 Suraj Kukadia1
Suraj Kukadia1 Therese Tillin
Therese Tillin Alun D. Hughes
Alun D. Hughes
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Physiol., 04 February 2019
Sec. Vascular Physiology
Volume 10 - 2019 | https://doi.org/10.3389/fphys.2019.00047
Dietary inorganic nitrate in beetroot can act as a source of nitric oxide and has been reported to lower brachial blood pressure (BP). This study examined the effect of inorganic nitrate in beetroot juice on aortic (central) BP acutely and over the subsequent 24-h period. A double blind, randomized, placebo-controlled crossover trial was performed in fifteen healthy, normotensive men and women (age 22–40 years). Participants were randomized to receive beetroot juice containing nitrate (6.5–7.3 mmol) or placebo beetroot juice from which nitrate had been removed (<0.06 mmol nitrate). Effects on aortic systolic BP were measured at 30 min (primary endpoint), 60 min and over a subsequent 24 h period using an ambulatory BP monitor. Carotid-femoral pulse wave velocity (cfPWV) was also measured at 30 min. Following a washout period, the procedure was repeated within 7 days with crossover to the opposite arm of the trial. Compared with placebo, ingestion of beetroot juice containing nitrate lowered aortic systolic BP at 30 min by 5.2 (1.9–8.5) mmHg [mean (95% confidence interval); p < 0.01]. A smaller effect on aortic systolic BP was observed at 60 min. There were minimal effects on brachial BP or cfPWV. Effects on aortic systolic BP were not sustained over the subsequent 24 h and there were no effects on other hemodynamic parameters during ambulatory monitoring. A single dose of beetroot juice containing nitrate lowers aortic BP more effectively than brachial BP in the short term, but the effects are comparatively short-lived and do not persist over the course of the same day.
High blood pressure (BP) affects up to a billion people worldwide and is an important risk factor for cardiovascular disease even at levels below those traditionally classified as hypertensive (Forouzanfar et al., 2017). In older people high BP is largely attributable to elevated systolic BP secondary to increased arterial stiffness (Franklin et al., 1997).
Dietary measures offer potential as large-scale, cost-effective, and low-risk interventions that may offer a population-based strategy to complement drug-based therapy targeted at high risk individuals. Beetroot is a rich source of dietary inorganic nitrate (Lidder and Webb, 2013). Inorganic nitrate is absorbed in the proximal small intestine and, via the enterosalivary circulation, can act as a source of nitrite anions and nitric oxide (Lidder and Webb, 2013). Nitric oxide, which is endogenously produced by endothelial cells, is a vasodilator with a range of vasoprotective functions (Moncada and Higgs, 1993). Tissue and blood nitrite, derived either from oxidation of nitric oxide or dietary sources of nitrite/nitrate, serves as a reservoir from which nitric oxide can be produced through acidification or via proteins, including hemoglobin, that possess nitrite-reductase activity (Shiva, 2013). This mechanism contributes to skeletal muscle vasodilation in response to hypoxia (Dinenno, 2016) and nitrite supplementation reduces the BP response to the metaboreflex in skeletal muscle in older adults (Schneider et al., 2018). Inorganic nitrite supplementation has also been reported to improve endothelial dysfunction and decrease arterial stiffness in aged mice (Sindler et al., 2011) and older humans with moderately elevated cardiovascular risk (Rammos et al., 2014).
Previous studies have examined short-term effects of beetroot juice on brachial BP (Larsen et al., 2006; Webb et al., 2008; Kapil et al., 2010, 2015; Gilchrist et al., 2011; Hobbs et al., 2012), but little is known about its effect on aortic (central) BP. Aortic BP has been shown to better predict incident cardiovascular disease than brachial BP (Vlachopoulos et al., 2010) and is more closely associated with vascular and cardiac target organ damage (Kollias et al., 2016). Organic nitrates, while differing in some respects from inorganic nitrite/nitrate, also act via production of nitric oxide (Omar et al., 2012) and reduce aortic more than brachial BP (Jiang et al., 2002). Whether dietary inorganic nitrate has similarly more marked effects on aortic pressure has not been studies. It is also established that ambulatory BP measured over 24 h is a better predictor of cardiovascular risk and total mortality than clinic measurements of BP (Banegas et al., 2018), and recently it has become possible to measure aortic BP over 24 h (Weiss et al., 2012).
We therefore hypothesized that dietary nitrate in beetroot juice would reduce aortic BP acutely after administration. We also aimed to examine its effect on aortic blood pressure over a 24-h period, arterial stiffness and other measures of vascular function, and to compare its effect on aortic and brachial systolic BP.
