 Herbert F. Jelinek
Herbert F. Jelinek Zhaoqi Q. Huang4,5
Zhaoqi Q. Huang4,5 Ahsan H. Khandoker
Ahsan H. Khandoker Hosen Kiat
Hosen Kiat- 1Australian School of Advanced Medicine, Macquarie University, Sydney, NSW, Australia
- 2Department of Biomedical Engineering, Khalifa University of Science, Technology and Research, Abu Dhabi, United Arab Emirates
- 3School of Community Health, Charles Sturt University, Albury, NSW, Australia
- 4Department of Cardiology, The Third Affiliated Hospital of Guangzhou Medical College, Guangzhou, China
- 5Department of Cardiac Rehabilitation, Sydney Adventist Hospital, Sydney, NSW, Australia
- 6Centre for Complementary Medicine Research, University of Western Sydney, Sydney, NSW, Australia
Coronary artery events requiring intervention are associated with depressed cardiac autonomic function. Whether a 6-week cardiac rehabilitation (CR) differs in effectiveness in improving exercise capacity (6MWT), cardiorespiratory function (peakVO2), and autonomic function (HRV) following either cardiac bypass surgery (CABG) or percutaneous coronary revascularization (PCI) is unknown. The current study therefore compared the change in 6MWT and peak VO2 to HRV variables following a 6-week CR program and with patients having either PCI or CABG. Thirty-eight patients, (PCI, n = 22 and CABG, n = 16) participated in the CR program and results for pre and post 6 min walk test (6MWT), peakVO2, and heart rate variability (HRV) were obtained. Our study has shown that a 6 weeks program following either PCI or CABG improves function. However, the effect on post-CABG differs to that of post-PCI patients. The change in distance walked (6MWT, metres) was higher in the CABG (Δ6MWT: 61, p < 0.001) compared to the PCI group (Δ6MWT: 41, p < 0.001). Maximum exercise capacity (peak VO2, ml/kg.min) also changed significantly with a greater change in the CABG group (ΔPCI: 0.7, p < 0.001; ΔCABG: 1.0, p < 0.001) but did not reach normal population values. Although an improvement in HRV parameters was noted for the PCI group, a statistically significant improvement in HRV was observed only in the CABG group for the following; SDNN (ms) (baseline vs. post-rehabilitation (median ± IQR): 31.2 ± 25.6 vs. 51.8 ± 23.1, p < 0.01), RMSSD (19.32 ± 19.9 vs. 42.1 ± 34.2, p < 0.01); LF (ms2) (191 ± 216 vs. 631 ± 693, p < 0.01) and HF (107 ± 201 vs. 449 ± 795.0, p < 0.05). A significant interaction in the PCI group but not in the CABG group was observed using correlation analysis between the 6MWT and peak VO2 with HRV parameters indicating that being healthier that is, a better 6MWT and peak VO2 led to better HRV results but no significant effect of CR in the PCI group. When the results were investigated for baseline 6MWT and peak VO2 effect using a covariate analysis, a significant influence of CR on HRV parameters was retained in the CABG group (p = 0.0072). Our study indicates that a 6-weeks CR program benefits both patient groups in terms of exercise capacity, cardiorespiratory function and autonomic nervous system modulation of heart rate, with CABG patients showing the most improvement. HRV can be a useful additional variable to gauge cardiac function following CR.
Introduction
Percutaneous coronary angioplasty intervention (PCI) and coronary artery bypass grafting (CABG) are effective and established treatments for clinically significant coronary artery disease (CAD) (Eagle et al., 2004; Bravata et al., 2007). The long-term survival benefits of cardiac rehabilitation (CR) among patients with CAD have been documented following several large-scale trials and meta-analyses with no direct comparisons between cardiac intervention (CABG vs. PCI) or current measures, including the 6-min walk test and peak oxygen volume (6MWT, peak VO2) (Giannuzzi et al., 2003; Taylor et al., 2004; Leon et al., 2005; Suaya et al., 2009). In recent papers there has been some speculation this may be due to an improvement in cardiac autonomic function (Lucini et al., 2002; Routledge et al., 2010).
The 6MWT is now used routinely to demonstrate the physical and physiological benefits of CR following coronary intervention with peak VO2 still used in major metropolitan hospitals (Fiorina et al., 2007). Recently Soumagne reported improvement in functional capacity following CR but did not report direct comparisons between PCI and CABG (Soumagne, 2012).
Heart rate variability (HRV) is a valid marker of cardiac autonomic activity and complexity that reflects sympathetic and parasympathetic balance and overall tone (Mäkikallio et al., 2006; Jelinek et al., 2010; McLachlan et al., 2010). HRV can be measured in both time and frequency domains, where global activity in the time domain is indicated by the standard deviation of the RR intervals (SDNN) and parasympathetic function by the root mean square of the standard deviation of the RR intervals (RMSSD) (TFESC, 1996). Sympathetic output in the frequency domain is loosely correlated with low frequency (LF) power, although a parasympathetic component has been noted, while parasympathetic/vagal output is in part correlated with high frequency (HF) power of the HRV spectrum (Grassi et al., 2009). The LF/HF ratio is a derived value from the calculated HF and LF spectral component (Reed et al., 2005; Billman, 2013). Reduced HRV may be associated with abnormal adaptability of the cardiac autonomic nervous system to changes in cardiac pathology and may increase risk of adverse or fatal cardiac events (Kleiger et al., 1987; Quintana et al., 1997; Weber et al., 1999; Jelinek et al., 2010).
