
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol. , 19 February 2019
Sec. Exercise Physiology
Volume 10 - 2019 | https://doi.org/10.3389/fphys.2019.00130
This article is part of the Research Topic Children's Exercise Physiology View all 29 articles
 Guillermo Felipe López-Sánchez1*
Guillermo Felipe López-Sánchez1* Maurizio Sgroi2Stefano D’Ottavio2Arturo Díaz-Suárez1
Maurizio Sgroi2Stefano D’Ottavio2Arturo Díaz-Suárez1 Sixto González-Víllora3
Sixto González-Víllora3 Nicola Veronese4
Nicola Veronese4 Lee Smith5
Lee Smith5The objective was to analyze body composition in children and adolescents of Southern Europe to identify prevalence of overweight and obesity. This investigation involved 512 girls and 488 boys between 7-to 19-years. Variables evaluated were Body Mass Index (BMI) and Fat Mass (FM; electrical bioimpedance). The references used to establish prevalence according to BMI were those of the World Health Organization (WHO) and the International Obesity Task Force (IOTF); in the case of FM, the Child Growth Foundation (CGF) reference was used. There were significant differences (p < 0.05) in the prevalence of overweight and obesity between the three classifications (32.3% according to IOTF, 37.3% according to WHO, and 39.8% according to CGF), being higher in males. WHO-IOTF concordance was substantial (kappa = 0.793), whereas concordances WHO-CGF (kappa = 0.504) and IOTF-CGF (kappa = 0.447) were moderate. The authors recommend evaluating overweight and obesity not only with BMI, but also with FM, and always specify the references used.
Overweight and obesity can be defined as an abnormal or excessive accumulation of fat that can be harmful toward one’s health (World Health Organization [WHO], 2017). Body mass index (BMI) is a simple indicator of the connection between weight and height that is frequently used to indirectly identify overweight and obesity (World Health Organization [WHO], 2017). The simplicity and low cost of BMI has made it a popular indicator to identify overweight and obesity in science and practice (McCarthy et al., 2006). However, BMI does not distinguish between increased mass in the form of fat, lean tissue or bone, and consequently, it may lead to significant misclassification. Therefore, due to excess fat being a pathology that defines obesity, it would be ideal to also evaluate total fat mass (McCarthy et al., 2006). The evaluation of fat mass per se allows one to obtain important information about the state of the health of the population under study, as well as identify those at risk of certain diseases (Alburquerque Sendín, 2008). For example, excessive fat mass has been shown to be associated with Type 2 Diabetes Mellitus (Abdullah et al., 2010), cancer (Renehan et al., 2008), coronary heart disease and associated risk factors (Bogers et al., 2007), depression (Luppino et al., 2010), and early mortality (Flegal et al., 2013), to list just a few.
Hence, it is clear when studying the prevalence of overweight and obesity, that it is highly recommended to evaluate not only BMI, but also the percentage of fat mass. In addition, consideration must be given to the cut off points used to classify children and adolescents, an aspect dealt with in previous studies (Wang and Wang, 2002; De Onis and Lobstein, 2010; Shields and Tremblay, 2010; Espín Ríos et al., 2013; Bergel et al., 2014; Lasarte-Velillas et al., 2015; Polo Martín et al., 2015). These studies investigated the prevalence of overweight and obesity but focused only on the cut-off points for BMI and not on cut-off points for fat mass. The present article adds to this literature by comparing cut-off points for BMI but also for fat mass, studying the three main international references: World Health Organization (WHO), International Obesity Task Force (IOTF), and Child Growth Foundation (CGF).
The main objective of this research is to evaluate the BMI and fat mass of children and adolescents residing in Southern Europe, studying the prevalence of overweight and obesity according to common international references of these two indicators, and observing the degree of concordance that these different classifications present. This will provide updated data on BMI, fat mass, and prevalence of overweight and obesity in children and adolescents residing in Southern Europe. Moreover, this study will provide evidence about differences between common international references when classifying children and adolescents weight status.