Fifteen healthy volunteers (eleven female and four male) consisting of medical students and members of staff of Imperial College London were recruited. Healthy participants aged over 18 years with no existing co-morbidities, including hypertension, or on any medication (other than oral contraceptive pill), were eligible for the study. Studies were performed at the International Centre for Circulatory Health, Imperial College London, United Kingdom. The study protocol was approved by the London-Fulham Research Ethics Committee, Charing Cross Hospital (Ref: 13/LO/0063). All participants gave written informed consent in accordance with the principles of the Declaration of Helsinki.
This study was designed as a double-blind, randomized, placebo-controlled crossover trial (Figure 1), all observers were blinded to allocation status and participants were randomized using a computer program. All individuals were required to abstain from drinking caffeine-containing beverages alcohol and smoking for 12 h prior to study days and during the study. During the 24-h period following ingestion of the study drinks, no other dietary restrictions were imposed except that participants were asked not to consume any food or drink containing beetroot. A “washout” period of at least 24 h and less than 7 days was chosen on the basis of the duration of action of beetroot seen in other studies (Cosby et al., 2003; Coles and Clifton, 2012). Ingestion of study drinks was performed at the same time of day.
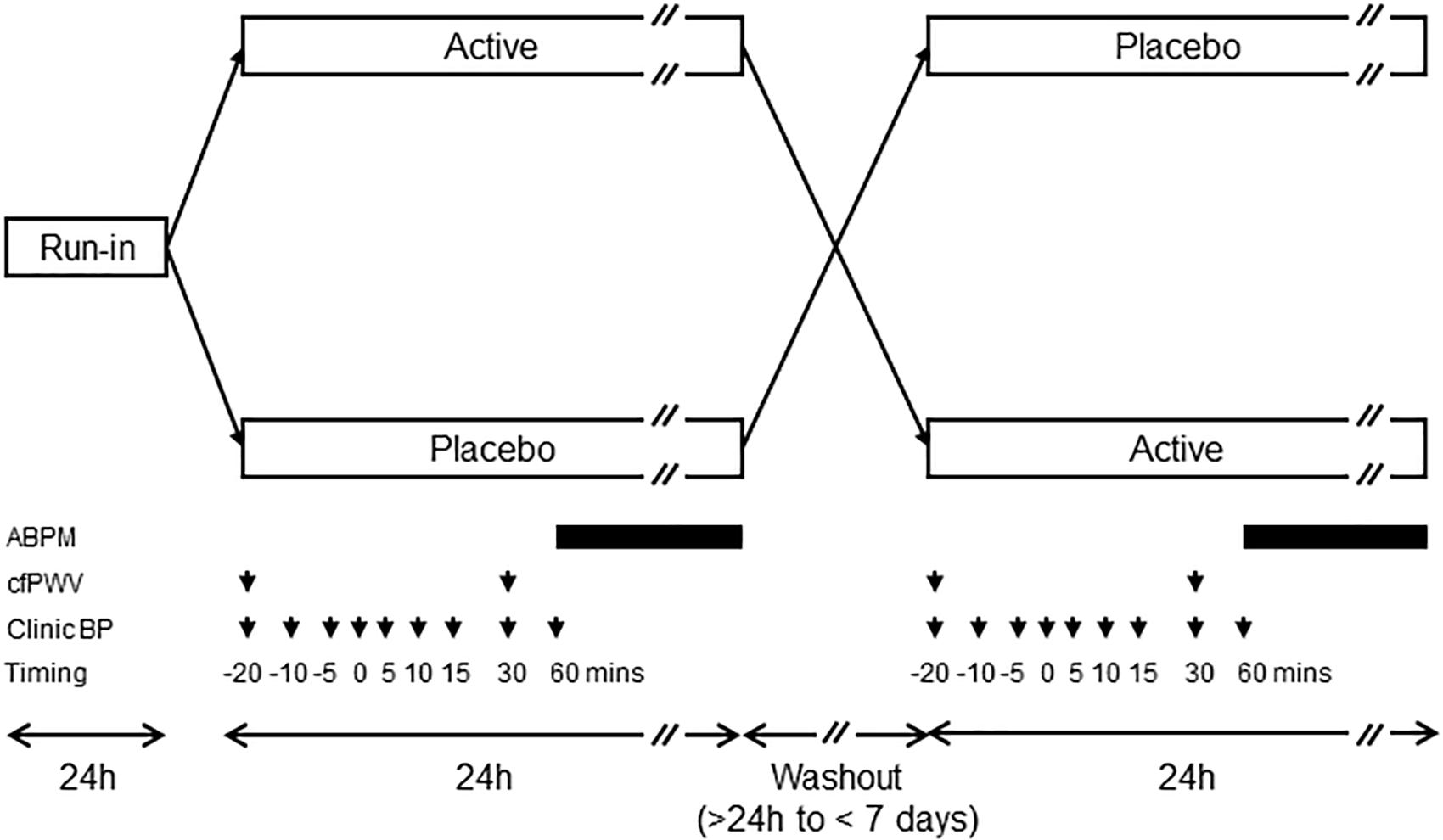
Figure 1. Diagram showing crossover design. Timings of measurements of clinic blood pressure (BP), carotid-femoral pulse wave velocity (cfPWV), and ambulatory blood pressure monitoring (ABPM) with respect to administration of placebo or active juice (time = 0) are indicated by the arrows and bars, respectively. ABPM was performed every 30 min during the day and hourly during the night.
