
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Physiol. , 06 October 2016
Sec. Integrative Physiology
Volume 7 - 2016 | https://doi.org/10.3389/fphys.2016.00448
This article is part of the Research Topic Celebrating Twenty Years of the Brazilian Symposium on Cardiovascular Physiology View all 23 articles
 José L. de Brito Alves1,2*
José L. de Brito Alves1,2* Vanessa P. de Sousa1Marinaldo P. Cavalcanti Neto3
Vanessa P. de Sousa1Marinaldo P. Cavalcanti Neto3 Marciane Magnani4
Marciane Magnani4 Valdir de Andrade Braga5João H. da Costa-Silva6
Valdir de Andrade Braga5João H. da Costa-Silva6 Carol G. Leandro6Hubert Vidal2
Carol G. Leandro6Hubert Vidal2 Luciano Pirola2
Luciano Pirola2Arterial hypertension (AH) is one of the most prevalent risk factors for cardiovascular diseases (CD) and is the main cause of deaths worldwide. Current research establish that dietary polyphenols may help to lower blood pressure (BP), thus contributing to the reduction of cardiovascular complications. In addition, the health benefits of probiotics on BP have also attracted increased attention, as probiotics administration modulates the microbiota, which, by interacting with ingested polyphenols, controls their bioavalability. The aim of the present mini-review is to summarize and clarify the effects of dietary polyphenols and probiotics administration on BP using combined evidence from clinical and experimental studies, as well as to discuss the current debate in the literature about the usefulness of this nutritional approach to manage BP. Clinical trials and experimental studies have demonstrated that consuming dietary polyphenols or probiotics in adequate amounts may improve BP, ranging from modest to greater effects. However, the mechanisms linking probiotic intake and reduced BP levels need to be further elucidated as a definitive consensus on the link between intake of polyphenols or probiotics and improvement of AH has not been reached yet.
Arterial hypertension (AH) affects more than 1 billion people and is the major risk factor for CD (Hedner et al., 2012). The cause of AH has been difficult to identify due to its multi-factorial nature, which involves genetic and environmental factors. A balanced and healthy diet plays a key role in the maintenance of the cardiovascular health status, which is a major determinant of lifespan. In the last decades, in both western and developing countries, the consumption of highly caloric—rich in fat and carbohydrates—and sodium-rich diets have become predominant, increasing the incidence of AH (Bjerregaard, 2010; Popkin, 2011).
The regulation of BP is one of the most complex physiological functions and depends on the integrated actions of cardiovascular, renal, neural and endocrine systems (Corry and Tuck, 1999; de Brito Alves et al., 2015). In addition, augmentation of proinflammatory markers, reactive oxygen species and dysfunction in energy metabolism are related to hypertensive conditions (Carthy, 2014).
Despite the advances in the understanding of the pathophysiology and pharmacotherapy of AH, interventional strategies helping to reduce BP levels remain one of the great problems to be developed. Studies have investigated the beneficial effect of dietary changes on BP levels and also identified a BP-lowering activity on different dietary compounds.
The intestine and its microbiota constitute an important site of interaction with the dietary compounds (Bäckhed et al., 2004), and in particular polyphenols, whose bioavailability is dependent on prior metabolization by the microbiota (Ozdal et al., 2016; Stevens and Maier, 2016). The interaction between gut microbiota and diet can affect the gut-immune homeostasis, cell proliferation, metabolism, and intestinal permeability (Ding et al., 2010). Growing evidence supports the notion that the gut microbiota plays an important role in the development of CD and AH (Khalesi et al., 2014; Jose and Raj, 2015), and dietary compounds might modulate the gut microbiota favoring or lowering the BP (Buettner et al., 2007; Anhê et al., 2015).
Accordingly, findings have suggested the notion that dietary polyphenols and probiotic supplementation could help alleviating AH, by altering the gut microbiota and favoring an antioxidant activity (Anhê et al., 2015; Gómez-Guzmán et al., 2015; Grosso et al., 2016), although null and contrary findings have also been reported (Ras et al., 2013). In the present mini-review, we summarize the current understanding emerging from experimental, clinical and epidemiological studies, on how dietary polyphenols and probiotics intake may help to lower BP in hypertensive conditions.
Polyphenols are a large and heterogeneous family of bioactive molecules found in numerous food sources. Generally defined as dietary antioxidants, polyphenols have been established as bioactive compounds that benefit human health via modulation of metabolism (Choi et al., 2014). Dietary polyphenols are mainly classified in catechins (proanthocyanidins), flavonols, flavanones, ellagitannins, and isoflavones. Studies have investigated the effects of dietary polyphenols, or their metabolites supplementation either via administration as polyphenol-enriched diets, polyphenol extracts from foods or as administration of specific polyphenolic compounds (e.g., quercetin, rutin, resveratrol, hesperidin, cinnamon) (Mendes-Junior et al., 2013; Amiot et al., 2016).
Dietary polyphenols have been shown to exert beneficial effects on markers for cardiovascular risk factors, including reduction of BP, improvement of endothelial function and lowering of plasma lipids. Mechanistically, it has been suggested that dietary polyphenols can alleviate hypertension through anti-inflammatory and anti-oxidant effects, and increased oxide nitric (NO) production (Davinelli and Scapagnini, 2016). The anti-inflammatory effect is associated with a reduced expression of the redox-sensitive nuclear factor-kB (NF-κB), while that the anti-oxidant effect of polyphenols is related to improved enzymatic activities of superoxide dismutase, catalase and glutathione peroxidase. In addition, polyphenols participate in the activation of the redox-sensitive phosphoinositide 3 (PI3)-kinase/Akt pathway, leading to increased formation of NO (Davinelli and Scapagnini, 2016). Taken together, all these pathways help to reduce blood pressure in hypertensive conditions.
Other studies have, however, reached negative or null effects. These effects have been investigated in several cohorts and randomized clinical trials (Table 1).