A total of thirteen schools from Southern Europe, nine from Southern Italy (regions of Lazio and Calabria) and four from Southern Spain (region of Murcia) were included in this study. The final sample was made up of 1,000 children and adolescents (512 female and 488 male) between the ages of 7 and 19 years. Excluded from the study were those children and adolescents who did not fulfill any of the recommendations for an adequate analysis of electric bioimpedance, described below. The estimated maximum sampling error at 95% confidence level (p ≤ 0.05) for a sample size of 1000 is ±3.1% (Wimmer, 2011).
This research project was carried out according to the International Code of Medical Ethics (Declaration of Helsinki) for experiments with human beings and, was approved by the Research Ethics Commission of the University of Murcia (No. 03/02/2012). Moreover, the parents/legal guardians of all the participants signed an informed consent form for their children and adolescents to take part. Also, children and adolescents provided assent. The children and adolescents were coded individually, and the details treated anonymously.
The measurements were carried out at school, in an indoor hall prepared for the occasion during the morning timetable. Height was measured with the portable height rod of Tanita model Leicester HR 001 (Tanita, Tokyo, Japan), with the precision of 0.1 cm and with the subjects standing up and barefooted. Weight and total fat mass were measured with the Tanita BC-418-MA Segmental Body Composition Analyzer (Tanita, Tokyo, Japan), with the corresponding correction for the weight of the clothes (underwear or short sleeve). The procedure required the subjects to be standing with bare feet on the places marked on the analyzer, at the same time as they held onto the handles, one in each hand. The analysis through electric bioimpedance lasted approximately 30 s per subject. BMI was calculated with the formula Weight (kg) / Height2 (m). Even though the Tanita BC-481-MA Analyzer provides separate measurements for the fat in the torso and the inferior and superior extremities, only the percentage of total fat mass was taken into consideration to analyze the prevalence of overweight and obesity in the study sample. As indicated by McCarthy et al. (2006), the equations used for this model are based on bioimpedance, weight, height and age, and were obtained through calibration and validation studied with Dual-energy X-ray absorptiometry (DXA) and BodPod, having a standard error of 2.7% for the body mass of boys and of 2.8% for girls. The validity of this method was also established by the studies carried out by Merritt and Ballinger (2003) and Prefontaine and Ballinger (2003). The software used to pass the data to the computer was Suite Biologica 7.1. Moreover, all recommendations to collect electric bioimpedance data were followed (Sgroi and De Lorenzo, 2011; TANITA, 2016). First, a letter was given to parents, teachers and participants explaining in detail procedures that had to be followed before data were collected, such as no excess of food and drink the day before, no intense exercise in the last 12 h, no alcohol consumed in the last 12 h, no metallic objects, no pace-makers, not done during the menstrual cycle and not during pregnancy. These aspects were also checked by researchers asking participants prior to data collection. Data were collected at 11.00 am, before lunch, to ensure that data were collected more than 3 h after participants woke, and to avoid participants eating and drinking 3 h prior to measurement. Finally, prior to data collection the participants were asked to urinate to follow standard procedure for biompedance measurement.
The references used to establish the prevalence of overweight and obesity according to the BMI were from the WHO (De Onis et al., 2007) and the IOTF (Cole et al., 2000; Lobstein et al., 2004; Cole and Lobstein, 2012); in the case of FM, CGF was used as a reference (McCarthy et al., 2006).
First, the normality of continuous variables was assessed through the Kolmogorov-Smirnov test. The medium values and the standard deviation (SD) of the BMI were calculated, along with the percentage of fat mass, globally, by gender and age. A gender comparison was carried out with the t-test for independent samples. Furthermore, the size of the effect was calculated using Cohen’s d (Cohen, 1988).