The active intervention containing dietary nitrate was administered as a 70 ml concentrated beetroot juice drink (Beet It Sport Stamina, Beet It Beetroot Products Company) which contained 6.5–7.3 mmol nitrate. “Nitrate-free” beetroot juice (containing <0.06 mmol nitrate) from the same company which was identical in appearance acted as placebo.
A questionnaire was administered to collect information on lifestyle, and personal and family medical history. Height was measured using a stadiometer and weight was measured using a Soehnle electronic scale.
Sitting clinic BP (aortic and brachial) and heart rate were measured using a Pulsecor device (Pulsecor, Auckland, New Zealand) (Park et al., 2014). Measurements of BP were made at 20, 10, and 5 min and immediately prior to ingestion of the active of placebo drink. Subsequent measurements of BP were made at 5, 10, 15, 30, and 60 min after ingestion. After the final Pulsecor measurement at 60 min, a 24 h BP monitoring device (Mobil-O-Graph®), which measures both aortic and brachial BP (Weiss et al., 2012), was fitted to the participant’s non-dominant arm. The Mobil-O-Graph® recorded BP at 30-min intervals throughout the day, and at hourly intervals during the night.
Carotid-femoral pulse wave velocity (cfPWV) was measured using a Vicorder device (Skidmore Medical Limited, Bristol, United Kingdom) applied to the neck and right thigh of all subjects according to current guidelines (Van Bortel et al., 2012). cfPWV was measured approximately 20 min before and 30 min after ingestion of active or placebo drink. An indirect estimate of aortic pulse wave velocity (iPWV) during 24 h BP measurement was also obtained from the Mobil-O-Graph® as previously described (Luzardo et al., 2012).
The sample size was chosen to detect a 4 mmHg treatment difference in the primary endpoint, aortic systolic BP (alpha = 0.05; 80% power) assuming a standard deviation (SD) of 5 mmHg.
Statistical analysis and randomization was performed using R 3.0.2. Sample characteristics are presented as mean ± SD for normally distributed data or median (25th, 75th centiles) for skewed data, or n (%) for categorical data. Results are presented as the treatment effect (95% confidence interval). Data were analyzed by means of linear mixed models with random intercepts and common slopes to study the treatment effect, adjusting for baseline measures immediately prior to ingestion. The assessment of period effects and interactions between period and treatment was done within the models by including a covariate for the period in which the treatment was given, and a covariate representing the interaction between the period and the treatment. When no evidence of period effects or interactions between period and treatment was found, these covariates were excluded using an analysis of deviance, which led to a final, more parsimonious, model. Model assumptions were verified by analyzing residuals plots, and robust linear mixed models were used when assumptions were violated. All statistical tests were two-sided and statistical significance for the primary endpoint was set at p < 0.05.
Participant characteristics are shown in Table 1; volunteers were predominantly young females, only two individuals smoked, body mass index was in the healthy range and alcohol intake was moderate.