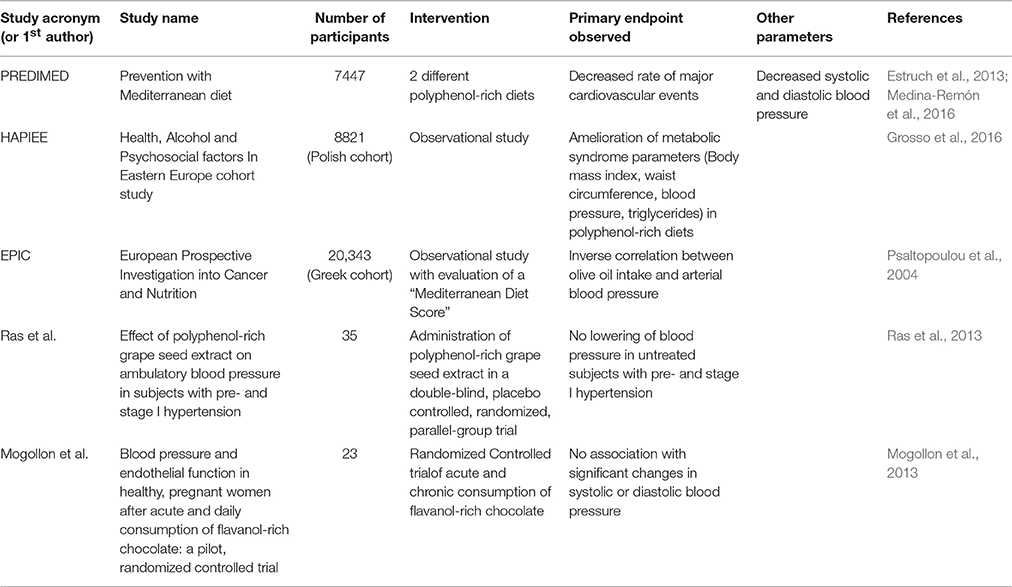
Table 1. Summary of the major studies investigating the relationship between dietary polyphenols intake and blood pressure/cardiovascular health.
In a small-scale randomized nutritional trial, the administration of a polyphenol-rich diet (approximately 3000 mg polyphenol/day) reduced postprandial triglyceride-rich lipoprotein plasma concentrations and oxidative stress in study participants with a high risk of CD (Annuzzi et al., 2014).
The beneficial effects of polyphenol supplementation have also been demonstrated in the larger PREDIMED (Prevention with Mediterranean Diet) cohort. In this study, the consumption of a Mediterranean diet—supplemented with extra-virgin olive oil or nuts—resulted in reduced incidence of cardiovascular events (myocardial infarction, stroke, or death from cardiovascular causes) (Estruch et al., 2013). Within the PREDIMED cohort, a sub-study on 1139 high-risk participants was performed in which two different polyphenol-rich diets (based on supplementation with extra-virgin olive oil or nuts) were randomly assigned. The increase in polyphenol intake—which was unequivocally identified as increased total urinary polyphenol excretion—was associated with decreased inflammatory biomarkers and a decrease of systolic and diastolic BP (Medina-Remón et al., 2016).
In the Polish population of the non-interventional HAPIEE cohort (Health, Alcohol and Psychosocial factors In Eastern Europe), elevated dietary intake of polyphenols was associated with lower body mass index (BMI), waist circumference (WC), BP and triglycerides, further suggesting that high polyphenols intake is inversely associated to metabolic syndrome and its clinical manifestations (Grosso et al., 2016). To ascertain whether olive oil polyphenols alleviate AH independently from the lipid component of olive oil, which is rich in monounsaturated fatty acids (MUFA), a double-blind, crossover dietary-intervention study was performed in which mildly hypertensive women received polyphenol-rich olive oil (approximately 30 mg/day) in a first dietary period, and polyphenol-free olive oil in a second dietary period. Interestingly, only polyphenol-rich olive oil decreased BP and improved endothelial function, underscoring the specific role of polyphenols within the olive oil (Moreno-Luna et al., 2012). In addition, in a randomized, double blind, controlled, crossover trial, the hypotensive and lipid-lowering capacity have also been demonstrated for olive leaf extract (Lockyer et al., 2015, 2016).
Although the studies presented above indicate that administration of dietary polyphenols might contribute to the control of BP, a definitive consensus has not been reached yet, as independent investigations did not support the hypothesis that dietary intake of polyphenols is beneficial to cardiovascular health (Ras et al., 2013).
Resveratrol (3,5,4′-trihydroxy-trans-stilbene) is a stilbenoid. Studies demonstrated that resveratrol possess an intrinsic cancer chemopreventive activity (Jang et al., 1997), and further interest on this molecule arose with the identification of its capability to increase lifespan when administered to experimental organisms including Saccharomyces cerevisiae, Caenorhabditis elegans, Drosophila melanogaster (Ingram et al., 2006), and mice (Baur et al., 2006). Furthermore, it was soon documented in animal models that resveratrol (i) protects from the development of obesity-dependent metabolic disorders (Fröjdö et al., 2008) and (ii) can be the molecule responsible for the cardio-protective effects of red wine (Wu et al., 2011).
Preclinical studies have investigated the effects of resveratrol administration on cardiovascular health. In spontaneously hypertensive rats (SHR) and in mice rendered hypertensive by angiotensin-II injection, resveratrol administration reduced oxidative stress in the endothelium, improved vascular function and attenuated AH (Dolinsky et al., 2013). Resveratrol supplementation to SHR dams during the perinatal period (from gestation to weaning of the offspring) alleviated the development of AH in the offspring at the adult age (Care et al., 2016). These finding have prompted the development of several small-scale clinical trials evaluating the effects of resveratrol supplementation on cardiovascular systems.
In some trials, resveratrol supplementation (range 200–300 mg/day) improved insulin resistance, glycemic profile and lipid metabolism (Wong et al., 2011; Chen et al., 2015). However, in other studies, 12-week supplementation with 500 mg/day resveratrol (Faghihzadeh et al., 2015) or 150 mg/day for 4 weeks (van der Made et al., 2015) did not change metabolic risk markers related to cardiovascular dysfunction.