Parasympathetic indices are reduced in patients within 24 h after PCI (Tseng et al., 1996; Osterhues et al., 1998; Wennerblom et al., 2000; Kanadasi et al., 2002). However, this reduction in parasympathetic function appears to be a transient phenomenon (Osterhues et al., 1998; Kanadasi et al., 2002; Janowska-Kulińska et al., 2009). In patients with greater than one target-vessel affected and/or with other comorbidities, HRV remains lower due to several factors (Tseng et al., 1996; Birand et al., 1998; Wennerblom et al., 2000; Kanadasi et al., 2002). In advanced heart failure with low left ventricular ejection fraction autonomic dysfunction may be due to a decrease in muscarinic receptor density, or changes in neuro-hormonal output leading to a decrease in parasympathetic output and an increase in sympathetic activity (Eckberg et al., 1971). In further studies, HRV has been shown to be independent of ejection fraction, extent of CAD and other variables, where a decreased HRV is a potent independent predictor of mortality in the 12 months following elective coronary angiography in patients without recent myocardial infarction (Rich et al., 1988). A number of studies have found that CR can improve both HRV and exercise capacity in patients following PCI (Chien et al., 2006; Munk et al., 2009; Baumert et al., 2011).
In general, outcomes for post-CABG reported in earlier studies differ to PCI in that impairment of cardiac autonomic regulation assessed by HRV remains suboptimal for several months or years post CABG and an increased risk of atrial fibrillation remains present (Demirel et al., 2002; Bauernschmitt et al., 2004; Cygankiewicz et al., 2004; Wu et al., 2005; Laitio et al., 2006; Kalisnik et al., 2007). Accordingly, strategies resulting in favorable recovery of cardiac autonomic tone as soon as possible after CABG may be clinically important in these patients. Long-term outpatient exercise-based CR has been reported to positively improve exercise capacity and cardiac autonomic function post-CABG hospital discharge in programs of 2 months duration or longer (Hirschhorn et al., 2008; Baumert et al., 2011). However, data evaluating the impact of CR on HRV in outpatients after CABG are limited (Iellamo et al., 2000; Baumert et al., 2011). It is uncertain whether short-term CR applied post-CABG during an outpatient CR program has a substantial beneficial impact on HRV and how this compares to current measures of exercise capacity (6MWT) and cardiorespiratory function (peak VO2). No study has directly compared the physiological parameters measured as 6MWT and peak VO2 and cardiac autonomic function improvements for CABG and PCI patients following a 6-week CR program.
The current study prospectively compared the impact of a 6 weeks CR program on baseline HRV parameters and exercise capacity outcomes with patients recovering from both PCI and CABG in a standardized program.
Methods
Participants
The project was conducted in accordance with ethics guidelines and approval by the Sydney Adventist Hospital and Charles Sturt University Human Ethics Research Committee. All participants were provided with an information sheet and gave informed consent.
The participants who agreed to participate in this study were prospectively and consecutively enrolled between July and December 2010 and part of the CR program at the Sydney Adventist Hospital, Wahroonga, NSW, Australia. All patients had revascularization procedures (either PCI or CABG) within 1 month of enrolment. Patients enrolled into CR were excluded from the study if the principal diagnosis was of cardiac failure, valvular surgery, or patients who had a documented myocardial infarction within 6 months prior to study enrolment. Participants were also excluded from the analysis if they were unable to complete the 6-week CR program or could not participate in the designated exercise program.
Rehabilitation Program
Exercise sessions were performed three times per week for 6 weeks at 55–70% of peak VO2, measured during the first exercise session at commencement of the CR program combined with a patient perceived exertion rating of 11–13 (fairly light to somewhat hard) on the Borg scale (Borg, 1982). The program included 16 periods of exercise training and six education sessions on cardiovascular risk factors, life style modification measures and the pathophysiology of atherosclerosis. The exercise component of the program was conducted according to the National Heart Foundation of Australia & Australian Cardiac Rehabilitation Association (NHFA and ACRA, 2004) guidelines. Each participant was given an individualized exercise program consisting of aerobic exercise (cycle ergometry, treadmill walking, and rowing) that was devised by an exercise physiologist to ensure the participants could exercise continually throughout the session at the prescribed level of intensity. Each session consisted of stretching and warm-up exercise (5–10 min), endurance training (15–20 min), resistance training (10–15 min), or strength training (10–15 min) and cool-down/relaxation exercise (5–10 min). Participants were also advised to complete a home walking program, as recommended by the National Heart Foundation to achieve 30 min of moderate intensity physical activity on most or all days of the week.