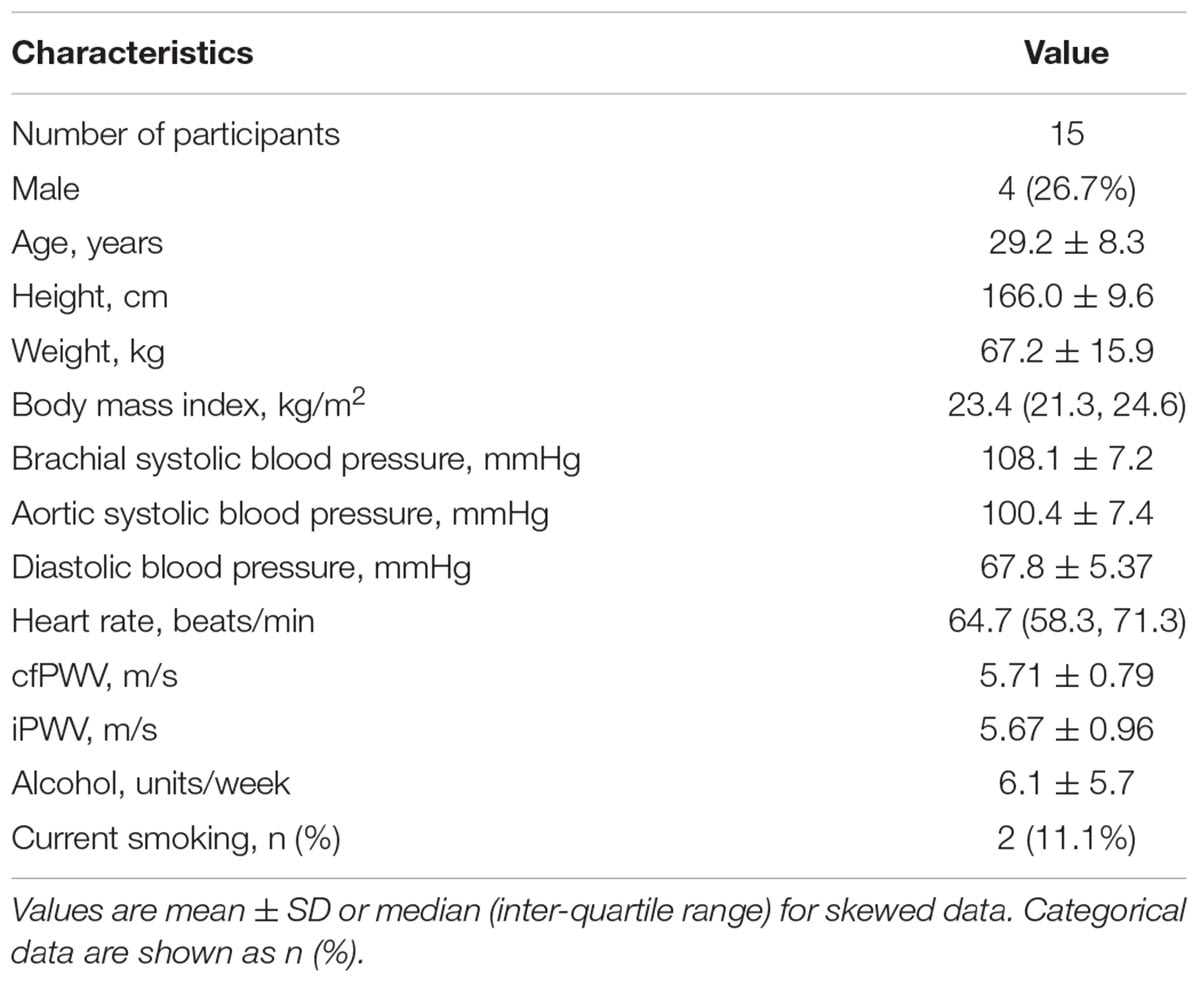
Table 1. Participant characteristics at recruitment, pre-intervention.
Ingestion of beetroot juice containing nitrate resulted in a lower aortic systolic BP at 30 min (primary endpoint) compared with placebo [difference (Δ) = -5.2 (-8.2, -2.2) mmHg; p < 0.01; Table 2]. Aortic systolic BP remained lower at 60 min after beetroot juice ingestion, although the difference was smaller [-3.2 (-6.6, 0.2) mmHg; Table 2].
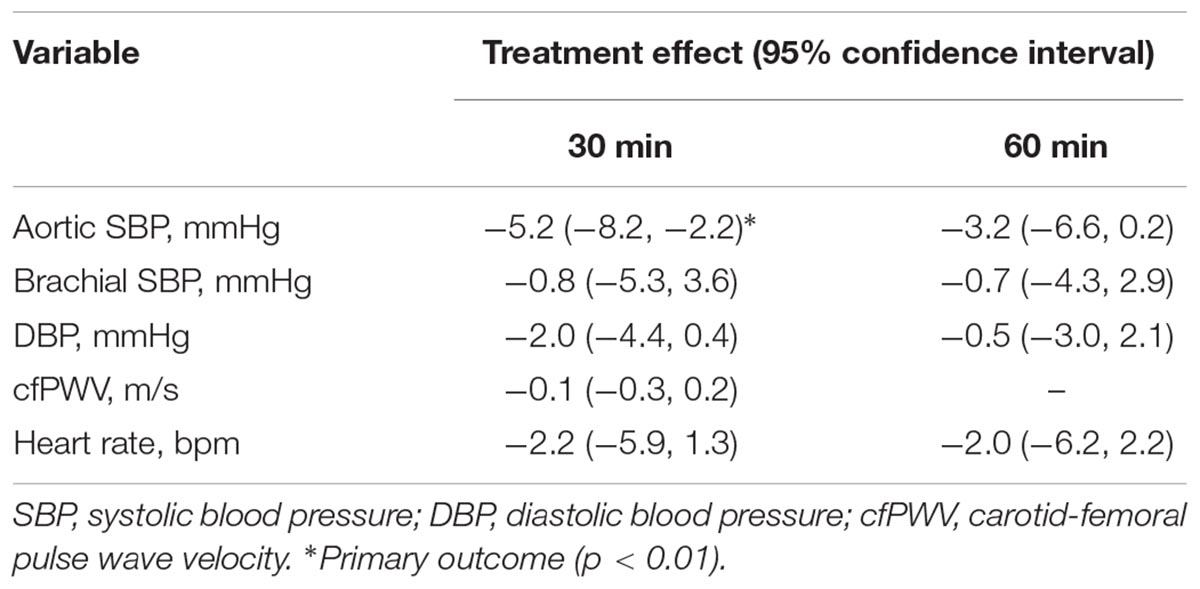
Table 2. Treatment effects and 95% confidence intervals of clinic measurements 30 and 60 min post-ingestion of beetroot juice compared to placebo.