In addition, the prevalence of overweight and obesity were calculated, by gender and age for the three references. The significant differences between references were calculated (Franklin, 2007) as well as the degree of concordance between each pair using the kappa coefficient (Cohen, 1960; Landis and Koch, 1977; Cerda and Villarroel, 2008). Traditionally, values <0 indicate no agreement, 0–0.20 slight, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 substantial, and 0.81–1 almost perfect agreement. Finally, the comparison of the prevalence of overweight and obesity between gender was carried out using the chi-square test (χ2). The significant value used was p < 0.05. The statistical package SPSS-22.0 (Statistical Package for the Social Sciences) and Microsoft Office Excel were used to carry out the analysis.
Table 1 shows the medium values and SD corresponding to the BMI and the percentage of fat mass of the 1000 children and adolescents from the sample. The results are shown organized in function to age and gender (Supplementary Figures S1, S2).
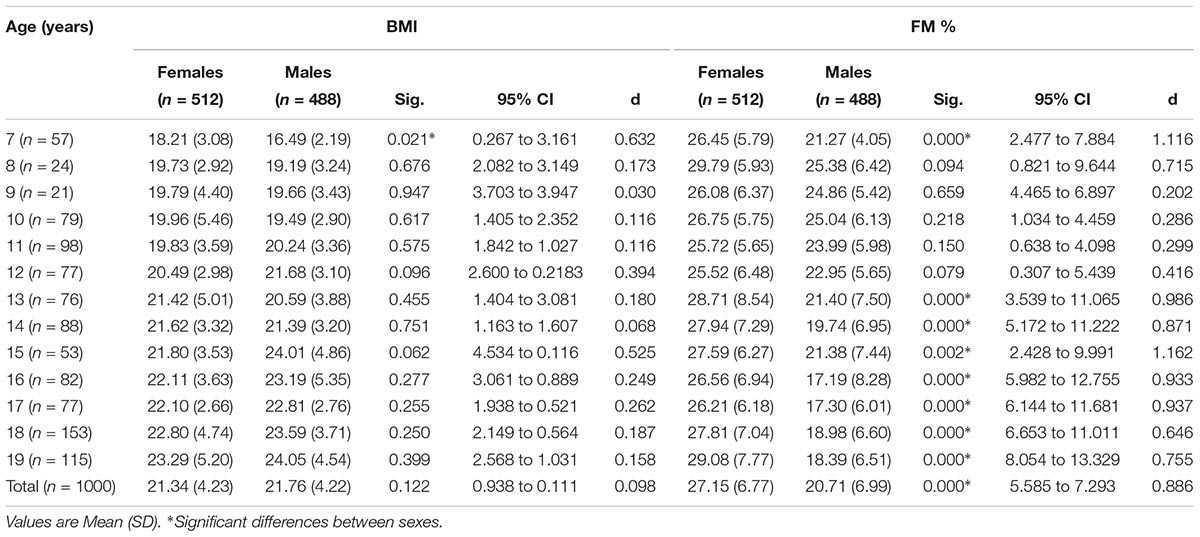
Table 1. Comparison of means of BMI and FM% (N = 1000).
It is noteworthy that girls show higher medium values of fat mass than boys (p < 0.0001; d = 0.886). The fat mass in the female gender was higher in all age groups, showing significant differences at 7 years of age and from 13 to 19 years of age.
Tables 2, 3 show the prevalence of “overweight/excess fat” and “obesity” by gender, age and globally by the three references which have been studied: WHO, IOTF, CGF. They also show the significant differences found between references. Moreover, Supplementary Figures S3–S8 show graphically the different prevalences found when classifying the sample with the 3 references used.