Data Collection
The 6-min walk test (6MWT) is a standard measure of functional walking capacity and as such provides insight into the likely effect of participation on patients' ability to carry out activities of daily living (Fiorina et al., 2007). This test consists of walking up and down an 18 m indoor track as many times as possible within a 6-min period (NHFA and ACRA, 2004; West et al., 2012). In accordance with the American Thoracic Society guidelines this test was conducted twice prior to commencing CR, with the better of the two tests recorded as baseline (Argyropoulos and Harper, 2002). Patients were allowed to rest if required, and the assessment was ceased if there was angina pectoris or undue shortness of breath, which would normally limit activity and/or necessitate the use of coronary vasodilator therapy. Patients were advised of elapsed time at each minute of the assessment. No other encouragement was given. The peak VO2 was collected throughout the 6MWT and calculated using the American College of Sports Medicine formula (ACSM, 2006).
A 20-min, 3-lead ECG recording (PowerLab 4/30, LabChart Version 7, Castle Hill, NSW, Australia) was obtained prior and post CR. Time series variables were analyzed over the 20-min recording range, whereas frequency domain measures were analyzed using the accepted 5-min successive interval method to avoid the influence of non-stationarity (Task Force, 1996). The time domain variables considered in this study were the mean RR interval and its standard deviation of the N-N intervals (SDNN), representing the overall HRV and its root mean square successive difference (rMSSD), representing the vagal tone. The frequency-domain variables measured were LF and HF and the ratio LF/HF, which provide information on vagal and sympathetic input modulating HRV (Carney et al., 2005).
Other information obtained from patients attending the CR included medications, blood pressure, smoking, and diabetes status. Height and weight were measured, and the body mass index (BMI) calculated. Waist circumference was measured within an accuracy of 0.1 cm. Blood pressure was measured with a clinical zero sphygmomanometer. The average of two measurements was used to determine blood pressure. A cardiac history questionnaire was given to all participants to ascertain any other factors that may impact on their exercise capacity and HRV.
Data Analysis
All the data were analyzed by LabChart version 7 (ADInstruments, Castle Hill, Sydney, Australia). In accordance with the American Thoracic Society guidelines (ATS, 2002), 6MWT results were expressed as an absolute value. Exercise capacity was expressed as peak VO2 in ml/kg.min.
Statistical analysis was performed using SPSS Version 20 (Copyright IBM Inc.). The Wilcoxon Signed-Ranks Test was used to compare HRV parameters for the CABG and PCI groups before and following CR. A student t-test was used to compare the 6MWT and peak VO2 results before and following CR. To assess the correlation on a nominal scale the Pearson's correlation test was used. Covariate analysis to model the influence of 6MWT and peak VO2 on effectiveness of CR was determined using Friedman's test. Differences were considered significant when p < 0.05. Values were expressed as means and standard deviation for normally distributed data and medians and interquartile range (IQR) if the data was not normally distributed.
Results
Baseline Values of Patients
Forty-two patients were consecutively enrolled after successful cardiac intervention procedures if they agree to the research and provided informed consent. The PCI group consisted of 25 patients and the CABG group of 17 patients. One patient was unable to complete the CR program, two missed the follow-up appointment and one patient was hospitalized during the rehabilitation program. No patients experienced angina during the exercise component of the rehabilitation program. Data from 22 patients in the PCI group and 16 patients in the CABG group were used for the final analysis.
There were no significant differences in risk profile including age, blood pressure, smoking, and diabetes, and clinical presentation between the two groups (Table 1). Medication use was similar between the two groups apart from a significant difference in the PCI group used angiotensin converting enzyme inhibitors (ACEI). One patient in the PCI group and two patients in the CABG group discontinued β-blocker therapy and were excluded from the analysis.
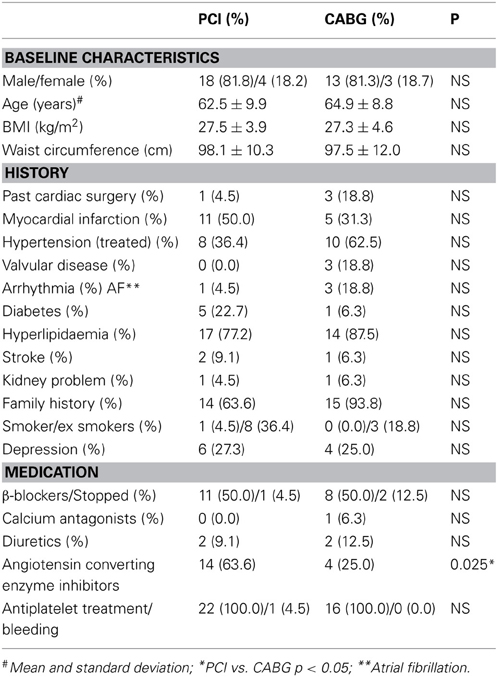
Table 1. Patient demographics and clinical history.