In contrast brachial systolic BP did not differ noticeably between active and placebo groups at 30 or 60 min post-ingestion, BP in the active group was slightly lower [-0.8 (-5.3, 3.6)/-2.0 (-4.4, 0.4) mmHg; Table 2] but the confidence intervals of both brachial systolic and diastolic BP included zero.
There was no evidence of either a period effect or a treatment x period interaction for either aortic or brachial systolic pressure. Effects on heart rate and cfPWV are shown in Table 2. None of these measurements differed between active and placebo drink at 30 or 60 min post-ingestion.
Average 24-h aortic systolic BP was -0.9 (-2.5, 0.7) mmHg (lower) after beetroot juice ingestion than after placebo but the 95% confidence interval included zero. Differences between treatments were small and confidence intervals included zero for all other ambulatory BP variables, including iPWV (Table 3). Supplementary Figures S1–S6 show the ambulatory measurements over the 24-h period, for active treatment and placebo.
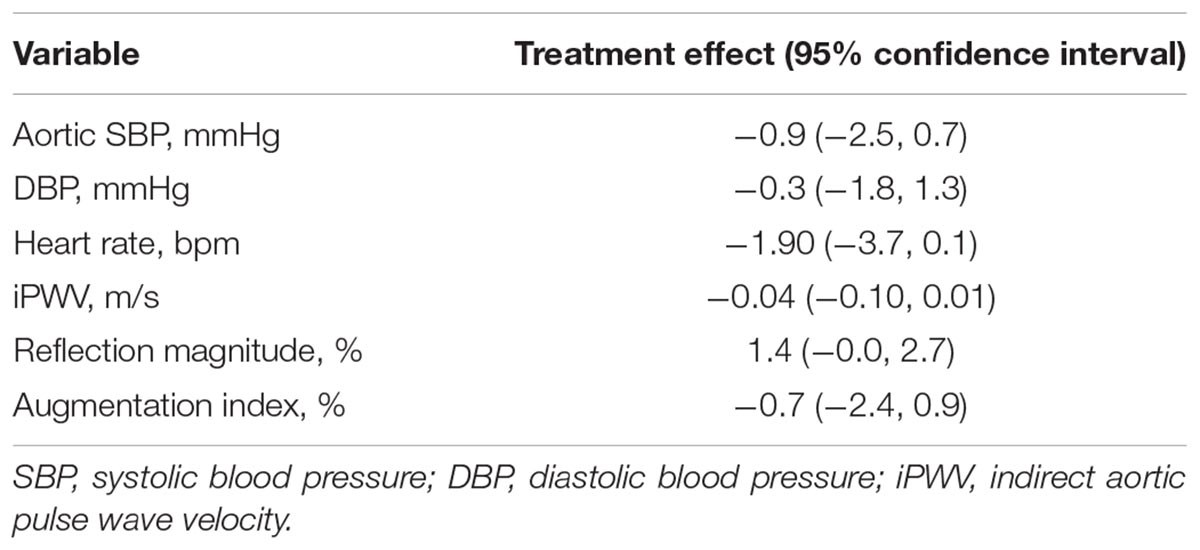
Table 3. Treatment effects and 95% confidence intervals of 24 h ambulatory measurements after beetroot juice ingestion compared to placebo.
There were no major adverse events. All participants were asked if they experienced any headaches, flushing or light-headedness; one participant complained of headache after consuming beetroot juice containing nitrate (active). This headache lasted for approximately 10 min. No other symptoms were reported by any of the participants.
This randomized, double blind, placebo-controlled crossover study has demonstrated that beetroot juice containing ∼7 mmol inorganic nitrate lowers aortic systolic BP by ∼5 mmHg compared with placebo, with the peak effect occurring approximately 30 min after ingestion. The effect of beetroot juice containing inorganic nitrate was more marked on aortic than brachial systolic BP and there was little or no effect of ingestion of inorganic nitrate on subsequent 24-h aortic BP.