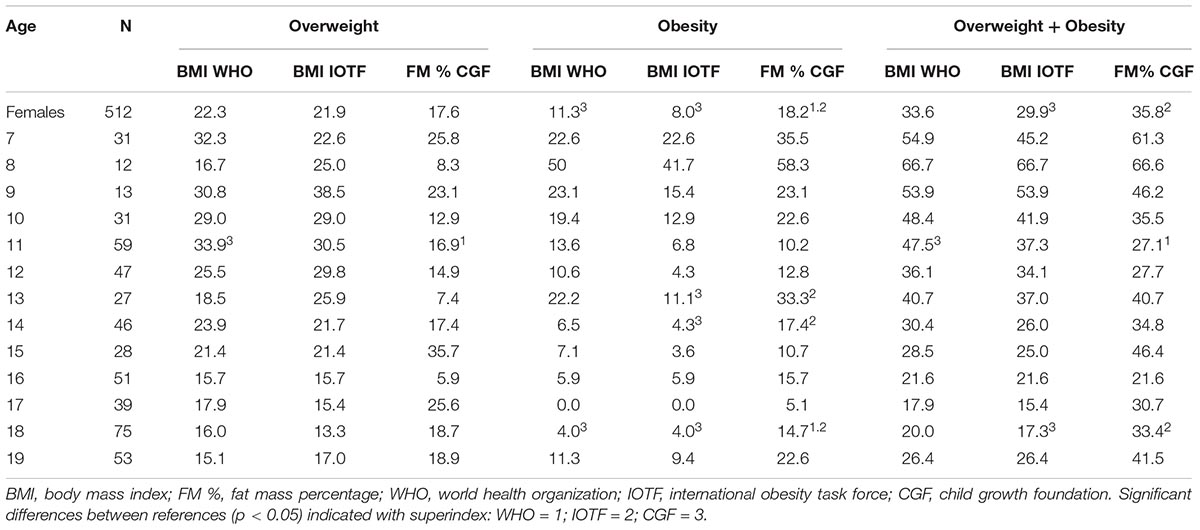
Table 2. Prevalence (%) of overweight and obesity of females by age (N = 512).
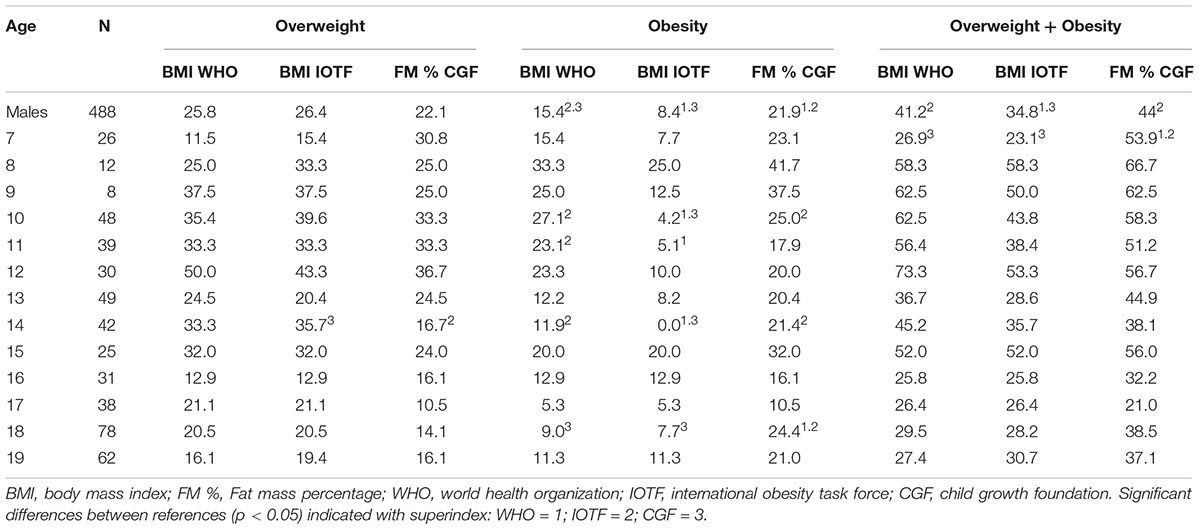
Table 3. Prevalence (%) of overweight and obesity of males by age (N = 488).