Clinical Variables
BMI and waist circumference were measured before and after CR. No significant differences were observed after the 6-week CR programme (Table 2).
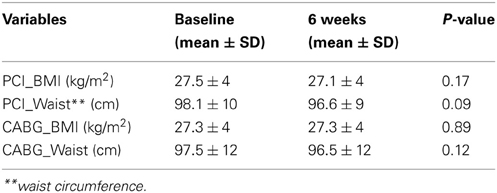
Table 2. BMI and waist circumference in the CABG and PCI groups.
Heart Rate Variability
Significant increases were seen for SDNN, RMSSD, LF, and HF in the CABG group following CR compared to baseline (Table 3).
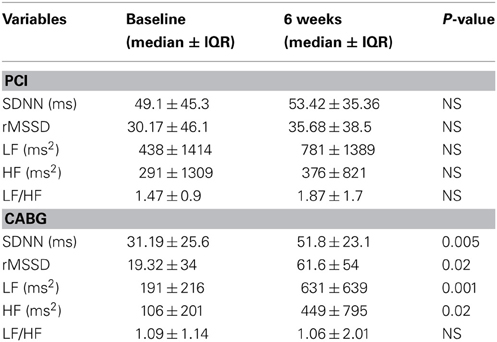
Table 3. Changes of the HRV indices in PCI and CABG group.
There was no significant change in HRV post CR in the PCI group for all HRV measures. Significant differences were seen for the majority of HRV measures for the CABG group when comparing post CR to baseline levels (Table 3).
Analysis of the difference in the extent of change (Δ) between the CABG and PCI groups for the time and frequency domain parameters following CR revealed no significant differences in the HRV parameters. However, CABG patients showed a greater improvement in all HRV measures.
A significant interaction in the PCI group but not in the CABG group was observed using covariant analysis between the 6MWT and peak VO2 with HRV parameters, indicating that being healthier that is, better 6MWT and peak VO2, led to better HRV results but no significant effect of CR in the PCI group. When the results were investigated for baseline 6MWT and peak VO2 in the CABG group a significant influence of CR on HRV parameters was retained in the CABG group (p = 0.0072).
Exercise Capacity
Clinically significant improvements in exercise capacity were observed in both PCI and CABG groups following CR as judged by the American Thoracic Society guidelines (2002), which stipulate that an increase of 54 m in the 6MWT is the minimum distance required (Table 4).
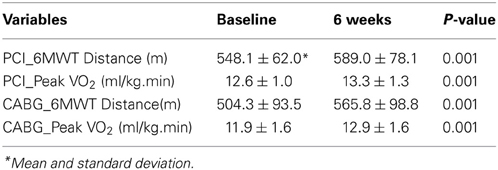
Table 4. 6MWT distance and metabolic variables in both groups at baseline and after 6 weeks.
Peak VO2 increased significantly in both groups. However, it remained below international and Australian population norms that are set between 20 and 35 ml/kg.min (see Table 4). CABG patients improved by 8% and PCI by 1% compared to baseline following the CR program.
Discussion
Our study is the first to investigate whether there is a difference in CR outcomes following a 6 week, moderate-intensity exercise program for patients that have undergone either CABG or PCI with differing levels of parasympathetic suppression at baseline (within the first month following intervention but immediately prior to rehabilitation). Effect of CR on HRV was compared to the traditional measures of 6MWT and peak VO2. CABG patients clearly entered the program with lower HRV parameters, particularly for LF power activity and total HRV, which may be due to more extensive myocardial or cardiovascular disease and the more invasive intervention (Santangeli et al., 2008; Lakusic et al., 2009). CABG intervention has been shown to decrease HRV post-CABG intervention with HRV parameters not improving past preoperative levels even after 6 months (Kuo et al., 1999). There were two principal findings: (1) CR significantly improved both HF power and LF power in the CABG group, which suggests significant changes to the extent or functionality of the autonomic nervous system, (2) CR had a significant impact on the exercise capacity in both groups. Our study also supports that a short 6-week CR program as recommended by the Australian guidelines is sufficient to improve exercise capacity, cardiorespiratory function regardless of intervention (PCI or CABG) and cardiac autonomic function in CABG patients (NHFA and ACRA, 2004). Our study agrees with previous reports that despite patients with diabetes having a higher risk of adverse cardiac events, adherence to a CR program can improve functional capacity (Hindman et al., 2005).
Time after intervention is an important component that influences CR outcomes. We recruited patients between 2 and 4 weeks after intervention and observed that the baseline values for HRV in the CABG group were much lower than for the PCI group in agreement with previous studies (Demirel et al., 2002; Cygankiewicz et al., 2004; Laitio et al., 2006). While there was a correlation between HRV parameters and 6MWT as well as peak VO2, this did not explain all the variance, hence indicating HRV is an independent physiological measure that provides information on the outcome of CR. HRV may be a more sensitive marker for effectiveness of improvement in cardiac function. HRV can be determined from 2-, 5-min, or longer lead II ECG recordings (Buchheit et al., 2007). 6MWT did show an improvement in both groups with only the CABG group meeting the recommended 56 meters cut-off compared to the PCI group. Peak VO2, demonstrated significant improvement as well for both groups, but results remained well below published population norms for our study and age range. This lower than previously reported outcome in peak VO2 may be due to higher baseline values on entry to the program especially in the PCI group or possibly due to patient motivation, home-based compliance, age, gender, and fitness of the patients. However, even modest improvements are correlated with better long-term outcomes in cardiorespiratory function (Swank et al., 2012).