Previous studies have examined the effect of dietary nitrate on brachial BP. Kapil et al. (2010) found that, compared with water, beetroot juice containing 5.5 mmol nitrate caused a peak reduction in brachial systolic BP of ∼5 mmHg at 3 h with no change in diastolic BP. It is possible that differences in drink composition or participant characteristics contributed to the greater effect on brachial BP seen in their study. For example, participants in their study typically had brachial systolic BP of ∼120 mmHg compared with 110 mmHg in our study and the effect of hypotensive agents tends to be greater with higher baseline BP (Messerli et al., 2015). Also, ingestion of water has been reported to increase brachial BP (Jordan et al., 2000), probably through a mechanism involving the sympathetic nervous system and elicited by hypo-osmolarity (May and Jordan, 2011); while this effect appears small in young individuals (Jordan et al., 2000) it may mean that water is an unsuitable control for beetroot juice. In another study, Coles and Clifton compared a beetroot and apple drink (∼7.5 mmol nitrate) with apple juice on 24-h systolic or diastolic BP, and found no significant effect, although they reported a non-significant ∼4 mmHg difference between active and placebo group 6 h after consumption (Coles and Clifton, 2012). We found minimal effects of nitrate-containing beetroot juice on brachial systolic BP, so our data suggest that measurement of brachial BP as opposed to aortic BP is likely to have underestimated the effect of inorganic nitrate in some previous studies. Siervo et al. (2013) conducted a meta-analysis and systematic review of 12 studies using beetroot juice supplementation and demonstrated a change in brachial systolic BP of -4.5 mmHg (95% CI: -6.4, -2.5; p < 0.001) with nitrate doses ranging from 5.1 to 45 mmol. In the meta-regression these researchers carried out, the mean differences in systolic BP were not correlated with study duration. In keeping with our findings, ambulatory BP was not lowered by beetroot juice in the two studies of normotensive individuals included in the systematic review (Coles and Clifton, 2012; Hobbs et al., 2012).
Our study has strengths and limitations. A randomized double-blind placebo control study is a robust design; the sample size is small but adequate to detect a clinically important reduction in BP. Many previous studies have not been blinded as low-nitrate water or isomolar potassium and sodium chloride solutions have been used as the placebo (Larsen et al., 2006; Webb et al., 2008; Kapil et al., 2010; Larsen et al., 2010; Bahra et al., 2012; Hobbs et al., 2012). Our data are limited in that they were conducted in young healthy individuals receiving a single dose of beetroot juice and may not generalize to older people with or without high BP, or to other dosing regimens or durations of administration. Additionally, our study only considered the hypotensive effect of inorganic nitrate in beetroot juice. A recent meta-analysis (Bahadoran et al., 2017) has provided evidence that beetroot juice may contain factors other than nitrate that lower BP; given the design of our study it is not possible to conclude anything about the effect of other factors in beetroot juice on BP.
It has been suggested that beetroot juice may have value as a population-based intervention to lower BP, although our data showing an apparently short duration of BP lowering raise questions regarding its usefulness in younger normotensive individuals. Nevertheless, even small reductions in BP could lead to a large reduction in incident cardiovascular disease on a population level (Strachan and Rose, 1991). Dietary approaches to BP reduction could be useful in the face of the rising incidences of both obesity and diabetes. It remains to be established whether dietary supplementation with beetroot juice or other nitrate-rich vegetables, extracts or juices, is an effective, safe and acceptable method of population-scale BP reduction.
In conclusion, nitrate-contained in beetroot juice lowered aortic systolic BP in normotensive individuals 30 min post-ingestion with minimal effects on brachial BP. This effect was of comparatively short duration and did not persist over 24-h. Previous studies only measuring brachial BP and not aortic BP may have underestimated the effects of inorganic nitrates on BP.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