A recent meta-analysis of 10 randomized clinical trials failed to show any benefit of resveratrol supplementation on cardiovascular risk factors. In particular resveratrol had no effect on systolic or diastolic BP (Sahebkar et al., 2015). However, an independent meta-analysis performed on more stringent adjudication criteria for study quality, including only six studies comprising a total of 247 subjects, suggested that resveratrol consumption decreased systolic BP (at the higher administered doses) while having no significant effects on diastolic BP (Liu et al., 2015). Given the absence of a clear consensus on the effects on resveratrol on the control of BP in humans, as opposed to the clear conclusions in rodent models, the need for larger and well-designed clinical trials, was solicited by the authors of both meta-analysis to definitely prove, or reject, a causal link between resveratrol administration and the control of BP (Novelle et al., 2015).
Quercetin [2-(3,4-dihydroxyphenyl)-3,5,7-trihydroxy-4H-chromen-4-one] is a polyphenolic compound belonging to the class of flavonoids, which is naturally found in apples, berries, and red wine (Sigel et al., 1977). Epidemiological data and dietary analysis indicated that quercetin could contribute to decrease the risk of coronary heart disease in elderly patients (Hertog et al., 1993). To test the hypothesis that quercetin reduces BP in hypertensive patients, a randomized, double-blind, placebo-controlled, crossover study was performed to test the efficacy of quercetin supplementation (730 mg quercetin/day for 28 days) in pre-hypertensive and stage-1 hypertensive volunteers. Quercetin supplementation reduced systolic, diastolic and mean arterial pressure in stage-1 hypertensive volunteers, while having no effect on pre-hypertensive participants (Edwards et al., 2007). More recently, data obtained from hypertensive patients, also indicated that quercetin supplementation (162 mg/day for 6 weeks) exert cardio-protective effect, with a decrease of 24 h systolic BP of 3.6 mmHg (Brüll et al., 2015). On the other hand, a recent similar study in overweight-to-obese adults with AH did not detect changes in post-prandial BP, nor endothelial function, upon acute administration of quercetin (54 mg in a single dose) (Brüll et al., 2016). The effects of quercetin administration are likely dependent on the doses and administration time-span. A recent meta-analysis of randomized controlled trials investigating the effects of quercetin on BP support the idea that quercetin doses greater than 500 mg/day have a significant effect on the reduction of BP (Serban et al., 2016).
Hesperidin (30, 5, 9-dihydroxy-40-methoxy-7-orutinosyl flavanone) is an abundant flavonoid found in citrus fruit, particularly in the peel of oranges and lemon (Sharma et al., 2015). Reports suggest that hesperidin exerts a cardio-protective action via its antioxidant and antihypertensive properties (Wilmsen et al., 2005), as also demonstrated in an ischemic heart disease model in diabetic rats (Agrawal et al., 2014) and in SHR (Yamamoto et al., 2008; Ikemura et al., 2012). Over the last years, a large body of studies in cell culture and animal models has elucidated the molecular targets and mechanisms of action of hesperidin. Besides its cardio-protective actions, hesperidin has also shown anticancer, anti-inflammatory, and neuroprotective properties (Roohbakhsh et al., 2015). However, at present, clinical studies regarding the therapeutic effects of hesperidin have not appeared, and pre-clinical testing in humans is warranted to confirm the beneficial effects observed in animal models.
Recently it has been suggested that dietary polyphenols consumption could help maintain intestinal homeostasis and metabolic health. In light of recent discoveries, studies have shown that dietary polyphenols can exert part of their beneficial action through modulation of the microbiota (Anhê et al., 2016). For example, it was demonstrated that a polyphenol-rich cranberry extract prevented obesity and the metabolic syndrome in diet-induced obesity through prebiotic effect on the gut microbiota (Anhê et al., 2015). The investigation on whether dietary polypnehols attenuate BP through beneficial actions on gut microbiota is a newly developing field and the underlying mechanisms remain to be elucidated.
The term probiotic means “for life” and it was first used to describe compounds produced by protozoa to stimulate the growth of other organisms (Lilly and Stillwell, 1965). Currently, the term probiotics refers to nonpathogenic microorganisms (bacteria or yeast) that, when ingested, are capable to reach the gut in sufficient amounts to confer health benefits (Parvez et al., 2006). Historically, probiotics derived from dairy products were the first to be isolated and studied (Tapsell, 2015). However, in the last decades, potentially probiotic strains from vegetable sources have also been isolated and their health benefits investigated (Rivera-Espinoza and Gallardo-Navarro, 2010; Vitali et al., 2012). Probiotics can be ingested either as supplements or incorporated in food or beverages in the form of dairy or non-dairy probiotic products (Jankovic et al., 2010; Vijaya Kumar et al., 2015). Despite the differences among the quantities of probiotic intake recommended by American or European Agencies to confer generic health claims, probiotic intake of around 106–108 CFU/g−1 (or mL−1) or 108–1010 CFU/day (CFU, colony forming units) have shown to be efficacious (Champagne et al., 2011).
Saccharomyces boulardii is the main nonpathogenic yeast being used as probiotic. In addition, numerous bacteria belonging to the Enterococcus, Pediococcus, Bacillus, Streptococcus, Lactococcus and Propionibacterium genera are recognized as potential candidates for probiotic status. It is important to highlight that the Lactobacillus (L.) and Bifidobacterium (B.) genera constitute the majority of probiotics found on the market (Wohlgemuth et al., 2010; Champagne et al., 2011). Particularly, the lactic acid bacteria L. acidophilus, L. casei, L. paracasei, L. fermentum, L. reuteri, L. plantarum, L. rhamnosus and L. salivarius, as well as B. bifidum, B. breve, B. infantis, B. lactis, B. longum and B. thermophilum are among the main probiotics species marketed worldwide (Vijaya Kumar et al., 2015).
The benefits of the ingestion of probiotics by humans seem to be related to the improvement of the gut microbiota status, increase of enterocyte's resistance to pathogens, decrease or almost total elimination of pathogenic microorganisms within the intestinal tract, alleviation of nutritional intolerances (e.g., increased tolerance to lactose), enhancement of macro- and micro-nutrients bioavailability, and the reduction of the prevalence of allergies in susceptible individuals (Sharma and Devi, 2014).