CR has been demonstrated to decrease mortality following PCI (Goel et al., 2011) and either improved survival or morbidity compared to no CR following CABG in longitudinal studies (Hedbäck et al., 2001). However, comparative studies addressing CR effectiveness with respect to the type of cardiac intervention (PCI vs. CABG) and improvement in HRV compared to the traditional measures of 6MWT and peak VO2 has not been investigated in the one study design. Our study indicates that CR following CABG may improve long-term outcome by reducing the risk of future sudden cardiac death by increasing parasympathetic tone and therefore HRV (Peng et al., 1995).
The effectiveness of CR is influenced by type of surgery and length of rehabilitation program (Eagle et al., 2004). CABG patients usually have more than one target vessel involved, post-operative pain, morbidity, and hence their recovery period is often longer. Patients undergoing PCI, on the other hand, can begin CR 24–48 h after PCI if there is no evidence of hematoma at the catheterization site (West et al., 2012). Length of CR may be a factor in its effectiveness, with many studies reporting an 8-week period (Austin et al., 2004; Freyssin et al., 2012).
Our study shows in a single center cohort that CR consistently improved HRV in patients following CABG even when pre CR values of 6MWT and peak VO2 are considered.
Conclusion
This study indicates that the effect of CR is of benefit to patients with reduced parasympathetic tone prior to the start of CR and that CR has a greater effect in post-CABG compared to post-PCI. In addition HRV is independent of 6MWT and peakVO2, suggesting that HRV is a useful additional measure to employ for CR.
Author Contributions
Herbert F. Jelinek: Lead investigator, organized study protocol, data interpretation, statistical analysis, and writing; Zhaoqi Q. Huang: Cardiologist, performing all experimental work, data analysis, and writing; Hosen Kiat: Cardiologist in charge, responsible for developing exercise protocol for participants, study protocol, interpretation, and writing of article; Dennis Chang: Data interpretation and writing of article; Ahsan H. Khandoker: ECG analysis, data interpretation, and writing of article.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to the physical therapists James Bank and Alexandra Scott, for their care of the patients undergoing cardiac rehabilitation. We would like to acknowledge Ms Sharyn Scott for her assistance with co-ordinating the study and all the staff of Sydney Adventist Hospital who assisted in the study. Associate Professor Ian Spence for valuable comments on a previous draft of this manuscript. ECG analysis was performed by Salah Mohamed Widatalla. Herbert Jelinek is currently on leave from Charles Sturt University, Albury, Australia.
References
ACSM. (2006). “ACSM's guidelines for exercise testing and prescription,” in ACSM's Guidelines for Exercise Testing and Prescription, 7th Edn. ed M. H. Whaley (Philadelphia: Lippincott Williams and Wilkins).
Argyropoulos, G., and Harper, M.-E. (2002). Invited review: uncoupling proteins and thermoregulation. J. Appl. Physiol. 92, 2187–2198. doi: 10.1152/japplphysiol.00994.2001
ATS committee on proficiency standards for clinical pulmonary function laboratories. (2002). ATS statement: guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 166, 111–117. doi: 10.1164/ajrccm.166.1.at1102
Austin, J., Williams, R., Ross, L., Moseley, L., and Hutchison, S. (2004). Randomised control trial of cardiac rehabilitation in elderly patients with heart failure. Eur. J. Heart Fail. 7, 411–417. doi: 10.1016/j.ejheart.2004.10.004
Bauernschmitt, R., Malberg, H., Wessel, N., Kopp, B., Schirmbeck, E. U., and Lange, R. (2004). Impairment of cardiovascular autonomic control in patients early after cardiac surgery. Eur. J. Cardiothorac. Surg. 25, 320–326. doi: 10.1016/j.ejcts.2003.12.019
Baumert, M., Schlaich, M. P., Nalivaiko, E., Lambert, E., Sari, C. I., Kaye, D. M., et al. (2011). Relation between QT interval variability and cardiac sympathetic activity in hypertension. Am. J. Physiol. Heart Circ. Physiol. 300, H1412–H1417. doi: 10.1152/ajpheart.01184.2010
Billman, G. E. (2013). The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 4:26. doi: 10.3389/fphys.2013.00026
Birand, A., Kudaiberdieva, G. Z., Batyraliev, T. A., Akgul, F., and Saliu, S. (1998). Relationship between components of heart rate variability and doppler echocardiographic indices of left ventricular systolic performance in patients with coronary artery disease. Int. J. Angiol. 7, 244–248. doi: 10.1007/BF01617403
Borg, G. (1982). Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 14, 377–381. doi: 10.1249/00005768-198205000-00012