AH and NC conceived and designed the study. SK and EC collected the data. SK, EC, and TT performed the analysis of the data. H-MD and TT undertook the statistical analysis. SK and AH wrote the paper with critical revisions from all authors. All authors provided approval for publication of the content and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AH receives support from the British Heart Foundation (PG/15/75/31748, CS/15/6/31468, and CS/13/1/30327). AH and NC receive support from the National Institutes of Health Research University College London Hospitals Biomedical Research Centre, and work in a unit that receives support from the UK Medical Research Council (Programme Code MC_UU_12019/1).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We are extremely grateful to all the people who took part in the study, and past and present members of the SABRE team who helped to recruit participants. We thank Daniel Key for his assistance with data management.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2019.00047/full#supplementary-material
Bahadoran, Z., Mirmiran, P., Kabir, A., Azizi, F., and Ghasemi, A. (2017). The nitrate-independent blood pressure-lowering effect of beetroot juice: a systematic review and meta-analysis. Adv. Nutr. 8, 830–838. doi: 10.3945/an.117.016717
Bahra, M., Kapil, V., Pearl, V., Ghosh, S., and Ahluwalia, A. (2012). Inorganic nitrate ingestion improves vascular compliance but does not alter flow-mediated dilatation in healthy volunteers. Nitric Oxide 26, 197–202. doi: 10.1016/j.niox.2012.01.004
Banegas, J. R., Ruilope, L. M., De La Sierra, A., Vinyoles, E., Gorostidi, M., De La Cruz, J. J., et al. (2018). Relationship between clinic and ambulatory blood-pressure measurements and mortality. N. Engl. J. Med. 378, 1509–1520. doi: 10.1056/NEJMoa1712231
Coles, L. T., and Clifton, P. M. (2012). Effect of beetroot juice on lowering blood pressure in free-living, disease-free adults: a randomized, placebo-controlled trial. Nutr. J. 11:106. doi: 10.1186/1475-2891-11-106
Cosby, K., Partovi, K. S., Crawford, J. H., Patel, R. P., Reiter, C. D., Martyr, S., et al. (2003). Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat. Med. 9, 1498–1505. doi: 10.1038/nm954
Dinenno, F. A. (2016). Skeletal muscle vasodilation during systemic hypoxia in humans. J. Appl. Physiol. 120, 216–225. doi: 10.1152/japplphysiol.00256.2015
Forouzanfar, M. H., Liu, P., Roth, G. A., Ng, M., Biryukov, S., Marczak, L., et al. (2017). Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990-2015. JAMA 317, 165–182. doi: 10.1001/jama.2016.19043
Franklin, S. S., Gustin, W. T., Wong, N. D., Larson, M. G., Weber, M. A., Kannel, W. B., et al. (1997). Hemodynamic patterns of age-related changes in blood pressure. The framingham heart study. Circulation 96, 308–315. doi: 10.1161/01.CIR.96.1.308
Gilchrist, M., Shore, A. C., and Benjamin, N. (2011). Inorganic nitrate and nitrite and control of blood pressure. Cardiovasc. Res. 89, 492–498. doi: 10.1093/cvr/cvq309
Hobbs, D. A., Kaffa, N., George, T. W., Methven, L., and Lovegrove, J. A. (2012). Blood pressure-lowering effects of beetroot juice and novel beetroot-enriched bread products in normotensive male subjects. Br. J. Nutr. 108, 2066–2074. doi: 10.1017/S0007114512000190
Jiang, X. J., O’rourke, M. F., Jin, W. Q., Liu, L. S., Li, C. W., Tai, P. C., et al. (2002). Quantification of glyceryl trinitrate effect through analysis of the synthesised ascending aortic pressure waveform. Heart 88, 143–148. doi: 10.1136/heart.88.2.143
Jordan, J., Shannon, J. R., Black, B. K., Ali, Y., Farley, M., Costa, F., et al. (2000). The pressor response to water drinking in humans: a sympathetic reflex? Circulation 101, 504–509.
Kapil, V., Khambata, R. S., Robertson, A., Caulfield, M. J., and Ahluwalia, A. (2015). Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: a randomized, phase 2, double-blind, placebo-controlled study. Hypertension 65, 320–327. doi: 10.1161/HYPERTENSIONAHA.114.04675
Kapil, V., Milsom, A. B., Okorie, M., Maleki-Toyserkani, S., Akram, F., Rehman, F., et al. (2010). Inorganic nitrate supplementation lowers blood pressure in humans: role for nitrite-derived no. Hypertension 56, 274–281. doi: 10.1161/HYPERTENSIONAHA.110.153536
Kollias, A., Lagou, S., Zeniodi, M. E., Boubouchairopoulou, N., and Stergiou, G. S. (2016). Association of central versus brachial blood pressure with target-organ damage: systematic review and meta-analysis. Hypertension 67, 183–190. doi: 10.1161/HYPERTENSIONAHA.115.06066
Larsen, F. J., Ekblom, B., Sahlin, K., Lundberg, J. O., and Weitzberg, E. (2006). Effects of dietary nitrate on blood pressure in healthy volunteers. N. Engl. J. Med. 355, 2792–2793. doi: 10.1056/NEJMc062800