Beneficial effects on intestinal permeability to macromolecules, including lipopolysaccharides and on gut inflammation are also considered as major mechanisms conferring health benefit to probiotics (Cani, 2014). A recent study in a germ-free mouse model has also shown that administration of probiotics belonging to the Lactobacillus genus may alleviate the negative effects of chronic under-nutrition on postnatal growth (Schwarzer et al., 2016).
Interestingly, experimental and clinical reports have demonstrated that improvement of the gut microbiota though probiotic supplementation might positively help in reducing BP in the hypertensive conditions (Ettinger et al., 2014; Jose and Raj, 2015; Mell et al., 2015).
Despite these findings, other reports has shown that the probiotic supplementation did not induce any significant alterations in BP, heart rate (HR) or cardiovascular risk markers, such as total cholesterol, low-density lipoprotein, pro-inflammatory markers (Barreto et al., 2014; Mahboobi et al., 2014; Ivey et al., 2015).
By using a hypertensive rat model treated with nitro-L-arginine methyl ester (L-NAME), it was demonstrated that the supplementation of fermented blueberries (very rich in polyphenols) containing L. plantarum (2 g/day for 4 weeks, containing 109 CFU) reduced systolic (by approximately 45%) and diastolic (by approximately 45%) BP in hypertensive animals (Ahrén et al., 2015). Mechanistically, it has been suggested that fermentation of blueberries by L. plantarum could reduce BP trough a mechanism involving a nitric oxide (NO)-dependent pathway (Ahrén et al., 2015). However, another study showed that adding probiotics to a blueberry-enriched diet did not enhance, and actually might have impaired the anti-hypertensive effect of blueberry consumption (Blanton et al., 2015).
In SHR, long-term administration of L. fermentum or L. coryniformis plus L. gasseri (3.3 × 1010 CFU/day, for 5 weeks) similarly induced a progressive reduction in the systolic arterial pressure without significant modifications of the HR (Gómez-Guzmán et al., 2015). This finding was linked to improved endothelial function, reduced vascular oxidative stress and decreased vascular inflammation in the aorta of SH rats (Gómez-Guzmán et al., 2015). Interestingly, recombinant L. plantarum expressing angiotensin converting enzyme inhibitory peptide was effective in the diminution of BP in SHR. This finding was linked to increased levels of NO, as well as decreased levels of endothelin and angiotensin II in plasma, heart, and kidney in SHR (Yang et al., 2015).
The treatment with the probiotic formulation termed VSL#3 (Streptococcus thermophilus, B. longum, B. breve, B. infantis, L. acidophilus, L. plantarum, L. casei, L. bulgaricus) prevented endothelial dysfunction and improved vascular oxidative stress most likely by reducing bacterial translocation and the local angiotensin system in the mesenteric artery of rats with portal hypertension (Rashid et al., 2014). Another mechanism involved in the antihypertensive effect of probiotics is the production of bioactive peptides with angiotensin converting enzyme (ACE) inhibitory properties during the fermentation process (Thushara et al., 2016). ACE inhibition, in turn, lowers the synthesis of angiotensin II, which result in attenuation of vasoconstriction and blood pressure.
Initial clinical testing of the hypothesis that probiotics could reduce BP has been performed in small-scale, double blind, placebo-controlled studies. For example, supplementation of the diet with L. plantarum for 6 week in a population of smokers of both genders resulted in reduced systolic BP, improvement of metabolic alterations and attenuated generation of reactive oxygen species (Naruszewicz et al., 2002). Nevertheless, in an investigation in postmenopausal women with metabolic syndrome, a 14 days supplementation with fermented or non-fermented milk supplemented with L. plantarum, did not result in an improvement of systolic or diastolic BP. However, a significant reduction in total cholesterol, low-density protein cholesterol, glucose, homocysteine and inflammatory biomarkers was observed (Barreto et al., 2014), although this was not associated to reduced arterial BP, perhaps because of the short duration of the study. Similarly, administration to obese hypertensive patients of an hypocaloric diet (1500 kcal/day), supplemented with cheese containing the probiotic L. plantarum showed a remarkable reduction of body mass index associated with decrease of BP when compared to a control group receiving the same diet without probiotic supplementation (Sharafedtinov et al., 2013).
In a randomized double-blind clinical trial on type 2 diabetic volunteers, the supplementation with probiotic soymilk (containing L. planetarium A7) did not change the anthropometric parameters (represented by body mass index and waist to hip ratio), however, it reduced both systolic and diastolic BP (Hariri et al., 2015).
On the other hand, a 6-weeks randomized, controlled, parallel, double blind, factorial study performed in overweight men and women, demonstrated that consumption of L. acidophilus and B. animalis (at a dose of 3 × 109 CFU/day) did not significantly alter BP, HR, total cholesterol, lox density lipoprotein, high density lipoprotein, or triglycerides (Ivey et al., 2015). Similarly, another double-blind randomized controlled study, found that L. acidophilus and B. bifidum supplementation did not reduce systolic or diastolic BP in healthy adults with hypercholesterolemia (Rerksuppaphol and Rerksuppaphol, 2015). These findings suggest that the choice of an appropriate strain, as also the optimal dosage is crucial to achieve ideal beneficial effects from probiotics.
The experimental and clinical findings summarized in this review suggest that dietary polyphenols or probiotic consumption may reduce BP and improve cardiovascular risk markers. Future studies investigating the effects of different polyphenolic compounds and probiotics, optimal dosage, intervention times, and studies on the underlying molecular mechanisms leading to improved control of BP are recommended to clarify the beneficial effects of dietary polyphenols and probiotics on AH. In addition, studies are needed to investigate the combined supplementation with dietary polyphenols and probiotics on the BP levels.