Bravata, D. M., Gienger, A. L., McDonald, K. M., Sundaram, V., Perez, M. V., Varghese, R., et al. (2007). Systematic review: the comparative effectiveness of percutaneous coronary interventions and coronary artery bypass graft surgery. Ann. Intern. Med. 147, 703–716. doi: 10.7326/0003-4819-147-10-200711200-00185
Buchheit, M., Papelier, Y., Laursen, P. B., and Ahmaidi, S. (2007). Noninvasive assessment of cardiac parasympathetic function: postexercise heart rate recovery or heart rate variability? Am. J. Physiol. Heart Circ. Physiol. 293, H8–H10. doi: 10.1152/ajpheart.00335.2007
Carney, R. M., Freedland, K. E., and Veith, R. C. (2005). Depression, the autonomic nervous system, and coronary heart disease. Psychosom. Med. 67, S29–S33. doi: 10.1097/01.psy.0000162254.61556.d5
Chien, M.-Y., Tsai, M.-W., and Wu, Y.-T. (2006). Does cardiac rehabilitation improve quality of life for a man with coronary artery disease who received percutaneous transluminal coronary angioplasty with insertion of a stent? Phys. Therapy 86, 1703–1710. doi: 10.2522/ptj.20050375
Cygankiewicz, I., Wranicz, J. K., Bolinska, H., Zaslonka, J., Jaszewski, R., and Zareba, W. (2004). Influence of coronary artery bypass grafting on heart rate turbulence parameters. Am. J. Cardiol. 94, 186–189. doi: 10.1016/j.amjcard.2004.03.059
Demirel, S., Akkaya, V., Oflaz, H., Tukek, T., and Erk, O. (2002). Heart rate variability after coronary artery bypass graft surgery: a prospective 3-year follow-up study. Ann. Noninvasive Electrocardiol. 7, 247–250. doi: 10.1111/j.1542-474X.2002.tb00171.x
Eagle, K. A., Guyton, R. A., Davidoff, R., Edwards, F. H., Ewy, G. A., Gardner, T. J., et al. (2004). ACC/AHA 2004 guideline update for coronary artery bypass graft surgery. Circulation 110, 1168–1176. doi: 10.1161/01.CIR.0000138790.14877.7D
Eckberg, D. L., Drabinsky, M., and Braunwald, E. (1971). Defective cardiac parasympathetic control in patients with heart disease. New Engl. J. Med. 285, 877–883. doi: 10.1056/NEJM197110142851602
Fiorina, C., Vizzardi, E., Lorusso, R., Maggio, M., De Cicco, G., Nodari, S., et al. (2007). The 6-min walking test early after cardiac surgery. Reference values and the effects of rehabilitation programme. Eur. J. Cardiothorac. Surg. 32, 724–729. doi: 10.1016/j.ejcts.2007.08.013
Freyssin, C., Verkindt, C., Prieur, F., Benaich, P., Maunier, S., and Blanc, P. (2012). Cardiac rehabilitation in chronic heart failure: effect of an 8-week, high-intensity interval training versus continuous training. Arch. Phys. Med. Rehabil. 93, 1359–1364. doi: 10.1016/j.apmr.2012.03.007
Giannuzzi, P., Mezzani, A., Saner, H., Björnstad, H., Fioretti, P., Mendes, M., et al. (2003). Physical activity for primary and secondary prevention. Position paper of the working group on cardiac rehabilitation and exercise physiology of the european society of cardiology. Eur. J. Cardiovasc. Prev. Rehabil. 10, 319. doi: 10.1097/01.hjr.0000086303.28200.50
Goel, K., Lennon, R. J., Tilbury, R. T., Squires, R. W., and Thomas, R. J. (2011). Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation 123, 2344–2352. doi: 10.1161/CIRCULATIONAHA.110.983536
Grassi, G., Arenare, F., Pieruzzi, F., Brambilla, G., and Mancia, G. (2009). Sympathetic activation in cardiovascular and renal disease. J. Nephrol. 22, 190–195.
Hedbäck, B., Perk, J., Härnblad, M., and Ohlsson, U. (2001). Cardiac rehabilitation after coronary artery bypass surgery: 10-year results on mortality, morbidity and readmissions to hospital. J. Cardiovasc. Risk 8, 153–158. doi: 10.1097/00043798-200106000-00006
Hindman, L., Falko, J. M., Lalonde, M., Snow, R., and Caulin-Glaser, T. (2005). Clinical profile and outcomes of diabetic and nondiabetic patients in cardiac rehabilitation. Am. Heart J. 150, 1046–1051. doi: 10.1016/j.ahj.2005.04.002
Hirschhorn, A. D., Richards, D., Mungovan, S. F., Morris, N. R., and Adams, L. (2008). Supervised moderate intensity exercise improves distance walked at hospital discharge following coronary artery bypass graft surgery–a randomised controlled trial. Heart Lung Circul. 17, 129–138. doi: 10.1016/j.hlc.2007.09.004
Iellamo, F., Legramante, J. M., Massaro, M., Raimondi, G., and Galante, A. (2000). Effects of a residential exercise training on baroreflex sensitivity and heart rate variability in patients with coronary artery disease. Circulation 102, 2588–2592. doi: 10.1161/01.CIR.102.21.2588
Janowska-Kulińska, A., Torzyñska, K., Markiewicz-Grochowalska, A., Sowiñska, A., Majewski, M., Jerzykowska, O., et al., (2009). Changes in heart rate variability caused by coronary angioplasty depend on the localisation of coronary lesions. Kardiol. Pol. 67, 130–138.
