Pedersen, S. H., Graff, C., Andersen, M. P., et al. (2009). The prognostic value of the Tpeak-Tend interval in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. J. Electrocardiol. 42, 555–560.
Lee, S., Li, K. H. C., Zhou, J., Leung, K. S. K., Lai, R. W. C., Li, G., et al. (2020). Outcomes in brugada syndrome patients with implantable cardioverter-defibrillators: insights from the sglt2 registry. Front. Physiol. 11:204. doi: 10.3389/fphys.2020.00204
Parisi, P., Oliva, A., Coll Vidal, M., Partemi, S., Campuzano, O., Iglesias, A., et al. (2013). Coexistence of epilepsy and Brugada syndrome in a family with SCN5A mutation. Epilepsy Res. 105, 415–418.
Sieira, J., Dendramis, G., and Brugada, P. (2016). Pathogenesis and management of Brugada syndrome. Nat. Rev. Cardiol. 13, 744–756.
Tiron, C., Campuzano, O., Perez-Serra, A., Mademont, I., Coll, M., Allegue, C., et al. (2015). Further evidence of the association between LQT syndrome and epilepsy in a family with KCNQ1 pathogenic variant. Seizure 25, 65–67.
Tse, G., Gong, M., Li, C. K. H., Leung, K. S. K., Georgopoulos, S., Bazoukis, G., et al. (2018a). Tpeak-Tend, Tpeak-Tend/QT ratio and Tpeak-Tend dispersion for risk stratification in Brugada Syndrome: A systematic review and meta-analysis. J. Arrhythm. 34, 587–597.
Tse, G., Li, K. H. C., Li, G., Liu, T., Bazoukis, G., Wong, W. T., et al. (2018b). Higher dispersion measures of conduction and repolarization in type 1 compared to non-type 1 Brugada syndrome patients: an electrocardiographic study from a single center. Front. Cardiovasc. Med. 5:132. doi: 10.3389/fphys.2020.00132
Viskin, S., Hochstadt, A., and Rosso, R. (2018). Type-I paradox of Brugada syndrome. J. Am. Heart Assoc. 7:e009298. doi: 10.1161/JAHA.118.009298
Xia, Y., Liang, Y., Kongstad, O., Holm, M., Olsson, B., and Yuan, S. (2005). Tpeak-Tend interval as an index of global dispersion of ventricular repolarization: evaluations using monophasic action potential mapping of the epi- and endocardium in swine. J. Interv. Card. Electrophysiol. 14, 79–87.
Keywords: Brugada, temporal, variability, repolarization, ECG
Citation: Lee S, Zhou J, Liu T, Letsas KP, Hothi SS, Vassiliou VS, Li G, Baranchuk A, Sy RW, Chang D, Zhang Q and Tse G (2020) Temporal Variability in Electrocardiographic Indices in Subjects With Brugada Patterns. Front. Physiol. 11:953. doi: 10.3389/fphys.2020.00953
Received: 06 April 2020; Accepted: 15 July 2020;
Published: 03 September 2020.
Edited by:
Ruben Coronel, University of Amsterdam, NetherlandsReviewed by:
Michelle M. Monasky, IRCCS Policlinico San Donato, ItalyDan Hu, Renmin Hospital of Wuhan University, China
Copyright © 2020 Lee, Zhou, Liu, Letsas, Hothi, Vassiliou, Li, Baranchuk, Sy, Chang, Zhang and Tse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qingpeng Zhang, cWluZ3BlbmcuemhhbmdAY2l0eXUuZWR1Lmhr; Gary Tse, Z2FyeS50c2VAZG9jdG9ycy5vcmcudWs=; Z2FyeXRzZTg2QGdtYWlsLmNvbQ==