Significant differences (p < 0.05) were found in the prevalence of overweight and obesity between the three classifications. The total prevalence of overweight and obesity was of 32.3% according to IOTF, 37.3% according to WHO and 39.8% according to CGF. The WHO-IOTF concordance was substantial (kappa = 0.793), meanwhile the WHO-CGF (kappa = 0.504) and IOTF-CGF (kappa = 0.447) concordances were moderate.
The χ2 test showed that there is no statistical significance when making a global comparison of the prevalence of overweight and obesity in function to gender. However, it was observed that male demonstrate a greater prevalence independent of the classification used.
The three classifications used found a high prevalence of overweight and obesity in the studied sample. There were significant differences between the classifications: 32.3% according to IOTF, 37.3% according to WHO and 39.8% according to CGF. The WHO-IOTF concordance was substantial (kappa = 0.793), meanwhile the WHO-CGF (kappa = 0.504) and IOTF-CGF (kappa = 0.447) concordances were moderate.
The results of this study contrast with those found by Espín Ríos et al. (2013) who evaluated the BMI of 178,894 students (91,517 boys and 87,377 girls) of ages 2 to 14 in the region of Murcia (Spain), classifying them according to the criteria provided by the WHO and IOTF. Espín Ríos et al. (2013) found a greater prevalence of overweight and obesity in girls in contrast to the present study: 42.1% according to the WHO and 33.2% according to IOTF, in comparison to the 33.6 and 29.9% in this study. In boys, they observed a prevalence of 45.2% according to the WHO and 30.9% according to IOTF, in comparison to the 41.2 and 34.8% in this study. In terms of both genders, there was a prevalence of 43.7% according to the WHO and of 32% according to IOTF, percentages that somewhat differ to the current study: 37.3 and 32.3%, respectively. These observed discrepancies may be explained by differences in samples sizes and the different populations studied (Spain and Spain/Italy). For example, Spain and Italy are countries of Southern Europe with a similar Mediterranean diet, however, the percentage of total fat in the diet of Spanish adolescents has been found to be higher than in the diet of Italian adolescents (Cruz, 2000).
The National Health Survey 2011–2012 carried out by the National Institute of Statistics “INE” (Spain), in children and adolescents aged 2 to 17 years (3,580,100 female and 3,883,500 male), determined the BMI of all the participants and obtained the following percentages for overweight, obesity and excess weight: girls (16.94% overweight, 9.56% obesity, 26.50% excess weight), boys (19.46% overweight, 9.57% obesity, and 29.03% excess weight). The percentage of excess weight obtained by the Instituto Nacional de Estadística [INE] (2012) in girls (26.50%) is lower than those obtained in the present study (33.6% according to the WHO, 29.9% according to IOTF, and 35.8% according to CGF). Moreover, in boys the percentage of excess weight which was obtained by the INE (29.03%) is lower than the percentages obtained in the present study (41.2% according to the WHO, 34.8% according to IOTF, and 44% according to CGF). When only children and adolescents from the region of Murcia were considered, the data of the INE determined the following percentages for overweight, obesity and excess weight: girls (9.77% overweight, 16.75% obesity, 26.52% excess weight), boys (19.16% overweight, 9.46% obesity and 25.62% excess weight). The percentage of excess weight obtained in Murcia by the Instituto Nacional de Estadística [INE] (2012) in girls is lower than those obtained in the present study (33.6% according to the WHO, 29.9% according to IOTF, and 35.8% according to CGF). Moreover, in boys the percentage of excess weight which was obtained in Murcia by the INE (25.62%) is lower than the percentages obtained in this study (41.2% according to the WHO, 34.8% according to IOTF, and 44% according to CGF). This suggests that excess weight is increasing in the region of Murcia, Spain.