Jelinek, H. F., Khandoker, A., Palaniswami, M., and McDonald, S. (2010). “Tone-entropy analysis as a cardiac risk stratification tool,” in Computers in Cardiology, (Belfast: Conference Paper, IEEE Press), 955–958.
Kalisnik, J. M., Avbelj, V., Trobec, R., and Gersak, B. (2007). Position-dependent changes in vagal modulation after coronary artery bypass grafting. Comput. Biol. Med. 37, 1404–1408. doi: 10.1016/j.compbiomed.2006.11.002
Kanadasi, M., Kudaiberdieva, G., and Birand, A. (2002). Effect of the final coronary arterial diameter after coronary angioplasty on heart rate variability responses. Ann. Noninvasive Electrocardiol. 7, 106–113. doi: 10.1111/j.1542-474X.2002.tb00150.x
Kleiger, R. E., Miller, J. P., Bigger Jr, J. T., and Moss, A. J. (1987). Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 59, 256–262. doi: 10.1016/0002-9149(87)90795-8
Kuo, C.-D., Chen, G.-Y., Lai, S.-T., Wang, Y.-Y., Shih, C.-C., and Wang, J.-H. (1999). Sequential changes in heart rate variability after coronary artery bypass grafting. Am. J. Cardiol. 83, 776–779. doi: 10.1016/S0002-9149(98)00989-8
Laitio, T. T., Huikuri, H. V., Koskenvuo, J., Jalonen, J., Mäkikallio, T. H., Helenius, H., et al. (2006). Long-term alterations of heart rate dynamics after coronary artery bypass graft surgery. Anesth. Analg. 102, 1026–1031. doi: 10.1213/01.ane.0000198674.90500.59
Lakusic, N., Slivnjak, V., Baborski, F., and Cerovec, D. (2009). Heart rate variability after off-pump versus on-pump coronary artery bypass graft surgery. Cardiol. Res. Pract. 2009:295376. doi: 10.4061/2009/295376
Leon, A. S., Franklin, B. A., Costa, F., Balady, G. J., Berra, K. A., Stewart, K. J., et al. (2005). Cardiac rehabilitation and secondary prevention of coronary heart disease. Circulation 111, 369–376. doi: 10.1161/01.CIR.0000151788.08740.5C
Lucini, D., Milani, R. V., Costantino, G., Lavie, C. J., Porta, A., and Pagani, M. (2002). Effects of cardiac rehabilitation and exercise training on autonomic regulation in patients with coronary artery disease. Am. Heart J. 143, 977–983. doi: 10.1067/mhj.2002.123117
Mäkikallio, T. H., Barthel, P., Schneider, R., Bauer, A., Tapanainen, J. M., Tulppo, M. P., et al. (2006). Frequency of sudden cardiac death among acute myocardial infarction survivors with optimized medical and revascularization therapy. Am. J. Cardiol. 97, 480–484. doi: 10.1016/j.amjcard.2005.09.077
McLachlan, C. S., Ocsan, R., Spence, I., Hambly, B., Matthews, S., and Jelinek, H. F. (2010). HRV indices in association with physical activity and resting heart rate in bradycardia. BUMC Proc. 23, 368–370.
Munk, P. S., Staal, E. M., Butt, N., Isaksen, K., and Larsen, A. I. (2009). High-intensity interval training may reduce in-stent restenosis following percutaneous coronary intervention with stent implantation: a randomized controlled trial evaluating the relationship to endothelial function and inflammation. Am. Heart J. 158, 734–741. doi: 10.1016/j.ahj.2009.08.021
NHFA, and ACRA. (2004). Recommended Framework for Cardiac Rehabilitation. Canberra, ACT: National Heart Foundation of Australia and Australian Cardiac Rehabilitation Association.