JB and LP drafted the work and revised critically for important intellectual content, wrote the paper, and performed the final review of the manuscript. Vd, MC, MM, VB, JC, CL, and HV contributed to the conception of the work and performed the final review of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Agrawal, Y. O., Sharma, P. K., Shrivastava, B., Ojha, S., Upadhya, H. M., Arya, D. S., et al. (2014). Hesperidin produces cardioprotective activity via PPAR-gamma pathway in ischemic heart disease model in diabetic rats. PLoS ONE 9:e111212. doi: 10.1371/journal.pone.0111212
Ahrén, I. L., Xu, J., Önning, G., Olsson, C., Ahrné, S., and Molin, G. (2015). Antihypertensive activity of blueberries fermented by Lactobacillus plantarum DSM 15313 and effects on the gut microbiota in healthy rats. Clin. Nutr. 34, 719–726. doi: 10.1016/j.clnu.2014.08.009
Amiot, M. J., Riva, C., and Vinet, A. (2016). Effects of dietary polyphenols on metabolic syndrome features in humans: a systematic review. Obes. Rev. 17, 573–586. doi: 10.1111/obr.12409
Anhê, F. F., Pilon, G., Roy, D., Desjardins, Y., Levy, E., and Marette, A. (2016). Triggering Akkermansia with dietary polyphenols: a new weapon to combat the metabolic syndrome? Gut Microbes 7, 146–153. doi: 10.1080/19490976.2016.1142036
Anhê, F. F., Roy, D., Pilon, G., Dudonné, S., Matamoros, S., Varin, T. V., et al. (2015). A polyphenol-rich cranberry extract protects from diet-induced obesity, insulin resistance and intestinal inflammation in association with increased Akkermansia spp. population in the gut microbiota of mice. Gut 64, 872–883. doi: 10.1136/gutjnl-2014-307142
Annuzzi, G., Bozzetto, L., Costabile, G., Giacco, R., Mangione, A., Anniballi, G., et al. (2014). Diets naturally rich in polyphenols improve fasting and postprandial dyslipidemia and reduce oxidative stress: a randomized controlled trial. Am. J. Clin. Nutr. 99, 463–471. doi: 10.3945/ajcn.113.073445
Bäckhed, F., Ding, H., Wang, T., Hooper, L. V., Koh, G. Y., Nagy, A., et al. (2004). The gut microbiota as an environmental factor that regulates fat storage. Proc. Natl. Acad. Sci. U.S.A. 101, 15718–15723. doi: 10.1073/pnas.0407076101
Barreto, F. M., Colado Simão, A. N., Morimoto, H. K., Batisti Lozovoy, M. A., Dichi, I., and Helena da Silva Miglioranza, L. (2014). Beneficial effects of Lactobacillus plantarum on glycemia and homocysteine levels in postmenopausal women with metabolic syndrome. Nutrition 30, 939–942. doi: 10.1016/j.nut.2013.12.004
Baur, J. A., Pearson, K. J., Price, N. L., Jamieson, H. A., Lerin, C., Kalra, A., et al. (2006). Resveratrol improves health and survival of mice on a high-calorie diet. Nature 444, 337–342. doi: 10.1038/nature05354
Bjerregaard, P. (2010). Nutritional transition – where do we go from here? J. Hum. Nutr. Diet. 23(Suppl. 1), 1–2. doi: 10.1111/j.1365-277X.2010.01091.x
Blanton, C., He, Z., Gottschall-Pass, K. T., and Sweeney, M. I. (2015). Probiotics blunt the anti-hypertensive effect of blueberry feeding in hypertensive rats without altering hippuric acid production. PLoS ONE 10:e0142036. doi: 10.1371/journal.pone.0142036
Brüll, V., Burak, C., Stoffel-Wagner, B., Wolffram, S., Nickenig, G., Muller, C., et al. (2015). Effects of a quercetin-rich onion skin extract on 24 h ambulatory blood pressure and endothelial function in overweight-to-obese patients with (pre-)hypertension: a randomised double-blinded placebo-controlled cross-over trial. Br. J. Nutr. 114, 1263–1277. doi: 10.1017/S0007114515002950
Brüll, V., Burak, C., Stoffel-Wagner, B., Wolffram, S., Nickenig, G., Muller, C., et al. (2016). Acute intake of quercetin from onion skin extract does not influence postprandial blood pressure and endothelial function in overweight-to-obese adults with hypertension: a randomized, double-blind, placebo-controlled, crossover trial. Eur. J. Nutr. doi: 10.1007/s00394-016-1185-1. [Epub ahead of print].
Buettner, R., Schölmerich, J., and Bollheimer, L. C. (2007). High-fat diets: modeling the metabolic disorders of human obesity in rodents. Obesity (Silver. Spring). 15, 798–808. doi: 10.1038/oby.2007.608
Cani, P. D. (2014). Metabolism in 2013: The gut microbiota manages host metabolism. Nat. Rev. Endocrinol. 10, 74–76. doi: 10.1038/nrendo.2013.240
Care, A. S., Sung, M. M., Panahi, S., Gragasin, F. S., Dyck, J. R., Davidge, S. T., et al. (2016). Perinatal resveratrol supplementation to spontaneously hypertensive rat dams mitigates the development of hypertension in adult offspring. Hypertension 67, 1038–1044. doi: 10.1161/HYPERTENSIONAHA.115.06793
Carthy, E. R. (2014). Autonomic dysfunction in essential hypertension: a systematic review. Ann. Med. Surg. (Lond.). 3, 2–7. doi: 10.1016/j.amsu.2013.11.002
Champagne, C. P., Ross, R. P., Saarela, M., Hansen, K. F., and Charalampopoulos, D. (2011). Recommendations for the viability assessment of probiotics as concentrated cultures and in food matrices. Int. J. Food Microbiol. 149, 185–193. doi: 10.1016/j.ijfoodmicro.2011.07.005
Chen, S., Zhao, X., Ran, L., Wan, J., Wang, X., Qin, Y., et al. (2015). Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: a randomized controlled trial. Dig. Liver Dis. 47, 226–232. doi: 10.1016/j.dld.2014.11.015
Choi, J. S., Islam, M. N., Ali, M. Y., Kim, E. J., Kim, Y. M., and Jung, H. A. (2014). Effects of C-glycosylation on anti-diabetic, anti-Alzheimer's disease and anti-inflammatory potential of apigenin. Food Chem. Toxicol. 64, 27–33. doi: 10.1016/j.fct.2013.11.020
Corry, D. B., and Tuck, M. L. (1999). Obesity, hypertension, and sympathetic nervous system activity. Curr. Hypertens. Rep. 1, 119–126. doi: 10.1007/s11906-999-0005-x
Davinelli, S., and Scapagnini, G. (2016). Polyphenols: a Promising Nutritional Approach to Prevent or Reduce the Progression of Prehypertension. High Blood Press. Cardiovasc. Prev. 23, 197–202. doi: 10.1007/s40292-016-0149-0
de Brito Alves, J. L., Nogueira, V. O., Cavalcanti Neto, M. P., Leopoldino, A. M., Curti, C., Colombari, D. S., et al. (2015). Maternal protein restriction increases respiratory and sympathetic activities and sensitizes peripheral chemoreflex in male rat offspring. J. Nutr. 145, 907–914. doi: 10.3945/jn.114.202804
Ding, S., Chi, M. M., Scull, B. P., Rigby, R., Schwerbrock, N. M., Magness, S., et al. (2010). High-fat diet: bacteria interactions promote intestinal inflammation which precedes and correlates with obesity and insulin resistance in mouse. PLoS ONE 5:e12191. doi: 10.1371/journal.pone.0012191
Dolinsky, V. W., Chakrabarti, S., Pereira, T. J., Oka, T., Levasseur, J., Beker, D., et al. (2013). Resveratrol prevents hypertension and cardiac hypertrophy in hypertensive rats and mice. Biochim. Biophys. Acta 1832, 1723–1733. doi: 10.1016/j.bbadis.2013.05.018
Edwards, R. L., Lyon, T., Litwin, S. E., Rabovsky, A., Symons, J. D., and Jalili, T. (2007). Quercetin reduces blood pressure in hypertensive subjects. J. Nutr. 137, 2405–2411.