Larsen, F. J., Weitzberg, E., Lundberg, J. O., and Ekblom, B. (2010). Dietary nitrate reduces maximal oxygen consumption while maintaining work performance in maximal exercise. Free Radic. Biol. Med. 48, 342–347. doi: 10.1016/j.freeradbiomed.2009.11.006
Lidder, S., and Webb, A. J. (2013). Vascular effects of dietary nitrate (as found in green leafy vegetables and beetroot) via the nitrate-nitrite-nitric oxide pathway. Br. J. Clin. Pharmacol. 75, 677–696. doi: 10.1111/j.1365-2125.2012.04420.x
Luzardo, L., Lujambio, I., Sottolano, M., Da Rosa, A., Thijs, L., Noboa, O., et al. (2012). 24-h ambulatory recording of aortic pulse wave velocity and central systolic augmentation: a feasibility study. Hypertens. Res. 35, 980–987. doi: 10.1038/hr.2012.78
May, M., and Jordan, J. (2011). The osmopressor response to water drinking. Am. J. Physiol. Regul. Integr. Comp. Physiol. 300, R40–R46. doi: 10.1152/ajpregu.00544.2010
Messerli, F. H., Bangalore, S., and Schmieder, R. E. (2015). Wilder’s principle: pre-treatment value determines post-treatment response. Eur Heart J 36, 576–579. doi: 10.1093/eurheartj/ehu467
Moncada, S., and Higgs, A. (1993). The L-arginine-nitric oxide pathway. N. Engl. J. Med. 329, 2002–2012. doi: 10.1056/NEJM199312303292706
Omar, S. A., Artime, E., and Webb, A. J. (2012). A comparison of organic and inorganic nitrates/nitrites. Nitric Oxide 26, 229–240. doi: 10.1016/j.niox.2012.03.008
Park, C. M., Korolkova, O., Davies, J. E., Parker, K. H., Siggers, J. H., March, K., et al. (2014). Arterial pressure: agreement between a brachial cuff-based device and radial tonometry. J. Hypertens. 32, 865–872. doi: 10.1097/HJH.0000000000000082
Rammos, C., Hendgen-Cotta, U. B., Sobierajski, J., Bernard, A., Kelm, M., and Rassaf, T. (2014). Dietary nitrate reverses vascular dysfunction in older adults with moderately increased cardiovascular risk. J. Am. Coll. Cardiol. 63, 1584–1585. doi: 10.1016/j.jacc.2013.08.691
Schneider, A. C., Hughes, W. E., Ueda, K., Bock, J. M., and Casey, D. P. (2018). Reduced blood pressure responsiveness to skeletal muscle metaboreflex activation in older adults following inorganic nitrate supplementation. Nitric Oxide 78, 81–88. doi: 10.1016/j.niox.2018.05.010
Shiva, S. (2013). Nitrite: a physiological store of nitric oxide and modulator of mitochondrial function. Redox Biol. 1, 40–44. doi: 10.1016/j.redox.2012.11.005
Siervo, M., Lara, J., Ogbonmwan, I., and Mathers, J. C. (2013). Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: a systematic review and meta-analysis. J. Nutr. 143, 818–826. doi: 10.3945/jn.112.170233
Sindler, A. L., Fleenor, B. S., Calvert, J. W., Marshall, K. D., Zigler, M. L., Lefer, D. J., et al. (2011). Nitrite supplementation reverses vascular endothelial dysfunction and large elastic artery stiffness with aging. Aging Cell 10, 429–437. doi: 10.1111/j.1474-9726.2011.00679.x
Strachan, D., and Rose, G. (1991). Strategies of prevention revisited: effects of imprecise measurement of risk factors on the evaluation of “high-risk” and “population-based” approaches to prevention of cardiovascular disease. J. Clin. Epidemiol. 44, 1187–1196. doi: 10.1016/0895-4356(91)90151-X
Van Bortel, L. M., Laurent, S., Boutouyrie, P., Chowienczyk, P., Cruickshank, J. K., De Backer, T., et al. (2012). Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 30, 445–448. doi: 10.1097/HJH.0b013e32834fa8b0
Vlachopoulos, C., Aznaouridis, K., O’rourke, M. F., Safar, M. E., Baou, K., and Stefanadis, C. (2010). Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur. Heart J. 31, 1865–1871. doi: 10.1093/eurheartj/ehq024
Webb, A. J., Patel, N., Loukogeorgakis, S., Okorie, M., Aboud, Z., Misra, S., et al. (2008). Acute blood pressure lowering, vasoprotective, and antiplatelet properties of dietary nitrate via bioconversion to nitrite. Hypertension 51, 784–790. doi: 10.1161/HYPERTENSIONAHA.107.103523
Keywords: beetroot, inorganic nitrate, blood pressure, pulse wave velocity, double-blind, randomized, placebo-controlled crossover study
Citation: Kukadia S, Dehbi H-M, Tillin T, Coady E, Chaturvedi N and Hughes AD (2019) A Double-Blind Placebo-Controlled Crossover Study of the Effect of Beetroot Juice Containing Dietary Nitrate on Aortic and Brachial Blood Pressure Over 24 h. Front. Physiol. 10:47. doi: 10.3389/fphys.2019.00047
Received: 14 October 2018; Accepted: 17 January 2019;
Published: 04 February 2019.
Edited by:
Andrew P. Braun, University of Calgary, CanadaReviewed by:
Ulf Simonsen, Aarhus University, DenmarkCopyright © 2019 Kukadia, Dehbi, Tillin, Coady, Chaturvedi and Hughes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alun D. Hughes, YWx1bi5odWdoZXNAdWNsLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.