Osterhues, H. H., Kochs, M., and Hombach, V. (1998). Time-dependent changes of heart rate variability after percutaneous transluminal angioplasty. Am. Heart J. 135, 755–761. doi: 10.1016/S0002-8703(98)70033-X
Peng, C. K., Havlin, S., Hausdorff, J. M., Mietus, J. E., Stanley, H. E., and Goldberger, A. L. (1995). Fractal mechanisms and heart rate dynamics: long-range correlations and their breakdown with disease. J. Electrocardiol. 28, 59–65. doi: 10.1016/S0022-0736(95)80017-4
Quintana, M., Storck, N., Lindblad, L., Lindvall, K., and Ericson, M. (1997). Heart rate variability as a means of assessing prognosis after acute myocardial infarction. Eur. Heart J. 18, 789. doi: 10.1093/oxfordjournals.eurheartj.a015344
Reed, M. J., Robertson, C. E., and Addison, P. S. (2005). Heart rate variability measurements and the prediction of ventricular arrhythmias. Q. J. Med. 98, 87–95. doi: 10.1093/qjmed/hci018
Rich, M. W., Saini, J. S., Kleiger, R. E., Carney, R. M., Tevelde, A., and Freedland, K. E. (1988). Correlation of heart rate variability with clinical and angiographic variables and late mortality after coronary angiography. Am. J. Cardiol. 62, 714–717. doi: 10.1016/0002-9149(88)91208-8
Routledge, F. S., Campbell, T. S., McFetridge-Durdle, J. A., and Bacon, S. L. (2010). Improvements in heart rate variability with exercise therapy. Can. J. Cardiol. 26, 303–312. doi: 10.1016/S0828-282X(10)70395-0
Santangeli, P., Sgueglia, G. A., Sestito, A., Lamendola, P., Mariani, L., Infusino, F., et al. (2008). Different effect of percutaneous and surgical coronary revascularization on cardiac autonomic function and inflammation in patients with stable angina. Int. J. Cardiol. 127, 269–270. doi: 10.1016/j.ijcard.2007.04.015
Suaya, J. A., Stason, W. B., Ades, P. A., Normand, S.-L. T., and Shepard, D. S. (2009). Cardiac rehabilitation and survival in older coronary patients. J. Am. Coll. Cardiol. 54, 25–33. doi: 10.1016/j.jacc.2009.01.078
Swank, A. M., Horton, J., Fleg, J. L., Fonarow, G. C., Keteyian, S., Goldberg, L., et al. (2012). Modest increase in peak VO2 is related to better clinical outcomes in chronic heart failure patients: results from heart failure and a controlled trial to investigate outcomes of exercise training (HF-ACTION). Circ. Heart Fail. 5, 579–585. doi: 10.1161/CIRCHEARTFAILURE.111.965186
Task Force. (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 93, 1043–1065. doi: 10.1161/01.CIR.93.5.1043
Taylor, R. S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani, H., Rees, K., et al. (2004). Exercise-based rehabilitation for patients with coronary artery disease: systematic review and meta-analysis of randomised controlled trials. Am. J. Med. 116, 682–692. doi: 10.1016/j.amjmed.2004.01.009
TFESC. (1996). Special report: heart rate variability standards of measurement, physiological interpretation, and clinical use. Circulation 93, 1043–1065. doi: 10.1161/01.CIR.93.5.1043
Tseng, C. D., Wang, T. L., Lin, J. L., Hsu, K. L., Chiang, F. T., and Tseng, Y. Z. (1996). The cause-effect relationship of sympathovagal activity and the outcome of percutaneous transluminal coronary angioplasty. Jpn. Heart J. 37, 455–462. doi: 10.1536/ihj.37.455
Weber, F., Schneider, H., Von Arnim, T., and Urbaszek, W. (1999). Heart rate variability and ischaemia in patients with coronary heart disease and stable angina pectoris. Eur. Heart J. 20, 38. doi: 10.1053/euhj.1998.1272
Wennerblom, B., Lurje, L., Solem, J., Tygesen, H., Uden, M., Vahisalo, R., et al. (2000). Reduced heart rate variability in ischemic heart disease is only partially caused by ischemia. An HRV study before and after PTCA. Cardiology 94, 146–151. doi: 10.1159/000047309
West, R. R., Jones, D. A., and Henderson, A. H. (2012). Rehabilitation after myocardial infarction trial (RAMIT): multi-centre randomised controlled trial of comprehensive cardiac rehabilitation in patients following acute myocardial infarction. Heart 98, 637–644. doi: 10.1136/heartjnl-2011-300302
Keywords: cardiac rehabilitation, exercise, percutaneous coronary angioplasty, coronary artery bypass drafting, heart rate variability
Citation: Jelinek HF, Huang ZQ, Khandoker AH, Chang D and Kiat H (2013) Cardiac rehabilitation outcomes following a 6-week program of PCI and CABG Patients. Front. Physiol. 4:302. doi: 10.3389/fphys.2013.00302
Received: 21 May 2013; Accepted: 02 October 2013;
Published online: 30 October 2013.
Edited by:
Karin Trimmel, Medical University of Vienna, AustriaReviewed by:
Peter Taggart, University College London, UKAlessandro Capucci, Universita' Politecnica delle Marche, Italy
Copyright © 2013 Jelinek, Huang, Khandoker, Chang and Kiat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Herbert F. Jelinek, School of Community Health, Charles Sturt University, Albury, 2640, Australia e-mail:aGplbGluZWtAY3N1LmVkdS5hdQ==