Estruch, R., Ros, E., and Martinez-Gonzalez, M. A. (2013). Mediterranean diet for primary prevention of cardiovascular disease. N. Engl. J. Med. 369, 676–677. doi: 10.1056/nejmoa1200303
Ettinger, G., MacDonald, K., Reid, G., and Burton, J. P. (2014). The influence of the human microbiome and probiotics on cardiovascular health. Gut Microbes 5, 719–728. doi: 10.4161/19490976.2014.983775
Faghihzadeh, F., Adibi, P., and Hekmatdoost, A. (2015). The effects of resveratrol supplementation on cardiovascular risk factors in patients with non-alcoholic fatty liver disease: a randomised, double-blind, placebo-controlled study. Br. J. Nutr. 114, 796–803. doi: 10.1017/S0007114515002433
Fröjdö, S., Durand, C., and Pirola, L. (2008). Metabolic effects of resveratrol in mammals–a link between improved insulin action and aging. Curr. Aging Sci. 1, 145–151. doi: 10.2174/1874609810801030145
Gómez-Guzmán, M., Toral, M., Romero, M., Jiménez, R., Galindo, P., Sánchez, M., et al. (2015). Antihypertensive effects of probiotics Lactobacillus strains in spontaneously hypertensive rats. Mol. Nutr. Food Res. 59, 2326–2336. doi: 10.1002/mnfr.201500290
Grosso, G., Stepaniak, U., Micek, A., Stefler, D., Bobak, M., and Pajak, A. (2016). Dietary polyphenols are inversely associated with metabolic syndrome in Polish adults of the HAPIEE study. Eur. J. Nutr. doi: 10.1007/s00394-016-1187-z. [Epub ahead of print].
Hariri, M., Salehi, R., Feizi, A., Mirlohi, M., Kamali, S., and Ghiasvand, R. (2015). The effect of probiotic soy milk and soy milk on anthropometric measures and blood pressure in patients with type II diabetes mellitus: a randomized double-blind clinical trial. ARYA Atheroscler. 11, 74–80.
Hedner, T., Kjeldsen, S. E., and Narkiewicz, K. (2012). State of global health–hypertension burden and control. Blood Press 21(Suppl 1), 1–2. doi: 10.3109/08037051.2012.704786
Hertog, M. G., Feskens, E. J., Hollman, P. C., Katan, M. B., and Kromhout, D. (1993). Dietary antioxidant flavonoids and risk of coronary heart disease: the Zutphen Elderly Study. Lancet 342, 1007–1011. doi: 10.1016/0140-6736(93)92876-U
Ikemura, M., Sasaki, Y., Giddings, J. C., and Yamamoto, J. (2012). Preventive effects of hesperidin, glucosyl hesperidin and naringin on hypertension and cerebral thrombosis in stroke-prone spontaneously hypertensive rats. Phytother. Res. 26, 1272–1277. doi: 10.1002/ptr.3724
Ingram, D. K., Zhu, M., Mamczarz, J., Zou, S., Lane, M. A., Roth, G. S., et al. (2006). Calorie restriction mimetics: an emerging research field. Aging Cell 5, 97–108. doi: 10.1111/j.1474-9726.2006.00202.x
Ivey, K. L., Hodgson, J. M., Kerr, D. A., Thompson, P. L., Stojceski, B., and Prince, R. L. (2015). The effect of yoghurt and its probiotics on blood pressure and serum lipid profile; a randomised controlled trial. Nutr. Metab. Cardiovasc. Dis. 25, 46–51. doi: 10.1016/j.numecd.2014.07.012
Jang, M., Cai, L., Udeani, G. O., Slowing, K. V., Thomas, C. F., Beecher, C. W., et al. (1997). Cancer chemopreventive activity of resveratrol, a natural product derived from grapes. Science 275, 218–220. doi: 10.1126/science.275.5297.218
Jankovic, I., Sybesma, W., Phothirath, P., Ananta, E., and Mercenier, A. (2010). Application of probiotics in food products–challenges and new approaches. Curr. Opin. Biotechnol. 21, 175–181. doi: 10.1016/j.copbio.2010.03.009
Jose, P. A., and Raj, D. (2015). Gut microbiota in hypertension. Curr. Opin. Nephrol. Hypertens. 24, 403–409. doi: 10.1097/MNH.0000000000000149
Khalesi, S., Sun, J., Buys, N., and Jayasinghe, R. (2014). Effect of probiotics on blood pressure: a systematic review and meta-analysis of randomized, controlled trials. Hypertension 64, 897–903. doi: 10.1161/HYPERTENSIONAHA.114.03469
Lilly, D. M., and Stillwell, R. H. (1965). Probiotics: growth-promoting factors produced by microorganisms. Science 147, 747–748. doi: 10.1126/science.147.3659.747
Liu, Y., Ma, W., Zhang, P., He, S., and Huang, D. (2015). Effect of resveratrol on blood pressure: a meta-analysis of randomized controlled trials. Clin. Nutr. 34, 27–34. doi: 10.1016/j.clnu.2014.03.009
Lockyer, S., Corona, G., Yaqoob, P., Spencer, J. P., and Rowland, I. (2015). Secoiridoids delivered as olive leaf extract induce acute improvements in human vascular function and reduction of an inflammatory cytokine: a randomised, double-blind, placebo-controlled, cross-over trial. Br. J. Nutr. 114, 75–83. doi: 10.1017/S0007114515001269
Lockyer, S., Rowland, I., Spencer, J. P., Yaqoob, P., and Stonehouse, W. (2016). Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids and inflammatory markers: a randomised controlled trial. Eur. J. Nutr. doi: 10.1007/s00394-016-1188-y. [Epub ahead of print].