In the study by the National Institute of Statistics “ISTAT” (Italy) in 2010, in those aged 6 to 17 years (3,368,000 female and 3,558,000 male), the BMI of the participants was determined, and the following percentages of excess weight were obtained, according to IOTF criteria: 23.2% of excess weight in girls and 28.9% of excess weight in boys. The percentage of excess weight obtained by Instituto Nacional de Estadística [INE] (2012) for girls (23.2%) was lower than the estimate obtained in this study by IOTF (29.9%). Moreover, in boys the percentage of excess weight obtained by the ISTAT (28.9%) is lower than the percentage obtained in the present study by the IOTF (34.8%). When only children and adolescents from the regions of Lazio and Calabria were considered, the data of the ISTAT determined the following percentage for excess weight: 27.0% of excess weight in Lazio and 30.4% of excess weight in Calabria. This suggests that excess weight is increasing in the regions of Lazio and Calabria.
Previous studies (Wang and Wang, 2002; Shields and Tremblay, 2010; Espín Ríos et al., 2013; Bergel et al., 2014; López-Sánchez et al., 2015) with different samples (schoolchildren from Ibero-American countries, Canada, United States, Russia and China) also found important differences when using different classifications to evaluate the prevalence of overweight and obesity according to BMI, in the same way as the current study. However, the present study also found significant differences with the cut-off points for fat mass, which is why it is essential to specify always the methods and references used until an agreement is reached.
The main strength of the present study is the comparison between cut-off points for BMI and fat mass in a sample of children and adolescents residing in Southern Europe. However, the present study is not without limitations, the sample was composed of 1000 children and adolescents from distinct geographic areas/countries and, although all the recommendations for an adequate analysis of electric bioimpedance were followed, the electrical bioimpedance is not the gold standard method to evaluate fat mass.
The present findings suggest that there is a high prevalence of overweight and obesity in children and adolescents residing in Southern Europe. However, prevalence estimates of overweight and obesity differ by methods and reference cut points. Higher prevalence was obtained with the classification of CGF (fat mass), followed by the classifications of WHO and IOTF (BMI).
A precise definition of overweight and obesity is needed, as well recommended methods for evaluation, and accurate cut-off points. The authors of this study recommend the evaluation of overweight and obesity not only by BMI, but also through the percentage of fat mass, and to always specify the references used to classify the sample.
It would also be convenient to carry out regular assessments in schools, which could be carried out by the Physical Education teacher because of the direct connection between the subject and overweight and obesity. This simple practice would provide updated reference values in any geographical location.
Finally, due to the high prevalence of overweight and obesity found in this study, it would be interesting to carry out intervention programs in children and adolescents, through physical activity and a dietary improvement, to reduce their fat mass and BMI values and develop healthy lifestyle habits. To control the dietary habits during these intervention programs, researchers should evaluate regularly the quality of the diet of the children and adolescents participating in the intervention. Future researchers should also consider the psychological factors of motivation and perceived motor competence, and the family influence, when carrying out intervention programs to ensure that the children and adolescents will adhere to any program put in place.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This research was funded by Seneca Foundation—Agency for Science and Technology of the Region of Murcia (Spain). Grant number: 19113/FPI/13 (GL-S).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank all the subjects that participated in this study. This manuscript includes content which first appeared in the doctoral thesis of the first author (López-Sánchez, 2017).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2019.00130/full#supplementary-material
Abdullah, A., Peeters, A., de Courten, M., and Stoelwinder, J. (2010). The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res. Clin. Pract. 89, 309–319. doi: 10.1016/j.diabres.2010.04.012
Alburquerque Sendín, F. (2008). Estudio Comparativo Intermetodológico de la Composición Corporal (Antropometría, BIA y DEXA). Ph.D. thesis, University of Salamanca, Salamanca.