Mahboobi, S., Iraj, B., Maghsoudi, Z., Feizi, A., Ghiasvand, R., Askari, G., et al. (2014). The effects of probiotic supplementation on markers of blood lipids, and blood pressure in patients with prediabetes: a randomized clinical trial. Int. J. Prev. Med. 5, 1239–1246.
Medina-Remón, A., Casas, R., Tressserra-Rimbau, A., Ros, E., Martínez-González, M. A., Fitó, M., et al. (2016). Polyphenol intake from a Mediterranean diet decreases inflammatory biomarkers related to atherosclerosis: A sub-study of The PREDIMED trial. Br. J. Clin. Pharmacol. doi: 10.1111/bcp.12986. [Epub ahead of print].
Mell, B., Jala, V. R., Mathew, A. V., Byun, J., Waghulde, H., Zhang, Y., et al. (2015). Evidence for a link between gut microbiota and hypertension in the Dahl rat. Physiol. Genomics 47, 187–197. doi: 10.1152/physiolgenomics.00136.2014
Mendes-Junior, L., Monteiro, M. M., Carvalho Ados, S., de Queiroz, T. M., and Braga Vde, A. (2013). Oral supplementation with the rutin improves cardiovagal baroreflex sensitivity and vascular reactivity in hypertensive rats. Appl. Physiol. Nutr. Metab. 38, 1099–1106. doi: 10.1139/apnm-2013-0091
Mogollon, J. A., Bujold, E., Lemieux, S., Bourdages, M., Blanchet, C., Bazinet, L., et al. (2013). Blood pressure and endothelial function in healthy, pregnant women after acute and daily consumption of flavanol-rich chocolate: a pilot, randomized controlled trial. Nutr. J. 12:41. doi: 10.1186/1475-2891-12-41
Moreno-Luna, R., Munoz-Hernandez, R., Miranda, M. L., Costa, A. F., Jimenez-Jimenez, L., Vallejo-Vaz, A. J., et al. (2012). Olive oil polyphenols decrease blood pressure and improve endothelial function in young women with mild hypertension. Am. J. Hypertens. 25, 1299–1304. doi: 10.1038/ajh.2012.128
Naruszewicz, M., Johansson, M. L., Zapolska-Downar, D., and Bukowska, H. (2002). Effect of Lactobacillus plantarum 299v on cardiovascular disease risk factors in smokers. Am. J. Clin. Nutr. 76, 1249–1255.
Novelle, M. G., Wahl, D., Diéguez, C., Bernier, M., and de Cabo, R. (2015). Resveratrol supplementation: where are we now and where should we go? Ageing Res. Rev. 21, 1–15. doi: 10.1016/j.arr.2015.01.002
Ozdal, T., Sela, D. A., Xiao, J., Boyacioglu, D., Chen, F., and Capanoglu, E. (2016). The reciprocal interactions between polyphenols and gut microbiota and effects on bioaccessibility. Nutrients 8:78. doi: 10.3390/nu8020078
Parvez, S., Malik, K. A., Ah Kang, S., and Kim, H. Y. (2006). Probiotics and their fermented food products are beneficial for health. J. Appl. Microbiol. 100, 1171–1185. doi: 10.1111/j.1365-2672.2006.02963.x
Popkin, B. M. (2011). Contemporary nutritional transition: determinants of diet and its impact on body composition. Proc. Nutr. Soc. 70, 82–91. doi: 10.1017/S0029665110003903
Psaltopoulou, T., Naska, A., Orfanos, P., Trichopoulos, D., Mountokalakis, T., and Trichopoulou, A. (2004). Olive oil, the Mediterranean diet, and arterial blood pressure: the Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 80, 1012–1018.