Bergel, M. L., Cesani, M. F., Cordero, M. L., Navazo, B., Olmedo, S., Quintero, F., et al. (2014). Valoración nutricional de escolares de tres países iberoamericanos: análisis comparativo de las referencias propuestas por la IOTF y la OMS. Nutr. Clín. Dietét. Hosp. 34, 8–15. doi: 10.12873/341berge
Bogers, R. P., Bemelmans, W. J., Hoogenveen, R. T., Boshuizen, H. C., Woodward, M., Knekt, P., et al. (2007). Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch. Intern. Med. 167, 1720–1728. doi: 10.1001/archinte.167.16.1720
Cerda, J., and Villarroel, L. (2008). Evaluación de la concordancia inter-observador en investigación pediátrica: coeficiente de Kappa. Rev. Chil. Pediatr. 79, 54–58. doi: 10.4067/S0370-41062008000100008
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 20, 37–46. doi: 10.1177/001316446002000104
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences, 2nd Edn. Hillsdale, MI: Lawrence Erlbaum.
Cole, T. J., Bellizzi, M. C., Flegal, K. M., and Dietz, W. H. (2000). Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320, 1240–1243. doi: 10.1136/bmj.320.7244.1240
Cole, T. J., and Lobstein, T. (2012). Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 7, 284–294. doi: 10.1111/j.2047-6310.2012.00064.x
Cruz, J. A. A. (2000). Dietary habits and nutritional status in adolescents over Europe-Southern Europe. Eur. J. Clin. Nutr. 54, S29–S35. doi: 10.1038/sj.ejcn.1600981
De Onis, M., and Lobstein, T. (2010). Defining obesity risk status in the general childhood population: which cut-offs should we use? Int. J. Pediatr. Obes. 5, 458–460. doi: 10.3109/17477161003615583
De Onis, M., Onyango, A. W., Borghi, E., Siyam, A., Nishida, C., and Siekmann, J. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 85, 660–667. doi: 10.2471/BLT.07.043497
Espín Ríos, M. I., Pérez Flores, D., Sánchez Ruíz, J. F., and Salmerón Martínez, D. (2013). Prevalencia de obesidad infantil en la Región de Murcia, valorando distintas referencias para el índice de masa corporal. Ann. Pediatr. 78, 374–381. doi: 10.1016/j.anpedi.2012.09.007
Flegal, K. M., Kit, B. K., Orpana, H., and Graubard, B. I. (2013). Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA 309, 71–82. doi: 10.1001/jama.2012.113905
Franklin, C. H. (2007). The Margin of Error for Differences in Polls. Available at: http://abcnews.go.com/images/PollingUnit/MOEFranklin.pdf
Instituto Nacional de Estadística [INE]. (2012). Encuesta Nacional de Salud 2011-2012: Índice de Masa Corporal en Población Infantil Según Sexo y Grupo de Edad. Población de 2 a 17 años (España). Madrid: Instituto Nacional de Estadística.
Istituto Nazionale di Statistica [ISTAT]. (2010). Eccesso di Peso nei Bambini e Ragazzi di 6-17 Anni nel 2010 (Italia). Rome: ISTAT.
Landis, J. R., and Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics 33, 159–174. doi: 10.2307/2529310
Lasarte-Velillas, J. J., Hernández-Aguilar, M. T., Martínez-Boyero, T., Soria-Cabeza, G., Soria-Ruiz, D., Bastarós-García, J. C., et al. (2015). Estimación de la prevalencia de sobrepeso y obesidad infantil en un sector sanitario de Zaragoza utilizando diferentes estándares de crecimiento. Ann. Pediatr. 82, 152–158. doi: 10.1016/j.anpedi.2014.03.005
Lobstein, T., Baur, L., Uauy, R., and IASO International Obesity TaskForce [IOTF]. (2004). Obesity in children and young people: a crisis in public health. Obes. Rev. 5, 4–85. doi: 10.1111/j.1467-789X.2004.00133.x
López-Sánchez, G. F. (2017). Body composition, Body image, Physical Activity and Health in Children and Adolescents. Ph.D. thesis, University of Murcia, Murcia. doi: 10.1111/j.1467-789X.2004.00133.x
López-Sánchez, G. F., Borrego-Balsalobre, F. J., and Díaz-Suárez, A. (2015). Fat mass and body mass index of 11-year-old schoolchildren from the Region of Murcia. TRANCES 7, 583–598.
Luppino, F. S., de Wit, L. M., Bouvy, P. F., Stijnen, T., Cuijpers, P., Penninx, B. W., et al. (2010). Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 67, 220–229. doi: 10.1001/archgenpsychiatry.2010.2
McCarthy, H. D., Cole, T. J., Fry, T., Jebb, S. A., and Prentice, A. M. (2006). Body fat reference curves for children. Int. J. Obes. 30, 598–602. doi: 10.1038/sj.ijo.0803232
Merritt, S., and Ballinger, D. (2003). Reliability and feasibility of Tanita body composition scale in high school physical education and health classes. Res. Q. Exerc. Sport. 74:A26.
Polo Martín, P., Abellán, J. J., Nájar Godoy, M., and Álvarez de Laviada Mulero, T. (2015). Tablas de crecimiento: impacto sobre la prevalencia de los trastornos nutritivos. Ann. Pediatr. 82, 325–337. doi: 10.1016/j.anpedi.2014.06.004
Prefontaine, M., and Ballinger, D. (2003). A comparison of body composition of junior high school girls in physical education using skinfolds and bioimpedance techniques. Res. Q. Exerc. Sport 74, A26–A27.
Renehan, A. G., Tyson, M., Egger, M., Heller, R. F., and Zwahlen, M. (2008). Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371, 569–578. doi: 10.1016/S0140-6736(08)60269-X
Sgroi, M., and De Lorenzo, A. (2011). Stato Nutrizionale, Dieta Mediterranea e Attivita’ Fisica: Analisi e Valutazione Della Composizione Corporea e Dello Stile di Vita di Una Popolazione Scolastica fra gli i 18 Anni, 11th Edn. Roma: Casa Editrice Scolastica Lombardi.
Shields, M., and Tremblay, M. S. (2010). Canadian childhood obesity estimates based on WHO, IOTF and CDC cut-points. Int. J. Pediatr. Obes. 5, 265–273. doi: 10.3109/17477160903268282
TANITA. (2016). Tanita Digital Scales for Body Fat & Weight: Body Composition Analyzer BC-418 Instruction Manual. Tokyo: TANITA.
Wang, Y., and Wang, J. Q. (2002). A comparison of international references for the assessment of child and adolescent overweight and obesity in different populations. Eur. J. Clin. Nutr. 56, 973–982. doi: 10.1038/sj.ejcn.1601415
Wimmer, R. (2011). Sampling Error Calculator. Available at: http://www.rogerwimmer.com/mmr/mmrsampling_error.htm
World Health Organization [WHO]. (2017). Obesity and Overweight. Available at: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Keywords: fat mass, BMI, nutritional status, WHO, IOTF, CGF
Citation: López-Sánchez GF, Sgroi M, D’Ottavio S, Díaz-Suárez A, González-Víllora S, Veronese N and Smith L (2019) Body Composition in Children and Adolescents Residing in Southern Europe: Prevalence of Overweight and Obesity According to Different International References. Front. Physiol. 10:130. doi: 10.3389/fphys.2019.00130
Received: 16 November 2018; Accepted: 01 February 2019;
Published: 19 February 2019.
Edited by:
Filipe Manuel Clemente, Polytechnic Institute of Viana do Castelo, PortugalReviewed by:
Ana Ruivo Alves, Polytechnic Institute of Beja, PortugalCopyright © 2019 López-Sánchez, Sgroi, D’Ottavio, Díaz-Suárez, González-Víllora, Veronese and Smith. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo Felipe López-Sánchez, Z2Zsc0B1bS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.