Rashid, S.K., Idris-Khodja, N., Auger, C., Alhosin, M., Boehm, N., Oswald-Mammosser, M., et al., (2014). Probiotics (VSL#3) prevent endothelial dysfunction in rats with portal hypertension: role of the angiotensin system. PLoS ONE 9:e97458. doi: 10.1371/journal.pone.0097458
Ras, R. T., Zock, P. L., Zebregs, Y. E., Johnston, N. R., Webb, D. J., and Draijer, R. (2013). Effect of polyphenol-rich grape seed extract on ambulatory blood pressure in subjects with pre- and stage I hypertension. Br. J. Nutr. 110, 2234–2241. doi: 10.1017/S000711451300161X
Rerksuppaphol, S., and Rerksuppaphol, L. (2015). A randomized double-blind controlled trial of lactobacillus acidophilus plus bifidobacterium bifidum versus placebo in patients with hypercholesterolemia. J. Clin. Diagn Res. 9, KC01–KC04. doi: 10.7860/jcdr/2015/11867.5728
Rivera-Espinoza, Y., and Gallardo-Navarro, Y. (2010). Non-dairy probiotic products. Food Microbiol. 27, 1–11. doi: 10.1016/j.fm.2008.06.008
Roohbakhsh, A., Parhiz, H., Soltani, F., Rezaee, R., and Iranshahi, M. (2015). Molecular mechanisms behind the biological effects of hesperidin and hesperetin for the prevention of cancer and cardiovascular diseases. Life Sci. 124, 64–74. doi: 10.1016/j.lfs.2014.12.030
Sahebkar, A., Serban, C., Ursoniu, S., Wong, N. D., Muntner, P., Graham, I. M., et al. (2015). Lack of efficacy of resveratrol on C-reactive protein and selected cardiovascular risk factors–Results from a systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol. 189, 47–55. doi: 10.1016/j.ijcard.2015.04.008
Schwarzer, M., Makki, K., Storelli, G., Machuca-Gayet, I., Srutkova, D., Hermanova, P., et al. (2016). Lactobacillus plantarum strain maintains growth of infant mice during chronic undernutrition. Science 351, 854–857. doi: 10.1126/science.aad8588
Serban, M. C., Sahebkar, A., Zanchetti, A., Mikhailidis, D. P., Howard, G., Antal, D., et al. (2016). Effects of quercetin on blood pressure: a systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 5:e002713. doi: 10.1161/JAHA.115.002713
Sharafedtinov, K. K., Plotnikova, O. A., Alexeeva, R. I., Sentsova, T. B., Songisepp, E., Stsepetova, J., et al. (2013). Hypocaloric diet supplemented with probiotic cheese improves body mass index and blood pressure indices of obese hypertensive patients–a randomized double-blind placebo-controlled pilot study. Nutr. J. 12:138. doi: 10.1186/1475-2891-12-138
Sharma, M., Akhtar, N., Sambhav, K., Shete, G., Bansal, A. K., and Sharma, S. S. (2015). Emerging potential of citrus flavanones as an antioxidant in diabetes and its complications. Curr. Top. Med. Chem. 15, 187–195. doi: 10.2174/1568026615666141209163013
Sharma, M., and Devi, M. (2014). Probiotics: a comprehensive approach toward health foods. Crit. Rev. Food Sci. Nutr. 54, 537–552. doi: 10.1080/10408398.2011.594185
Sigel, H., Fischer, B., and Prijs, B. (1977). Biological implications from the stability of ternary complexes in solution.1 Mixed-ligand complexes with manganese (II) and other 3d ions. J. Am. Chem. Soc. 99, 4489–4496. doi: 10.1021/ja00455a047
Stevens, J. F., and Maier, C. S. (2016). The chemistry of gut microbial metabolism of polyphenols. Phytochem. Rev. 15, 425–444. doi: 10.1007/s11101-016-9459-z
Tapsell, L. C. (2015). Fermented dairy food and CVD risk. Br. J. Nutr. 113(Suppl 2), S131–S135. doi: 10.1017/s0007114514002359
Thushara, R. M., Gangadaran, S., Solati, Z., and Moghadasian, M. H. (2016). Cardiovascular benefits of probiotics: a review of experimental and clinical studies. Food Funct. 7, 632–642. doi: 10.1039/C5FO01190F
van der Made, S. M., Plat, J., and Mensink, R. P. (2015). Resveratrol does not influence metabolic risk markers related to cardiovascular health in overweight and slightly obese subjects: a randomized, placebo-controlled crossover trial. PLoS ONE 10:e0118393. doi: 10.1371/journal.pone.0118393
Vijaya Kumar, B., Vijayendra, S. V., and Reddy, O. V. (2015). Trends in dairy and non-dairy probiotic products - a review. J. Food Sci. Technol. 52, 6112–6124. doi: 10.1007/s13197-015-1795-2
Vitali, B., Minervini, G., Rizzello, C. G., Spisni, E., Maccaferri, S., Brigidi, P., et al. (2012). Novel probiotic candidates for humans isolated from raw fruits and vegetables. Food Microbiol. 31, 116–125. doi: 10.1016/j.fm.2011.12.027
Wilmsen, P. K., Spada, D. S., and Salvador, M. (2005). Antioxidant activity of the flavonoid hesperidin in chemical and biological systems. J. Agric. Food Chem. 53, 4757–4761. doi: 10.1021/jf0502000
Wohlgemuth, S., Loh, G., and Blaut, M. (2010). Recent developments and perspectives in the investigation of probiotic effects. Int. J. Med. Microbiol. 300, 3–10. doi: 10.1016/j.ijmm.2009.08.003
Wong, R. H., Howe, P. R., Buckley, J. D., Coates, A. M., Kunz, I., and Berry, N. M. (2011). Acute resveratrol supplementation improves flow-mediated dilatation in overweight/obese individuals with mildly elevated blood pressure. Nutr. Metab. Cardiovasc. Dis. 21, 851–856. doi: 10.1016/j.numecd.2010.03.003
Wu, J. M., Hsieh, T. C., and Wang, Z. (2011). Cardioprotection by resveratrol: a review of effects/targets in cultured cells and animal tissues. Am. J. Cardiovasc. Dis. 1, 38–47.
Yamamoto, M., Suzuki, A., and Hase, T. (2008). Short-term effects of glucosyl hesperidin and hesperetin on blood pressure and vascular endothelial function in spontaneously hypertensive rats. J. Nutr. Sci. Vitaminol. 54, 95–98. doi: 10.3177/jnsv.54.95
Keywords: probiotics, hypertension, blood pressure, dietary polyphenols
Citation: de Brito Alves JL, de Sousa VP, Cavalcanti Neto MP, Magnani M, Braga VA, Costa-Silva JH, Leandro CG, Vidal H and Pirola L (2016) New Insights on the Use of Dietary Polyphenols or Probiotics for the Management of Arterial Hypertension. Front. Physiol. 7:448. doi: 10.3389/fphys.2016.00448
Received: 22 May 2016; Accepted: 20 September 2016;
Published: 06 October 2016.
Edited by:
Jean-Pierre Montani, University of Fribourg, SwitzerlandReviewed by:
Sergio Davinelli, University of Molise, ItalyCopyright © 2016 de Brito Alves, de Sousa, Cavalcanti Neto, Magnani, Braga, Costa-Silva, Leandro, Vidal and Pirola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José L. de Brito Alves, am9zZV9sdWl6XzYxQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.